Venous Thromboembolism in Cancer: Role of LMWH and Optimal Duration of Therapy
|
|
|
- Eustace Parker
- 6 years ago
- Views:
Transcription
1 Venous Thromboembolism in Cancer: Role of LMWH and Optimal Duration of Therapy Craig M Kessler, MD MACP Lombardi Comprehensive Care Center Georgetown University Medical Center Washington, DC


2 COI Financial Disclosures Grant/Research Support: Bayer, GlaxoSmithKline, sanofi-aventis, Eisai Pharmaceuticals Consultant: Bayer, sanofi-aventis, Eisai Pharmaceuticals, Merck Speaker s Bureau: None

3 Cancer, Mortality, and VTE Epidemiology and Risk 4- to 6-fold increased risk for VTE in CA vs non-ca pts 3-fold increased risk for recurrent VTE in CA vs. non- CA patients CA patients undergoing surgery have a 2-fold increased risk for postoperative VTE Death rate from CA is four-fold higher if patient has concurrent VTE VTE 2 nd most common cause of death in ambulatory cancer patients (tied with infection) Heit et al Arch Int Med 2000;160: and 2002;162: ; Prandoni et al Blood 2002;100: ; White et al Thromb Haemost 2003;90: ; Sorensen et al New Engl J Med 2000;343: ); Levitan et al Medicine 1999;78: ; Khorana et al J Thromb Haemost 2007;5:632-4
4 Venous Thromboembolism in Cancer Patients Of all cases of VTE: 20% occur in cancer patients Of all cancer patients: 0.5% will have symptomatic VTE As high as 50% have VTE at autopsy Compared to patients without cancer: Higher risk of first and recurrent VTE (12/1000 vs 2/1000) Higher risk of bleeding on anticoagulants Higher risk of dying- VTE is 2 nd highest cause of death in hospitalized CA pts behind Ca alone VTE may be presenting sign of occult malignancy 10% with idiopathic VTE develop CA within 2 yrs 20% have recurrent idiopathic VTE 25% have bilateral DVT Lee & Levine. Circulation 2003;107:I17 I21; Blom et. al. JAMA 2005;293:715;; Bura et. al., J Thromb Haemost 2004;2:445-51
5 Interface of Clotting Activation and Tumor Biology Tumor Cell TF FVII/FVIIa Blood Coagulation Activation VEGF THROMBIN PAR-2 TF FIBRIN Angiogenesis IL-8 Angiogenesis Endothelial cells Falanga and Rickles, New Oncology:Thrombosis, 2005;1:9-16
6 VTE in Hospitalized Cancer Patients 7.0 VTE patients on chemotherapy VTE all patients 6.0 DVT all patients PE all patients 5.0 Rate of VTE (%) Cancer Years
7 Risk of VTE Varies Over The Natural History of Cancer Risk (Odds Ratio) Hospitalization Diagnosis Chemotherapy Metastasis Remission Time End of life Risk of VTE in the cancer population Risk of VTE in the general population (Rao MV, et al. In: Khorana and Francis, eds. Cancer-Associated Thrombosis; 2007)

8 Effect of Malignancy on Risk of VTE Population-based case-control (MEGA) study N=3220 consecutive patients with 1 st VTE vs. n=2131 control subjects CA patients = OR 7x VTE risk vs. non-ca patients 53.5 Adjusted odds ratio Hematologicall Lung Gastrointestinal Breast Distant metastases 0 to 3 months 3 to 12 months 1 to 3 years 5 to 10 years > 15 years Time from diagnosis Silver In: The Hematologist - modified from Blom et. al. JAMA 2005;293:715
9 Independent Risk Factors for DVT/PE Risk Factor/Characteristic Odds Ratio Recent surgery w/ institutionalization Trauma Institutionalization without recent surgery 7.98 Malignancy with chemotherapy 6.53 Prior CVAD or pacemaker 5.55 Prior superficial vein thrombosis 4.32 Malignancy without chemotherapy 4.05 Neurologic disease w/ extremity paresis 3.04 Serious liver disease 0.10 Heit JA, et al. Thromb Haemost. 2001;86:
10 VTE Incidence In Various Tumors (Otten, et al. Haemostasis 2000;30:72. Lee & Levine. Circulation 2003;107:I17). Oncology Setting Breast cancer (Stage I & II) w/o further tx Breast cancer (Stage I & II) w/ chemo Breast cancer (Stage IV) w/ chemo Non-Hodgkin s lymphomas w/ chemo Hodgkin s disease w/ chemo Advanced cancer (1-year survival=12%) High-grade glioma Multiple myeloma (thalidomide + chemo) Renal cell carcinoma Solid tumors (anti-vegf + chemo) VTE Incidence 0.2% 2% 8% 3% 6% 9% 26% 28% 43% 47%

11 A Meta-analysis: Relative risks of venous thromboembolism in cancer patients vs the general population Horsted F, et al. (2012) PLoS Med 9(7): e
12 Chemotherapy Regimens and Risks for VTE Chemotherapy Regimen VTE Rate (%) Thalidomide + gemcitabine + fluoururacil 43 Thalidomide + doxorubicin Bevacizumab + ESA 30 Thalidomide + Dexamethasone Cisplatin + gemcitabine 17.6 CMFVP 7-18 Fluouracil + leucovorin Lenalidomide + dexamethasone 9-15 Asparaginase 4-14 Bevacizumab 11 Epirubicin + cyclophosphamide 10 Cisplatin + bleomycin 8.4 Tamoxifen 0-8 Brown A. Am J Health-Syst Pharm. 69:2012
13 Antithrombotic Therapy: Choices Nonpharmacologic (Prophylaxis) Pharmacologic (Prophylaxis & Treatment) Intermittent Pneumatic Compression Elastic Stockings Unfractionated Heparin (UH) Low Molecular Weight Heparin (LMWH) and indirect anti-xa (Fondaparinux) Inferior Vena Cava Filter Oral Anticoagulants Novel Oral Agents: Direct anti-xa inhibitors Direct anti-iia, Inhibitors
14 Goals of VTE Treatment in the CA Patient Prevent fatal PE Prevent recurrent VTE and thrombus extension Minimize long term sequelae of VTE, e.g. Postthrombotic syndrome, pulmonary HBP, etc Avoid major bleeding complications Overcome anticoagulation resistance/hypercoag Circumvent drug-drug interactions and dietary variability Treat concurrent arterial thromboses Affect survival?
15 Thrombosis and Survival: Likelihood of Death After Hospitalization 1.00 DVT/PE and Malignant Disease Probability of Death Malignant Disease DVT/PE Only Nonmalignant Disease Number of Days Levitan N, et al. Medicine 1999;78:285
16 Long-term Treatment of Patients With PE: ACCP Evidence-Based Clinical Practice Guidelines, 9th ed, 2012 In patients with PE and active cancer, if there is a low or moderate bleeding risk, we recommend extended anticoagulant therapy over 3 months of therapy (Grade 1B), and if there is a high bleeding risk, we suggest extended anticoagulant therapy (Grade 2B). Remarks: In all patients who receive extended anticoagulant therapy, the continuing use of treatment should be reassessed at periodic intervals (eg, annually).
17 Long-term Treatment of Patients With PE: ACCP Evidence-Based Clinical Practice Guidelines, 9th ed, 2012 In patients with PE and cancer, we suggest LMWH over VKA therapy (Grade 2B). In patients with PE and cancer who are not treated with LMWH, we suggest VKA over dabigatran or rivaroxaban for long-term tx (Grade 2C). Remarks ( ): Choice of tx in pts with and without CA is sensitive to the individual pt's tolerance for daily injections, need for lab monitoring, and tx costs. Treatment of VTE with dabigatran or rivaroxaban, in addition to being less burdensome to patients, may prove to be associated with better clinical outcomes than VKA and LMWH therapy. When these guidelines were being prepared (October 2011), postmarketing studies of safety were not available. Given the paucity of currently available data and that new data are rapidly emerging, we give weak ecommendation in favor of VKA and LMWH therapy over dabigatran and rivaroxaban, and we have not made any recommendation in favor of one of the new agents over the other.
18 Duration of Long-term Anticoagulant Therapy ACCP Evidence-Based Clinical Practice Guidelines, 9th ed, 2012 In patients with DVT of the leg and active cancer, if the risk of bleeding is not high, we recommend extended anticoagulant therapy over 3 months of therapy (Grade 1B), and if there is a high bleeding risk, we suggest extended anticoagulant therapy (Grade 2B). Remarks (3.1.3, 3.1.4, ): Duration of treatment of patients with isolated distal DVT refers to patients in whom a decision has been made to treat with anticoagulant therapy; however, it is anticipated that not all patients who are diagnosed with isolated distal DVT will be given anticoagulants (see section 2.3). In all patients who receive extended anticoagulant therapy, the continuing use of treatment should be reassessed at periodic intervals (eg, annually).
19 Choice of Anticoagulant Regimen for Long-term Therapy ACCP Evidence-Based Clinical Practice Guidelines, 9th ed, 2012 In patients with DVT of the leg and cancer, we suggest LMWH over VKA therapy (Grade 2B). In patients with DVT and cancer who are not treated with LMWH, we suggest VKA over dabigatran or rivaroxaban for long-term therapy (Grade 2B). Remarks ( ): Choice of treatment in patients with and without cancer is sensitive to the individual patient's tolerance for daily injections, need for laboratory monitoring, and treatment costs. LMWH, rivaroxaban, and dabigatran are retained in patients with renal impairment, whereas this is not a concern with VKA. Treatment of VTE with dabigatran or rivaroxaban, in addition to being less burdensome to patients, may prove to be associated with better clinical outcomes than VKA and LMWH therapy. When these guidelines were being prepared (October 2011), postmarketing studies of safety were not available. Given the paucity of currently available data and that new data are rapidly emerging, we give a weak recommendation in favor of VKA and LMWH therapy over dabigatran and rivaroxaban, and we have not made any recommendations in favor of one of the new agents over the other.
20 Long-term Anticoagulation for Patients With UEDVT: ACCP Evidence-Based Clinical Practice Guidelines, 9th ed, 2012 In patients who have UEDVT that is associated with a central venous catheter that is removed, we recommend 3 months of anticoagulation over a longer duration of therapy in patients with no cancer (Grade 1B), and we suggest this in patients with cancer (Grade 2C). In patients who have UEDVT that is associated with a central venous catheter that is not removed, we recommend that anticoagulation is continued as long as the central venous catheter remains over stopping after 3 months of treatment in patients with cancer (Grade 1C), and we suggest this in patients with no cancer (Grade 2C).
21 Treatment of Cancer-Associated VTE Study Design Length of Therapy (Months) N Recurrent VTE (%) Major Bleeding (%) Death (%) CLOT Trial (Lee 2003) Dalteparin OAC NS NS CANTHENOX (Meyer 2002) Enoxaparin OAC LITE (Hull ISTH 2003) Tinzaparin OAC NS NS ONCENOX (Deitcher ISTH 2003) Enox (Low) Enox (High) OAC NS NS NR
22 PATIENT POPULATION CHARACTERISTICS CANTHANOX ONCENOX Main-LITE CLOT SEX 55% Female 54.3% Female 49% Female 51% Female AGE Mean 66 ± 13 65% > 60 69% 60 Mean 62 ±13 TYPE OF MALIGNANCY 22% Breast 15% GI 11% Lung 11% Heme 24% Stage III 58% Stage IV 12% Heme 21% Breast 18% GI 15% Lung 10% Heme

23 CANTHANOX TRIAL: TREATMENT REGIMENS Initial 3 Month Treatment Period Enoxaparin 1.5mg/kg SQ daily for 3 Months Patients Cancer + VTE Enoxaparin 1.5mg/kg SQ daily Determine whether LMWH is superior to warfarin for the secondary prophylaxis of VTE in patients with cancer Warfarin sodium daily for 3 Months (INR ) 146 patients at 25 clinical centers in France Enrollment terminated at 4 years due to slow accrual
24 CANTHANOX TRIAL: EFFICACY OUTCOMES Major Bleed or Recurrent VTE (3 MONTHS) Recurrent VTE Warfarin N = (21.1%) Enoxaparin N = 67 Relative Risk Increase 7 (10.5%) 2.02 (95%CI: ) P value NS 3 2 NS Major Bleed 12 (6 fatal) 5 (0 fatal) NS
25 CANTHANOX TRIAL: SAFETY OUTCOME Warfarin N = 71 Enoxaparin N = 67 Relative Risk Increase P value Mortality 3 MONTH 17 (22.7%) 8 (11.3%) 2.01 NS Causes Progression of Malignancy 56% Major Bleeding 24%
26 ONCENOX TRIAL: TREATMENT REGIMENS Population Patients Cancer + VTE Initial Enoxaparin 1mg/kg SC twice daily Treatment Period 6 Months Enoxaparin 1mg/kg SC daily Enoxaparin 1.5 mg/kg SC daily Warfarin sodium daily (INR )
27 ONCENOX TRIAL: EFFICACY OUTCOMES at 6 MOS Recurrent VTE Enoxaparin 1mg/kg - 2 Patients (6.9%) 1 patient not in intention to treat analysis - DVT Enoxaparin 1.5mg/kg - 2 Patients (6.3%) 1 patient not in intention to treat analysis - DVT Warfarin - 3 Patients (10%) Not Statistically Significant No cases of Pulmonary Emboli
28 ONCENOX TRIAL: SAFETY OUTCOMES at 6 MOS Major Bleeding Enoxaparin 1mg/kg 2 patients (6.5%) Enoxaparin 1.5mg/kg 4 patients (11.1%) Warfarin 1 patient (2.9%) Not Statistically Significant
29 MAIN LITE CANCER TRIAL: TREATMENT REGIMENS Patient Cancer + VTE Initial Tinzaparin 175 IU/kg SC daily (5 days) UFH continuous infusion (5 days) (titrated by APTT) Treatment Period 3 Months Tinzaparin 175 IU/kg SC daily for 3 months Warfarin sodium daily for 3 months (INR ) Continuation of anticoagulation after 3months was left to the primary attending physician
30 MAIN LITE CANCER TRIAL: EFFICACY OUTCOMES Warfarin N = 100 Tinzaparin N = 100 Relative Risk P value Recurrent VTE 3 Months 12 Months* NS P = Pulmonary Emboli 7 2
31 MAIN LITE CANCER TRIAL: SAFETY OUTCOMES Bleeding 3 Mo All Major Minor Mortality 3 Mo 12 Mo Warfarin N = (INR>4 in 2/7) 17 (INR>4 in 2/17) Tinzaparin N = Relative Risk P value NS NS


32 Standard Treatment of VTE Can We Do Better Than This? Initial treatment 5 to 7 days LMWH or UFH Long-term therapy > 3 months Vitamin K antagonist (INR )
33 30 Recurrent VTE and bleeding during anticoagulant treatment Patients with cancer and venous thrombosis Hazard ratio 3.2 [ ] Hazard ratio 2.2 [ ] Recurrent VTE, % Cancer 21% No Cancer 7% Major Bleeding, % Cancer 12% No Cancer 5% Time (months) Time (months) Prandoni P et al. Blood 2002; 100:
34 CLOT: Landmark Cancer/VTE Trial Dalteparin CANCER PATIENTS WITH ACUTE DVT or PE Randomization [N = 677] Dalteparin Oral Anticoagulant Primary Endpoints: Recurrent VTE and Bleeding Secondary Endpoint: Survival Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, 2003;349:146
35 The CLOT Trial Study Schema Dalteparin 200 IU/kg OD Control Group Vitamin K antagonist (INR 2.0 to 3.0) x 6 mo Experimental Group Dalteparin 200 IU/kg OD x 1 mo then ~150 IU/kg OD x 5 mo 5 to 7 days 1 month 6 months Lee AY, et al. N Engl J Med. 2003;349:
36 Landmark CLOT Cancer Trial Reduction in Recurrent VTE Probability of Recurrent VTE, % No data on VTE recurrence or safety with LMWH >6 mos 5 Recurrent VTE Risk reduction = 52% p-value = Days Post Randomization OAC Dalteparin Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, 2003;349:146
37 Bleeding Events in CLOT Dalteparin N=338 OAC N=335 P-value* Major bleed 19 ( 5.6%) 12 ( 3.6%) 0.27 Any bleed 46 (13.6%) 62 (18.5%) * Fisher s exact test Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, 2003;349:146


38 CLOT 12-month Mortality All Patients Probability of Survival, % Dalteparin HR 0.94 P-value = Days Post Randomization Lee A, et al. ASCO. 2003
39 Oral Anticoagulant Therapy in Cancer Patients: Problematic Warfarin therapy is complicated by: Difficulty maintaining tight therapeutic control, due to anorexia, vomiting, drug interactions, etc. > 200 known food, drug, and botanical interactions Frequent interruptions for thrombocytopenia and procedures Difficulty in venous access for monitoring Increased risk of both recurrence and bleeding Pts with CA maintain therapeutic INRs ~43% of the time vs 53% in non-ca Is it reasonable to substitute long-term LMWH for warfarin? When? How? Why?
 Copyright 2009 The Cochrane Collaboration.")
40 Anticoagulation for the long term treatment of venous thromboembolism in patients with cancer (Review) Copyright 2009 The Cochrane Collaboration. Published by JohnWiley & Sons, Ltd.


41 Anticoagulation for the long term treatment of venous thromboembolism in patients with cancer (Review) Copyright 2009 The Cochrane Collaboration. Published by JohnWiley & Sons, Ltd.
42 50 vs 44 events (Riva vs warfarin) 10.3% vs 11.4% (Rva vs warfarin; P=0.23) 1.1% vs 2.2% (Riva vs warfarin P=.003) Einstein-PE Study Open labeled, randomized acute symptomatic PE DVT Riva 15 mg bid X 20d, then 20 mg qd vs LMWH bridged warfarin Pts observed over 9 mos Outcomes:symptomatic VTE; relevant /major bleeding Riva alone: noninferior to wafarin for the initial and longterm treatment of pulmonary embolism; a potentially improved benefit risk profile <5% of pts with CA N Engl J Med 2012; 366:
43 Caveats of Einstein-PE for Cancer Patients: Should these results affect current recommendations for the prevention of recurrent VTE in cancer? <5% of over 4800 patients with cancer Controls received LMWH/warfarin; CLOT showed LMWH alone is superior to warfarin in cancer to prevent recurrent VTE Recurrent VTE in Riva cohort (2) vs warfarin (3) is too small to detect significant difference Recurrent VTE in CA (2%) is much lower than CLOT (12%); Low risk pts in this study? Only a head-to-head comparison of long-term LMWH vs rivaroxaban alone can answer the question
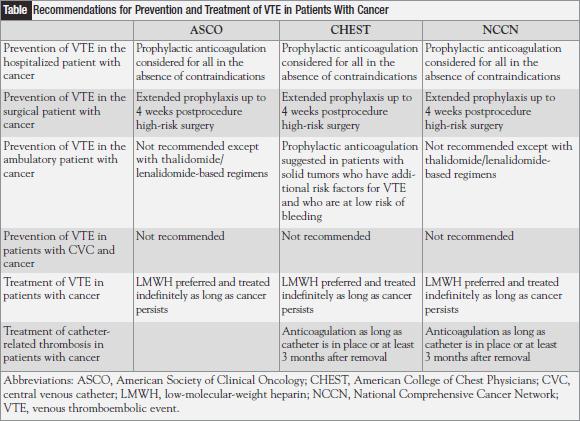
44 CONCLUSION: MAJOR GUIDELINES National Cancer Comprehensive Network American Society of Clinical Oncology (2012) American College of Chest Physicians (2012) Initial Therapy LMWH, UFH, or Fondaparinux LMWH for 5-10 days LMWH, UFH, or Fondaparinux Long Term Therapy LMWH indefinite in active cancer LMWH for 6 months VKA if LMWH unavailable Indefinite therapy while cancer active LMWH for 3-6 months (Grade 1A) VKA or LMWH indefinitely or until cancer is resolved (Grade 1C)
45 Treatment Factors: Cancer Surgery OR 95% CI RISTOS Prospective Registry Study 31 Departments of Surgery in Italy, n = 2,373 pts Prior VTE Anaesthesia >2 hr Bedrest >72 hr Advanced disease Age >60 years Agnelli, Ann Surg 2006; 243: 89-95
46 2012
47 Independent Risk Factors for Chemotherapy-associated VTE Patient Safety in Surgery Study a revealed the following independent predictors for VTE: Disseminated CA OR= Chemotherapy in last 30d OR=1.829 Transfusion > 4 U PRBCs in 72 h pre-op OR= Chemotherapy associated with a 2.2-fold increase in VTE compared to no chemotx b Rates of VTE rose faster in CA pts on chemotx vs no chemotx (47% increase vs 26%) a Rogers SO et al. JAmCollSurg.2007;204:1211; b Blom et al. JTH. 2006;4:529
48 Prophylaxis in Surgical Patients LMWH vs. UFH Abdominal or pelvic surgery for cancer (mostly colorectal) LMWH once daily vs. UFH tid for 7 10 days post-op DVT on venography at day 7 10 and symptomatic VTE Study N Design Regimens ENOXACAN double-blind enoxaparin vs. UFH Canadian Colorectal DVT Prophylaxis double-blind enoxaparin vs. UFH 1. ENOXACAN Study Group. Br J Surg 1997;84: McLeod R, et al. Ann Surg 2001;233:


 McLeod R, et al.")
49 Prophylaxis in Surgical Patients Incidence of Outcome Event 16.9% 13.9% P= % 2.7% Canadian Colorectal DVT Prophylaxis Trial N=234 N=241 VTE (Cancer) McLeod R, et al. Ann Surg 2001;233: Major Bleeding (All)
50 Extended Prophylaxis in Surgical Patients Incidence of Outcome Event 12.0% P= % 3.6% 1.8% 0.6% 5.1% 0% 0.4% ENOXACAN II N=167 N=165 NNT = 14 VTE Prox Any Major DVT Bleeding Bleeding Bergqvist D, et al. (for the ENOXACAN II investigators) N Engl J Med 2002;346:
51 Akl EA et al. Arch Intern Med ;168:1261-9
52 Akl EA et al. Cochrane Database Syst Rev. (11):CD009447, LMWH vs UFH as Perioperative VTE Prophylaxis in Cancer Patients: Trend Toward Reduced Incidence of PE P=0.24

53 Use of VTE thromboembolism prophylaxis stratified by year of diagnosis: Stuck despite Evidence Based Facts Wright et al. Obstet Gynecol 2011.
54 Summary Prophylaxis for Central Venous Access Devices in Cancer Patients Recent studies demonstrate a low incidence of symptomatic catheter-related thrombosis (~4%) Routine prophylaxis is not warranted to prevent catheter-related thrombosis, but catheter patency rates/infections have not been studied Low-dose LMWH and fixed-dose warfarin have not been shown to be effective for preventing symptomatic and asymptomatic thrombosis
55 Chaukiyal P et al. Thromb Haemost. 2008;99:38
56 Treatment of CVAD-Related DVT in Cancer Patients (NCCN guidelines) Remove device if no longer needed or anticoagulation is contraindicated If device is removed, anticoagulate with LMWH for 5-7 d to minimize embolization, if feasible If device remains, anticoagulate for 3 mos or as long as device in place, whichever is longest If DVT progresses despite anticoagulation, pull it Thrombolysis can be used safely in CA pts with UE DVTs (Kim HS et al. J Vasc Surg 2008;47:388)
57 Catheter related thrombosis and factor V Leiden in CA patients Reference Patients Number of pts Type of catheter Thrombosis n (%) F V Leiden n (%) OR Ratcliffe 35 Solid and heme 84 CVP 10 (11.9%) 3 (30%) NS Fijnheer 6 Allo SCT 277 Tunneled Hickman 33 (12%) 7 (21.2%) 7.7 ( ) Mandalà 8 van Rooden 9 Breast 300 cancer Various patients Port-A- Cath Different types 2 25 (8.3%) 5 (20%) 75 (30%) 12 (16%) 6.1 ( ) 2.7 ( ) Tesselaar19 Solid cancer 101 Arm ports/chest ports 18 (18%) 1 (5.6%) 0.6 ( ) Abdelkefi11 Heme SCT 171 Non tunneled catheters 13 (7.6%) 4 (30.8%) 3.3 ( ) Beckers MMT et al. Thrombosis Research 2010;125,
58 ASCO Recommendations for VTE Prophylaxis in Patients with Cancer Summary-2012 Patient Group Recommended Not Recommended Hospitalized patients with cancer Ambulatory patients with cancer receiving chemotherapy Patients with cancer undergoing surgery Patients with cancer with established VTE VTE prophylaxis with anticoagulants Myeloma patients receiving thalidomide or lenalidomide + chemotherapy/ dexamethasone. LMWH or adjusted dose warfarin. Or low dose ASA (low risk) Prophylaxis with low-dose UFH or LMWH Prophylaxis with mechanical methods for patients with contraindications to pharmacologic methods Pharmacologic treatment for at least 6 months. Consider continued anticoagulation beyond 6 months in those with active cancer. If bleeding or contraindication to anticoagulation Otherwise, no routine prophylaxis Consider mechanical methods when contraindications to anticoagulation. - To improve survival - Not recommended
59 Primary Prophylaxis with Parenteral Anticoagulation in CA Patients (heparin vs placebo) No Overall Survival Advantage at 12 Months Subset analysis: Limited SCLC (Altinbas 2004; Lebeau 1994) vs other CA (P = 0.03) : RR 0.86 at 1 yr P=0.12 No differences bet advanced vs nonadvanced CAs Akl EA et al. Cochrane Database of Systematic Reviews 4: 2011,

60 Primary Prophylaxis with Parenteral Anticoagulation in CA Patients (heparin vs placebo) Significant Survival Advantage at 24 Months P=0.001 Akl EA et al. Cochrane Database of Systematic Reviews 4: 2011,
61 RCTs of Thromboprophylaxis in Ambulatory Cancer Patients Low Molecular Weight Heparin Trial N Treatment Chemo Duration VTE Major Bleeding FAMOUS Solid tumors (Stage III/IV) TOPIC-I Breast (Stage IV) TOPIC-2 NSCLC (Stage IV) 385 Dalteparin Placebo 353 Certoparin Placebo 547 Certoparin Placebo PRODIGE 186 Dalteparin Glioma Placebo 64% 12 months 2.4% 3.3% 100% 6 months 4% 4% 100% 6 months 4.5% 8.3% months 11% 17% 0.5% 0 1.7% 0 3.7% 2.2% 5.1% 1.2% SIDERAS Solid Tumors (Stage IV) 141 Dalteparin Placebo/Control 54% Indefinitely 5.9% 7.1% 2.9% 7.1% PROTECHT Solid Tumors (Stage III/IV) 1166 Nadroparin 2:1 Placebo 100% < 4 months with chemo 1.4% 2.9% 0.7% 0 1. Kakkar AK, et al. J Clin Oncol. 2004;22: Haas SK, et al. J Thromb Haemost. 2005(suppl 1): abstract OR Perry JR et al. Proc ASCO Sideras K et al. Mayo Clin Proc 2006; 81: Agnelli G et al. Am Soc Hemat, 2008
62 RCTs of Thromboprophylaxis in Ambulatory Cancer Patients Low Molecular Weight Heparin Trial N Treatment Chemo Duration VTE Major Bleeding CONKO-04 Pancreatic CA FRAGEM Pancreatic CA 312 Enoxaparin 1 mg/kg/d X3mos and then 40 mg/d Observation 123 Dalteparin Control SAVE-ONCO 3200 Semuloparin 20 mg/d X3-7 mos Placebo 100% NNT=12 30 weeks 87%Reduced symptonatic VTE 14.5% 5% 100% 3 months 12% 31% 100% 3-7 months locally adv lung, bladder, GI, GU 6.3% 9.9% P=0.6 NA 1.2% 1.2% 3.4% P= % PHACS Duke and Uof R 229 Dalteparin Standard of care All nonheme CA 3 months VTE risk 3 (No brainca) NA NA MicroTEC 227 Enoxaparin Standard of Care Lung, colon, pancreas 6mos TF MP NA NA Sideras K, et al.mayo Clin Proc. 2006;81(6): ; Reiss H, et al. J Clin Oncol. 2010;28(suppl):15s. Abstract 4033; Maraveyas A, et al. Joint ECCO Congress;September 20-24,2009;Berlin, Germany. Abstract O



63
64 Semuloparin: SAVE ONCO The Game Changer? Randomized study Semuloparin 20mg daily vs. placebo until change of chemotherapy 3,212 randomized patients 68% metastatic CA : 37% lung, 29% colon-rectum 1.2% ULMWH vs. 3.4% VTE = 64% risk reduction (p<0.0001, intent-to-treat analysis); also 59% reduction in PE rate (OR 0.41) No heterogeneity in the benefit was observed for cancer stage or tumor location. 1.2% ULMWH vs. 1.1% had major bleeding (HR=1.05) 2.8% ULMWH vs. 2.0% had clinically relevant bleeding (HR=1.40) J Clin Oncol 29: 2011 (suppl; abstr LBA9014) Accessed 13 October 2011
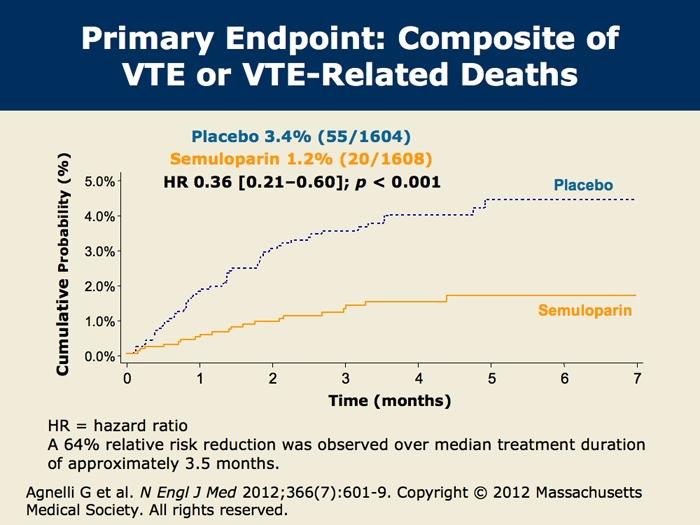
65 64% RRR
66 VTE Prediction Risk Score Chemotherapy Associated Thrombosis Development cohort 8% Validation cohort Rate of VTE (%) 7% 6% 5% 4% 3% 2% Venous Thromboembolism P < 0.001* *Overall test of significance High P<.001 Intermediate P<.001 Low Time (Days) 1.8% 2.0% 7.1% 6.7% 1% 0% 0.8% 0.3% n=734 n=374 n=1,627 n=842 n=340 n=149 RISK SCORE: Low (0) Intermediate (1-2) High (>3) Khorana AA et al. Blood. 2008; 111:
67 Cumulative incidence of VTE for cancer patients initially without of VTE according to the presence of tissue factor-bearing microparticles Tissue factor-bearing microparticle-positive (dashed line, N=16) tissue factor-bearing microparticle-negative (solid line, N=44)
68 3% cancer patients included Goldhaber SZ et al. N Engl J Med 2011:365:2167
69 A randomized phase II trial of apixaban for the prevention of thromboembolism in patients with metastatic cancer Patients receiving either first-line or second-line chemotherapy for advanced or metastatic lung, breast, gastrointestinal, bladder, ovarian or prostate cancers, cancer of unknown origin, myeloma or selected lymphomas Randomized to 5 mg, 10 mg or 20 mg once daily for 12 weeks of apixaban or placebo in a double-blind manner for 12 weeks. Double blind study design 93 patients received Apixaban 5, 10, 20 mg daily; 32 received placebo Rate of major bleeding in the 93 apixaban patients was 2.2% (95% confidence interval %). There were no fatal bleeds. Three placebo patients had symptomatic VTE; Apixaban = N0 VTE Levine MN et al J Thromb Haemost ;5:
70 Unresolved Clinical Questions 1. Should patients with cancer receive anticoagulation for VTE prophylaxis while hospitalized? Which one? Duration? 2. Should ambulatory patients with cancer receive VTE prophylaxis during systemic chemotherapy? 3. What is the best method for treatment of patients with cancer with established VTE to prevent recurrence? Duration? 4. Should patients with cancer receive anticoagulants in the absence of established VTE to improve survival? 5. What is role of novel new oral anticoagulants and semuloparin in CA patients? Lyman GH et al: J Clin Oncol 2007; 25:
71
72 Venous Thromboembolism in Cancer: Role of LMWH and Optimal Duration of Therapy Craig M Kessler, MD MACP Lombardi Comprehensive Care Center Georgetown University Medical Center Washington, DC The optimal anticoagulation regimens for the primary or secondary prevention of VTE in cancer patients have been slow to be established due to the variability of intrinsic procoagulant properties among different tumor types and their stage and grades; the potential contribution of chemotherapy or adjunctive therapies to the thrombogenic potential of malignancies; and the comorbidities of cancer, such as the thrombocytopenia from chemotherapy, the complications of central venous access devices, and the presence of visceral tumor involvement, which increases the risks of untoward hemorrhage. Furthermore, medical oncologists have been very reluctant to extrapolate the potential benefits of long term anticoagulation to their patients even though they have been clearly demonstrated in other categories of acute medical scenarios. This may be related in part to the fact that VTE treatment and secondary prophylaxis regimens have yet to convincingly improve the overall survival or performance status in cancer patients. This is in spite of the guideline recommendations from professional organizations such as the American College of Chest Physicians and the National Cancer Center Network. From the patient perspective, long term anticoagulation has not been adopted because of the inconvenience of using subcutaneously injected agents, their increased costs, and the fact that many insurance plans do reimburse for them. VTE is the second highest cause of death in hospitalized cancer patients, behind the cancer itself. This reflects the intrinsic biology of the malignancy to affect all aspects of coagulation-platelet activation, endothelial perturbation, thrombin generation, and modulation of fibrinolysis and angiogenesis. The fibrin scaffold anchors the tumor and facilitates its metastasis through the vascular wall. Targeting the tumor procoagulant properties may alter the systemic procoagulant effects of tumors and may alter cancer progression. The increased risk for VTE in CA patients varies over the course of the disease and relates to the primary site of CA and its stage and grade, the type of chemotherapy employed, and whether the patient undergoes surgery (twice the risk of postoperative DVT and three times the risk of fatal PE compared with that for patients without cancer). Comorbidities may also contribute to the VTE risk, e.g. thrombophilia, morbid obesity, previous VTE, presence of CVADs, etc. Anticoagulation strategies must take all of these issues into account. Data on primary VTE prophylaxis in cancer patients are scare due to the small number of cancer patients who have been recruited into the major landmark studies on this clinical topic. All of the professional organizational guidelines have recognized the increased risk of VTE complications in the acutely ill medical patient hospitalized with cancer and all have recommended implementation of VTE prophylaxis for this cohort unless contraindicated. The large
73 EXCLAIM (1) and MAGELLAN (2) studies examined the extended use (30 days) of VTE prophylaxis in order to determine if the in-hospital advantage of VTE prophylaxis could be improved upon, realizing that the predominant risk of VTE development occurs about 3 weeks post-discharge. They studies both demonstrated that active anticoagulation significantly decreased the incidence of VTE over days versus placebo. However, both studies induced significantly higher clinically relevant bleeding risks over days. The risk to benefit relationship thus did not favor the use of extended anticoagulation in acutely ill medical patients. The studies included only 3% (EXCLAIM) and 7% (MAGELLAM) of their study population with cancer and it is not clear whether these overall results can be extrapolated to the cancer cohort, which typically has experienced increased VTE despite adequate anticoagulation and increased bleeding complications with any VTE drug prophylaxis regimen. In addition, the MAGELLAN study introduced the first use of rivaroxaban for extended VTE prophylaxis. This oral specific anti-xa medication showed superiority versus parenteral enoxaparin in VTE reduction; however, it is not clear that the net benefit associated with the specific dosing regimen would convey to a cancer cohort; the small number of cancer patients recruited into the study further limits accurate assessment. The ADOPT trial, which included 3% cancer patients in each study arm, compared extended VTE prophylaxis (30 days) with apixaban (another specific oral anti-xa anticoagulant) to standard prophylaxis with enoxaparin. The investigators reported that apixaban was no more effective than enoxaparin, and the apixaban regimen was associated with significantly more major bleeding events (3). These findings of non-inferiority of efficacy and increased bleeding will hinder acceptance of this specific anti-xa drug over enoxaparin for use in extended VTE prophylaxis in severely ill patients. Again, the antithrombotic effectiveness and safety of apixaban in the cancer population is difficult to determine from the ADOPT study, but a pilot trial suggests that it can be given safely (2.2% incidence of bleeding). (4) The benefits of extended duration of VTE prophylaxis in the cancer population was formerly confirmed in the surgery population. The presence of disseminated cancer, the recent use of chemotherapy, the need for extensive transfusions, and the anesthesia time all were associated with increased rates of VTE complications. While the ENOXACAN II (6) trial established the benefit of extended enoxaparin administration (30 days post op) to reduce VTE complications in patients undergoing abdominal or pelvic surgery for their cancer (predominantly colorectal), a recent Cochrane meta-analysis (5) showed non-statistically significant trends for survival or PE incidence for LMWH versus unfractionated heparin administered subcutaneously 5000 Units BID or TID. There was also a slight trend toward increased bleeding complications for LMWH. LMWH has proved superior to warfarin in extended or short term VTE prophylaxis in cancer surgery patients. The guideline sets from all professional societies recommend perioperative VTE prophylaxis in cancer patients with the highest level of evidence based data. Much attention has been focused on secondary prophylaxis against recurrent VTE in the cancer population, but the seminal study remains the CLOT study. (7) This well performed prospective, multicenter, adequately powered, randomized trial has also been the major determinant in establishing the superiority of LMWH, specifically dalteparin, as the superior anticoagulant to administer for prevention of secondary VTE in cancer patients. Dalteparin is the only LMWH which has been granted FDA approval for this indication. There was a 52% reduced incidence in VTE episodes in the dalteparin arm versus warfarin over a 6 month period, accomplished with comparable rates of bleeding complications. There is a current study evaluating whether the
74 extended use of dalteparin up to a year can convey additional reductions in VTE development. Recently, the Einstein-PE trial reported their 9 month observation of long term anticoagulation with the oral specific anti-xa agent, rivaroxaban, versus LMWH-bridged warfarin in a general medical population. There were <5% cancer patients in this study, which showed that rivaroxaban alone was non-inferior to warfarin for the initial and long term treatment of pulmonary embolism with or without DVT and with an improved benefit-risk profile with low rates of bleeding. Whether this advantage will eventually be proven to be applicable to the cancer population overall remains to be established. (8) An interesting aspect to VTE prophylaxis is whether primary prophylaxis for the ambulatory cancer patient receiving chemotherapy is beneficial to VTE prevention or even to enhance patient survival. All of the professional society guidelines do not recommend this approach although chemotherapy is certainly appreciated to raise the risk of VTE. The guidelines generally carve out multiple myeloma in their recommendations since the use of anti-angiogenic medications (lenalidomide or thalidomide), often administered in conjunction with high dose corticosteroids, raise the risk of VTE in this disease substantially. Thus, most guidelines recommend the use of ASA 81 mg daily for low VTE risk individuals on such regimens and the use of warfarin or LMWH for high VTE risk patients over the duration of therapy. For those with solid tumor malignancies, primary prophylaxis while receiving out-patient chemotherapy appears to be beneficial for those with lung, pancreatic, and GI cancer. This subset advantage was observed in the Protecht study (9), in which over 1100 patients with various cancers were randomized to receive nadroparin (a LMWH) versus placebo over 4 months and demonstrated a statistically significant reduction in VTE events (p=0.02) without increased bleeding risks. More recently, the SAVE-ONCO trial (10) was published and demonstrated superior VTE protection in a high risk population (N=3200) with locally advanced GI, GU, bladder and lung cancer treated with an ultra low molecular weight heparin. Semuloparin, a novel ULMWH with high anti-factor Xa and residual anti-factor IIa activities, induced a 64% risk reduction in VTE without increased bleeding. Such studies should be evaluated by professional societies to alter their stances on primary prophylaxis since it appears that certain subsets of cancer patients may definitely benefit. Unfortunately, there does not appear to be any survival advantage to this regimen. In the future, individualized anticoagulation regimens will likely be developed, based on clinical risk factor profiling, such as promoted by Khorana et al (11). One promising laboratory predictor of risk may be the measurement of circulating microparticles, a surrogate measure of tissue factor generation by the tumor. There are important questions left to be answered about optimal duration of VTE prophylaxis in cancer patients. What is the role of the novel oral anti-iia and anti-xa medications and what is their bleeding potential in cancer patients? Will all agents convey equal benefits or toxicities? Will anti-iia agents promote improved cancer survival versus anti-xa since tumor progression may occur in the presence of thrombin? If bleeding events occur, how should one reverse the anticoagulant effects of LMWHs or the novel oral agents? How can one use these agents in the context of evolving renal insufficiency in many patients on chemotherapy? Finally, how do we encourage the clinical to initiate anticoagulation in cancer patients in those scenarios which have
75 1A or 1B recommendations from professional society guidelines based on high quality evidence based data? References: 1. Hull RD et al. Extended-duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial. Ann Intern Med. 2010;153: Cohen AT et al. Extended-duration rivaroxaban thromboprophylaxis in acutely ill medical patients: MAGELLAN study protocol. J Thromb Thrombolysis. 2011;31: Goldhaber SZ et al. Apixaban versus Enoxaparin for Thromboprophylaxis in Medically Ill Patients. N Engl J Med 2011:365: Levine MN et al. A randomized phase II trial of apixaban for the prevention of thromboembolism in patients with metastatic cancer. J Thromb Haemost 2012; 10: Akl EA, et al. Anticoagulation for the long term treatment of venous thromboembolism in patients with cancer. Cochrane Database of Systematic Reviews 2008, Issue 2. Art. No.: CD DOI: / CD pub2. 6. Bergqvist D, et al. (for the ENOXACAN II investigators). Duration of thromboprophylaxis against venous thromboembolism with enoxaparin after surgery for cancer. N Engl J Med 2002;346: Lee AY, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003;349: The EINSTEIN PE Investigators. Oral Rivaroxaban for the Treatment of Symptomatic Pulmonary Embolism. N Engl J Med 2012; 366: Agnelli G et al. Nadroparin for the prevention of thromboembolic events in ambulatory patients with metastatic or locally advanced solid cancer receiving chemotherapy: a randomised, placebo-controlled, double-blind study. Lancet Oncol. 2009;10: ) Agnelli G et al. Semuloparin for Thromboprophylaxis in Patients Receiving Chemotherapy for Cancer. N Engl J Med 2012; 366:
76 11) Khorana AA et al. Development and validation of a predictive model for chemotherapyassociated thrombosis.blood 2008; 111:
Venous Thrombo-Embolism. John de Vos Consultant Haematologist RSCH
 Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
PRIMARY THROMBOPROPHYLAXIS IN AMBULATORY CANCER PATIENTS: CURRENT GUIDELINES
 PRIMARY THROMBOPROPHYLAXIS IN AMBULATORY CANCER PATIENTS: CURRENT GUIDELINES Mario Mandalà, MD Unit of Clinical Research Department of Oncology and Haematology Papa Giovanni XXIII Hospital Cancer Center
PRIMARY THROMBOPROPHYLAXIS IN AMBULATORY CANCER PATIENTS: CURRENT GUIDELINES Mario Mandalà, MD Unit of Clinical Research Department of Oncology and Haematology Papa Giovanni XXIII Hospital Cancer Center
Cancer Associated Thrombosis An update.
 Cancer Associated Thrombosis An update. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway LIQUID
Cancer Associated Thrombosis An update. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway LIQUID
In the Clinic: Annals Sweta Kakaraparthi 1/23/15
 In the Clinic: Annals Sweta Kakaraparthi 1/23/15 Case Scenerio 56 year old female with breast cancer presents to the clinic for her 3 month followup! She is concerned about blood clots and asks you about
In the Clinic: Annals Sweta Kakaraparthi 1/23/15 Case Scenerio 56 year old female with breast cancer presents to the clinic for her 3 month followup! She is concerned about blood clots and asks you about
New oral anticoagulants and Palliative Care.
 New oral anticoagulants and Palliative Care. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway
New oral anticoagulants and Palliative Care. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway
Are guidelines for anticoagulation useful in cancer patients?
 Session 3 Striking a Balance Between Bleeding and the Risk of Thrombosis in Cancer Patients Are guidelines for anticoagulation useful in cancer patients? Sebastian Szmit Department of Pulmonary Circulation
Session 3 Striking a Balance Between Bleeding and the Risk of Thrombosis in Cancer Patients Are guidelines for anticoagulation useful in cancer patients? Sebastian Szmit Department of Pulmonary Circulation
Venous Thromboembolism (VTE) in Myeloma. Christine Chen May 2017
 in Myeloma. Christine Chen May 2017") Venous Thromboembolism (VTE) in Myeloma Christine Chen May 2017 Objectives 1. Review the magnitude of the problem and why myeloma patients are at risk of VTE 2. Discuss thromboprophylaxis approaches in
Venous Thromboembolism (VTE) in Myeloma Christine Chen May 2017 Objectives 1. Review the magnitude of the problem and why myeloma patients are at risk of VTE 2. Discuss thromboprophylaxis approaches in
CANCER ASSOCIATED THROMBOSIS. Pankaj Handa Department of General Medicine Tan Tock Seng Hospital
 CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
Cancer Associated Thrombosis: six months and beyond. Farzana Haque Hull York Medical School
 Cancer Associated Thrombosis: six months and beyond Farzana Haque Hull York Medical School Disclosure I have no disclosure The Challenge of Anticoagulation in Patients with Venous Thromboembolism and Cancer
Cancer Associated Thrombosis: six months and beyond Farzana Haque Hull York Medical School Disclosure I have no disclosure The Challenge of Anticoagulation in Patients with Venous Thromboembolism and Cancer
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
THROMBOPROPHYLAXIS IN CANCER PATIENTS
 CANCER ASSOCIATED THROMBOSIS THROMBOPROPHYLAXIS IN CANCER PATIENTS Cancer is an important risk factor for venous thromboembolism (VTE). Research has shown that 4-20% of 1 patients with cancer experience
CANCER ASSOCIATED THROMBOSIS THROMBOPROPHYLAXIS IN CANCER PATIENTS Cancer is an important risk factor for venous thromboembolism (VTE). Research has shown that 4-20% of 1 patients with cancer experience
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS
 EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS Samuel Z. Goldhaber, MD Director, VTE Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS Samuel Z. Goldhaber, MD Director, VTE Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
New Hope for VTE Burden in Ambulatory Cancer Patients
 New Hope for VTE Burden in Ambulatory Cancer Patients Essam Abo-El-Nazar MS, FRCS Consultant Liver Surgeon King Fahd Hospital Jeddah-KSA Prof. of Surgery Imperial College London-UK My talk today What is
New Hope for VTE Burden in Ambulatory Cancer Patients Essam Abo-El-Nazar MS, FRCS Consultant Liver Surgeon King Fahd Hospital Jeddah-KSA Prof. of Surgery Imperial College London-UK My talk today What is
Epidemiology of Thrombosis in Patients with Malignancy. Cancer and Venous Thromboembolism. Chew HK, Arch Int Med, Feb Blom et al, JAMA, Feb 2005
 Cancer and Venous Thromboembolism Objectives 1. Epidemiology of thrombosis in patients with malignancy 2. Anticancer agents and thrombosis 3. Current treatment protocols at UHN 4. Prevention of DVT 5.
Cancer and Venous Thromboembolism Objectives 1. Epidemiology of thrombosis in patients with malignancy 2. Anticancer agents and thrombosis 3. Current treatment protocols at UHN 4. Prevention of DVT 5.
Results from RE-COVER RE-COVER II RE-MEDY RE-SONATE EXECUTIVE SUMMARY
 Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in the treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE) and the prevention of recurrent DVT and PE Results from
Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in the treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE) and the prevention of recurrent DVT and PE Results from
Medical Patients: A Population at Risk
 Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
La terapia del TEV nel paziente oncologico nell'era dei DOAC
 XXVI CONGRESSO NAZIONALE FCSA Bologna, 5-7 Novembre 2015 Tromboembolismo venoso La terapia del TEV nel paziente oncologico nell'era dei DOAC ANNA FALANGA Immunoematologia e Medicina Trasfusionale e Centro
XXVI CONGRESSO NAZIONALE FCSA Bologna, 5-7 Novembre 2015 Tromboembolismo venoso La terapia del TEV nel paziente oncologico nell'era dei DOAC ANNA FALANGA Immunoematologia e Medicina Trasfusionale e Centro
Cancer associated thrombosis. 17 th November 2016 Simon Noble Clinical Professor Palliative Medicine Cardiff University Wales, UK
 Cancer associated thrombosis 17 th November 2016 Simon Noble Clinical Professor Palliative Medicine Cardiff University Wales, UK Today What is VTE? How does CAT differ? Initial anticoagulation Anticoagulation
Cancer associated thrombosis 17 th November 2016 Simon Noble Clinical Professor Palliative Medicine Cardiff University Wales, UK Today What is VTE? How does CAT differ? Initial anticoagulation Anticoagulation
Prophylaxie primaire sur le patient ambulatoire. Marc Carrier
 Prophylaxie primaire sur le patient ambulatoire Marc Carrier Marc Carrier In compliance with COI policy, SSVQ requires the following disclosures to the session audience: Research Support/P.I. Employee
Prophylaxie primaire sur le patient ambulatoire Marc Carrier Marc Carrier In compliance with COI policy, SSVQ requires the following disclosures to the session audience: Research Support/P.I. Employee
Cancer and the Heparins
 Cancer and the Heparins Wim P Ceelen, MD, PhD, FACS Department of GI Surgery - UZ Gent Senior Clinical Researcher - FWO Overview Mechanisms of cancer induced thrombosis Guidelines for prevention and treatment
Cancer and the Heparins Wim P Ceelen, MD, PhD, FACS Department of GI Surgery - UZ Gent Senior Clinical Researcher - FWO Overview Mechanisms of cancer induced thrombosis Guidelines for prevention and treatment
Cancer Associated Thrombosis
 Cancer Associated Thrombosis Can we use DOACs? D R. C Y N T H I A W U MD F R C P ( C ) D I V I S I O N O F H E M A T O L O G Y F A M I L Y P H Y S I C I A N S A N D C A N C E R C O N T R O L A P R I L
Cancer Associated Thrombosis Can we use DOACs? D R. C Y N T H I A W U MD F R C P ( C ) D I V I S I O N O F H E M A T O L O G Y F A M I L Y P H Y S I C I A N S A N D C A N C E R C O N T R O L A P R I L
Is There a Role for Prophylaxis in Cancer Patients During Therapy?
 Victor F. Tapson, MD, FCCP, FRCP Professor of Medicine Director, Center for Pulmonary Vascular Disease Division of Pulmonary and Critical Care Duke University Medical Center Durham, N.C. USA Is There a
Victor F. Tapson, MD, FCCP, FRCP Professor of Medicine Director, Center for Pulmonary Vascular Disease Division of Pulmonary and Critical Care Duke University Medical Center Durham, N.C. USA Is There a
Thromboembolism and cancer: New practices. Marc Carrier
 Thromboembolism and cancer: New practices Marc Carrier Marc Carrier Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board Leo Pharma, BMS No relevant
Thromboembolism and cancer: New practices Marc Carrier Marc Carrier Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board Leo Pharma, BMS No relevant
incidence of cancer-associated thrombosis (CAT) is further increased by additional risk factors such as chemotherapeutic 2
 is further increased by additional risk factors such as chemotherapeutic 2") CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
Oral rivaroxaban versus standard therapy for the acute and continued treatment of symptomatic deep vein thrombosis. The EINSTEIN DVT study.
 Oral rivaroxaban versus standard therapy for the acute and continued treatment of symptomatic deep vein thrombosis. The EINSTEIN DVT study Comments Harald Darius, Berlin Disclosures for Harald Darius Research
Oral rivaroxaban versus standard therapy for the acute and continued treatment of symptomatic deep vein thrombosis. The EINSTEIN DVT study Comments Harald Darius, Berlin Disclosures for Harald Darius Research
Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1
 CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
Venous Thromboembolism Prophylaxis: Checked!
 Venous Thromboembolism Prophylaxis: Checked! William Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University of Toronto National Lead, VTE Prevention, Safer
Venous Thromboembolism Prophylaxis: Checked! William Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University of Toronto National Lead, VTE Prevention, Safer
10/8/2012. Disclosures. Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines. Goals and Objectives. Outline
 Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
The risk of venous thromboembolism is four to seven times as
 review article Dan L. Longo, M.D., Editor Prophylaxis against Venous Thromboembolism in Ambulatory Patients with Cancer Jean M. Connors, M.D. The risk of venous thromboembolism is four to seven times as
review article Dan L. Longo, M.D., Editor Prophylaxis against Venous Thromboembolism in Ambulatory Patients with Cancer Jean M. Connors, M.D. The risk of venous thromboembolism is four to seven times as
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
New Oral Anticoagulants Prevention and Treatment of DVT and PE
 New Oral Anticoagulants Prevention and Treatment of DVT and PE Grigoris T Gerotziafas Groupe de Thrombose Equipe de recherche ER2UPMC Interactions cellulaires tumorales et leur environnement et réponses
New Oral Anticoagulants Prevention and Treatment of DVT and PE Grigoris T Gerotziafas Groupe de Thrombose Equipe de recherche ER2UPMC Interactions cellulaires tumorales et leur environnement et réponses
Thromboprophylaxis for medical patients with cancer: what do the guidelines say?
 ith Thromboprophylaxis for medical patients with cancer: what do the guidelines say? Practice Points Hospitalized medically ill cancer patients should receive parenteral thromboprophylaxis for the duration
ith Thromboprophylaxis for medical patients with cancer: what do the guidelines say? Practice Points Hospitalized medically ill cancer patients should receive parenteral thromboprophylaxis for the duration
DOACs in CAT. Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD
 DOACs in CAT Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD Case 65 year old post menopausal female Left breast lesion Oct 2015 Biopsy Invasive ductal carcinoma Lumpectomy with SNB- pt1cno
DOACs in CAT Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD Case 65 year old post menopausal female Left breast lesion Oct 2015 Biopsy Invasive ductal carcinoma Lumpectomy with SNB- pt1cno
Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders
 SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
Cancer and Thrombosis
 Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
New Oral Anticoagulant Drugs in the Prevention of DVT
 New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
Management of Cancer Associated Thrombosis (CAT) where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth
 where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth") Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis
Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis
Cancer Associated Thrombosis Review and Update. Family Practice Oncology CME Day November 21 st 2015 Erica Peterson
 Cancer Associated Thrombosis Review and Update Family Practice Oncology CME Day November 21 st 2015 Erica Peterson Disclosures No conflicts of interest to declare Objectives To review evidence in cancer-associated
Cancer Associated Thrombosis Review and Update Family Practice Oncology CME Day November 21 st 2015 Erica Peterson Disclosures No conflicts of interest to declare Objectives To review evidence in cancer-associated
Tissue Factor-positive Microparticles in Cancerassociated
 Tissue Factor-positive Microparticles in Cancerassociated Thrombosis Nigel Mackman, Ph.D., FAHA John C. Parker Distinguished Professor of Medicine Director of the UNC McAllister Heart Institute Co-Director
Tissue Factor-positive Microparticles in Cancerassociated Thrombosis Nigel Mackman, Ph.D., FAHA John C. Parker Distinguished Professor of Medicine Director of the UNC McAllister Heart Institute Co-Director
Non commercial use only. The treatment of venous thromboembolism with new oral anticoagulants. Background
 Italian Journal of Medicine 2013; volume 7(s8):29-35 The treatment of venous thromboembolism with new oral anticoagulants Davide Imberti AUSL Piacenza, Italy ABSTRACT Traditional anticoagulants, such as
Italian Journal of Medicine 2013; volume 7(s8):29-35 The treatment of venous thromboembolism with new oral anticoagulants Davide Imberti AUSL Piacenza, Italy ABSTRACT Traditional anticoagulants, such as
Management of Cancer Associated VTE
 Management of Cancer Associated VTE Jean M. Connors, MD 2017 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine HMS
Management of Cancer Associated VTE Jean M. Connors, MD 2017 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine HMS
Cancer Associated Thrombosis
 Cancer Associated Thrombosis Pantep Angchaisuksiri, MD Professor of Medicine Mahidol University, Thailand Adjunct Associate Professor University of North Carolina, Chapel Hill, USA Piccioli A. J Thromb
Cancer Associated Thrombosis Pantep Angchaisuksiri, MD Professor of Medicine Mahidol University, Thailand Adjunct Associate Professor University of North Carolina, Chapel Hill, USA Piccioli A. J Thromb
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients. David Liff MD Oklahoma Heart Institute Vascular Center
 DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
Duration of Anticoagulant Therapy. Linda R. Kelly PharmD, PhC, CACP September 17, 2016
 Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
RISK FACTORS. Cancer type. Cancer stage
 CANCER ASSOCIATED THROMBOSIS RISK FACTORS The link between cancer and thrombosis is well established, with malignancy recognised as the most important individual risk factor for venous thromboembolism
CANCER ASSOCIATED THROMBOSIS RISK FACTORS The link between cancer and thrombosis is well established, with malignancy recognised as the most important individual risk factor for venous thromboembolism
Focus: l embolia polmonare Per quanto la terapia anticoagulante orale? Giulia Magnani 27 Gennaio, 2018
 Focus: l embolia polmonare Per quanto la terapia anticoagulante orale? Giulia Magnani 27 Gennaio, 2018 NO DISCLOSURE Pulmonary Embolism Venous thromboembolism (VT) is the third most common cause of cardiovascular
Focus: l embolia polmonare Per quanto la terapia anticoagulante orale? Giulia Magnani 27 Gennaio, 2018 NO DISCLOSURE Pulmonary Embolism Venous thromboembolism (VT) is the third most common cause of cardiovascular
GLIOMA - VENOUS THROMBOEMBOLISM. Miguel Navarro. Hospital Universitario de Salamanca-IBSAL
 GLIOMA - VENOUS THROMBOEMBOLISM Miguel Navarro. Hospital Universitario de Salamanca-IBSAL GLIOMA - VTE GLIOMA - VTE The two string problem Substantial risk for developing VTE Concern antithrombotic agents
GLIOMA - VENOUS THROMBOEMBOLISM Miguel Navarro. Hospital Universitario de Salamanca-IBSAL GLIOMA - VTE GLIOMA - VTE The two string problem Substantial risk for developing VTE Concern antithrombotic agents
My Cancer Patient Has a Clot- Can I prescribe a Direct Oral Anticoagulant (DOAC)?
?") My Cancer Patient Has a Clot- Can I prescribe a Direct Oral Anticoagulant (DOAC)? November 24, 2018 Erica Peterson MD, FRCPC University of British Columbia Disclosures I participate in clinical research
My Cancer Patient Has a Clot- Can I prescribe a Direct Oral Anticoagulant (DOAC)? November 24, 2018 Erica Peterson MD, FRCPC University of British Columbia Disclosures I participate in clinical research
Obesity, renal failure, HIT: which anticoagulant to use?
 Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Fatal P.E. Historic 1-2% Current %
 Dr. (Prof.) Anil Arora MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London, UK) Senior
Dr. (Prof.) Anil Arora MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London, UK) Senior
Spontane und Tumor-assoziierte VTE: womit wie lange antikoagulieren
 Spontane und Tumor-assoziierte VTE: womit wie lange antikoagulieren Paul Kyrle Allgemeines Krankenhaus Wien Disclosures relevant for this presentation Consultancies, member of advisory boards, speaker
Spontane und Tumor-assoziierte VTE: womit wie lange antikoagulieren Paul Kyrle Allgemeines Krankenhaus Wien Disclosures relevant for this presentation Consultancies, member of advisory boards, speaker
Is Oral Rivaroxaban Safe and Effective in the Treatment of Patients with Symptomatic DVT?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 1-1-2013 Is Oral Rivaroxaban Safe and Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 1-1-2013 Is Oral Rivaroxaban Safe and Effective
ASH 2011: Clinically Relevant Highlights Regarding Venous Thromboembolism and Anticoagulation
 ASH 2011: Clinically Relevant Highlights Regarding Venous Thromboembolism and Anticoagulation Stephan Moll Department of Medicine, Division of Hematology-Oncology, University of North Carolina School of
ASH 2011: Clinically Relevant Highlights Regarding Venous Thromboembolism and Anticoagulation Stephan Moll Department of Medicine, Division of Hematology-Oncology, University of North Carolina School of
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Primary prophylaxis for venous thromboembolism in ambulatory cancer patients receiving chemotherapy (Review)
") Primary prophylaxis for venous thromboembolism in ambulatory cancer patients receiving chemotherapy (Review) Di Nisio M, Porreca E, Otten HM, Rutjes AWS source: https://doi.org/10.7892/boris.59961 downloaded:
Primary prophylaxis for venous thromboembolism in ambulatory cancer patients receiving chemotherapy (Review) Di Nisio M, Porreca E, Otten HM, Rutjes AWS source: https://doi.org/10.7892/boris.59961 downloaded:
J Clin Oncol 31: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 31 NUMBER 17 JUNE 10 2013 JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C I A L A R T I C L E Gary H. Lyman, Nicole M. Kuderer, and Jeffrey M. Clarke, Duke University and Duke Cancer Institute, Durham;
VOLUME 31 NUMBER 17 JUNE 10 2013 JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C I A L A R T I C L E Gary H. Lyman, Nicole M. Kuderer, and Jeffrey M. Clarke, Duke University and Duke Cancer Institute, Durham;
DOACs in SPECIAL POPULATIONS
 DOACs in SPECIAL POPULATIONS Ann K Wittkowsky PharmD, CACP, FASHP, FCCP Clinical Professor University of Washington School of Pharmacy Director, Anticoagulation Services UWMedicine Department of Pharmacy
DOACs in SPECIAL POPULATIONS Ann K Wittkowsky PharmD, CACP, FASHP, FCCP Clinical Professor University of Washington School of Pharmacy Director, Anticoagulation Services UWMedicine Department of Pharmacy
Aspirin as Venous Thromboprophylaxis
 Canadian Society of Internal Medicine Nov 2, 2017 Aspirin as Venous Thromboprophylaxis Bill Geerts, MD, FRCPC Thromboembolism Consultant, Sunnybrook HSC Professor of Medicine, University of Toronto Disclosures
Canadian Society of Internal Medicine Nov 2, 2017 Aspirin as Venous Thromboprophylaxis Bill Geerts, MD, FRCPC Thromboembolism Consultant, Sunnybrook HSC Professor of Medicine, University of Toronto Disclosures
Frequently Asked Questions about Cancer Associated Thrombosis
 + Frequently Asked Questions about Cancer Associated Thrombosis Atlantic Canada Oncology Group Annual Meeting June 13 th, 2015 Sudeep Shivakumar, Dalhousie University + Conflict of Interest Disclosures
+ Frequently Asked Questions about Cancer Associated Thrombosis Atlantic Canada Oncology Group Annual Meeting June 13 th, 2015 Sudeep Shivakumar, Dalhousie University + Conflict of Interest Disclosures
Objectives. Venous Thromboembolism (VTE) Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?
 Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?") Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis
 BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism
 Cardiol Ther (2018) 7:1 13 https://doi.org/10.1007/s40119-018-0107-0 REVIEW A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism Andrew
Cardiol Ther (2018) 7:1 13 https://doi.org/10.1007/s40119-018-0107-0 REVIEW A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism Andrew
Report dei gruppi di lavoro >> [ Trombosi e cancro ]
![Report dei gruppi di lavoro >> [ Trombosi e cancro ]](/thumbs/91/106293601.jpg "Report dei gruppi di lavoro >> [ Trombosi e cancro ]") Report dei gruppi di lavoro >> [ Trombosi e cancro ] Relatori: A. FALANGA, M. MARCHETTI 27-28 ottobre 2008 Borgo S. Luigi Monteriggioni (Siena) Trombosi e cancro - Copyright FSE 1 Gruppo di lavoro 2 [
Report dei gruppi di lavoro >> [ Trombosi e cancro ] Relatori: A. FALANGA, M. MARCHETTI 27-28 ottobre 2008 Borgo S. Luigi Monteriggioni (Siena) Trombosi e cancro - Copyright FSE 1 Gruppo di lavoro 2 [
PROGNOSIS AND SURVIVAL
 CANCER ASSOCIATED THROMBOSIS PROGNOSIS AND SURVIVAL Since French internist Armand Trousseau reported the occurrence of mysterious thrombotic disorders in cancer patients in the mid-19th century, the link
CANCER ASSOCIATED THROMBOSIS PROGNOSIS AND SURVIVAL Since French internist Armand Trousseau reported the occurrence of mysterious thrombotic disorders in cancer patients in the mid-19th century, the link
Factor Xa Inhibition in the Management of Venous Thromboembolism: Important Safety Information. Important Safety Information (cont d)
") Factor Xa Inhibition in the Management of Venous Thromboembolism: The Role of Fondaparinux WARNING: SPINAL/EPIDURAL HEMATOMAS Epidural or spinal hematomas may occur in patients who are anticoagulated with
Factor Xa Inhibition in the Management of Venous Thromboembolism: The Role of Fondaparinux WARNING: SPINAL/EPIDURAL HEMATOMAS Epidural or spinal hematomas may occur in patients who are anticoagulated with
When and How to Use the Newly Approved Oral Anticoagulants to Treat Acute Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) Ian del Conde, MD
 and Pulmonary Embolism (PE) Ian del Conde, MD") When and How to Use the Newly Approved Oral Anticoagulants to Treat Acute Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) Ian del Conde, MD December 12, 2015 Disclosures CONSULTANT Merck; New Haven
When and How to Use the Newly Approved Oral Anticoagulants to Treat Acute Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) Ian del Conde, MD December 12, 2015 Disclosures CONSULTANT Merck; New Haven
The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for
: Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for") The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for Anticoagulation Services Sanford USD Medical Center Sioux Falls,
The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for Anticoagulation Services Sanford USD Medical Center Sioux Falls,
The clinical relevance of AMPLIFY programme
 Venice October 16th 2015 The clinical relevance of AMPLIFY programme Francesco Dentali Department of Clinical Medicine Insubria University Varese Disclosures Bayer Bristol-Myers Squibb/Pfizer Boehringer
Venice October 16th 2015 The clinical relevance of AMPLIFY programme Francesco Dentali Department of Clinical Medicine Insubria University Varese Disclosures Bayer Bristol-Myers Squibb/Pfizer Boehringer
Update on thrombosis 13/07/2017. To focus on
 Update on thrombosis Oxford Advanced Course 2017 Simon Noble Clinical Professor Palliative and Supportive Medicine Cardiff University Wales, UK To focus on Changing thrombogenicity of cancer What is the
Update on thrombosis Oxford Advanced Course 2017 Simon Noble Clinical Professor Palliative and Supportive Medicine Cardiff University Wales, UK To focus on Changing thrombogenicity of cancer What is the
THROMBOPROPHYLAXIS: NON-ORTHOPEDIC SURGERY
 THROMBOPROPHYLAXIS: NON-ORTHOPEDIC SURGERY OBJECTIVE: To outline a practical approach for the prevention of venous thromboembolism (VTE) in patients undergoing non-orthopedic surgery. BACKGROUND: VTE is
THROMBOPROPHYLAXIS: NON-ORTHOPEDIC SURGERY OBJECTIVE: To outline a practical approach for the prevention of venous thromboembolism (VTE) in patients undergoing non-orthopedic surgery. BACKGROUND: VTE is
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF
 Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Venous Thromboembolic Disease Update
 Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
DOACs and CAT. 05 May 2017 NTW St Thomas Hospital
 DOACs and CAT Alexander (Ander) Cohen Vascular Medicine / Haematology Guy s and St Thomas Hospitals, King s College, London 05 May 2017 NTW St Thomas Hospital Disclosures for Dr. Alexander (Ander) T. Cohen
DOACs and CAT Alexander (Ander) Cohen Vascular Medicine / Haematology Guy s and St Thomas Hospitals, King s College, London 05 May 2017 NTW St Thomas Hospital Disclosures for Dr. Alexander (Ander) T. Cohen
Clinical practice guidelines for prophylaxis of venous thomboembolism in cancer patients
 618 Theme Issue Article Clinical practice guidelines for prophylaxis of venous thomboembolism in cancer patients Corinne Frere 1 ; Dominique Farge 2 1 Assistance Publique Hôpitaux de Marseille, Timone
618 Theme Issue Article Clinical practice guidelines for prophylaxis of venous thomboembolism in cancer patients Corinne Frere 1 ; Dominique Farge 2 1 Assistance Publique Hôpitaux de Marseille, Timone
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Top 5 (or so) Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE
 Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE") Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS
 ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Review Guideline recommendations for the treatment of established VTE Initial treatment (fi rst 10 days) Panel 1:
 Panel 1:") International clinical practice guidelines including guidance for direct oral anticoagulants in the treatment and prophylaxis of venous thromboembolism in patients with cancer Dominique Farge, Henri Bounameaux,
International clinical practice guidelines including guidance for direct oral anticoagulants in the treatment and prophylaxis of venous thromboembolism in patients with cancer Dominique Farge, Henri Bounameaux,
Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement. Marilyn Szekendi, PhD, RN
 Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement Marilyn Szekendi, PhD, RN ANA 7 th Annual Nursing Quality Conference, February 2013 Research Team Banafsheh Sadeghi,
Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement Marilyn Szekendi, PhD, RN ANA 7 th Annual Nursing Quality Conference, February 2013 Research Team Banafsheh Sadeghi,
Status of anticoagulation therapy in 2016: Is there a need for venous revascularization?
 Status of anticoagulation therapy in 2016: Is there a need for venous revascularization? Rupert M. Bauersachs Dept. of Vascular Medicine, Darmstadt Center of Thrombosis Hemostasis, Mainz Status of anticoagulation
Status of anticoagulation therapy in 2016: Is there a need for venous revascularization? Rupert M. Bauersachs Dept. of Vascular Medicine, Darmstadt Center of Thrombosis Hemostasis, Mainz Status of anticoagulation
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies
 VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
Update on the Management of Cancer Associated VTE
 Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
2/28/16. Cancer and Venous Thromboembolism. Outline. 1. Pathophysiology and Clinical Relevance. No Disclosures
 Cancer and Venous Thromboembolism No Disclosures Bob Richard, MD PhD VA Puget Sound Assoc Prof UW School of Medicine Outline 1. Pathophysiology and Clinical Relevance 2. Screening For Occult Malignancy
Cancer and Venous Thromboembolism No Disclosures Bob Richard, MD PhD VA Puget Sound Assoc Prof UW School of Medicine Outline 1. Pathophysiology and Clinical Relevance 2. Screening For Occult Malignancy
New Anticoagulants Therapies
 New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
TRANSPARENCY COMMITTEE OPINION. 18 April 2007
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 April 2007 ARIXTRA 2.5 mg/0.5 ml, solution for injection in prefilled syringe Pack of 2 (CIP: 359 225-4) Pack of
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 April 2007 ARIXTRA 2.5 mg/0.5 ml, solution for injection in prefilled syringe Pack of 2 (CIP: 359 225-4) Pack of
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Challenges in Anticoagulation and Thromboembolism
 Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Keynote lecture: Oral anticoagulation and DVT
 Keynote lecture: Oral anticoagulation and DVT What is the evidence? Is there a need to anticoagulate every lower leg DVT? Disclosure Speaker name:...sebastian Schellong... I have the following potential
Keynote lecture: Oral anticoagulation and DVT What is the evidence? Is there a need to anticoagulate every lower leg DVT? Disclosure Speaker name:...sebastian Schellong... I have the following potential
Duration of Anticoagulation? Peter Verhamme MD, PhD Department of Cardiovascular Medicine University of Leuven Belgium
 Duration of Anticoagulation? Peter Verhamme MD, PhD Department of Cardiovascular Medicine University of Leuven Belgium Disclosures Honoraria and research support: Daiichi-Sankyo, Boehringer Ingelheim,
Duration of Anticoagulation? Peter Verhamme MD, PhD Department of Cardiovascular Medicine University of Leuven Belgium Disclosures Honoraria and research support: Daiichi-Sankyo, Boehringer Ingelheim,
C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School
 Novel Strategies to Prevent Pulmonary Embolism and DVT: APEX Trial and Substudies C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School Conflict of Interest Statement 2 Present Research/Grant
Novel Strategies to Prevent Pulmonary Embolism and DVT: APEX Trial and Substudies C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School Conflict of Interest Statement 2 Present Research/Grant
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Treatment of cancer-associated venous thromboembolism by new oral anticoagulants: a meta-analysis
 Original Article Page of 9 Treatment of cancer-associated venous thromboembolism by new oral anticoagulants: a meta-analysis Satyanarayana R. Vaidya, Sonu Gupta, Santhosh R. Devarapally, Department of
Original Article Page of 9 Treatment of cancer-associated venous thromboembolism by new oral anticoagulants: a meta-analysis Satyanarayana R. Vaidya, Sonu Gupta, Santhosh R. Devarapally, Department of
Slide 1. Slide 2. Slide 3. Outline of This Presentation
 Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
ADVANCES IN ANTICOAGULATION
 ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants