Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer
|
|
|
- Shanon Shaw
- 6 years ago
- Views:
Transcription
1 Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer Optimal Management of Incidental Pulmonary Nodule Ramin Khorasani, MD, MPH Vice Chair, Department of Radiology Director, Center for Evidence-Based Imaging Brigham and Women s Hospital Associate Professor of Radiology Harvard Medical School Boston, MA
2 Overview Use case examples to illustrate issues and risks associated with suboptimal management of incidental pulmonary nodules Review imaging criteria for interpretation of pulmonary nodules Describe published guidelines for management of incidental pulmonary nodules Demonstrate next generation IT tools designed to help improve management of incidental pulmonary nodules
3 Patient #1

4 November 2006: 64 F Cardiac CT

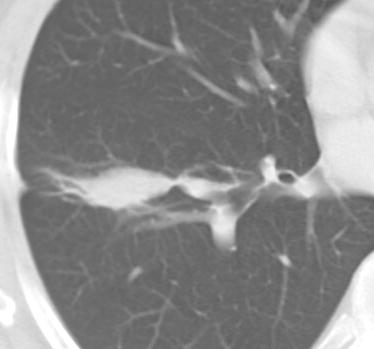
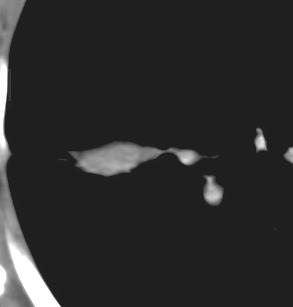
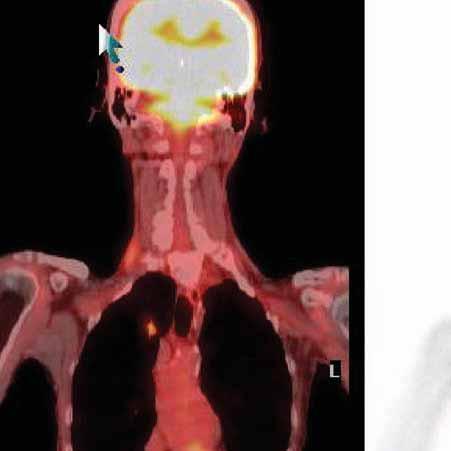
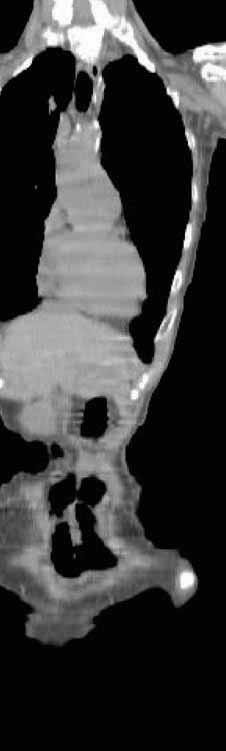
5 December 2007: History: Confusion, Brain mass Image at follow up
6 Patient #2

7 May 2005: History: Fever

8 December 2006: History: SOB

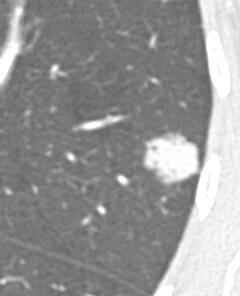
9 December 2006
10 Patient 3 LLQ pain? Diverticulitis form ED

11 Images at presnetation
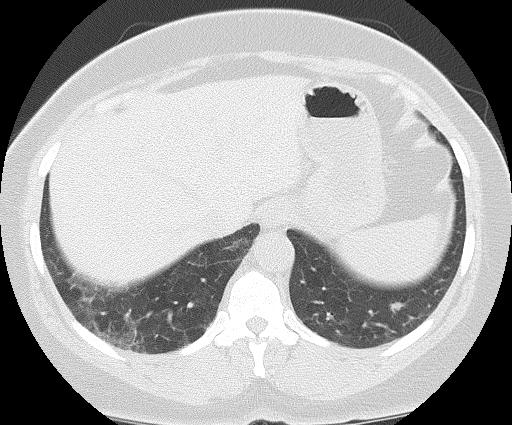
12
13 What are the performance gaps? Optimum care of these patients requires: [Address the urgent clinical need and relevant imaging findings which led to imaging, as routine screening with CXR, CT not recommended based on current evidence] Must improve detection, diagnosis, communication, appropriate follow up and management of incidental pulmonary nodules

14 Ann Louise Puopolo, BSN, RN Director, Loss Prevention & Patient Safety
15 Top CRICO Cancer-related Cases with a diagnosis-related allegation number of cases breast colorectal lung prostate N = 160 CRICO PL cases asserted 1/1/98 10/1/08 with a diagnosis-related major allegation and final diagnosis of breast, colorectal, lung or prostate cancer. Ramin Total incurred Khorasani, losses= $109 MD, million. 2009
16 CRICO Lung Cancer Outpatient Cases responsible service 8 $10,000,000 7 claim count total incurred $9,000,000 number of cases $8,000,000 $7,000,000 $6,000,000 $5,000,000 $4,000,000 $3,000,000 $2,000,000 total incurred 1 $1,000,000 0 Internal Medicine Radiology Hematology Immunology And Allergy $0 Oncology (Medical) N=17 outpatient PL cases asserted 1/1/03-10/1/08 with a final diagnosis of lung cancer and a diagnosis-related major allegation. Total Incurred=aggregate of expenses, reserves, and payments on open and closed cases.
17 CRICO Lung Cancer Outpatient Cases By Assert Year By Loss Year All events 8 6 High Medium Low 8 6 Cases asserted in past five years Statute of Limitations N=17 outpatient PL cases asserted 1/1/03-10/1/08 with a final diagnosis of lung cancer and a diagnosis-related major allegation. Severity Scale: High= Death, Permanent Grave, Permanent Major or Permanent Significant Medium= Permanent Minor, Temporary Major or Temporary Minor Low= Temporary Insignificant, Emotional Only or Legal Issue Only
18 CRICO Lung Cancer Outpatient Cases diagnosis-related process of care Step # cases % of cases 1. Patient notes problem and seeks care 2. History/physical and evaluation of symptoms 3. Order of diagnostic/lab tests 4. Performance of tests 5. Interpretation of tests 6. Receipt/transmittal of test results 7. Physician follow up with patient 8. Referral management 9. Patient compliance with follow-up plan 1 6% % 82% 6% 53% 29% 24% 0% 0% Total incurred $12,416 $7,082,698 $14,433,64 6 $1,040,000 $9,490,766 $5,217,968 $5,745,182 $0 $0 N=24 outpatient PL cases asserted 1/1/03-10/1/08 with a final diagnosis of lung cancer and a diagnosis-related major allegation. Total Incurred=aggregate of expenses, reserves, and payments on open and closed cases.
19 Top Contributing Factors Issue % of cases* Misinterpretation of diagnostic studies 44% Communication among providers patient condition 20% Failure/delay in ordering diagnostic test 12% Test result management 11% Patient did not receive result Result not received by clinician other Insufficient/lack of documentation adverse event 8% Reliance on negative finding w/ continued symptoms 8% Failure to establish differential diagnosis 7% Failure to respond to patient s concerns 7% Possible technical problem 7% *A case may have multiple factors identified. N=75 PL cases asserted 1/1/03-6/30/08 with a physician specialty or responsible service of Radiology.
20 CRICO Lung Cancer Outpatient Cases physician specialty General Medicine Radiology/Imaging Hematology/Oncology General Surgery Rheumatology/Immunology Neurosurgery Ent defendant counts 31 physician defendants named in 17 outpatient PL cases asserted 1/1/03-10/1/08 with a final diagnosis of lung cancer and a diagnosis-related major allegation.
21 Summary CRICO Lung cancer outpatient cases asserted 1/1/03 10/1/08 # cases asserted 17 Average indemnity incurred $1,067,694 Lung cancer outpatient cases closed 1/1/03 10/1/08 # cases closed 18 % cases closed with payment 44% Average indemnity payment $969,989 # cases closed with payment >=$1 million 2
22 Lung Cancer It is estimated that 219,440 men and women (116,090 men and 103,350 women) will be diagnosed with and 159,390 men and women will die of cancer of the lung and bronchus in 2009* More men die from lung cancer than colorectal, prostate and pancreatic cancers combined More women die from lung cancer than breast, uterine and ovarian cancers combined *Reference: National Cancer Institute:

23 Reference: National Cancer Institute
24 5 year Relative Survival Rate for Non-Small Cell Lung Cancer Reference: American Cancer Society
25 Detection
26 Imaging as a screening tool CXR screening has not been shown to reduce disease specific mortality Several Low dose CT(LDCT) trials already completed Routine use as a screening tool not supported by current evidence No reduction in disease specific mortality High false positive rate National Lung Screening Trial ongoing, reporting by mid-2010
27 National Lung Screening Trial NLST Compares CT vs Chest X-Ray for reducing lung cancer specific mortality Smokers aged years 53,000 participants at 30 sites Reporting in 2010
28 National Lung Screening Trial (NLST) Nodule < 4 mm in diameter no follow-up between annual screens Nodule > 4 mm minimum f/u 6 mo in addition to annual screens Nodules that grow, are spiculated or large go on to biopsy or resection
29 CT Screening Trials No. Screened % Nodules Lung Ca Stage I Kaneko (1996) % 93 Sone (1998) % 84 Henschke (1999) % 2.7% 85 Swensen (2000) % 1.3% 71 Dederick (2002) % 1.3% 58 Nawa (2002) % 0.4% 86%
30 LDCT Missed Lung Cancer 1443 individuals (5,418 CT s) 7/22 retrospectively found Size - 6 mm (range 4-13 mm) 6 Stage 1; 1 Stage 2 Kakinuma, 1999
31 MISSED CANCERS General population-32 of 83 missed initially 88% stage 1A Sizes detection error (9.8 mm) interpretation error (15.9 mm) Detection errors 91% GGO Interpretation errors TB, fibrosis Li. Radiology 2002; 225
32 MISSED NODULES Missed nodules many < 4mm Factors - location, partial volume, parenchymal disease Most proven missed cancers are early stage lesions at diagnosis
33 NODULE SIZE AS RISK FACTOR FOR CA: Results of Baseline Study (N = 233) Size (mm) # % Tiny nodules-very low incidence of cancer Henschke C. Lancet 1999; 354

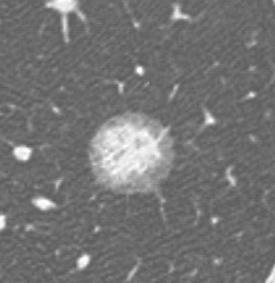
34 Adenocarcinoma 40 year old female
35 Diagnosis and Management

36 RaminReference: Khorasani, MD, MacMahon 2009 H MB BCh, et al. Radiology 2005; 237:
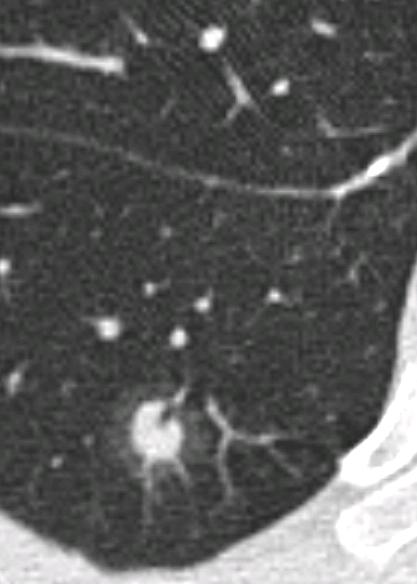
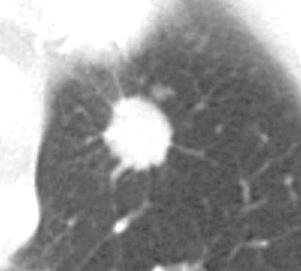
37 Size Radiologic Interpretation: NODULE FEATURES Growth rate Stable in 2 years: benign Malignant: doubling time 30days to 180 days Internal characteristics Ca++: benign Ground glass opacities Shape, margins and contour Benign features: Smooth, round Malignant features: Spiculated Satelite lesions: (granulomatous process)


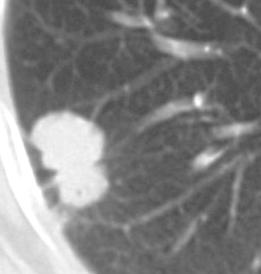
38 CALCIFIED GRANULOMA Narrow collimation advantage

39 Inflammatory nodule -12 month resolution
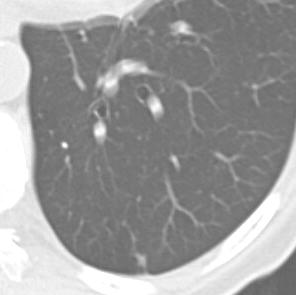
40 Ca+ INDETERMINATE NODULE 4-7 mm Thin-section CT at 6 m. Benign Indeterminate CT at 12 mo size > 8mm PET or Biopsy size Biopsy or PET CT at 24 mo size Biopsy or PET


41 6 m follow up: No Change

42 Inflammatory opacity 6 m


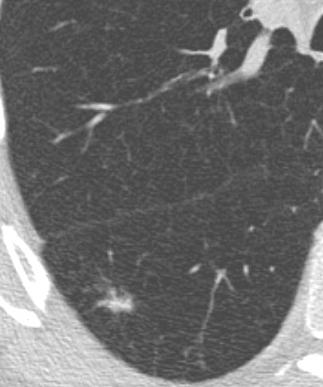
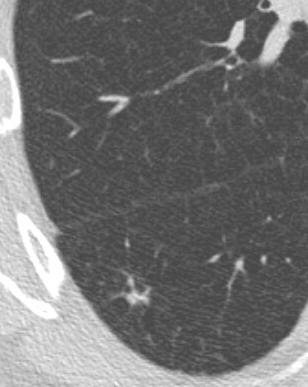
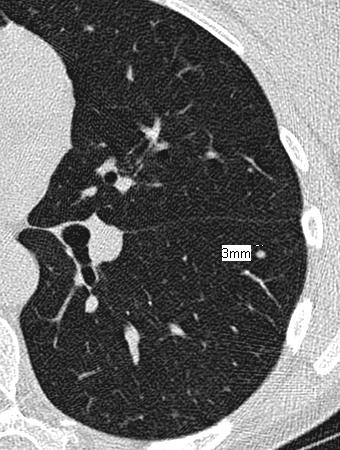
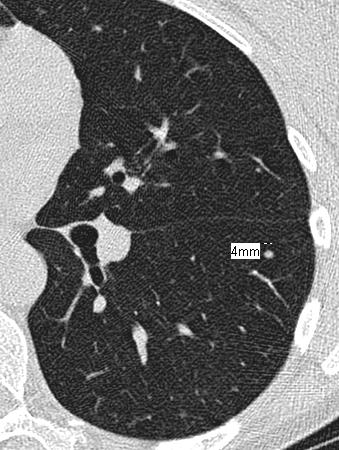
43 6mm HRCT 9mm Baseline CT 6 m Increase in size Adenocarcinoma, papillary type
44 NODULE GROWTH DOUBLING TIME -Stable in 2 years: benign -Malignant: doubling time 30days to 18 months
45 DETECTING VOLUME CHANGE: SMALL NODULES volume doubling volume doubling 4 mm 5 mm 6.2 mm 3 cm 3.75 cm 4.70 cm
46 Inter-observer Variation
47 VARIABLES IN NODULE SIZING Scan technique-collimation, reconstruction interval, F.O.V. Observer variables, cursor location

48 Adenocarcinoma Initial scan At 10 months
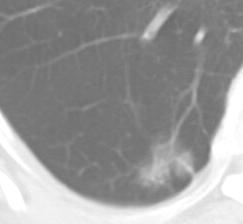
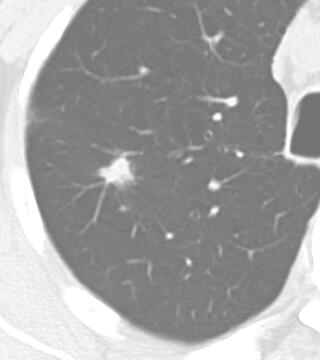
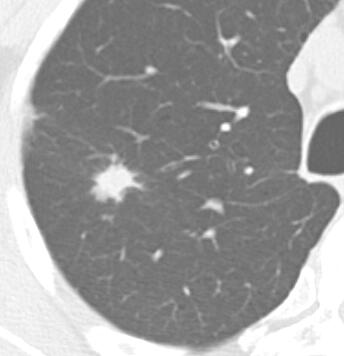
49 SHAPE, MARGINS, & CONTOUR Smooth, round - benign Spiculated (corona radiata) - malignant Satellite lesions - granulomatous process

50 Baseline 6 m. MAI GRANULOMA
51 Adenocarcinoma Squamous cell carcinoma

52 Bronchoalveolar carcinoma
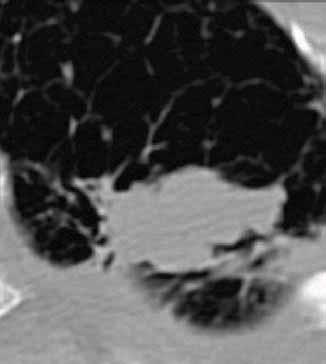
53 GROUND GLASS OPACITIES (GGO)


54 Screen 6 m 9 m Bronchoalveolar Carcinoma

55 CAUSES OF GGO Slow growing bronchoalveolar carcinoma Atypical adenomatous hyperplasia Organizing pneumonia Inflammatory pseudotumor Lymphoma
56 GGO: CT / PATHOLOGY 43 GGO`s < 2 cm resected BAC 23;Adenocarcinoma 11; AAH 9 GGO and solid component 93% malignant Nakata Chest 2002
57 INDETERMINATE NODULE (8-20 mm) PET-FDG SCAN (-) 3+12 mo F/U CT (+) FDG Biopsy/VATS/ Lobectomy
58 THORACIC NEEDLE BIOPSY Sensitivity - 90% overall Nodules < 15mm PPV-100%, NPV- 88% Benign diagnoses > 80% with small cutting needles Pneumothorax & hemorrhage 5-30%
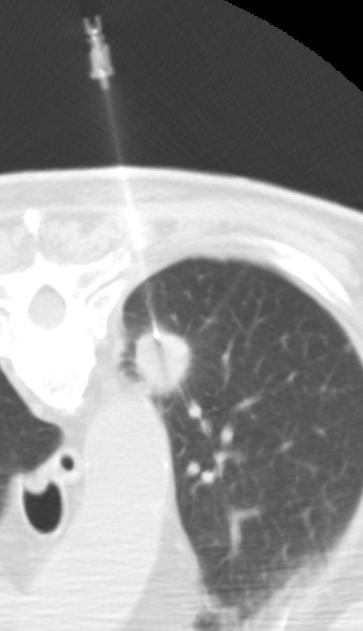
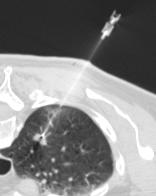
59 CT Fluoroscopic biopsy
60 FDG IMAGING (PET) Overnight fasting: scan mins post injection 1 mg Ativan muscle relaxant Attenuation correction allows calculation of absolute FDG uptake rates

61 ADENOCARCINOMA 1 YEAR GROWTH - PET+
62 PET and Indeterminate SPN (< 3 cm) METANALYSIS-Gould (JAMA 2001) 40 studies with 1474 focal pulmonary lesions where PET performed Sensitivity of 96.8 % and a specificity of 77.8% PET improves characterization of SPN with very high negative predictive value PET use for pulmonary nodules Watch and wait is a safe strategy in PET-negative nodules Malignancy must be excluded in PET-positive nodules LIMITATIONS: Small nodules (< 6-7 mm) have higher false negative rate False positives associated with inflammation, granulomatous disease, fungal infections

63 LUL 1 cm Adenocarcinoma Emphysema


64 8mm nodule Unchanged at 6 months - Negative PET scan

65 Organizing Pneumonia Mild PET Activity
66 FALSE NEGATIVES Bronchoalveolar cell carcinomas Carcinoid Small slow growing adenocarcinoma Acellular tumor
67 PET/CT ADVANTAGES Distinguish physiologic uptake from tumor Precise localization of uptake Localize uptake to specific nodes Single examination - staging






68
69 Summary: PET and SPN Negative PET most likely benign but can be followed rather than biopsied Positive PET should be considered potentially malignant- consider biopsy or resection
70 Communication Among Caregivers
71 National Patient Safety Goal Joint Commission Goal 2: Improve the effectiveness of communication among caregivers 2A. For verbal or telephone orders or for telephonic reporting of critical test results, verify the complete order or test result by having the person receiving the information record and "read-back" the complete order or test result. Ref:
72 National Patient Safety Goal Joint Commission Goal 2: Improve the effectiveness of communication among caregivers 2C. Measure, assess and, if appropriate, take action to improve the timeliness of reporting, and the timeliness of receipt by the responsible licensed caregiver, of critical test results and values.. Ref:
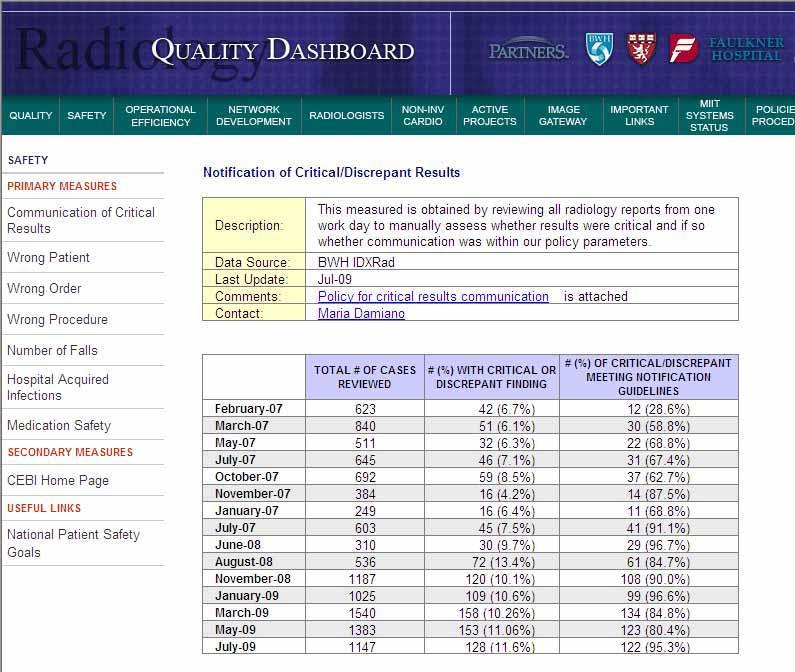
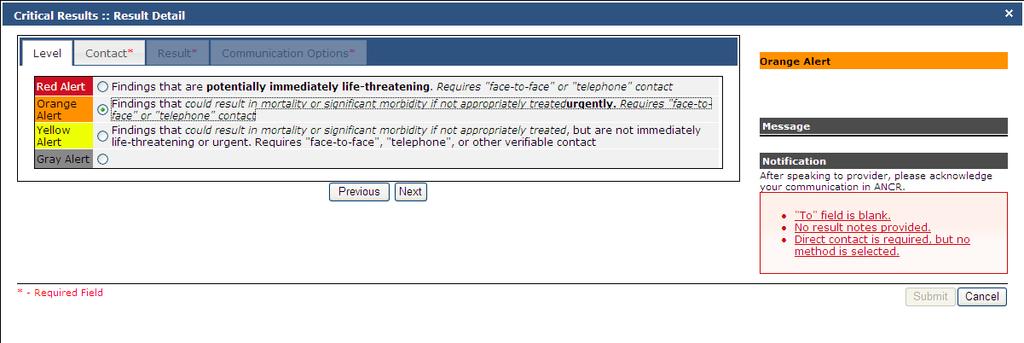
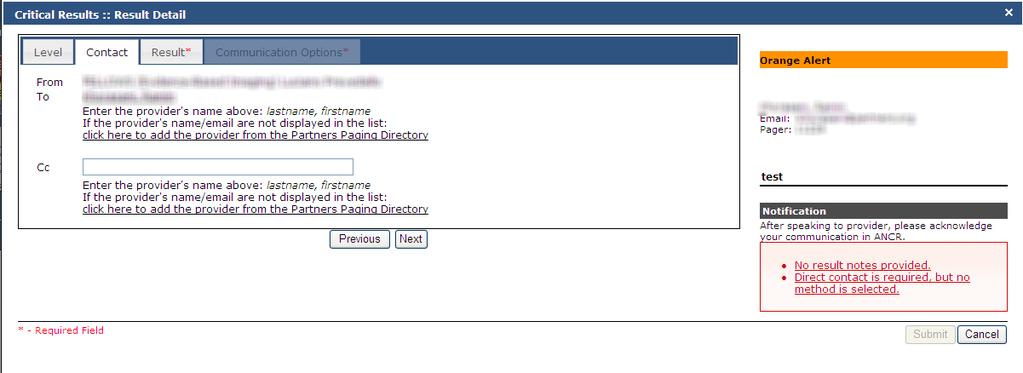
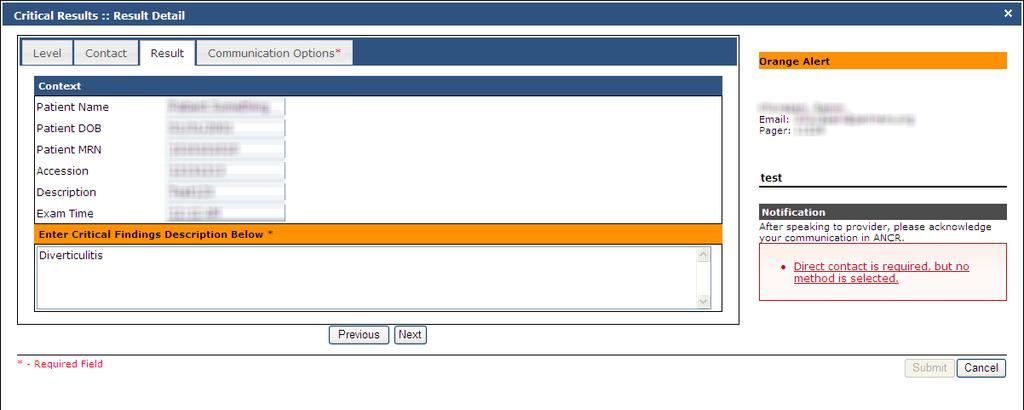
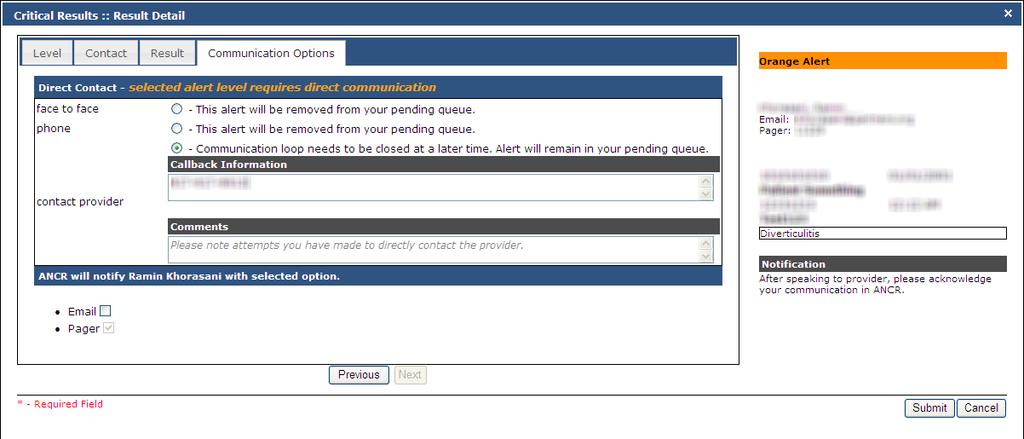
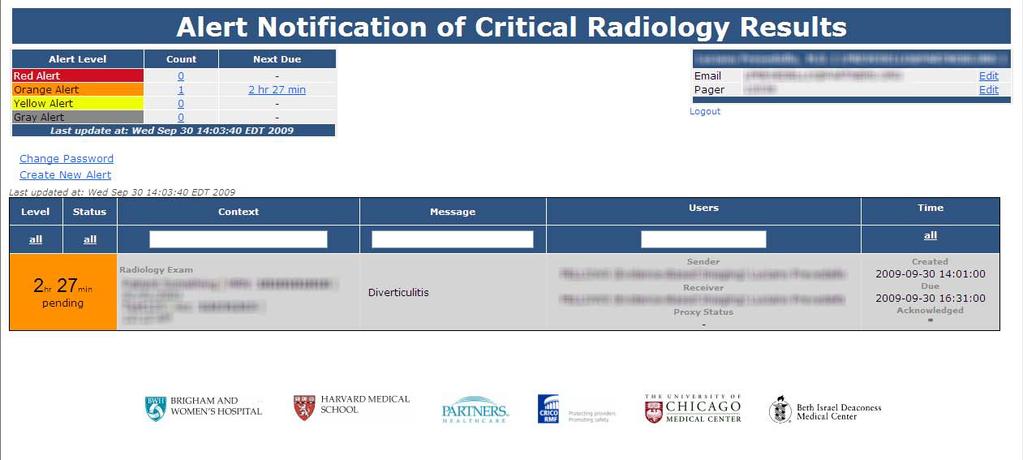
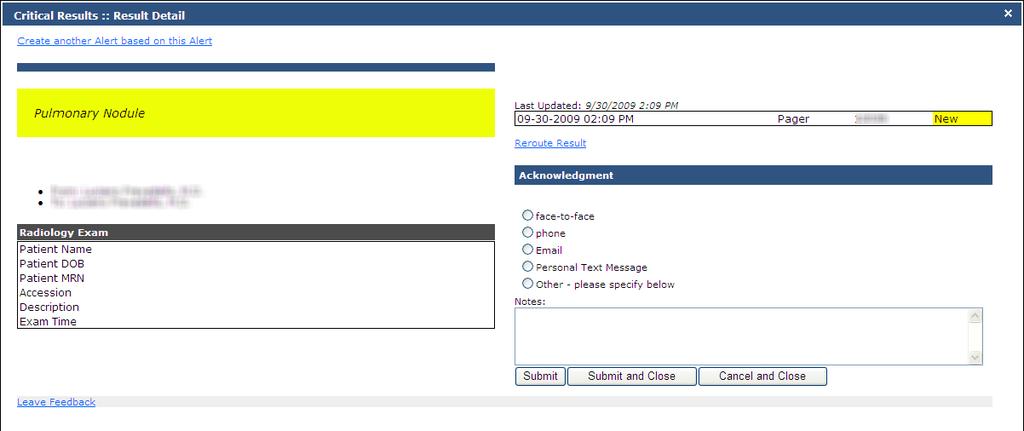
73 BWH Policies and procedures: [Definitions & Functional Requirements for Enabling IT tools] Department of Radiology, Brigham and Woman s Hospital Policy for Communicating Critical and/or Discrepant Results (approved 1/31/2006) Purpose: Notification of the patient s healthcare provider when the radiologist determines that an imaging study has new and unexpected findings that could result in mortality or significant morbidity. Policy: 1. Radiology findings requiring direct notification of a member of the patient s care team (defined as a healthcare professional immediately responsible for the care of the patient, including requesting physician, covering physician, attending physician, physician assistant, nurse, or nurse practitioner): Critical: a new/unexpected radiologic finding that could result in mortality or significant morbidity if appropriate diagnostic and/or therapeutic follow-up steps are not undertaken Discrepant: An interpretation that is significantly different from a preliminary interpretation, when the preliminary interpretation has been accessible to the patient care team and the difference in interpretations may alter the patient s diagnostic workup or management 2. Timelines for notification: Radiology reports should be read and signed in a timely manner [Note 1], and critical/discrepant results should be communicated as soon as possible after they are discovered. In all cases, successful communication should occur within the following timelines, which depend on the urgency level of the findings: Red alert (new/unexpected findings that are potentially immediately life-threatening, such as tension pneumothorax, ischemic bowel, or intracerebral hemorrhage): These results require immediate interruptive notification of the ordering physician, covering physician, or other care team member who can initiate the appropriate clinical action for the patient. In all such cases, notification must be within 60 minutes of discovery of findings Orange alert (new/unexpected findings that could result in mortality or significant morbidity if not appropriately treated urgently [within 2-3 days], such as an intra-abdominal abscess or impending pathological hip fracture): Notification must be within 3 hours of discovery of findings Yellow alert (new/unexpected findings that could result in mortality or significant morbidity if not appropriately treated, but are not immediately life-threatening or urgent, such as a nodule on a chest x-ray or a solid renal mass on an ultrasound examination): Notification must be within 3 days of discovery of findings If no member of the patient s care team can be contacted in a timely fashion, an escalation process is defined [Note 2] to assure that the communication occurs within the above timelines. 3. Mode of Communication: Red and orange alerts must be communicated via face-to-face or telephone contact. Yellow alerts can be communicated in one of these ways, or via another method that allows the communicator to verify that notification was successful. As per JCAHO, is not a verifiable method of communication of critical/discrepant results. 4. The person communicating the critical/discrepant radiological finding should be certain that the member of the patient care team is aware of the critical nature of the findings. 5. The details of the communication must be clearly documented in the radiology report, preferably in or immediately following the Impression section of the report or as an addendum if the report was finalized before communication is complete. Documentation must contain the following information: a. Name of the communicator b. Date and time reported c. Name of recipient of the notification Sample statement: Critical findings were communicated by Dr. Radiologist to Dr. Surgeon at 5 PM on Wednesday December 15 th, The Radiology Department will monitor and measure compliance with the policy [Note 3]
74
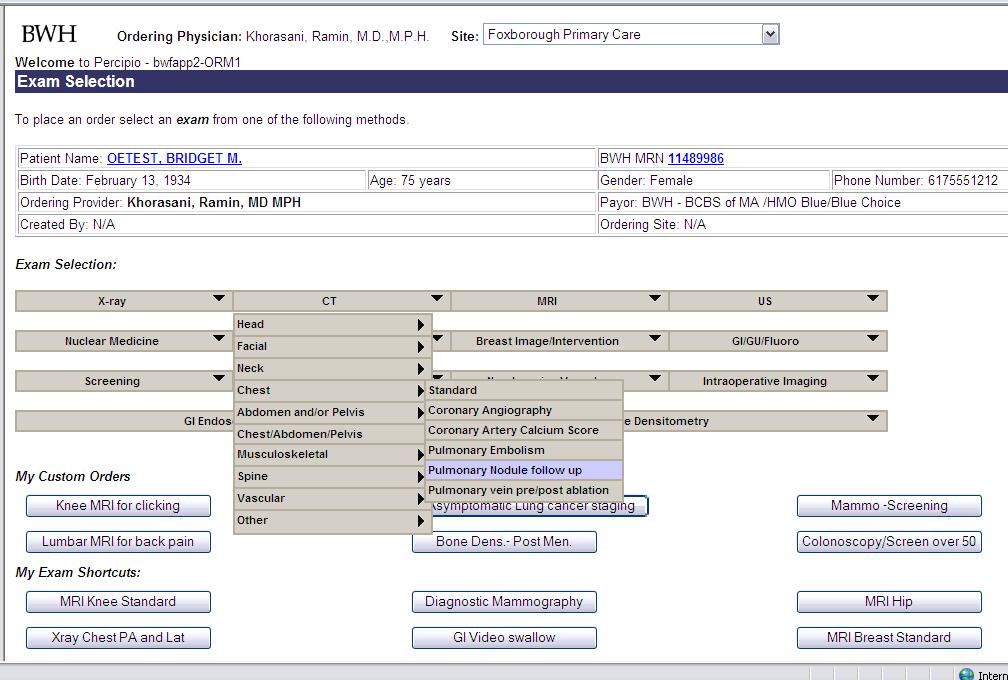
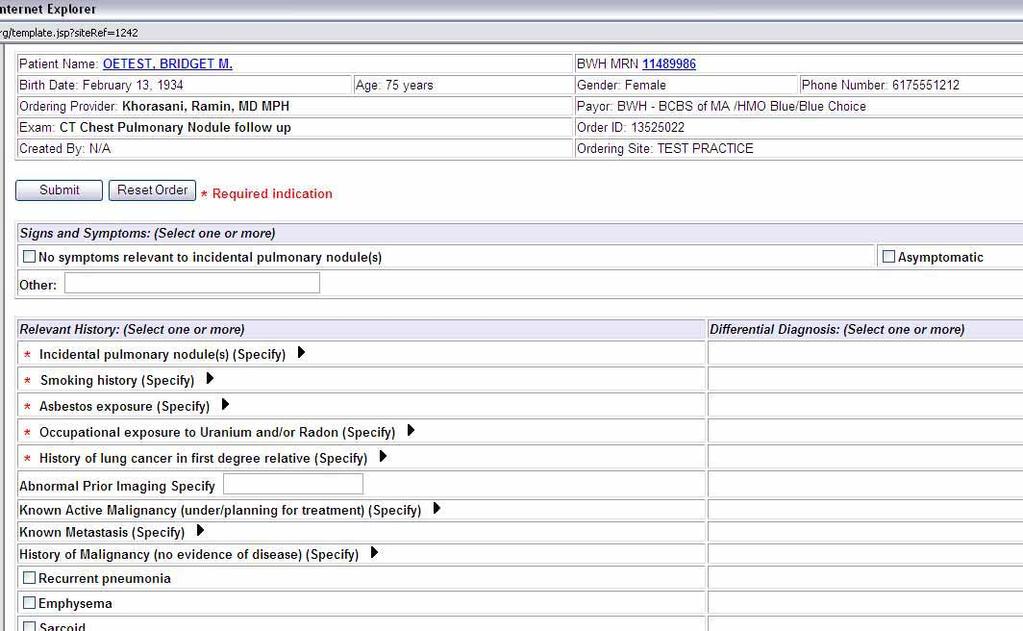
75 Examples of Next Generation IT tools for improved management of incidental pulmonary nodules


76 Computer Aided Tools Improved nodule detection in large data sets Reduce reading times Quantification volume measurements Characterization



77 Baseline CT 12 month Follow up CT
78
79
80
81 Powerscribe Radiology Screen
82
83
84
85
86
87
88
89 Summary Optimal management of Incidental pulmonary nodules will improve patient safety and quality of care Suboptimal care is a source of patient harm and malpractice risk Improvements in detection, diagnosis, appropriate followup and management of these nodules will benefit from next generation IT tools embedded in physician workflow
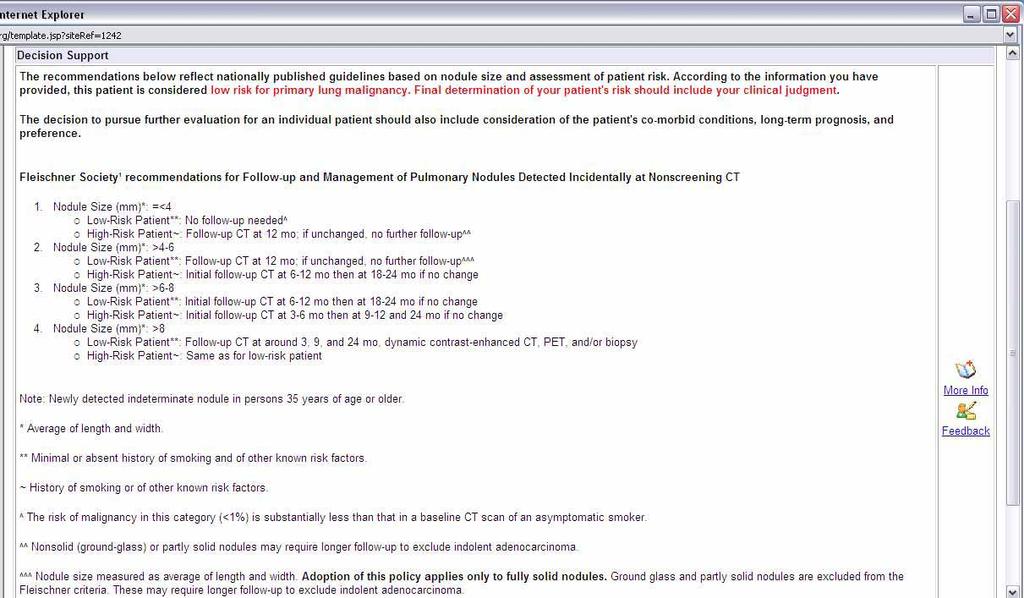
90 What you can do today! Encourage leaders at your institution to include incidental lung nodules as a key component of optimizing communication of critical results (A Joint Commission mandate) Follow Fleishner Society guidelines for management of small indeterminate pulmonary nodules
91 Fleischner Society Small Nodule Followup Nodule Size Low Risk Pt High Risk Pt </=4 mm None 12 m No -stop 4 6 mm 12 m No -stop 6-12 m; No then m 6 8 mm 6-12 m If no then m 3-6 m If no then m > 8 mm CT 3, 9, 24 m or CE CT; PET; or biopsy Radiology Nov, 2005
92 Thank you Special thanks to (for material provided for this workshop): Francine Jacobson, MD, Luciano Prevedello, MD,
GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES
 Venice 2017 GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES Heber MacMahon MB, BCh Department of Radiology The University of Chicago Disclosures Consultant for Riverain Medical
Venice 2017 GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES Heber MacMahon MB, BCh Department of Radiology The University of Chicago Disclosures Consultant for Riverain Medical
PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES. https://tinyurl.com/hmpn2018
 PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES Heber MacMahon MB, BCh Department of Radiology The University of Chicago https://tinyurl.com/hmpn2018 Disclosures Consultant
PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES Heber MacMahon MB, BCh Department of Radiology The University of Chicago https://tinyurl.com/hmpn2018 Disclosures Consultant
LUNG NODULES: MODERN MANAGEMENT STRATEGIES
 Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
CT Screening for Lung Cancer for High Risk Patients
 CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Lung Cancer Screening: To Screen or Not to Screen?
 Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI
 Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI Pulmonary Nodules Well-circumscribed, radiographic opacities measuring 3 cm in diameter Surrounded by aerated lung Not associated with atelectesis
Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI Pulmonary Nodules Well-circumscribed, radiographic opacities measuring 3 cm in diameter Surrounded by aerated lung Not associated with atelectesis
Learning Objectives. 1. Identify which patients meet criteria for annual lung cancer screening
 Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
I appreciate the courtesy of Kusumoto at NCC for this presentation. What is Early Lung Cancers. Early Lung Cancers. Early Lung Cancers 18/10/55
 I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
Deppen S, et al. Annals of Thoracic Surgery 2011;92:
 Deppen S, et al. Annals of Thoracic Surgery 2011;92:428-33. http://www.nationmaster.com/graph/ mor_his-mortality-histoplasmosis http://www.humirarems.com/brochure.aspx Baddley, John W., et al. Emerging
Deppen S, et al. Annals of Thoracic Surgery 2011;92:428-33. http://www.nationmaster.com/graph/ mor_his-mortality-histoplasmosis http://www.humirarems.com/brochure.aspx Baddley, John W., et al. Emerging
Approach to Pulmonary Nodules
 Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
What to know and what to make of it
 Lung Cancer Screening: What to know and what to make of it J. Matthew Reinersman, MD Assistant Professor of Surgery Division of Thoracic and Cardiovascular Surgery Department of Surgery University of Oklahoma
Lung Cancer Screening: What to know and what to make of it J. Matthew Reinersman, MD Assistant Professor of Surgery Division of Thoracic and Cardiovascular Surgery Department of Surgery University of Oklahoma
Evidence based approach to incidentally detected subsolid pulmonary nodule. DM SEMINAR July 27, 2018 Harshith Rao
 Evidence based approach to incidentally detected subsolid pulmonary nodule DM SEMINAR July 27, 2018 Harshith Rao Outline Definitions Etiologies Risk evaluation Clinical features Radiology Approach Modifications:
Evidence based approach to incidentally detected subsolid pulmonary nodule DM SEMINAR July 27, 2018 Harshith Rao Outline Definitions Etiologies Risk evaluation Clinical features Radiology Approach Modifications:
Screening for Lung Cancer: Are We There Yet?
 Screening for Lung Cancer: Are We There Yet? Kavita Garg, MD Professor of Radiology University of CO, Denver Mountain States Cancer Conference Nov 6 th 2010 The Epidemiology of Lung Cancer Tobacco is the
Screening for Lung Cancer: Are We There Yet? Kavita Garg, MD Professor of Radiology University of CO, Denver Mountain States Cancer Conference Nov 6 th 2010 The Epidemiology of Lung Cancer Tobacco is the
Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2
 Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2 The Committee for Management of CT-screening-detected Pulmonary Nodules 2009-2011 The Japanese Society of CT Screening
Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2 The Committee for Management of CT-screening-detected Pulmonary Nodules 2009-2011 The Japanese Society of CT Screening
Lung Cancer Diagnosis for Primary Care
 Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
Pulmonary Nodules. Michael Morris, MD
 Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis
 19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
DENOMINATOR: All final reports for CT imaging studies with a finding of an incidental pulmonary nodule for patients aged 35 years and older
 Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
The small subsolid pulmonary nodules. What radiologists need to know.
 The small subsolid pulmonary nodules. What radiologists need to know. Poster No.: C-1250 Congress: ECR 2016 Type: Educational Exhibit Authors: L. Fernandez Rodriguez, A. Martín Díaz, A. Linares Beltrán,
The small subsolid pulmonary nodules. What radiologists need to know. Poster No.: C-1250 Congress: ECR 2016 Type: Educational Exhibit Authors: L. Fernandez Rodriguez, A. Martín Díaz, A. Linares Beltrán,
SCBT-MR 2015 Incidentaloma on Chest CT
 SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium Incidental
SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium Incidental
Lung Cancer Screening:
 Lung Cancer Screening: Maximizing Gain and Dealing with Pandora s Box Mark M. Fuster, MD Division of Pulmonary & Critical Care UCSD Department of Medicine & VA San Diego Healthcare Service San Diego, CA
Lung Cancer Screening: Maximizing Gain and Dealing with Pandora s Box Mark M. Fuster, MD Division of Pulmonary & Critical Care UCSD Department of Medicine & VA San Diego Healthcare Service San Diego, CA
The Spectrum of Management of Pulmonary Ground Glass Nodules
 The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
Positron Emission Tomography in Lung Cancer
 May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
With recent advances in diagnostic imaging technologies,
 ORIGINAL ARTICLE Management of Ground-Glass Opacity Lesions Detected in Patients with Otherwise Operable Non-small Cell Lung Cancer Hong Kwan Kim, MD,* Yong Soo Choi, MD,* Kwhanmien Kim, MD,* Young Mog
ORIGINAL ARTICLE Management of Ground-Glass Opacity Lesions Detected in Patients with Otherwise Operable Non-small Cell Lung Cancer Hong Kwan Kim, MD,* Yong Soo Choi, MD,* Kwhanmien Kim, MD,* Young Mog
Managing Error in Ambulatory Care
 Ann L. Puopolo, BSN, RN Current Clinical Issues in Primary Care Managing Error in Ambulatory Care Ann Louise Puopolo, BSN,RN Director, Loss Prevention & Patient Safety Risk Management Foundation of the
Ann L. Puopolo, BSN, RN Current Clinical Issues in Primary Care Managing Error in Ambulatory Care Ann Louise Puopolo, BSN,RN Director, Loss Prevention & Patient Safety Risk Management Foundation of the
Pulmonary Nodules: When to worry, when to chill. Douglas Arenberg Associate Professor Pulmonary & Critical Care
 Pulmonary Nodules: When to worry, when to chill Douglas Arenberg Associate Professor Pulmonary & Critical Care Disclosure MDCH Grant Funds to improve tobacco cessation service in the Michigan Medicine
Pulmonary Nodules: When to worry, when to chill Douglas Arenberg Associate Professor Pulmonary & Critical Care Disclosure MDCH Grant Funds to improve tobacco cessation service in the Michigan Medicine
Christine Argento, MD Interventional Pulmonology Emory University
 Christine Argento, MD Interventional Pulmonology Emory University Outline Lung Cancer Statistics Prior Studies for Lung Cancer Screening NLST Studies Following NLST Future Directions Lung Cancer American
Christine Argento, MD Interventional Pulmonology Emory University Outline Lung Cancer Statistics Prior Studies for Lung Cancer Screening NLST Studies Following NLST Future Directions Lung Cancer American
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
The Maine Lung Cancer Coalition. Working Together to Reduce Lung Cancer in Maine
 The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
Small Pulmonary Nodules: Our Preliminary Experience in Volumetric Analysis of Doubling Times
 Small Pulmonary Nodules: Our Preliminary Experience in Volumetric Analysis of Doubling Times Andrea Borghesi, MD Davide Farina, MD Roberto Maroldi, MD Department of Radiology University of Brescia Brescia,
Small Pulmonary Nodules: Our Preliminary Experience in Volumetric Analysis of Doubling Times Andrea Borghesi, MD Davide Farina, MD Roberto Maroldi, MD Department of Radiology University of Brescia Brescia,
THE BENEFITS OF BIG DATA
 THE BENEFITS OF BIG DATA Disclosures I am a named inventor on a number of patents and patent applications relating to the evaluation of pulmonary nodules on CT scans of the chest which are owned by Cornell
THE BENEFITS OF BIG DATA Disclosures I am a named inventor on a number of patents and patent applications relating to the evaluation of pulmonary nodules on CT scans of the chest which are owned by Cornell
Published Pulmonary Nodule Guidelines A Synthesis
 Published Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj Royal Brompton Hospital London 4/28/2015 1 And very soon to be published Published ^ Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj
Published Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj Royal Brompton Hospital London 4/28/2015 1 And very soon to be published Published ^ Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj
A Comprehensive Cancer Center Designated by the National Cancer Institute
 N C I C C C A Comprehensive Cancer Center Designated by the National Cancer Institute Screening and Early Detection of Lung Cancer: Ready for Practice? David S. Ettinger, MD, FACP, FCCP Alex Grass Professor
N C I C C C A Comprehensive Cancer Center Designated by the National Cancer Institute Screening and Early Detection of Lung Cancer: Ready for Practice? David S. Ettinger, MD, FACP, FCCP Alex Grass Professor
A Review of Medical Malpractice Claims from the CRICO Comparative Benchmarking System
 A Review of Medical Malpractice Claims from the CRICO Comparative Benchmarking System (CBS: a national database of medical malpractice claims from captive & commercial insurers across the US ) Note: I
A Review of Medical Malpractice Claims from the CRICO Comparative Benchmarking System (CBS: a national database of medical malpractice claims from captive & commercial insurers across the US ) Note: I
Imaging Decisions Start Here SM
 Owing to its high resolution and wide anatomic coverage, dynamic first-pass perfusion 320-detector-row CT outperforms PET/CT for distinguishing benign from malignant lung nodules, researchers from Japan
Owing to its high resolution and wide anatomic coverage, dynamic first-pass perfusion 320-detector-row CT outperforms PET/CT for distinguishing benign from malignant lung nodules, researchers from Japan
LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University
 LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University Objective LDCT lung cancer screening (LCS) Potential Benefits & Harms Recommendation of
LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University Objective LDCT lung cancer screening (LCS) Potential Benefits & Harms Recommendation of
VHA Demonstration Project for Lung Cancer Screening Using Low-Dose Chest CT Screening
 VHA Demonstration Project for Lung Cancer Screening Using Low-Dose Chest CT Screening ATS San Francisco 2016 James K. Brown MD 1, Kathryn L. Rice, MD 2 (1) San Francisco VA (2) Minneapolis VAMC Disclosures
VHA Demonstration Project for Lung Cancer Screening Using Low-Dose Chest CT Screening ATS San Francisco 2016 James K. Brown MD 1, Kathryn L. Rice, MD 2 (1) San Francisco VA (2) Minneapolis VAMC Disclosures
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Comparison of three mathematical prediction models in patients with a solitary pulmonary nodule
 Original Article Comparison of three mathematical prediction models in patients with a solitary pulmonary nodule Xuan Zhang*, Hong-Hong Yan, Jun-Tao Lin, Ze-Hua Wu, Jia Liu, Xu-Wei Cao, Xue-Ning Yang From
Original Article Comparison of three mathematical prediction models in patients with a solitary pulmonary nodule Xuan Zhang*, Hong-Hong Yan, Jun-Tao Lin, Ze-Hua Wu, Jia Liu, Xu-Wei Cao, Xue-Ning Yang From
Veterans Health Administration Lung Cancer Screening Demonstration Project: Results & Lessons Learned
 Veterans Health Administration Lung Cancer Screening Demonstration Project: Results & Lessons Learned Jane Kim, MD, MPH Acting Chief Consultant for Preventive Medicine National Center for Health Promotion
Veterans Health Administration Lung Cancer Screening Demonstration Project: Results & Lessons Learned Jane Kim, MD, MPH Acting Chief Consultant for Preventive Medicine National Center for Health Promotion
LUNG CANCER SCREENING: LUNG CANCER SCREENING: THE TIME HAS COME LUNG CANCER: A NATIONAL EPIDEMIC
 : THE TIME HAS COME Physician Leader, Lung Cancer Multi-Disciplinary Program Fletcher Allen Health Care Annual Meeting Montpelier, VT - April 25, 2014 Gerald S. Davis, MD Professor of Medicine University
: THE TIME HAS COME Physician Leader, Lung Cancer Multi-Disciplinary Program Fletcher Allen Health Care Annual Meeting Montpelier, VT - April 25, 2014 Gerald S. Davis, MD Professor of Medicine University
Early Detection of Lung Cancer. Amsterdam March 5 th 2010
 Early Detection of Lung Cancer Amsterdam March 5 th 2010 Rob J van Klaveren, MD, PhD Dept. of Pulmonology Erasmus MC Rotterdam, the Netherlands Early Detection and Screening - Questions to be addressed
Early Detection of Lung Cancer Amsterdam March 5 th 2010 Rob J van Klaveren, MD, PhD Dept. of Pulmonology Erasmus MC Rotterdam, the Netherlands Early Detection and Screening - Questions to be addressed
The solitary pulmonary nodule: Assessing the success of predicting malignancy
 The solitary pulmonary nodule: Assessing the success of predicting malignancy Poster No.: C-0829 Congress: ECR 2010 Type: Scientific Exhibit Topic: Chest Authors: R. W. K. Lindsay, J. Foster, K. McManus;
The solitary pulmonary nodule: Assessing the success of predicting malignancy Poster No.: C-0829 Congress: ECR 2010 Type: Scientific Exhibit Topic: Chest Authors: R. W. K. Lindsay, J. Foster, K. McManus;
Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center
 You Smoke, You Get Lung Cancer, You Die: Can Screening Change this Paradigm? Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center AATS Saturday 4/28/2012 Cancer Screening Cancer
You Smoke, You Get Lung Cancer, You Die: Can Screening Change this Paradigm? Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center AATS Saturday 4/28/2012 Cancer Screening Cancer
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Lung Cancer screening :
 Lung Cancer screening : Pro-Contra SAMO interdisciplinary workshop on chest tumors 27 and 28 january 2017 Prof L.P.Nicod Sevice de pneumologie CHUV-Lausanne -CH Lung Cancer How big is the problem? Epidemiology
Lung Cancer screening : Pro-Contra SAMO interdisciplinary workshop on chest tumors 27 and 28 january 2017 Prof L.P.Nicod Sevice de pneumologie CHUV-Lausanne -CH Lung Cancer How big is the problem? Epidemiology
Communication of Critical and/or Discrepant Findings. Stephen Alden, Lorie Cavalli and Bobby Kalb, MD Effective Date: 08/01/08
 DEPARTMENT OF MEDICAL IMAGING POLICIES, PROCEDURES AND PROTOCOLS Subject: Policy: Communication of Critical and/or Discrepant Findings RR003 Author: Stephen Alden, Lorie Cavalli and Bobby Kalb, MD Effective
DEPARTMENT OF MEDICAL IMAGING POLICIES, PROCEDURES AND PROTOCOLS Subject: Policy: Communication of Critical and/or Discrepant Findings RR003 Author: Stephen Alden, Lorie Cavalli and Bobby Kalb, MD Effective
Will CT screening reduce overall lung cancer mortality? Associate Professor of Radiology Department of Medical Imaging UHN / MSH / WCH
 Will CT screening reduce overall lung cancer mortality? Heidi Roberts MD FRCP(C) Heidi Roberts, MD, FRCP(C) Associate Professor of Radiology Department of Medical Imaging UHN / MSH / WCH Screening - Requirements
Will CT screening reduce overall lung cancer mortality? Heidi Roberts MD FRCP(C) Heidi Roberts, MD, FRCP(C) Associate Professor of Radiology Department of Medical Imaging UHN / MSH / WCH Screening - Requirements
May-Lin Wilgus. A. Study Purpose and Rationale
 Utility of a Computer-Aided Diagnosis Program in the Evaluation of Solitary Pulmonary Nodules Detected on Computed Tomography Scans: A Prospective Observational Study May-Lin Wilgus A. Study Purpose and
Utility of a Computer-Aided Diagnosis Program in the Evaluation of Solitary Pulmonary Nodules Detected on Computed Tomography Scans: A Prospective Observational Study May-Lin Wilgus A. Study Purpose and
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
I9 COMPLETION INSTRUCTIONS
 The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
ANATOMIC PATHOLOGY Faculty Meeting, November 12, Communication of Critical Values: An Update
 ANATOMIC PATHOLOGY Faculty Meeting, November 12, 2007 Communication of Critical Values: An Update PROCEDURE TITLE: Communication of Critical Values UNIFIED DEPARTMENTAL POLICY NUMBER: PURPOSE: To implement
ANATOMIC PATHOLOGY Faculty Meeting, November 12, 2007 Communication of Critical Values: An Update PROCEDURE TITLE: Communication of Critical Values UNIFIED DEPARTMENTAL POLICY NUMBER: PURPOSE: To implement
Role of CT in Lung Cancer Screening: 2010 Stuart S. Sagel, M.D.
 Role of CT in Lung Cancer Screening: 2010 Stuart S. Sagel, M.D. Lung Cancer 219,440 new cases/year in U.S. (2009) 169,390 deaths/year in U.S. mortality greater than from breast, colon, prostate CA combined
Role of CT in Lung Cancer Screening: 2010 Stuart S. Sagel, M.D. Lung Cancer 219,440 new cases/year in U.S. (2009) 169,390 deaths/year in U.S. mortality greater than from breast, colon, prostate CA combined
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
None
 2014 None rosemary clooney Cancer is one of the most common diseases in the developed world: 1 in 4 deaths are due to cancer 1 in 17 deaths are due to lung cancer Lung cancer is the most common
2014 None rosemary clooney Cancer is one of the most common diseases in the developed world: 1 in 4 deaths are due to cancer 1 in 17 deaths are due to lung cancer Lung cancer is the most common
Lung Cancer and CT Screening
 Lung Cancer and CT Screening Samer Kanaan, MD February 17 th, 2012 Goals Understand the Societal impact of Lung Cancer Identify Risk Factors for Lung Cancer List Diagnostic Tests Available for Lung Cancer
Lung Cancer and CT Screening Samer Kanaan, MD February 17 th, 2012 Goals Understand the Societal impact of Lung Cancer Identify Risk Factors for Lung Cancer List Diagnostic Tests Available for Lung Cancer
SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art
 SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality
SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality
Guidelines for the Management of Pulmonary Nodules Detected by Low-dose CT Lung Cancer Screening
 Guidelines for the Management of Pulmonary Nodules Detected by Low-dose CT Lung Cancer Screening 1. Introduction In January 2005, the Committee for Preparation of Clinical Practice Guidelines for the Management
Guidelines for the Management of Pulmonary Nodules Detected by Low-dose CT Lung Cancer Screening 1. Introduction In January 2005, the Committee for Preparation of Clinical Practice Guidelines for the Management
Disclosures. Overview. Selection the most accurate statement: Updates in Lung Cancer Screening 5/26/17. No Financial Disclosures
 Updates in Lung Cancer Screening Disclosures No Financial Disclosures Neil Trivedi, MD Associate Professor of Clinical Medicine SF VAMC Pulmonary and Critical Care Director, Bronchoscopy & Interventional
Updates in Lung Cancer Screening Disclosures No Financial Disclosures Neil Trivedi, MD Associate Professor of Clinical Medicine SF VAMC Pulmonary and Critical Care Director, Bronchoscopy & Interventional
PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE?
 PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE? MICHAEL K. GOULD, MD SENIOR RESEARCH SCIENTIST DIRECTOR FOR HEALTH SCIENCES & IMPLEMENTATION SCIENCE
PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE? MICHAEL K. GOULD, MD SENIOR RESEARCH SCIENTIST DIRECTOR FOR HEALTH SCIENCES & IMPLEMENTATION SCIENCE
MANAGEMENT RECOMMENDATIONS
 1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
Lung. 10/24/13 Chest X-ray: 2.9 cm mass like density in the inferior lingular segment worrisome for neoplasm. Malignancy cannot be excluded.
 Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan
 What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan Small Lung Nodules What to do with small lung nodules? We biopsy them when requested What are our accuracy
What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan Small Lung Nodules What to do with small lung nodules? We biopsy them when requested What are our accuracy
Error, Injury & Loss in Medical Imaging. Matthew J Fleishman MD MMM FACR
 Error, Injury & Loss in Medical Imaging Matthew J Fleishman MD MMM FACR Disclosures: None Objectives 1. Magnitude of errors & $ losses 2. Basis for major errors 3. Strategies to mitigate error, injury
Error, Injury & Loss in Medical Imaging Matthew J Fleishman MD MMM FACR Disclosures: None Objectives 1. Magnitude of errors & $ losses 2. Basis for major errors 3. Strategies to mitigate error, injury
C2 COMPLETION INSTRUCTIONS
 The C2 Form is completed for each screening exam at T0, T1, and T2. The C2 Form is to be completed by each of the following ACRIN-NLST study staff: the research associate (study coordinator), CT technologist,
The C2 Form is completed for each screening exam at T0, T1, and T2. The C2 Form is to be completed by each of the following ACRIN-NLST study staff: the research associate (study coordinator), CT technologist,
Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer
 November 2010 Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer Laura Myers, Harvard Medical School, Year III Clinical Presentation 79yo woman with cough productive of green
November 2010 Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer Laura Myers, Harvard Medical School, Year III Clinical Presentation 79yo woman with cough productive of green
Example of lung screening
 Justification of the use of CT for individual health assessment of asymptomatic people How to obtain evidence for IHA - Example of lung screening Mathias Prokop, MD PhD Professor of Radiology Radboud University
Justification of the use of CT for individual health assessment of asymptomatic people How to obtain evidence for IHA - Example of lung screening Mathias Prokop, MD PhD Professor of Radiology Radboud University
CT Lung Screening Implementation Challenges: ALA/ATS Implementation Microsite
 CT Lung Screening Implementation Challenges: ALA/ATS Implementation Microsite Andrea McKee, MD Chair Radiation Oncology Lahey Hospital and Medical Center November 2018 2016 data, 3 years after ACS recommendation
CT Lung Screening Implementation Challenges: ALA/ATS Implementation Microsite Andrea McKee, MD Chair Radiation Oncology Lahey Hospital and Medical Center November 2018 2016 data, 3 years after ACS recommendation
Low-Dose CT: Clinical Studies & the Radiologist Perspective
 Low-Dose CT: Clinical Studies & the Radiologist Perspective RD-ASiR RD-MBIR SD-FBP RD=0.35 msv (80% dose reduction) Perry J. Pickhardt, MD UW School of Medicine & Public Health Low-Dose CT: Clinical Overview
Low-Dose CT: Clinical Studies & the Radiologist Perspective RD-ASiR RD-MBIR SD-FBP RD=0.35 msv (80% dose reduction) Perry J. Pickhardt, MD UW School of Medicine & Public Health Low-Dose CT: Clinical Overview
National Optimal Lung Cancer Pathway
 National Optimal Lung Cancer Pathway This document was produced by the Lung Clinical Expert Group 2017 Document Title: National Optimal Lung Cancer Pathway and Implementation Guide Date of issue: August
National Optimal Lung Cancer Pathway This document was produced by the Lung Clinical Expert Group 2017 Document Title: National Optimal Lung Cancer Pathway and Implementation Guide Date of issue: August
Lung Cancer Screening: Now What?
 Lung Cancer Screening: Now What? Gerold Bepler, M.D., Ph.D. Director, President & CEO Michigan Cancer Consortium, 2013 Annual Meeting, Lansing, MI, 11/20/13 Lung Cancer #1 Cause of Cancer Death for & *
Lung Cancer Screening: Now What? Gerold Bepler, M.D., Ph.D. Director, President & CEO Michigan Cancer Consortium, 2013 Annual Meeting, Lansing, MI, 11/20/13 Lung Cancer #1 Cause of Cancer Death for & *
DISCLOSURE. Lung Cancer Screening: The End of the Beginning. Learning Objectives. Relevant Financial Relationship(s) Off Label Usage
 Off Label Usage") Peninsula Regional Medical Center 12 th Annual Lung Cancer Conference March 9, 2017 Lung Cancer Screening: The End of the Beginning David E. Midthun M.D. Professor of Medicine College of Medicine, Mayo
Peninsula Regional Medical Center 12 th Annual Lung Cancer Conference March 9, 2017 Lung Cancer Screening: The End of the Beginning David E. Midthun M.D. Professor of Medicine College of Medicine, Mayo
LCA Lung Clinical Forum. 21 st October 2014
 LCA Lung Clinical Forum 21 st October 2014 Welcome Dr Liz Sawicka Chair - LCA Lung Pathway Group Succession planning Dr Kate Haire Consultant in Public Health Medicine, LCA Commissioning Intentions for
LCA Lung Clinical Forum 21 st October 2014 Welcome Dr Liz Sawicka Chair - LCA Lung Pathway Group Succession planning Dr Kate Haire Consultant in Public Health Medicine, LCA Commissioning Intentions for
Right infrahilar nodule
 Right infrahilar nodule Search Infrahilar nodule Nov 9, 2015.. CT chest showed a right infrahilar mass 3.5 2.5 cm along with multiple bilateral lung nodules of size 9 to 11 mm. Bronchoscopy. Jun 13, 2015.
Right infrahilar nodule Search Infrahilar nodule Nov 9, 2015.. CT chest showed a right infrahilar mass 3.5 2.5 cm along with multiple bilateral lung nodules of size 9 to 11 mm. Bronchoscopy. Jun 13, 2015.
Objectives. Why? Why? Background 11/5/ % incurable disease at presentation Locally advanced disease Metastasis. 14% 5 year survival
 Objectives Appraise lung cancer screening trials results Review screening guidelines Lung Cancer Screening: Past, Present and Future Chi Wan Koo, MD Koo.chiwan@mayo.edu Discuss recommendations essential
Objectives Appraise lung cancer screening trials results Review screening guidelines Lung Cancer Screening: Past, Present and Future Chi Wan Koo, MD Koo.chiwan@mayo.edu Discuss recommendations essential
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
Faster Cancer Treatment Indicators: Use cases
 Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
Ultralow Dose Chest CT with MBIR
 Ultralow Dose Chest CT with MBIR Ella A. Kazerooni, M.D. Professor & Director Cardiothoracic Radiology Associate Chair for Clinical Affairs University of Michigan Disclosures Consultant: GE Healthcare
Ultralow Dose Chest CT with MBIR Ella A. Kazerooni, M.D. Professor & Director Cardiothoracic Radiology Associate Chair for Clinical Affairs University of Michigan Disclosures Consultant: GE Healthcare
An Introduction to PET Imaging in Oncology
 January 2002 An Introduction to PET Imaging in Oncology Janet McLaren, Harvard Medical School Year III Basics of PET Principle of Physiologic Imaging: Allows in vivo visualization of structures by their
January 2002 An Introduction to PET Imaging in Oncology Janet McLaren, Harvard Medical School Year III Basics of PET Principle of Physiologic Imaging: Allows in vivo visualization of structures by their
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Liquid Biopsies. Next Generation Cancer Molecular Diagnostics
 Liquid Biopsies Next Generation Cancer Molecular Diagnostics Forward Looking Statements 2 Statements pertaining to future financial and/or operating results, future research, diagnostic tests and technology
Liquid Biopsies Next Generation Cancer Molecular Diagnostics Forward Looking Statements 2 Statements pertaining to future financial and/or operating results, future research, diagnostic tests and technology
The Role of PET / CT in Lung Cancer Staging
 July 2004 The Role of PET / CT in Lung Cancer Staging Vlad Vinarsky, Harvard Medical School Year IV Patient AM HPI: 81 yo F p/w hemoptysis x 1 month LLL lesion on CXR, not responsive to Abx 35 pack-year
July 2004 The Role of PET / CT in Lung Cancer Staging Vlad Vinarsky, Harvard Medical School Year IV Patient AM HPI: 81 yo F p/w hemoptysis x 1 month LLL lesion on CXR, not responsive to Abx 35 pack-year
CT Fluoroscopy-Guided vs Multislice CT Biopsy ModeGuided Lung Biopies:a preliminary experience
 CT Fluoroscopy-Guided vs Multislice CT Biopsy ModeGuided Lung Biopies:a preliminary experience Poster No.: C-0097 Congress: ECR 2016 Type: Scientific Exhibit Authors: A. Casarin, G. Rech, C. Cicero, A.
CT Fluoroscopy-Guided vs Multislice CT Biopsy ModeGuided Lung Biopies:a preliminary experience Poster No.: C-0097 Congress: ECR 2016 Type: Scientific Exhibit Authors: A. Casarin, G. Rech, C. Cicero, A.
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
DOH LUNG CANCER SCREENING SERVICE SPECIFICATIONS
 DOH LUNG CANCER SCREENING SERVICE SPECIFICATIONS December 2018 Page 1 of 18 Document Title: Document Ref. Number: DOH Lung Cancer Screening Service Specifications PH/NCD/LCSC/SR/0.9 Version: 0.9 Approval
DOH LUNG CANCER SCREENING SERVICE SPECIFICATIONS December 2018 Page 1 of 18 Document Title: Document Ref. Number: DOH Lung Cancer Screening Service Specifications PH/NCD/LCSC/SR/0.9 Version: 0.9 Approval
Screening Programs background and clinical implementation. Denise R. Aberle, MD Professor of Radiology and Engineering
 Screening Programs background and clinical implementation Denise R. Aberle, MD Professor of Radiology and Engineering disclosures I have no disclosures. I have no conflicts of interest relevant to this
Screening Programs background and clinical implementation Denise R. Aberle, MD Professor of Radiology and Engineering disclosures I have no disclosures. I have no conflicts of interest relevant to this
Lung Cancer Screening: Benefits and limitations to its Implementation
 Lung Cancer Screening: Benefits and limitations to its Implementation Rolando Sanchez, MD Clinical Assistant Professor Pulmonary-Critical Care Medicine University of Iowa Lung cancer - Epidemiology Cancer
Lung Cancer Screening: Benefits and limitations to its Implementation Rolando Sanchez, MD Clinical Assistant Professor Pulmonary-Critical Care Medicine University of Iowa Lung cancer - Epidemiology Cancer
I8 COMPLETION INSTRUCTIONS
 The I8 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I8 Form documents comparison review of the baseline screen (DR Form) with any historical images available. At T1
The I8 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I8 Form documents comparison review of the baseline screen (DR Form) with any historical images available. At T1
New Visions in PET: Surgical Decision Making and PET/CT
 New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
Goals of Presentation
 Goals of Presentation Review context of lung cancer screening why is it important? Review data from NLST supporting screening with lowdose CT (LDCT) scanning Discuss the pros and cons of LDCT screening
Goals of Presentation Review context of lung cancer screening why is it important? Review data from NLST supporting screening with lowdose CT (LDCT) scanning Discuss the pros and cons of LDCT screening
Guide to Understanding Lung Cancer
 Guide to Understanding Lung Cancer Lung cancer is the second most common cancer overall for men and women in the U.S., with an estimated 222,500 new cases in 2017. However, lung cancer is the most common
Guide to Understanding Lung Cancer Lung cancer is the second most common cancer overall for men and women in the U.S., with an estimated 222,500 new cases in 2017. However, lung cancer is the most common
Lung Cancer Screening. Ashish Maskey MD Interventional Pulmonology UK Health Care Dec 1 st 2017
 Lung Cancer Screening Ashish Maskey MD Interventional Pulmonology UK Health Care Dec 1 st 2017 Nearly one in six American adults currently smoke cigarettes An estimated 40 million adults in the United
Lung Cancer Screening Ashish Maskey MD Interventional Pulmonology UK Health Care Dec 1 st 2017 Nearly one in six American adults currently smoke cigarettes An estimated 40 million adults in the United
Quality Assurance Program
 Quality Assurance Program Argus Radiology is proud to be a Joint Commission Accredited Teleradiology Company. OUR QUALITY MISSION Our internal and external Quality Assurance programs ensure your patients
Quality Assurance Program Argus Radiology is proud to be a Joint Commission Accredited Teleradiology Company. OUR QUALITY MISSION Our internal and external Quality Assurance programs ensure your patients
A Chronology of Advancements in the Diagnosing of Lung Nodules
 November 17, 2017 A Chronology of Advancements in the Diagnosing of Lung Nodules Presenter: Daniel P. Harley, MD, MSB, FACS Surgical Director of the Angelos Center for Lung Diseases 1 Pulmonary Nodules
November 17, 2017 A Chronology of Advancements in the Diagnosing of Lung Nodules Presenter: Daniel P. Harley, MD, MSB, FACS Surgical Director of the Angelos Center for Lung Diseases 1 Pulmonary Nodules