Rotating-shield brachytherapy (RSBT) for cervical cancer
|
|
|
- Milo Bailey
- 6 years ago
- Views:
Transcription

 thesis, University of Iowa, 2012. http://ir.uiowa.")
1 University of Iowa Iowa Research Online Theses and Dissertations Summer 2012 Rotating-shield brachytherapy (RSBT) for cervical cancer Wenjun Yang University of Iowa Copyright 2012 Wenjun Yang This thesis is available at Iowa Research Online: Recommended Citation Yang, Wenjun. "Rotating-shield brachytherapy (RSBT) for cervical cancer." MS (Master of Science) thesis, University of Iowa, Follow this and additional works at: Part of the Biomedical Engineering and Bioengineering Commons
2 ROTATING-SHIELD BRACHYTHERAPY (RSBT) FOR CERVICAL CANCER by Wenjun Yang A thesis submitted in partial fulfillment of the requirements for the Master of Science degree in Biomedical Engineering in the Graduate College of The University of Iowa July 2012 Thesis Supervisor: Assistant Professor Ryan T. Flynn
3 Copyright by WENJUN YANG 2012 All Rights Reserved
4 Graduate College The University of Iowa Iowa City, Iowa CERTIFICATE OF APPROVAL MASTER S THESIS This is to certify that the Master s thesis of Wenjun Yang has been approved by the Examining Committee for the thesis requirement for the Master of Science degree in Biomedical Engineering at the July 2012 graduation. Thesis Committee: Ryan T. Flynn, Thesis Supervisor Joseph M. Reinhardt John E. Bayouth Yusung Kim
5 ACKNOWLEDGEMENTS I would like to give my sincere thanks to all who help me to finish this thesis: To Ryan Flynn for his direction, patience and the great support throughout my master study. To Yusung Kim for his generous help on the clinical knowledge and suggestions on my manuscript. To Xiaodong Wu for his instructions on the algorithms to lead our research to go deeper. To Yunlong Liu and Xing Li, for their cooperation and making the study a happy time. To my parents, for their great encouragement no matter I m scoring 100 or 0. To my fiancee, Yan Zhang, for letting me know what s really important. ii
6 ABSTRACT Purpose: To assess rotating shield brachytherapy (RSBT) delivered with electronic brachytherapy (ebt) sources compared to intracavitary (IC) and intracavitary plus supplemental interstitial brachytherapy (IC+IS BT) delivered with a conventional 192 Ir source. Method and Materials: An in-house treatment planning system (TPS) for RSBT was developed, and IC, IC+IS and RSBT treatment plans were simulated for 5 patients with bulky (>40cc) advanced cervical cancer high-risk target volumes (HR-CTVs). All treatment planning was based on magnetic resonance (MR) images with HR-CTV, bladder, rectum, and sigmoid colon contouring done by a radiation oncologist. A bio- and MRI-compatible polycarbonate (Makrolon Rx3158) intrauterine applicator was simulated for IC and RSBT, and the Vienna applicator was simulated for IC+IS BT. 192 Ir was used as the radiation source of IC and IC+IS BT, and the Xoft Axxent TM ebt source was used for RSBT. A 0.5 mm thick tungsten shield was used for RSBT. Two shield models, with azimuthal 45, zenith 180 (RSBT-45) and azimuthal 180, zenith 180 (RSBT-180) was selected in this study. BT planning was done by escalating: maximizing HR-CTV dose without exceeding bladder, rectum, and sigmoid dose tolerances. The total dose for each plan included both the external beam radiation therapy (EBRT) and BT doses. Results: The minimal dose of the hottest 90% of HR-CTV volume (D90) and treatment time was selected as the metric of plan evaluation. RSBT and IC+IS BT had higher D90 than IC BT for all 5 patients. For RSBT-180/IC+IS, the D90 ratio ranged from 66% to 100%, with average of 86%; the treatment time ratio ranged from 137% to 208%, with average of 169%. For RSBT-45/IC+IS, the D90 ratio ranged from 101% to iii
7 123%, with the average of 113%; the treatment time ratio ranged from 749% to 1188%, with the average of 907%. Conclusions: RSBT for advanced cervical cancer can provide variant D90 and treatment time with different azimuthal angles. For RSBT-45, the D90 was improved at the cost of increased treatment time. For RSBT-180, the treatment time was strictly controlled but D90 was not guaranteed. There will be an angle to achieve the balance of D90 and treatment time. iv
8 TABLE OF CONTENTS LIST OF TABLES... VI LIST OF FIGURES... VII CHAPTER 1 INTRODUCTION Cervical cancer Standard of care for cervical cancer Brachytherapy Rotating-shield brachytherapy Rationale of our study...4 CHAPTER 2 MATERIALS AND METHODS Treatment planning system (TPS) of RSBT Patients and dose prescriptions Radiation Source and applicator Delivery technique Dose calculation Optimization methods Evaluation metric...17 CHAPTER 3 RESULTS D90 and treatment time statistics DVH curve Dose distribution map Effect of azimuthal angle Effect of zenith angle...22 CHAPTER 4 DISCUNSSION AND CONCLUSION...23 REFERENCES...25 v
9 LIST OF TABLES Table 1-1. Local control and survival rate by stage...2 Table 2-1. The terminologies defined in RS-IMBT...13 Table 2-2. Variables of modified-tg-43 dose calculation equation...15 Table 2-3. Main variables defined in the optimization equation...17 vi
10 LIST OF FIGURES Figure 1-1. Vienna applicator for IC+IS and IC BT...3 Figure 1-2. BrachyVision, the BT planning system used at UIHC...5 Figure 2-1. Flow chart of the in-house TPS for RSBT...6 Figure 2-2. Geometry of MRI image slice and patient position...7 Figure 2-3. Physician delineated contour for the bladder of patient Figure 2-4. MRI image and reconstructed 3D structure for HR-CTV and OAR...8 Figure 2-5. Geometry design of the RSBT shield...10 Figure 2-6. Shield open area with different azimuth and zenith angles...11 Figure 2-7. RSBT coordinate system for dose calculation and shield rotating&moving Figure 2-8. RSBT source with shield rotating and shifting process Figure 3-1. D90 and treatment time comparison between RSBT and IC+IS BT...18 Figure 3-2. DVH of 5 patients with RSBT-180, RSBT-45, IC and IC+IS BT...19 Figure 3-3. Dose distribution map for 5 patients with IC, IC+IS, RSBT-180 and RSBT Figure 3-4. RSBT parameter selection curve...21 vii
11 1 CHAPTER 1 INTRODUCTION 1.1 Cervical cancer Cervical cancer is a malignant neoplasm of the cervix uteri or cervical area. It is the leading cause of cancer mortality in women in developing countries and third most common gynecological cancer in the US [1]. One of the most common symptoms of cervical cancer is abnormal vaginal bleeding, but there may be no symptoms in the early stages [2, 3]. More than 90% of cervical cancer is caused by Human papillomavirus (HPV) infection [3, 4]. Not all of the causes of cervical cancer are known, and several other contributing factors include smoking [5] chlamydia infection, stress and stress-related disorders, dietary factors, hormonal contraception, multiple pregnancies, exposure to the hormonal drug diethylstilbestrol, and family history of cervical cancer [6]. In 2011, more then 12,000 newly diagnosed cervical cancer cases were reported in the U.S., with the death rate of about 33.8% [7]. The death rate is related to the cancer stage, which is shown in Table 1. Cervical cancer cases of stage IB2 to stage IV were studied in this work since these advanced-staged cancer cases tend to receive brachytherapy and have bulky volume (>40cc) to benefit from our treatment method.
12 2 Table 1-1 [1]. Local control and survival rate by stage Local control rate 5 years survival IA % IA % IB % IB % IB % IB % IIA 80-85% IIA 75% IIB 60-80% IIB 60-65% IIIA 60% IIIA 25-50% IIIB 50-60% IIIB 25-50% IVA 30% IVA 15-30% IVB <10% 1.2 Standard of care for cervical cancer Early stages (IB1 and IIA less than 4 cm) can be treated with radical hysterectomy with removal of the lymph nodes or radiation therapy. Radiation therapy is given as external beam radiotherapy to the pelvis and brachytherapy (internal radiation). Patients treated with surgery who have high risk features found on pathologic examination are given radiation therapy with or without chemotherapy in order to reduce the risk of relapse [1]. Larger early stage tumors (IB2 and IIA more than 4 cm) may be treated with radiation therapy and cisplatin-based chemotherapy, hysterectomy (which then usually requires adjuvant radiation therapy), or cisplatin chemotherapy followed by hysterectomy [1]. Advanced stage tumors (IIB-IVA) are treated with radiation therapy and cisplatinbased chemotherapy [1].
![3 1.3 Brachytherapy Brachytherapy (BT) plays a crucial role in the treatment of invasive cervical cancer from stage I to IV, especially in advanced stage (IB2 or higher) [8, 9].](/docs-images/74/70313906/images/13-0.jpg "It is an intracavitary (IC) high-dose-rate (HDR) radiation therapy, delivering much higher dose per fraction than external beam radiotherapy (EBRT) to the target tumor volume without violating the")
![organs at risk (OAR) toxicity threshold because of the very high dose gradient around the source (about 10% per mm) [9].](/docs-images/74/70313906/images/13-1.jpg "Conventionally, a radiation source with a radially symmetric dose distribution is used in brachytherapy.")
13 3 1.3 Brachytherapy Brachytherapy (BT) plays a crucial role in the treatment of invasive cervical cancer from stage I to IV, especially in advanced stage (IB2 or higher) [8, 9]. It is an intracavitary (IC) high-dose-rate (HDR) radiation therapy, delivering much higher dose per fraction than external beam radiotherapy (EBRT) to the target tumor volume without violating the organs at risk (OAR) toxicity threshold because of the very high dose gradient around the source (about 10% per mm) [9]. Conventionally, a radiation source with a radially symmetric dose distribution is used in brachytherapy. As a result, the OAR around the cervical cancer, such as bladder, sigmoid and rectum restrict the radiation dose that can be delivered to the non-symmetric extensions of bulky (>4 cm) tumors [10]. To compensate for the sometimes poor conformance of the intracavitaryonly dose distribution, needle-based intracavitary plus interstitial (IC+IS) BT is can be used [8-14]. Figure 1-1 is one example of the applicator used in IC and IC+IS BT. Figure 1-1. Vienna applicator for IC+IS and IC BT. (a) Vienna applicator with ring and needle [11], (b) Stockholm based intracavitary applicator [15]
14 4 1.4 Rotating-shield brachytherapy Rotating shield brachytherapy (RSBT) was conceptually proposed by Ebert in 2002 [16]. It delivered the dose through a partially shielded radiation source in an optimized step-shot fashion to improve tumor dose conformity. It s a type of intensitymodulated brachytherapy (IMBT) in which the amount of time the shield is pointed in a given direction is controlled. RSBT may be less invasive than interstitial BT since there is no need of needles, and the extra time for setting up interstitial applicator is spared. With the electronic radiation source which is with relatively low energy (26 kev on average), RSBT enables clinical staff to be in the treatment room during delivery, and would eliminate the need for an expensive shielded room for conventional BT. Thus patients could be treated in a room next to the MRI or CT room, reducing the added complexity of transporting patients between the BT suite and the imaging room. Other groups have studied the theoretical effectiveness of RSBT for prostate [17] and breast [18] cancer. 1.5 Rationale of our study In this work, we proposed to apply RSBT with electronic source for cervical cancer with bulky (>40cc) volume. With the relatively low source energy (average 26ev), we could use 2mm-thick tungsten shield which can be placed into the IC BT applicator. We also developed a treatment planning system for RSBT to compare the treatment result with conventional IC and IC+IS BT. Commercially available HDR-BT planning systems of which we are aware are capable of IC+IS BT. Figure 1-2 is the user interface of BrachyVision, the BT planning system used at the University of Iowa Hospitals and Clinics (UIHC). From this planning
 for cervical cancer.")
15 5 system, we can check different slices of the patient MRI image, high-risk clinical target volume (HR-CTV) of cervical cancer, OAR and applicator position, and different dose coverage. This system is for conventional IC or IC+IS only. In this work we developed an in-house RSBT treatment planning system (TPS) for cervical cancer. The TPS generates RSBT optimized dose distributions based on patient image data exported from BrachyVision, and is capable of dose and dose-volume histogram (DVH) display for treatment plan evaluation. Figure 1-2. BrachyVision, the BT planning system used at UIHC
16 6 CHAPTER 2 MATERIALS AND METHODS 2.1 Treatment planning system (TPS) of RSBT The flow chart of our in-house TPS is shown in figure 2-1. The TPS was developed in the Matlab programming environment. For the first step in the treatment planning process, an image reading tool was developed to read in the patient MR image and the contour data of HR-CTV and OAR from DICOM files exported from BrachyVision. Since the MRI image was acquired with a rotation angle, α, along the X axis, a simple image transform (rotation and translation) is necessary to align the image slice with the physical MRI slice, as shown in figure 2-2. Figure 2-1. Flow chart of the in-house TPS for RSBT

 (b) Figure 2-3.")
17 7 Figure 2-2. Geometry of MRI image slice and patient position The image rotation matrix of α is stored in the header of the DICOM file, and the image registration is achieved by multiplying the image coordinates by the inverse rotation matrix. The figure 2-3 shows the bladder contour before and after registration. (a) (b) Figure 2-3. Physician delineated contour for the bladder of patient 1. (a) The bladder contour before registration, (b) The bladder contour after registration
 (b) Figure 2-4. MRI image and reconstructed 3D structure for HR-CTV and OAR.")

18 8 The images after registration were used to construct the 3D grid for dose calculation. As shown in figure 2-4, the binary masks for HR-CTV and OAR were constructed. And then the space relationship can be founded between the applicator and the volumes. (a) (b) Figure 2-4. MRI image and reconstructed 3D structure for HR-CTV and OAR. (a) Transverse MRI of cervical cancer and adjacent organs, (b) Reconstructed 3D binary masks of tumor and OARs The cervical cancer cases, materials, and the dose optimization and calculation mechanism will be discussed in the following sections. 2.2 Patients and dose prescriptions Five patients with biopsy-confirmed cervical cancer (treated from 2009 to 2010) having large high risk CTV (HR-CTV) were selected based on the tumor volume (>40cc) and shape. Large HR-CTV cases were selected because we found that even the MRIguided, conformal HDR-BT technique was limited to provide proper dose-hr-ctv conformity. And so such cases need IC+IS BT to provide better dose-tumor coverage,
19 9 which will benefit from RSBT [8]. The cancer International Federation of Gynecology and Obstetrics (FIGO) stage ranged from IB to IVA, with lymph node and parametrial involvement and maximum dimension greater than 4 cm. Curative radiation therapy (RT) was performed, consisting of external beam RT with concomitant chemotherapy followed by HDR-BT (5.5 Gy per fraction with 5 fractions). To cover parametrial regions, an EBRT boost (5.4 Gy with 1.8 Gy fraction size) was performed. High-resolution (3.0 Tesla) MR images were acquired with a Siemens MAGNETOM Trio 3T MR scanner (Siemens Medical Solutions, Erlangen, Germany). HR-CTV and OAR that clinically delineated (using GEC-ESTRO guidelines [8]) on T2-weighted MRI were retrospectively imported into the in-house TPS. Clinically reconstructed source-pathway information of a tandem was imported into an applicator-source-pathway. The detail of MRI scanning protocol and scanning method, such as Brachytherapy Eye View was reported in our previous study. One BT plan was assumed to be repeated during subsequent BT fractions. The MRI images were acquired from the first fraction. The linear-quadratic parameters used were: α/β = 3 Gy for OAR and α/β = 10 Gy for tumor [19]. The final dose result was the summation of EBRT and dose/fraction multiplied by fraction number in BT. We used the OAR dose constraints of D2cc 75 Gy 3 for rectum and sigmoid, D2cc 90 Gy 3 for bladder, which is consistent with that used by other groups [9, 20]. 2.2 Radiation Source and applicator For RSBT, we simulated the same applicator as that in intracavitary BT as shown in figure 1-1. We proposed an electronic radiation source, Xoft Axxent TM for RSBT, since with the relatively low energy (26.8 kev), only 0.5 mm thick tungsten shield is
![10 needed to reduce the transmission to less than 0.1%. According to Ebert s study [16], the more transmission, the poorer dose conformity can be achieved.](/docs-images/74/70313906/images/20-0.jpg "In our study, we assumed the shield was rotated along the curved axis of the applicator. There are two other reason why we selected the Xoft Axxent TM (Xoft Inc.")
20 10 needed to reduce the transmission to less than 0.1%. According to Ebert s study [16], the more transmission, the poorer dose conformity can be achieved. In our study, we assumed the shield was rotated along the curved axis of the applicator. There are two other reason why we selected the Xoft Axxent TM (Xoft Inc., Sunnyvale, CA) miniature x-ray (photon) tube as the radiation source for RSBT. First, its dose rate in water at 2 cm lateral to the source axis is greater than 1 Gy/min, which is comparable to that of 192 Ir BT, preventing a significant treatment time increase for RS- IMBT. Second, the transmission of the low energy (26.8 kev average) photons emitted by the ebt source can be reduced to 0.1% with only 0.5mm of tungsten shield. Over 2 cm of gold or tungsten would be required to achieve a similar shield transmission for 192 Ir photons, which is too much to fit inside an intracavitary uterine applicator. (a) (b) Figure 2-5. Geometry design of the RSBT shield. (a) Front view, with the azimuthal angle defined window width (b) Side view, with the zenith angle defined window height. Radiation source is placed at the center of the shield, and the azimuth and zenith angle define the window size. The line-shape radiation source is simulated as a point

21 11 As shown in figure 2-5, a 0.5 mm thick shield made of tungsten was applied around the radiation source to modify the intensity. With different shield azimuth and zenith angle, the dose shape could be modified. In conventional BT with 192 Ir, no shield was used. The dose distribution is illustrated as figure 2-6. The source was simulated as a point source and the shield open area is modulated by the azimuthal and zenith angle. In the following sections, all the dose distribution will be illustrated as pyramid shape. In this work, we assumed shield photon transmission was zero. It is ignorable at the tumor edge, which is the key parameter of the emission time optimization. (a) (b) Figure 2-6. Shield open area with different azimuth and zenith angles. (a) azimuth angle = 45, zenith angle = 45, (b) azimuth angle = 90, zenith angle = 120
22 Delivery technique Figure 2-7. RSBT coordinate system for dose calculation and shield rotating&moving. The ebt source is placed in the applicator positions sequentially. The dashed pyramid indicates the azimuthal and zenith shield emission angles. Every point in the space is defined in two coordinate systems: the laboratory and source coordinate system. The shield is rotated along z' k. The dwell time of each position is optimized using a linear least square optimization technique. After a full rotation at one dwell position, the source moves to the next one and the process is repeated. As shown in figure 2-7, the radiation source was simulated to be placed at the dwell positions sequentially within the applicator. At each dwell position, the radiation source was rotated around z' k. The number of emission per dwell position can be specified by the user. The emission time was optimized with a linear least square optimizer such that the dose distribution would conform to the tumor shape. The source moved to the next dwell position and repeated this process after a 360 rotation.
23 13 Table 2-1. The terminologies defined in RS-IMBT Dwell position Emission n N j Δγ γ j Δφ Δθ The stop positions of the radiation source within the applicator Dose delivery at each dwell position. The number of emissions at each dwell position as shield rotating is set by user The number of dwell positions in one RS-IMBT treatment The number of emissions at each dwell position The index of emissions. If there are 16 emissions at each dwell position, each emission is indexed with j = 0 15 The emission step angle, which is the angle the shield travelled between emission j and j+1. Δγ = 2π/N The angle between the current shield central line and that of emission j = 0. γ j = jδγ, where j = 0 N-1 The shield azimuthal angle, as shown in figure 2-5 (a). min(δφ) = Δγ, such that there isn t any cold point not covered between each emission. The shield zenith angle, as shown in figure 2-5 (b). The number of dwell position, n is determined by Δθ, such that there isn t any cold position between each dwell position. In this study, we specified n = 8 and N = 16. With 8 dwell positions, the distance between each one is about 5 mm, which is a typical value in clinical situations. The number of 16 emissions provided a fine enough intensity-modify resolution. We used different shield azimuth angle, Δφ, from 45 to 180 in out study. Since N = 16, π /8 is the minimal value allowed (min(δφ) = Δγ = 360 /N). In this case as shown in figure 2-8 (a), it s a non-overlapping rotation: at emission j = 4 and j = 5, the shield covered and only just covered that area, with no overlapping. While with larger Δφ (Δφ > Δγ) as shown in figure 2-8 (b), there is an overlapping between each emission, such as j = 4 and j = 5. We also used different shield zenith angle, Δθ, from 90 to 180. Figure 2-8 (c) and 2-8 (d) shows the relationship between the dwell position distance and Δθ.
24 14 (a) (b) (c) (d) Figure 2-8. RSBT source with shield rotating and shifting process (a) the shield azimuth angle is equal to the rotation step angle, so that there isn t overlap between each rotation, (b) The shield azimuth angle is greater than the rotation step angle, which brings overlap between each rotation, (c) The minimal zenith angle is shown such that there won t be any cold points outside the applicator, (d) The zenith angle is larger so there will be overlap between dwell positions. Two azimuthal angle shields (45 and 180 ) with constant zenith angle (180 ) were applied to all the 5 patients. They are called RSBT-45 and RSBT-180. These two angles were selected to represent fine and broad azimuthal shield angles, and are not expected to be optimal choices. More shield model with different azimuthal and zenith angle was applied only to patient 1, to investigate the effect of azimuthal and zenith angle.
25 Dose calculation The TG-43 method was used for dose calculation, and the medium through which the photons transmitted was assumed to be water. D j,k ( r, Δφs, Δθ s ) = S k Λ G k ( r ) ( r0 ) g r s k G k ( ) F k r Equation1 Modified-TG-43 equation for dose calculation ( ) Tj,k ( r, Δφs, Δθ s ) The definition of each function in equation 1 and the corresponding approximated functions are shown in table 2. Table 2-2. Variables of modified-tg-43 dose calculation equation D j,k r, Δφs, Δθ s ( ) S k Dose rate of any point of jth dwell position and kth emission in the laboratory coordinate system. It depends on the position r, the azimuth angle Δφ s, and the zenith angle Δθ s of the shield. Air strength kerma constant, in unit of cgy*cm 2 /hr Λ Dose rate constant, in unit of cm 2 G k r ( ) Geometry function of mass density and the distance from the radiation source. In this study the medium intensity is assumed to be 1g/ cm 3 and G k ( r ) is assumed to be G k ( r ) = 1 r 2. T j,k g( r s k ) Radial dose function, theoretically it s g(r) = e µr, we used the TG- F k r r, Δφs, Δθ s 43 formalism in this paper ( ) Anisotropy function, which accounts for the anisotropy dose distribution caused by the applicator ( ) 1, if r is inside the shield open area, 0, if shielded
26 Optimization methods With the prescription dose specified by user, which in this study is 27.5 Gy, a least-squares optimization method was used to determine the emission times at each emission of all the dwell positions. The emission times were then uniformly scaled as high as possible such that none of the rectum, bladder, or sigmoid GEC-ESTRO recommended D 2cc values was exceeded. The objective and update function is shown in Equation 2 and 3. K Ew ( ) = [ β kc(0, ) ( di d i, k) + βk C(,0) ( di d i, k) + T k= 1 k i Tk β C ( d d ) + β C ( d d ) V+ 2 V+ V 2 V k V+ V (0, D ) i k k Δ (0, ΔD ) i k Equation 2[21]. Optimization objective function k k w ( t+ 1) j = w 1 K + + V+ V+ V V β k Dd ij i, k + β k Dd ij i, k + β kdk Dij + β kdk Dij k 1 V V t = T + + k i Ii i Ii i Ii i Ii j K 1 + V+ V β k Dd ij i + β k Dd ij i + β k Dd ij i + β k Dd ij i k = 1 T + V+ V k i Ii i Ii i Ii i Ii Equation 3[21]. Optimization update equation
27 17 Table 2-3. Main variables defined in the optimization equation w K T k β d i d + i,k The weights of each beamlet, to be optimized, with dimension of N(dwell position)*n(emission), unit of hour The number of organs considered in the optimizer The number of voxels of the kth organ The penalty factor for different situations The prescription dose on tumor surface The dose greater than prescription in the ith voxel, kth organ d i,k The dose less than prescription in the ith voxel, kth organ d V + k The overdose threshold for dose-volume parameter d V k The underdose threshold for dose-volume parameter D ij The dose delivered to the ith voxel, by source at jth emission 2.6 Evaluation metric With the MRI-guided TPS, the tumor volume uncertainty was reduced[20, 22] thus a higher structure related parameter, the minimal dose value for the hottest 90% tumor volume (D90), was used to evaluate the treatment quality for HR-CTV, without violation of recommendations of GEC ESTRO. The minimal dose of the hottest 2cc of OAR (D2cc) is the constraint of the OAR. The treatment time for IC, IC+IS and RSBT was calculated in our TPS to check if the increased treatment time of RSBT was clinically acceptable.


28 18 CHAPTER 3 RESULTS 3.1 D90 and treatment time statistics The comparison of D90 and treatment time of different BT methods for 5 patients are shown in figure 3-1. For RSBT-180/IC+IS, the D90 ratio ranged from 0.66 to 1.00, with average of 0.86; the treatment time ratio ranged from 1.37 to 2.08, with average of For RSBT-45/IC+IS, the D90 ratio ranged from 1.01 to 1.23, with the average of 1.13; the treatment time ratio ranged from 7.49 to 11.88, with the average of Figure 3-1. D90 and treatment time comparison between RSBT and IC+IS BT 3.2 DVH curve The DVH for all the 5 patients are shown in figure 3-2.


29 19 Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Figure 3-2. DVH of 5 patients with RSBT-180, RSBT-45, IC and IC+IS BT 3.3 Dose distribution map The dose distribution map for the 5 patients are shown in figure 3-3.





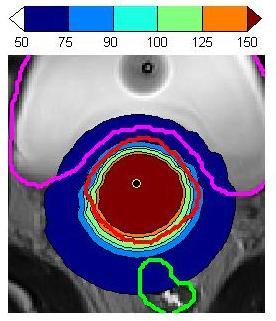


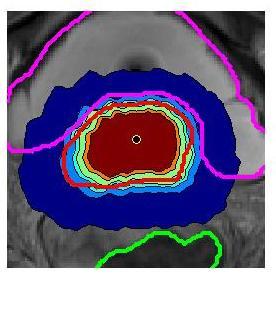

30 20 IC IC+IS RSBT 180⁰ RSBT 45⁰ Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Figure 3-3. Dose distribution map for 5 patients with IC, IC+IS, RSBT-180 and RSBT-45
31 Effect of azimuthal angle We applied a series shield with different azimuthal angle for patient 1 RSBT treatment. The treatment time is basically inverse linearly dependent on the azimuthal angle. There is one optimal azimuthal angle to achieve the best D90. The time-d90 curve is shown in figure 3-4. Figure 3-4. RSBT parameter selection curve. One spot represents one experiment with different azimuthal angle. Green spots represent applicable angles, and red ones represent inapplicable angles As shown in figure 3-4, each spot means an experiment with different azimuthal but fixed zenith angle. The treatment time and D90 of different azimuthal angle consists
32 22 an outer boarder called purrito curve. The RSBT azimuthal angle should be selected right on this curve since other angle to the left of the curve means longer treatment time yet worse D90. It also can be seen that physicians could select the proper azimuthal angle based on this curve if the treatment time or D90 is with priority. 3.5 Effect of zenith angle For patient 1, we applied different zenith angles RSBT with the constant azimuthal angle. But because of the irregular open area shape of the shield, there appeared cold area when the zenith angle is <120. So there was not large feasible range for zenith angle and the effect of zenith angle is not clear.
33 23 CHAPTER 4 DISCUNSSION AND CONCLUSION The treatment outcome, in terms of D90, of RS-BT is always better than intracavitary BT, which is shown in the DVH curves. The advantage of RSBT over interstitial BT is highly dependent on the tumor shape and azimuthal angle selected. We can group patient 1 and 2 together since the D90 of RSBT with 180 azimuthal angle is at least similar to that of interstitial BT. The RSBT in these two cases will provide less invasiveness and cost acceptable extra treatment time which is less than 5 min/fraction. For patients 3,4, and 5, the RSBT-180 is less effective than IC+IS since it lowers the D90 below that of interstitial BT. We can see from figure 3-1 that the 45 RSBT will always get the best treatment outcome, the highest D90 but the extra treatment time will be very large in terms of more than 30 min/fraction. So, for some cervical cancer shapes, RSBT with 180 azimuthal angle is a good alternative for interstitial BT, such as patient 1 and 2. However, for other irregular shapes, RSBT with finer angle such as 45 could be considered but much more treatment time is required. The dose calculation model in our study is an approximation. We are currently using a point source model, without considering the shield transmission (<0.1%) and photon scattering. It is reasonable to assume that the dosimetric results of our study are upper bounds of the treatment outcomes of RSBT, since all these neglected factors will only cause irregular dose distribution thus decrease the D90 result. Another problem is the escalated dose result is one BT fraction 5. In real clinical treatment, the tumor and OAR locations and size change with time, especially for
34 24 HR-CTV. An MRI scan is thus required just prior to RSBT delivery in order to ensure organ structures of the proper sizes and extends are used for planning. In our simulation study, the result shows RSBT could provide higher D90 than conventional IC+IS BT. More experimental work will be needed in the future to verify our computational results. Moreover, our results show that the parameter selection for RSBT is very important for different tumor shapes. An algorithm that automatically searches the best set of parameters will be helpful for making the treatment plan. (3 out of 5 is better with 45, not 60% of all patients) (tg43 method is not specific for shield)
35 25 REFERENCES 1. R. Scott Bermudez, K.H., and I-Chow Hsu, Cervical Cancer, in Handbook of Evidence-based Radiation p Canavan, T.P. and N.R. Doshi, Cervical cancer. American family physician, (5): p Kumar, V.A., Abul K.; Fausto, Nelson; & Mitchell, Richard N, ed. Robbins Basic Pathology (8th ed.). 2007, Saunders Elsevier Walboomers, J.M., et al., Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. The Journal of pathology, (1): p Gadducci, A., et al., Smoking habit, immune suppression, oral contraceptive use, and hormone replacement therapy use and cervical carcinogenesis: a review of the literature. Gynecological endocrinology : the official journal of the International Society of Gynecological Endocrinology, (8): p Society, A.C., ed. What Causes Cancer of the Cervix? Siegel, R., et al., Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA: a cancer journal for clinicians, (4): p Haie-Meder, C., et al., Recommendations from Gynaecological (GYN) GEC- ESTRO Working Group (I): concepts and terms in 3D image based 3D treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology, (3): p Potter, R., et al., Recommendations from gynaecological (GYN) GEC ESTRO working group (II): concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy-3d dose volume parameters and aspects of 3D image-based anatomy, radiation physics, radiobiology. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology, (1): p Shah, A.P., et al., Toxicity associated with bowel or bladder puncture during gynecologic interstitial brachytherapy. International journal of radiation oncology, biology, physics, (1): p Dimopoulos, J.C., et al., The Vienna applicator for combined intracavitary and interstitial brachytherapy of cervical cancer: clinical feasibility and preliminary results. International journal of radiation oncology, biology, physics, (1): p Kirisits, C., et al., The Vienna applicator for combined intracavitary and interstitial brachytherapy of cervical cancer: design, application, treatment planning, and dosimetric results. International journal of radiation oncology, biology, physics, (2): p
36 Syed, A.M., et al., Long-term results of low-dose-rate interstitial-intracavitary brachytherapy in the treatment of carcinoma of the cervix. International journal of radiation oncology, biology, physics, (1): p Lin, L., et al., The use of directional interstitial sources to improve dosimetry in breast brachytherapy. Medical Physics, (1): p Alain Gerbaulet, R.P.t., Christine Haie-Meder, Cervix Carcinoma, in The GEC- ESTRO handbook of brachytherapy, R.P.t. Alain Gerbaulet, Jean-Jacques Mazeron, Harm Meertens, Erik Van Limbergen, Editor p Ebert, M.A., Possibilities for intensity-modulated brachytherapy: technical limitations on the use of non-isotropic sources. PHYSICS IN MEDICINE AND BIOLOGY, (14): p Prada, P.J., et al., High-dose-rate intensity modulated brachytherapy with external-beam radiotherapy improves local and biochemical control in patients with high-risk prostate cancer. Clinical & translational oncology : official publication of the Federation of Spanish Oncology Societies and of the National Cancer Institute of Mexico, (7): p Shi, C., et al., Three dimensional intensity modulated brachytherapy (IMBT): dosimetry algorithm and inverse treatment planning. Medical Physics, (7): p Fowler, J.F., The linear-quadratic formula and progress in fractionated radiotherapy. The British journal of radiology, (740): p Tanderup, K., et al., From point A to the sculpted pear: MR image guidance significantly improves tumour dose and sparing of organs at risk in brachytherapy of cervical cancer. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology, (2): p Flynn, R., A Comparison Of Intensity Modulated X-Ray Therapy To Intensity Modulated proton Therapy For the Delivery Of Non-Uniform Dose Distributions, in Medical physics2007, University of Wisconsin. p Hamilton, C.S. and M.A. Ebert, Volumetric uncertainty in radiotherapy. Clinical Oncology, (6): p
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer
 for Gynaecological Cancer") Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER
 SAUDI JOURNAL OF OBSTETRICS AND GYNECOLOGY VOLUME 11 NO. 2 1430 H - 2009 G 3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER DR YASIR BAHADUR 1, DR CAMELIA CONSTANTINESCU 2,
SAUDI JOURNAL OF OBSTETRICS AND GYNECOLOGY VOLUME 11 NO. 2 1430 H - 2009 G 3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER DR YASIR BAHADUR 1, DR CAMELIA CONSTANTINESCU 2,
MR-Guided Brachytherapy
 MR-Guided Brachytherapy Joann I. Prisciandaro, Ph.D. The Department of Radiation Oncology University of Michigan Outline Traditional 2D technique for brachytherapy treatment planning Transition to MR-guided
MR-Guided Brachytherapy Joann I. Prisciandaro, Ph.D. The Department of Radiation Oncology University of Michigan Outline Traditional 2D technique for brachytherapy treatment planning Transition to MR-guided
The New ICRU/GEC ESTRO Report in Clinical Practice. Disclosures
 The New ICRU/GEC ESTRO Report in Clinical Practice Christian Kirisits, MSc, PhD; Richard Pötter, MD Medical University of Vienna, Vienna, Austria On behalf of the Committee: B. Erickson, C. Haie Meder,
The New ICRU/GEC ESTRO Report in Clinical Practice Christian Kirisits, MSc, PhD; Richard Pötter, MD Medical University of Vienna, Vienna, Austria On behalf of the Committee: B. Erickson, C. Haie Meder,
INTRODUCTION PATIENT. J. Radiat. Res., 52, (2011)
") J. Radiat. Res., 52, 54 58 (2011) Regular Paper Intracavitary Combined with CT-guided Interstitial Brachytherapy for Locally Advanced Uterine Cervical Cancer: Introduction of the Technique and a Case Presentation
J. Radiat. Res., 52, 54 58 (2011) Regular Paper Intracavitary Combined with CT-guided Interstitial Brachytherapy for Locally Advanced Uterine Cervical Cancer: Introduction of the Technique and a Case Presentation
High resolution (3 Tesla) MRI-guided conformal brachytherapy for cervical cancer: consequences of different high-risk CTV sizes
 MRI-guided conformal brachytherapy for cervical cancer: consequences of different high-risk CTV sizes") Original paper High resolution (3 Tesla) MRI-guided conformal brachytherapy for cervical cancer: consequences of different high-risk CTV sizes Physics Contributions James W. Anderson, PhD 1, Junyi Xia,
Original paper High resolution (3 Tesla) MRI-guided conformal brachytherapy for cervical cancer: consequences of different high-risk CTV sizes Physics Contributions James W. Anderson, PhD 1, Junyi Xia,
Linking DVH-parameters to clinical outcome. Richard Pötter, Medical University of Vienna, General Hospital of Vienna, Austria
 Linking DVH-parameters to clinical outcome Richard Pötter, Medical University of Vienna, General Hospital of Vienna, Austria Outline DVH parameters for HR CTV (D90) and OAR (2 ccm) simple integration of
Linking DVH-parameters to clinical outcome Richard Pötter, Medical University of Vienna, General Hospital of Vienna, Austria Outline DVH parameters for HR CTV (D90) and OAR (2 ccm) simple integration of
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring)
") Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Course Directors: Teaching Staff: Guest Lecturers: Local Organiser: ESTRO coordinator: Melissa Vanderijst, project manager (BE)
") ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2017 Course Directors: Richard
ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2017 Course Directors: Richard
Comparison of rectal and bladder ICRU point doses to the GEC ESTRO volumetric doses in Cervix cancer
 Comparison of rectal and bladder ICRU point doses to the GEC ESTRO volumetric doses in Cervix cancer Poster No.: RO-0049 Congress: RANZCR FRO 202 Type: Authors: Scientific Exhibit G. Govindarajulu, A.
Comparison of rectal and bladder ICRU point doses to the GEC ESTRO volumetric doses in Cervix cancer Poster No.: RO-0049 Congress: RANZCR FRO 202 Type: Authors: Scientific Exhibit G. Govindarajulu, A.
Course Directors: Teaching Staff: Guest Lecturers: Local Organiser: ESTRO coordinator: Melissa Vanderijst, project manager (BE)
") ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2016 Course Directors: Richard
ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2016 Course Directors: Richard
GYN GEC-ESTRO/ICRU 89 Target Concept. Richard Pötter Medical University Vienna
 GYN GEC-ESTRO/ICRU 89 Target Concept Richard Pötter Medical University Vienna GYN GEC ESTRO RECOMMENDATIONS-BACKGROUND From 2D to 3D/4D Historical difficulties in communicating results of cervical BT due
GYN GEC-ESTRO/ICRU 89 Target Concept Richard Pötter Medical University Vienna GYN GEC ESTRO RECOMMENDATIONS-BACKGROUND From 2D to 3D/4D Historical difficulties in communicating results of cervical BT due
Compensator-based intensity modulated brachytherapy for cervical cancer
 Compensator-based intensity modulated brachytherapy for cervical cancer Xing Li Department of Physics and Astronomy, University of Iowa, 203 Van Allen Hall, 52242 Abstract We introduce compensator-based
Compensator-based intensity modulated brachytherapy for cervical cancer Xing Li Department of Physics and Astronomy, University of Iowa, 203 Van Allen Hall, 52242 Abstract We introduce compensator-based
Intracavitary + Interstitial Techniques Rationale
 Vienna, 14. 15. May, 2018 Intracavitary + Interstitial Techniques Rationale Primoz Petric NCCCR, HMC, Doha Dimensions of prescribed dose: different levels Prescribed dose Standard loading Modified loading
Vienna, 14. 15. May, 2018 Intracavitary + Interstitial Techniques Rationale Primoz Petric NCCCR, HMC, Doha Dimensions of prescribed dose: different levels Prescribed dose Standard loading Modified loading
Course Directors : Teaching Staff : Guest Lecturer: Local Organiser: ESTRO coordinators: Melissa Vanderijst and Marta Jayes, project managers (BEL)
") ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Florence, Italy 28 September -2 October 2014 Course Directors
ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Florence, Italy 28 September -2 October 2014 Course Directors
MRI Guided GYN Brachytherapy: Clinical Considerations
 MRI Guided GYN Brachytherapy: Clinical Considerations AAPM Junzo Chino MD Duke Radiation Oncology 8/8/2013 Disclosures none Learning Objectives Historical Context: Film based Brachytherapy Advantages of
MRI Guided GYN Brachytherapy: Clinical Considerations AAPM Junzo Chino MD Duke Radiation Oncology 8/8/2013 Disclosures none Learning Objectives Historical Context: Film based Brachytherapy Advantages of
Recent Advances and current status of radiotherapy for cervix cancer
 Recent Advances and current status of radiotherapy for cervix cancer Richard Pötter MD Department of Radiation Oncology, Medical University of Vienna, Austria ICARO-2, IAEA, Vienna, June, 24, 2017 Recent
Recent Advances and current status of radiotherapy for cervix cancer Richard Pötter MD Department of Radiation Oncology, Medical University of Vienna, Austria ICARO-2, IAEA, Vienna, June, 24, 2017 Recent
Preliminary reports. Primoz Petric, MD, MSc, Robert Hudej, PhD, Maja Music, MD. Abstract. Introduction
 Original article Preliminary reports pre-planning, based on insertion of the applicator in para-cervical anaesthesia: preliminary results of a prospective study Primoz Petric, MD, MSc, Robert Hudej, PhD,
Original article Preliminary reports pre-planning, based on insertion of the applicator in para-cervical anaesthesia: preliminary results of a prospective study Primoz Petric, MD, MSc, Robert Hudej, PhD,
Dose-Volume Histogram Analysis in Point A-based Dose Prescription of High-dose-rate Brachytherapy for Cervical Carcinoma
 Showa Univ J Med Sci 30 2, 227 235, June 2018 Original Dose-Volume Histogram Analysis in Point A-based Dose Prescription of High-dose-rate Brachytherapy for Cervical Carcinoma Rei KOBAYASHI 1, Yoshikazu
Showa Univ J Med Sci 30 2, 227 235, June 2018 Original Dose-Volume Histogram Analysis in Point A-based Dose Prescription of High-dose-rate Brachytherapy for Cervical Carcinoma Rei KOBAYASHI 1, Yoshikazu
Image guided brachytherapy in cervical cancer Clinical Aspects
 Image guided brachytherapy in cervical cancer Clinical Aspects Richard Pötter MD Department of Radiation Oncology, Medical University of Vienna, Austria ICARO-2, IAEA, Vienna, June, 22, 2017 Outline Tumor
Image guided brachytherapy in cervical cancer Clinical Aspects Richard Pötter MD Department of Radiation Oncology, Medical University of Vienna, Austria ICARO-2, IAEA, Vienna, June, 22, 2017 Outline Tumor
High dose-rate tandem and ovoid brachytherapy in cervical cancer: dosimetric predictors of adverse events
 Romano et al. Radiation Oncology (2018) 13:129 https://doi.org/10.1186/s13014-018-1074-2 RESEARCH Open Access High dose-rate tandem and ovoid brachytherapy in cervical cancer: dosimetric predictors of
Romano et al. Radiation Oncology (2018) 13:129 https://doi.org/10.1186/s13014-018-1074-2 RESEARCH Open Access High dose-rate tandem and ovoid brachytherapy in cervical cancer: dosimetric predictors of
CT Guided Contouring: Challenges and Pitfalls
 CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
Local Organiser: Madhup Rastogi, Radiation Oncologist, Ram Manohar Lohia Institute of Medical Sciences, Lucknow
 2 nd ESTRO-AROI GYN Teaching Course 3D Radiotherapy with a Special Emphasis on Implementation of MRI / CT Based Brachytherapy in Cervical Cancer 8-11 March 2018 Lucknow, India AROI Course Directors: Umesh,
2 nd ESTRO-AROI GYN Teaching Course 3D Radiotherapy with a Special Emphasis on Implementation of MRI / CT Based Brachytherapy in Cervical Cancer 8-11 March 2018 Lucknow, India AROI Course Directors: Umesh,
CT Guided Contouring: Challenges and Pitfalls
 CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
Version A European study on MRI-guided brachytherapy in locally advanced cervical cancer EMBRACE (ENDORSED BY GEC ESTRO)
") A European study on MRI-guided brachytherapy in locally advanced cervical cancer EMBRACE (ENDORSED BY GEC ESTRO) 1 Contents: 1. ABBREVIATIONS... 4 2. SUMMARY... 5 3. INTRODUCTION AND PRINCIPLES OF IMAGE
A European study on MRI-guided brachytherapy in locally advanced cervical cancer EMBRACE (ENDORSED BY GEC ESTRO) 1 Contents: 1. ABBREVIATIONS... 4 2. SUMMARY... 5 3. INTRODUCTION AND PRINCIPLES OF IMAGE
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
EMBRACE- Studien Analysen und Perspektiven
 EMBRACE- Studien Analysen und Perspektiven Alina Sturdza EMBRACE study group Outline Historical development of GEC ESTRO Gyn Group Historical development of the MRI compatible applicators Presentation
EMBRACE- Studien Analysen und Perspektiven Alina Sturdza EMBRACE study group Outline Historical development of GEC ESTRO Gyn Group Historical development of the MRI compatible applicators Presentation
Image based Brachytherapy- HDR applications in Gynecological Tumors
 Image based Brachytherapy- HDR applications in Gynecological Tumors Yakov Pipman, D. Sc. North Shore LIJ Health System Sites amenable to treatment with HDR Brachytherapy GYN Breast Prostate Head and Neck
Image based Brachytherapy- HDR applications in Gynecological Tumors Yakov Pipman, D. Sc. North Shore LIJ Health System Sites amenable to treatment with HDR Brachytherapy GYN Breast Prostate Head and Neck
Advances in Image-guided Brachytherapy
 Advances in Image-guided Brachytherapy Hospital Authority Convention 2016 Terry Wong, Physicist Department of Medical Physics Pamela Youde Nethersole Eastern Hospital Introduction What is Brachytherapy?
Advances in Image-guided Brachytherapy Hospital Authority Convention 2016 Terry Wong, Physicist Department of Medical Physics Pamela Youde Nethersole Eastern Hospital Introduction What is Brachytherapy?
Basics of Cervix Brachytherapy. William Small, Jr., MD Professor and Chairman Loyola University Chicago
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Brachytherapy William Small, Jr., MD Professor and Chairman Loyola University Chicago Cervix Cancer Education Symposium, January
Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Brachytherapy William Small, Jr., MD Professor and Chairman Loyola University Chicago Cervix Cancer Education Symposium, January
REVISITING ICRU VOLUME DEFINITIONS. Eduardo Rosenblatt Vienna, Austria
 REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
Specialised Services Clinical Access Policy: Enhanced Image Guided Brachytherapy (IGBT) Service for the Treatment of Gynaecological Malignancies
 Service for the Treatment of Gynaecological Malignancies") Specialised Services Clinical Access Policy: Enhanced Image Guided Brachytherapy (IGBT) Service for the Treatment of Gynaecological Malignancies Document Author: Assistant Director Evidence Evaluation
Specialised Services Clinical Access Policy: Enhanced Image Guided Brachytherapy (IGBT) Service for the Treatment of Gynaecological Malignancies Document Author: Assistant Director Evidence Evaluation
Challenging Cases in Cervical Cancer: Parametrial Boosting. Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin
 Challenging Cases in Cervical Cancer: Parametrial Boosting Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin Disclosure Chart Rounds participant No COI Learning Objectives Discuss the challenges
Challenging Cases in Cervical Cancer: Parametrial Boosting Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin Disclosure Chart Rounds participant No COI Learning Objectives Discuss the challenges
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer?
 Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas Dept. of Medical Physics & Engineering, Strahlenklinik, Klinikum Offenbach GmbH 63069 Offenbach, Germany
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas Dept. of Medical Physics & Engineering, Strahlenklinik, Klinikum Offenbach GmbH 63069 Offenbach, Germany
Definitions. Brachytherapy in treatment of cancer. Implantation Techniques and Methods of Dose Specifications. Importance of Brachytherapy in GYN
 Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Knowledge-Based IMRT Treatment Planning for Prostate Cancer: Experience with 101. Cases from Duke Clinic. Deon Martina Dick
 Knowledge-Based IMRT Treatment Planning for Prostate Cancer: Experience with 101 Cases from Duke Clinic by Deon Martina Dick Department of Medical Physics Duke University Date: Approved: Joseph Lo, Chair
Knowledge-Based IMRT Treatment Planning for Prostate Cancer: Experience with 101 Cases from Duke Clinic by Deon Martina Dick Department of Medical Physics Duke University Date: Approved: Joseph Lo, Chair
 https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
Brachytherapy in Africa
 Brachytherapy in Africa Deanine Halliman PhD Sr. Director Medical Affairs Elekta Brachytherapy Burden of cervical cancer in Africa est. 2012 incidence per 100,000 women Bouassa M, et al. Cervical cancer
Brachytherapy in Africa Deanine Halliman PhD Sr. Director Medical Affairs Elekta Brachytherapy Burden of cervical cancer in Africa est. 2012 incidence per 100,000 women Bouassa M, et al. Cervical cancer
BASIC CLINICAL RADIOBIOLOGY
 INT6062: Strengthening Capacity for Cervical Cancer Control through Improvement of Diagnosis and Treatment BASIC CLINICAL RADIOBIOLOGY Alfredo Polo MD, PhD Applied Radiation Biology and Radiotherapy Section
INT6062: Strengthening Capacity for Cervical Cancer Control through Improvement of Diagnosis and Treatment BASIC CLINICAL RADIOBIOLOGY Alfredo Polo MD, PhD Applied Radiation Biology and Radiotherapy Section
IMRT - the physician s eye-view. Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia
 IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
Comprehensive and Practical Brachytherapy March 04-8 March 2018, Ljubljana, Slovenia Day 1 Sunday 4 March 2018
 Day 1 Sunday 4 March 2018 Welcome and Summary of the course 13:00-13:20 15 introduction 13:20-13:50 30 Radioactivity Radioactivity: What we need to know Characteristics of LDR-PDR-HDR, radiobiological
Day 1 Sunday 4 March 2018 Welcome and Summary of the course 13:00-13:20 15 introduction 13:20-13:50 30 Radioactivity Radioactivity: What we need to know Characteristics of LDR-PDR-HDR, radiobiological
presenting Brachytherapy with focus on Gynecological Cancers
 Good Afternoon I am Bulent Aydogan and I will be presenting Brachytherapy with focus on Gynecological Cancers 1 I have nothing to disclose 2 3 4 Now IstheQuiztime time 5 6 7 Brachtheray has a long history
Good Afternoon I am Bulent Aydogan and I will be presenting Brachytherapy with focus on Gynecological Cancers 1 I have nothing to disclose 2 3 4 Now IstheQuiztime time 5 6 7 Brachtheray has a long history
Dosimetric comparison of interstitial brachytherapy with multi-channel vaginal cylinder plans in patients with vaginal tumors
 Mendez et al. Radiation Oncology (2017) 12:84 DOI 10.1186/s13014-017-0821-0 RESEARCH Open Access Dosimetric comparison of interstitial brachytherapy with multi-channel vaginal cylinder plans in patients
Mendez et al. Radiation Oncology (2017) 12:84 DOI 10.1186/s13014-017-0821-0 RESEARCH Open Access Dosimetric comparison of interstitial brachytherapy with multi-channel vaginal cylinder plans in patients
The Evolution of RT Techniques for Gynaecological Cancers in a developing country context
 The Evolution of RT Techniques for Gynaecological Cancers in a developing country context Hannah Simonds Stellenbosch University/ Tygerberg Academic Hospital ESMO Africa 2017 I have no disclosures External
The Evolution of RT Techniques for Gynaecological Cancers in a developing country context Hannah Simonds Stellenbosch University/ Tygerberg Academic Hospital ESMO Africa 2017 I have no disclosures External
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments
 Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer
 A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005 Advantages of inflatable multichannel endorectal applicator in the neo-adjuvant treatment of patients with locally advanced
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005 Advantages of inflatable multichannel endorectal applicator in the neo-adjuvant treatment of patients with locally advanced
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer?
 Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas 1,3, Natasa Milickovic 1, Nikolaos Zamboglou 2 1 Dept. of Medical Physics & Engineering, 2 Strahlenklinik,
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas 1,3, Natasa Milickovic 1, Nikolaos Zamboglou 2 1 Dept. of Medical Physics & Engineering, 2 Strahlenklinik,
Healthcare Professional Guide
 Healthcare Professional Guide Brachytherapy: The precise answer for tackling gynecological cancers Because life is for living Radiotherapy: a cornerstone of gynecological cancer care Gynecological cancers
Healthcare Professional Guide Brachytherapy: The precise answer for tackling gynecological cancers Because life is for living Radiotherapy: a cornerstone of gynecological cancer care Gynecological cancers
Vagina. 1. Introduction. 1.1 General Information and Aetiology
 Vagina 1. Introduction 1.1 General Information and Aetiology The vagina is part of internal female reproductive system. It is an elastic, muscular tube that connects the outside of the body to the cervix.
Vagina 1. Introduction 1.1 General Information and Aetiology The vagina is part of internal female reproductive system. It is an elastic, muscular tube that connects the outside of the body to the cervix.
From position verification and correction to adaptive RT Adaptive RT and dose accumulation
 From position verification and correction to adaptive RT Adaptive RT and dose accumulation Hans de Boer Move away from Single pre-treatment scan Single treatment plan Treatment corrections by couch shifts
From position verification and correction to adaptive RT Adaptive RT and dose accumulation Hans de Boer Move away from Single pre-treatment scan Single treatment plan Treatment corrections by couch shifts
Original Date: June 2013 Page 1 of 7 Radiation Oncology Last Review Date: September Implementation Date: December 2014 Clinical Operations
 National Imaging Associates, Inc. Clinical guideline CERVICAL CANCER Original Date: June 2013 Page 1 of 7 Radiation Oncology Last Review Date: September 2014 Guideline Number: NIA_CG_223 Last Revised Date:
National Imaging Associates, Inc. Clinical guideline CERVICAL CANCER Original Date: June 2013 Page 1 of 7 Radiation Oncology Last Review Date: September 2014 Guideline Number: NIA_CG_223 Last Revised Date:
Utrecht Interstitial Applicator Shifts and DVH Parameter Changes in 3D CT-based HDR Brachytherapy of Cervical Cancer
 DOI:http://dx.doi.org/10.7314/APJCP.2015.16.9.3945 RESEARCH ARTICLE Utrecht Interstitial Applicator Shifts and DVH Parameter Changes in 3D CT-based HDR Brachytherapy of Cervical Cancer Dan Shi &, Ming-Yuan
DOI:http://dx.doi.org/10.7314/APJCP.2015.16.9.3945 RESEARCH ARTICLE Utrecht Interstitial Applicator Shifts and DVH Parameter Changes in 3D CT-based HDR Brachytherapy of Cervical Cancer Dan Shi &, Ming-Yuan
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
Defining Target Volumes and Organs at Risk: a common language
 Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
ART for Cervical Cancer: Dosimetry and Technical Aspects
 ART for Cervical Cancer: Dosimetry and Technical Aspects D.A. Jaffray, Ph.D. Radiation Therapy Physics Princess Margaret Cancer Centre/Techna/Ontario Cancer Institute Professor Departments of Radiation
ART for Cervical Cancer: Dosimetry and Technical Aspects D.A. Jaffray, Ph.D. Radiation Therapy Physics Princess Margaret Cancer Centre/Techna/Ontario Cancer Institute Professor Departments of Radiation
Modern Interstitial GYN Brachytherapy. Conflicts: 8/3/2016. Modern Interstitial GYN Brachytherapy. 1. Use of MR
 Advances and Innovations in Image-Guided Brachytherapy Modern Interstitial GYN Brachytherapy Antonio Damato, PhD Brigham and Women s Hospital Conflicts: Travel grant from Elekta Consulting agreement with
Advances and Innovations in Image-Guided Brachytherapy Modern Interstitial GYN Brachytherapy Antonio Damato, PhD Brigham and Women s Hospital Conflicts: Travel grant from Elekta Consulting agreement with
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Corporate Medical Policy
 Corporate Medical Policy Intensity Modulated Radiation Therapy (IMRT) of Abdomen and File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_abdomen_and_pelvis
Corporate Medical Policy Intensity Modulated Radiation Therapy (IMRT) of Abdomen and File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_abdomen_and_pelvis
Outline - MRI - CT - US. - Combinations of imaging modalities for treatment planning
 Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Changing Paradigms in Radiotherapy
 Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
Developments in Directional Brachytherapy William Y. Song, PhD, DABR
 Developments in Directional Brachytherapy William Y. Song, PhD, DABR Medical Physicist Dept. Radiation Oncology Massey Cancer Center Director CAMPEP Graduate Program Virginia Commonwealth University Associate
Developments in Directional Brachytherapy William Y. Song, PhD, DABR Medical Physicist Dept. Radiation Oncology Massey Cancer Center Director CAMPEP Graduate Program Virginia Commonwealth University Associate
Johannes C. Athanasios Dimopoulos
 BrachyNext Symposium Miami Beach, USA, May 30 31, 2014 Imaging Modalities: Current Challenges and Future Directions Johannes C. Athanasios Dimopoulos Imaging Modalities: Current Challenges and Future Directions
BrachyNext Symposium Miami Beach, USA, May 30 31, 2014 Imaging Modalities: Current Challenges and Future Directions Johannes C. Athanasios Dimopoulos Imaging Modalities: Current Challenges and Future Directions
Medical Dosimetry Graduate Certificate Program IU Graduate School & The Department of Radiation Oncology IU Simon Cancer Center
 Medical Dosimetry Graduate Certificate Program IU Graduate School & The Department of Radiation Oncology IU Simon Cancer Center All students accepted into the Medical Dosimetry Graduate Certificate Program
Medical Dosimetry Graduate Certificate Program IU Graduate School & The Department of Radiation Oncology IU Simon Cancer Center All students accepted into the Medical Dosimetry Graduate Certificate Program
Clinical implementation of multisequence MRIbased adaptive intracavitary brachytherapy for cervix cancer
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 Clinical implementation of multisequence MRIbased adaptive intracavitary brachytherapy for cervix cancer Jacqueline
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 Clinical implementation of multisequence MRIbased adaptive intracavitary brachytherapy for cervix cancer Jacqueline
Radiation Damage Comparison between Intensity Modulated Radiotherapy (IMRT) and Field-in-field (FIF) Technique In Breast Cancer Treatments
 and Field-in-field (FIF) Technique In Breast Cancer Treatments") Radiation Damage Comparison between Intensity Modulated Radiotherapy () and Field-in-field (FIF) Technique In Breast Cancer Treatments Huisi Ai 1 and Hualin Zhang 2 1. Department of Radiation Oncology,
Radiation Damage Comparison between Intensity Modulated Radiotherapy () and Field-in-field (FIF) Technique In Breast Cancer Treatments Huisi Ai 1 and Hualin Zhang 2 1. Department of Radiation Oncology,
MRI in Cervix and Endometrial Cancer
 28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
Evaluation of Normal Tissue Complication Probability and Risk of Second Primary Cancer in Prostate Radiotherapy
 Evaluation of Normal Tissue Complication Probability and Risk of Second Primary Cancer in Prostate Radiotherapy Rungdham Takam Thesis submitted for the degree of Doctor of Philosophy in The School of Chemistry
Evaluation of Normal Tissue Complication Probability and Risk of Second Primary Cancer in Prostate Radiotherapy Rungdham Takam Thesis submitted for the degree of Doctor of Philosophy in The School of Chemistry
Advances in Gynecologic Brachytherapy
 Advances in Gynecologic Brachytherapy Anuj V Peddada, M.D. Director Department of Radiation Oncology Penrose Cancer Center Colorado Springs, CO USA Brachytherapy Issues in Gyn/onc Cervix Endometrial Rational
Advances in Gynecologic Brachytherapy Anuj V Peddada, M.D. Director Department of Radiation Oncology Penrose Cancer Center Colorado Springs, CO USA Brachytherapy Issues in Gyn/onc Cervix Endometrial Rational
ESTRO-CARO Teaching Course on Image-guided cervix radiotherapy - With a special focus on adaptive brachytherapy Hilton Hotel Toronto Toronto, Canada
 ESTRO-CARO Teaching Course on Image-guided cervix radiotherapy - With a special focus on adaptive brachytherapy Hilton Hotel Toronto Toronto, Canada 4 April - 6 April 2016 Course Directors: Richard Pötter,
ESTRO-CARO Teaching Course on Image-guided cervix radiotherapy - With a special focus on adaptive brachytherapy Hilton Hotel Toronto Toronto, Canada 4 April - 6 April 2016 Course Directors: Richard Pötter,
Recent proceedings in Brachytherapy Physics
 Recent proceedings in Brachytherapy Physics Frank-André Siebert UKSH, Campus Kiel, Germany Clinic of Radiotherapy Dept. Medical Physics Physical characteristics of brachytherapy (Courtesy Luc Beaulieu,
Recent proceedings in Brachytherapy Physics Frank-André Siebert UKSH, Campus Kiel, Germany Clinic of Radiotherapy Dept. Medical Physics Physical characteristics of brachytherapy (Courtesy Luc Beaulieu,
Accuracy Requirements and Uncertainty Considerations in Radiation Therapy
 Departments of Oncology and Medical Biophysics Accuracy Requirements and Uncertainty Considerations in Radiation Therapy Introduction and Overview 6 August 2013 Jacob (Jake) Van Dyk Conformality 18 16
Departments of Oncology and Medical Biophysics Accuracy Requirements and Uncertainty Considerations in Radiation Therapy Introduction and Overview 6 August 2013 Jacob (Jake) Van Dyk Conformality 18 16
Cervical cancer is a disease in which malignant (cancer) cells form in the tissues of the cervix.
 cells form in the tissues of the cervix.") Cervical Cancer Cervical cancer is a disease in which malignant (cancer) cells form in the tissues of the cervix. The cervix is the lower, narrow end of the uterus (the hollow, pear-shaped organ where
Cervical Cancer Cervical cancer is a disease in which malignant (cancer) cells form in the tissues of the cervix. The cervix is the lower, narrow end of the uterus (the hollow, pear-shaped organ where
Chapters from Clinical Oncology
 Chapters from Clinical Oncology Lecture notes University of Szeged Faculty of Medicine Department of Oncotherapy 2012. 1 RADIOTHERAPY Technical aspects Dr. Elemér Szil Introduction There are three possibilities
Chapters from Clinical Oncology Lecture notes University of Szeged Faculty of Medicine Department of Oncotherapy 2012. 1 RADIOTHERAPY Technical aspects Dr. Elemér Szil Introduction There are three possibilities
Index. T1 and T2-weighted images, 189
 Index A Aarhus University Hospital, Denmark applicator selection and BT application clinical assessment, 187 188 insertion, US guidance, 188 metastatic para-aortic node cases, 187 contouring protocol,
Index A Aarhus University Hospital, Denmark applicator selection and BT application clinical assessment, 187 188 insertion, US guidance, 188 metastatic para-aortic node cases, 187 contouring protocol,
Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors
 for locally advanced pancreatic tumors") Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors Anna Bruynzeel, Radiation Oncologist VU University Medical Center, Amsterdam, The Netherlands Current standard
Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors Anna Bruynzeel, Radiation Oncologist VU University Medical Center, Amsterdam, The Netherlands Current standard
Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w
 Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w Quality assurance Classical implant systems w Manchester
Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w Quality assurance Classical implant systems w Manchester
Corporate Medical Policy
 Corporate Medical Policy Intensity-Modulated Radiation Therapy (IMRT) of the Prostate File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_the_prostate
Corporate Medical Policy Intensity-Modulated Radiation Therapy (IMRT) of the Prostate File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_the_prostate
Interstitial Brachytherapy. Low dose rate brachytherapy. Brachytherapy alone cures some cervical cancer. Learning Objectives
 Interstitial Learning Objectives To discuss practical aspects of selection and insertion techniques for interstitial brachytherapy and their relation to clinical trials Akila Viswanathan, MD MPH Johns
Interstitial Learning Objectives To discuss practical aspects of selection and insertion techniques for interstitial brachytherapy and their relation to clinical trials Akila Viswanathan, MD MPH Johns
Efficient SIB-IMRT planning of head & neck patients with Pinnacle 3 -DMPO
 Investigations and research Efficient SIB-IMRT planning of head & neck patients with Pinnacle 3 -DMPO M. Kunze-Busch P. van Kollenburg Department of Radiation Oncology, Radboud University Nijmegen Medical
Investigations and research Efficient SIB-IMRT planning of head & neck patients with Pinnacle 3 -DMPO M. Kunze-Busch P. van Kollenburg Department of Radiation Oncology, Radboud University Nijmegen Medical
NIH Public Access Author Manuscript Int J Radiat Oncol Biol Phys. Author manuscript; available in PMC 2015 July 01.
 NIH Public Access Author Manuscript Published in final edited form as: Int J Radiat Oncol Biol Phys. 2014 July 1; 89(3): 674 681. doi:10.1016/j.ijrobp.2014.03.005. Dosimetric Consequences of Interobserver
NIH Public Access Author Manuscript Published in final edited form as: Int J Radiat Oncol Biol Phys. 2014 July 1; 89(3): 674 681. doi:10.1016/j.ijrobp.2014.03.005. Dosimetric Consequences of Interobserver
Brachytherapy Planning and Quality Assurance
 Brachytherapy Planning and Quality Assurance Classical implant systems Most common clinical applications and modern dosimetry methods Quality assurance Classical implant systems Manchester (Paterson-Parker)
Brachytherapy Planning and Quality Assurance Classical implant systems Most common clinical applications and modern dosimetry methods Quality assurance Classical implant systems Manchester (Paterson-Parker)
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป
 ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy
 Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
Therapeutic Medical Physics. Stephen J. Amadon Jr., Ph.D., DABR
 Therapeutic Medical Physics Stephen J. Amadon Jr., Ph.D., DABR Outline 1. Why physicists are needed in medicine 2. Branches of medical physics 3. Physics in Radiation Oncology 4. Treatment types and Treatment
Therapeutic Medical Physics Stephen J. Amadon Jr., Ph.D., DABR Outline 1. Why physicists are needed in medicine 2. Branches of medical physics 3. Physics in Radiation Oncology 4. Treatment types and Treatment
Venezia Advanced Gynecological Applicator Reaching beyond
 Venezia Advanced Gynecological Applicator Reaching beyond Advanced Gynecological Applicator Venezia is FDA cleared and CE marked, but is not available in all markets. 1 Helping clinicians improve patients
Venezia Advanced Gynecological Applicator Reaching beyond Advanced Gynecological Applicator Venezia is FDA cleared and CE marked, but is not available in all markets. 1 Helping clinicians improve patients
Pulsed Dose Rate for GYN Brachytherapy
 Pulsed Dose Rate for GYN Brachytherapy Firas Mourtada,, Ph.D. Department of Radiation Physics Dose equivalency to LDR Brief Introduction Radiobiology Dose Distribution: Radial dose function Source anisotropy
Pulsed Dose Rate for GYN Brachytherapy Firas Mourtada,, Ph.D. Department of Radiation Physics Dose equivalency to LDR Brief Introduction Radiobiology Dose Distribution: Radial dose function Source anisotropy
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
Outline. Contour quality control. Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT)
") Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT) James Kavanaugh, MS DABR Department of Radiation Oncology Division of Medical Physics Outline Importance
Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT) James Kavanaugh, MS DABR Department of Radiation Oncology Division of Medical Physics Outline Importance
Optimization methods for high dose rate brachytherapy treatment planning. Elodie R. Mok Tsze Chung
 Optimization methods for high dose rate brachytherapy treatment planning by Elodie R. Mok Tsze Chung A thesis submitted in conformity with the requirements for the degree of Master of Applied Science Graduate
Optimization methods for high dose rate brachytherapy treatment planning by Elodie R. Mok Tsze Chung A thesis submitted in conformity with the requirements for the degree of Master of Applied Science Graduate
BLADDER RADIOTHERAPY PLANNING DOCUMENT
 A 2X2 FACTORIAL RANDOMISED PHASE III STUDY COMPARING STANDARD VERSUS REDUCED VOLUME RADIOTHERAPY WITH AND WITHOUT SYNCHRONOUS CHEMOTHERAPY IN MUSCLE INVASIVE BLADDER CANCER (ISRCTN 68324339) BLADDER RADIOTHERAPY
A 2X2 FACTORIAL RANDOMISED PHASE III STUDY COMPARING STANDARD VERSUS REDUCED VOLUME RADIOTHERAPY WITH AND WITHOUT SYNCHRONOUS CHEMOTHERAPY IN MUSCLE INVASIVE BLADDER CANCER (ISRCTN 68324339) BLADDER RADIOTHERAPY
ARROCase: Locally Advanced Endometrial Cancer
 ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
MRI Based treatment planning for with focus on prostate cancer. Xinglei Shen, MD Department of Radiation Oncology KUMC
 MRI Based treatment planning for with focus on prostate cancer Xinglei Shen, MD Department of Radiation Oncology KUMC Overview How magnetic resonance imaging works (very simple version) Indications for
MRI Based treatment planning for with focus on prostate cancer Xinglei Shen, MD Department of Radiation Oncology KUMC Overview How magnetic resonance imaging works (very simple version) Indications for
The Role of Radiation in the Management of Gynecologic Cancers. Scott Glaser, MD
 The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD Nothing to disclose DISCLOSURE Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical
The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD Nothing to disclose DISCLOSURE Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Staging and Treatment Update for Gynecologic Malignancies
 Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER
 ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER Bro. Dr. Collie Miller IARC/WHO Based on trends in the incidence of cancer, the International Agency for Research on Cancer (IARC) and WHO
ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER Bro. Dr. Collie Miller IARC/WHO Based on trends in the incidence of cancer, the International Agency for Research on Cancer (IARC) and WHO
Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI)
 for Craniospinal Irradiation (CSI)") Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI) Tagreed AL-ALAWI Medical Physicist King Abdullah Medical City- Jeddah Aim 1. Simplify and standardize
Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI) Tagreed AL-ALAWI Medical Physicist King Abdullah Medical City- Jeddah Aim 1. Simplify and standardize
NEWER RADIATION (3 D -CRT, IMRT, IGRT) TECHNIQUES FOR CERVICAL CANCERS (COMMON PELVIC TUMORS)
 TECHNIQUES FOR CERVICAL CANCERS (COMMON PELVIC TUMORS)") NEWER RADIATION (3 D -CRT, IMRT, IGRT) TECHNIQUES FOR CERVICAL CANCERS (COMMON PELVIC TUMORS) Umesh Mahantshetty, DMRT, MD, DNBR Associate Professor, Radiation Oncology Convener: Urology Disease Management
NEWER RADIATION (3 D -CRT, IMRT, IGRT) TECHNIQUES FOR CERVICAL CANCERS (COMMON PELVIC TUMORS) Umesh Mahantshetty, DMRT, MD, DNBR Associate Professor, Radiation Oncology Convener: Urology Disease Management