Common Consultations in Outpatient Hematology in 30 mins. Lala Cornelius, MD
|
|
|
- Ethan Farmer
- 6 years ago
- Views:
Transcription
1 Common Consultations in Outpatient Hematology in 30 mins Lala Cornelius, MD
2 Disclosures: None
3 Objectives: 1- Decrease referrals to heme/onc for mild heme abnormalities (leukocytosis, thrombocytopenia) 2- Appropriate evaluation and manaegment of thrombocytosis; 3- Identify areas of concern re: low platelet counts, when to worry about bleeding and when to worry about thrombosis 4-Identify normal variation in leukocytosis and common reversible etiologies
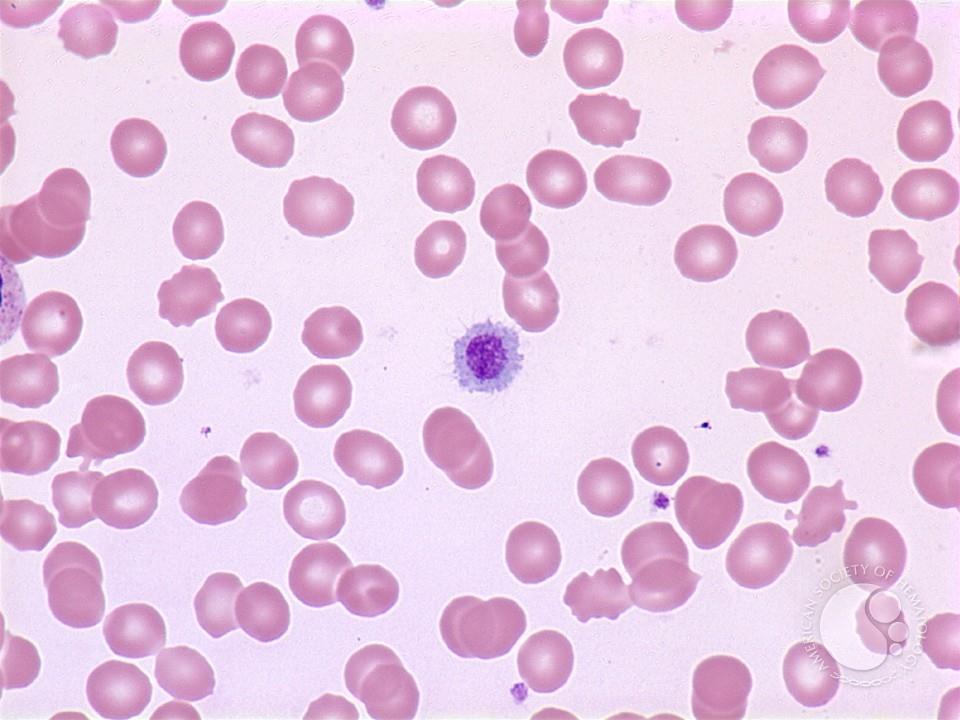
4 Case I A 22 y old woman is seen by her PCP because of her plt count of 5K. She felt healthy until 1 week ago, when she noticed that she was bruising easily and had gingival bleeding with flossing. She has no significant medical history and is not taking any medications. Her plt count 1 year ago was normal. On PE: scattered ecchymosis over arms and petechia over the shins. There is no lymphadenopathy or splenomegaly. CBC : Hgb, 12 (normal) WBC 7.9 with normal Diff ; plt 3K

5
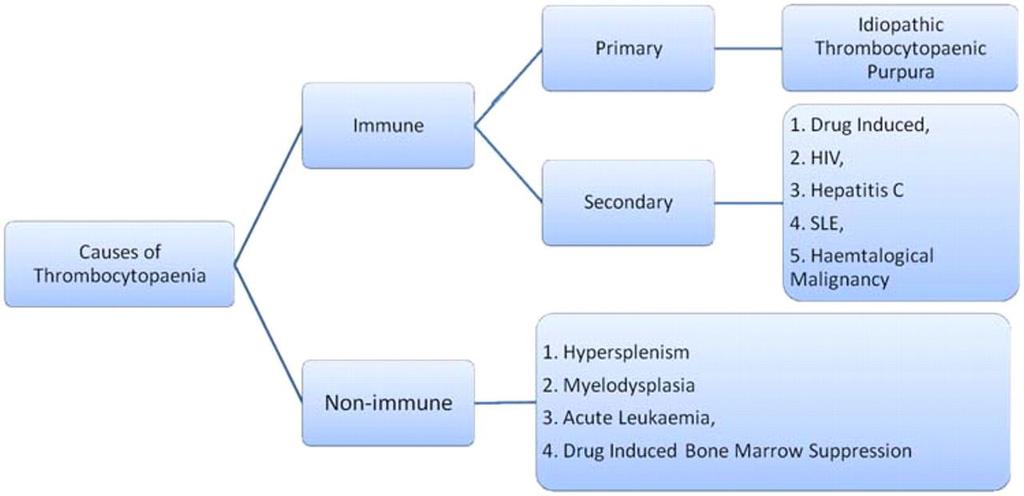
6 ITP Diagnosis of exclusion Hx and PE normal (apart from symptoms and HX of bleeding) Specifically no splenomegaly, no drugs, no viral infections (incl HIV ), no SLE or other autoimmune disease CBC -isolated thrombocytopenia
7
8
9 ITP Acute 2-6 years old No sex predilection Prior infection Abrupt onset Plst <20 K 6-8 weeks duration Usually spontaneous remissions Chronic yrs Women 3:1 No infection Insidious Plts 20-80K Chronic Unusual remission
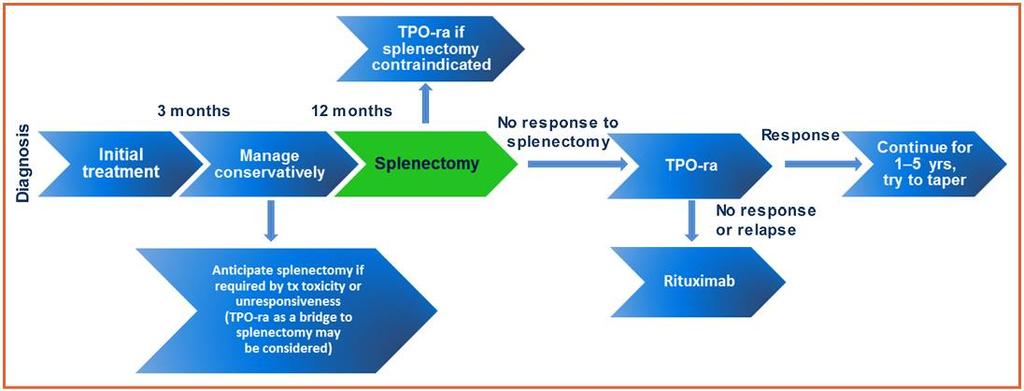
10 Recommendations for surgery Surgery Dental prophylaxis(cleaning/scaling) Simple dental extraction Complex Dental Extraction Minor Surgery Major Surgery Major Neurosurgery Recommended plts counts >20-30,000 > 30,000 >50,000 >50,000 >50,000 >100,000 Cuker A and Cines DB Hematology 2010 ; p
11 ITP practice guideline- adult Rx with steroids is indicated When plts<20-30,000 When plts <50,000 and there is significant mucous membrane bleeding Hospitalization is indicated: In patients with plts<20,000 & significant mucous membrane bleeding (wet purpura )or in noncompliant pt George JN et al, Blood 1996; 88:3-4

12 Wet purpura
13 ITP steroid Rx Prednisone orally 1 mg/kg Improvement usually within 3 days Max improvement in 14 days Dexamethasone orally 40 mg x4 Max response at 7 days, 50% sustained response Plts counts < 90,000 high relapse risk, most within 3 months Cheng Y et et al, NEJM 2003;349:831-6
14
15 Clinical Pearl 1- ITP Most pts with stable mild thrombocytopenia (plts counts K) do not develop worsening thrombocytopenia or other autoimmune disease
16
17 Case 2 A 22 y old woman found to have gradually decreasing plt counts from 180K to 38 K over the past 4 months Her only medication is valproic acid started 12 months ago and which has led to good seizure control She reports no episodes of bleeding and there is no obvious bruising or petechia on PE
18 Drug-induced thrombocytopenia Frequency is uncertain Frequency of medication use increases with age Frequency of alternative medicine use is increasing at all ages Usually first diagnosed as ITP Correct diagnosis is essential to : -Avoid inappropriate treatment -Prevent recurrences
19 Clinical Pearl 2- Drug Induced Thrombocytopenia Thrombocytopenia caused by medication may be immune mediated or dose dependent
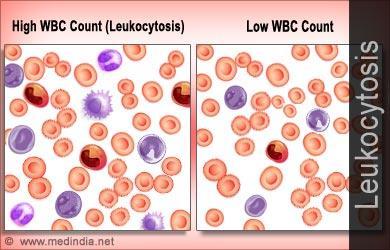
20 Case 3 A 55 y old man was found to have a leukocytosis on routine CBC. The patient has no fatigue, fever, chills, night sweats, or unintentional weight loss. His other medical problems include well controlled HTN and allergic rhinitis. He has smoked 1 pack of cigarettes per day for the last 30 years. Meds: HCTZ PE: afebrile and VSS, exam is negative for lymphadenopathy or splenomegaly CBC: diff elevation of absolute number of leukocytes with increase in immature neutrophilic cells His Hgb and plts are normal and WBC is stable in comparison with 4 weeks ago
21 Elevation of WBC count Acute rapid: changes in distribution (demargination) Chronic elevation: chances in production and release from storage
22 If myeloid cells are present, the leukocytosis should be stratified into neutrophilia, monocytosis, basophilia, or eosinophilia; more than one type of leukocytosis may be present
23
24
25 Clinical Pearl 3A-Leukocytosis Smoking one of the most common causes in asymptomatic patient The leukocyte count in smoker can be 25% higher than value within normal range After smoking cessation WBC can normalize
26 Differential Diagnosis of Neutrophilia Secondary to other illnesses Infection Acute: demargination/release storage pool Chronic: granulomatous dx (leukoerythroblastic) Stress Drug induced (steroids, B-agonist, lithium) Chronic inflammation (including smoking-one of the most common causes) Post-splenectomy Non-hematologic malignancy Marrow stimulation (ITP, hemolysis, CMT) Sterile inflammation (MI, burn)
27 Clinical Pearl 3B-Neutrophilia Neutrophilia should prompt examination for left shift, signs of activated neutrophils, basophilia, dysplasia, and degree of leukocytosis. Most neutrophilias are reactive in nature. WBC count < /L, but usually < /L, is typical. Signs of activated neutrophils, mild left shift, and an absence of basophilia all suggest a reactive process.
28 Differential Diagnosis of Neutrophila Primary Hematologic Disease CML (BCR-ABLE) Other myeloproliferative neoplasm- usually will have elevated Hg or plt counts or splenomegaly (JAK2)
29 Clinical Pearl 3C- Leukocytosis Marked leukocytosis of > /L, marked left shift, dysplasia, or basophilia should prompt a BM examination to evaluate for a myeloid malignancy. Basophilia, although rare, is most suggestive of a MPN, especially CML. PCR for BCR-ABL1 and JAK2 mutational studies can be performed in blood, but a BM examination with cytogenetic studies should also be performed
30 Case 4 23 y old college student who plays football presents to his PCP with 2 week Hx of extreme fatigue and sore throat and new onset fever of 101F. He has no significant PMHx. On PE: T 101.2F and he has posterior cervical lymphadenopathy, splenomegaly, an erythematous posterior pharynx with whitish-gray exudate and generalized macularpapular rash on his trunk and neck. He takes proton pump inhibitor fro GERD. His Lab work : Hgb, plt- normal; WBC 12.9; differential Neutr- 22%(low); Lymp-75%( high); Mono -3% ( normal); Baso- 1%( normal)
31 Clinical Pearl 4A 50% have splenomegaly and at risk of rare complication as spontaneous or traumainduced splenic rupture should avoid sports
32 Differential diagnosis of lymphocytosis Secondary to Illness Viral illnesses Mononucleosis s-m CMV EBV HIV Pertussis Cat scratch disease Toxoplasmosis Babesiosis Drug reaction Reactive granular lymphocytosis Post splenectomy lymphocytosis
33 Differential diagnosis of lymphocytosis Primary hematologic disease CLL Monoclonal B cell lymphocytosis
34 Clinical Pearl 4B Age of the patient (CLL is more common in middle-aged to elderly adults) Correlation with clinical findings is necessary; a monospot test for EBV or viral serologies can also be performed, Hx of prior diagnosis of lymphoma A pleomorphic lymphocytosis favors a reactive lymphocytosis. If monomorphic lymphocytosis is present, a lymphoproliferative disorder should be searched for using flow cytometric immunophenotyping. Depending on these results, select molecular genetic tests will be helpful. (Refer to Hematology) A BM biopsy or extramedullary tissue biopsy may be necessary for a final diagnosis of lymphoma.
35 Differential diagnosis of Eosinophilia Secondary to Illness Allergic rhinitis Asthma Tissue invasive parasite Bronchopulmonary aspergillosis HIV Vasculitis Adrenal insufficiency GI symptoms (infection, IBD) Occult malignancy
36 Differential diagnosis of Eosinophilia Primary hematologic disease Hypereosinophilic syndrome
37 Clinical Pearl 4C Most eosinophilias are reactive in nature and should be evaluated Once reactive eosinophilias are excluded, myeloid and lymphoid neoplasms with eosinophilia and PDGFRA, PDGFRB, and FGFR1 should be searched for by performing a BM examination, cytogenetic studies, and FISH or PCR for the PDGFRA mutation (Refer to Hematology)
38 Differential diagnosis of Monocytosis Secondary to Other illnesses Pregnancy TB Syphilis Sarcoidosis SLE Aslenia Corticosterids
39 Clinical Pearl 4D Most monocytoses are reactive in nature. If reactive causes have been excluded, a persistent monocytosis of more than 3 months or the findings of dysplasia, blast cells, or significant left shift should trigger a BM examination to evaluate for malignancy. (Refer to Hematology)
40 Differential diagnosis of monocytosis Primary hematologic disease Juvenile myelomocytic leukemia Chronic myelomonocytic leukemia Acute monoblastic/monocytic leukemia CML Atypical (BCR-ABL negative) CML Myelodysplastic/myeloproliferative neoplasms, unclassifiable
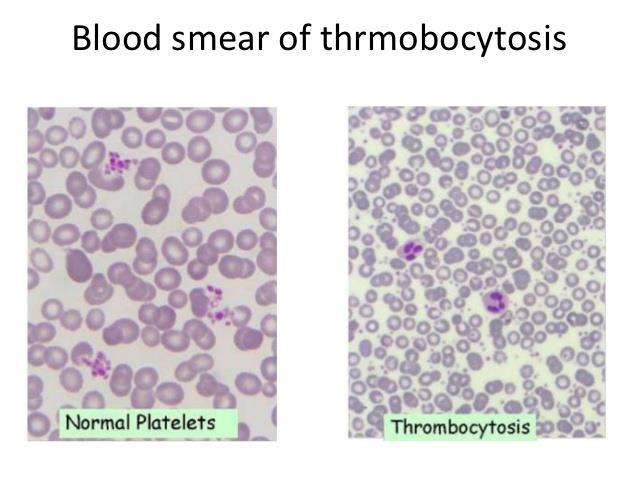
41 Case 5 A 45 year old previously healthy female landscaper complains of increasing fatigue and numbness on her face and legs for 3 weeks. CBC plts 1,062K Her iron studies and inflammatory markers (Sed rate and C reactive protein)-normal FISH BCR-ABL: negative Jak-2: mutated
42
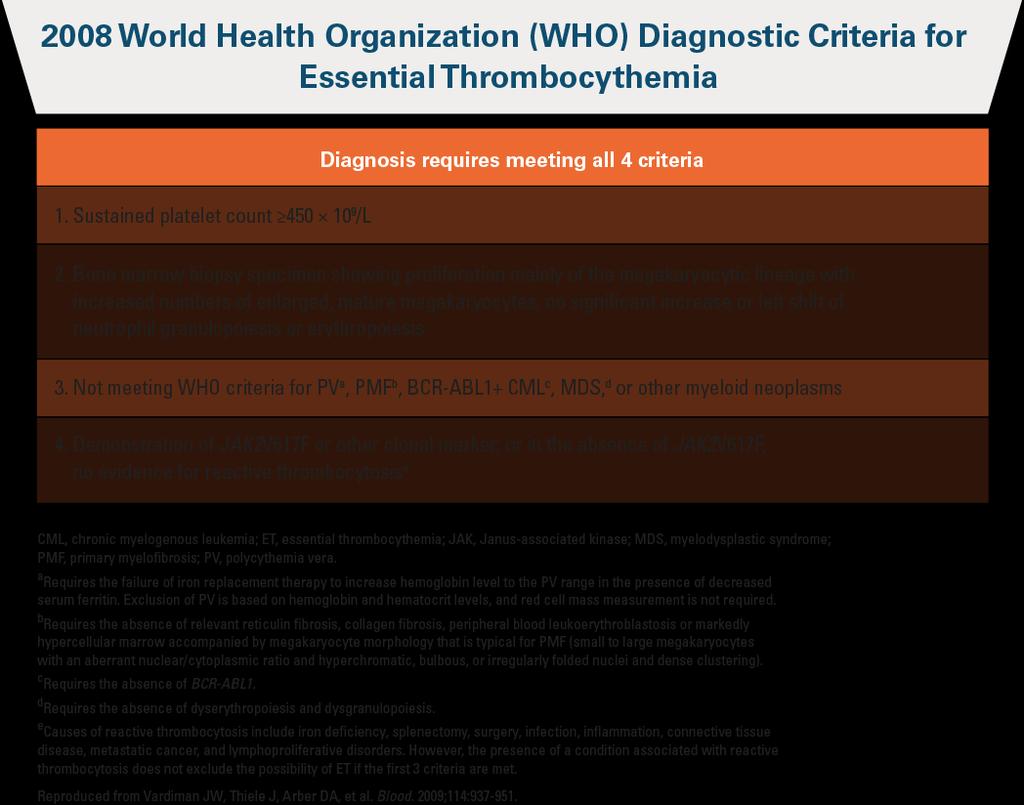
43 Thrombocytosis Primary Essential Thrombocythemia Other forms of myeloproliferative disorderschronic myelogenous leukemia, polycythemia vera, myelofibrosis
44

45
46 Primary Driver Mutations for Essential Thrombocythemia Jak2V617F mutation in % of the pts Clarified that mutation is a primary cause of thrombosis MPLW515L &K - 5% CALR 30% in 2013 Triple negative ET - 10%
47
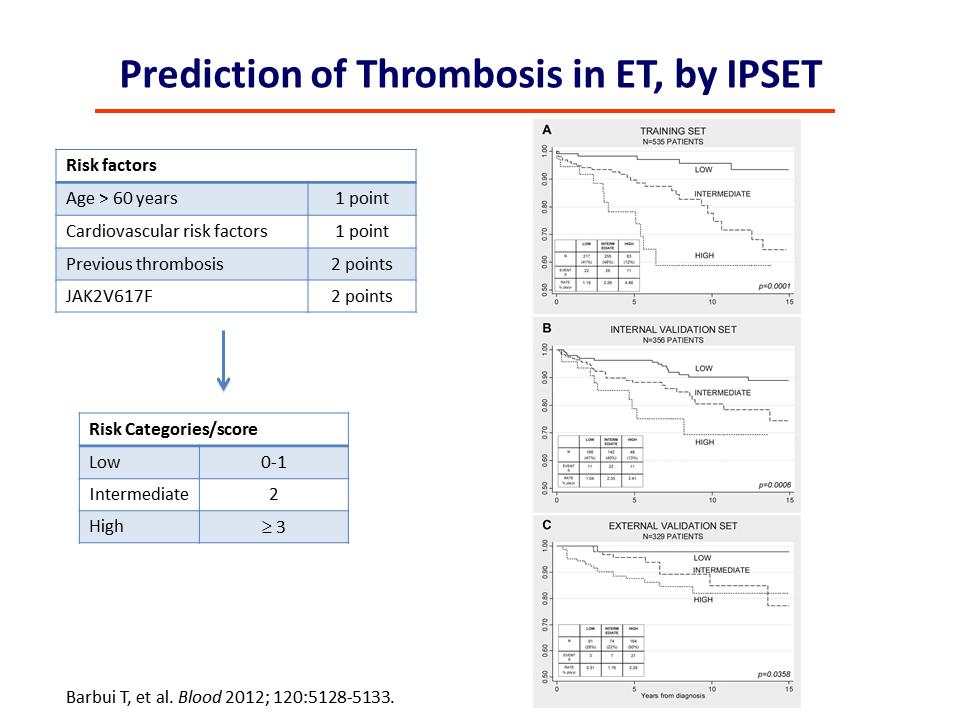
48 Essential thrombocythemia clinical features Chronic thrombocytosis (often extreme, >1million ) Many pts are asymptomatic Vasomotor symptoms: headache, syncope, visual disturbances, atypical chest pain, erythromelalgia (typically ASA-responsive) Thrombocytosis major cause of morbidity and mortality Both arterial and venous; unusual sites No clear association with plts counts Paradoxical increase in bleeding complications Risk factors /associations; -Extreme thrombocytosis >1 million ( controversial) -Use of ASA>325 mg /day or other NSAIDS -Acquired WVD Splenomegaly
49 Thrombocytosis Secondary Inflammation Surgery (which leads to increase inflammatory state ) Hyposplenism or asplenia Hemorrhage or/ and iron deficiency Malignancy Trauma Infection
50 Clinical Pearl 5 Increased level of inflammatory mediators IL- 1b,IL-6, IL-11 have been associated with reactive thrombocytosis C-reactive protein is a surrogate marker for increased IL-6; can suggest an occult inflammation Absolute value of plt counts can not help distinguish reactive thrombocytosis from ET
51
52 Appendix
53 Life span of Myeloid cells Maturation in bone marrow: 7-10 days Circulation in peripheral blood: 3-6 hours Residence in tissues: 2-3 days Peripheral neutrophil counts <5 % of total WBC pool, 2% of the total WBC lifespan
54 White blood cell count Myeloid precursors 20% Storage pool 75% Marginating pool 3% Circulating pool 2%
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms. Daniel A. Arber, MD Stanford University
 Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Polycythemia Vera and other Myeloproliferative Neoplasms. A.Mousavi
 Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss
 Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Disorders of Blood Cells & Blood Coagulation
 Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Approach To Leucocytosis
 C H A P T E R 58 Approach To Leucocytosis Madhuchanda Kar, S Kartthik, Prantar Chakrabarti ABSTRACT Leukocytosis means elevation of WBC count for the patient s age. Leukocytosis might be because of lymphoid
C H A P T E R 58 Approach To Leucocytosis Madhuchanda Kar, S Kartthik, Prantar Chakrabarti ABSTRACT Leukocytosis means elevation of WBC count for the patient s age. Leukocytosis might be because of lymphoid
Adult Acute leukemia. Matthew Seftel. August
 Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Platelet and WBC disorders
 Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas. James J. Stark, MD, FACP
 Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
HEFT Pathology Guideline. GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia
 HEFT Pathology Guideline GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia Produced by: Dr Charalampos Kartsios (Consultant Haematologist) and Muhammad Javed
HEFT Pathology Guideline GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia Produced by: Dr Charalampos Kartsios (Consultant Haematologist) and Muhammad Javed
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Polycthemia Vera (Rubra)
") Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Complete Blood Count PSI AP Biology
 Complete Blood Count PSI AP Biology Name: Objective Students will examine how the immunological response affects molecules in the blood. Students will analyze three complete blood counts and create diagnoses
Complete Blood Count PSI AP Biology Name: Objective Students will examine how the immunological response affects molecules in the blood. Students will analyze three complete blood counts and create diagnoses
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Diagnostic Approach for Eosinophilia and Mastocytosis. Curtis A. Hanson, M.D.
 Diagnostic Approach for Eosinophilia and Mastocytosis Curtis A. Hanson, M.D. 2014 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2014 MFMER slide-2 Molecular Classification
Diagnostic Approach for Eosinophilia and Mastocytosis Curtis A. Hanson, M.D. 2014 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2014 MFMER slide-2 Molecular Classification
Symptoms and Signs in Hematology/ 2013
 Symptoms and Signs in Hematology/ 2013 Abdallah Abbadi.MD.FRCP Professor of Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Diseases of Blood & Blood forming organs A- Benign
Symptoms and Signs in Hematology/ 2013 Abdallah Abbadi.MD.FRCP Professor of Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Diseases of Blood & Blood forming organs A- Benign
Clinical & Laboratory Assessment
 Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Contemporary perspectives and initial management of pediatric ITP. William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA
 Contemporary perspectives and initial management of pediatric ITP William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA Case Presentation 5 year old female Bruises on trunk, extremities
Contemporary perspectives and initial management of pediatric ITP William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA Case Presentation 5 year old female Bruises on trunk, extremities
Case #16: Diagnosis. T-Lymphoblastic lymphoma. But wait, there s more... A few weeks later the cytogenetics came back...
 Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
The Complete Blood Count
 The Complete Blood Count (Cartesian Thinking at Its Best) A SEM Image of Normal Human Blood Laurie Larsson February 22, 2010 Anatomy and Philology II Dr. Danil Hammoudi Introduction A complete blood count
The Complete Blood Count (Cartesian Thinking at Its Best) A SEM Image of Normal Human Blood Laurie Larsson February 22, 2010 Anatomy and Philology II Dr. Danil Hammoudi Introduction A complete blood count
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and
 Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
[COMPREHENSIVE GENETIC ASSAY PANEL ON
 2014 SN GENELAB AND RESEARCH CENTER DR. SALIL VANIAWALA, PH.D [COMPREHENSIVE GENETIC ASSAY PANEL ON MYELOPROLIFERATIVE NEOPLASMS] SN Genelab presents one of the most comprehensive genetic assay panel for
2014 SN GENELAB AND RESEARCH CENTER DR. SALIL VANIAWALA, PH.D [COMPREHENSIVE GENETIC ASSAY PANEL ON MYELOPROLIFERATIVE NEOPLASMS] SN Genelab presents one of the most comprehensive genetic assay panel for
Case Presentation. Attilio Orazi, MD
 Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination
 Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination Arati V. Rao, M.D. Division of Medical Oncology and Geriatrics Duke University Medical Center Durham
Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination Arati V. Rao, M.D. Division of Medical Oncology and Geriatrics Duke University Medical Center Durham
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
GP CME. James Liang Consultant Haematologist. Created by: Date:
 GP CME James Liang Consultant Haematologist Date: Created by: Scenario 52 year old European male Fit and well Brother recently diagnosed with diabetes PMHx Nil Social Hx Ex-smoker stopped 5 years ago (20
GP CME James Liang Consultant Haematologist Date: Created by: Scenario 52 year old European male Fit and well Brother recently diagnosed with diabetes PMHx Nil Social Hx Ex-smoker stopped 5 years ago (20
HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor
: Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor") HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor I. Description of the rotation: During this rotation, the resident will gain
HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor I. Description of the rotation: During this rotation, the resident will gain
Western Health Specialist Clinics Access & Referral Guidelines
 Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
The Internists Approach to Polycythemia and Implications of Uncontrolled Disease
 The Internists Approach to Polycythemia and Implications of Uncontrolled Disease Mary Jo K. Voelpel, DO, FACOI, MA, CS Associate Clinical Professor MSU-COM Disclosures NONE Overview 1. Objectives 2. Case
The Internists Approach to Polycythemia and Implications of Uncontrolled Disease Mary Jo K. Voelpel, DO, FACOI, MA, CS Associate Clinical Professor MSU-COM Disclosures NONE Overview 1. Objectives 2. Case
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Policy Specific Section:
 Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Case #1. 65 yo man with no prior history presented with leukocytosis and circulating blasts: Bone marrow biopsy was performed
 Case #1 65 yo man with no prior history presented with leukocytosis and circulating blasts: WBC 187.4K/uL ; Hgb 10.0gm/dL; Platelet 68K/uL Neutrophil % 25.0% Lymphocyte % 38.0% Monocyte % 12.0% Metamyelocyte
Case #1 65 yo man with no prior history presented with leukocytosis and circulating blasts: WBC 187.4K/uL ; Hgb 10.0gm/dL; Platelet 68K/uL Neutrophil % 25.0% Lymphocyte % 38.0% Monocyte % 12.0% Metamyelocyte
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
All Wales Lymphoma Panel Lymphoma Course April 2015 Wales Millennium Centre Cardiff
 All Wales Lymphoma Panel Lymphoma Course 23-24 April 2015 Wales Millennium Centre Cardiff Case Histories Online slides at: http://dental.uwcm.ac.uk:82/awlp%20course%202015/view.apml? Professor Sebastian
All Wales Lymphoma Panel Lymphoma Course 23-24 April 2015 Wales Millennium Centre Cardiff Case Histories Online slides at: http://dental.uwcm.ac.uk:82/awlp%20course%202015/view.apml? Professor Sebastian
2013 Pathology Student
 About this guide If you re reading this introduction, it means you are probably either a) covering hematopathology in your pathology class right now, or b) studying for boards. Either way, you ve come
About this guide If you re reading this introduction, it means you are probably either a) covering hematopathology in your pathology class right now, or b) studying for boards. Either way, you ve come
CHALLENGING CASES PRESENTATION
 CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
The primary medical content categories of the blueprint are shown below, with the percentage assigned to each for a typical exam:
 Hematology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified hematologist
Hematology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified hematologist
Disclosures/COI. Cases in Hematopathology. Outline. Heme Path Findings Not to Miss. Normal Peripheral Smear 6/30/2016
 Disclosures/COI Cases in Hematopathology Vamsi Kota Assistant Professor Department of Hematology & Medical Oncology Leukemia/BMT I have no disclosures or conflicts of interest regarding this presentation.
Disclosures/COI Cases in Hematopathology Vamsi Kota Assistant Professor Department of Hematology & Medical Oncology Leukemia/BMT I have no disclosures or conflicts of interest regarding this presentation.
Extramedullary precursor T-lymphoblastic transformation of CML at presentation
 Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Anemia. A case-based approach. David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017
 Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Hematology: Challenging Cases with Your Participation COPYRIGHT
 Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
5/5/2010. Goldilocks picture from
 Sometimes platelet counts are TOO LOW; Goldilocks and the Three Platelets Robert T. Means, Jr., M.D. Professor & Senior Associate Chair Department of Internal Medicine University of Kentucky Lexington
Sometimes platelet counts are TOO LOW; Goldilocks and the Three Platelets Robert T. Means, Jr., M.D. Professor & Senior Associate Chair Department of Internal Medicine University of Kentucky Lexington
MDS/MPN MPN MDS. Discolosures. Advances in the Diagnosis of Myeloproliferative Neoplasms. Myeloproliferative neoplasms
 Discolosures Advances in the Diagnosis of Myeloproliferative Neoplasms Consulting income from Promedior, Inc. Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical
Discolosures Advances in the Diagnosis of Myeloproliferative Neoplasms Consulting income from Promedior, Inc. Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical
Case History: A 45 Year Old Female Presenting with Fatigue, High Platelets and Splenomegaly. Clinical Approach, Investigations and Management
 Cronicon OPEN ACCESS EC GASTROENTEROLOGY AND DİGESTİVE SYSTEM Case Report Case History: A 45 Year Old Female Presenting with Fatigue, High Platelets and Splenomegaly. Clinical Approach, Investigations
Cronicon OPEN ACCESS EC GASTROENTEROLOGY AND DİGESTİVE SYSTEM Case Report Case History: A 45 Year Old Female Presenting with Fatigue, High Platelets and Splenomegaly. Clinical Approach, Investigations
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
MYELOPROLIFERATIVE NEOPLASMS
 9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
Hematopathology Case Study
 www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
Easy Trick to Spot Leukemia for Pediatricians
 Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
5/21/2018. Disclosures. Objectives. Normal blood cells production. Bone marrow failure syndromes. Story of DNA
 AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
Diseases Of The Blood
 Diseases Of The Blood DR. Associate Professor Of Pathology Faculty Of Medicine Ain Shams University Red Blood Cells and Anemia RBC=4-6 million/mm 2 Hb=12-18 g/dl Oxygen Carrying Molecule Hemoglobin Tetramer:
Diseases Of The Blood DR. Associate Professor Of Pathology Faculty Of Medicine Ain Shams University Red Blood Cells and Anemia RBC=4-6 million/mm 2 Hb=12-18 g/dl Oxygen Carrying Molecule Hemoglobin Tetramer:
Case Report Immune Thrombocytopenia and JAK2V617F Positive Essential Thrombocythemia: Literature Review and Case Report
 Hindawi Case Reports in Hematology Volume 2017, Article ID 3725089, 4 pages https://doi.org/10.1155/2017/3725089 Case Report Immune Thrombocytopenia and JAK2V617F Positive Essential Thrombocythemia: Literature
Hindawi Case Reports in Hematology Volume 2017, Article ID 3725089, 4 pages https://doi.org/10.1155/2017/3725089 Case Report Immune Thrombocytopenia and JAK2V617F Positive Essential Thrombocythemia: Literature
Abstracting Hematopoietic Neoplasms
 CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
Hypereosinophili c syndrome
 Hypereosinophili c syndrome Eosinophilia Eosinophilia is commonly defined as an elevated percentage of eosinophils, with an absolute eosinophil count > 500 cells per cubic millimeter Secondary Primary
Hypereosinophili c syndrome Eosinophilia Eosinophilia is commonly defined as an elevated percentage of eosinophils, with an absolute eosinophil count > 500 cells per cubic millimeter Secondary Primary
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228
 2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Leukocyte Disorders. Dr Alauldeen Mudhafar Zubair
 Leukocyte Disorders Dr Alauldeen Mudhafar Zubair Composition of blood Specialized connective tissue Blood cells (formed elements) suspended in plasma Blood volume: 5-6 liters (approx 1.5 gal) in males
Leukocyte Disorders Dr Alauldeen Mudhafar Zubair Composition of blood Specialized connective tissue Blood cells (formed elements) suspended in plasma Blood volume: 5-6 liters (approx 1.5 gal) in males
GOOD MORNING! Thursday, July Heidi Murphy, MD Leslie Carter-King, MD
 GOOD MORNING! Thursday, July 10 2014 Heidi Murphy, MD Leslie Carter-King, MD PREP QUESTION Almost all infants experience a transient increase in bilirubin concentrations known as physiologic jaundice during
GOOD MORNING! Thursday, July 10 2014 Heidi Murphy, MD Leslie Carter-King, MD PREP QUESTION Almost all infants experience a transient increase in bilirubin concentrations known as physiologic jaundice during
12 Dynamic Interactions between Hematopoietic Stem and Progenitor Cells and the Bone Marrow: Current Biology of Stem Cell Homing and Mobilization
 Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
The Power of Peripheral Blood Smears: Apparent Diagnostic Clues (Part 1) (Wednesday, October 19, 2011)
 (Wednesday, October 19, 2011)") The Power of Peripheral Blood Smears: Apparent Diagnostic Clues (Part 1) (Wednesday, October 19, 2011) By Gene Gulati, Ph.D., SH(ASCP) Conflict of Interest None Plan for the Course Review blood smears,
The Power of Peripheral Blood Smears: Apparent Diagnostic Clues (Part 1) (Wednesday, October 19, 2011) By Gene Gulati, Ph.D., SH(ASCP) Conflict of Interest None Plan for the Course Review blood smears,
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
Hematology 101. Cindy Rogers, MT(ASCP) Diagnostics System Specialist
 Diagnostics System Specialist") Hematology 101 Cindy Rogers, MT(ASCP) Diagnostics System Specialist More Acronyms...» CBC» RBC» HGB» HCT» WBC» MPV» PLT» RDW» DIFF» H&H» Complete Blood Count» Red Blood Cell» Hemoglobin» Hematocrit» White
Hematology 101 Cindy Rogers, MT(ASCP) Diagnostics System Specialist More Acronyms...» CBC» RBC» HGB» HCT» WBC» MPV» PLT» RDW» DIFF» H&H» Complete Blood Count» Red Blood Cell» Hemoglobin» Hematocrit» White
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Part 4 MYELOID NEOPLASMS
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
Juvenile Myelomonocytic Leukemia (JMML)
") Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
MOC HEM - General Hematopathology (Mandatory 50-Question Module)
") MOC HEM - General Hematopathology (Mandatory 50-Question Module) acute monoblastic/monocytic leukemia infectious mononucleosis adult T cell leukemia/lymphoma in situ follicular lymphoma ALL; phenotypes
MOC HEM - General Hematopathology (Mandatory 50-Question Module) acute monoblastic/monocytic leukemia infectious mononucleosis adult T cell leukemia/lymphoma in situ follicular lymphoma ALL; phenotypes
MOC HEM - General Hematopathology (Mandatory 50-Question Module)
") MOC HEM - General Hematopathology (Mandatory 50-Question Module) acute monoblastic/monocytic leukemia infectious mononucleosis adult T cell leukemia/lymphoma in situ follicular lymphoma ALL; phenotypes
MOC HEM - General Hematopathology (Mandatory 50-Question Module) acute monoblastic/monocytic leukemia infectious mononucleosis adult T cell leukemia/lymphoma in situ follicular lymphoma ALL; phenotypes
Understanding Your Blood Work Results
 Understanding Your Blood Work Results Carlos Besses, MD, hd Hematology Department Hospital del Mar - IMIM, Barcelona Carlos Besses Disclosures Novartis Honorarium Speaker Shire Honorarium Speaker Galena
Understanding Your Blood Work Results Carlos Besses, MD, hd Hematology Department Hospital del Mar - IMIM, Barcelona Carlos Besses Disclosures Novartis Honorarium Speaker Shire Honorarium Speaker Galena
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Kaaren Reichard Mayo Clinic Rochester
 Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Refresher in Blood Cell Morphology. Tracy I. George, MD Professor of Pathology University of Utah
 Refresher in Blood Cell Morphology Tracy I. George, MD Professor of Pathology University of Utah No financial conflicts of interest Objectives Recognize non-neoplastic and neoplastic disorders in the peripheral
Refresher in Blood Cell Morphology Tracy I. George, MD Professor of Pathology University of Utah No financial conflicts of interest Objectives Recognize non-neoplastic and neoplastic disorders in the peripheral
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Managing ET in Tiziano Barbui MD
 Managing ET in 2019 Tiziano Barbui MD (tbarbui@asst-pg23.it) Hematology and Foundation for Clinical Research, Hospital Papa Giovanni XXIII Bergamo, Italy Managing ET in 2019 Establish diagnosis Risk Stratification
Managing ET in 2019 Tiziano Barbui MD (tbarbui@asst-pg23.it) Hematology and Foundation for Clinical Research, Hospital Papa Giovanni XXIII Bergamo, Italy Managing ET in 2019 Establish diagnosis Risk Stratification
Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML
 reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Myelodysplastic Syndromes Myeloproliferative Disorders
 Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Drop of Blood Unravels Mysteries. Prof. Salma Afrose Department of Hematology Dhaka Medical College
 Drop of Blood Unravels Mysteries Prof. Salma Afrose Department of Hematology Dhaka Medical College Peripheral Blood Film (PBF) PBF is a laboratory workup that involves cytology of Peripheral blood cell
Drop of Blood Unravels Mysteries Prof. Salma Afrose Department of Hematology Dhaka Medical College Peripheral Blood Film (PBF) PBF is a laboratory workup that involves cytology of Peripheral blood cell
MYELODYSPLASTIC AND MYELOPROLIFERATIVE
 MYELODYSPLASTIC AND MYELOPROLIFERATIVE DISORDERS Pediatric Hemato-Oncology Division Medical Faculty University of Sumatera Utara 1 MYELODYSPLASIA SYNDROME A group of disorder defect in hematopoetic cell
MYELODYSPLASTIC AND MYELOPROLIFERATIVE DISORDERS Pediatric Hemato-Oncology Division Medical Faculty University of Sumatera Utara 1 MYELODYSPLASIA SYNDROME A group of disorder defect in hematopoetic cell
Table 8.1. Epidemiology of Leukemia in the United States (2010) Annual Deaths. Mean Age. Percentage of All Leukemias (%) (Number of New Cases)
 Annual Deaths. Mean Age. Percentage of All Leukemias (%) (Number of New Cases)") Table 8.1. Epidemiology of Leukemia in the United States (2010) Type of Leukemia Annual Incidence (Number of New Cases) Percentage of All Leukemias (%) Annual Deaths Mean Age Acute lymphocytic 5,330 12
Table 8.1. Epidemiology of Leukemia in the United States (2010) Type of Leukemia Annual Incidence (Number of New Cases) Percentage of All Leukemias (%) Annual Deaths Mean Age Acute lymphocytic 5,330 12
MYELOPROLIFERATIVE NEOPLASMS. Matthew Ulrickson, MD Banner MD Anderson Cancer Center September 20, 2016
 MYELOPROLIFERATIVE NEOPLASMS Matthew Ulrickson, MD Banner MD Anderson Cancer Center September 20, 2016 Matthew.Ulrickson@bannerhealth.com Objectives Discuss an approach to increased cell counts Discuss
MYELOPROLIFERATIVE NEOPLASMS Matthew Ulrickson, MD Banner MD Anderson Cancer Center September 20, 2016 Matthew.Ulrickson@bannerhealth.com Objectives Discuss an approach to increased cell counts Discuss
Platelet Disorders. By : Saja Al-Oran
 Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Hematopathology Case Study
 Hematopathology Case Study AMP Outreach Course 2009 AMP Annual Meeting John Greg Howe Ph.D. Department of Laboratory Medicine Yale University School of Medicine November 19, 2009 HISTORY Case History An
Hematopathology Case Study AMP Outreach Course 2009 AMP Annual Meeting John Greg Howe Ph.D. Department of Laboratory Medicine Yale University School of Medicine November 19, 2009 HISTORY Case History An
Borderline cytopenias. Dr Taku Sugai Consultant Haematologist
 Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data
 Post-HCT Data") Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
ACCME/Disclosures 4/13/2016. Clinical History
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
CHAPTER:4 LEUKEMIA. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY 8/12/2009
 LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
Disclosure: Objectives/Outline. Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations. Nothing to disclose.
 RC1 Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations RC2 Disclosure: Nothing to disclose Henry Moon Lecture: UCSF Annual Conference Kathryn Foucar, MD kfoucar@salud.unm.edu May
RC1 Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations RC2 Disclosure: Nothing to disclose Henry Moon Lecture: UCSF Annual Conference Kathryn Foucar, MD kfoucar@salud.unm.edu May
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities
 WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
Patterns of Lymphoid Neoplasia in Peripheral Blood. Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure
 Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Bio& 242 Unit 3 / Lecture 1
 Bio& 242 Unit 3 / Lecture 1 Major Functions of Blood The body contains 4 to 6 liters of blood with an average ph of 7.35 to 7.45. Functions include: Transport Oxygen, Carbon Dioxide, Nutrients, Hormones,
Bio& 242 Unit 3 / Lecture 1 Major Functions of Blood The body contains 4 to 6 liters of blood with an average ph of 7.35 to 7.45. Functions include: Transport Oxygen, Carbon Dioxide, Nutrients, Hormones,
MYELOPROLIFARATIVE NEOPLASMS. Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin).
, FRCP(Edin).") MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,