Lesions of the oral cavity Salivary glands. See Oral pathology
|
|
|
- Peregrine Townsend
- 5 years ago
- Views:
Transcription
1 Lesions of the oral cavity Salivary glands See Oral pathology
2 Esophagus From highly lethal Ca to bland esophagitis. Dysphagia, heartburn, hematemesis, melena. Anatomic and motor disorders: Stenosis - adults, dysphagia, lower esophagus narrowing due to reflux and inflammation Atresia and fistula - newborn with aspiration (absence of lumen), tracheoesophageal fistula (may be together) Mucosal webs - acquired mucosal membrane occluding the lumen Diverticula - nocturnal regurgitation, acquired outpouching of the wall
3 Esophagus Hiatal hernia: Separation of the diaphragmatic crura and widening of the space between the muscular crura. Two patterns: 1/axial (sliding) hernia - 95 % of cases, protrusion of stomach through the diaphragm, bell-shaped, 2/paraesophageal (rolling) - separate portion of stomach, cause obscure. Heartburn, regurgitation of food, incompetence of sphincter. Obesity! Complications - ulceration, bleeding, perforation.

4
5 Esophagus Achalasia: "Failure to relax" of lower esophageal sphincter in swallowing aperistalsis, partial or incomplete relaxation of the lower sphincter, increased resting tone of the lower sphincter Impaired arrangement of innervation. Secondary - destruction of the myenteric plexus Chagas' disease (Trypanosoma cruzi). Progressive dilatation of proximal esophagus, inflammation, thickening, nocturnal regurgitation, young adults, childhood, risk of squamous Ca.
6 Esophagus Laceration (Mallory-Weiss syndrome): Longitudinal tears - chronic alcoholics inadequate relaxation of the musculature of lower sphincter during vomiting. Mucosal tear - bleeding, wall tear - ulcer, mediastinitis
7 Esophagus Varices: Porto-caval anastomoses Liver cirrhosis - portal hypertension 2/3 of all cirrhotic patients massive hemorrhage, 40% die during first episode, 1/2 within 1Y

8

9

10
11 Esophagus Esophagitis: gastric intubation, uremia, irritant foods, alcohol, smoking, radiation, chemotherapy Higher incidence in Northern Iran and China Mild - hyperemia, severe - ulceration Heartburn, regurgitation, chest pain (mimicking MI), bleeding, Barrett

12

13

14
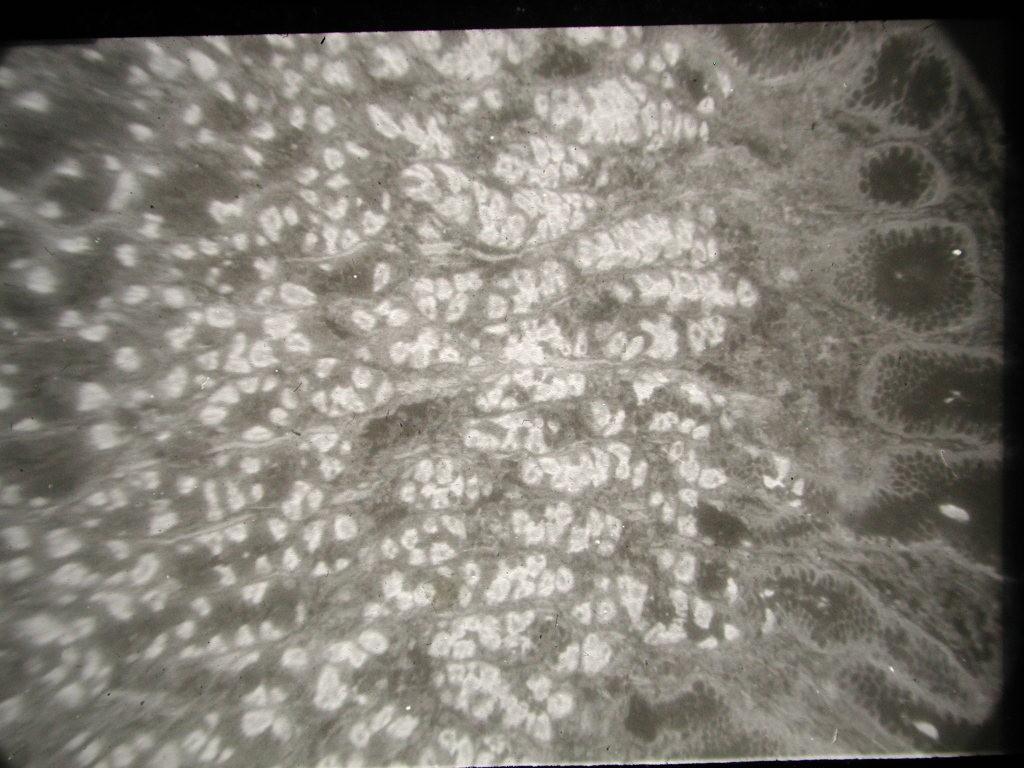
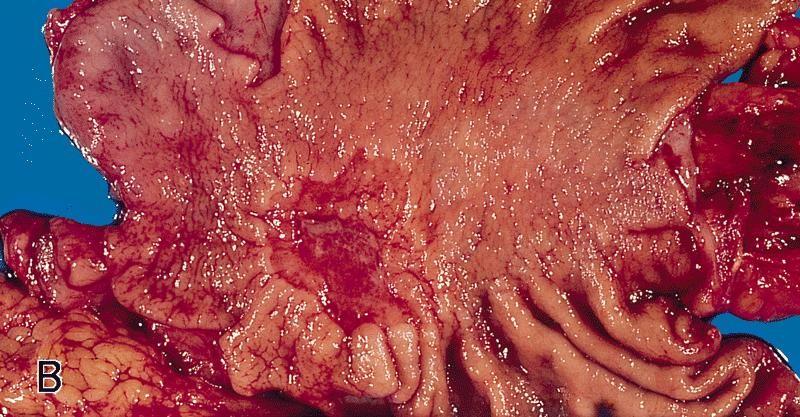
15 Esophagus Barrett's esophagus: long-lasting reflux, abnormal metaplastic columnar epithelium with goblet cells low ph - ulcers, 30-40x increased risk of adenoca. red, velvety mucosa - up from gastroesophageal junction or isolated islands in the distal esophagus

16

17

18

19

20
21 Esophageal tumors Benign tumors papilloma Leiomyoma Lipoma Etc.
22 Esophageal carcinoma squamous cell Ca Risk factors:» esophagitis, achalasia, PlummerVinson sy (microcytic hypochromic anemia, atrophic glossitis)» Life style - alcohol, tobacco» Genetic - tylosis (hyperkeratosis of palms and soles) - Northern Iran» Barrett - adenoca» Long prodromes, dysplastic changes.

23
24 Esophageal carcinoma Grossly: 1/polypoid 2/ulcerative 3/diffuse AdenoCa: Barrett - distal esophagus Weight loss, anorexia, fatigue, pain related to swallowing Biopsy, surgery

25

26

27

28

29

30

31

32

33

34
35 Stomach From bland gastritis to carcinoma. Congenital. pyloric stenosis, diaphragmatic hernia, gastric heterotopia (esophagus, small intestine - Meckel). Heartburn, vague pain, hematemesis, melena. Gastritis: Inflammation of gastric mucosa. Acute or chronic

36
37 Chronic gastritis Type B > frequent x acute atrophy or metaplasia Helicobacter pylori, persists for decades enzymes + toxins + noxious chemicals from recruited neutrophils Intestinal metaplasia - dysplasia Proliferation of lymphoid tissue - ML Hypochlorhydria Type A autoimmune - antibodies x parietal cells atrophy - loss of acid + intrinsic factor achlorhydria pernicious anemia hypergastrinemia
38

39

40

41

42

43

44

45
46 Peptic ulcers Erosion mucosa Ulcer lamina muscularis mucosae and deeper Acute or chronic Gastric x duodenal Loss of balance betwen protective and aggressive forces Most frequent cause = Helicobacter p. Helicobacter pylori - > 70% gastric ulcers Only 10-20% patients with Helicobacter pylori develop peptic ulcer. Unknown interactions. Zollinger-Ellison sy - hypergastrinemia Cigarette smoking, alcohol. corticosteroids, stress
47 Acute peptic ulcers Acute ulcers: Mainly in stomach, rare in duodenum stress trauma, surgical injury of CNS, extensive burns, gastric irritant drugs Small - up to 1 cm, anywhere in the stomach, usually multiple. Adjacent mucosa without inflammation

48
49 Chronic peptic ulcers Chronic u. - several cm Elevated walls - radial mucosal folds. Gastritis is almost always associated. Complications: penetration - to omentum, liver, pancreas perforation peritonitis bleeding - melena, exsanguination Symptoms - burning and boring pain, weight loss, hemorrhage. Pain is worse at night, relieved by alakali or food

50

51
52 Tumors Epithelial tumors predominate Polyps: 1/ hyperplastic % - not true neoplasms 2/ fundic gland polyps - 10% - dilated glands 3/ adenomatous - 5% - true neoplasms All more frequent in chronic gastritis.
53 Gastric carcinoma AdenoCa (95%), Geographical incidence - most common in Japan, Hungary. AdenoCa - two forms 1/ intestinal type - from intestinal metaplasia - chronic gastritis - male predominance - nitrites, smoked foods, Helicobacter pylori, pernicious anemia 2/ diffuse type - in younger, directly from gastric glands - risk factors unknown
54 Gastric carcinoma Localization- pylorus, antrum, cardia, remainder of the body and fundus Early cancer - mucosa, submucosa Morphology: 1/ exophytic 2/ flat 3/ ulcerative Leather-bottle stomach - scirhous carcinoma (linitis plastica)
55 Gastric carcinoma Histology: 1/ intestinal type 2/ diffuse - "signet ring" cells Metastasis - regional lymph nodes, supraclavicular node (Virchow's). Krukenberg tumor (ovary), liver Symptoms - abdominal discomfort, weight loss, pain. Therapy surgery Prognosis very bad in advanced
56

57

58

59

60

61
62 Small intestine developmental anomalies Atresia - segmental Stenosis - segmental Duplication Meckel's diverticulum - failure of involution of omphalomesenteric duct, 34 cm long, distal ileum, asymptomatic, gastric metaplasia, islands of pancreatic tissue

63
64 Large intestine developmental anomalies Malrotation - cecum in left upper abdomen (confusing appendicitis), Hirschprung disease - megacolon
65 Hirschprung disease - congenital megacolon Aganglionic segment of intestinal wall - 1/5 of cases longer segment, rarely - the whole colon. Males predominate (4:1). Sometimes extreme dilatation (1520 cm in diam.) - ulcers, stercoral peritonitis. resection of aganglionic segment (frozen sections intraoperative). x Acquired megacolon: 1/Chagas's disease - trypanosomes destroy the plexus 2/obstruction by the tumor 3/toxic megacolon 4/functional psychosomatic disorder

66
67 Vascular disorders Ischemic bowel disease: Acute occlusion infarction. end-arteries - transmural necrosis venous obstruction (thrombosis) hemorrhagic infarsation.
68 Vascular disorders Conditions 1/ arterial thrombosis - AS, vasculitis, surgical accidents, oral contraceptives 2/ arterial embolism 3/ venous thrombosis 4/ non-occlusive ischemia - shock, dehydration, cardiac failure
69 Vascular disorders Transmural infarction - dark red hemorrhagic, gangrene (bacteria), perforation Mural and mucosal - multifocal, ulcerations, inflammation, pseudomembrane Symptoms - usually in older patients, transmural - severe pain, bloody diarrhea, shock, high mortality Mural and mucosal - abdominal distention, bleeding, pain, may be fatal but may heal

70

71

72
73 Vascular disorders Angiodysplasia: Tortuous dilatation of mucosal and submucosal vessels - cecum, 6th decade, bleeding hereditary hemorrhagic teleangiectasia (Osler-Weber-Rendu sy) isolated lesions, cause - mechanical factors Hemorrhoids: Varices - rectum and anus, after the age of 50, pregnancy, obstipation, liver cirrhosis Complications - bleeding, prolaps, thrombosis
74 Diarrheal diseases Bacterial enterocolitis: Toxins (Staphylococcus aureus, Vibrio, Clostridium perfringens,, Clostridium botulinum), Salmonella (typhi, enteritidis) - S. typhi - typhoid fever Shigella - distal colon. Campylobacter jejuni - superficial ulcers. Yersinia enterocolitica - lymph node granulomas (lymphadentis mesenterialis). Vibrio cholerae - small intestine, mucus depleted crypts. Clostridium difficile - pseudomembranous colitis. Clostrdium perfringens - severe necritizing enterocolitis with perforation (pigbel)
75 Diarrheal diseases Viral gastroenteritis - (gastritis less pronounced in a case of all gastroenteric cases): Rotavirus, Norwalk virus, other viruses (adenovirus, calcivirus, astrovirus) Protozoal infection: Entamoeba histolytica Giardia lamblia
76 Malabsorption syndromes Impaired absorption of fats, proteins, carbohydrates, electrolytes, minerals, and water Most common - due to pancreatitis, celiac sprue, and Crohn's disease
77 Malabsorption syndromes Pancreatic insufficiency - chronic pancreatitis, cystic fibrosis. Bacterial overgrowth - osmotic diarrhea, steatorrhea Lactose intolerance - inherited disaccharidase deficiency - milk intolerance
78 Malabsorption syndromes Gluten-sensitive enteropathy = celiac sprue non-infectious - crossreactivity sensitivity to gluten (grains of wheat, oat, barley, rye) epithelial damage Tropical sprue - infection (unknown), diffuse enteritis, ATB treatment Whipple's disease - intestine, CNS, joints macrophages laden by Gram+ Tropheryma whippelii ATB treatment, males, 4-5th decade
79 Idiopathic inflammatory bowel disease Crohn's disease Ulcerative colitis
80 Idiopathic inflammatory bowel disease Crohn's disease segmental transmural inflammation, fibrosis and thickening, usually terminal ileum and caecum "skips", anywhere in GIT (systemic disease accompanied by uveitis, sacroilitis, polyarthritis, sclerosing cholangoitis Any age, most 2nd - 3rd decade Symptoms - non-characteristic - pain, fever, diarrhea, sometimes bleeding, remissions, relapses
81 Idiopathic inflammatory bowel disease transmural, mucosal damage, granulomas, fissures and fistulae ulcers in mucosa, mucosal inflammation, granulomas dysplastic changes, higher risk of Ca Complications - fistulae to other bowel loops, urinary bladder, vagina, skin, abdominal abscesses, intestinal strictures

82
83 Idiopathic inflammatory bowel disease Ulcerative colitis limited to mucosa and submucosa. Starts in rectum, extends proximally (whole colon) Systemic disease - migratory polyarthritis, uveitis, sclerosing cholangitis Any age, peak years Symptoms - pain, bloody mucosal diarrhea, weight loss Extraintestinal manifestations - migratory polyarthritis Dg - endoscopy, biopsy
84 Idiopathic inflammatory bowel disease Ulcerative colitis Granulomas & skip lesions absent, little fibrosis Rectum+sigmoideum - 80%, entire colon 10%. Bleeding, edema, inflammatory pseudopolyps ulcers - longitudinal, sometimes gangrene, mucosal atrophy Diffuse inflammatory infiltrate, crypt abscesses ulcer healing - submucosal fibrosis Dysplastic changes, high risk of Ca (duration & extent of disease play a role)

85

86
87 Colonic diverticulosis Congenital - all three layers - Meckel. Most - acquired - anywhere in GIT, mostly in sigmoid colon nerves and vessels penetrate internal (circular) muscular layer - defects Older age, Western countries (low fiber diet) Symptoms - asymptomatic, discomfort diverticulitis - pain, abscess formation. Treatment - high-fiber diet, diverticulitis - surgery
88 Colonic diverticulosis Two factors: 1/ peristaltic contractions - elevation of pressure 2/ focal defects of muscular wall Appearance - up to 1 cm, usually sigmoid, adjacent to teniae, thin-walled Complications - inflammation diverticulitis, perforation - peritonitis, adhesions

89
90 Bowel obstruction Hernias - protrusion of pouchlike, serosalined sac of peritoneum - hernial sac. Inguinal, femoral, umbilical canal, surgical scars. Retroperitoneal hernia - Treitz ligament. Segments of viscera trapped, Incarceration ischemia necrosis (hemorrhagic infarction), ileus Acute abdomen!
91 Bowel obstruction Intussusception - proximal segment to distal Volvulus - twisting of the loops or other structures (ovary) - small bowel usually - obstruction, infarction
92

93
94 Tumors High incidence of colorectal Ca in Czech Republic Vast majority- large intestine Polyps Sessile Pedunculated non-neoplastic - inflammatory Hyperplastic adenomatous polyps Mesenchymal lymphoid
95 Tumors Non-neoplastic polyps - increase with age, 90% of all polyps, hyperplastic - small (up to 5 mm), singly or multiple, no malignant potential! Juvenile polyps - hamartomatous, cystic glands, children younger than 5 years. In adults - retention polyps - long stalk, occur in rectum Peutz-Jeghers polyps - hamartomatous smooth muscle within mucosal stroma
96 Adenomas Small to large, large intestine, dysplastic changes Majority of all adenoca arise from adenomas Symptoms - asymtomatic, occult bleeding, bleeding, anemia. Polyp in Vater's ampulla biliary obstruction. All adenomas potentially malignant Three types: 1/tubular 2/villous 3/tubulovillous

97

98

99
100 Adenomas Tubular - most common, pedunculated, branching glands, dysplasia biopsy sometimes intramucosal Ca - invasive growth into the stalk Villous - larger, sessile - up to 10 cm in diam., higher risk Tubulovillous - admixture. Risk of Ca - size, histology, grade of dysplasia
101 Familial polyposis syndromes Autosomal dominant, familial adenomatous polyposis (FAP) Gardner sy - more than 100 Most - tubullar adenomas Risk of Ca - 100% by mid life. Hereditary nonpolyposis colorectal cancer (HNPCC) - autosomal dominant (Lynch's sy) - high risk of colorectal Ca and endometrial Ca

102
103 Colorectal carcinoma Large intestine (98%), 6-7th decade Higher risk - adenomas, ulcerative colitis M>F High USA, Europe Low India, South America, Africa. Japan Dietary causes: 1/ low-fiber 2/ high content of refined carbohydrates 3/ high content of animal fat 4/ low vitamin A, C, and E
104 Colorectal carcinoma Distribution of Ca proximal colon - polypoid, fungating mass. Sigmoid&rectum - circular, stenosing Both penetrate up to the serosal surface Symptoms - silent, fatigue, iron deficiency anemia Right sided bleeding Rectal stenosis Meta - regional LN, liver, lungs, bones Detection - occult bleeding test, colonoscopy, biopsy, CT - spread (metastases) Therapy surgery, radiation, chemotherapy

105

106

107

108

109

110

111
112 Small intestinal tumors Only 3-6% of GIT tumors AdenoCa - unusual, circular growth duodenum (ampula), LN spread Carcinoid - producing hormones (serotonine) derived from neuroendocrine cells low-grade malignant, local infiltrative growth, meta rare Small bowel, appendix, rectum, bronchi
113 Small intestinal tumors Carcinoid yellow-tan, desmoplasia Mitoses rare Asymptomatic - hormones metabolized in liver Carcionid sy - (cutaneous flushes, diarrhea, asthma, heart fibrosis (pulmonary + tricuspid valve) - hepatic metastases. GIT malignant lymphoma - usually nonhodgkin, MALToma, H. pylori!

114
115 Appendix Acute appenicitis - acute abdomen. oxyuris vermicularis Mucocele - dilatation of the lumen by mucus - non-tumorous obstruction (fecalith) - mucosal atrophy rarely mucocele ruptures mucoperitoneum

116
117 Appendical tumors Carcinoid Mucinous cystadenoma cystadenoca Pseudomyxoma peritonei = mucus+tumor cells, implantation metastasis Jelly like material in peritoneal cavity
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
1. Esophageal diverticulum located above the upper esophageal sphincter is called
 Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Polyps in general: is a descriptive term of forming a mass that is exophytic & polypoid.
 ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
The Nature of Disease Pathology for the Health Professions. Chapter 11. Disorders of the GI Tract. Lecture 11
 The Nature of Disease Pathology for the Health Professions Thomas H. McConnell Chapter 11 Disorders of the GI Tract Lecture 11 Review of the GI Tract Anatomy & Function Figures from: McConnell, The Nature
The Nature of Disease Pathology for the Health Professions Thomas H. McConnell Chapter 11 Disorders of the GI Tract Lecture 11 Review of the GI Tract Anatomy & Function Figures from: McConnell, The Nature
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Pathology of Intestinal Obstruction. Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College
 Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
USMLE Step 1 Problem Drill 17: Gastrointestinal System
 USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
2nd week. preexam. GIT system. Atyaf group. Qs team
 2nd week preexam GIT system Qs team 2nd week 2009 Atyaf group بسم االله الرحمن الرحيم 1) a patient with autoimmune gastritis. He is not likely to develop: A. H.pylori colonization. B. pernicious anemia.
2nd week preexam GIT system Qs team 2nd week 2009 Atyaf group بسم االله الرحمن الرحيم 1) a patient with autoimmune gastritis. He is not likely to develop: A. H.pylori colonization. B. pernicious anemia.
GASTROINTESTINAL TRACT
 GASTROINTESTINAL TRACT ESOPHAGUS Clinical manifestations: 1-Dysphagia (difficulty in swallowing), which is attributed either to deranged esophageal motor function or to narrowing or obstruction of the
GASTROINTESTINAL TRACT ESOPHAGUS Clinical manifestations: 1-Dysphagia (difficulty in swallowing), which is attributed either to deranged esophageal motor function or to narrowing or obstruction of the
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
GASTROINTESTINAL TRACT
 GASTROINTESTINAL TRACT A 40 yr old man complains of difficulty of swallowing & a tendency to regurgitate his food--------- YOUR DIAGNOSIS IS-------- ESOPHAGUS Clinical manifestations: 1-Dysphagia (difficulty
GASTROINTESTINAL TRACT A 40 yr old man complains of difficulty of swallowing & a tendency to regurgitate his food--------- YOUR DIAGNOSIS IS-------- ESOPHAGUS Clinical manifestations: 1-Dysphagia (difficulty
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies
 Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 30 The Digestive System Lesson 2: Pathology of the Digestive System Lesson Objectives Upon completion
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 30 The Digestive System Lesson 2: Pathology of the Digestive System Lesson Objectives Upon completion
GI tract pathology MCQs
 GI tract pathology MCQs 1):The most common cause of intestinal obstruction is A. volvulus B. neoplasm C. intussusception D. hernia E. adhesions 2):A filling defect on a barium examination of the gastrointestinal
GI tract pathology MCQs 1):The most common cause of intestinal obstruction is A. volvulus B. neoplasm C. intussusception D. hernia E. adhesions 2):A filling defect on a barium examination of the gastrointestinal
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
The surface mucous cells and the cardiac and pyloric glands secrete mucus which protects the stomach from self-digestion.
 PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
The term inflammatory bowel disease is used to designate two related inflammatory intestinal disorders:
 3. Disorders of the Small and Large Intestines a. Irritable Bowel Syndrome: The term irritable bowel syndrome is used to describe a functional gastrointestinal disorder characterized by a variable combination
3. Disorders of the Small and Large Intestines a. Irritable Bowel Syndrome: The term irritable bowel syndrome is used to describe a functional gastrointestinal disorder characterized by a variable combination
Gastrointestinal Malignancies. Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline
 Gastrointestinal Malignancies Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline Esophagus normal anatomy Hollow tube 23-25cm long in adults Extends from pharynx to level of
Gastrointestinal Malignancies Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline Esophagus normal anatomy Hollow tube 23-25cm long in adults Extends from pharynx to level of
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX
 Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
NCD for Fecal Occult Blood Test
 NCD for Fecal Occult Blood Test Applicable CPT Code(s): 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal
NCD for Fecal Occult Blood Test Applicable CPT Code(s): 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal
Unexpected Findings at Endoscopy
 The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
Oesophageal Disorders
 Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
HCPCS Codes (Alphanumeric, CPT AMA) ICD-9-CM Codes Covered by Medicare Program
 ICD-9-CM Codes Covered by Medicare Program") HCPCS s (Alphanumeric, CPT AMA) 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal neoplasm screening ICD-9-CM
HCPCS s (Alphanumeric, CPT AMA) 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal neoplasm screening ICD-9-CM
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
General description: Detailed description:
 18. Course Description: General description: This course focuses on Gastro Intestinal system to understand structures, biochemical aspects, physiological functions, pathological disorders, microbial, parasitic
18. Course Description: General description: This course focuses on Gastro Intestinal system to understand structures, biochemical aspects, physiological functions, pathological disorders, microbial, parasitic
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Acquired Megacolon: 1. Chaga s disease. 2. Organic obstruction by tumour or stricture. 3. Toxic megacolon in UC and CD. 4. Functional obstruction.
 GIT DISEASES : Small And Large Intestines: Meckel s Diverticulum: It results form failure of involution of omphalo-mesentric duct. It is a blind ended tubular protrusion up to 6 cm long, usually seen in
GIT DISEASES : Small And Large Intestines: Meckel s Diverticulum: It results form failure of involution of omphalo-mesentric duct. It is a blind ended tubular protrusion up to 6 cm long, usually seen in
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT.
 PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
GIT RADIOLOGY. Water-soluble contrast media (e.g. gastrograffin) are the other available agents.which doesn t cause inflammatory peritonitis..
 are the other available agents.which doesn t cause inflammatory peritonitis..") GIT RADIOLOGY Imaging techniques-general principles: Contrast examinations: Barium sulphate is the best contrast for GIT (with good mucosal coating & excellent opacification & being inert); but is contraindicated
GIT RADIOLOGY Imaging techniques-general principles: Contrast examinations: Barium sulphate is the best contrast for GIT (with good mucosal coating & excellent opacification & being inert); but is contraindicated
Tumors of the Intestines. Malignant Lesion. Adenocarcinoma. sessile Serrated Adenomas
 Tumors of the Intestines Non-Neoplastic Polyps Neoplastic Epithelial Polyps Other Tumors Hyperplastic, Hamartomatous, Juvenile, Peutz-Jeghers, Inflammatory abd Lymphoid Polyphs Benign Polyphs Malignant
Tumors of the Intestines Non-Neoplastic Polyps Neoplastic Epithelial Polyps Other Tumors Hyperplastic, Hamartomatous, Juvenile, Peutz-Jeghers, Inflammatory abd Lymphoid Polyphs Benign Polyphs Malignant
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
The Digestive System. Chapter
 The Digestive System Chapter 15.1 Functions: mechanical and chemical breakdown of food *absorption of nutrients Consists of alimentary canal and accessory organs Wall of the Alimentary Canal 15.2 Characteristics
The Digestive System Chapter 15.1 Functions: mechanical and chemical breakdown of food *absorption of nutrients Consists of alimentary canal and accessory organs Wall of the Alimentary Canal 15.2 Characteristics
Inflammatory Bowel Disease When is diarrhea not just diarrhea?
 Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Diet and Gastrointestinal Problems
 Chapter 20 Diet and Gastrointestinal Problems Objectives Explain uses of diet therapy in gastrointestinal disturbances Identify foods allowed and disallowed in therapeutic diets discussed Adapt normal
Chapter 20 Diet and Gastrointestinal Problems Objectives Explain uses of diet therapy in gastrointestinal disturbances Identify foods allowed and disallowed in therapeutic diets discussed Adapt normal
Digestive system L 2. Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section
 Digestive system L 2 Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section objectives 1-Describe the general structure of digestive tract: a-mucosa. b-submucosa. c-muscularis externa d-adventitia
Digestive system L 2 Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section objectives 1-Describe the general structure of digestive tract: a-mucosa. b-submucosa. c-muscularis externa d-adventitia
Pathogenesis Most individuals with the infection also have the associated gastritis but are asymptomatic
 STOMACH Chronic Gastritis The presence of chronic inflammatory changes in the mucosa leading eventually to mucosal atrophy and epithelial metaplasia. In the Western world the prevalence of chronic gastritis
STOMACH Chronic Gastritis The presence of chronic inflammatory changes in the mucosa leading eventually to mucosal atrophy and epithelial metaplasia. In the Western world the prevalence of chronic gastritis
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1. January 06, 2012
 PATHOLOGY LAB #1. January 06, 2012") MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
Alimentary Canal (I)
") Alimentary Canal (I) Esophagus and Stomach (Objectives) By the end of this lecture, the student should be able to discuss the microscopic structure in correlation with the function of the following organs:
Alimentary Canal (I) Esophagus and Stomach (Objectives) By the end of this lecture, the student should be able to discuss the microscopic structure in correlation with the function of the following organs:
A 35 yr old man presents with a month history of burning epigastric pain that occurs between meals------
 A 35 yr old man presents with a month history of burning epigastric pain that occurs between meals------ The pain can be relieved by food or antiacids------ He denies taking aspirin or NSAID------ Lab
A 35 yr old man presents with a month history of burning epigastric pain that occurs between meals------ The pain can be relieved by food or antiacids------ He denies taking aspirin or NSAID------ Lab
Table of Contents Section I: Esophagus 1. Topographic Relations of the Esophagus 2. Musculature of the Esophagus 3. Arterial Blood Supply of the
 Table of Contents Section I: Esophagus 1. Topographic Relations of the Esophagus 2. Musculature of the Esophagus 3. Arterial Blood Supply of the Esophagus 4. Venous Drainage of the Esophagus 5. Innervation
Table of Contents Section I: Esophagus 1. Topographic Relations of the Esophagus 2. Musculature of the Esophagus 3. Arterial Blood Supply of the Esophagus 4. Venous Drainage of the Esophagus 5. Innervation
Digestive System. Digestion Myths
 Digestive System Digestion Myths Myth # 1 Ulcers: Spicy food and stress cause stomach ulcers. Myth # 2 Heartburn: Smoking a cigarette helps relieve heartburn. Myth # 3 Celiac Disease: Celiac disease is
Digestive System Digestion Myths Myth # 1 Ulcers: Spicy food and stress cause stomach ulcers. Myth # 2 Heartburn: Smoking a cigarette helps relieve heartburn. Myth # 3 Celiac Disease: Celiac disease is
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
HISTOLOGY. GIT Block 432 Histology Team. Lecture 1: Alimentary Canal (1) (Esophagus & Stomach) Done by: Ethar Alqarni Reviewed by: Ibrahim Alfuraih
 (Esophagus & Stomach) Done by: Ethar Alqarni Reviewed by: Ibrahim Alfuraih") HISTOLOGY Lecture 1: Alimentary Canal (1) (Esophagus & Stomach) Done by: Ethar Alqarni Reviewed by: Ibrahim Alfuraih Color Guide: Black: Slides. Red: Important. Green: Doctor s notes. Blue: Explanation.
HISTOLOGY Lecture 1: Alimentary Canal (1) (Esophagus & Stomach) Done by: Ethar Alqarni Reviewed by: Ibrahim Alfuraih Color Guide: Black: Slides. Red: Important. Green: Doctor s notes. Blue: Explanation.
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Chapter 34. Nursing Care of Patients with Lower Gastrointestinal Disorders
 Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Esophageal Disorders. Gastrointestinal Diseases. Peptic Ulcer Disease. Wireless capsule endoscopy. Diseases of the Small Intestine 7/24/2010
 Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
GASTROINTESTINAL SYSTEM
 GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Summary of the Home Health Prospective Payment System Final Rule FY 2014
 Summary of the Home Health Prospective Payment System Final Rule FY 2014 Medicare and Medicaid Programs; Home Health Prospective Payment System Rate Update for CY 2014, Home Health Quality Reporting Requirements,
Summary of the Home Health Prospective Payment System Final Rule FY 2014 Medicare and Medicaid Programs; Home Health Prospective Payment System Rate Update for CY 2014, Home Health Quality Reporting Requirements,
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
CT EVALUATION OF GASTRIC LESIONS:
 CT EVALUATION OF GASTRIC LESIONS: Pictural essay Hasni Bouraoui I, Kahloun A, Jemni H, Elouni F, Moulahi H, Daadoucha A, Ben Ali A, Sriha B, Tlili Graies K Departments of Radiology, Gastro enterology,
CT EVALUATION OF GASTRIC LESIONS: Pictural essay Hasni Bouraoui I, Kahloun A, Jemni H, Elouni F, Moulahi H, Daadoucha A, Ben Ali A, Sriha B, Tlili Graies K Departments of Radiology, Gastro enterology,
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal Disorders
 Gastrointestinal Disorders Objectives: Disorders of the esophagus and stomach Disorders of the small and large intestine Appendicitis Part 1: Disorders of the esophagus and stomach 1 Dysphagic Disorders
Gastrointestinal Disorders Objectives: Disorders of the esophagus and stomach Disorders of the small and large intestine Appendicitis Part 1: Disorders of the esophagus and stomach 1 Dysphagic Disorders
GI update. Common conditions and concerns my patients frequently asked about
 GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GASTRIC HETEROTOPIA IN THE ILEUM WITH ULCERATION AND CHRONIC BLEEDING
 GASTROENTEROLOGY 66: 113-117, 1974 Copyright 1974 by The Williams & Wilkins Co. Vol. 66, No.1 Printed in U.S.A. CASE REPORTS GASTRIC HETEROTOPIA IN THE ILEUM WITH ULCERATION AND CHRONIC BLEEDING KARIM
GASTROENTEROLOGY 66: 113-117, 1974 Copyright 1974 by The Williams & Wilkins Co. Vol. 66, No.1 Printed in U.S.A. CASE REPORTS GASTRIC HETEROTOPIA IN THE ILEUM WITH ULCERATION AND CHRONIC BLEEDING KARIM
Chapter Outline. Structural defects. Obstructive disorders. Preview from Notesale.co.uk Page 3 of 98. Cleft lip and cleft palate
 Structural defects Chapter Outline Cleft lip and cleft palate Page 3 of 98 Esophageal atresia and tracheoesophageal fistula Hernias Obstructive disorders Hypertrophic pyloric stenosis Intussusception Anorectal
Structural defects Chapter Outline Cleft lip and cleft palate Page 3 of 98 Esophageal atresia and tracheoesophageal fistula Hernias Obstructive disorders Hypertrophic pyloric stenosis Intussusception Anorectal
Small Bowel Cases. Introduction. Introduction, Continued 12/7/2011. Lesions Found on endoscopic biopsies Just Like Signing Out
 Small Bowel Cases Lesions Found on endoscopic biopsies Just Like Signing Out Introduction Small intestinal biopsies have a few special pitfalls, for example: Neuroendocrine tumors are readily mistaken
Small Bowel Cases Lesions Found on endoscopic biopsies Just Like Signing Out Introduction Small intestinal biopsies have a few special pitfalls, for example: Neuroendocrine tumors are readily mistaken
CT Evaluation of Bowel Wall Thickening. Dr: Adel El Badrawy; M.D. Lecturer of Radio Diagnosis Faculty of Medicine Mansoura University.
 CT Evaluation of Bowel Wall Thickening By Dr: Adel El Badrawy; M.D. Lecturer of Radio Diagnosis Faculty of Medicine Mansoura University. The CT findings of bowel wall thickening includes 1 Degree of thickening.
CT Evaluation of Bowel Wall Thickening By Dr: Adel El Badrawy; M.D. Lecturer of Radio Diagnosis Faculty of Medicine Mansoura University. The CT findings of bowel wall thickening includes 1 Degree of thickening.
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
Inflammatory Bowel Disease Ischemic bowel disease
 Inflammatory Bowel Disease Ischemic bowel disease Inflammatory Bowel Disease The two disorders that comprise IBD are: ulcerative colitis Crohn disease The distinction between ulcerative colitis and Crohn
Inflammatory Bowel Disease Ischemic bowel disease Inflammatory Bowel Disease The two disorders that comprise IBD are: ulcerative colitis Crohn disease The distinction between ulcerative colitis and Crohn
Patho Basic Chronic Inflammatory Bowel Diseases. Jürg Vosbeck Pathology
 Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Gastric ulcer Duodenal ulcer Pancreatitis Ileus. Barbora Konečná
 Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
... Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment.
 Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Pathology of the Alimentary System Lecture 6 Diseases of intestine
 Systemic Pathology I - VPM 221 Pathology of the Alimentary System Lecture 6 Diseases of intestine Enrique Aburto Fall 2014 VII. Small & Large Intestines Structure & Function Long coiled tube, large surface
Systemic Pathology I - VPM 221 Pathology of the Alimentary System Lecture 6 Diseases of intestine Enrique Aburto Fall 2014 VII. Small & Large Intestines Structure & Function Long coiled tube, large surface
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Gastrointestinal Tract. Anatomy of GI Tract. Anatomy of GI Tract. (Effective February 2007) (1%-5%)
 (1%-5%)") Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
FY 2016 MCRCEDP Approved ICD-10 Code List
 Approved List C18.0 Malignant neoplasm of cecum C18.1 Malignant neoplasm of appendix C18.2 Malignant neoplasm of ascending colon C18.3 Malignant neoplasm of hepatic flexure C18.4 Malignant neoplasm of
Approved List C18.0 Malignant neoplasm of cecum C18.1 Malignant neoplasm of appendix C18.2 Malignant neoplasm of ascending colon C18.3 Malignant neoplasm of hepatic flexure C18.4 Malignant neoplasm of
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract
 Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract Eric J. May 1, Shannon P. Sheedy 1, Joel G. Fletcher 1, Mark J. Truty 2, Thomas C. Smyrk 3, Jeff L. Fidler 1 1. Radiology,
Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract Eric J. May 1, Shannon P. Sheedy 1, Joel G. Fletcher 1, Mark J. Truty 2, Thomas C. Smyrk 3, Jeff L. Fidler 1 1. Radiology,
(b) Stomach s function 1. Dilution of food materials 2. Acidification of food (absorption of dietary Fe in small intestine) 3. Partial chemical digest
 Stomach s function 1. Dilution of food materials 2. Acidification of food (absorption of dietary Fe in small intestine) 3. Partial chemical digest") (1) General features a) Stomach is widened portion of gut-tube: between tubular and spherical; Note arranged of smooth muscle tissue in muscularis externa. 1 (b) Stomach s function 1. Dilution of food
(1) General features a) Stomach is widened portion of gut-tube: between tubular and spherical; Note arranged of smooth muscle tissue in muscularis externa. 1 (b) Stomach s function 1. Dilution of food
Diseases of the gastrointestinal system. H Awad Lecture 2: small intestine/ part 2 and appendix
 Diseases of the gastrointestinal system H Awad Lecture 2: small intestine/ part 2 and appendix Malabsorption most important causes of malabsorption: Celiac disease tropical sprue Lactase deficiency Whipple
Diseases of the gastrointestinal system H Awad Lecture 2: small intestine/ part 2 and appendix Malabsorption most important causes of malabsorption: Celiac disease tropical sprue Lactase deficiency Whipple
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Module 2 Heartburn Glossary
 Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
(A) Diarrhea. (B) Stomach cramps. (C) Dehydration due to excess fluid loss. (D) A, B, and C are correct. (E) Only answer B is correct.
 Diarrhea. (B) Stomach cramps. (C) Dehydration due to excess fluid loss. (D) A, B, and C are correct. (E) Only answer B is correct.") Human Anatomy - Problem Drill 21: The Digestive System Question No. 1 of 10 1. A 26-year-old male is treated in the emergency department for severe gastrointestinal disturbance. Which of the following
Human Anatomy - Problem Drill 21: The Digestive System Question No. 1 of 10 1. A 26-year-old male is treated in the emergency department for severe gastrointestinal disturbance. Which of the following
Development of pancreas and Small Intestine. ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama
 Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
The Digestive System Laboratory
 The Digestive System Laboratory 1 The Digestive Tract The alimentary canal is a continuous tube stretching from the mouth to the anus. Liver Gallbladder Small intestine Anus Parotid, sublingual, and submaxillary
The Digestive System Laboratory 1 The Digestive Tract The alimentary canal is a continuous tube stretching from the mouth to the anus. Liver Gallbladder Small intestine Anus Parotid, sublingual, and submaxillary
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
The stomach is formed of three parts: -
 The stomach is formed of three parts: - (a) CARDIAC STOMACH: - It receives the oesophagus through Cardiac aperture guarded by a cardiac sphincter which prevents regurgitation of food. (b) FUNDIC PART:
The stomach is formed of three parts: - (a) CARDIAC STOMACH: - It receives the oesophagus through Cardiac aperture guarded by a cardiac sphincter which prevents regurgitation of food. (b) FUNDIC PART:
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
01/26/2010 GENERAL SURGERY ABSITE ANATOMY ANATOMY. Yvonne M. Carter, MD Georgetown University Medical Center. Layers. mucosa. squamous epithelium
 GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
58 year old male complaining of 3-week history of increasing epigastric pain
 Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Gastrointestinal pathology 1. Upper GI tract
 Gastrointestinal pathology 1. Upper GI tract Tumors of The Salivary Glands Benign Malignant Pleomorphic adenoma (50%) Mucoepidermoid cc (15%) Warthin tumor (5%) Adenocarcinoma NOS (6%) Oncocytoma (2%)
Gastrointestinal pathology 1. Upper GI tract Tumors of The Salivary Glands Benign Malignant Pleomorphic adenoma (50%) Mucoepidermoid cc (15%) Warthin tumor (5%) Adenocarcinoma NOS (6%) Oncocytoma (2%)
F A M N O P R S ! D !
 A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
Manar Hajeer. Hashem Dujaily. Nasser AlDoghmi
 1 Manar Hajeer Hashem Dujaily Nasser AlDoghmi Diseases of The Esophagus Esophagus A hollow, highly distensible muscular tube. Clarification: Tube: it is the connection between epiglottis and stomach through
1 Manar Hajeer Hashem Dujaily Nasser AlDoghmi Diseases of The Esophagus Esophagus A hollow, highly distensible muscular tube. Clarification: Tube: it is the connection between epiglottis and stomach through
The Digestive System
 The Digestive System Identify the Structure and Function. Mesentery of the Large Intestine The mesentery functions to connect the visceral organs to the abdominal wall. Identify the Structure. Nasal Cavity
The Digestive System Identify the Structure and Function. Mesentery of the Large Intestine The mesentery functions to connect the visceral organs to the abdominal wall. Identify the Structure. Nasal Cavity
Alimentary Tract. Wang Lin 王琳 Department of pathology School of basic medical sciences
 Alimentary Tract Wang Lin 王琳 Department of pathology School of basic medical sciences Alimentary Tract Carcinoma Peptic ulcer Carcinoma Gastritis Peptic ulcer Carcinoma Appendicitis Anatomy of the stomach
Alimentary Tract Wang Lin 王琳 Department of pathology School of basic medical sciences Alimentary Tract Carcinoma Peptic ulcer Carcinoma Gastritis Peptic ulcer Carcinoma Appendicitis Anatomy of the stomach
Study on prevalence of neoplastic lesions of the esophagus in patients referred to health centers of Ahvaz in the years
 Available online at www.ijmrhs.com ISSN No: 29-5886 International Journal of Medical Research & Health Sciences, 26, 5, :5-54 Study on prevalence of neoplastic lesions of the esophagus in patients referred
Available online at www.ijmrhs.com ISSN No: 29-5886 International Journal of Medical Research & Health Sciences, 26, 5, :5-54 Study on prevalence of neoplastic lesions of the esophagus in patients referred
Disorders of the Stomach. 3- Pancreatic and gastric heteretopia.
 GASTROINTESTINAL TRACT Lec 5-6 TUCOM-DEP. OF PATHOLOGY CONGENITAL ANOMALIES: 1- Diaphragmatic Hernia. 2- pyloric stenosis. Disorders of the Stomach 3- Pancreatic and gastric heteretopia. Diaphragmatic
GASTROINTESTINAL TRACT Lec 5-6 TUCOM-DEP. OF PATHOLOGY CONGENITAL ANOMALIES: 1- Diaphragmatic Hernia. 2- pyloric stenosis. Disorders of the Stomach 3- Pancreatic and gastric heteretopia. Diaphragmatic