Low-Cost High Resolution Microendoscopy for the Detection of Esophageal Squamous Cell Neoplasia: An International Trial
|
|
|
- Bryce Armstrong
- 5 years ago
- Views:
Transcription
1 Low-Cost High Resolution Microendoscopy for the Detection of Esophageal Squamous Cell Neoplasia: An International Trial High Resolution Microendoscopy for ESCN Detection Marion-Anna Protano 1, Hong Xu 2, Guiqi Wang 3, Alexandros D. Polydorides 4, Sanford M. Dawsey 5, Junsheng Cui 6, Liyan Xue 7, Fan Zhang 2, Timothy Quang 8, Mark C. Pierce 9, Dongsuk Shin 8, Richard A. Schwarz 8, Manoop S. Bhutani 10, Michelle Lee 1, Neil Parikh 11, Chin Hur 12, Weiran Xu 2, Erin Moshier 13, James Godbold 13, Josephine Mitcham 1, Courtney Hudson 1, Rebecca R. Richards- Kortum 8 *, Sharmila Anandasabapathy 1* 1. Division of Gastroenterology, The Mount Sinai Medical Center, New York, NY 2. Department of Endoscopy, The First Hospital of Jilin University, Changchun, Jilin, China 3. Department of Endoscopy, Cancer Institute and Hospital, The Chinese Academy of Medical Sciences, Beijing, China 4. Department of Pathology, The Mount Sinai Medical Center, New York, NY 5. Division of Cancer Epidemiology and Genetics, National Cancer Institute, Bethesda, MD 6. Department of Pathology, The First Hospital of Jilin University, Changchun, Jilin, China 7. Department of Pathology, Cancer Institute and Hospital, The Chinese Academy of Medical Sciences, Beijing, China 8. Department of Bioengineering, Rice University, Houston, TX 9. Biomedical Engineering, Rutgers University, Piscataway, NJ 10. Department of Gastroenterology, Hepatology and Nutrition, The University of Texas MD Anderson Cancer Center, Houston, TX 11. Division of Digestive Diseases, Yale University, New Haven, CT 12. GI Unit & Institute for Technology Assessment, Massachusetts General Hospital, Boston, MA 13. Department of Preventative Medicine, The Mount Sinai Medical Center, New York, NY, * These authors contributed equally to the work. Grant support: This work was supported by the grants NCI R21 CA and ClinicalTrials.gov, Number NCT Abbreviations: Esophageal sqaumous cell neoplasia (ESCN); high resolution microendocsopy (HRME); Lugol s chromoendoscopy (LCE); high-definition white light endoscopy (HD-WLE); confocal laser endomicroscopy (CLE) Corresponding Author: Sharmila Anandasabapathy, MD Professor of Medicine and Gastroenterology Baylor Global Initiatives One Baylor Plaza 1
2 Houston, TX Telephone: Fax: Disclosures: Richard A. Schwarz holds a patent related to optical diagnostic technologies that have been licensed to Remicalm LLC. Chin Hur has a financial relationship outside the submitted work with Gilead Pharmaceuticals. The remaining authors declare no conflict of interest. ABSTRACT: Background and Aims: Esophageal squamous cell neoplasia (ESCN) has high mortality due to late detection. In high risk regions such as China, screening is performed by Lugol s chromoendoscopy (LCE). LCE has low specificity resulting in unnecessary tissue biopsy with subsequent increase in procedure cost and risk. The purpose of this study is to evaluate the accuracy of a novel, low-cost high resolution microendoscope (HRME) as an adjunct to LCE. Methods: In this prospective trial, 147 consecutive high-risk patients were enrolled from two US and two Chinese tertiary centers. Three expert and four novice endoscopists performed white light endoscopy followed by LCE and HRME. All optical images were compared to gold standard of histopathology. Results: Using a per biopsy analysis, sensitivity of LCE vs. LCE + HRME was 96% vs. 91% (p=0.0832), specificity 48% vs. 88% (p<0.001), PPV 22% vs 45% (p<0.0001), NPV 98% vs. 98% (p=0.3551), and overall accuracy 57% vs. 90% (p<0.001). Using a per patient analysis, sensitivity of LCE vs. LCE + HRME was 100% vs. 95% (p=0.16), specificity 29% vs. 79% (p<0.001), PPV 32% vs. 60%, 100% vs. 98%, and accuracy 47% vs. 83% (p<0.001). With use of HRME, 136 biopsies (60%; 95% CI: 53-66%) could have been spared, and 55 patients (48%; 95% CI: 38-57%) spared any biopsy. Conclusion: In this trial, HRME improved the accuracy of LCE for ESCN screening and surveillance. HRME may be a cost-effective optical biopsy adjunct to LCE, potentially reducing unnecessary biopsy and facilitating real-time decision-making in globally underserved regions; ClinicalTrials.gov, NCT Keywords: Esophageal neoplasm; endoscopy; early detection of cancer 2
3 INTRODUCTION Esophageal squamous cell neoplasia (ESCN) is the sixth leading cause of cancer death worldwide with only one in five patients surviving more than three years because of diagnosis at an advanced stage. 1,2,3 In the developing world, ESCN is more common than adenocarcinoma, with particularly high prevalence in northern China, Central Asia, and Iran. 4 In northern China, age-standardized incidence rates exceed 100 per 100,000 per year, compared to the US which is about 1.4 per 100,000. 4,5 This geographic variation likely stems from a multitude of factors including low socioeconomic status, diet, nutritional deficiencies, and thermal injury. 3 In high-risk regions, endoscopic screening has been implemented, albeit inconsistently and with limited success. The reasons for these shortcomings are multifactorial and include lack of funding, infrastructure and trained personnel. 6 Given these constraints, a low-cost, portable and accurate method of diagnosing ESCN would be invaluable in improving early detection in resource-limited settings. Early diagnosis of ESCN offers significant opportunity to improve outcomes. When detected at an early stage (severe dysplasia or intramucosal carcinoma), endoscopic treatment can be performed by endoscopic mucosal resection or radiofrequency ablation with dramatically improved morbidity and survival rates of >90%. 7,8,9,10 Unfortunately, intramucosal neoplasia can appear as small erosions, flat mucosal lesions, or normal mucosa making it difficult to visualize on routine high-definition white light endoscopy (HD-WLE) even for advanced 3
4 endoscopists. 11 Currently, endoscopic screening and surveillance is performed in high-risk patients using Lugol s chromoendoscopy (LCE). 12,13,14 Although LCE increases the sensitivity of HD-WLE to > 95%, specificity remains poor (< 65%) as inflammation and benign mucosal changes mimic neoplasia, resulting in unnecessary biopsies (LCE positive, pathology negative) and increased cost. 15,16 Repeat procedures are always necessary after LCE if treatment is warranted, therefore increasing time and cost, as well as possible patient loss to follow up. Advanced endoscopic imaging solutions have been developed but widespread dissemination has been limited by high cost or limited accuracy. Confocal laser endomicroscopy (CLE) provides 1100x magnified, subcellular views of the esophageal epithelium and can differentiate ESCN from benign esophageal mucosa with high diagnostic accuracy (>95%). 17,18,19 Current CLE platforms are expensive (>$150,000) and available in only a few tertiary care centers worldwide. 17,18 Narrow band imaging, an image-enhancement technology, uses narrow bandwidth filters of different wavelengths to visualize the microvasculature including intrapapillary capillary loop patterns. Despite a high 20,21, 22, accuracy as high as 95%, similar to LCE, NBI is limited by poor specificity. 23,24 Additionally, NBI is operator dependent, with experienced endoscopists outperforming novice (for example, sensitivity of 100% for experienced endoscopists vs 53% for novice in one study on a per-lesion basis). 23 4
5 To address these issues, we developed a novel, low cost (< $3,500), portable, battery-operated, high-resolution microendoscope (HRME) that provides subcellular resolution images when used with a topical fluorescent agent. 25,26,27,28,29,30,31 When inserted through the endoscope s accessory channel and placed in gentle contact with the mucosa, the one millimeter fiber-optic microendoscope provides clear delineation of cellular features, including nuclear size, crowding, and pleomorphism. Nuclear size can be quantified using image analysis software, assisting the endoscopist to rapidly differentiate benign epithelium from neoplasia in real-time (Figure 1). The aims of this international, multicenter trial were to evaluate the accuracy and efficiency of this novel approach in the hands of both expert and novice endoscopists performing ESCN screening and surveillance. Specifically we compared (1) the performance characteristics of LCE vs. LCE + HRME in the hands of both expert and novice microendoscopists and (2) the number of LCE positive biopsies saved and patients saved any biopsy with use of HRME. Our goal is to see if HRME can enhance the current gold standard of LCE by increasing specificity and decreasing unnecessary biopsies. METHODS Study design and patient selection This prospective, single-arm study was approved by the Institutional Review Boards at the Icahn School of Medicine at Mount Sinai, New York, NY (GCO# 5
6 /GCO# ); Rice University, Houston, TX ; MD Anderson Cancer Center, Houston, TX ( ); First University Hospital, Changchun, China; and Cancer Institute and Hospital, the Chinese Academy of Medical Sciences (CICAMS), Beijing, China. The two Chinese sites are both areas of high incidence of ESCN. One hundred and forty-seven consecutive patients previously scheduled for upper endoscopy with LCE were enrolled. Screening subjects were from high-risk provinces (northern China) or had a history of oropharyngeal cancer (United States). Surveillance subjects had a history of esophageal dysplasia or suspected, unlocalized neoplasia (China and United States). All subjects were 18 years of age and required to sign informed consent and complete a follow-up telephone interview 2-5 days post-procedure. Study exclusion criteria were known cancer >2 cm (a clinical scenario in which there would have been no role for endoscopic therapy and microendoscopy would not have changed management), allergy to the fluorescent agent proflavine, active gastrointestinal bleeding, and contraindication to endoscopy (patients who could not undergo endoscopy or sedation for standard medical reasons, such as early pregnancy or significant cardiopulmonary disease/hemodynamic instability, or those who could not undergo biopsies, such as presence of varices). High resolution microendoscopy (HRME) HRME methodology has been described previously. 25,26, 30 Briefly, the HRME is a battery-powered, portable, fluorescence microscope, with a one millimeter 6
7 diameter flexible fiber-optic probe. The commercially available fiber-bundle probe (Sumitomo, Fujikura, and Schott) contains 30,000 optical fibers with approximately 4 µm core spacing and imaging diameters of 330 µm, 720 µm, and 1400 µm and is inserted through the endoscopic biopsy channel. When placed in gentle contact with mucosa, histopathologic-like images are obtained in real time, at a subcellular resolution. Excitation light from a 455 nm light-emitting diode is delivered through the fiber bundle. The fluorescent emission from proflavine (with peak absorption and emission wavelengths of 455 nm and 515 nm, respectively) is collected through the fiber bundle and imaged onto a digital camera. The probe provides a 720 µm diameter field of view and 4.5 µm spatial resolution. It can be disinfected by soaking in glutaraldehyde solution and can be used times before the probe s fiber surface needs repolishing. Repolishing takes approximately minutes and can be done repeatedly without affecting probe performance or longevity. Image analysis interpretation software To facilitate objective, real-time interpretation, image analysis software was used to identify morphologic features that could classify HRME images as neoplastic (high grade dysplasia, cancer) or benign. A two-class linear discriminant algorithm was developed and evaluated using 375 images of esophageal tissue obtained in a pilot trial. 31 The diagnostic value of the following features were analyzed: nuclear size, nuclear-to-cytoplasmic ratio, nearest internuclear distance, nuclear eccentricity, nuclear solidity, and the major axis of the ellipse 7
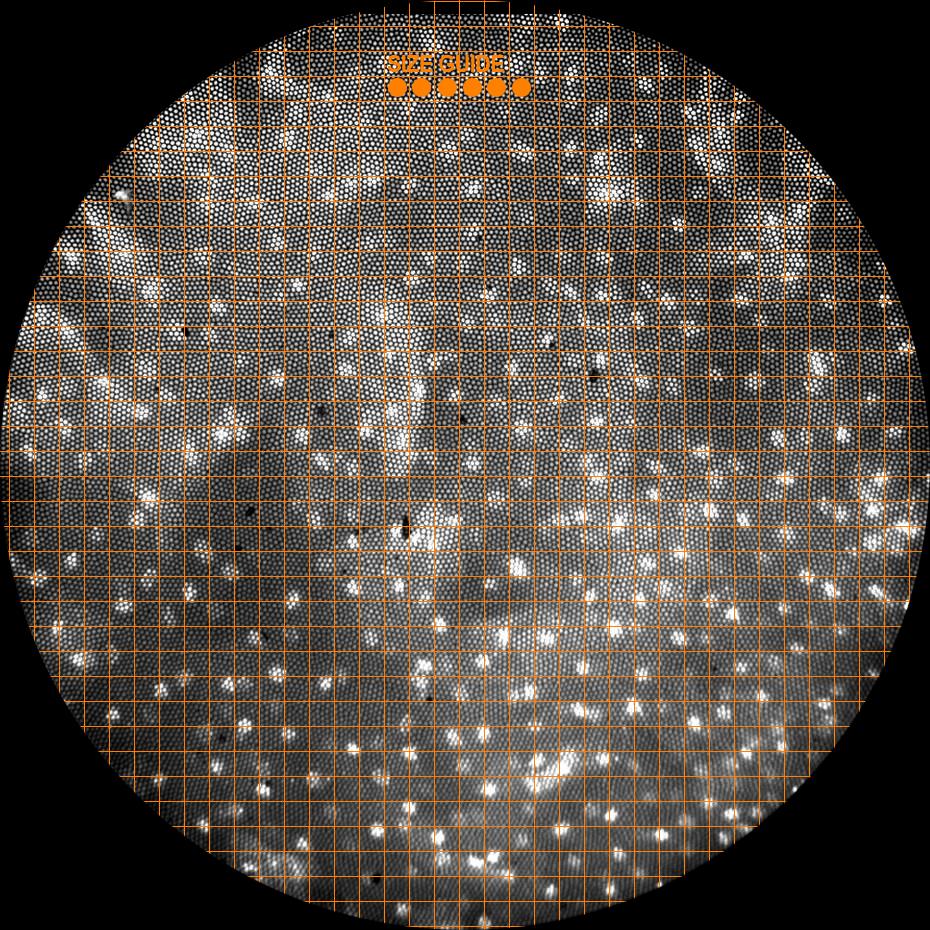
8 best approximating each nucleus. The single best performing feature for differentiating neoplastic from non-neoplastic tissue was mean nuclear area, with neoplastic samples showing mean nuclear area greater than 15.1 µm. 31 Based on these findings, we developed tools to assist endoscopists performing HRME imaging with objective, real-time visual assessment of nuclear size and spacing throughout the trial. HRME images were displayed in real time with two visual assists superimposed: 1) 15.1 µm dots were placed on the top of each image frame and 2) a grid with 19.4 µm spacing was overlaid on each image frame to aid endoscopists in identifying whether the majority of nuclei in the image exceeded the 15.1 um diameter threshold. Training in the interpretation of HRME for ESCN Seven endoscopists (three experienced, four novice) performed HD-WLE with LCE (the current gold standard for screening) followed by HRME. Experienced endoscopists had performed >50 microendoscopy exams and novice endoscopists had no prior experience using HRME. Prior to patient enrollment, all seven endoscopists viewed a training slideshow describing the various features of the HRME ESCN classification system, 32 including still HRME images and six HRME videos. Endoscopists were instructed to classify tissue as neoplastic if the majority of nuclei in the image exceeded the 15.1 um reference marker. After viewing the training set, each endoscopist was shown a test set of 40 new HRME movies. Endoscopists were blinded to the HD-WLE and LCE 8
9 images and histopathology. An accuracy of 80% on this initial test was achieved by each endoscopist prior to trial participation and patient enrollment. Performing endoscopy with HRME HD-WLE using LCE dye-stain (12 g iodine + 24 g potassium iodide in 1000 ml water) was performed with an Olympus 180 endoscope, using only the white light mode, in each patient. Per standard of care, LCE voiding lesions were identified and targeted for one to two biopsies based on size. LCE voiding lesions ranged in size from 2 mm to 2 cm (less than 2 mm lesions are typically not biopsied). While LCE voiding (abnormal) areas were targeted for imaging and biopsy, it should be noted that residual LCE dye did not interfere with HRME imaging quality, in part due to the bright fluorescence of the proflavine dye. Prior to biopsy of each LCE voiding lesion, HRME imaging was performed of the entire lesion. For HRME imaging, an average of 4.77 ml (1-10 ml) topical proflavine hemisulfate 0.01% (w/v) was sprayed on each LCE-voiding area (total amount was based on size/number of LCE lesions). Proflavine was used under an Investigational New Drug (IND) application from the Food and Drug Administration (IND #102,217). After proflavine application, the HRME probe was inserted through the endoscope biopsy channel and placed on mucosa to evaluate each targeted area (< 30 seconds). For each optical site, digital videos were acquired at 12 frames per second for a total of three seconds and recorded using a foot pedal controlled by the endoscopist. Thus, a typical 5-7 mm LCEvoiding area was imaged with 5-7 still images. At each imaged site, the 9
10 endoscopist s impression (neoplastic, non-neoplastic) was recorded during the procedure for each modality (LCE, HRME), which was used to determine the performance characteristics of HRME (Figure 2). To ensure accurate biopsy correlation, all imaged areas prior to biopsy were marked with a dimple created by pressing the probe against the mucosa. This target was used for biopsy correlation. The entire HRME process added an additional four to six minutes to the standard endoscopic evaluation. To determine both the device and LCE s performance characteristics and sensitivity, 25% of the total biopsies obtained were from LCEavid (normal) areas. All specimens were processed and sectioned both transversely and longitudinally in a standardized manner. Reference Standard Pathology All slides received a local site (standard of care) pathology diagnosis in addition to a centralized diagnosis by a single, expert gastrointestinal pathologist (AP), who was blinded to the endoscopic, HRME, and local pathology results. For the purposes of this study, the final diagnosis was a binary classification of either non-neoplasia (normal, inflammation, low-grade dysplasia) or neoplasia (highgrade dysplasia, ESCN). 33 Moderate dysplasia was re-classified as low-grade or high-grade dysplasia depending on whether architectural and cytological abnormalities were confined to the lower half of the squamous epithelium or also involved the upper half. The classification used was consistent with other studies 10
11 in ESCN with high grade dysplasia and neoplasia as a primary end point since they are more clinically relevant and a threshold for actionable diagnosis. 20,21,22,23,24 Discrepant diagnoses were reviewed in tandem by two pathologists (AP, SD) for a consensus diagnosis. Statistical analysis Sample size calculations to provide adequate power were done for the primary outcome of specificity. In particular, a sample size of n = 120 patients with no evidence of biopsy-confirmed neoplasia would provide 88% power to detect a difference in specificities of 63% for LCE and of 75% for LCE + HRME. This calculation is based on a comparison of paired samples; in this study the pairing occurs as a result of each subject receiving an examination by each of the two modalities. 34 The overall recruitment goal was based on an estimate that approximately one-third of all subjects with a history of neoplasia would have at least one positive biopsy. nquery Advisor v7.0 was used for this calculation. The parameters of sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for each method with the patient as unit of observation (per patient analyses) were estimated using observed proportions; the corresponding 95% confidence intervals are exact binomial intervals. 35 The comparison of each of these parameters estimated using the standard method (LCE) to the same parameter estimated using the new proposed method (LCE + HRME) was carried out using a log-binomial model that took into account the 11
12 correlations that arose when the same patient was assessed by each of the two methods. 36 Comparison of these parameters between novice and expert endoscopists was done also using a log-binomial model. For the per biopsy analyses, log-binomial models were used to account for the correlations that arose from there being multiple specimens from the same patient as well as correlations that arose from using both methods on the same patient. These models produced estimates of the relevant parameters, the associated confidence intervals, and p-values. To test whether the number of biopsies required (or number of patients requiring a biopsy) using LCE + HRME results could have been significantly reduced below the number required based on LCE alone, a chi-square test was performed on the binomial proportion defined by the number of biopsies (or, patients with biopsy) classified as positive by LCE but negative by HRME divided by the total number of biopsies (patients with biopsy) performed. This chi-square test tested the null hypothesis that the above proportion was zero, which would be the case if HRME provided no useful information to eliminate false positive LCE readings. All authors had access to the study data and reviewed and approved the final manuscript. RESULTS Patient characteristics 12
13 From August 2010 to August 2013, a total of 147 patients were enrolled: thirty from Mount Sinai, 7 from MD Anderson, 31 from First University Hospital, and 79 from CICAMS. The prevalence of neoplasia at each site (neoplasia positive patients/total number of patients) was 43% in the US and 19% in China. This difference was likely due to the fact that more of the US patients were in surveillance, whereas routine screening was done in those provinces of China. In the US, one experienced and one novice microendoscopist scoped 37 patients. In China, two experienced and 3 novice microendoscopists scoped 110 patients. Of the 147 patients, 87 (59%) were male, 112 (76%) were Chinese, 26 (18%) were Caucasian. Median age was 60 (range 30-81), and the indication for the procedure was initial screening in 42 (29%) and surveillance in 105 (71%). In the screening group, 2% patients had neoplasia compared to 34% in the surveillance group. Endoscopic characteristics are shown in Table 1. Nodularity and ulcers were all less than 2 centimeters, and no obvious localized carcinoma was included. Of note, there were no complications or side effectives from proflavine. Performance Characteristics Per Biopsy Analysis: A total of 386 biopsies were taken from 147 patients. There were 159 biopsies taken for the false negative rate. Sensitivity of LCE compared to LCE + HRME was 96% vs. 91% (p=0.0832), specificity 48% vs. 88% (p<0.001), PPV 22% vs. 45% (p<0.0001), NPV 98% vs. 98% (p=0.3551), and overall accuracy 57% vs. 90% (p<0.001). This data and accompanying 13
14 confidence intervals are shown in Table 2. Thus, the addition of HRME significantly increased the specificity and overall accuracy of LCE. Per Patient Analysis: For each patient, there was a range of zero to six LCE voiding lesions. Sensitivity of LCE compared to LCE + HRME was 100% vs. 95% (p=0.16), specificity 29% vs. 79% (p<0.001), PPV 32% vs. 60%, NPV 100% vs. 98%, and accuracy 47% vs. 83% (p<0.001) (Table 2). On a per patient basis, there was a statistically significant improvement in specificity and overall accuracy without significant change in sensitivity. First University Hospital had 5 patients that were HRME positive, pathology positive; Mount Sinai had 16; MD Anderson had zero; and CICAMS had 14. Biopsies Saved: There were a total of 227 LCE positive biopsies and only 88 LCE + HRME positive biopsies; thus, 139 biopsies could have been spared (61%; 95% CI: 55-68%) with use of HRME (Figure 3). Only 3 biopsies (1%; 95% CI 0.3-4%) would have been spared in error (negative on HRME, positive on pathology). There were a total of 115 LCE positive patients and only 58 LCE + HRME positive patients; thus, 57 patients could have been spared (50%; 95% CI: 40-59%) with use of HRME (Figure 3). Only 2 patients (2%; 95% CI 0.2-6%) would have been spared in error (negative on HRME, positive on pathology). The addition of HRME to LCE would have theoretically decreased the average number of biopsies obtained per patient (2.63 LCE vs LCE + HRME) by allowing targeted tissue sampling. 14
15 Novice vs. experienced endoscopists: biopsy and patient based analysis Using a per biopsy analysis, accuracy of LCE + HRME for novice vs. experienced endoscopists was 88% vs. 90%, with comparable sensitivity 89% vs. 92%, specificity 87% vs. 89%, PPV 44% vs. 67%, and NPV 99% vs. 98%. Using a per patient analysis, accuracy of LCE + HRME for the novice vs. experienced endoscopists was 79% vs. 89%, sensitivity 88% vs. 100%, specificity 77% vs. 83%, PPV 47% vs. 75%, and NPV 96% vs. 100% (Table 3). There was no significant difference between novice and experts in accuracy, sensitivity, specificity or NPV. DISCUSSION With global cancer rates rising, there is an increasing need for robust, costeffective diagnostic technology that can be used in low-resource areas by less experienced clinical providers. Given the cost and performance limitation of currently available techniques, an accurate, easily interpretable imaging modality for diagnosing ESCN in real-time would be invaluable. Such a technology could reduce the number of unnecessary biopsies, enable immediate endoscopic therapy of neoplasia, and decrease repeat procedures and loss of patients to follow up. This is the first prospective, in vivo study assessing the accuracy and biopsy efficiency of the low-cost HRME as an adjunct to Lugol s screening for ESCN. Indeed, the role of such an optical biopsy technology is to complement and 15
16 enhance red-flag imaging (LCE) by improving accuracy and efficiency. In this international, multi-center trial, HRME imaging significantly improved specificity and accuracy of the LCE gold-standard. On a per biopsy basis, specificity and accuracy improved from 48% to 88% and 57% to 90%, respectively. On a per patient basis, specificity and accuracy improved from 29% to 79% and 47% to 83%, respectively, without a statistically significant reduction in sensitivity. In this study, we enrolled consecutive subjects undergoing screening or surveillance and those in the surveillance had a prior history of dysplasia (low grade, moderate dysplasia) or suspected, unlocalized neoplasia (high grade or cancer) with nodules < 2 cm in size. We did not include subjects with lesions > 2 cm where there would have been no role for endoscopic therapy and where the HRME would not have had a clinical impact (i.e.: larger and localized cancers). Of all the indeterminate and smaller lesions (ulcers and nodules < 2 cm) that were imaged with the HRME, 42% were neoplastic and 58% were benign (inflammation, esophagitis, etc.). Thus, there clearly was still a role for the HRME in making a diagnosis in these indeterminate lesions. This trial demonstrates that the use of HRME, in conjunction with LCE, can accurately differentiate neoplasia. Fifty-five patients would have been saved any biopsy (48%) and 136 biopsies (60%) taken with LCE could have been prevented with addition of HRME. Given that pathology costs frequently exceed endoscopy costs, this reduction in tissue sampling may offer a significant cost-saving advantage as well as prevent delays in diagnosis and treatment. 16
17 Interestingly, there was no significant difference in accuracy between novice and experienced endoscopists (90% vs. 88%) in the per biopsy analysis. The ability of novice endoscopists to effectively learn HRME is a significant advantage over current CLE imaging, which has shown considerably lower accuracy in the hands of novice (84%) vs. experienced (96%) endoscopists in Barrett s esophagus, as there are no formal studies evaluated ESCC. 37 Over half of the procedures in our study were performed in rural hospitals in northern China by endoscopists with no prior microendoscopy experience. This is significantly different from most CLE trials, which have been performed in tertiary centers, and from most NBI trials, which have shown a significant difference in the performance of novice and experienced endoscopists, due to the significant learning curve associated with the interpretation of specific vascular and mucosal changes. 23 CLE relies on interpretation of complex glandular, cellular and vascular patterns which may result in a steeper learning curve. 38 It is likely that the use of objective, quantifiable image-analysis criteria and software size guides accounted for the rapid learning curve and consistent performance of all endoscopists, both novice and expert There are no formal studies comparing HRME to CLE. The CLE systems are commercially available instruments with the advantage of extensive industrial design, testing, and support from established medical device companies. The HRME described in this trial is currently developed in an academic setting and not commercially available. The goal of this system is not to compete with CLE 17
18 but provide a lower-cost, portable alternative in low-resource areas with less experienced providers. The lateral resolution of HRME is only slight inferior to that of CLE (HRME: 4.4 µm, probe-based CLE: 1.0 and 3.5 µm, CLE 0.7 µm). HRME and CLE have similar frame rates (12 frames/second for both HRME and probe-based CLE, 1.2 frames/second for CLE). The field of view is slightly superior for HRME compared to CLE (HRME: 0.41 mm 3, probe-based CLE 0.05 to 0.28 mm 3, CLE 0.23 mm 3 ). Our results combining HRME and LCE are close to that of CLE for the detection of ESCN. CLE has been shown to have 95% accuracy while HRME had 90% accuracy in this trial. 17,20,22,24 While there are no guidelines for squamous neoplasia, current guidelines developed by the American Society of Gastrointestinal Endoscopy for esophageal adenocarcinoma suggest that a threshold sensitivity 90%, specificity 80%, and NPV 98% are needed for an imaging technology to replace standard biopsy protocol. 37 The only imaging modality currently meeting these benchmarks is CLE. 37 Our results reveal sensitivity, specificity and NPV of 95%, 79%, and 98% (per patient). Again, while there are no such guidelines for ESCN, these results are promising. Our study has several strengths. It was performed prospectively, in real-time in low- and high-resource clinical settings by both novice and experienced endoscopists. Pathologic interpretation was standardized by the use of a single, expert gastrointestinal pathologist. Because the HRME device is affordable, 18
19 portable and battery-powered, it was easily used in both low- and high-resource settings, suggesting the potential for it to be implemented successfully in lowresource settings. Additionally, the use of a simple software overlay to assist in visual interpretation of HRME images by providing a semi-quantitative assessment of nuclear size increases the likelihood of successful technology dissemination, aiding less experienced clinicians. Several limitation exist as well. First, HRME is, at present, not commercially available and proflavine is an investigational drug. Secondly, there were three lesions that were positive on LCE that were incorrectly interpreted as negative on HRME, which accounts for the slightly lower sensitivity of HRME. Two of these biopsies had focal dysplasia and one was originally moderate dysplasia. In the focal dysplasia, there was one small area of moderate dysplasia in low grade dysplasia. In moderate dysplasia, surface changes are not pronounced requiring deeper imaging to differentiate moderate from low grade dysplasia. HRME only images superficially (10 µm), 39 and the deeper epithelial changes will not be appreciated. This is a limitation of the technology, which may explain the false negative interpretation. Additionally, larger lesions will take longer to image with HRME (approximately 2-3 minutes additional) which may be more laborious. As mentioned previously, our group is developing a new mosaicking software to stitch these images together of larger surface area in a smoother fashion. This will enhance the ease and accuracy of imaging by allowing larger areas to be scanned more quickly. 19
20 Lastly, our study did not blind endoscopists to the LCE s read. This, however, was done by design as HRME is meant to be used in a complementary role to Lugol s. Indeed, the HRME is meant as a second-pass, confirmatory technology, not a red-flag screening modality. The ultimate goal of such a device is to reduce biopsy costs and facilitate real-time decision making (biopsy, no biopsy, or treat neoplasia immediately). In summary, this prospective, international trial demonstrates that the accuracy of HRME imaging is comparable to other advanced, more costly imaging modalities such as CLE. The use of HRME as an adjunct to LCE may decrease the number of biopsies and provide the opportunity to diagnose and treat ESCN in a single session. This may reduce cost, decrease loss of follow up, and prevent delays in diagnosis and treatment. A formal cost-effectiveness analysis and a randomized trial is planned to validate these findings. Figure Legends Figure 1. (A) Device configuration. (B) The device is battery operated and easily fits in a briefcase. (C) To facilitate objective, real-time assessment of nuclear size and spacing, a grid with 19.4 µm spacing was superimposed on the display monitor and 15.1 µm diameter dots were placed; this image is normal esophageal mucosa. 20
21 Figure 2. Lugol s unstained areas are imaged with HRME and an optical biopsy is obtained with the corresponding tissue biopsy (original magnification 100x) of the area. Only one of the two Lugol s abnormal areas was neoplastic (upper panel). REFERENCES 1. Umar SB, Fleischer DE. Esophageal cancer: epidemiology, pathogenesis, and prevention. Nat Clin Pract Gastroenterol Hepatol 2008;5: Polednak AP. Trends in survival for both histologic types of esophageal cancer in US surveillance, epidemiology and end results areas. Int J Cancer 2003;105: Hongo M, Nagasaki Y, Shoji T. Epidemiology of esophageal cancer: Orient to Occident. Effects of chronology, geography, and ethnicity. J of Gastroenterol Hepatol 2009;24: Wei WQ, Abnet CC, Lu N, et al. Risk factors of oesophageal squamous dysplasia in adult inhabitants of a high-risk region of China. Gut 2005;54: Howlander N, Noone AM, Krapcho M, et al (eds). SEER Cancer Statistics Review, , National Cancer Institute. Bethesda, MD, 21
22 based on November 2013 SEER data submission, posted to SEER website, April Lin Y, Totsuka Y, He Y, et al. Epidemiology of esophageal cancer in Japan and China. J Epidemiol 2013;23: Pech O, Gossner L, May A, et al. Endoscopic resection of superficial esophageal squamous-cell carcinomas: Western experience. Am J Gastroenterol 2004;99: Katada C, Muto M, Saito D, et al. Clinical outcome after endoscopic mucosal resection for esophageal squamous cell carcinoma invading the muscularis mucosae: a multicenter, retrospective cohort study. Endoscopy 2007;39: Bergman JJ, Zhang YM, He S, et al. Outcomes from a prospective trial of endoscopic radiofrequency ablation of early squamous cell neoplasia of the esophagus. Gastrointest Endosc 2011;74: Becker V, Bajbouj M, Schmid RM, et al. Multimodal endoscopic therapy for multifocal intraepithelial neoplasia and superficial esophageal squamous cell carcinoma a case series. Endoscopy 2011;43: Sidorenko EI, Sharma P. High resolution chromoendoscopy in the esophagus. 22
23 Gastrointest Endosc Clin N Am 2004;14: Reddymasu SC, Sharma P. Advances in endoscopic imaging of the esophagus. Gastroenterol Clin N Am 2008;37: Dawsey SM, Fleischer DE, Wang GQ, et al. Mucosal iodine staining improves endoscopic visualization of squamous dysplasia and squamous cell carcinoma in Linxian, China. Cancer 1998;83: Hashimoto CL, Iriya ER, Baba, et al. Lugol s dye spray chromoendoscopy establishes early diagnosis of esophageal cancer in patients with primary head and neck cancer. Am J Gastroenterol 2005;100: Yoshida Y, Goda K, Tajiri H, et al. Assessment of novel endoscopic techniques for visualizing superficial esophageal squamous cell carcinoma: autofluorescence and narrow-band imaging. Dis Esophagus 2009;22: Freitag CPF, Barros SGS, Kruel CDP, et al. Esophageal dysplasia are detected by endoscopy with Lugol in patients at risk for squamous cell carcinoma in southern Brazil. Dis Esophagus 1999;12:
24 17. Pech O, Rabenstein T, Manner H, et al. Confocal laser endomicroscopy for in vivo diagnosis of early squamous cell carcinoma of the esophagus. Clin Gastroenterol Hepatol 2008;6: Liu H, Li QY, Yu T, et al. Confocal laser endomicroscopy for superficial esophageal squamous cell carcinoma. Endoscopy 2009;41: Deinert K, Kiesslich R, Vieth M, et al. In-vivo microvascular imaging of early squamous-cell cancer cancer of the esophagus by confocal laser microendoscopy. Endoscopy 2007;39: Muto M, Minashi K, Yano T, et al. Early detection of the superficial squamous cell carcinoma in the head and neck region and esophagus by narrow band imaging: a multicenter randomized controlled trial. J Clin Onc 2010;28: Ide E, Carneiro FO, Frazao MS, et al. Endoscopic detection of early esophageal squamous cell carcinoma in patients with achalasia: narrow-band imaging versus Lugol s staining [published online ahead of print July 9, 2013]. J Oncol 2013;doi:1155.nm Ide E, Maluf-Filho F, Chaves DM, et al. Narrow-band imaging without magnification for detecting early esophageal squamous cell carcinoma. World J Gastroenterol 2011;17:
25 23. Ishihara R, Takeuchi Y, Chatani R, et al. Prospective evaluation of narrowband imaging endoscopy for screening of esophageal squamous mucosal highgrade neoplasia in experienced and less experienced endoscopists. Dis Esophagus 2010;23: Takenaka R, Kawahara Y, Okada H, et al. Narrow-band imaging provides reliable screening for esophageal malignancy in patients with head and neck cancers. Am J Gastroenterol 2009;104: Pierce M, Dihua Y, Richards-Kortum R. High-resolution fiber-optic microendoscopy for in situ cellular imaging. J Vis Exp 2011;47: Muldoon TJ, Pierce MC, Nida DL, et al. Subcellular-resolution molecular imaging within living tissue by fiber microendoscopy. Opt Express 2007;15: Muldoon TJ, Anandasabapathy S, Maru D, et al. High-resolution imaging in Barrett s esophagus: a novel, low-cost endoscopic microscope. Gastrointest Endosc 2008;68:
26 28. Muldoon TJ, Thekkek N, Roblyer D, et al. Evaluation of quantitative image analysis criteria for the high-resolution detection of neoplasia in Barrett s esophagus. J Biomed Opt 2010;15: Vila PM, Polydorides AD, Protano MA, et al. Accuracy and inter-rater reliability for the diagnosis of Barrett's neoplasia among new and experienced users of a novel, low-cost, portable microendoscope. In Gastroenterology, presented at Digestive Disease Week;May 7-11, 2011;Chicago, Illinois. 30. Pierce MC, Vila PM, Polydorides AD, et al. Low-Cost endomicroscopy in the esophagus and colon. Am J Gastroenterol 2011;106: Shin D, Protano MA, Polydorides AD, et al. Quantitative analysis of highresolution microendoscopic images for diagnosis of esophageal squamous cell carcinoma. [published online ahead of print July 25, 2014]. Clin Gastroenterol Hepatol 2014;doi: Protano MA, Xu H, Zhang F, et al. Low-cost microendoscopy for the diagnosis of esophageal squamous cell neoplasia in northern China: an evaluation of interobserver agreement and accuracy. In Gastroenterology, presented at Digestive Disease Week;May 7-11, 2011;Chicago, Illinois. 26
27 33. Bosman FT, Carneiro F, Hruban RH, et al. World Health Organization Classification of Tumours of the Digestive System. 4 th ed. Lyon, France: World Health Organization; Miettinen OS. On the matched-pairs design in the case of all-or-none responses. Biometrics 1986;24: Blyth CR, Still HA. Binomial confidence intervals. Journal of the Am Stat Assoc 1983;78: Spiegelman D, Hertzmark E. Easy SAS calculations for risk or prevalence ratios and differences. Am J Epidemiol 2005;162: Canto MI, Anandasabapathy S, Brugge W, et al. In vivo endomicroscopy improves detection of Barrett s esophagus-related neoplasia: a multicenter international randomized controlled trial. Gastrointest Endosc 2014;79: Iguchi Y, Niwa Y, Miyahara R. Pilot study on confocal endomicroscopy for diagnosis of the depth of squamous cell esophageal cancer in vivo. J Gatroenterol Hepatol 2009;24: Koucky MH, Pierce MC. Axial response of high-resolution microendscopy in scattering media. Biomed Opt Express 2013;4:
28 Authors names in bold designate shared co-first authors. Table 1. Clinical features of patients Age, median years (range) 60 (31-80) Gender, n (%) Male 87 (59%) Female 60 (41%) Ethnicity, n (%) Caucasian 26 (18%) Chinese 112 (76%) African American 3 (2%) Hispanic 6 (4%) Indication for procedure, n (%) Screening 42 (29%) Surveillance 105 (71%) Macroscopic appearance, n (%) Nodularity 11 (7%) Ulceration 7 (5%) Neither 128 (87%) Both 1 (1%) Sites, n (%) First University 31 (21%) Mount Sinai 30 (20%) MD Anderson 7 (5%) CICAMS 79 (54%) Table 2. Per biopsy and per patient analysis of LCE versus LCE + HRME Per Biopsy Analysis Per Patient Analysis n=386 biopsies n=147 patients LCE LCE + HRME LCE LCE + HRME Sensitivity 97% [90-100] 90% [81-99] 100%[91-100] 95% [82-99] Specificity 48% [43-53] 88% 1 [84-92] 29% [21-39] 79% 1 [70-86] PPV 22% [16-31%] 45% 1 [33-61] 32% [24-41] 60% [47-73] NPV 98% [96-100] 97% [96-99] 100%[89-100] 98% [92-99] Accuracy 57% [52-62] 90% 1 [86-93] 47% [39-55] 83% 1 [76-89] 1 p< Table 3. Per biopsy and per patient analysis of experienced versus novice endoscopists using LCE + HRME Per Biopsy Analysis Per Patient Analysis n=386 biopsies n=147 patients Novice Experts Novice Experts Sensitivity 90% [77-100] 90% [79-100] 88% [62-98] 100%[84-100] Specificity 88% [83-94] 89% [83-95] 77% [66-86] 83% [67-93] 28
29 PPV 40% [27-58] 55% [40-77] 47% [28-66] 75% [55-89] NPV 98% [96-99] 97% [94-99] 96% [88-99] 100%[89-100] Accuracy 88% [83-94] 90% [85-95] 79% [69-87] 89% [78-95] 29


30 Figure 1. High Resolution Microendoscope (HRME). (A) (B) (C) 100 µm




31 Figure 2. Lugol s chromoendoscopy and HRME. 100 µm 100 µm

32 Figure 3. Comparison of total number of mucosal biopsies obtained and total number of patients requiring a biopsy with LCE versus LCE + HRME * * * 58* 50 0 LCE LCE+HRME LCE LCE+HRME Per Biopsy Per Pa7ent *p <0.001 Note: 3 biopsies and 2 patients would have been spared in error (HRME negative, path positive)
ABSTRACT. High Resolution Microendoscopy for Quantitative Diagnosis of Esophageal Neoplasia. Dongsuk Shin
 ii ABSTRACT High Resolution Microendoscopy for Quantitative Diagnosis of Esophageal Neoplasia by Dongsuk Shin Esophageal cancer is the eighth most common cancer in the world. Cancers of the esophagus account
ii ABSTRACT High Resolution Microendoscopy for Quantitative Diagnosis of Esophageal Neoplasia by Dongsuk Shin Esophageal cancer is the eighth most common cancer in the world. Cancers of the esophagus account
Quantitative analysis of high-resolution microendoscopic images for diagnosis of neoplasia in patients with Barrett s esophagus
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 Quantitative analysis of high-resolution microendoscopic images for diagnosis of neoplasia in patients with
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 Quantitative analysis of high-resolution microendoscopic images for diagnosis of neoplasia in patients with
Accepted Article. Parikh 1 This article is protected by copyright. All rights reserved.
 In-vivo classification of colorectal neoplasia using high-resolution microendoscopy: improvement with experience 1 Running Title: HRME for colon polyps Neil D. Parikh M.D. 1 ; Daniel Perl B.A. 2 ; Michelle
In-vivo classification of colorectal neoplasia using high-resolution microendoscopy: improvement with experience 1 Running Title: HRME for colon polyps Neil D. Parikh M.D. 1 ; Daniel Perl B.A. 2 ; Michelle
Philip Chiu Associate Professor Department of Surgery, Prince of Wales Hospital The Chinese University of Hong Kong
 Application of Chromoendoscopy, NBI and AFI in Esophagus why, who, and how? Philip Chiu Associate Professor Department of Surgery, Prince of Wales Hospital The Chinese University of Hong Kong Cancer of
Application of Chromoendoscopy, NBI and AFI in Esophagus why, who, and how? Philip Chiu Associate Professor Department of Surgery, Prince of Wales Hospital The Chinese University of Hong Kong Cancer of
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Advances in Endoscopic Imaging
 Advances in Endoscopic Imaging SGNA meeting February 20, 2010 Amar R. Deshpande, MD Asst Professor of Medicine Division of Gastroenterology University of Miami Miller School of Medicine Objectives To recognize
Advances in Endoscopic Imaging SGNA meeting February 20, 2010 Amar R. Deshpande, MD Asst Professor of Medicine Division of Gastroenterology University of Miami Miller School of Medicine Objectives To recognize
Discrimination of Benign and Neoplastic Mucosa with a High- Resolution Microendoscope
 Page 1 of 21 Discrimination of Benign and Neoplastic Mucosa with a High- Resolution Microendoscope (HRME) in Head and Neck Cancer Peter M. Vila, MSPH 1, Chan W. Park, MD 1, Mark C. Pierce, PhD 2, Gregg
Page 1 of 21 Discrimination of Benign and Neoplastic Mucosa with a High- Resolution Microendoscope (HRME) in Head and Neck Cancer Peter M. Vila, MSPH 1, Chan W. Park, MD 1, Mark C. Pierce, PhD 2, Gregg
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Gastrointestinal Imaging
 Endoscopic Imaging of Gastroesophageal Reflux Disease Kerry B Dunbar, MD Assistant Professor of Medicine, Division of Gastroenterology and Hepatology, Johns Hopkins University School of Medicine Abstract
Endoscopic Imaging of Gastroesophageal Reflux Disease Kerry B Dunbar, MD Assistant Professor of Medicine, Division of Gastroenterology and Hepatology, Johns Hopkins University School of Medicine Abstract
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis
 Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Research Article High-Resolution Optical Imaging of Benign and Malignant Mucosa in the Upper Aerodigestive Tract: An Atlas for Image-Guided Surgery
 International Scholarly Research Network ISRN Minimally Invasive Surgery Volume 2012, Article ID 364285, 9 pages doi:10.5402/2012/364285 Research Article High-Resolution Optical Imaging of Benign and Malignant
International Scholarly Research Network ISRN Minimally Invasive Surgery Volume 2012, Article ID 364285, 9 pages doi:10.5402/2012/364285 Research Article High-Resolution Optical Imaging of Benign and Malignant
Confocal Laser Endomicroscopy
 Confocal Laser Endomicroscopy Policy Number: 2.01.87 Last Review: 3/2018 Origination: 3/2013 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for
Confocal Laser Endomicroscopy Policy Number: 2.01.87 Last Review: 3/2018 Origination: 3/2013 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for
Chromoendoscopy as an Adjunct to Colonoscopy
 Chromoendoscopy as an Adjunct to Colonoscopy Policy Number: 2.01.84 Last Review: 1/2018 Origination: 7/2017 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide
Chromoendoscopy as an Adjunct to Colonoscopy Policy Number: 2.01.84 Last Review: 1/2018 Origination: 7/2017 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett s esophagus
 E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
University Mainz. Early Gastric Cancer. Ralf Kiesslich. Johannes Gutenberg University Mainz, Germany. Early Gastric Cancer 15.6.
 Ralf Kiesslich Johannes Gutenberg University Mainz, Germany DIAGNOSIS Unmask lesions - Chromoendoscopy -NBI Red flag technology - Autofluorescence Surface and detail analysis - Magnifying endoscopy - High
Ralf Kiesslich Johannes Gutenberg University Mainz, Germany DIAGNOSIS Unmask lesions - Chromoendoscopy -NBI Red flag technology - Autofluorescence Surface and detail analysis - Magnifying endoscopy - High
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Vital staining and Barrett s esophagus
 Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
LARYNGEAL DYSPLASIA. Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital
 LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
BENEFIT APPLICATION BLUE CARD/NATIONAL ACCOUNT ISSUES
 Medical Policy BCBSA Ref. Policy: 2.01.84 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/Computed
Medical Policy BCBSA Ref. Policy: 2.01.84 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/Computed
High-resolution imaging in Barrett s esophagus: a novel, low-cost endoscopic microscope
 NEW METHODS: Clinical Endoscopy High-resolution imaging in Barrett s esophagus: a novel, low-cost endoscopic microscope Timothy J. Muldoon, BS, Sharmila Anandasabapathy, MD, Dipen Maru, MD, Rebecca Richards-Kortum,
NEW METHODS: Clinical Endoscopy High-resolution imaging in Barrett s esophagus: a novel, low-cost endoscopic microscope Timothy J. Muldoon, BS, Sharmila Anandasabapathy, MD, Dipen Maru, MD, Rebecca Richards-Kortum,
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Medical Policy. MP Confocal Laser Endomicroscopy
 Medical Policy BCBSA Ref. Policy: 2.01.87 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.80 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
Medical Policy BCBSA Ref. Policy: 2.01.87 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.80 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
Comparison of the Diagnostic Usefulness of Conventional Magnification and Near-focus Methods with Narrow-band Imaging for Gastric Epithelial Tumors
 ORIGINAL ARTICLE ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2015.15.1.39 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2015;15(1):39-43 Comparison of the Diagnostic Usefulness
ORIGINAL ARTICLE ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2015.15.1.39 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2015;15(1):39-43 Comparison of the Diagnostic Usefulness
Optical Molecular Imaging in the Gastrointestinal Tract. * corresponding author after publication. # corresponding author for proofs
 Optical Molecular Imaging in the Gastrointestinal Tract Jennifer Carns 1a#, PhD, Pelham Keahey 1b, BS, Timothy Quang 1c, BS, Sharmila Anandasabapathy 2d, MD, Rebecca Richards-Kortum 1e*, PhD * corresponding
Optical Molecular Imaging in the Gastrointestinal Tract Jennifer Carns 1a#, PhD, Pelham Keahey 1b, BS, Timothy Quang 1c, BS, Sharmila Anandasabapathy 2d, MD, Rebecca Richards-Kortum 1e*, PhD * corresponding
Use of In Vivo Real-Time Optical Imaging for Esophageal Neoplasia
 MOUNT SINI JOURNL OF MEDICINE 78:894 904, 2011 894 Use of In Vivo Real-Time Optical Imaging for Esophageal Neoplasia PeterM.Vila,MSPH, 1 Nadhi Thekkek, 2 Rebecca Richards-Kortum, PhD, 2 and Sharmila nandasabapathy,
MOUNT SINI JOURNL OF MEDICINE 78:894 904, 2011 894 Use of In Vivo Real-Time Optical Imaging for Esophageal Neoplasia PeterM.Vila,MSPH, 1 Nadhi Thekkek, 2 Rebecca Richards-Kortum, PhD, 2 and Sharmila nandasabapathy,
Confocal Laser Endomicroscopy of the Colon
 clinical imaging Confocal Laser Endomicroscopy of the Colon Dan Ionut Gheonea, Adrian Saftoiu, Tudorel Ciurea, Carmen Popescu, Claudia Valentina Georgescu, Anca Malos Research Center of Gastroenterology
clinical imaging Confocal Laser Endomicroscopy of the Colon Dan Ionut Gheonea, Adrian Saftoiu, Tudorel Ciurea, Carmen Popescu, Claudia Valentina Georgescu, Anca Malos Research Center of Gastroenterology
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Helicobacter pylori Improved Detection of Helicobacter pylori
 DOI:http://dx.doi.org/10.7314/APJCP.2016.17.4.2099 RESEARCH ARTICLE Improved Detection of Helicobacter pylori Infection and Premalignant Gastric Mucosa Using Conventional White Light Source Gastroscopy
DOI:http://dx.doi.org/10.7314/APJCP.2016.17.4.2099 RESEARCH ARTICLE Improved Detection of Helicobacter pylori Infection and Premalignant Gastric Mucosa Using Conventional White Light Source Gastroscopy
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Computer aided optical diagnosis of polyps. Dr Michael Byrne Vancouver General Hospital University of British Columbia
 Computer aided optical diagnosis of polyps Dr Michael Byrne Vancouver General Hospital University of British Columbia Conflict of Interest/disclosures Satis Operations Inc (partner in ai4gi venture)----ceo
Computer aided optical diagnosis of polyps Dr Michael Byrne Vancouver General Hospital University of British Columbia Conflict of Interest/disclosures Satis Operations Inc (partner in ai4gi venture)----ceo
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018
 MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
Magnifying Endoscopy and Chromoendoscopy of the Upper Gastrointestinal Tract
 Magnifying Endoscopy and Chromoendoscopy of the Upper Gastrointestinal Tract Alina M.Boeriu 1, Daniela E.Dobru 1, Simona Mocan 2 1) Department of Gastroenterology, University of Medicine and Pharmacy;
Magnifying Endoscopy and Chromoendoscopy of the Upper Gastrointestinal Tract Alina M.Boeriu 1, Daniela E.Dobru 1, Simona Mocan 2 1) Department of Gastroenterology, University of Medicine and Pharmacy;
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Corporate Medical Policy
 Corporate Medical Policy Chromoendoscopy as an Adjunct to Colonoscopy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: chromoendoscopy_as_an_adjunct_to_colonoscopy 7/2012 11/2017
Corporate Medical Policy Chromoendoscopy as an Adjunct to Colonoscopy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: chromoendoscopy_as_an_adjunct_to_colonoscopy 7/2012 11/2017
Early detection and treatment for Esophageal Cancer in Africa
 Early detection and treatment for Esophageal Cancer in Africa Dr Michael Mwachiro Tenwek Hospital NCI-IARC ESCC Tumor Workshop Where is Tenwek Hospital? Tenwek Nairobi Tenwek Hospital Identification of
Early detection and treatment for Esophageal Cancer in Africa Dr Michael Mwachiro Tenwek Hospital NCI-IARC ESCC Tumor Workshop Where is Tenwek Hospital? Tenwek Nairobi Tenwek Hospital Identification of
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions
 Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Clinical studies of indicative biopsies in opportunistic screening in high risk population of oesophageal cancer.
 Biomedical Research 2017; 28 (9): 4121-4125 ISSN 0970-938X www.biomedres.info Clinical studies of indicative biopsies in opportunistic screening in high risk population of o. Jie Gao #, Ailan Xian #, Tingfeng
Biomedical Research 2017; 28 (9): 4121-4125 ISSN 0970-938X www.biomedres.info Clinical studies of indicative biopsies in opportunistic screening in high risk population of o. Jie Gao #, Ailan Xian #, Tingfeng
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters.
 Real-Time Increased Detection of Neoplastic Tissue in Barrett s Esophagus with Probe-Based Confocal Laser Endomicroscopy: Final Results of an International Multicenter, Prospective, Randomized, Controlled
Real-Time Increased Detection of Neoplastic Tissue in Barrett s Esophagus with Probe-Based Confocal Laser Endomicroscopy: Final Results of an International Multicenter, Prospective, Randomized, Controlled
Nakamura et al. BMC Cancer (2016) 16:743 DOI /s y
 16:743 DOI /s y") Nakamura et al. BMC Cancer (2016) 16:743 DOI 10.1186/s12885-016-2787-y RESEARCH ARTICLE Open Access Natural history of superficial head and neck squamous cell carcinoma under scheduled follow-up endoscopic
Nakamura et al. BMC Cancer (2016) 16:743 DOI 10.1186/s12885-016-2787-y RESEARCH ARTICLE Open Access Natural history of superficial head and neck squamous cell carcinoma under scheduled follow-up endoscopic
1. Introduction. Correspondence should be addressed to Edson Ide;
 Oncology Volume 203, Article ID 736756, 6 pages http://dx.doi.org/0.55/203/736756 Research Article Endoscopic Detection of Early Esophageal Squamous Cell Carcinoma in Patients with Achalasia: Narrow-Band
Oncology Volume 203, Article ID 736756, 6 pages http://dx.doi.org/0.55/203/736756 Research Article Endoscopic Detection of Early Esophageal Squamous Cell Carcinoma in Patients with Achalasia: Narrow-Band
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Geisinger Clinic Annual Progress Report: 2011 Nonformula Grant
 Geisinger Clinic Annual Progress Report: 2011 Nonformula Grant Reporting Period July 1, 2012 June 30, 2013 Nonformula Grant Overview The Geisinger Clinic received $1,000,000 in nonformula funds for the
Geisinger Clinic Annual Progress Report: 2011 Nonformula Grant Reporting Period July 1, 2012 June 30, 2013 Nonformula Grant Overview The Geisinger Clinic received $1,000,000 in nonformula funds for the
Radiofrequency ablation for early esophageal squamous cell neoplasia
 Radiofrequency ablation for early esophageal squamous cell neoplasia Authors Y. M. Zhang 1, J. J. G. H. M. Bergman 2, B. Weusten 2, 3, S. M. Dawsey 4, D. E. Fleischer 5,N.Lu 6,S.He 1,G.Q.Wang 1 Institutions
Radiofrequency ablation for early esophageal squamous cell neoplasia Authors Y. M. Zhang 1, J. J. G. H. M. Bergman 2, B. Weusten 2, 3, S. M. Dawsey 4, D. E. Fleischer 5,N.Lu 6,S.He 1,G.Q.Wang 1 Institutions
Image Analysis of Magnifying Endoscopy for Differentiation between Early Gastric Cancers and Gastric Erosions
 Showa Univ J Med Sci 29 3, 297 306, September 2017 Original Image Analysis of Magnifying Endoscopy for Differentiation between Early Gastric Cancers and Gastric Erosions Shotaro HANAMURA, Kuniyo GOMI,
Showa Univ J Med Sci 29 3, 297 306, September 2017 Original Image Analysis of Magnifying Endoscopy for Differentiation between Early Gastric Cancers and Gastric Erosions Shotaro HANAMURA, Kuniyo GOMI,
Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia
: Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia") UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD
 CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process
 MEASURE TYPE: Process") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions
 Acta Medica Marisiensis 2016;62(2):182-186 DOI: 10.1515/amma-2016-0004 RESEARCH ARTICLE The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions Boeriu Alina
Acta Medica Marisiensis 2016;62(2):182-186 DOI: 10.1515/amma-2016-0004 RESEARCH ARTICLE The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions Boeriu Alina
Endoscopic Management of Barrett s Esophagus
 Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Novel endoscopic observation in Barrett s oesophagus using high resolution magnification endoscopy and narrow band imaging
 Alimentary Pharmacology & Therapeutics Novel endoscopic observation in Barrett s oesophagus using high resolution magnification endoscopy and narrow band imaging G. K. ANAGNOSTOPOULOS*, K. YAO*, P. KAYE,
Alimentary Pharmacology & Therapeutics Novel endoscopic observation in Barrett s oesophagus using high resolution magnification endoscopy and narrow band imaging G. K. ANAGNOSTOPOULOS*, K. YAO*, P. KAYE,
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases
 Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Correlation between Gastric Mucosal Morphologic Patterns and Histopathological Severity of
 Hindawi Publishing Corporation BioMed Research International Volume 2015, Article ID 808505, 7 pages http://dx.doi.org/10.1155/2015/808505 Research Article Correlation between Gastric Mucosal Morphologic
Hindawi Publishing Corporation BioMed Research International Volume 2015, Article ID 808505, 7 pages http://dx.doi.org/10.1155/2015/808505 Research Article Correlation between Gastric Mucosal Morphologic
Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France
 Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France Barrett s esophagus (BE) is an acquired condition in which the normal squamous epithelium
Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France Barrett s esophagus (BE) is an acquired condition in which the normal squamous epithelium
Novel Optical Research at UPMC
 Novel Optical Research at UPMC Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology, & Nutrition University of Pittsburgh Medical Center Background Patients with UC and CD of
Novel Optical Research at UPMC Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology, & Nutrition University of Pittsburgh Medical Center Background Patients with UC and CD of
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading?
 Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Copyright. Pelham Keahey
 Copyright Pelham Keahey 2015 RICE UNIVERSITY Structured Illumination in a Fiber-Optic Microendoscope to Image Nuclear Morphometry in Columnar Epithelium by Pelham Keahey A THESIS SUBMITTED IN PARTIAL FULFILLMENT
Copyright Pelham Keahey 2015 RICE UNIVERSITY Structured Illumination in a Fiber-Optic Microendoscope to Image Nuclear Morphometry in Columnar Epithelium by Pelham Keahey A THESIS SUBMITTED IN PARTIAL FULFILLMENT
Current Management: Role of Radiofrequency Ablation
 Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
The Paris classification of colonic lesions
 The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
Barrett s Esophagus. Radiofrequency Ablation with the HALO Technology A Reference Book
 Radiofrequency Ablation with the HALO Technology A Reference Book 540 Oakmead Parkway, Sunnyvale, CA 94085 What is Barrett s esophagus? Barrett s esophagus is a change that occurs within the cellular lining
Radiofrequency Ablation with the HALO Technology A Reference Book 540 Oakmead Parkway, Sunnyvale, CA 94085 What is Barrett s esophagus? Barrett s esophagus is a change that occurs within the cellular lining
REPORT. McMahon Publishing Group. PENTAX Medical i-scan Technology for Improved Endoscopic Evaluations
 Brought to You by MAY 2014 PENTAX Medical i-scan Technology for Improved Endoscopic Evaluations Endoscopy plays a vital role in the diagnosis and clinical management of diseases of the gastrointestinal
Brought to You by MAY 2014 PENTAX Medical i-scan Technology for Improved Endoscopic Evaluations Endoscopy plays a vital role in the diagnosis and clinical management of diseases of the gastrointestinal
Yanfang Chen, 1,2 Ye Zhao, 1,2 Xiaojing Zhao, 2 and Ruihua Shi Introduction
 Gastroenterology Research and Practice Volume 2016, Article ID 3741456, 7 pages http://dx.doi.org/10.1155/2016/3741456 Research Article Clinical Outcomes of Endoscopic Submucosal Dissection for Early Esophageal
Gastroenterology Research and Practice Volume 2016, Article ID 3741456, 7 pages http://dx.doi.org/10.1155/2016/3741456 Research Article Clinical Outcomes of Endoscopic Submucosal Dissection for Early Esophageal
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Current Management of Low-Grade Dysplasia in Barrett Esophagus
 Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Is Radiofrequency Ablation Effective In Treating Barrett s Esophagus Patients with High-Grade Dysplasia?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series
 E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
Recommended by ELS! NARROW BAND IMAGING IN ENT Review of Clinical Evidence.
 Recommended by ELS! NARROW BAND IMAGING IN ENT Review of Clinical Evidence. 307 HIGH DEFINITION NARROW BAND IMAGING TECHNICAL PRINCIPLE Narrow Band Imaging (NBI) NBI is an optical image enhancement technology
Recommended by ELS! NARROW BAND IMAGING IN ENT Review of Clinical Evidence. 307 HIGH DEFINITION NARROW BAND IMAGING TECHNICAL PRINCIPLE Narrow Band Imaging (NBI) NBI is an optical image enhancement technology
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: April 15, 2017 2.01.80 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus 2.01.84 Chromoendoscopy as an Adjunct to Colonoscopy 6.01.32 Virtual
FEP Medical Policy Manual Effective Date: April 15, 2017 2.01.80 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus 2.01.84 Chromoendoscopy as an Adjunct to Colonoscopy 6.01.32 Virtual
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease
 ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Chromoendoscopy - Should It Be Standard of Care in IBD?
 Chromoendoscopy - Should It Be Standard of Care in IBD? John F. Valentine, MD, FACG Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Utah What is the point of
Chromoendoscopy - Should It Be Standard of Care in IBD? John F. Valentine, MD, FACG Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Utah What is the point of
Identification of gastric atrophic changes: from histopathology to endoscopy
 Evidence in perspective 533 Identification of gastric atrophic changes: from histopathology to endoscopy Authors Mário Dinis-Ribeiro 1,2, Ernst J. Kuipers 3 Institutions Bibliography DOI http://dx.doi.org/
Evidence in perspective 533 Identification of gastric atrophic changes: from histopathology to endoscopy Authors Mário Dinis-Ribeiro 1,2, Ernst J. Kuipers 3 Institutions Bibliography DOI http://dx.doi.org/
Confocal Laser Endomicroscopy. Description
 Subject: Confocal Laser Endomicroscopy Page: 1 of 15 Last Review Status/Date: June 2016 Confocal Laser Endomicroscopy Description Confocal laser endomicroscopy (CLE), also known as confocal fluorescent
Subject: Confocal Laser Endomicroscopy Page: 1 of 15 Last Review Status/Date: June 2016 Confocal Laser Endomicroscopy Description Confocal laser endomicroscopy (CLE), also known as confocal fluorescent
Endoscopic diagnosis and management of early squamous cell carcinoma of esophagus
 Review Article Endoscopic diagnosis and management of early squamous cell carcinoma of esophagus Hon-Chi Yip, Philip Wai-Yan Chiu Division of Upper Gastrointestinal and Metabolic Surgery, Department of
Review Article Endoscopic diagnosis and management of early squamous cell carcinoma of esophagus Hon-Chi Yip, Philip Wai-Yan Chiu Division of Upper Gastrointestinal and Metabolic Surgery, Department of
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
The white globe appearance (WGA): a novel marker for a correct diagnosis of early gastric cancer by magnifying. endoscopy with narrow-band imaging (M-
: a novel marker for a correct diagnosis of early gastric cancer by magnifying. endoscopy with narrow-band imaging (M-") E120 The white globe appearance (WGA): a novel marker for a correct diagnosis of early gastric cancer by magnifying endoscopy with narrow-band imaging (M-NBI) Authors Hisashi Doyama 1, Naohiro Yoshida
E120 The white globe appearance (WGA): a novel marker for a correct diagnosis of early gastric cancer by magnifying endoscopy with narrow-band imaging (M-NBI) Authors Hisashi Doyama 1, Naohiro Yoshida
Esophageal cancer Study: China Story
 NCI-IARC Tumor workshop: Esophageal Squamous Cell Carcinoma Esophageal cancer Study: China Story Youlin Qiao, Shaoming Wang Dept. of Cancer Epidemiology Cancer Institute/Hospital Chinese Academy of Medical
NCI-IARC Tumor workshop: Esophageal Squamous Cell Carcinoma Esophageal cancer Study: China Story Youlin Qiao, Shaoming Wang Dept. of Cancer Epidemiology Cancer Institute/Hospital Chinese Academy of Medical
CDx Diagnostics THE NEW STANDARD FOR QUALITY GI CARE
 CDx Diagnostics THE NEW STANDARD FOR QUALITY GI CARE STUDYDESIGN 16 major academic GI centers participated in a double-blind, randomized, crossover study in which 160 high-risk patients undergoing BE surveillance
CDx Diagnostics THE NEW STANDARD FOR QUALITY GI CARE STUDYDESIGN 16 major academic GI centers participated in a double-blind, randomized, crossover study in which 160 high-risk patients undergoing BE surveillance
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Fluorescence Spectroscopy: A New Approach in Cervical Cancer
 DOI 10.1007/s13224-012-0298-6 ORIGINAL ARTICLE : A New Approach in Cervical Cancer Pandey Kiran Pradhan Asima Agarwal Asha Bhagoliwal Ajay Agarwal Nidhi Received: 2 June 2008 / Accepted: 7 August 2012
DOI 10.1007/s13224-012-0298-6 ORIGINAL ARTICLE : A New Approach in Cervical Cancer Pandey Kiran Pradhan Asima Agarwal Asha Bhagoliwal Ajay Agarwal Nidhi Received: 2 June 2008 / Accepted: 7 August 2012
Medicare Advantage Medical Policy
 Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
The incidence of esophageal adenocarcinoma is rising in the ENDOSCOPY CORNER
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:843 847 ENDOSCOPY CORNER Acetic Acid Spray Is an Effective Tool for the Endoscopic Detection of Neoplasia in Patients With Barrett s Esophagus GAIUS LONGCROFT
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:843 847 ENDOSCOPY CORNER Acetic Acid Spray Is an Effective Tool for the Endoscopic Detection of Neoplasia in Patients With Barrett s Esophagus GAIUS LONGCROFT
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: April 15, 2018 Related Policies: 2.01.80 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus 2.01.84 Chromoendoscopy as an Adjunct to Colonoscopy
FEP Medical Policy Manual Effective Date: April 15, 2018 Related Policies: 2.01.80 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus 2.01.84 Chromoendoscopy as an Adjunct to Colonoscopy
About Omics Group conferences
 About Omics Group OMICS Group International through its Open Access Initiative is committed to make genuine and reliable contributions to the scientific community. OMICS Group hosts over 400 leading-edge
About Omics Group OMICS Group International through its Open Access Initiative is committed to make genuine and reliable contributions to the scientific community. OMICS Group hosts over 400 leading-edge
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia
 ...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
Confocal Laser Endomicroscopy. Populations Interventions Comparators Outcomes Individuals: With suspected or known colorectal lesions
 Protocol Confocal Laser Endomicroscopy (20187) Medical Benefit Effective Date: 07/01/13 Next Review Date: 03/19 Preauthorization No Review Dates: 03/13, 03/14, 03/15, 03/16, 03/17, 03/18 Preauthorization
Protocol Confocal Laser Endomicroscopy (20187) Medical Benefit Effective Date: 07/01/13 Next Review Date: 03/19 Preauthorization No Review Dates: 03/13, 03/14, 03/15, 03/16, 03/17, 03/18 Preauthorization
Diagnostic value of autofluorescence imaging combined with narrow band imaging in intraepithelial neoplasia of Barrett s esophagus
 JBUON 2015; 20(2): 399-405 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Diagnostic value of autofluorescence imaging combined with narrow band
JBUON 2015; 20(2): 399-405 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Diagnostic value of autofluorescence imaging combined with narrow band