Malignant Melanoma, what s new? Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
|
|
|
- Dorthy James
- 5 years ago
- Views:
Transcription

1 Malignant Melanoma, what s new? Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg

2 Melanoma Epidemiology: Incidence and Mortality Estimated 2012 Global Incidence and Mortality by WHO Region (all ages, both sexes) Europe Incidence 104,192 Deaths 23,509 Americas Incidence 88,246 Deaths 15,764 East Mediterranean Incidence 1815 Deaths 910 Africa Incidence 6082 Deaths 3318 South-East Asia Incidence 4012 Deaths 2183 Western Pacific Incidence 27,772 Deaths 9802 In 2012, there were 232,130 cases of melanoma worldwide There were 55,489 deaths due to melanoma worldwide Globocan. Accessed October 7, For Dabrafenib/Trametinib advisory board only. Not for external distribution.

3 Southern Africa, 2008 Estimated agestandardised incidence & mortality rates in men
4 Southern Africa, 2008 Estimated agestandardised incidence & mortality rates in women
5 Advanced Melanoma: Overview Accounts for ~ 1% of skin cancer diagnosed in the US [1,2] New cases, 2016 (estimated): 76,380 Deaths, 2016 (estimated): 10,130 5-yr survival rate for metastatic disease: 15% to 20% Multiple new therapeutic agents/regimens have been approved since 2011 Immune checkpoint inhibitors BRAF and MEK inhibitors Oncolytic virus therapy 1. Siegel RL, et al. CA Cancer. 2016;66: Balch R, et al. J Clin Oncol. 2009;27: Slide credit: clinicaloptions.com
6 THERAPY OF METASTATIC DISEASE
7 Monotherapy for the Treatment of Metastatic Melanoma Monotherapy with chemotherapy is relatively ineffective in treatment of metastatic melanoma Chemotherapies Response Rate DTIC 5.3% 28% Temozolomide 13.5% 24% Fotemustine 15.5% 24.2% Paclitaxel 3.6% Vindesine 12% 26% *
8 > 3000 Trials Between 1970 and 2010 Had No Real Clinical Impact Clinical Trial Publications (n)* Total number of clinical trial publications*: Publication Yr *Data collected using PubMed; US National Library of Medicine and National Institutes of Health.
 2 Rb (6%) 3 AKT3 (43% 60%) 4 RAS (9% 30%*) 5,6 PTEN (7% 19%) 8,9 MITF (10%) 10 KIT")
9 Molecular Pathways in Melanoma Key signalling pathways that are important in melanoma and that represent potential novel therapeutic targets have been identified 1 Alterations in several oncogenes, tumour suppressor genes, and their related pathways have been identified in melanoma, to varying extents BRAF ( 50%) 2 Rb (6%) 3 AKT3 (43% 60%) 4 RAS (9% 30%*) 5,6 PTEN (7% 19%) 8,9 MITF (10%) 10 KIT (8%) 3 p53 (0% 10%) 7 CDKN2A (28%) 3 AKT = protein kinase B; BRAF = rapidly accelerated fibrosarcoma isoform B; CDKN2A = cyclin-dependent kinase inhibitor 2A; KIT = Hardy-Zuckerman 4 feline sarcoma viral oncogene homolog; MITF = microphthalmia-associated transcription factor; p53 = protein 53; PTEN = phosphatase and tensin homolog; RAS = rat sarcoma; Rb = retinoblastoma. * The frequency of RAS mutation identified in melanoma is isoform-dependent. 5,6 1. Sekulic A, et al. Mayo Clin Proc 2008;83: Flaherty KT, et al. Cancer 2010;116: Omholt K, et al. Clin Cancer Res 2003;9: Forbes SA, et al. 9 Nucleic Acids Res 2010;38:D Box NF, et al. Pigment Cell Melanoma Res 2008;21: Stahl JM, et al. Cancer Res 2004;64: Birck A, et al. J Invest Dermatol 2000;114: Davies H, et al. Nature 2002;417: Çelebi JT, et al. J Med Genet 2000;37: Garraway LA, et al. Nature 2005;436:
10 Metastatic Melanoma: Treatment Advances Immunotherapy Target host Targeted Therapy Target tumor
11 Therapy of Metastatic Disease 1. Molecular Targeted therapies (anti- BRAF and others). 2. Immunotherapy (IL2, anti CTLA-4 and others)
12 Targeted Therapy Targeted cancer therapies are drugs or other molecules that block the growth and spread of cancer by interfering with specific changes or mutations in a pathway Many of these therapies focus on proteins that are involved in cell signaling pathways, which form a complex communication system that governs basic cellular functions and activities, such as cell division, cell movement, cell responses to specific external stimuli, and even cell death By blocking signals that tell cancer cells to grow and divide uncontrollably, targeted cancer therapies can help stop cancer progression and may induce cancer cell death
13 Targeted therapy The development of targeted therapies requires: The identification of a target The development of a therapy. Most targeted therapies are either small-molecule drugs or monoclonal antibodies By focusing on molecular and cellular changes that are specific to cancer, targeted cancer therapies may be more effective than other types of treatment, including chemotherapy and radiotherapy, and less harmful to normal cells
14 MAP Kinase Pathway Targeting in Melanoma < 5% melanomas (mucosal, acral) ckit KIT inhibitors: imatinib, nilotinib, dasatinib [4] ~ 20% melanomas (> age) [2,3] NRAS ~ 50% melanomas (< age) [2,3] ckit, NRAS, BRAF mutated in ~ 70% of melanomas, usually mutually exclusive [1] BRAF MEK ERK BRAF inhibitors: vemurafenib, dabrafenib [4] MEK inhibitors:cobimetinib tramatenib, [4] Oncogenic cell proliferation and survival 1. Sosman JA, et al. ASCO 2011 Educational Book. 2. Arkenau HT, et al. Br J Cancer. 2011;104: Thomas N, et al. Cancer Epidemiol Biomarkers Prev. 2007;16: Nikolaou VA, et al. J Invest Dermatol. 2012;132:
15



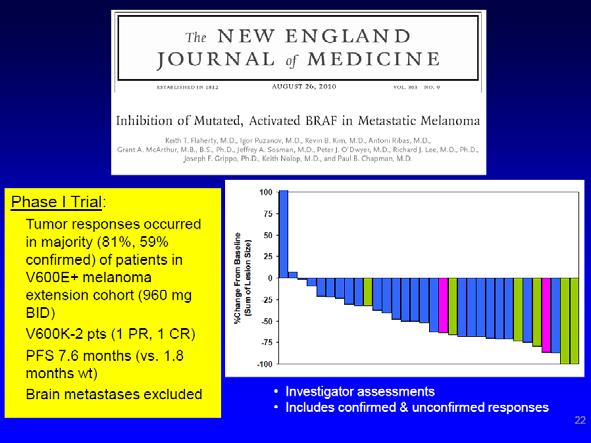
16 1. Flaherty KT, et al. N Engl J Med. 2010;363: Sosman JA, et al. N Engl J Med. 2012;366: Chapman PB, et al. N Engl J Med. 2011;364: Vemurafenib: Tumor Response by Metastatic Stage Flaherty 2010 [1] Sosman 2012 [2] Chapman 2011 [3]
 Dose escalation (N=55) V60 0 MM (N= 32) Previously treated (N 132) V600 Primary")
 V600 Co-Primary endpoints: OS, PFS Vemurafenib 1:1 DTIC DDI")

17 Vemurafenib Development: The BRIM Program Phase I Single-arm Phase II (NP22657) Phase III (NO25026) Dose escalation (N=55) V60 0 MM (N= 32) Previously treated (N 132) V600 Primary endpoint: BORR Secondary endpoints: PFS, OS, safety, QTc Clinical Pharmacology Studies Previously untreated (N= 675) V600 Co-Primary endpoints: OS, PFS Vemurafenib 1:1 DTIC DDI Relative BA Food Effect Mass Balance PK/PD BA=bioavailability; BORR=best overall RR; CRC=colorectal cancer; DDI=drug-drug interaction; PD=pharmacodynamics; PK=pharmacokinetics; QTc=corrected QT interval.
18 BRIM3: A Phase III Trial of Vemurafenib vs Dacarbazine (DTIC) Screening BRAFV600E mutation Stratification Stage ECOG PS (0 vs 1) LDH level ( vs nl) Geographic region R Vemurafenib (n = 337) 960 mg PO BID DTIC (n = 338) 1,000 mg/m 2 IV q3wk Coprimary endpoints: Overall and progression-free survival rates Chapman PB et al. N Engl J Med 2011;364(26):
 70 60 50 Dacarbazine (N = 274) 40 30 Median 1.6 mo Median 5.3 mo 20 10 0 0 1 2 3 4 5 6 7 8 9 10 11 12 Months Chapman PB et al. N Engl J Med 2011;364(26):2507-16.")
19 Progression-Free Survival (December 30, 2010 Cutoff) Progression-free survival(%) Hazard ratio 0.26 (95% CI; ) Log-rank p < Vemurafenib (N = 275) Dacarbazine (N = 274) Median 1.6 mo Median 5.3 mo Months Chapman PB et al. N Engl J Med 2011;364(26): Copyright 2011 Massachusetts Medical Society. All rights reserved.
20 In an open-label, multicenter international study, patients with untreated or previously treated melanoma and a BRAF/600 mutation received oral Vemurafenib 960 mg twice a day. The primary endpoint was safety. All analyses were done on the safety population, which included all patients who received at least one dose of Vemurafenib. This study was approved by the local authorities. All patients signed an informed consent. Larkin J. et al Lancet Oncol Apr;15(4):436-44
21 South African Patients Global study (n=3222) Global study % SA subset (n=34) SA subset % Male % 26 76,5% Female % 8 23,5% Age: Median 55 NA 53,5 NA Age: Range NA NA Age < % 32 94,1% Age > % 2 5,9% Time since metastatic diagnosis: Median 5,7 NA 5,3 NA Time since metastatic diagnosis: Range NA NA Time since metastatic diganosis: Mean 12,8 NA 12,8 NA Time since metastatic diagnosis: SD 21,6 NA 27,7 NA M1a % 6 17,6%
22 Proven Efficacy - BRIM Studies Phase I: 2 nd line (previous systemic therapy, n=32 [with BRAF mutation]) 1 RR = 56% mpfs >7 months mos = 12.6 months BRIM1 Phase II: 2 nd line, n=132 2 RR = 53% mpfs = 6.8 months mos = 15.9 months BRIM2 Phase III: 1 st line(no prior systemic therapy, n=337 treated with vemurafenib vs. n=338 treated with dacarbazine) 3,4 RR = 48% mpfs = 6.9 months vs. 1.6 months (HR = 0.38) mos = 13.6 months vs. 9.7 months (HR = 0.70) BRIM3 1) Flaherty KT, Puzanov I, Kim KB, et al. Inhibition of mutated, activated BRAF in metastatic melanoma. N Engl J Med. 2010;363: ) Sosman JA, Kim KB, Schuchter L, et al. Survival in BRAF V600-mutant advanced melanoma treated with vemurafenib. N Engl J Med. 2012;366: ) Chapman PB, Hauschild A, Robert C, et al. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N Engl J Med. 2011;364: ) Chapman PB, Hauschild A, Robert C, et al. Updated overall survival (OS) results for BRIM-3, a phase III randomized, openlabel, multicenter trial comparing BRAF inhibitor vemurafenib (vem) with dacarbazine (DTIC) in previously untreated patients with BRAFV600E-mutated melanoma. J Clin Oncol 30, 2012 (suppl; abstr 8502^). Presented at ASCO 2012, Chicago USA.
23


24 Tumor Response to Vemurafenib Baseline, 3/15/2011 Cycle 4 Day 1, 6/8/2011 PLX4032 = RG7204 = vemurafenib
25

 and")
26 Cutaneous SCC Keratoacanthoma (KA) Subtype #8520 Lacouture et al. Characteristics of KA subtype Raised button-like, central crater Well-differentiated neoplasm with low probability of invasion/metastasis Can grow rapidly; may involute and regress Typically treated by excision Did not result in treatment discontinuation Observed with RAF inhibitors Occurred on sun-exposed skin Association with HRAS (15/18) and NRAS (1/18) mutation in skin (higher then sporadic (6/53)
27
28 Mechanisms of Resistance to Vemurafenib PDGFRb or IGF1R Nazarian et al. Nature 2010 NRASQ61 Nazarian et al. Nature 2010 Villanueva et al. Cancer Cell 2010 BRAF inh CRAF PI3Ki or AKTi COT BRAFV600E Poulikakos et al. Nature 2011 Johannessen et al. Nature 2010 MEK MEK-dependent progression PI3K P MEKi Wagle et al. JCO 2011 ERK P Survival AKT MEK-independent progression
29 Conclusions Blockade of V600 mutated BRAF pathway is efficacious in advanced malignant melanoma Vemurafenib provides an OS benefit Rapid Responses, but resistance develops SCC and KA in a quarter of pts SA data follows the reported data in the multicentric international study

30 BREAK-3 Study Design Pivotal first-line study for patients with advanced melanoma with a BRAF V600 mutation Hauschild A, Grob JJ, Demidov LV, et al. Dabrafenib in BRAF-mutated metastatic melanoma: a multicentre, open-label, phase 3 randomised For Dabrafenib/Trametinib advisory board only. Not for external distribution. controlled trial. Lancet. 2012;380(9839):

31 BREAK-3 Follow-Up Investigator PFS Analysis For Dabrafenib/Trametinib advisory board only. Not for external distribution.
32 PFS (%) Single-Agent BRAF Inhibition vs Dacarbazine in Advanced Melanoma: PFS Dabrafenib [1] Dacarbazine (n = 63) HR: 0.30 (95% Cl: ; P <.0001) Dabrafenib (n = 187) Hauschild A, et al. Lancet Oncol. 2012;380: Chapman PB, et al. N Engl J Med. 2011;364: Vemurafenib [2] HR: 0.26 (95% Cl: ; P <.001) Vemurafenib (n = 275) Dacarbazine (n = 274) Mos ORR: 50% vs 6% with dacarbazine PFS (%) Mos ORR: 48% vs 5% with dacarbazine Slide credit: clinicaloptions.com
33 BRAF Inhibitors: Approved Indications in Advanced Melanoma Dabrafenib Single agent (150 mg PO BID) for unresectable or metastatic melanoma with BRAF V600E mutation In combination with trametinib (2 mg QD) for unresectable or metastatic melanoma with BRAF V600E/K mutation Vemurafenib Single agent (960 mg PO BID) for unresectable or metastatic melanoma with BRAF V600E mutation In combination with cobimetinib for unresectable or metastatic melanoma with BRAF V600E/K mutation Dabrafenib [package insert]. November Vemurafenib [package insert]. November Slide credit: clinicaloptions.com
34 One step beyond: MEK inhibition RTK RAS 40-60% of melanomas ATP ATP BRAF V600E MEK ERK Trametinib Cobimetinib Cellular Proliferation
35 Rationale for combination of dabrafenib and trametinib in BRAF-mutant tumours BRAF inhibitor (dabrafenib) OS: 20.1 months 1 PFS: 6.9 months 2 ORR: 59% 2 Hyperproliferative skin AEs 1,2 MEK inhibitor (trametinib) OS: 15.6 months 3 PFS: 4.8 months 4 RR: 22% 4 Rash AE 3,4 Preclinical BRAFi + MEKi 5 Delays BRAFi resistance Reduces hyperproliferative skin AEs 1. Grob JJ, et al. Poster presented at SMR 2014; 2. Hauschild A, et al. Poster presented at ASCO 2013; 3. Schadendorf D, et al. Poster presented at SMR 2013; 4. Flaherty KT, et al. N Engl J Med 2012;367:107 14; 5. King AJ, et al. PLoS ONE 2013;8:e RAS Mutant BRAF MEK perk Proliferatio n Survival Invasion Metastasis Goals of combination are to: Suppress MAPKdependent resistance mechanism Improve PFS, RR and OS Prolong duration of response Reduce the incidence of BRAFi-induced proliferative skin lesions AE=adverse event; BRAFi=BRAF inhibitor; HR=hazard ratio; MAPK=mitogen-activated protein kinase; MEK=MAPK kinase; MEKi=MEK inhibitor; ORR=objective response rate; OS=overall survival; perk=phosphorylated extracellular signal-regulated kinase; PFS=progression-free survival; RR=response rate. For distribution in response to an unsolicited request for medical information subject to local NP4 approval
36 Phase III evidence: COMBI-d study (MEK115306, NCT ) A Phase III, randomised, double-blind study comparing the combination of the BRAF inhibitor dabrafenib and the MEK inhibitor trametinib to the BRAF inhibitor dabrafenib in untreated patients with unresectable (stage IIIC) or metastatic (stage IV) BRAF V600E/K mutation-positive cutaneous melanoma MEK study (NCT )
37 Phase III evidence: COMBI-v study (MEK116513, NCT ) A Phase III, randomised, open-label study comparing the combination of the BRAF inhibitor dabrafenib and the MEK inhibitor trametinib to the BRAF inhibitor vemurafenib in subjects with unresectable (stage IIIC) or metastatic (stage IV) BRAF V600E/K mutation-positive cutaneous melanoma
38 COMBI-v and COMBI-d: Combination therapy Study design COMBI-v 1 COMBI-d 2 Eligibility criteria included: 18 years S Stage IIIC/IV melanoma C BRAF V600E/K R positive E ECOG PS status 0 or 1 E No prior systemic N therapy I No prior treatment with a BRAF inhibitor N or MEK inhibitor G Treated/stable brain metastases Eligibility criteria included: 18 years S Stage IIIC/IV melanoma C BRAF V600E/K R positive E ECOG PS status 0 or 1 E No prior systemic N therapy I No prior treatment with a BRAF inhibitor N or MEK inhibitor G Treated/stable brain metastases ECOG PS=Eastern Cooperative Group Performance Status. BRAF V600E/K BRAF V600E/K R A N D O M I S A T I O N R A N D O M I S A T I O N Inte Fina rim l OS OS anal anal Dabrafenib + trametinib ysis ysis n= mg BID + 2mg QD Vemurafenib n= mg BID Fina Foll l owup anal ysis anal Dabrafenib + trametinib (PFS ysis n=211 ) (OS) 150mg BID + 2mg QD Dabrafenib + placebo n= mg BID + placebo QD 1. Robert C et al. Oral presentation at ESMO Abstract LBA4_PR; 2. Long GV, et al. Lancet 2015;386:
39 COMBI-v and COMBI-d: Combination therapy Consistent PFS benefit Proportion alive without progression Median PFS for combination COMBI-v: 12.6 mo ( ) COMBI-d: 11.0 mo ( ) COMBI-d dabrafenib + trametinib* 1 Dabrafenib monotherapy* 1 COMBI-v dabrafenib + trametinib 2 Vemurafenib monotherapy 2 Number at risk COMBI-d D + T 1 Dabrafenib 1 COMBI-v D + T 2 Vemurafenib Time from randomisation, months *Data cut-off: January 2015; Data cut-off: March Long GV, et al. Lancet 2015;386:444 51; 2. Robert C, et al. Oral presentation at ECC 2015, Abstract 3301.
40 COMBI-v and COMBI-d: Combination therapy Consistent OS benefit Proportion alive Number at risk COMBI-d D + T 2 Dabrafenib 1 COMBI-v D + T 1 Vemurafenib Adjusted HR (95% CI) p value COMBI-v dabrafenib + trametinib 1 Vemurafenib monotherapy 2 COMBI-d dabrafenib + trametinib 2 Dabrafenib monotherapy 1 COMBI-v 1 COMBI-d 2 Dabrafenib + Dabrafenib + Vemurafenib Dabrafenib trametinib trametinib (n=352) (n=212) (n=352) (n=211) 0.66 ( ) 0.71 ( ) <0.001* Median OS for combination COMBI-v: 25.6 mo (22.6 NR) 1 COMBI-d: 25.1 mo (19.2 NR) Time from randomisation, months Robert C, et al. Oral presentation at ECC 2015, Abstract 3301; 2. Long GV, et al. Lancet 2015;386: *Adjusted stopping boundaries: two-sided p< for the efficacy analysis and p> for the futility analysis.
41
42


43 Oncology Centre and BRAF Positive Clinic

44 THANK YOU
45
46

47
48 Combi-V Study of Dabrafenib + Trametinib vs Vemurafenib: OS Dabrafenib + trametinib Vemurafenib OS (%) D+T (n = 352) Vemurafenib (n = 352) 20 Median, mos NR 17.2 (95% CI) (18.3-NR) (16.4-NR) Adjusted HR (95% CI) 0.69 ( ) 2-sided P value (stopping (<.0214) boundary) Mos Robert C, et al. N Engl J Med. 2015;372: Slide credit: clinicaloptions.com

49 Therapeutic Decision Making in Advanced Melanoma: An Interactive Online Tool The CCO Advanced Melanoma Interactive Decision Support Tool uses these 7 variables to make treatment recommendations. Available at: clinicaloptions.com/melanomatool Slide credit: clinicaloptions.com
50 COMBI-d: Consort diagram 947 patients screened 524 ineligible 423 randomised (ITT population) 211 assigned to dabrafenib + trametinib group 2 did not receive dabrafenib + trametinib 1 randomised in error 1 not compliant 209 received study drug (safety population) 212 assigned to dabrafenib + placebo group 1 did not receive dabrafenib + placebo as randomised in error 211 received study drug (safety population) 145 discontinued 115 disease progression 22 adverse events 4 withdrew consent 2 investigator discretion 2 protocol deviations 176 discontinued 150 disease progression 13 adverse events 9 withdrew consent 3 investigator discretion 1 lost to follow-up 64 still on treatment by 12 January still on treatment by 12 January 2015 Long GV, et al. Lancet 2015;386: For distribution in response to an unsolicited request for medical information subject to local NP4 approval
51 COMBI-d: Patient demographics, baseline characteristics, and stratification factors Dabrafenib + trametinib (n=211) Dabrafenib (n=212) Total (N=423) Age, median (range) 55.0 (22 89) 56.5 (22 86) 56.0 (22 89) Male sex, n (%) 111 (53) 114 (54) 225 (53) ECOG PS, n (%) (73) 150 (71) 305 (72) 1 55 (26) 61 (29) 116 (27) Disease stage, n (%) Stage IIIc, stage IV (M1a + M1b) 69 (33) 73 (34) 142 (34) Stage IV (M1c) 142 (67) 138 (65) 280 (66) Patient had visceral disease at baseline, n (%) 165 (78) 145 (68) 310 (73) <3 disease sites at baseline, n (%) 109 (52) 119 (56) 228 (54) No prior immunotherapy, n (%) 155 (73) 151 (71) 306 (72) Stratification factors BRAF V600 mutation status, n (%) V600E mutation-positive 179 (85) 181 (85) 360 (85) V600K mutation-positive 32 (15) 30 (14) 62 (15) LDH levels, n (%) ULN LDH 133 (63) 140 (66) 273 (65) Data on file. >ULN LDH 77 (36) 71 (33) ITT population. 148 (35) For distribution in response to an unsolicited request for medical information subject to local NP4 approval
52 COMBI-d: Summary of results Summary of survival data Summary of response data Dabrafenib + trametinib (n=210) Dabrafenib (n=210) CR, n (%) 33 (16) 28 (13) PR, n (%) 111 (53) 84 (40) ORR, n (%) 95% CI Difference in ORR, % (95% CI), p value Dabrafenib + trametinib (n=211) 144 (69) ( ) Dabrafenib (n=212) Median PFS, months (95% CI) 11.0 ( ) 8.8 ( ) Adjusted HR (95% CI) 2-sided p value 0.67 ( ) Median OS, months (95% CI) 25.1 (19.2 NR) 18.7 ( ) Adjusted HR (95% CI) 2-sided p value 0.71 ( ) 0.011* Median follow-up, months (53) Duration of response, months (95% CI) 12.9 ( ) 10.6 ( ) Long GV, et al. Lancet 2015;386:444 51; Data on file. *Adjusted stopping boundaries: two-sided p< for the efficacy analysis and p> for the futility analysis; Data are missing for one patient in the combination therapy group and two patients in the vemurafenib group because these patients did not have measurable disease at baseline. For distribution in response to an unsolicited request for medical information subject to local NP4 approval
53 COMBI-d (at January 2015): Updated PFS at final OS analysis Proportion alive and progression free Number at risk abrafenib + trametinib Dabrafenib Long GV, et al. Lancet 2015;386: Progressed, n (%) Median PFS, months (95% CI) HR (95% CI) 2-sided p value Dabrafenib + trametinib (n=211) Dabrafenib (n=212) 139 (66) 162 (76) 11.0 ( ) 0.67 ( ) ( ) Time from randomisation (months) ITT population. For distribution in response to an unsolicited request for medical information subject to local NP4 approval
54 COMBI-d (at January 2015): OS at final OS analysis 1.0 Dabrafenib + trametinib (n=211) Dabrafenib (n=212) Died, n (%) 99 (47) 123 (58) 0.8 Median OS, months (95% CI) 25.1 (19.2 NR) 18.7 ( ) Proportion alive HR (95% CI) 2-sided p value 0.71 ( ) Time from randomisation, months Number at risk Long GV, et al. Lancet 2015;386: ITT population. For distribution in response to an unsolicited request for medical information subject to local NP4 approval
55 COMBI-d (at January 2015): OS landmarks at final OS analysis OS landmarks, % (95% CI) Dabrafenib + trametinib (n=211) Dabrafenib (n=212) 1 year 74 (67 79) 68 (61 74) 2 years 51 (44 58) 42 (35 49) Long GV, et al. Lancet 2015;386: ITT population. For distribution in response to an unsolicited request for medical information subject to local NP4 approval
56 COMBI-d (at January 2015): Response at final OS analysis Dabrafenib + trametinib (n=210) Investigator assessment Dabrafenib (n=210) Best response, n (%) CR 33 (16) 28 (13) PR 111 (53) 84 (40) SD 50 (24) 66 (31) PD 13 (6) 19 (9) Not evaluable 3 (1) 13 (6) Response rate, n (%) CR + PR 144 (69) 112 (53) 95% CI (62, 75) (46, 60) Difference in response rate, % CR + PR 15 95% CI for difference ( ) p value Median duration of response for dabrafenib + trametinib was 12.9 months and for dabrafenib was 10.6 months Long GV, et al. Lancet 2015;386:444 51; Data on file. ITT population. For distribution in response to an unsolicited request for medical information subject to local NP4 approval
57 COMBI-d: Conclusions Updates from final OS analysis Improved overall survival with dabrafenib + trametinib combination vs dabrafenib HR 0.71; p= % reduction in risk of death Median OS of 25.1 months vs 18.7 months 2-year OS >50% Improved progression-free survival with combination vs dabrafenib HR 0.67; p< % reduction in risk of death Median PFS of 11.0 months vs 8.8 months Efficacy data clinically relevant for patients with BRAF V600 mutation-positive metastatic melanoma, where an unmet medical need remains Safety profile consistent with previously reported results No new safety concerns Pyrexia most notable risk with combination vs dabrafenib Fewer cutaneous hyperproliferative events with combination vs dabrafenib Additional landmark OS and safety analyses planned Long GV, et al. Lancet 2015;386: For distribution in response to an unsolicited request for medical information subject to local NP4 approval
58 COMBI-v: Summary of results Summary of survival data 1 Dabrafenib + trametinib Vemurafenib (n=352) (n=352) Median OS, months (95% CI) 25.6 (22.6 NR) 18.0 ( ) Adjusted HR (95% CI) 2-sided p value 0.66 ( ) <0.001 Median follow-up (months) Median PFS, months (95% CI) 12.6 ( ) 7.3 ( ) Adjusted HR (95% CI) 2-sided p value 0.61 ( ) <0.001 Summary of response data 1 Dabrafenib + trametinib Vemurafenib (n=351) (n=350) Complete response, n (%) 59 (17) 36 (10) Partial response, n (%) 172 (49) 150 (43) Stable disease, n (%) 87 (25) 102 (29) Progressive disease, n (%) 22 (6) 39 (11) ORR, n (%) 95% CI 231 (66) (53) Difference in ORR, % (95% CI) 13 ( ) p value Duration of response, months (95% CI) 13.8 ( ) 8.5 ( ) 1. Robert C, et al. Oral presentation at ECC 2015, Abstract 3301; 2. Data on file. For distribution in response to an unsolicited request for medical information subject to local NP4 approval
59 COMBI-d: Eligibility criteria 18 years Histologically confirmed cutaneous melanoma that is either stage IIIc (unresectable) or stage IV (metastatic) BRAF V600E/K mutation-positive as tested by a central reference laboratory 1 measurable lesion (based on RECIST 1.1) ECOG PS score 0 or 1 No prior systemic therapy in the advanced or metastatic setting (but adjuvant setting is allowed) Ipilimumab treatment must end at least 8 weeks prior to randomisation No prior treatment with a BRAF inhibitor or MEK inhibitor Treated and stable brain metastases Long GV, et al. N Engl J Med 2014; 371: supplementary appendix. RECIST=Response Evaluation Criteria in Solid Tumors For distribution in response to an unsolicited request for medical information subject to local NP4 approval
60 Part C: Conclusions Combined dabrafenib 150mg + trametinib 2mg prolonged PFS, ORR, DoR and OS compared with dabrafenib alone in BRAF V600-mutant metastatic melanoma: 1 3 Median PFS was 9.4 vs 5.8 months (HR: 0.39; p<0.001) 1,2 ORR was 76% vs 54% (p=0.03) 1,2 DoR was 10.5 vs 5.6 months 2 Median OS was 25.0 vs 20.2 months based on most recent data 3 12-month OS: 80 vs 70% 24-month OS: 51 vs 44% 36-month OS: 38 vs 31% Combined dabrafenib + trametinib safety profile is tolerable and manageable 1 3 Most common AEs were pyrexia, chills and fatigue 1. Long GV, et al. Oral presented at ESMO 2012, Abstract LBA27; 2. Flaherty KT, et al. N Engl J Med 2012;367: ; 3. Daud A, et al. J Clin Oncol 2015;33(Suppl):Abstract For distribution in response to an unsolicited request for medical information subject to local NP4 approval
61 COMBI-v: Study design Combination of dabrafenib + trametinib vs vemurafenib N=1644 Interim OS analysis Eligibility 18 screened years criteria R (202 events) Stage included: IIIC/IV A Dabrafenib + trametinib melanoma S N n=352 BRAF V600E/K C D positive R 150mg twice daily + O ECOG PS status E M 2mg daily BRAF 0 or 1 E I No prior systemic V600E/K N S Vemurafenib therapy I A n=352 No prior treatment N T with a BRAF I G 960mg twice daily inhibitor or MEK O N=1645 inhibitor N Treated/stable brain Stratification: metastases LDH (>ULN vs ULN) and BRAF mutation (V600E vs V600K) Primary endpoint: OS Secondary endpoints: PFS, ORR, DoR, safety Final OS analysis (280 events planned) Robert C, et al. N Engl J Med 2015;372:30 9; Robert C, et al. Oral presentation at ESMO 2014, Abstract LBA4_PR; For distribution in response to an unsolicited request for medical information subject to local NP4 approval
62 COMBI-v: Study population ITT, n Dabrafenib + trametinib Vemurafenib Total All randomised patients whether or not treatment was administered Safety, n All patients who received 1 dose of study treatment Robert C, et al. N Engl J Med 2015;372:30 9. For distribution in response to an unsolicited request for medical information subject to local NP4 approval
63 COMBI-v (at March 2015): OS at final analysis Proportion alive Median OS, months (95% CI) Dabrafenib + trametinib Vemurafenib (N=352) (N=352) 25.6 (22.6 NR) 18.0 ( ) 1.0 HR (95% CI) 0.66 ( ) Log-rank p value 0.9 <0.001 (2-sided) Time from randomisation (months) Patients at risk Dabrafenib trametinib Vemurafenib Robert C, et al. Oral presentation at ECC 2015, Abstract NR=not reported For distribution in response to an unsolicited request for medical information subject to local NP4 approval
64 COMBI-v (at March 2015): Landmark OS analysis Proportion alive 1.0 HR (95% CI) 0.66 ( ) Log-rank p value 0.9 < yr OS (2-sided) % 1.5-yr OS % 2-yr OS yr OS 51% 64% yr OS % 2-yr OS % Time from randomisation (months) Robert C, et al. Oral presentation at ECC 2015, Abstract Median OS, months (95% CI) Dabrafenib + trametinib Vemurafenib (N=352) (N=352) 25.6 (22.6 NR) 18.0 ( ) Patients at risk Dabrafenib trametinib Vemurafenib NR=not reported For distribution in response to an unsolicited request for medical information subject to local NP4 approval
65 COMBI-v (at March 2015): Response rates Best confirmed response Dabrafenib + trametinib (n=351) Vemurafenib (n=350) Complete response, n (%) 59 (17) 36 (10) Partial response, n (%) 172 (49) 150 (43) Stable disease, n (%) 87 (25) 102 (29) Progressive disease, n (%) 22 (6) 39 (11) Not evaluable, n (%) 12 (3) 25 (7) ORR, n (%) 95% CI 231 (66) (53) Difference in ORR, % (95% CI) 13 ( ) p value Duration of response, months (95% CI) 13.8 ( ) 8.5 ( ) Robert C, et al. Oral presentation at ECC 2015, Abstract Data cut-off: March For distribution in response to an unsolicited request for medical information subject to local NP4 approval
66 COMBI-v: Summary Dabrafenib + trametinib showed improved efficacy vs vemurafenib in BRAF V600- mutant melanoma Improved median OS (25.6 vs 18.0 months) 34% reduction in risk of death (HR 0.66; 95% CI ; p <0.001) Improved 2-year survival (51% vs 38%) Improved median PFS (12.6 vs 7.3 months; HR 0.61; p <0.001) Improved ORR (66% vs 53%) and DOR (13.8 vs 8.5 months) Longest benefit in patients with LDH ULN (2-year OS rate 66%) Manageable AE profile with no new safety signals Higher incidence of pyrexia and ejection fraction decrease in combination arm Lower incidence of cutaneous malignancies and hyperproliferative events in combination arm Lower incidence and severity of photosensitivity in combination arm Overall results comparable to COMBI-d study Improved OS and PFS shown with dabrafenib + trametinib combination therapy vs dabrafenib or vemurafenib monotherapy Robert C, et al. Oral presentation at ECC 2015, Abstract 3301; Data on file. For distribution in response to an unsolicited request for medical information subject to local NP4 approval
67 COMBI-d and COMBI-v: Landmark OS analysis Proportion alive Median 1-year OS for combination COMBI-v: 73% (68 77) 1 COMBI-d: 74% (67 79) 2 Median 2-year OS for combination COMBI-v: 51% (45 57) 1 COMBI-d: 51% (44 58) Number at risk Time from randomisation, months COMBI-d D + T COMBI-v D + T Robert C, et al. Oral presentation at ECC 2015, Abstract 3301; 2. Long GV, et al. Lancet 2015;386: For distribution in response to an unsolicited request for medical information subject to local NP4 approval
 11 (4) 25 (10) Partial response, n (%) 100 (40) 142 (57) Stable disease, n (%) 105 (42) 49 (20) *Only patients who had both pre and post tumour evaluations are included.")
68 cobrim (GO28141; phase III): Best tumour response Patients with confirmed objective response % (95% CI)* Vemurafenib + placebo (n=248) Cobimetinib + vemurafenib (n=247) 45 (38 51) 68 (61 73) Complete response, n (%) 11 (4) 25 (10) Partial response, n (%) 100 (40) 142 (57) Stable disease, n (%) 105 (42) 49 (20) *Only patients who had both pre and post tumour evaluations are included. CI = confidence interval; RECIST = Response Evaluation Criteria in Solid Tumours; SLD = the sum of the diameters of investigator identified target lesion per RECIST v 1.1. Data cutoff: May 9, 2014 Larkin J, et al. N Engl J Med. 2014;371:
69 cobrim: Summary of selected adverse events *Includes specific terms chorioretinopathy and retinal detachment. No cases of retinal vein occlusion were reported. SCC = squamous cell carcinoma. Larkin J, et al. N Engl J Med. 2014;371:
70 cobrim: Summary cobrim efficacy data confirmed clinical benefit of addition of cobimetinib to vemurafenib in BRAF V600 mutated melanoma months PFS for cobimetinib + vemurafenib 7.2 months PFS for placebo + vemurafenib (HR 0.58; 95% CI, ) ORR 69.6% for cobimetinib + vemurafenib and 50% for placebo + vemurafenib Common AEs were usually grade 1 or 2 Managed with dose modification and supportive care Permanent discontinuation of the combination due to AEs was relatively uncommon Rates of discontinuation were similar in the arms, indicating tolerability of the combination regimen Transient MEK inhibitor-related serous retinopathy was usually mild and resolved with no long-term sequelae Larkin J, et al. Oral presentation at 51 st ASCO Annual Meeting May 29 June 2, 2015; Chicago, Illinois.
71 NEMO: Conclusions Prolonged PFS, improved response rates achieved with binimetinib in pts with NRAS-mutant melanoma [1] PFS (median): 2.8 vs 1.5 mos (HR: 0.62; 95% CI: ; P <.001) Benefit evident across subgroups, including those receiving prior immunotherapy (n = 85; 5.5 vs 1.6 mos for binimetinib vs dacarbazine) Binimetinib safety profile consistent with other MEK inhibitors [2,3] Investigators concluded that binimetinib is an effective new therapy for NRAS-mutant melanoma, a pt population with unmet clinical needs 1. Dummer R, et al. ASCO Abstract Trametinib [package insert]. 3. Cobimetinib [package insert]. Slide credit: clinicaloptions.com
72 NEMO: Adverse Events Binimetinib (n = 269) Dacarbazine (n = 114) Selected AEs, % All Grades * Grade 3/4 All Grades * Grade 3/4 Total Skin-related Rash Dermatitis acneiform Gastrointestinal Diarrhea Nausea Vomiting Muscle-related (blood CPK increase) Other Peripheral edema Fatigue Asthenia Hypertension AST increased Decreased appetite < *> 15% of Ejection pts in any fraction treatment decreased group. > 2 % of pts in 11 any treatment group Other grade Neutropenia 3/4 AEs > 2%; binimetinib: general physical 1 health deterioration 1 (4%), ALT increase 18 (3%); dacarbazine: 9 anemia (10%), Thrombocytopenia leukopenia (7%), decreased neutrophil 1count (7%), ALT increase < 1 (6%), lymphopenia 15 (5%), GGT 4 increase (5%) Dummer R, et al. ASCO Abstract Slide credit: clinicaloptions.com
73
74 cobrim: Patient characteristics Characteristic Vemurafenib + placebo (n=248) Vemurafenib + cobimetinib (n=247) Median age, years (range) 55 (25 85) 56 (23 88) Sex, n (%) Male Female ECOG Performance Status, n (%) (57) 108 (44) 164 (67) 80 (33) 0 (0) 146 (59) 101 (41) 184 (76) 58 (24) 1 (<1) Elevated LDH, n (%) 104 (43) 1 (<1) History of brain metastases, n (%) 2 (0.8) 1 (<1) Geographic region, n (%) Australia/New Zealand/Israel Europe North America Melanoma stage at enrollment, n (%) Unresectable stage IIIC Stage IV, M1a Stage IV, M1b Stage IV, M1c 38 (15) 184 (74) 26 (11) 13 (5) 40 (16) 42 (17) 153 (62) 40 (16) 182 (74) 25 (10) 21 (9) 40 (16) 40 (16) 146 (59) Median follow-up (range), months 14.2 ( ) LDH, lactate dehydrogenase. Data cutoff: Jan 16, 2015 Larkin J, et al. Oral presentation at 51 st ASCO Annual Meeting May 29 June 2, 2015; Chicago, Illinois.
75 cobrim : Updated investigator-assessed PFS Kaplan-Meier Plot for PFS Intent-to-Treat Population Survival Distribution Function (%) ITT Population Vem + Pbo n = 248 Cobi + Vem n = 247 PFS events, n (%) 180 (72.6) 143 (57.9) Median PFS, months (95% CI) HR a (95% CI) b ( ) 0.58 b ( ) 12.3 b ( ) Data cutoff of January 16, 2015 was 1 year from enrollment of last patient Cobimetinib + vemurafenib (n=247) Placebo + vemurafenib (n=248) Censored + 1 Months 5 Months 9 Months 13 Months 17 Months 21 Months 25 Months No. of patients at risk Time Vemurafenib + cobimetinib Vemurafenib + placebo a Stratified HR. b The median PFS was 6.2 months in Pbo + Vem, and 9.9 months in Cobi + Vem (HR, 0.51; 95% CI, ) at the May 9, 2014 data cutoff. Larkin J, et al. Oral presentation at 51 st ASCO Annual Meeting May 29 June 2, 2015; Chicago, Illinois.
76 cobrim: Overall survival Vemurafenib + placebo Cobimetinib + vemurafenib Overall survival events, n Median overall survival NE NE 9-month overall survival (95% CI), % 72.5 ( ) 81.1 ( ) HR (95% CI) p-value, two-sided 0.65 ( ) p=0.046* *Descriptive p-value. Did not cross the pre-specified stopping boundary for the interim analysis (boundary p< ); CI = confidence interval; HR = hazard ratio; NE = not estimable. Data cutoff: May 9, 2014 Larkin J, et al. N Engl J Med. 2014;371:
77 cobrim: Updated response rates Vemurafenib + placebo n=248 Cobimetinib + vemurafenib n=247 Complete response (CR), n (%) 26 (10.5) 39 (15.8) Partial response, n (%) 98 (39.5) 133 (53.8) Objective response rate (ORR), n (%) Difference in ORR, % Duration of response Patients with event, n (%) Median (95% CI) Range At the primary analysis 2 : ORR was 45% (vem + placebo) and 68% (vem + cobi) CR was 4% (vem + placebo) and 10% (vem + cobi) 124 (50.0) (95% CI, ) 73 (58.9) 9.2 ( ) a (95% CI, ) 172 (69.6) (95% CI, ) 84 (48.8) 13.0 ( ) Larkin J, et al. Oral presentation at 51 st ASCO Annual Meeting May 29 June 2, 2015; Chicago, Illinois. 2. Larkin J et al. N Engl J Med. 2014;371:
78 Overall Survival (December 30, 2010 Cutoff) Hazard ratio 0.37 (95% CI; ) Log-rank p < Chapman PB et al. N Engl J Med 2011;364(26): Copyright 2011 Massachusetts Medical Society. All rights reserved.
Targeted Therapies in Melanoma
 Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
BRAF Inhibitors in Metastatic disease. Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia
 Inhibitors in Metastatic disease Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia Disclosures Research Support Pfizer & Cellgene Consultant Provectus Mortality from Melanoma
Inhibitors in Metastatic disease Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia Disclosures Research Support Pfizer & Cellgene Consultant Provectus Mortality from Melanoma
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
Overall Survival in COLUMBUS: A Phase 3 Trial of Encorafenib (ENCO) Plus Binimetinib (BINI) vs Vemurafenib (VEM) or ENCO in BRAF-Mutant Melanoma
 Plus Binimetinib (BINI) vs Vemurafenib (VEM) or ENCO in BRAF-Mutant Melanoma") Overall Survival in COLUMBUS: A Phase 3 Trial of Encorafenib (ENCO) Plus Binimetinib (BINI) vs Vemurafenib () or ENCO in BRAF-Mutant Melanoma, Paolo A. Ascierto, Helen J. Gogas, Ana Arance, Mario Mandala,
Overall Survival in COLUMBUS: A Phase 3 Trial of Encorafenib (ENCO) Plus Binimetinib (BINI) vs Vemurafenib () or ENCO in BRAF-Mutant Melanoma, Paolo A. Ascierto, Helen J. Gogas, Ana Arance, Mario Mandala,
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Response and resistance to BRAF inhibitors in melanoma
 Response and resistance to BRAF inhibitors in melanoma Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center Disclosures Roche/Genentech: consultant GlaxoSmithKline: consultant BRAF mutations
Response and resistance to BRAF inhibitors in melanoma Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center Disclosures Roche/Genentech: consultant GlaxoSmithKline: consultant BRAF mutations
The Development of Encorafenib (LGX818) and Binimetinib (MEK162) in Patients With Metastatic Melanoma
 and Binimetinib (MEK162) in Patients With Metastatic Melanoma") The Development of Encorafenib (LGX818) and Binimetinib (MEK162) in Patients With Metastatic Melanoma Reinhard Dummer, 1 Keith Flaherty, 2 Richard Kefford, 3 Paolo A. Ascierto, 4 Laure Moutouh-de Parseval,
The Development of Encorafenib (LGX818) and Binimetinib (MEK162) in Patients With Metastatic Melanoma Reinhard Dummer, 1 Keith Flaherty, 2 Richard Kefford, 3 Paolo A. Ascierto, 4 Laure Moutouh-de Parseval,
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
ASCO / COLUMBUS ENCORE PRESENTATION June 4, 2018
 ASCO / COLUMBUS ENCORE PRESENTATION June 4, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions of the Private
ASCO / COLUMBUS ENCORE PRESENTATION June 4, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions of the Private
Approaches To Treating Advanced Melanoma
 Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
BRAF/MEK inhibitors in the systemic treatment of advanced skin melanoma
 QUALITY OF LIFE IN ONCOLOGY Review article BRAF/MEK inhibitors in the systemic treatment of advanced skin melanoma Maksymilian Kruczała, Aleksandra Grela-Wojewoda, Marek Ziobro Clinic of Systemic and Metastatic
QUALITY OF LIFE IN ONCOLOGY Review article BRAF/MEK inhibitors in the systemic treatment of advanced skin melanoma Maksymilian Kruczała, Aleksandra Grela-Wojewoda, Marek Ziobro Clinic of Systemic and Metastatic
Best Practices in the Treatment and Management of Metastatic Melanoma. Melanoma
 Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
The information in this activity is intended for healthcare professionals based outside of the United States. This activity may contain information
 The information in this activity is intended for healthcare professionals based outside of the United States. This activity may contain information on products outside the approved indications where you
The information in this activity is intended for healthcare professionals based outside of the United States. This activity may contain information on products outside the approved indications where you
MELANOMA: THE BEST OF THE YEAR Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone
 MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
Normal RAS-RAF (MAPK) pathway signaling
 pathway signaling") BRAF-Mutations in Melanomas L. Mazzucchelli Istituto Cantonale di Patologia, Locarno 77. Annual Meeting Swiss Society of Pathology, Lucerne 2011 Sponsored by Roche Pharma Switzerland Melanoma has increased
BRAF-Mutations in Melanomas L. Mazzucchelli Istituto Cantonale di Patologia, Locarno 77. Annual Meeting Swiss Society of Pathology, Lucerne 2011 Sponsored by Roche Pharma Switzerland Melanoma has increased
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Array BioPharma Jefferies 2016 Global Healthcare Conference. June 9, 2016
 Array BioPharma Jefferies 216 Global Healthcare Conference June 9, 216 Safe Harbor Statement 2 Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
Array BioPharma Jefferies 216 Global Healthcare Conference June 9, 216 Safe Harbor Statement 2 Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
BRAF Inhibition in Melanoma
 BRAF Inhibition in Melanoma New York City, Mar 22-23, 2013 Bartosz Chmielowski, MD, PhD Assistant Clinical Professor University of California Los Angeles Disclosures Speaker Bureau: BMS, Genentech, Prometheus
BRAF Inhibition in Melanoma New York City, Mar 22-23, 2013 Bartosz Chmielowski, MD, PhD Assistant Clinical Professor University of California Los Angeles Disclosures Speaker Bureau: BMS, Genentech, Prometheus
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD
 Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
presentation session & clinical Keith T. Flaherty, M.D. Abramson Cancer Center of the University of Pennsylvania
 Melanoma: highlights from the oral presentation session & clinical science symposium at ASCO 2009 Keith T. Flaherty, M.D. Abramson Cancer Center of the University of Pennsylvania Abstracts to be discussed
Melanoma: highlights from the oral presentation session & clinical science symposium at ASCO 2009 Keith T. Flaherty, M.D. Abramson Cancer Center of the University of Pennsylvania Abstracts to be discussed
Unmet Need Mucosal and Uveal Melanoma
 Unmet Need Mucosal and Uveal Melanoma Matteo Carlino Crown Princess Mary Cancer Centre Westmead and Blacktown Hospitals Melanoma Institute Australia The University of Sydney. Cutaneous Overall Survival
Unmet Need Mucosal and Uveal Melanoma Matteo Carlino Crown Princess Mary Cancer Centre Westmead and Blacktown Hospitals Melanoma Institute Australia The University of Sydney. Cutaneous Overall Survival
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma
 With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma") Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Breakthrough and Landscape of Acral and Mucosal Melanomas. Jun Guo. M.D., Ph.D Peking University Cancer Hospital & Institute
 Breakthrough and Landscape of Acral and Mucosal Melanomas Jun Guo. M.D., Ph.D Peking University Cancer Hospital & Institute Current status of advanced melanoma Current status of advanced MM Targeted therapy
Breakthrough and Landscape of Acral and Mucosal Melanomas Jun Guo. M.D., Ph.D Peking University Cancer Hospital & Institute Current status of advanced melanoma Current status of advanced MM Targeted therapy
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic
 Dabrafenib for treating unresectable, advanced or metastatic") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic BRAF V600 mutation-positive melanoma mutation-positive melanoma
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal (STA) Dabrafenib for treating unresectable, advanced or metastatic BRAF V600 mutation-positive melanoma mutation-positive melanoma
New treatments in melanoma
 New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine
New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine
Histology independent indications in oncology. The BRAF Story. Yibing Yan PhD Roche / Genentech
 Histology independent indications in oncology The BRAF Story Yibing Yan PhD Roche / Genentech 1 Introduction the discovery Case study in BRAF mutant melanoma heterogeneity within the tumour variability
Histology independent indications in oncology The BRAF Story Yibing Yan PhD Roche / Genentech 1 Introduction the discovery Case study in BRAF mutant melanoma heterogeneity within the tumour variability
Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer
 Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer Axel Grothey, M.D., Professor of Oncology, Clinical and Translational Science Division of Medical Oncology Mayo Clinic, Rochester,
Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer Axel Grothey, M.D., Professor of Oncology, Clinical and Translational Science Division of Medical Oncology Mayo Clinic, Rochester,
New Therapeutic Approaches to Malignant Melanoma
 2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3
 ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Flaherty KT, Infante JR, Daud A, et al. Combined BRAF and MEK
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Flaherty KT, Infante JR, Daud A, et al. Combined BRAF and MEK
Updates in Metastatic Melanoma
 SCSHP 214 Annual Meeting Updates in Metastatic Melanoma LeAnn B. orris, PharmD, BCPS, BCOP Assistant Professor South Carolina College of Pharmacy Background Estimated 76,69 new cases in 213 Increasing
SCSHP 214 Annual Meeting Updates in Metastatic Melanoma LeAnn B. orris, PharmD, BCPS, BCOP Assistant Professor South Carolina College of Pharmacy Background Estimated 76,69 new cases in 213 Increasing
ASCO 2014: The Future is Here. What I Will Talk About. George W. Sledge MD Stanford University School of Medicine
 ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
vemurafenib 240mg film-coated tablet (Zelboraf ) SMC No. (792/12) Roche Products Ltd.
 SMC No. (792/12) Roche Products Ltd.") Resubmission vemurafenib 240mg film-coated tablet (Zelboraf ) SMC No. (792/12) Roche Products Ltd. 08 November 2013 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Resubmission vemurafenib 240mg film-coated tablet (Zelboraf ) SMC No. (792/12) Roche Products Ltd. 08 November 2013 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
BRAF Genetic Testing to Select Melanoma or Glioma Patients for Targeted Therapy
 Medical Policy Manual Genetic Testing, Policy No. 41 BRAF Genetic Testing to Select Melanoma or Glioma Patients for Targeted Therapy Next Review: August 2019 Last Review: July 2018 Effective: August 1,
Medical Policy Manual Genetic Testing, Policy No. 41 BRAF Genetic Testing to Select Melanoma or Glioma Patients for Targeted Therapy Next Review: August 2019 Last Review: July 2018 Effective: August 1,
INIBITORE di BRAF nel MELANOMA
 INIBITORE di BRAF nel MELANOMA Paola Agnese Cassandrini Negrar,29 novembre 2016 BRAF is a serine/threonine protein kinasi encoded on chromosome 7q34 that activates the MAP kinase/erksegnaling pathway
INIBITORE di BRAF nel MELANOMA Paola Agnese Cassandrini Negrar,29 novembre 2016 BRAF is a serine/threonine protein kinasi encoded on chromosome 7q34 that activates the MAP kinase/erksegnaling pathway
BRAF Gene Mutation Testing To Select Melanoma Patients for BRAF Inhibitor Targeted Therapy. Original Policy Date
 MP 2.04.66 BRAF Gene Mutation Testing To Select Melanoma Patients for BRAF Inhibitor Targeted Therapy Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date
MP 2.04.66 BRAF Gene Mutation Testing To Select Melanoma Patients for BRAF Inhibitor Targeted Therapy Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date
BRAF Gene Variant Testing To Select Melanoma or Glioma Patients for Targeted Therapy
 BRAF Gene Variant Testing To Select Melanoma or Glioma Patients for Targeted Therapy Policy Number: 2.04.77 Last Review: 12/2018 Origination: 4/2013 Next Review: 12/2019 Policy Blue Cross and Blue Shield
BRAF Gene Variant Testing To Select Melanoma or Glioma Patients for Targeted Therapy Policy Number: 2.04.77 Last Review: 12/2018 Origination: 4/2013 Next Review: 12/2019 Policy Blue Cross and Blue Shield
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology
 Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Carcinoma de Tiroide: Teràpies Diana
 Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Combination Approaches in Melanoma: A Balancing Act
 Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer. Valle J et al. N Engl J Med 2010;362(14):
:") Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer Valle J et al. N Engl J Med 2010;362(14):1273-81. Introduction > Biliary tract cancers (BTC: cholangiocarcinoma, gall bladder cancer,
Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer Valle J et al. N Engl J Med 2010;362(14):1273-81. Introduction > Biliary tract cancers (BTC: cholangiocarcinoma, gall bladder cancer,
Update on Targeted Therapy in Melanoma
 Update on Targeted Therapy in Melanoma Seville June 2013 James Larkin FRCP PhD London UK Overview What are the targets in melanoma? BRAF / KIT / NRAS / GNAQ / MEK DNA / microtubules CTLA4 / PD1 / PDL1
Update on Targeted Therapy in Melanoma Seville June 2013 James Larkin FRCP PhD London UK Overview What are the targets in melanoma? BRAF / KIT / NRAS / GNAQ / MEK DNA / microtubules CTLA4 / PD1 / PDL1
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
BRAF Gene Mutation Testing to Select Melanoma Patients for BRAF Inhibitor Targeted Therapy
 Section: Medicine Effective Date: January 15, 2015 Subsection: Laboratory/Pathology Original Policy Date: March 9, 2012 Subject: BRAF Gene Mutation Testing to Select Melanoma Last Review Status/Date: December
Section: Medicine Effective Date: January 15, 2015 Subsection: Laboratory/Pathology Original Policy Date: March 9, 2012 Subject: BRAF Gene Mutation Testing to Select Melanoma Last Review Status/Date: December
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Melanoma Clinical Trials and Real World Experience
 Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
OUR EXPERIENCES WITH ERLOTINIB IN SECOND AND THIRD LINE TREATMENT PATIENTS WITH ADVANCED STAGE IIIB/ IV NON-SMALL CELL LUNG CANCER
 & OUR EXPERIENCES WITH ERLOTINIB IN SECOND AND THIRD LINE TREATMENT PATIENTS WITH ADVANCED STAGE IIIB/ IV NON-SMALL CELL LUNG CANCER Interim Data Report of TRUST study on patients from Bosnia and Herzegovina
& OUR EXPERIENCES WITH ERLOTINIB IN SECOND AND THIRD LINE TREATMENT PATIENTS WITH ADVANCED STAGE IIIB/ IV NON-SMALL CELL LUNG CANCER Interim Data Report of TRUST study on patients from Bosnia and Herzegovina
Eric Van Cutsem University Hospitals Leuven, Belgium
 BEACON CRC Study Safety Lead-in: Assessment of the BRAF Inhibitor Encorafenib + MEK Inhibitor Binimetinib + Anti Epidermal Growth Factor Receptor Antibody Cetuximab for BRAF V600E Metastatic Colorectal
BEACON CRC Study Safety Lead-in: Assessment of the BRAF Inhibitor Encorafenib + MEK Inhibitor Binimetinib + Anti Epidermal Growth Factor Receptor Antibody Cetuximab for BRAF V600E Metastatic Colorectal
pan-canadian Oncology Drug Review Final Clinical Guidance Report Trametinib (Mekinist) for Metastatic Melanoma October 22, 2013
 for Metastatic Melanoma October 22, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Trametinib (Mekinist) for Metastatic Melanoma October 22, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Trametinib (Mekinist) for Metastatic Melanoma October 22, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Supplementary Online Content
 Supplementary Online Content Jänne PA, van den Heuvel MM, Barlesi F, et al. Effect of selumetinib plus docetaxel compared with docetaxel alone and progression-free survival in patients with KRASmutant
Supplementary Online Content Jänne PA, van den Heuvel MM, Barlesi F, et al. Effect of selumetinib plus docetaxel compared with docetaxel alone and progression-free survival in patients with KRASmutant
Personalized Cancer Medicine. Conceptual,Organizational,Financial Challenges
 Personalized Cancer Medicine Conceptual,Organizational,Financial Challenges SHANGHAI 6 July, 2012 What is breast cancer? The old perception The New Family of Diseases Perception / Molecular Portraits What
Personalized Cancer Medicine Conceptual,Organizational,Financial Challenges SHANGHAI 6 July, 2012 What is breast cancer? The old perception The New Family of Diseases Perception / Molecular Portraits What
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes. Disclosures
 Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico
 Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Update on Melanoma. Main Themes
 Update on Melanoma Antoni Ribas, M.D. Professor of Medicine, Surgery, and Medical and Molecular Pharmacology University of California Los Angeles (UCLA) and the Jonsson Comprehensive Cancer Center Main
Update on Melanoma Antoni Ribas, M.D. Professor of Medicine, Surgery, and Medical and Molecular Pharmacology University of California Los Angeles (UCLA) and the Jonsson Comprehensive Cancer Center Main
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Long GV, Hauschild A, Santinami M, et al. Adjuvant dabrafenib
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Long GV, Hauschild A, Santinami M, et al. Adjuvant dabrafenib
Outcomes of Patients With Metastatic Melanoma Treated With Immunotherapy Prior to or After BRAF Inhibitors
 Outcomes of Patients With Metastatic Melanoma Treated With Immunotherapy Prior to or After BRAF Inhibitors Allison Ackerman, MD, PhD 1 ; Oliver Klein, MD 2 ; David F. McDermott, MD 1 ; Wei Wang, PhD 3
Outcomes of Patients With Metastatic Melanoma Treated With Immunotherapy Prior to or After BRAF Inhibitors Allison Ackerman, MD, PhD 1 ; Oliver Klein, MD 2 ; David F. McDermott, MD 1 ; Wei Wang, PhD 3
First-Line Ribociclib + Letrozole for Postmenopausal Women With HR+, HER2-, Advanced Breast Cancer: First Results From the Phase III MONALEESA-2 Study
 First-Line Ribociclib + Letrozole for Postmenopausal Women With HR+, HER2-, Advanced Breast Cancer: First Results From the Phase III MONALEESA-2 Study Abstract LBA1 Hortobagyi GN, Stemmer SM, Burris HA,
First-Line Ribociclib + Letrozole for Postmenopausal Women With HR+, HER2-, Advanced Breast Cancer: First Results From the Phase III MONALEESA-2 Study Abstract LBA1 Hortobagyi GN, Stemmer SM, Burris HA,
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know
 Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Horizon Scanning in Oncology
 Horizon Scanning in Oncology Trametinib for advanced or metastatic BRAF V600 mutation-positive melanoma DSD: Horizon Scanning in Oncology Nr. 34 ISSN online 2076-5940 Horizon Scanning in Oncology Trametinib
Horizon Scanning in Oncology Trametinib for advanced or metastatic BRAF V600 mutation-positive melanoma DSD: Horizon Scanning in Oncology Nr. 34 ISSN online 2076-5940 Horizon Scanning in Oncology Trametinib
Media Release. Basel, 21 July 2017
 Media Release Basel, 21 July 2017 CHMP recommends EU approval for Roche s TECENTRIQ (atezolizumab) in a specific type of metastatic lung and two types of metastatic bladder cancer TECENTRIQ as a potential
Media Release Basel, 21 July 2017 CHMP recommends EU approval for Roche s TECENTRIQ (atezolizumab) in a specific type of metastatic lung and two types of metastatic bladder cancer TECENTRIQ as a potential
Vemurafenib in metastatic melanoma patients with brain metastases: an open-label, single-arm, phase 2, multicentre study
 Annals of Oncology 28: 634 641, 2017 doi:10.1093/annonc/mdw641 Published online 19 December 2016 ORIGINAL ARTICLE Vemurafenib in metastatic melanoma patients with brain metastases: an open-label, single-arm,
Annals of Oncology 28: 634 641, 2017 doi:10.1093/annonc/mdw641 Published online 19 December 2016 ORIGINAL ARTICLE Vemurafenib in metastatic melanoma patients with brain metastases: an open-label, single-arm,
Cancer Treatments Subcommittee of PTAC Meeting held 22 April (minutes for web publishing)
") Cancer Treatments Subcommittee of PTAC Meeting held 22 April 2016 (minutes for web publishing) Cancer Treatments Subcommittee minutes are published in accordance with the Terms of Reference for the Pharmacology
Cancer Treatments Subcommittee of PTAC Meeting held 22 April 2016 (minutes for web publishing) Cancer Treatments Subcommittee minutes are published in accordance with the Terms of Reference for the Pharmacology
BRAF inhibitors Anti-angiogenic therapy Other molecular targets Discussion
 If you experience any technical difficulties call 8-274-939 or e-mail informed@commpartners.com Slides will advance automatically. You can also advance/ review the presentation using the control buttons
If you experience any technical difficulties call 8-274-939 or e-mail informed@commpartners.com Slides will advance automatically. You can also advance/ review the presentation using the control buttons
ESMO GI / BEACON CRC SAFETY LEAD-IN ENCORE PRESENTATION June 23, 2018
 ESMO GI / BEACON CRC SAFETY LEAD-IN ENCORE PRESENTATION June 23, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
ESMO GI / BEACON CRC SAFETY LEAD-IN ENCORE PRESENTATION June 23, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
CombiRT in Metastatic Melanoma Trial
 CombiRT in Metastatic Melanoma Trial An open-label, single-arm, phase I/II, multicenter study to evaluate the safety and efficacy of the combination of dabrafenib, trametinib and palliative radiotherapy
CombiRT in Metastatic Melanoma Trial An open-label, single-arm, phase I/II, multicenter study to evaluate the safety and efficacy of the combination of dabrafenib, trametinib and palliative radiotherapy
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove)
") Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Innovations in Immunotherapy - Melanoma. Systemic Therapies October 27, 2018 Charles L. Bane, MD
 Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
BCCA Protocol Summary for the Treatment of BRAF V600 Mutation- Positive Unresectable or Metastatic Melanoma using vemurafenib and cobimetinib
 BCCA Protocol Summary for the Treatment of BRAF V600 Mutation- Positive Unresectable or Metastatic Melanoma using vemurafenib and cobimetinib Protocol Code Tumour Group Contact Physician USMAVVC Skin and
BCCA Protocol Summary for the Treatment of BRAF V600 Mutation- Positive Unresectable or Metastatic Melanoma using vemurafenib and cobimetinib Protocol Code Tumour Group Contact Physician USMAVVC Skin and
Melanoma BRAF mutado y terapias dirigidas. Javier Medina Martínez Hospital Virgen de la Salud, Toledo
 Melanoma BRAF mutado y terapias dirigidas Javier Medina Martínez Hospital Virgen de la Salud, Toledo Enfermedad avanzada: Seguimiento a largo plazo Retratamiento Metástasis cerebrales Adyuvancia November-2017
Melanoma BRAF mutado y terapias dirigidas Javier Medina Martínez Hospital Virgen de la Salud, Toledo Enfermedad avanzada: Seguimiento a largo plazo Retratamiento Metástasis cerebrales Adyuvancia November-2017
K-Ras signalling in NSCLC
 Targeting the Ras-Raf-Mek-Erk pathway Egbert F. Smit MD PhD Dept. Pulmonary Diseases Vrije Universiteit VU Medical Centre Amsterdam, The Netherlands K-Ras signalling in NSCLC Sun et al. Nature Rev. Cancer
Targeting the Ras-Raf-Mek-Erk pathway Egbert F. Smit MD PhD Dept. Pulmonary Diseases Vrije Universiteit VU Medical Centre Amsterdam, The Netherlands K-Ras signalling in NSCLC Sun et al. Nature Rev. Cancer
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Corporate Medical Policy
 Corporate Medical Policy BRAF Gene Variant Testing to Select Melanoma or Glioma Patients File Name: Origination: Last CAP Review: Next CAP Review: Last Review: braf_gene_variant_testing_to_select_melanoma_or_glioma_patients_for_targeted_
Corporate Medical Policy BRAF Gene Variant Testing to Select Melanoma or Glioma Patients File Name: Origination: Last CAP Review: Next CAP Review: Last Review: braf_gene_variant_testing_to_select_melanoma_or_glioma_patients_for_targeted_
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
The Biology and Therapeutic Approach to BRAF-Mutant Cutaneous Melanoma
 The Biology and Therapeutic Approach to BRAF-Mutant Cutaneous Melanoma Kevin Wood, MD, and Jason Luke, MD, FACP Abstract Knowledge regarding the biology and therapeutic value of BRAF mutations in melanoma
The Biology and Therapeutic Approach to BRAF-Mutant Cutaneous Melanoma Kevin Wood, MD, and Jason Luke, MD, FACP Abstract Knowledge regarding the biology and therapeutic value of BRAF mutations in melanoma
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Array BioPharma Third Quarter of F2018 Update MAY 9, 2018
 Array BioPharma Third Quarter of F2018 Update MAY 9, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions of the
Array BioPharma Third Quarter of F2018 Update MAY 9, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions of the
Initial Results from an Open-label, Doseescalation Phase I Study of the Oral BRAF Inhibitor LGX818 in BRAF V600 mutant Advanced Melanoma
 Initial Results from an Open-label, Doseescalation Phase I Study of the Oral BRAF Inhibitor LGX818 in BRAF V600 mutant Advanced Melanoma Reinhard Dummer, 1 Caroline Robert, 2 Marta Nyakas, 3 Grant McArthur,
Initial Results from an Open-label, Doseescalation Phase I Study of the Oral BRAF Inhibitor LGX818 in BRAF V600 mutant Advanced Melanoma Reinhard Dummer, 1 Caroline Robert, 2 Marta Nyakas, 3 Grant McArthur,
The changing landscape of medical management of stage III and IV melanoma Current treatments and what s on the horizon
 The changing landscape of medical management of stage III and IV melanoma Current treatments and what s on the horizon Samantha Bowyer Medical Oncologist Rockingham General Hospital Historical perspective
The changing landscape of medical management of stage III and IV melanoma Current treatments and what s on the horizon Samantha Bowyer Medical Oncologist Rockingham General Hospital Historical perspective
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Array BioPharma Second Quarter of F2018 Update FEBRUARY 6, 2018
 Array BioPharma Second Quarter of F2018 Update FEBRUARY 6, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
Array BioPharma Second Quarter of F2018 Update FEBRUARY 6, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
Trabectedin in ASTS. Le Cesne A, et al. J Clin Oncol. 2018;36(suppl): Abstract
: Abstract") Results of a Prospective Randomized Phase III T-SAR Trial Comparing Trabectedin vs Best Supportive Care (BSC) in Patients With Pretreated Advanced Soft Tissue Sarcoma (ASTS) Abstract 11508 Le Cesne A,
Results of a Prospective Randomized Phase III T-SAR Trial Comparing Trabectedin vs Best Supportive Care (BSC) in Patients With Pretreated Advanced Soft Tissue Sarcoma (ASTS) Abstract 11508 Le Cesne A,
Modern therapy in oncology Metastatic melanoma
 Modern therapy in oncology Metastatic melanoma Anna Buda-Nowak Oncology Department; University Hospital in Cracow Melanoma Malignant skin neoplasm derived from neuroectodermal melanomatous cells. The incidence:
Modern therapy in oncology Metastatic melanoma Anna Buda-Nowak Oncology Department; University Hospital in Cracow Melanoma Malignant skin neoplasm derived from neuroectodermal melanomatous cells. The incidence:
Targe:ng HER2 in Metasta:c Breast Cancer in 2014
 Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer