Medical Treatment for Melanoma Sanjiv S. Agarwala, MD
|
|
|
- Gwenda Bradley
- 5 years ago
- Views:
Transcription
1 Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA
2 Disclosures None
3 Overview Current Therapy for Metastatic Disease Immunotherapy Targeted Therapy Current Status of Adjuvant Therapy
4 Transforming the Landscape Immunotherapy Target host Hit a Target Targeted Therapy Target tumor
5 Current Therapeutic Options for Patients with Metastatic Melanoma For BRAF-WT Patients Immunotherapy Monotherapy or combination? For BRAF+ Patients Immunotherapy or targeted therapy What is the correct sequence?
6 Current Therapeutic Options for Patients with Metastatic Melanoma For BRAF-WT Patients Immunotherapy Monotherapy or combination? For BRAF+ Patients Immunotherapy or targeted therapy What is the correct sequence?
7 Targeted Immunotherapy = Checkpoint Inhibitors
8 What is a Check-Point?







9 T-Cell Activity Is Regulated By Immune Checkpoints to Limit Autoimmunity 1 Dendritic cell TUMOR Inactivated T cell Immune checkpoints, such as CTLA-4, PD-1, LAG-3, and TIM-3 function at different phases in the immune response to regulate the duration and level of the T- cell response. - - Checkpoints CTLA-4 = cytotoxic T-lymphocyte antigen 4; PD-1 = programmed cell death protein 1; LAG-3 = lymphocyte activation gene 3; TIM-3 = T-cell immunoglobulin and mucin protein Pardoll DM. Nat Rev Cancer. 2012;12: Activated T cell Checkpoints LYMPH NODE Inactivated T cell
10 What is a Check-Point Inhibitor?







11 Immunotherapy Immune System Cytokines Antigens Regulatory molecules (CTLA-4, PD-1)
12 Check-Point Inhibitors Approved for Melanoma Anti CTLA4 (ipilimumab) Anti PD-1 (pembrolizumab, nivolumab) Combination anti CTLA-4 and anti-pd1 (ipilimumab and nivolumab)
13 Clinical Results with Ipilimumab (2 nd and 1st line) Ipilimumab vs vaccine and Ipi + DTIC vs DTIC HR: 0.66 and 0.68 Pre-treated pts Ipi 3 mg/kg +/- gp100 HR: 0.72 First line Ipi 10 mg/kg + DTIC Hodi FS, et al. N Engl J Med. 2010;363: Robert C, et al. N Engl J Med. 2011;364:
14 Overall Survival (%) Immune Checkpoint Inhibitors Provide Durable Long-term Survival for Patients with Advanced Melanoma IPI (Pooled analysis) 1 N=1, Years 1. Schadendorf et al. J Clin Oncol 2015;33: ; 2. Current analysis; 3. Poster presentation by Dr. Victoria Atkinson at SMR 2015 International Congress. 14
15 Ipilimumab became the standard of care in 2011 But can we do better?

 Line")




16 Keynote-006 Front-line Pembrolizumab vs Ipilimumab Patients Unresectable, stage III or IV melanoma 1 prior therapy, excluding anti CTLA-4, PD-1, or PD-L1 agents Known BRAF status b ECOG PS 0-1 No active brain metastases No serious autoimmune disease Stratification factors: ECOG PS (0 vs 1) Line of therapy (first vs second) PD-L1 status (positive c vs negative) R 1:1:1 Pembrolizumab 10 mg/kg IV Q2W Pembrolizumab 10 mg/kg IV Q3W Ipilimumab 3 mg/kg IV Q3W x 4 doses Primary end points: PFS and OS Secondary end points: ORR, duration of response, safety a Patients enrolled from 83 sites in 16 countries. b Prior anti-braf targeted therapy was not required for patients with normal LDH levels and no clinically significant tumor-related symptoms or evidence of rapidly progressing disease. c Defined as membranous PD-L1 expression in 1% of tumor cells as assessed by IHC using the 22C3 antibody.

17 Tumor Response (irrc, investigator)
18 OS (%) PFS (%) Kaplan-Meier Estimates of Survival (Median Follow-Up, 33.9 mo) No Risk Pembro Overall Survival Events, n HR (95% CI) Median, mo (95% CI) Pembrolizumab , ( ) 32.3 (24.5-NR) Ipilimumab ( ) Months 55% 42% % 39% Pembro Ipilimumab Ipilimumab PFS per irrc by Investigator Events, n HR (95% CI) Median, mo (95% CI) Pembrolizumab , ( ) 8.3 ( ) Ipilimumab ( ) Months 34% 15% % 14% Adapted from Robert C, et al. ASCO Abstract 9504.
19 Slide 14
20 Slide 15
21 Slide 16
22 Anti PD-1 is better than ipilimumab frontline and responses are durable even after stopping treatment But what about combining CTLA-4 and PD-1?

23 Slide 6 Presented By Jedd Wolchok at 2015 ASCO Annual Meeting
24 Updated Response To Treatment NIVO+IPI (N=314) NIVO (N=316) IPI (N=315) ORR, % (95% CI)* 58.9 ( ) 44.6 ( ) 19.0 ( ) Best overall response % Complete response Partial response Stable disease Progressive disease Unknown Median duration of response, months (95% CI) NR (NR NR) 31.1 (31.1 NR) 18.2 (8.3 NR) *By RECIST v1.1; NR = not reached. At the 18-month DBL, the CR rate for NIVO+IPI, NIVO and IPI was 12.1%, 9.8% and 2.2%, respectively Database lock: Sept 13, 2016, minimum f/u of 28 months 24
25 Progression-free Percentage Survival of PFS (%) Updated Progression-Free Survival Median PFS, mo (95% CI) HR (95% CI) vs. IPI HR (95% CI) vs. NIVO 50% 43% NIVO+IPI (N=314) NIVO (N=316) IPI (N=315) 11.7 ( ) 0.42 ( ) 0.76 ( ) 43% 37% 6.9 ( ) 0.54 ( ) 2.9 ( ) NIVO+IPI NIVO 18% IPI 12% Months Patients at risk: NIVO+ IPI NIVO IPI Database lock: Sept 13, 2016, minimum f/u of 28 months 7
26 Updated Survival Data in CheckMate-067 Trial of IPI vs. NIVO vs. IPI/NIVO Median OS, months (95% CI) HR (99.5% CI) vs. IPI HR (99.5% CI) vs. NIVO NIVO + IPI (N=314) NIVO (N=316) IPI (N=315) NR 0.55 ( )* 0.88 ( ) NR (29.1-NR) 0.63 ( )* 20 ( ) *P< Larkin J, et al. AACR Abstract CT075. Database lock: September 13, Minimum follow-up of 28 months
27 Decision Point. Immunotherapy PD-1 alone PD-1/CTLA-4 Combination
28 Checkmate 067: Safety Summary With an additional 19 months of follow-up, safety was consistent with the initial report 1 NIVO+IPI (N=313) NIVO (N=313) IPI (N=311) Patients reporting event, % Any Grade Grade 3-4 Any Grade Grade 3-4 Any Grade Grade 3-4 Treatment-related adverse event (AE) Treatment-related AE leading to discontinuation Treatment-related death, n (%) 2 (0.6) a 1 (0.3) b 1 (0.3) b Most select AEs were managed and resolved within 3-4 weeks (85 100% across organ categories) ORR was 70.7% for pts who discontinued NIVO+IPI due to AEs, with median OS not reached a Cardiomyopathy (NIVO+IPI, n=1); Liver necrosis (NIVO+IPI, n=1). Both deaths occurred >100 days after the last treatment. b Neutropenia (NIVO, n=1); colon perforation (IPI, n=1) Larkin J, et al. NEJM 2015;373:
29 Checkmate 067: Safety Onset Grade 3 4 Treatment-Related Select AEs Skin (n=18) Skin (n=5) Gastrointestinal (n=46) Gastrointestinal (n=7) Endocrine (n=15) Endocrine (n=2) Hepatic (n=60) 14.1 ( ) Longer Time to Resolution Hepatic (n=8) 3.7 ( ) Pulmonary (n=3) 6.7 ( ) Pulmonary (n=1) Renal (n=6) 5.6 ( ) 7.4 ( ) 19.4 ( ) 26.3 ( ) 12.1 ( ) Toxicity Earlier 28.6 ( ) 7.4 ( ) 11.3 ( ) 50.9 ( ) NIVO+IPI NIVO Renal (n=1) Weeks Circles represent medians; bars signify ranges Larkin J et al ECC 2015
30
31 Can a biomarker help us decide?




32 ORR, % (95% CI) Keynote 001 Pembrolizumab PD-L1 Expression and Response ORR, RECIST v PD-L1 Negative 0% Staining APS = 0 APS, Allred proportion score. Analysis cut-off date: October 18, PD-L1 Positive 1-10% Staining APS = 2 PD-L1 Positive 10-33% Staining APS = 3 PD-L1 Positive % Staining APS = 5 0 APS 0 n = 28 APS 1 n = 24 Negative APS 2 n = 72 APS 3 n = 54 Positive APS 4 n = 32 APS 5 n = 34 Daud A et al, ASCO 2015
33 OS (%) OS by Tumor PDL-1 Expression at a 1% Cutoff OS (%) PD-L1 Expression Level <1% PD-L1 Expression Level 1% <1% PD-L1 NIVO+IPI NIVO IPI 1% PD-L1 NIVO+IPI NIVO IPI Median OS, mo (95% CI) NR (26.5 NR) 23.5 (13.0 NR) 18.6 ( ) Median OS, mo (95% CI) NR NR 22.1 ( ) 100 HR (95% CI) vs NIVO 0.74 ( ) 100 HR (95% CI) vs NIVO 1.03 ( ) % 49% 41% % 67% 48% ORR of 54.5% for NIVO+IPI and 35.0% for NIVO 10 ORR of 65.2% for NIVO+IPI and 55.0% for NIVO Months Patients at risk: NIVO+IPI NIVO IPI Months Patients at risk: NIVO+IPI NIVO IPI
34 PFS and OS Subgroup Analyses (All Randomized Patients) Descriptive comparison between NIVO+IPI and NIVO Patients Unstratified Hazard Ratio Unstratified Hazard Ratio (95% CI) Subgroup NIVO+IPI NIVO PFS OS PFS OS Overall <65 years years BRAF Mutant BRAF Wild-type ECOG PS = ECOG PS = M0/M1a/M1b M1c LDH ULN LDH > ULN LDH > 2 x ULN PD-L1 5% PD-L1 <5% NIVO+IPI NIVO NIVO+IPI NIVO 2 34
35 Current Therapeutic Options for Patients with Metastatic Melanoma For BRAF-WT Patients Immunotherapy Monotherapy or combination? For BRAF+ Patients Immunotherapy or targeted therapy What is the correct sequence?
 B-RAF: 50% c-kit: 5-10% c-kit: 10-20%")
36 Melanoma is not one disease (Curtin et al, N Engl J Med 353: , 2005) B-RAF: 50% c-kit: 5-10% c-kit: 10-20% c-kit:15-30%
37 MAPK Pathway Growth Factors RAS BRAF MEK ERK Cell proliferation and survival
38 BRAF Mutation Growth Factors RAS BRAF BRAF mutation is present in ~50% of melanomas MEK ERK Increased cell proliferation and survival
39 MAPK Pathway Targeted Therapy BRAFi (dabrafenib) PFS HR, 0.37 vs DTIC 1 Hyperproliferative skin AEs BRAFi (vemurafenib) PFS HR, 0.38 vs DTIC 2 Hyperproliferative skin AEs PFS HR, 0.45 vs chemotherapy 3 MEKi (trametinib) RAS mutbraf MEK perk Proliferation, Survival, Invasion, Metastasis BRAFi + MEKi ph III studies Dabrafenib + trametinib (D + T) PFS HR, 0.67 vs dabrafenib 4 OS HR, 0.71 vs dabrafenib 4 PFS HR, 0.56 vs vemurafenib 5 OS HR, 0.69 vs vemurafenib 5 Vemurafenib + cobimetinib PFS HR, 0.58 vs vemurafenib 6 OS HR, 0.70 vs vemurafenib 6 Decreased hyperproliferative skin AEs 4,5,6 1. Hauschild A, et al. Lancet. 2012;380(9839): McArthur GA, et al. Lancet Oncol. 2014;15(3): Flaherty KT, et al. N Engl J Med. 2012;367(2): Long GV, et al. Lancet. 2015;386(9992): Robert C, et al. N Engl J Med. 2015;372(1): Atkinson V, et al. Presented at:society for Melanoma Research 2015 Congress.
40 Decision Point. BRAF mutation test BRAF V600 mutation negative Immunotherapy Immunotherapy Or BRAF V600 mutation positive MAP-K Targeted Therapy
41 Slide 34 Presented By Axel Hauschild at 2014 ASCO Annual Meeting

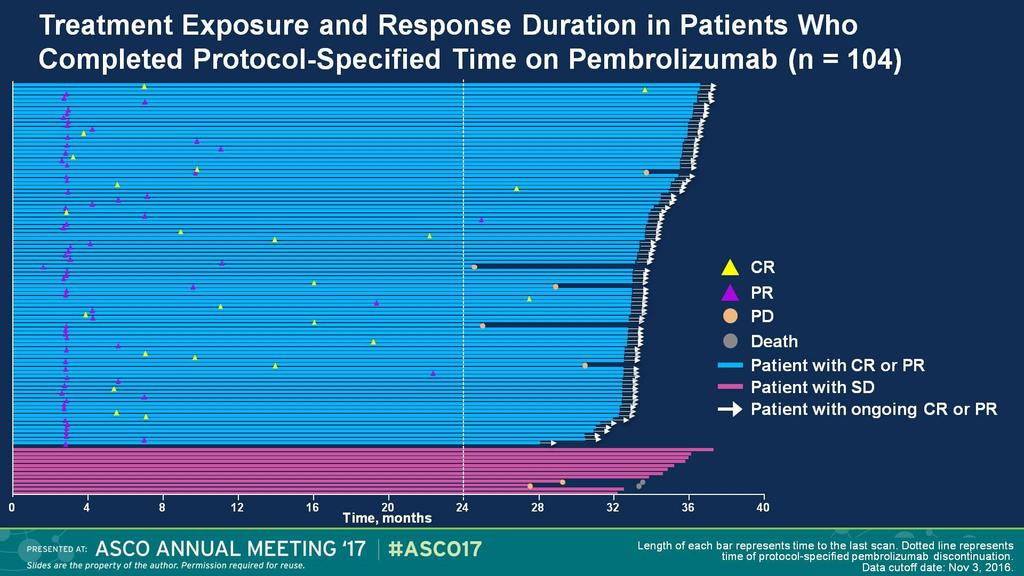
42 Dabrafenib + Trametinib: Long Term FU Part C: Study Design (phase 2)
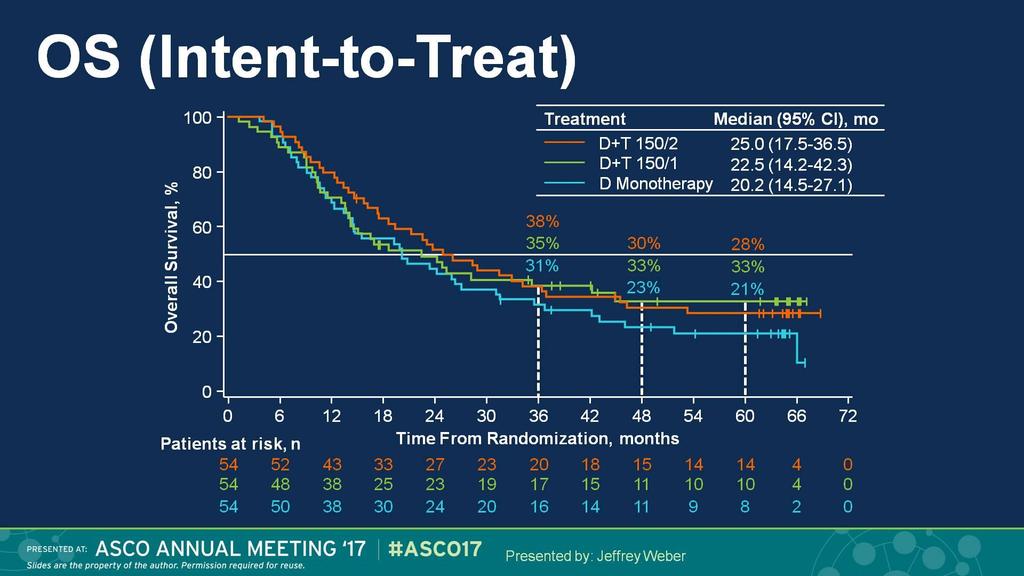
43 OS (Intent-to-Treat)
44 Pembro Keynote 001: 4 Year OS
45 Phase III KEYNOTE-006: PFS in Prespecified Subgroups Overall Male Female Age <65 y Age 65 y White race US Rest of world ECOG PS ECOG PS Favors Pembro Hazard Ratio Pembrolizumab Q2W vs ipilimumab Analysis cut-off date: September 3, Favors IPI First-line therapy Second-line therapy PD-L1 positive PD-L1 negative BRAF wild type BRAF mutant, 95 prior anti-braf 96 BRAF mutant, no prior anti-braf No prior immunotherapy Pembrolizumab Q3W vs ipilimumab Favors Pembro Hazard Ratio Favors IPI
46 Change From Baseline, % KEYNOTE-001: Phase I RECIST Response (v1.1) Total population n=581 ORR 33% CR 8% 71% IPI-T IPI-N Treatment naïve n=152 ORR 45% CR 14% 80% 2 mg/kg Q3W 10 mg/kg Q3W 10 mg/kg Q2W Median Change: 36% Median Change: 54% Analysis cut-off date: October 18, 2014; Median follow up 21 mo Daud A et al ASCO 2015
47 BRAF Inhibitors Second line Vemurafenib 1 Dabrafenib 2 Phase RR 56% 57% 57% 56% 59% 59% PFS OS Chapman PB, et al. N Engl J Med 2011;364: (updated Chapman et al. ASCO 2012); Sosman JA, et al. N Engl J Med 2012;366: ; 2. Hauschild A, et al. Lancet 2012;380: (updated Hauschild et al. ASCO 2013); Ascierto PA, et al. J Clin Oncol 2013; 31:
48 Progression-Free Survival, % D+T: Long Term FU LDH < ULN and < 3 metastatic sites (ITT) Overall Survival, % Progression-Free Survival Overall Survival % 40 25% 25% % 57% 60 51% 58% 40 42% 31% % 8% 8% Patients at risk, n Time From Randomization, months Patients at risk, n Time From Randomization, months PRESENTED BY J WEBER AT ASCO 2017
49 Contemplating the Options EA6134 Anti-PD1 therapy BRAF-targeted therapy
50 Will sequence not matter in the future??
51 Percent alive Percent alive Percent alive Combining Targeted Therapy With Immunotherapy BRAF inhibitor alone or BRAF + MEK inhibitors rapid and clinically significant responses Immunotherapy less frequent objective responses, but clinically significant durability Combining targeted therapy with immunotherapy Can harness and perpetuate the enhanced anti-tumor response following targeted inhibition May lead to durable response and prolonged survival Melanoma survival curves depending on the type of therapy Targeted therapy Immunotherapy Combination? Years Years Years Figure modified from Ribas A et al. Clin Cancer Res 2012 and Hamid O et al. SMR 2015.


52 Targeted-Immuno Triplets: BRAF + MEK + PD1/L1 Dabrafenib+Trametinib +Durvalumab Dabrafenib+Trametinib +Pembrolizumab Vemurafenib+Cobimetinib +Atezolizumab 100 Multiple Triplet Combinations Launching Into Phase III: Dabrafenib + Trametinib + Pembrolizumab Dabrafenib + Trametinib + PDR Vemurafenib + Cobimetinib + Atezolizumab Time, weeks Change From Baseline in Sum of Longest Diameter of Target Lesion, % Change From Baseline, % Ribas et al. ASCO 2015 Ribas et al. ASCO 2016 Hwu et al. ECCO 2016
53 Overview Current Therapy for Metastatic Disease Immunotherapy Targeted Therapy Current Status of Adjuvant Therapy
54 Distribution of Melanoma Burden by Stage Unresectable Stage III, IV Intermediate and high-risk resectable Stage IIB, IIC, III Systemic Therapy Adjuvant Therapy Low risk resectable MIS Stage IA, IB, IIA Prevention The burden of high risk disease dwarfs that of advanced melanoma and is an important clinical problem
55 Adjuvant Therapy The Old Interferon The New Ipilimumab The Future
56 Adjuvant IFN-α Regimens Schedule Dose Frequency Duration Low Dose Intermediate Dose 3 MIU 3 x weekly months Induction 10 MIU 5 x weekly 4 weeks Maintenance 10 MIU 3 x weekly months High Dose 5 MIU 3 x weekly 24 months Induction 20 MIU/m 2 5 x weekly 4 weeks Maintenance 10 MIU/m 2 3 x weekly 11 months Short Course Induction X 1 20 MIU/m 2 5 x weekly 4 weeks Intermittent Induction X 3 20 MIU/m 2 20 MIU/m 2 5 x weekly for 4 weeks Q 4 months
57 Proportion alive and relapse-free E1684: Updated Efficacy (ITT at 12.6 yr Median Follow-up) Relapse-Free Survival Log-rank test: P 2 =.02; P 1 =.01 Treatment groups (N = 286) High-dose IFN Observation Time, yr Overall Survival Log-rank test: P 2 =.18; P 1 =.09. Treatment groups (N = 286) High-dose IFN Observation Time, yr Observation High-dose IFN Total Dead or relapsed Alive or relapsed-free Median Observation High-dose IFN Total Dead Alive Median
58 Tweaking Interferon Shorten the duration of HDI high dose IV only Use pegylated IFN once weekly dosing, lower dose with comparable AUC
59 Study design: ECOG 1697 Patients with intermediateand high-risk melanoma Defined as T3: Breslow thickness 6th ed) >1.5 mm (AJCC >2.0 mm (AJCC 7th ed) or Any thickness with microscopically positive nodal disease (N1a N2a) R A N D O M I Z A T I O N 1:1 Postoperative adjuvant IFN alfa-2b 20 MU/m 2 /day for 5 days/week 4 weeks Observation Agarwala SS et al. J Clin Oncol March 2017
60 E1697 Induction Only HD IFN vs Observation Agarwala SS et al: Journal of Clinical Oncology 35, no. 8 (March 2017)
61 EORTC (PEG-IFN): Design Patients (n=1,256): Resected TxN1-2M0 melanoma, within 7 weeks of lymphadenectomy Randomization Observation Stratified by: Microscopic (N1) vs. palpable (N2) 1 vs. 2-4 vs. 5+ nodes Breslow Ulceration Gender Site Peg-IFN alfa-2b Induction (8 weeks) 6 µg/kg/week Maintenance (5 years or distant metastasis) 3 µg/kg/week Dose reduction to 3, 2, 1 to maintain performance status Primary Endpoints: Relapse-free survival (RFS) Distant metastasis-free survival (DMFS)
62 Patients Alive Without Relapse (%) EORTC 18991: RFS Observation Peg-IFN- 2b 4-yr rate (SE) 38.9% (2.2) 45.6% (2.2) Median (mos) p =.01 HR = 0.82 (95% CI 0.71, 0.96) (yrs) O N No. Patients At Risk Peg-IFN- 2b Observation Eggermont et al, 2008.
63 Adjuvant Therapy The Old Interferon The New Ipilimumab The Future
64 Ipilimumab in Melanoma Standard Dose 3mg/kg Approved in metastatic melanoma High Dose 10mg/kg Approved in adjuvant therapy of melanoma
65 Ipilimumab (HD) vs Placebo EORTC 18071/CA : Study Design High-risk, stage III, completely resected melanoma N=951 R N=475 N=476 INDUCTION Ipilimumab 10 mg/kg Q3W X4 INDUCTION Placebo Q3W X4 Week 1 Week 12 Week 24 MAINTENANCE Ipilimumab 10 mg/kg Q12W up to 3 years MAINTENANCE Placebo Q12W up to 3 years Treatment up to a maximum 3 years, or until disease progression, intolerable toxicity, or withdrawal Stratification factors: Stage (IIIA vs IIIB vs IIIC 1-3 positive lymph nodes vs IIIC 4 positive lymph nodes) Regions (North America, European countries and Australia) Eggermont et al Lancet Onc 16:
66 Primary Endpoint: Recurrence-free Survival (IRC) Patients Alive Without Relapse (%) Patients at Risk Ipilimumab Placebo Median: 17.1 mo Ipilimumab 10 mg/kg Placebo Ipilimum ab Placebo Events/patients 234/ /476 HR (95% CI)* 0.75 ( ) Log-rank P value* Year RFS rate (%) Year RFS rate (%)** *Stratified by stage. **Data are not yet mature. Median: 26.1 mo Months Eggermont et 66 al Lancet Oncol 16:522-30,
67 Patients alive (%) EORTC 18071: Overall Survival CI = confidence interval; NR = not reached. 5-year difference 11% Ipilimumab Placebo Deaths/patients 162 / / 476 Hazard ratio (95.1% CI)* 0.72 ( ) Log-rank P value* % 54% Years O N Number of patients at risk : *Stratified by stage at randomization Ipilimumab Placebo Eggermont AMM et al NEJM 2016
68 Safety Summary Ipilimumab (n = 471) Any Grade 3/4 Grade Placebo (n = 474) Any Grade 3/4 grade Any AE, % Treatment-related AE, % Treatment-related AE discontinuation, % Any immune-related AE, % No new deaths due to drug-related AEs compared with the primary analysis o 5 patients (1.1%) in the ipilimumab group 3 patients with colitis (2 with gastrointestinal perforations) 1 patient with myocarditis 1 patient had multiorgan failure with Guillain-Barré syndrome o No deaths related to study drug in the placebo group 68
69 E1609 Phase III Ipilimumab Patients with resectable stage IIIB or IIIC or IV (M1a or M1b) N= R A N D O M I Z E Ipilimumab 10mg/kg Ipilimumab 3mg/kg High dose interferon Primary Endpoint: RFS, OS Secondary Endpoints: Safety, Quality of life, immunologic correlates of RFS, OS Completed accrual: 8/2014- Results anticipated: 2018 Study Chair: A Tarhini Clinicaltrials.gov

70 RFS: Ipi10 vs. Ipi3<br />(Concurrently randomized patients)<br />
71 Slide 15

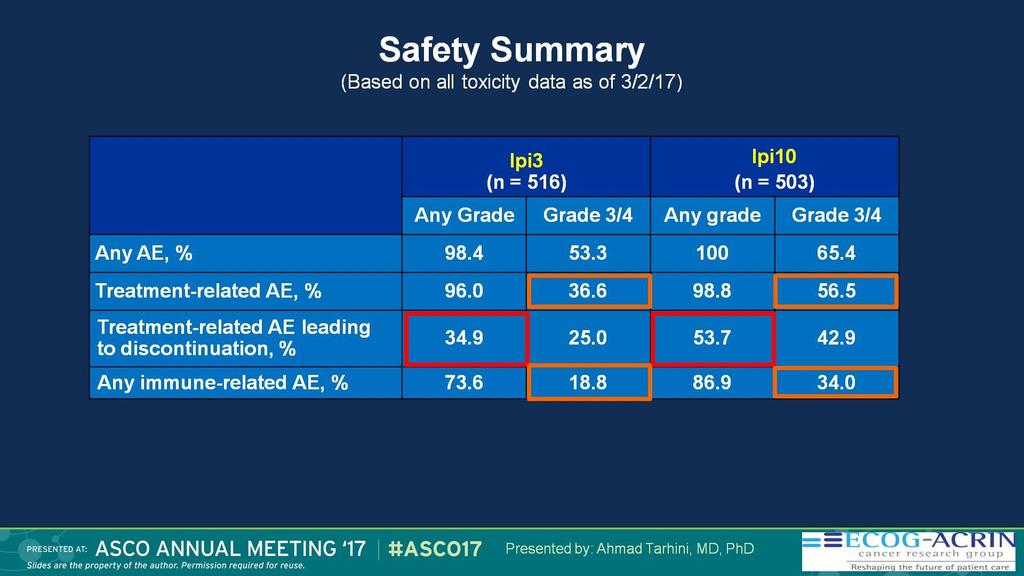
72 Treatment Related Deaths
73 Adjuvant Therapy The Old Interferon The New Ipilimumab The Future
74 The Future Anti PD-1 antibodies are better than anti CTLA-4 in metastatic melanoma Makes sense to test them in adjuvant therapy What about BRAF+ patients?
75 CA : CA : Study Design Patients with high-risk, completely resected stage IIIB/IIIC or stage IV melanoma 1:1 n = 453 n = 453 Stratified by: 1) Disease stage: IIIB/C vs IV M1a-M1b vs IV M1c 2) PD-L1 status at a 5% cutoff in tumor cells NIVO 3 mg/kg IV Q2W and IPI placebo IV Q3W for 4 doses then Q12W from week 24 IPI 10 mg/kg IV Q3W for 4 doses then Q12W from week 24 and NIVO placebo IV Q2W Follow-up Maximum treatment duration of 1 year Enrollment period: March 30, 2015 to November 30,
76 RFS (%) Primary Endpoint: RFS 100 NIVO IPI Events/patients 154/ / Median (95% CI) NR NR (16.6, NR) HR (97.56% CI) 0.65 (0.51, 0.83) 80 Log-rank P value < % 61% 66% 53% NIVO IPI Number of patients at risk NIVO IPI Months
77 Safety Summary NIVO (n = 452) IPI (n = 453) AE, n (%) Any grade Grade 3/4 Any grade Grade 3/4 Any AE 438 (97) 115 (25) 446 (98) 250 (55) Treatment-related AE 385 (85) 65 (14) 434 (96) 208 (46) Any AE leading to discontinuation Treatment-related AE leading to discontinuation 44 (10) 21 (5) 193 (43) 140 (31) 35 (8) 16 (4) 189 (42) 136 (30) There were no treatment-related deaths in the NIVO group There were 2 (0.4%) treatment-related deaths in the IPI group (marrow aplasia and colitis), both >100 days after the last dose 77
78 EORTC 1325/ KEYNOTE 054
79 Adjuvant Targeted Therapy
80 Key eligibility criteria Completely resected, high-risk stage IIIA (lymph node metastasis > 1 mm), IIIB, or IIIC cutaneous melanoma BRAF V600E/K mutation Surgically free of disease 12 weeks before randomization ECOG performance status 0 or 1 No prior radiotherapy or systemic therapy Stratification BRAF mutation status (V600E, V600K) Disease stage (IIIA, IIIB, IIIC) COMBI-AD: STUDY DESIGN R A N D O M I Z A T I O N N = 870 1:1 Treatment: 12 months a Dabrafenib 150 mg BID + trametinib 2 mg QD (n = 438) 2 matched placebos (n = 432) Follow-up b until end of study c Primary endpoint: RFS d Secondary endpoints: OS, DMFS, FFR, safety BID, twice daily; DMFS, distant metastasis free survival; ECOG, Eastern Cooperative Oncology Group; FFR, freedom from relapse; OS, overall survival; QD, once daily; RFS, relapse-free survival. a Or until disease recurrence, death, unacceptable toxicity, or withdrawal of consent; b Patients were followed for disease recurrence until the first recurrence and thereafter for survival; c The study will be considered complete and final OS analysis will occur when 70% of randomized patients have died or are lost to follow-up; d New primary melanoma considered as an event. 80
81 Proportion Alive and Relapse Free RELAPSE-FREE SURVIVAL (PRIMARY ENDPOINT) 1 y, 88% y, 56% 2 y, 67% P = y, 58% Group Dabrafenib plus trametinib Events, n (%) 166 (38) Placebo 248 (57) Median (95% CI), mo NR (44.5-NR) 16.6 ( ) HR (95% CI) 0.47 ( ); P < y, 44% 3 y, 39% No. at Risk Dabrafenib plus trametinib Placebo NR, not reached Months From Randomization
82 Proportion Alive OVERALL SURVIVAL (FIRST INTERIM ANALYSIS) 1 y, 97% 1 y, 94% 2 y, 91% 2 y, 83% 3 y, 86% 3 y, 77% Group Dabrafenib plus trametinib Events, n (%) 60 (14) Placebo 93 (22) Median (95% CI), mo NR (NR-NR) NR (NR-NR) HR (95% CI) 0.57 ( ); P =.0006 a No. at Risk Months From Randomization Dabrafenib plus trametinib Placebo a Prespecified significance boundary (P = ). 82
83 Conclusions: Metastatic Monotherapy or combination immunotherapy are both appropriate options for all patients Anti-PD1 is better than anti-ctla4 Improved RR, PFS and OS Less toxicity Combination anti-ctla4 and anti-pd1 has higher RR and PFS compared to anti-pd1 but not improved OS and higher toxicity
84 Conclusions: Adjuvant Therapy IFN is in retirement phase Ipilimumab high-dose is FDA-approved but should not be used PD-1 beats ipilimumab BRAF/MEK combo for BRAF+ patients
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know
 Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
MELANOMA: THE BEST OF THE YEAR Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone
 MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
New Therapeutic Approaches to Malignant Melanoma
 2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD
 Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer
Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer
Who is the Ideal Candidate for PEG Intron?
 Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology
 Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
ASCO 2014: The Future is Here. What I Will Talk About. George W. Sledge MD Stanford University School of Medicine
 ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
Immunotherapy for Melanoma. Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France
 Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
What we learned from immunotherapy in the past years
 What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Clinical Trials and Real World Experience
 Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
Adjuvant Therapy of High Risk Melanoma
 Adjuvant Therapy of High Risk Melanoma William Sharfman, MD, FACP Associate Professor of Oncology and Dermatology Johns Hopkins University School of Medicine July 5, 2012 Adjuvant options for Stage IIB/C
Adjuvant Therapy of High Risk Melanoma William Sharfman, MD, FACP Associate Professor of Oncology and Dermatology Johns Hopkins University School of Medicine July 5, 2012 Adjuvant options for Stage IIB/C
Treatment and management of advanced melanoma: Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC
 Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Best Practices in the Treatment and Management of Metastatic Melanoma. Melanoma
 Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
Combination Approaches in Melanoma: A Balancing Act
 Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3
 ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
Immunoterapia e melanoma maligno metastatico: siamo partiti da li. Vanna Chiarion Sileni Istituto Oncologico Veneto
 Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
Revolution in der adjuvanten Therapie des Melanoms? Was bleibt? Was wird sich verändern?
 Revolution in der adjuvanten Therapie des Melanoms? Was bleibt? Was wird sich verändern? Dr. Peter Mohr, Elbeklinikum Buxtehude Hautkrebszentrum Oktober 217 Approved treatments for melanoma in the adjuvant
Revolution in der adjuvanten Therapie des Melanoms? Was bleibt? Was wird sich verändern? Dr. Peter Mohr, Elbeklinikum Buxtehude Hautkrebszentrum Oktober 217 Approved treatments for melanoma in the adjuvant
Approaches To Treating Advanced Melanoma
 Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Unmet Need Mucosal and Uveal Melanoma
 Unmet Need Mucosal and Uveal Melanoma Matteo Carlino Crown Princess Mary Cancer Centre Westmead and Blacktown Hospitals Melanoma Institute Australia The University of Sydney. Cutaneous Overall Survival
Unmet Need Mucosal and Uveal Melanoma Matteo Carlino Crown Princess Mary Cancer Centre Westmead and Blacktown Hospitals Melanoma Institute Australia The University of Sydney. Cutaneous Overall Survival
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
New treatments in melanoma
 New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine
New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove)
") Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico
 Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma
 Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy
 New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
Immunotherapies in melanoma: regulatory perspective. Jorge Camarero (AEMPS)
") Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Review of immunotherapy in melanoma
 Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Overall Survival in COLUMBUS: A Phase 3 Trial of Encorafenib (ENCO) Plus Binimetinib (BINI) vs Vemurafenib (VEM) or ENCO in BRAF-Mutant Melanoma
 Plus Binimetinib (BINI) vs Vemurafenib (VEM) or ENCO in BRAF-Mutant Melanoma") Overall Survival in COLUMBUS: A Phase 3 Trial of Encorafenib (ENCO) Plus Binimetinib (BINI) vs Vemurafenib () or ENCO in BRAF-Mutant Melanoma, Paolo A. Ascierto, Helen J. Gogas, Ana Arance, Mario Mandala,
Overall Survival in COLUMBUS: A Phase 3 Trial of Encorafenib (ENCO) Plus Binimetinib (BINI) vs Vemurafenib () or ENCO in BRAF-Mutant Melanoma, Paolo A. Ascierto, Helen J. Gogas, Ana Arance, Mario Mandala,
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Innovations in Immunotherapy - Melanoma. Systemic Therapies October 27, 2018 Charles L. Bane, MD
 Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
ASCO 2014 Highlights*
 ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
Metastasectomy for Melanoma What s the Evidence and When Do We Stop?
 Metastasectomy for Melanoma What s the Evidence and When Do We Stop? Vernon K. Sondak, M D Chair, Moffitt Cancer Center Tampa, Florida Focus on Melanoma London, UK October 15, 2013 Disclosures Dr. Sondak
Metastasectomy for Melanoma What s the Evidence and When Do We Stop? Vernon K. Sondak, M D Chair, Moffitt Cancer Center Tampa, Florida Focus on Melanoma London, UK October 15, 2013 Disclosures Dr. Sondak
Targeted Therapies in Melanoma
 Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Melanoma in Focus: Update on Novel Therapy, Emerging Agents, and Optimizing Patient Care Presentation 1
 Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
ASCO / COLUMBUS ENCORE PRESENTATION June 4, 2018
 ASCO / COLUMBUS ENCORE PRESENTATION June 4, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions of the Private
ASCO / COLUMBUS ENCORE PRESENTATION June 4, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions of the Private
The Current Status of Immune Checkpoint Inhibitors: Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb
 The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
Immune checkpoint inhibition in melanoma. John Haanen
 Immune checkpoint inhibition in melanoma John Haanen ESMO Preceptorship Singapore 217 Immune Checkpoint inhibitors Immune checkpoints play an important role in immune tolerance Cancer hijacks many of these
Immune checkpoint inhibition in melanoma John Haanen ESMO Preceptorship Singapore 217 Immune Checkpoint inhibitors Immune checkpoints play an important role in immune tolerance Cancer hijacks many of these
BRAF Inhibitors in Metastatic disease. Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia
 Inhibitors in Metastatic disease Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia Disclosures Research Support Pfizer & Cellgene Consultant Provectus Mortality from Melanoma
Inhibitors in Metastatic disease Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia Disclosures Research Support Pfizer & Cellgene Consultant Provectus Mortality from Melanoma
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Cutaneous melanoma: new developments for 2018
 Cutaneous melanoma: new developments for 2018 and beyond KIM MARGOLIN, M.D., FASCO CITY OF HOPE MEDICAL ONCOLOGY CORONADO, CALIFORNIA SEPTEMBER 20, 2018 DISCLOSURE Consultant for ImaginAb, Nektar Therapeutics,
Cutaneous melanoma: new developments for 2018 and beyond KIM MARGOLIN, M.D., FASCO CITY OF HOPE MEDICAL ONCOLOGY CORONADO, CALIFORNIA SEPTEMBER 20, 2018 DISCLOSURE Consultant for ImaginAb, Nektar Therapeutics,
Melanoma: novità ESMO 2017
 Melanoma: novità ESMO 2017 Vincenzo Picone Istituto dermopatico dell Immacolata (IDI) AGENDA Metastatico CheckMate 067 Adiuvante LBA7_PR - BRIM8: a randomized, double-blind, placebo-controlled study of
Melanoma: novità ESMO 2017 Vincenzo Picone Istituto dermopatico dell Immacolata (IDI) AGENDA Metastatico CheckMate 067 Adiuvante LBA7_PR - BRIM8: a randomized, double-blind, placebo-controlled study of
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
Kombination von Checkpointinhibitoren beim malignen Melanom
 Kombination von Checkpointinhibitoren beim malignen Melanom Dirk Jäger Medizinische Onkologie Nationales Centrum für Tumorerkrankungen Universitätsklinikum Heidelberg Ipilimumab beim metastasierten Melanom
Kombination von Checkpointinhibitoren beim malignen Melanom Dirk Jäger Medizinische Onkologie Nationales Centrum für Tumorerkrankungen Universitätsklinikum Heidelberg Ipilimumab beim metastasierten Melanom
Update on Targeted Therapy in Melanoma
 Update on Targeted Therapy in Melanoma Seville June 2013 James Larkin FRCP PhD London UK Overview What are the targets in melanoma? BRAF / KIT / NRAS / GNAQ / MEK DNA / microtubules CTLA4 / PD1 / PDL1
Update on Targeted Therapy in Melanoma Seville June 2013 James Larkin FRCP PhD London UK Overview What are the targets in melanoma? BRAF / KIT / NRAS / GNAQ / MEK DNA / microtubules CTLA4 / PD1 / PDL1
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
 for patients with ECOG PS 0-1 as indicated in the CheckMate-067 trial. Upon reconsideration of the Initial Recommendation, perc noted PAG s feedback requesting guidance on extrapolating eligibility to
for patients with ECOG PS 0-1 as indicated in the CheckMate-067 trial. Upon reconsideration of the Initial Recommendation, perc noted PAG s feedback requesting guidance on extrapolating eligibility to
Amerikanischer Krebskongress 2018
 Congress-Lightning Amerikanischer Krebskongress 218 Dermatoonkologie Prof. Dr. Ralf Gutzmer, Hannover Melanom adjuvant Melanom palliativ Nicht-melanozytäre Hauttumore Adjuvant Therapy With Nivolumab Versus
Congress-Lightning Amerikanischer Krebskongress 218 Dermatoonkologie Prof. Dr. Ralf Gutzmer, Hannover Melanom adjuvant Melanom palliativ Nicht-melanozytäre Hauttumore Adjuvant Therapy With Nivolumab Versus
Surgical Treatment of Melanoma Across the Disease Spectrum:
 AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of
AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
LESSONS LEARNT Melanoma Academic Perspective
 LESSONS LEARNT Melanoma Academic Perspective Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosures
LESSONS LEARNT Melanoma Academic Perspective Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosures
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Ipilimumab ASCO Data Review and Discussion Webcast. Monday, June 2, 2008
 Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Outcomes of Patients With Metastatic Melanoma Treated With Immunotherapy Prior to or After BRAF Inhibitors
 Outcomes of Patients With Metastatic Melanoma Treated With Immunotherapy Prior to or After BRAF Inhibitors Allison Ackerman, MD, PhD 1 ; Oliver Klein, MD 2 ; David F. McDermott, MD 1 ; Wei Wang, PhD 3
Outcomes of Patients With Metastatic Melanoma Treated With Immunotherapy Prior to or After BRAF Inhibitors Allison Ackerman, MD, PhD 1 ; Oliver Klein, MD 2 ; David F. McDermott, MD 1 ; Wei Wang, PhD 3
Melanoma BRAF mutado y terapias dirigidas. Javier Medina Martínez Hospital Virgen de la Salud, Toledo
 Melanoma BRAF mutado y terapias dirigidas Javier Medina Martínez Hospital Virgen de la Salud, Toledo Enfermedad avanzada: Seguimiento a largo plazo Retratamiento Metástasis cerebrales Adyuvancia November-2017
Melanoma BRAF mutado y terapias dirigidas Javier Medina Martínez Hospital Virgen de la Salud, Toledo Enfermedad avanzada: Seguimiento a largo plazo Retratamiento Metástasis cerebrales Adyuvancia November-2017
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes. Disclosures
 Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Highlights STOMACH CANCER
 UPDATES and NEWS from the Gastrointestinal Cancers Symposium in San Francisco Roma, 10-11 Febbraio 2017 Highlights STOMACH CANCER Lorenzo Fornaro, MD Unit of Medical Oncology 2 Azienda Ospedaliero-Universitaria
UPDATES and NEWS from the Gastrointestinal Cancers Symposium in San Francisco Roma, 10-11 Febbraio 2017 Highlights STOMACH CANCER Lorenzo Fornaro, MD Unit of Medical Oncology 2 Azienda Ospedaliero-Universitaria
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Immune checkpoint inhibition in melanoma
 Immune checkpoint inhibition in melanoma John Haanen ESMO Preceptorship Zürich 217 Disclosures I have provided consultation, attended advisory boards, and/or provided lectures for: Pfizer, MSD, BMS, IPSEN,
Immune checkpoint inhibition in melanoma John Haanen ESMO Preceptorship Zürich 217 Disclosures I have provided consultation, attended advisory boards, and/or provided lectures for: Pfizer, MSD, BMS, IPSEN,
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma
 With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma") Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Melanoma: What else beyond Checkpoint Inhibitor pathway?
 Melanoma: What else beyond Checkpoint Inhibitor pathway? Jose Lutzky MD, FACP Director, Mount Sinai Melanoma Program Miami Beach, Florida Clinical Associate Professor, Wertheim School of Medicine, FIU,
Melanoma: What else beyond Checkpoint Inhibitor pathway? Jose Lutzky MD, FACP Director, Mount Sinai Melanoma Program Miami Beach, Florida Clinical Associate Professor, Wertheim School of Medicine, FIU,
 Overall Survival (OS) Analysis From an Expanded Access Program (EAP) of Nivolumab (NIVO) in Combination with Ipilimumab (IPI) in Patients with Advanced Melanoma (MEL) David Hogg, Paul B. Chapman, 2 Mario
Overall Survival (OS) Analysis From an Expanded Access Program (EAP) of Nivolumab (NIVO) in Combination with Ipilimumab (IPI) in Patients with Advanced Melanoma (MEL) David Hogg, Paul B. Chapman, 2 Mario
Recent Advances in Lung Cancer: Updates from ASCO Updates from ESMO, AACR and ASCO
 Recent Advances in Lung Cancer: Updates from ASCO 2018 Updates from ESMO, AACR and ASCO Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University
Recent Advances in Lung Cancer: Updates from ASCO 2018 Updates from ESMO, AACR and ASCO Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University
Update on Melanoma. Main Themes
 Update on Melanoma Antoni Ribas, M.D. Professor of Medicine, Surgery, and Medical and Molecular Pharmacology University of California Los Angeles (UCLA) and the Jonsson Comprehensive Cancer Center Main
Update on Melanoma Antoni Ribas, M.D. Professor of Medicine, Surgery, and Medical and Molecular Pharmacology University of California Los Angeles (UCLA) and the Jonsson Comprehensive Cancer Center Main
Melanoma- Fighting the Dark Side
 Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
General Information, efficacy and safety data
 Horizon Scanning in Oncology Horizon Scanning in Oncology 23 rd Prioritization 2 nd quarter 2015 General Information, efficacy and safety data Eleen Rothschedl Anna Nachtnebel Priorisierung XXIII HSS Onkologie
Horizon Scanning in Oncology Horizon Scanning in Oncology 23 rd Prioritization 2 nd quarter 2015 General Information, efficacy and safety data Eleen Rothschedl Anna Nachtnebel Priorisierung XXIII HSS Onkologie
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Priming the Immune System to Kill Cancer and Reverse Tolerance. Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics
 Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Presentation Number: LBA18_PR. Lecture Time: 09:15-09:27. Speakers: Heinz-Josef J. Lenz (Los Angeles, US) Background
 Background") LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Debate 1 Are treatments for small cell lung cancer getting better? No:
 Debate 1 Are treatments for small cell lung cancer getting better? No: Taofeek Owonikoko, MD, PhD Associate Professor Department of Hematology & Medical Oncology Winship Cancer Institute of Emory University
Debate 1 Are treatments for small cell lung cancer getting better? No: Taofeek Owonikoko, MD, PhD Associate Professor Department of Hematology & Medical Oncology Winship Cancer Institute of Emory University
Idera Pharmaceuticals
 Idera Pharmaceuticals ILLUMINATE-204 Clinical Data Update December 2018 Forward Looking Statements and Other Important Cautions This presentation contains forward-looking statements within the meaning
Idera Pharmaceuticals ILLUMINATE-204 Clinical Data Update December 2018 Forward Looking Statements and Other Important Cautions This presentation contains forward-looking statements within the meaning