Management of EGFR-Mutation Positive Metastatic Non-Small Cell Lung Cancer
|
|
|
- Donald Collins
- 5 years ago
- Views:
Transcription



1 Management of EGFR-Mutation Positive Metastatic Non-Small Cell Lung Cancer Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center Rogerio Lilenbaum, MD Yale Cancer Center/Smilow Cancer Hospital EGFR Mutation in Advanced NSCLC: NCCN, Florida 2016 Rogerio Lilenbaum, MD Professor of Medicine Yale Cancer Center Chief Medical Officer Smilow Cancer Hospital




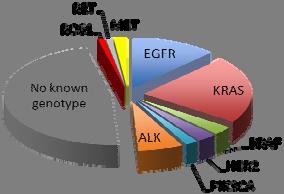
2 Molecular Targeted Therapy in Cancer Personalized Medicine in Lung Cancer No known genotype


 on Ion Torrent 2 weeks Tier 3: Whole exome sequencing")
3 Molecular Alterations in Lung Adenocarcinoma SURVIVAL drivernotx drivertx nodriver YEARS Note: Does not include ROS1 or RET Sholl LM et al, 2015; Johnson BE, et al. ASCO 2013 Tumor Profiling at Yale Tier 1: Reflex testing using TaqMan platform 5 to 7 days Tier 2: Oncomine Cancer Panel (143 genes and >40 translocations/fusions) on Ion Torrent 2 weeks Tier 3: Whole exome sequencing with future custom panels per organ system specification 2-3 weeks



4 EGFR Mutations High ORR with EGFR TKIs with exon 19 deletion / exon 21 L858R point mutation Most common in never smokers, females, patients with East Asian ethnicity, and adenocarcinomas Blencke S, et al. J Biol Chem 2003; Lynch TJ, et al. N Engl J Med 2004;350: Paez JG, et al. Science 2004;304: * * The NCCN NSCLC Guidelines Panel strongly endorses broader molecular profiling with the goal of identifying rare driver mutations for which effective drugs may already be available, or to appropriately counsel patients regarding the availability of clinical trials. Broad molecular profiling is a key component of the improvement of care of patients with NSCLC. See Emerging Targeted Agents for Patients With Genetic Alterations (NSCL-H).
 250 mg/day PC offered to gefitinib patients upon progression Carboplatin")
 ORR (%) 43.0 32.2 P=0.0001 52% of patients on the C + P arm received subsequent TKI therapy Mok, et al. N Engl J Med. 2009;361:947. Ohe, et al. ASCO. 2009 (abstr #8044).")
 Secondary endpoints: ORR, OS, QOL, diseaserelated symptoms, safety Exploratory biomarkers: EGFR mutation, EGFR gene copy number, EGFR protein expression IPASS:")
5 Gefitinib vs Carboplatin/Paclitaxel for Clinically Selected Chemotherapy-Naïve Patients With Advanced NSCLC in Asia (IPASS) Eligibility: Chemotherapy-naïve Age 18 years Adenocarcinoma Never or light ex-smokers Life expectancy >12 weeks Measurable stage IIIB/IV disease N=1217 Endpoint R A N D O M I Z E G N=609 Gefitinib (G) 250 mg/day PC offered to gefitinib patients upon progression Carboplatin (C) AUC 5 or 6 Paclitaxel (P) 200 mg/m 2 q3w* *Limited to maximum of 6 cycles. mpfs 5.7 mos 5.8 mos mos 18.8 mos 17.4 mos C + P N=608 HR/OR (95% CI) ( ) P< ( ) P= ( ) ORR (%) P= % of patients on the C + P arm received subsequent TKI therapy Mok, et al. N Engl J Med. 2009;361:947. Ohe, et al. ASCO (abstr #8044). Yang, et al. ESMO (abstr LBA2). Primary endpoint: PFS (noninferiority) Secondary endpoints: ORR, OS, QOL, diseaserelated symptoms, safety Exploratory biomarkers: EGFR mutation, EGFR gene copy number, EGFR protein expression IPASS: PFS and OS in EGFR Mutation Positive and Negative Patients Probability of Progression-Free Survival PFS (2008) Gefitinib EGFR M+ Gefitinib EGFR M- C/P EGFR M+ C/P EGFR M Time From Randomization (months) Gefitinib M Gefitinib M C/P M C/P M Probability of Survival Mutation - OS (2010) Mutation Time From Randomization (months) Patients at risk excludes censored patients and those who have experienced an event. Yang, et al. ESMO (abstr LBA2).
6 Randomized Trials of EGFR TKI vs CT in 1st Line Rx Study ORR PFS (mo) HR OS EURTAC 58% vs 15% 9.7 vs ND OPTIMAL 83% vs 36% 13.1 vs ND NEJ % vs 31% 10.8 vs ND WJTOG % vs 31% 9.2 vs ND IPASS 71% vs 47% 9.5 vs ND LUX LUNG 3 56% vs 23% 11.1 vs ND LUX LUNG 6 67% vs 23% 11.0 vs 5.6 NR NR Mok et al. N Engl J Med 2009;361:947 57; Han et al. J Clin Oncol 2012;30:1122 8; Mitsudomi et al. Lancet Oncol 2010;11:121 8; Mitsudomi et al. J Clin Oncol 2012;30(Suppl.): Abstract 7521; Maemondo et al. N Engl J Med 2010;362:2380 8; Zhou et al. Lancet Oncol 2011;12:735 42; Zhou et al. J Clin Oncol 2012;30(Suppl.): Abstract 7520; Rosell et al. Lancet Oncol 2012;13: EURTAC Study Patients Chemonaïve Age 18 years Known EGFR mutation L858R Del19 PS 0-2 Measurable stage IIIB / IV disease N= 173 Erlotinib (150 mg / day) N=86 1:1 randomization Platinum + docetaxel or gemcitabine* N=87 Endpoints Primary Progression-free survival Secondary Objective response rate Overall survival EGFR mutation detection from serum *Investigator could choose cisplatin or carboplatin and also docetaxel vs. gemcitabine Chemotherapy was given for up to 4 cycles Rosell et al, Lancet 2012
7 EURTAC Results 9.4 mo 5.2 mo Rosell et al, Lancet 2012 LUX-Lung 3 and 6: design Stage IIIB/IV adenocarcinoma of the lung Presence of EGFR mutation in the tumor tissue* No prior treatment with chemotherapy for advanced/metastatic disease or EGFR inhibitors ECOG PS 0 or 1 Randomization 2:1 Stratification by EGFR mutation type: Del19/L858R/other and by race (LUX-Lung 3 only): Asian/non-Asian Afatinib 40 mg orally once daily LUX-Lung 3 1 : Cisplatin + pemetrexed up to 6 cycles LUX-Lung 6 2 : Cisplatin + gemcitabine up to 6 cycles Primary endpoint: PFS (independent review) Secondary end points: ORR, DCR, OS, PRO, safety *EGFR29: 19 deletions in exon 19, 3 insertions in exon 20, L858R, L861Q, T790M, G719S, G719A and G719C (or G719X), S768I. 1. Sequist et al. J Clin Oncol. 2013;31:3327; 2. Wu et al. Lancet Oncol. 2014;15:213.
8 Overall Survival with Afatinib by EGFR mutation categories Estimated OS probability Del19 Afatinib Chemo n=236 n=119 Median, months HR (95%CI), p-value 0.59 ( ), p= Estimated OS probability Median, months HR (95%CI), p-value L858R Afatinib Chemo n=183 n= ( ), p= Time (months) No of patients Afatinib Chemo Time (months) No of patients Afatinib Chemo Yang et al, 2015 Afatinib vs Chemotherapy in the first-line setting: Combined OS analysis in patients with common EGFR mutations Estimated OS probability Afatinib Chemo n=419 n=212 Median, months HR (95%CI), p-value 0.81 ( ), p= No of patients Afatinib Chemo Yang et al, Time (months)
 and presence of brain metastases (yes vs no) 1:1 Afatinib 40 mg once daily Gefitinib 250 mg once daily Primary endpoints: PFS (independent review) #, TTF,")
9 LUX Lung 7 Study Design Stage IIIb/IV adenocarcinoma of the lung EGFR mutation (Del19 and/or L858R) in the tumor tissue # No prior treatment for advanced/metastatic disease ECOG PS 0 1 Randomization Stratified by mutation type (Del19 vs L858R) and presence of brain metastases (yes vs no) 1:1 Afatinib 40 mg once daily Gefitinib 250 mg once daily Primary endpoints: PFS (independent review) #, TTF, OS Secondary endpoints: ORR, time to and duration of response, duration of disease control, tumor shrinkage, HRQoL, safety # local or central test # Tumor assessment performed at week 4, 8, every 8 weeks until w64 and every 12 weeks thereafter Treatment beyond progression allowed if deemed beneficial by investigator. Park et al. Ann Oncol. 2015;26: (suppl 9; abstract LBA2). Afatinib is approved in a number of markets, including the EU, Japan, Taiwan and Canada and in the U.S. for use in patients with distinct types of EGFR mutation positive NSCLC. Registration conditions differ internationally, please refer to locally approved prescribing information. Afatinib is under regulatory review by health authorities in other countries worldwide. Objective Response and Disease Control Rates P = % 70% 60% 56% ORR 40% 20% 0% Afatinib 112/160 Afatinib Gefitinib 89/159 Gefitinib Median DoR, months (95% CI) 10.1 (7.8, 11.1) 8.4 ( ) Park et al. Ann Oncol. 2015;26: (suppl 9; abstract LBA2). Disease control rate (N) 91.3% (146) 87.4% (139)
10 PFS by Independent Review 1.0 Afatinib Gefitinib Median, mo HR (95% CI) P value 0.73 ( ) Estimated PFS probability %* Afatinib Gefitinib 18% % 8% No. at risk: Time of progression free survival (months) Afatinib Gefitinib Park et al. Ann Oncol. 2015;26: (suppl 9; abstract LBA2); * P= P= Common Adverse Events Following Use of EGFR TKIs Afatinib (n=229) 1 Erlotinib (n=84) 2 Gefitinib (n=1126) 3 Adverse event, % Any grade Grade 3+ Any grade Grade 3+ Any grade Grade 3+ Diarrhea Rash Paronychia Stomatitis/mucositis * Pruritus Dry skin Skin reactions Nail disorders Includes acne, acne pustular, dermatitis, dermatitis acneiform, dermatitis exfoliative, drug eruption, dry skin, erythema, exfoliative rash, folliculitis, pruritus, pruritus generalized, rash, rash erythematous, rash generalized, rash macular, rash maculopapular, rash papular, rash pruritic, rash pustular, rash vesicular, skin exfoliation, skin toxicity, xeroderma Includes ingrowing nail, nail bed infection, nail disorder, nail infection, onychoclasis, onycholysis, paronychia *Only includes mucositis for erlotinib package insert.
11 Maximum change from baseline (%) Tumor shrinkage in patients with uncommon mutations * * * De novo T790M (n=14): Response rate = 14% T790M alone(*), T790M+Del19, T790M+L858R, T790M+G719X, T790M+L858R+G719X Exon 20 insertions (n=20): Response rate = 8.7% Other (n=33): Response rate = 71% L861Q, G719X, G719X+S768I, G719X+L861Q, E709G or V+L858R, S768I+L858R, S768I, L861P, P848L, R776H+L858R, L861Q+Del19, K739_1744dup6 8 patients were not included due to insufficient data Progression-free survival and overall survival in patients Median PFS, months (range) Median OS, months (range) De novo T790M n= ( ) 14.9 ( ) Exon 20 insertions n= ( ) 9.4 ( ) Other n= ( ) 18.6 ( ) T790M + L858R, n=6 Patient PFS OS * 24.4* Median T790M + Del19, n=3 Patient PFS OS Median Patient data censored; NE = not estimable
12 Erlotinib +/- Bevacizumab Study Design Chemotherapy-naïve Stage IIIB/IV NSCLC or postoperative recurrence Non-squamous Activating EGFR mutations* Exon 19 deletion Exon 21 L858R Age 20 years PS 0 1 No brain metastasis Stratification factors: sex, smoking status, clinical stage, EGFR mutation type *T790M excluded R 1:1 Erlotinib 150mg/d + Bevacizumab 15mg/kg q3w (n = 75) Erlotinib 150mg/d (n = 75) Primary endpoint: PFS (RECIST v1.1, independent review) Secondary endpoints: OS, tumor response, QoL, safety Exploratory endpoint: biomarker assessment PD PD First-Line Erlotinib +/- Bevacizumab PFS probability EB E Median (months) HR 0.54 (95% CI: ) P value* *log-rank test, two-sided Number at risk Time (months) EB E EB E

13 Afatinib + Cetuximab at MTD: Responses by T790M mutation Maximum percentage decrease from baseline (%) T790M+ T790M EGFR wt Uninformative for T790M 32% RR Overall PFS 4.7 mos Median duration of confirmed response 8.0 mos Patient index sorted by maximum % decrease Janjigian et al ESMO 12 S1403: A randomized phase II/III trial of afatinib plus cetuximab versus afatinib alone in treatment naïve patients with advanced, EGFR mutation positive NSCLC PIs: Goldberg; Politi; Lilenbaum


 Maturity: 31% Median PFS, months (95% CI) NC (12.3, NC) Maturity: 40% NC (11.1, NC) Maturity: 30% NC (13.7, NC) Maturity: 35% Maximum DoR, months 18.0+ 12.6+ 18.")
14 DoR and PFS in osimertinib (AZD9291) first line cohorts (investigator assessed) Probability of response Number of patients at month: 80 mg 160 mg Duration of response AZD mg Censored observation AZD mg Censored observation Month Probability of response AZD mg AZD mg Progression free survival Censored observation Censored observation Number of Month patients at risk: 80 mg mg mg N= mg N=25 Total N=45 80 mg N= mg N=30 Total N=60 Median DoR, months (95% CI) 13.6 (11.1, NC) Maturity: 35% NC (9.7, NC) Maturity: 28% NC (12.3, NC) Maturity: 31% Median PFS, months (95% CI) NC (12.3, NC) Maturity: 40% NC (11.1, NC) Maturity: 30% NC (13.7, NC) Maturity: 35% Maximum DoR, months Remaining in response, % (95% CI) 9 months 12 months 89 (64, 97) 76 (46, 90) 78 (56, 90) 69 (45, 84) 83 (68, 92) 71 (53, 83) Maximum PFS, months Remaining alive and progression-free, % (95% CI) 9 months 12 months 83 (64, 93) 75 (55, 87) 80 (60, 90) 69 (48, 82) 81 (69, 89) 72 (58, 82) Ramalingam SS et al. Proc ASCO 2015 FLAURA Study Design Enrollment by local a or central b EGFR mutation testing of biopsy sample Stratified by: Asian/ non Asian Ex19del/ L858R Oral osimertinib (80 mg/d) Randomize patients 1:1 EGFR TKI standard of care c : oral gefitinib (250 mg/d) or oral erlotinib (150 mg/d) RECIST 1.1 assessment every 6 weeks until objective PD Patients randomized to standard of care may receive osimertinib after progression d Primary objective: efficacy by PFS a With central laboratory assessment performed for sensitivity; b cobas EGFR Mutation Test; c Sites to select either gefitinib or erlotinib as the sole comparator prior to site initiation; d Patients randomized to the standard of care treatment arm may receive open label treatment with osimertinib on central confirmation of both objective disease progression and T790M positive tumor. PFS2 = second progression free survival (time from randomization to second progression). NCT Clinical study report available at
15 Conclusions Gefitinib, erlotinib, and afatinib are appropriate options Afatinib has demonstrated an OS benefit in patients with Del 19 mutations Afatinib showed superior ORR, PFS, and TTF in 1 st line therapy against gefitinib At the current recommended doses, afatinib has a higher rate of toxicity Combination of bevacizumab and erlotinib showed better PFS compared to erlotinib alone Ongoing studies are evaluating the role of cetuximab in combination with afatinib vs afatinib alone Osimertinib is being evaluated in 1 st line Management of EGFR Mutation Positive Metastatic Non Small Cell Lung Cancer Treatment of Patients With Sensitizing EGFR Mutation Positive NSCLC and Acquired Resistance to EGFR TKIs Leora Horn, MD MSc Associate Professor of Medicine Clinical Director of Thoracic Oncology Research Program Associate Vice Chancellor for Faculty Development Vanderbilt Ingram Cancer Center Nashville, TN USA


16 Case One 64 year old, Caucasian, male former smoker diagnosed with stage IV non small cell lung cancer, adenocarcinoma histology, positive for EGFR exon deletion 19. He is treated with erlotinib 150 mg daily and after 4 years is found to have progression in a single lung lesion. What do you recommend? 1. Biopsy the lung lesion 2. Switch to chemotherapy 3. Start on afatinib 4. Start on osimertinib 5. Radiation to the lung lesion Audience Polling Results
17 Acquired Resistance to EGFR TKIs When treated with EGFR TKIs, 70% of patients with activating mutations will have tumor regression and a median PFS of 1 year. Once these responding patients progress, they have developed acquired resistance to gefitinib, erlotinib or afatinib. In Acquired Resistance Oncogene addiction persists Median post progression survival is 16 months Mok T et al NEJM 2009; Jackman D et al JCO 2009 Criteria for Acquired Resistance Previously received treatment with single agent sensitizing EGFR TKI (gefitinib, erlotinib or afatinib). Either of the following: Documented partial response (PR) or complete response (CR) or Durable (> 6 months) clinical benefit (stable disease) while on sensitizing EGFR TKI Systemic progression of disease while on continuous treatment with sensitizing EGFR TKI during the last 30 days. No intervening systemic therapy between cessation of sensitizing EGFR TKI and initiation of new therapy. Jackman D et al JCO 2009






18 Acquired Resistance to EGFR TKIs in Lung Cancer Day 0 4 months 25 months Growing bone lesion Growing lung lesion Pao W et al PLoS Med 2: e Mechanism of Acquired Resistance to EGFR TKIs Camidge, D. R. et al Nat. Rev. Clin. Oncol



19 Type of Progression Drives Therapy: Three PD Subtypes PD Subtype Systemic PD Oligo PD CNS PD (Sanctuary) Gandara et al., Clinical Lung Cancer 2013 ASPIRATION: Phase II First line Erlotinib in Sensitizing EGFR Mutation Positive NSCLC Continued After Progression Study Design Chemotherapy naїve Stage IV or recurrent NSCLC EGFR exon mutation (except T790M) ECOG PS 0 2 (N=207) Erlotinib 150 mg/day PFS 1 PD by RECIST Erlotinib 150 mg/day PD by physician assessment PFS 2 Primary endpoint: PFS (time to RECIST PD or death) Secondary endpoints: PFS2 (time to off erlotinib PD if erlotinib was extended beyond RECIST PD), PFS1 in exon 19 deletion/l858r subsets, OS, ORR/DCR/BOR, safety BOR=best overall response; ECOG PS=Eastern Cooperative Oncology Group performance status. Park, et al. Presented at: ESMO (abstr 1223O).


.")
20 ASPIRATION: PFS1 and PFS2 In patients receiving post PD erlotinib (n=93) PFS1 was 11.0 months Difference between PFS1 and PFS2 was an additional 3.1 months Survival Probability months 14.1 months PFS1 PFS Progression Free Survival Time, Months Secondary endpoints, ITT population ORR : 66.2% DCR : 82.6% Median OS: 31.0 months (95% CI, 27.3 not reached) PD=progressive disease. Park, et al. Presented at: ESMO (abstr 1223O). Disease Flare Rapid acceleration of disease progression resulting in hospitalization and/or death after discontinuation of gefitinib or erlotinib and before initiation of study drug. Last day of TKI Off EGFR TKI Resumed TKI Day 0 Day 21 Day 42 Chaft J et al CCR 2011

* <4 weeks prior to study randomization Primary endpoint: PFS Secondary endpoints: OS, ORR, DCR, safety,")
 and RECIST version 1.")
21 Results **Flare progression of disease leading to hospitalization or death during washout 14 patients (23%, 95% CI, 14 35%) had a disease flare** 61 protocol eligible patients 47 uneventful washout periods 3 patient deaths 3 patients went on to clinical trial treatment 8 patients instructed to restart TKI, removed from trial Chaft J et al CCR 2011 IMPRESS: Phase III Trial of Gefitinib vs Gefitinib + CT Beyond Progression in Sensitizing EGFR Mutation Positive NSCLC Enrollment Period: March 2012 December 2013 Stage IIIB/IV EGFR mutation positive NSCLC WHO PS 0 1 Chemotherapy naïve Achieved CR/PR 4 months or SD >6 months with first line gefitinib Disease progression (RECIST)* <4 weeks prior to study randomization Primary endpoint: PFS Secondary endpoints: OS, ORR, DCR, safety, HRQoL Exploratory endpoint: Biomarkers Cisplatin (75 mg/m 2 ) + Pemetrexed 500 mg/m 2 ( 6 cycles) + Gefitinib 250 mg (given until PD) Cisplatin (75 mg/m 2 ) + Pemetrexed 500 mg/m 2 IV ( 6 cycles) + Placebo 250 mg *Progressive disease based on radiological evaluation (modified Jackman s criteria) and RECIST version 1.1. Tumor assessments were performed 4 weeks before start of treatment (baseline) and every 6 weeks (±7 days) after randomization until progressive disease. Randomization did not include stratification factors; analyses were adjusted for 2 covariates; age (<65 vs 65 years) and prior response to gefitinib (SD vs PR+CR). CR=complete response; CT=chemotherapy; DCR=disease control rate; HRQoL=Health Related Quality of Life; ORR=objective response rate; PR=partial response; SD=stable disease; WHO PS=World Health Organization performance status. Mok, et al. Presented at: ESMO. 2014; Lancet Oncology 16:990 8 (2015) R A N D O M I Z E 1:1
 98 (73.7) 107 (81.1) HR*=0.86 (95% CI, 0.65-1.13); P=0.")
22 IMPRESS: PFS (Primary Endpoint; ITT) Gefitinib Placebo Probability of PFS Gefitinib (n=133) Placebo (n=132) (n=133) (n=132) Median PFS, months Number of events, n (%) 98 (73.7) 107 (81.1) HR*=0.86 (95% CI, ); P=0.273 Patients at risk: Gefitinib Placebo Time of Randomization, Months Patient Characteristics were Balanced with the Exception of: Gefitinib (n=133) Placebo (n=132) 65 years, % Brain metastases (baseline), % CR or PR/SD to first line gefitinib, % 68/32 76/24 *Primary cox analysis with covariates. An HR <1 implies a lower risk of progression with gefitinib Mok, et al. Presented at: ESMO. 2014; Lancet Oncology 16:990 8 (2015) Case Continued He is treated with SBRT to the primary lung lesion but 12 months later develops new disease in the bones and hip pain as well and small bilateral lung nodules. What do you recommend? 1. Biopsy of a growing lesion 2. Switch to chemotherapy 3. Start on afatinib 4. Start on osimertinib 5. Do something else
.")
23 Audience Polling Results Osimertinib (AZD9291) Primary endpoint AURA extension: to investigate the safety, tolerability and efficacy (ORR) of AZD9291 (assessed by BICR). AURA2: ORR according to RECIST 1.1 (assessed by BICR). Patients with confirmed EGFRm locally advanced or metastatic NSCLC who have progressed following prior therapy with an approved EGFR TKI T790M positive Central T790M mutation testing of biopsy sample collected following confirmed disease progression on the most recent treatment regimen* T790M negative Not eligible for enrolment Patients received AZD mg QD until disease progression Key inclusion criteria Aged 18 ( 20 in Japan). Confirmation of tumor EGFR mutation associated with EGFR TKI sensitivity (including G719X, exon 19 del, L858R, L861Q). Measurable disease at baseline. WHO performance status 0 or 1. Acceptable organ function. Stable brain metastases allowed. For patients third line AURA extension: disease progression following at least two lines of prior therapy including at least one EGFR TKI. AURA2: disease progression following at least two lines of prior therapy including both an EGFR TKI and a platinum based doublet chemotherapy. *T790 EGFR mutation identified by EGFR Mutation Test BICR, blinded independent central review; EGFR, epidermal growth factor receptor; NSCLC, non small cell lung cancer; ORR, objective response rate; RECIST, Response Evaluation Criteria in Solid Tumours; TKI, tyrosine kinase inhibitor; WHO, World Health Organization Poster #365 presented by Glenwood D. Goss at the ECC 2015 European Cancer Congress
 64 (35 88) 63 (35 89) Race: White / Asian / other / not reported 38 / 57 / 3 / 2 34 / 63 / 3 / 0 36 / 60 / 3 / 1 Histology: adenocarcinoma / other 97 / 3 96 / 4 97 / 3 WHO performance status: 0 /")
24 Characteristic, % Baseline demographics and disease characteristics AURA extension (n=201) AURA2 (n=210) Total (n=411)* Sex: male / female 34 / / / 68 Age: median (range), years 62 (37 89) 64 (35 88) 63 (35 89) Race: White / Asian / other / not reported 38 / 57 / 3 / 2 34 / 63 / 3 / 0 36 / 60 / 3 / 1 Histology: adenocarcinoma / other 97 / 3 96 / 4 97 / 3 WHO performance status: 0 / 1 / 2 34 / 66 / 1 40 / 60 / 0 37 / 63 / 0 Brain metastases Treatment: second line / third line 30 / / / 69 EGFR TKI as last therapy: <30 days 30 days EGFR mutation type by last test: Exon 19 del / L858R / G719X / S7681 / Exon 20 ins *Full analysis set: n=411. Evaluable for response analysis set: n=398; 13 patients did not have measurable disease at baseline by independent central review Protocol deviation: inclusion criteria states patients should have a WHO performance status of 0 or 1 Last regimen prior to start of treatment with AZD9291 EGFR, epidermal growth factor receptor; TKI, tyrosine kinase receptor; WHO, World Health Organization / 25 / 2 / 2 / 1 65 / 32 / 2 / 1 / 1 68 / 29 / 2 / 2 / 1 Poster #365 presented by Glenwood D. Goss at the ECC 2015 European Cancer Congress Response rate By blinded independent central review. Evaluable for response analysis set (n=398). Mean best percentage change in target lesion size 45%, standard deviation 28.0 (median best percentage change 47.6%; range: 100% to +90.8%) Poster #365 presented by Glenwood D. Goss at the ECC 2015 European Cancer Congress
25 Progression free survival Median progression free survival in months: 9.7 (95% CI 8.3, NC), maturity: 39% By blinded independent central review. Patients with confirmed objective response (n=263), maturity 23%. Blue dotted lines represent 95% CI CI, confidence interval; NC, not calculated Poster #365 presented by Glenwood D. Goss at the ECC 2015 European Cancer Congress Most frequent adverse events (all causality) AE, number (%) of patients Grade 1 Grade 2 Grade 3 Unknown Total (n=411) AE by preferred term occurring in 15% of patients overall Diarrhea 147 (36) 21 (5) 4 (1) 2 (1) 174 (42) Rashes and acnes (grouped terms) 149 (36) 18 (4) 2 (1) 1 (0) 170 (41) Dry skin 88 (21) 7 (2) (23) Paronychia 52 (13) 20 (5) (18) Nausea 58 (14) 9 (2) 2 (1) 0 69 (17) Decreased appetite 49 (12) 13 (3) 3 (1) 0 65 (16) Constipation 50 (12) 8 (2) 1 (0) 3 (1) 62 (15) Select AEs of interest ILD and pneumonitis 4 (1) 0 7 (2) 0 11 (3) Hyperglycemia 3 (1) 1 (0) 1 (0) 0 5 (1) QT prolongation 9 (2) 3 (1) 5 (1) 0 17 (4) AE, adverse event; ILD, interstitial lung disease Poster #365 presented by Glenwood D. Goss at the ECC 2015 European Cancer Congress
 * * * * * * * * * * * ORR to date: 58% * * * * * * * * * * * * * * * * * * * * Sequist et al.")
 14 (10) 1 (1) 0 Hyperglycemia and IGT 19 (14) 11 (8) 22 (16) 0 Diarrhea 19 (14) 4 (3) 0 0 Vomiting 13 (9) 1 (1) 3 (2) 0 Decreased appetite 10 (7) 10 (7) 1 (1) 0 Myalgia")
26 Rociletinib (CO 1686): Best response in Phase 1 and early Phase 2 expansion cohort patients Centrally confirmed T790M+ patients within therapeutic dose range (N=40) 10 0 *Ongoing Change from Baseline (%) * * * * * * * * * * * ORR to date: 58% * * * * * * * * * * * * * * * * * * * * Sequist et al., ASCO 2014; NEJM 372: (2015) Adverse events Treatment related adverse events* occurring in >10% of CO 1686 patients (N=72) treated at efficacious doses, % (n) Preferred term Grade 1 Grade 2 Grade 3 Grade 4 Nausea 19 (14) 14 (10) 1 (1) 0 Hyperglycemia and IGT 19 (14) 11 (8) 22 (16) 0 Diarrhea 19 (14) 4 (3) 0 0 Vomiting 13 (9) 1 (1) 3 (2) 0 Decreased appetite 10 (7) 10 (7) 1 (1) 0 Myalgia 10 (7) 1 (1) 0 0 QTc prolonged 4 (3) 4 (3) 7 (5) 0 *excluding malignancy related adverse events (eg, disease progression) 4% (3) patients with any form of rash, all Grade 1 Sequist et al., ASCO 2014
 Both confirmed and unconfirmed responses Investigator assessment a Investigator assessment of target")

 T790M+: 40.9% (18/44) 50% (1/2) exon 20 insertion Yu H., Oxnard G., Spira A., et al.")
27 ASP8273: Preliminary Results: Phase 1/2 Study in Asian Subjects (Phase 2 Part) Best Change (%) from Baseline of Target Lesions in T790M+ Subjects a * Preliminary ORR: 64% (n=45/70) Both confirmed and unconfirmed responses Investigator assessment a Investigator assessment of target lesion changes only Indicates unconfirmed response in target lesions, but ORR is progressive disease based on new or non target lesions * Subject was withdrawn from the study with unconfirmed stable disease in target lesions; Azuma K., Nokihara H., Murakami H., et al: Japanese Lung Cancer Society Meeting Nov 2015 ASP8273 Preliminary Results: US Phase 1 Study * ** *Unconfirmed PR Antitumor activity has been observed at doses of > 100 mg: ORR: 36.8% (25/68) T790M+: 40.9% (18/44) 50% (1/2) exon 20 insertion Yu H., Oxnard G., Spira A., et al. AACR EORTC NCI Meeting Nov 2015 Boston
28 Preliminary Results: US Phase 1 Study Treatment Emergent AE s ( > 10%) 95 patients received a dose of ASP8273 (25 500mg) Table reflects doses which will be utilized in future studies and events which occurred in at least 10% of pts Treatment Emergent Adverse Events Occurring in 10% of the Total Population, n (%) Diarrhea Nausea Fatigue Constipation Hyponatremia Vomiting Dizziness Paraesthesia Cough 100 mg (n=12) 200 mg (n=12) 300 mg* (n=48) Total (N=72) Overall 1 (8) 2 (17) 17 (35) 20 (28) Grade (2) 1 (1.4) Overall 3 (25) 4 (33) 10 (21) 17 (24) Grade 3 1(8) (1.4) Overall 3 (25) 2 (17) 6 (13) 11 (15) Grade Overall 2 (17) 3 (25) 6 (13) 11 (15) Grade Overall 2 (17) 2(17) 6 (13) 10 (14) Grade 3 2 (17) 1 (8) 4 (8) 7 (10) Overall 1 (8) 3 (25) 7 (15) 11 (15) Grade 3 1 (8) (1.4) Overall 1 (8) 3 (25) 7 (15) 11 (15) Grade (2) 1 (1.4) Overall 0 1 (8) 5 (10) 10 (11) Grade Overall 1 (8) 3(25) 3 (6) 7 (10) Grade Yu H., Oxnard G., Spira A., et al. AACR EORTC NCI Meeting Nov 2015 Boston; modified Lux Lung 1 Randomized Phase II/III comparing afatinib to placebo in patients who had progressed following at least 12 weeks of gefitinib or erlotinib (EGFR mutation not required) RR was 7% for afatinib vs. 1% for placebo 141 patients had tumors available for molecular testing 96 patients: sensitizing EGFR mutation positive, 76 (79%) had common mutations, Median PFS was 3.3 months for afatinib vs. 1.1 months placebo (HR 0.38; p < ) in patients with sensitizing EGFR mutation positive NSCLC Median PFS was 1.8 months for both afatinib and placebo in patients negative for sensitizing EGFR mutations Median overall survival was 10.3 months for afatinib vs months for placebo (HR 1.08; p = 0.74) Miller et al., Lancet Oncology 5:528 (2012)
29 Phase Ib Study: Afatinib+ Cetuximab Phase Ib, open label, multicenter trial in the US and The Netherlands Primary endpoints: RECIST 1.1 Response and PFS, with imaging at Week 4, 8, 12, and every 8 weeks thereafter Key eligibility criteria: Inclusion Pathologically confirmed NSCLC Presence of EGFR drug sensitizing mutations or RECIST response, or SD 6 months on prior EGFR TKI Gefitinib/erlotinib as last systemic treatment Disease progression on treatment with erlotinib or gefitinib within 30 days Biopsy (available) at time of acquired resistance ECOG PS 0 2 Exclusion Prior treatment with EGFR targeting antibodies Symptomatic brain metastases or disease progression only in CNS SD = stable disease; i.v. = intravenous; RECIST = Response Evaluation Criteria in Solid Tumors. Janjigian et a., Cancer Discover 2014 Afatinib + Cetuximab at MTD: Responses by T790M mutation Maximum percentage decrease from baseline (%) T790M+ T790M EGFR wt Uninformative for T790M Overall PFS 4.7 mos Janjigian et a., Cancer Discover Patient index sorted by maximum % decrease
 Headache 2 (3) 25 (41) Paronychia 1 (2) 18 (30) Vomiting 1 (2) 18 (30) Blood Based Testing (cfdna) in detection of biomarkers Crowley E et al. Nat Rev Clin Oncol.")
30 Most Frequent Adverse Events Adverse event n=61 Grade 3 n (%) All Grades n (%) Rash 5 (8) 53 (87) Diarrhea 3 (5) 40 (66) Xerosis 1 (2) 34 (56) Fatigue 2 (3) 31 (51) Skin fissures 29 (48) Nausea 27 (44) Headache 2 (3) 25 (41) Paronychia 1 (2) 18 (30) Vomiting 1 (2) 18 (30) Blood Based Testing (cfdna) in detection of biomarkers Crowley E et al. Nat Rev Clin Oncol. 2013;10(8):


31 Blood Based Testing in TIGER X Trial: Sensitivity and Specificity of cfdna Analysis Reference: Sequist, L. ASCO Annual Meeting, Blood Based Testing in TIGER X: ORR by Tumor or cfdna Analysis Sequist, L. ASCO Annual Meeting, 2015.
32


33 Conclusions In patients with sensitizing EGFR mutation positive NSCLC who progress on a first or second generation EGFR TKI, the type of progression determines treatment option All patients should have a biopsy to evaluate for T790M prior to switching systemic therapy In patients where a tissue biopsy is not possible, a serum based test for T790M is reasonable Osimertinib is approved for patients who are T790M positive (with more agents on the way)
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
Targeted Therapies for Advanced NSCLC
 Targeted Therapies for Advanced NSCLC Current Clinical Developments Friday, June 3, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016 ASCO Annual Meeting
Targeted Therapies for Advanced NSCLC Current Clinical Developments Friday, June 3, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016 ASCO Annual Meeting
Inhibidores de EGFR Noemi Reguart, MD, PhD Hospital Clínic Barcelona IDIPAPS
 Inhibidores de EGFR Noemi Reguart, MD, PhD Hospital Clínic Barcelona IDIPAPS Driver Mutations to Classify Lung Cancer Unknown 36% KRAS 25% EGFR 15% ALK 4% HER2 2% Double Mut 2% BRAF 2% PIK3CA
Inhibidores de EGFR Noemi Reguart, MD, PhD Hospital Clínic Barcelona IDIPAPS Driver Mutations to Classify Lung Cancer Unknown 36% KRAS 25% EGFR 15% ALK 4% HER2 2% Double Mut 2% BRAF 2% PIK3CA
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
J. C.-H. Yang 1, L.V. Sequist 2, S. L. Geater 3, C.-M. Tsai 4, T. Mok 5, M. H. Schuler 6, N. Yamamoto 7, D. Massey 8, V. Zazulina 8, Yi-Long Wu 9
 Activity of afatinib in uncommon epidermal growth factor receptor (EGFR) mutations: Findings from three prospective trials of afatinib in EGFR mutation-positive lung cancer J. C.-H. Yang 1, L.V. Sequist
Activity of afatinib in uncommon epidermal growth factor receptor (EGFR) mutations: Findings from three prospective trials of afatinib in EGFR mutation-positive lung cancer J. C.-H. Yang 1, L.V. Sequist
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
The Rapidly Changing World of EGFR Mutation-Positive Acquired Resistance
 The Rapidly Changing World of EGFR Mutation-Positive Acquired Resistance H. Jack West, MD Swedish Cancer Institute Seattle, WA GRACE Targeted Therapies Forum September 16, 2017 Cleveland, OH EGFR Mutation-Positive
The Rapidly Changing World of EGFR Mutation-Positive Acquired Resistance H. Jack West, MD Swedish Cancer Institute Seattle, WA GRACE Targeted Therapies Forum September 16, 2017 Cleveland, OH EGFR Mutation-Positive
EGFR Mutation-Positive Acquired Resistance: Dominance of T790M
 Treatment of EGFR Mutation-Positive Acquired Resistance: T790M+ or T790M- H. Jack West, MD Swedish Cancer Institute, Seattle, WA EGFR Mutation-Positive Acquired Resistance: Dominance of T790M Yu, Clin
Treatment of EGFR Mutation-Positive Acquired Resistance: T790M+ or T790M- H. Jack West, MD Swedish Cancer Institute, Seattle, WA EGFR Mutation-Positive Acquired Resistance: Dominance of T790M Yu, Clin
Molecular Targets in Lung Cancer
 Molecular Targets in Lung Cancer Robert Ramirez, DO, FACP Thoracic and Neuroendocrine Oncology November 18 th, 2016 Disclosures Consulting and speaker fees for Ipsen Pharmaceuticals, AstraZeneca and Merck
Molecular Targets in Lung Cancer Robert Ramirez, DO, FACP Thoracic and Neuroendocrine Oncology November 18 th, 2016 Disclosures Consulting and speaker fees for Ipsen Pharmaceuticals, AstraZeneca and Merck
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Quale sequenza terapeutica nella malattia EGFR+
 Trattamento della malattia avanzata oncogene-addicted Quale sequenza terapeutica nella malattia EGFR+ Chiara Bennati AUSL della Romagna Ravenna, Italy A matter of fact Outline Can we improve PFS/OS with
Trattamento della malattia avanzata oncogene-addicted Quale sequenza terapeutica nella malattia EGFR+ Chiara Bennati AUSL della Romagna Ravenna, Italy A matter of fact Outline Can we improve PFS/OS with
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Management Strategies for Lung Cancer Sensitive or Resistant to EGRF Inhibitors
 Management Strategies for Lung Cancer Sensitive or Resistant to EGRF Inhibitors Conor E. Steuer, MD Assistant Professor The Winship Cancer Institute of Emory University July 27, 2017 1 Lung Cancer One
Management Strategies for Lung Cancer Sensitive or Resistant to EGRF Inhibitors Conor E. Steuer, MD Assistant Professor The Winship Cancer Institute of Emory University July 27, 2017 1 Lung Cancer One
Sequencing in EGFR-Mutated NSCLC: Does Order Matter?
 Sequencing in EGFR-Mutated NSCLC: Does Order Matter? Maximilian J. Hochmair, MD Otto Wagner Hospital Vienna, Austria Disclosures Honoraria: AstraZeneca, AbbVie, Pfizer, Boehringer Ingelheim, Roche, MSD,
Sequencing in EGFR-Mutated NSCLC: Does Order Matter? Maximilian J. Hochmair, MD Otto Wagner Hospital Vienna, Austria Disclosures Honoraria: AstraZeneca, AbbVie, Pfizer, Boehringer Ingelheim, Roche, MSD,
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Next Generation EGFR Inhibitors
 Next Generation EGFR Inhibitors Tony Mok MD Li Shu Fan Medical Foundation Professor of Clinical Oncology Dept. of Clinical Oncology The Chinese University of Hong Kong EGFR TKIs First Generation -Gefitinib
Next Generation EGFR Inhibitors Tony Mok MD Li Shu Fan Medical Foundation Professor of Clinical Oncology Dept. of Clinical Oncology The Chinese University of Hong Kong EGFR TKIs First Generation -Gefitinib
Emerging Algorithm for Optimal Sequencing of EGFR TKIs in EGFR Mutation Positive NSCLC
 Emerging Algorithm for Optimal Sequencing of EGFR TKIs in EGFR Mutation Positive NSCLC Keunchil Park, MD, PhD Samsung Medical Center, Sungkyunkwan University School of Medicine Faculty Disclosure Consulting
Emerging Algorithm for Optimal Sequencing of EGFR TKIs in EGFR Mutation Positive NSCLC Keunchil Park, MD, PhD Samsung Medical Center, Sungkyunkwan University School of Medicine Faculty Disclosure Consulting
Osimertinib Activity in Patients With Leptomeningeal Disease From Non-Small Cell Lung Cancer: Updated Results From the BLOOM Study
 Osimertinib Activity in Patients With Leptomeningeal Disease From Non-Small Cell Lung Cancer: Updated Results From the BLOOM Study Abstract 9002 Yang JC, Kim DW, Kim SW, Cho BC, Lee JS, Ye X, Yin X, Yang
Osimertinib Activity in Patients With Leptomeningeal Disease From Non-Small Cell Lung Cancer: Updated Results From the BLOOM Study Abstract 9002 Yang JC, Kim DW, Kim SW, Cho BC, Lee JS, Ye X, Yin X, Yang
Agenda. 6:30pm 7:00pm. Dinner. 7:00pm 7:15pm. NSCLC Treatment in 2014: Focus on Use of 2nd Generation TKIs in Clinical Practice.
 Agenda 6:30pm 7:00pm Dinner 7:00pm 7:15pm Welcome and Introductions Natasha Leighl, MD 7:15pm 7:50pm 7:50pm 8:00pm NSCLC Treatment in 2014: Focus on Use of 2nd Generation TKIs in Clinical Practice Questions
Agenda 6:30pm 7:00pm Dinner 7:00pm 7:15pm Welcome and Introductions Natasha Leighl, MD 7:15pm 7:50pm 7:50pm 8:00pm NSCLC Treatment in 2014: Focus on Use of 2nd Generation TKIs in Clinical Practice Questions
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse?
 Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC. Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy
 PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy Prognostic versus predictive Prognostic: In presence of the biomarker patient outcome
PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy Prognostic versus predictive Prognostic: In presence of the biomarker patient outcome
Optimum Sequencing of EGFR targeted therapy in NSCLC. Dr. Sema SEZGİN GÖKSU Akdeniz Univercity, Antalya, Turkey
 Optimum Sequencing of EGFR targeted therapy in NSCLC Dr. Sema SEZGİN GÖKSU Akdeniz Univercity, Antalya, Turkey Lung cancer NSCLC SCLC adeno squamous EGFR ALK ROS1 BRAF HER2 KRAS EGFR Transl Lung Cancer
Optimum Sequencing of EGFR targeted therapy in NSCLC Dr. Sema SEZGİN GÖKSU Akdeniz Univercity, Antalya, Turkey Lung cancer NSCLC SCLC adeno squamous EGFR ALK ROS1 BRAF HER2 KRAS EGFR Transl Lung Cancer
Changing demographics of smoking and its effects during therapy
 Changing demographics of smoking and its effects during therapy Egbert F. Smit MD PhD. Dept. Pulmonary Diseases, Vrije Universiteit Medical Centre, Amsterdam, The Netherlands Smoking prevalence adults
Changing demographics of smoking and its effects during therapy Egbert F. Smit MD PhD. Dept. Pulmonary Diseases, Vrije Universiteit Medical Centre, Amsterdam, The Netherlands Smoking prevalence adults
Treatment of EGFR-Mutation+ NSCLC in 1st- and 2nd-Line
 Treatment of EGFR-Mutation+ NSCLC in 1st- and 2nd-Line Martin Reck David F. Heigener Department of Thoracic Oncology Hospital Grosshansdorf Germany Identification of driver mutation in tumor specimens
Treatment of EGFR-Mutation+ NSCLC in 1st- and 2nd-Line Martin Reck David F. Heigener Department of Thoracic Oncology Hospital Grosshansdorf Germany Identification of driver mutation in tumor specimens
Improving outcomes for NSCLC patients with brain metastases
 Improving outcomes for NSCLC patients with brain metastases Martin Schuler West German Cancer Center, Essen, Germany In Switzerland, afatinib is approved as monotherapy for patients with non-small cell
Improving outcomes for NSCLC patients with brain metastases Martin Schuler West German Cancer Center, Essen, Germany In Switzerland, afatinib is approved as monotherapy for patients with non-small cell
Slide 1. Slide 2 Maintenance Therapy Options. Slide 3. Maintenance Therapy in the Management of Non-Small Cell Lung Cancer. Maintenance Chemotherapy
 Slide 1 Maintenance Therapy in the Management of Non-Small Cell Lung Cancer Frances A Shepherd, MD FRCPC Scott Taylor Chair in Lung Cancer Research Princess Margaret Hospital, Professor of Medicine, University
Slide 1 Maintenance Therapy in the Management of Non-Small Cell Lung Cancer Frances A Shepherd, MD FRCPC Scott Taylor Chair in Lung Cancer Research Princess Margaret Hospital, Professor of Medicine, University
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
EGFR TKI sequencing: does order matter?
 EGFR TKI sequencing: does order matter? Nicolas Girard Thorax Institut Curie-Montsouris, Paris, France In Switzerland, afatinib is approved as monotherapy for patients with non-small cell lung cancer (Stage
EGFR TKI sequencing: does order matter? Nicolas Girard Thorax Institut Curie-Montsouris, Paris, France In Switzerland, afatinib is approved as monotherapy for patients with non-small cell lung cancer (Stage
EGFR MUTATIONS: EGFR PATHWAY AND SELECTION OF FIRST-LINE THERAPY WITH TYROSINE KINASE INHIBITORS
 EGFR MUTATIONS: EGFR PATHWAY AND SELECTION OF FIRST-LINE THERAPY WITH TYROSINE KINASE INHIBITORS Federico Cappuzzo Istituto Clinico Humanitas IRCCS Rozzano-Italy The EGFR/HER Family Ligand binding domain
EGFR MUTATIONS: EGFR PATHWAY AND SELECTION OF FIRST-LINE THERAPY WITH TYROSINE KINASE INHIBITORS Federico Cappuzzo Istituto Clinico Humanitas IRCCS Rozzano-Italy The EGFR/HER Family Ligand binding domain
Slide 1. Slide 2. Slide 3. Disclosures. Personalized Medicine for Advanced NSCLC in East Asia. No conflicts related to this presentation
 Slide 1 12 th International Lung Cancer Conference Personalized Medicine for Advanced NSCLC in East Asia Masahiro Tsuboi, M.D., Ph.D. Group Chair, Lung Cancer Surgical Study Group in Japan Clinical Oncology
Slide 1 12 th International Lung Cancer Conference Personalized Medicine for Advanced NSCLC in East Asia Masahiro Tsuboi, M.D., Ph.D. Group Chair, Lung Cancer Surgical Study Group in Japan Clinical Oncology
D Ross Camidge, MD, PhD
 i n t e r v i e w D Ross Camidge, MD, PhD Dr Camidge is Director of the Thoracic Oncology Clinical Program and Associate Director for Clinical Research at the University of Colorado Cancer Center in Aurora,
i n t e r v i e w D Ross Camidge, MD, PhD Dr Camidge is Director of the Thoracic Oncology Clinical Program and Associate Director for Clinical Research at the University of Colorado Cancer Center in Aurora,
Maintenance paradigm in non-squamous NSCLC
 Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Overall survival with afatinib versus chemotherapy in patients with NSCLC harboring common EGFR
 Overall survival with afatinib versus chemotherapy in patients with NSCLC harboring common EGFR mutations: subgroup analyses by race/ethnicity in LUX-Lung 3 and LUX-Lung 6 Yi-Long Wu, 1 Lecia V Sequist,
Overall survival with afatinib versus chemotherapy in patients with NSCLC harboring common EGFR mutations: subgroup analyses by race/ethnicity in LUX-Lung 3 and LUX-Lung 6 Yi-Long Wu, 1 Lecia V Sequist,
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
State of the Art Treatment of Lung Cancer Ravi Salgia, MD, PhD
 State of the Art Treatment of Lung Cancer Ravi Salgia, MD, PhD Professor and Chair Arthur & Rosalie Kaplan Chair Medical Oncology and Therapeutics Research Nothing to disclose DISCLOSURE Objectives Lung
State of the Art Treatment of Lung Cancer Ravi Salgia, MD, PhD Professor and Chair Arthur & Rosalie Kaplan Chair Medical Oncology and Therapeutics Research Nothing to disclose DISCLOSURE Objectives Lung
Targeted therapies for advanced non-small cell lung cancer. Tom Stinchcombe Duke Cancer Insitute
 Targeted therapies for advanced non-small cell lung cancer Tom Stinchcombe Duke Cancer Insitute Topics ALK rearranged NSCLC ROS1 rearranged NSCLC EGFR mutation: exon 19/exon 21 L858R and uncommon mutations
Targeted therapies for advanced non-small cell lung cancer Tom Stinchcombe Duke Cancer Insitute Topics ALK rearranged NSCLC ROS1 rearranged NSCLC EGFR mutation: exon 19/exon 21 L858R and uncommon mutations
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007
 Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007 Bruce E. Johnson, MD Dana-Farber Cancer Institute, Brigham and Women s Hospital, and Harvard
Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007 Bruce E. Johnson, MD Dana-Farber Cancer Institute, Brigham and Women s Hospital, and Harvard
INNOVATION IN LUNG CANCER MANAGEMENT. Federico Cappuzzo Department of Oncology-Hematology, AUSL della Romagna, Ravenna, Italy
 INNOVATION IN LUNG CANCER MANAGEMENT Federico Cappuzzo Department of Oncology-Hematology, AUSL della Romagna, Ravenna, Italy FIRST-LINE THERAPY FOR METASTATIC NSCLC IN 216 Stratification for EGFR, ALK
INNOVATION IN LUNG CANCER MANAGEMENT Federico Cappuzzo Department of Oncology-Hematology, AUSL della Romagna, Ravenna, Italy FIRST-LINE THERAPY FOR METASTATIC NSCLC IN 216 Stratification for EGFR, ALK
Frequency of Epidermal Growth Factor Mutation Status and Its Effect on Outcome of Patients with Adenocarcinoma of the Lung
 Journal of Cancer Therapy, 2014, 5, 1012-1020 Published Online September 2014 in SciRes. http://www.scirp.org/journal/jct http://dx.doi.org/10.4236/jct.2014.511106 Frequency of Epidermal Growth Factor
Journal of Cancer Therapy, 2014, 5, 1012-1020 Published Online September 2014 in SciRes. http://www.scirp.org/journal/jct http://dx.doi.org/10.4236/jct.2014.511106 Frequency of Epidermal Growth Factor
IRESSA (Gefitinib) The Journey. Anne De Bock Portfolio Leader, Oncology/Infection European Regulatory Affairs AstraZeneca
 The Journey. Anne De Bock Portfolio Leader, Oncology/Infection European Regulatory Affairs AstraZeneca") IRESSA (Gefitinib) The Journey Anne De Bock Portfolio Leader, Oncology/Infection European Regulatory Affairs AstraZeneca Overview The Drug The Biomarker and Clinical Trials Sampling Lessons Learned The
IRESSA (Gefitinib) The Journey Anne De Bock Portfolio Leader, Oncology/Infection European Regulatory Affairs AstraZeneca Overview The Drug The Biomarker and Clinical Trials Sampling Lessons Learned The
Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement. Reference Slides Introduction
 Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement Reference Slides Introduction EML4-ALK Fusion Oncogene Key Driver in 3% to 7% NSCLC Inversion or Translocation
Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement Reference Slides Introduction EML4-ALK Fusion Oncogene Key Driver in 3% to 7% NSCLC Inversion or Translocation
IMPORTANT PATHWAYS TO TARGET IN (ADVANCED) NSCLC:
 NSCLC:") IMPORTANT PATHWAYS TO TARGET IN (ADVANCED) NSCLC: A focus on EGFR-inhibition and implications for clinical practice Floriana Morgillo, MD PhD and Morena Fasano, MD PhD Faculty of Medicine, Università degli
IMPORTANT PATHWAYS TO TARGET IN (ADVANCED) NSCLC: A focus on EGFR-inhibition and implications for clinical practice Floriana Morgillo, MD PhD and Morena Fasano, MD PhD Faculty of Medicine, Università degli
Targeted Therapy for NSCLC: EGFR and ALK Fadlo R. Khuri, MD
 EGFR and ALK Fadlo R. Khuri, MD President, American University of Beirut Professor of Medicine July 26, 2018 A great year end! Targeted Therapy for NSCLC: Evolving Landscape of Lung Adenocarcinoma NSCLC
EGFR and ALK Fadlo R. Khuri, MD President, American University of Beirut Professor of Medicine July 26, 2018 A great year end! Targeted Therapy for NSCLC: Evolving Landscape of Lung Adenocarcinoma NSCLC
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer.
 Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf
 MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf OUTLINE Background and Concept Switch Maintenance Continuation Maintenance
MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf OUTLINE Background and Concept Switch Maintenance Continuation Maintenance
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? VEGF Is the Only Angiogenic Factor Present Throughout the Tumor Life Cycle
 Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer
 Non-Small Cell Lung Cancer") Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Making the first decision: EGFR mutation-positive NSCLC in the advanced setting
 ELCC May 217, Switzerland Making the first decision: EGFR mutation-positive NSCLC in the advanced setting Noemí Reguart, MD, PhD Hospital Clínic de Barcelona, Spain Disclosures Consultant or Advisory Role
ELCC May 217, Switzerland Making the first decision: EGFR mutation-positive NSCLC in the advanced setting Noemí Reguart, MD, PhD Hospital Clínic de Barcelona, Spain Disclosures Consultant or Advisory Role
Target therapy nel NSCLC con EGFR M+ Cesare Gridelli Division of Medical Oncology S.G. Moscati Hospital Avellino (Italy)
") Target therapy nel NSCLC con EGFR M+ Cesare Gridelli Division of Medical Oncology S.G. Moscati Hospital Avellino (Italy) cgridelli@libero.it First-Line Treatment of Advanced NSCLC EGFR-mutation analysis
Target therapy nel NSCLC con EGFR M+ Cesare Gridelli Division of Medical Oncology S.G. Moscati Hospital Avellino (Italy) cgridelli@libero.it First-Line Treatment of Advanced NSCLC EGFR-mutation analysis
Maintenance Therapy for Advanced NSCLC: Which Patients, Which Approach?
 Maintenance Therapy for Advanced NSCLC: Which Patients, Which Approach? Mark A. Socinski, MD Visiting Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology
Maintenance Therapy for Advanced NSCLC: Which Patients, Which Approach? Mark A. Socinski, MD Visiting Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology
Post-marketing observational study of Japanese patients with EGFR mutation-positive (EGFRm+) NSCLC treated with daily afatinib (final report)
 NSCLC treated with daily afatinib (final report)") Post-marketing observational study of Japanese patients with EGFR mutation-positive (EGFRm+) NSCLC treated with daily afatinib (final report) Nobuyuki Yamamoto, 1 Toshihiro Nukiwa, 2 Yoichi Nakanishi,
Post-marketing observational study of Japanese patients with EGFR mutation-positive (EGFRm+) NSCLC treated with daily afatinib (final report) Nobuyuki Yamamoto, 1 Toshihiro Nukiwa, 2 Yoichi Nakanishi,
Summary of the risk management plan (RMP) for Tagrisso (osimertinib)
 for Tagrisso (osimertinib)") EMA/2497/2016 Summary of the risk management plan (RMP) for Tagrisso (osimertinib) This is a summary of the risk management plan (RMP) for Tagrisso, which details the measures to be taken in order to ensure
EMA/2497/2016 Summary of the risk management plan (RMP) for Tagrisso (osimertinib) This is a summary of the risk management plan (RMP) for Tagrisso, which details the measures to be taken in order to ensure
Exploring Personalized Therapy for First Line Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC)
") Exploring Personalized Therapy for First Line Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC) Suresh S. Ramalingam, MD Director of Thoracic Oncology Associate Professor Emory University Atlanta,
Exploring Personalized Therapy for First Line Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC) Suresh S. Ramalingam, MD Director of Thoracic Oncology Associate Professor Emory University Atlanta,
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW. Erlotinib for the third or fourth-line treatment of NSCLC January 2012
 Disease background LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Erlotinib for the third or fourth-line treatment of NSCLC January 2012 Lung cancer is the second most common cancer in the UK (after breast),
Disease background LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Erlotinib for the third or fourth-line treatment of NSCLC January 2012 Lung cancer is the second most common cancer in the UK (after breast),
Afatinib in patients with EGFR mutation-positive NSCLC harboring uncommon mutations: overview of clinical data
 Afatinib in patients with EGFR mutation-positive NSCLC harboring uncommon mutations: overview of clinical data Oscar Arrieta, 1 Pedro De Marchi, 2 Nobuyuki Yamamoto, 3 Chong-Jen Yu, 4 Sai-Hong I Ou, 5
Afatinib in patients with EGFR mutation-positive NSCLC harboring uncommon mutations: overview of clinical data Oscar Arrieta, 1 Pedro De Marchi, 2 Nobuyuki Yamamoto, 3 Chong-Jen Yu, 4 Sai-Hong I Ou, 5
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Lung Cancer. Karen Reckamp, MD Medical Director, Clinical Research. Click to edit Master Presentation Date
 Advances in Targeted Therapy for Lung Cancer Karen Reckamp, MD Medical Director, Clinical Research City of Hope Comprehensive Cancer Center Click to edit Master Presentation Date Disclosures Consultant
Advances in Targeted Therapy for Lung Cancer Karen Reckamp, MD Medical Director, Clinical Research City of Hope Comprehensive Cancer Center Click to edit Master Presentation Date Disclosures Consultant
TKI en primera línea EGFR mutado:importancia del equilibrio eficacia tolerabilidad
 TKI en primera línea EGFR mutado:importancia del equilibrio eficacia tolerabilidad Dra Pilar Lianes Barragan Consorcio Sanitario del Maresme (Barcelona) Indice Epidemiología TKI en primera línea Eficacia
TKI en primera línea EGFR mutado:importancia del equilibrio eficacia tolerabilidad Dra Pilar Lianes Barragan Consorcio Sanitario del Maresme (Barcelona) Indice Epidemiología TKI en primera línea Eficacia
Best of ASCO 2014 Lung
 Best of ASCO 214 Lung Heather Wakelee, MD Associate Professor of Medicine, Oncology Stanford Cancer Institute Stanford, California USA Outline ALK: 82: 1st line crizotinib Profile 114 83: ASCEND ceritinib
Best of ASCO 214 Lung Heather Wakelee, MD Associate Professor of Medicine, Oncology Stanford Cancer Institute Stanford, California USA Outline ALK: 82: 1st line crizotinib Profile 114 83: ASCEND ceritinib
Joachim Aerts Erasmus MC Rotterdam, Netherlands. Drawing the map: molecular characterization of NSCLC
 Joachim Aerts Erasmus MC Rotterdam, Netherlands Drawing the map: molecular characterization of NSCLC Disclosures Honoraria for advisory board/consultancy/speakers fee Eli Lilly Roche Boehringer Ingelheim
Joachim Aerts Erasmus MC Rotterdam, Netherlands Drawing the map: molecular characterization of NSCLC Disclosures Honoraria for advisory board/consultancy/speakers fee Eli Lilly Roche Boehringer Ingelheim
Best of ASCO 2014: Highlights in Metastatic Non-Small Cell Lung Cancer
 Best of ASCO 2014: Highlights in Metastatic Non-Small Cell Lung Cancer Howard (Jack) West, M JackWestM@gmail.com @JackWestM Swedish Cancer Institute Seattle, WA Best of ASCO 2014 Seattle, WA Learning Objectives
Best of ASCO 2014: Highlights in Metastatic Non-Small Cell Lung Cancer Howard (Jack) West, M JackWestM@gmail.com @JackWestM Swedish Cancer Institute Seattle, WA Best of ASCO 2014 Seattle, WA Learning Objectives
Personalized Medicine for Advanced NSCLC in East Asia
 Personalized Medicine for Advanced NSCLC in East Asia - Update treatment strategy for NSCLC based on Japanese clinical practice guideline - Masahiro Tsuboi, M.D., Ph.D. Associate-professor, School of Medicine,
Personalized Medicine for Advanced NSCLC in East Asia - Update treatment strategy for NSCLC based on Japanese clinical practice guideline - Masahiro Tsuboi, M.D., Ph.D. Associate-professor, School of Medicine,
NSCLC: Terapia medica nella fase avanzata. Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza
 NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
Osimertinib as first-line treatment of EGFR mutant advanced nonsmall-cell
 Editorial Osimertinib as first-line treatment of EGFR mutant advanced nonsmall-cell lung cancer Chong-Kin Liam Department of Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia
Editorial Osimertinib as first-line treatment of EGFR mutant advanced nonsmall-cell lung cancer Chong-Kin Liam Department of Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia
Sao Paulo, Abril 2014
 Tratamento de Manutencao e outros Sao Paulo, Abril 2014 Rogerio C. Lilenbaum, M.D. Professor of Medicine Yale Cancer Center Chief Medical Officer Smilow Cancer Hospital What Is Maintenance Therapy? Use
Tratamento de Manutencao e outros Sao Paulo, Abril 2014 Rogerio C. Lilenbaum, M.D. Professor of Medicine Yale Cancer Center Chief Medical Officer Smilow Cancer Hospital What Is Maintenance Therapy? Use
Long term survival in EGFR positive NSCLC patient. Dr.ssa G. Zago Oncologia Medica 2 Istituto Oncologico Veneto, IOV
 Long term survival in EGFR positive NSCLC patient Dr.ssa G. Zago Oncologia Medica 2 Istituto Oncologico Veneto, IOV Medical history and diagnosis Male, caucasian 60 years old Former smoker (stop > 15 years)
Long term survival in EGFR positive NSCLC patient Dr.ssa G. Zago Oncologia Medica 2 Istituto Oncologico Veneto, IOV Medical history and diagnosis Male, caucasian 60 years old Former smoker (stop > 15 years)
2 nd line Therapy and Beyond NSCLC. Alan Sandler, M.D. Oregon Health & Science University
 2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
Hacia una mayor individualización clínica en el CPNM. J.M. Sánchez Torres H.U. Princesa, Madrid
 Hacia una mayor individualización clínica en el CPNM J.M. Sánchez Torres H.U. Princesa, Madrid Lung cancer histologic subtypes NSCLC (80-85%) SCLC (15-20%) Squamous carcinoma (25 30%) Non-squamous carcinoma
Hacia una mayor individualización clínica en el CPNM J.M. Sánchez Torres H.U. Princesa, Madrid Lung cancer histologic subtypes NSCLC (80-85%) SCLC (15-20%) Squamous carcinoma (25 30%) Non-squamous carcinoma
CURRENT STANDARD OF CARE OF LUNG CANCER. Maroun El-Khoury, MD Consultant Oncologist/Hematologist American Hospital Dubai President of Medical staff
 CURRENT STANDARD OF CARE OF LUNG CANCER Maroun El-Khoury, MD Consultant Oncologist/Hematologist American Hospital Dubai President of Medical staff Biopsy: Establish Diagnosis, Determine Histologic Subtype,
CURRENT STANDARD OF CARE OF LUNG CANCER Maroun El-Khoury, MD Consultant Oncologist/Hematologist American Hospital Dubai President of Medical staff Biopsy: Establish Diagnosis, Determine Histologic Subtype,
Recent Advances in Lung Cancer: Updates from ASCO 2017
 Recent Advances in Lung Cancer: Updates from ASCO 2017 Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University of Pennsylvania 6/15/2017
Recent Advances in Lung Cancer: Updates from ASCO 2017 Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University of Pennsylvania 6/15/2017
1st line chemotherapy and contribution of targeted agents
 ESMO PRECEPTORSHIP PROGRAMME NON-SM ALL-CELL LUNG CANCER 1st line chemotherapy and contribution of targeted agents Yi-Long Wu Guangdong Lung Cancer Institute Guangdong General Hospital Guangdong Academy
ESMO PRECEPTORSHIP PROGRAMME NON-SM ALL-CELL LUNG CANCER 1st line chemotherapy and contribution of targeted agents Yi-Long Wu Guangdong Lung Cancer Institute Guangdong General Hospital Guangdong Academy
Targeted therapy in NSCLC: do we progress? Prof. Dr. V. Surmont. Masterclass 27 september 2018
 Targeted therapy in NSCLC: do we progress? Prof. Dr. V. Surmont Masterclass 27 september 2018 Outline Introduction EGFR TKI ALK TKI TKI for uncommon driver mutations Take home messages The promise of
Targeted therapy in NSCLC: do we progress? Prof. Dr. V. Surmont Masterclass 27 september 2018 Outline Introduction EGFR TKI ALK TKI TKI for uncommon driver mutations Take home messages The promise of
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
Nivolumab: esperienze italiane nel carcinoma polmonare avanzato
 NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Molecular Analysis for Targeted Therapy of Non-Small-Cell Lung Cancer Page 1 of 52 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Molecular Analysis for Targeted
Molecular Analysis for Targeted Therapy of Non-Small-Cell Lung Cancer Page 1 of 52 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Molecular Analysis for Targeted
GIOTRIF (AFATINIB*) For journalists outside the US/UK/Canada only 1. WHAT IS GIOTRIF (AFATINIB*)? 2. HOW DOES GIOTRIF (AFATINIB*) WORK?
 For journalists outside the US/UK/Canada only 1. WHAT IS GIOTRIF (AFATINIB*)? 2. HOW DOES GIOTRIF (AFATINIB*) WORK?") For journalists outside the US/UK/Canada only GIOTRIF (AFATINIB*) 1. What is GIOTRIF (afatinib*)? 2. How does GIOTRIF (afatinib*) work? 3. Data overview 4. Clinical potential 5. GIOTRIF (afatinib*) approval
For journalists outside the US/UK/Canada only GIOTRIF (AFATINIB*) 1. What is GIOTRIF (afatinib*)? 2. How does GIOTRIF (afatinib*) work? 3. Data overview 4. Clinical potential 5. GIOTRIF (afatinib*) approval
Sequence or intercalation of use of targeted agents and Chemotherapy Definition of progression under TKI
 ESMO PRECEPTORSHIP PROGRAMME NON-SM ALL-CELL LUNG CANCER Strategic Approaches Sequence or intercalation of use of targeted agents and Chemotherapy Definition of progression under TKI Yi-Long Wu Guangdong
ESMO PRECEPTORSHIP PROGRAMME NON-SM ALL-CELL LUNG CANCER Strategic Approaches Sequence or intercalation of use of targeted agents and Chemotherapy Definition of progression under TKI Yi-Long Wu Guangdong
Original Article. Abstract
 Japanese Journal of Clinical Oncology, 2015, 45(7) 670 676 doi: 10.1093/jjco/hyv054 Advance Access Publication Date: 15 April 2015 Original Article Original Article Efficacy of chemotherapy after first-line
Japanese Journal of Clinical Oncology, 2015, 45(7) 670 676 doi: 10.1093/jjco/hyv054 Advance Access Publication Date: 15 April 2015 Original Article Original Article Efficacy of chemotherapy after first-line
ASCO Highlights and Controversies in advanced Lung Cancer. Torino, 11 giugno 2015
 ASCO 2015 Highlights and Controversies in advanced Lung Cancer Torino, 11 giugno 2015 Paolo Bironzo AOU S Luigi Gonzaga - Orbassano Scuola di Specializzazione in Oncologia Medica Università di Torino What
ASCO 2015 Highlights and Controversies in advanced Lung Cancer Torino, 11 giugno 2015 Paolo Bironzo AOU S Luigi Gonzaga - Orbassano Scuola di Specializzazione in Oncologia Medica Università di Torino What
1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC
 1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC Dr Ross Soo, FRACP National University Cancer Institute, Singapore National University Health System Cancer Science
1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC Dr Ross Soo, FRACP National University Cancer Institute, Singapore National University Health System Cancer Science
Profilo di tossicita degli inibitori di EGFR
 Dipartimento di Oncologia direttore dr. Gianpiero Fasola NSCLC EGFR mutato: quali opzioni terapeutiche? Profilo di tossicita degli inibitori di EGFR Padova 17 settembre 2105 Alessandro Follador TKis in
Dipartimento di Oncologia direttore dr. Gianpiero Fasola NSCLC EGFR mutato: quali opzioni terapeutiche? Profilo di tossicita degli inibitori di EGFR Padova 17 settembre 2105 Alessandro Follador TKis in
Rociletinib (CO-1686) April, 2015
 April, 2015") Rociletinib (CO-1686) April, 2015 Lung adenocarcinoma is increasingly treated according to driver mutation Lung cancer incidence Worldwide: 1.2M cases per year UK: 43K cases per year Activating mutations
Rociletinib (CO-1686) April, 2015 Lung adenocarcinoma is increasingly treated according to driver mutation Lung cancer incidence Worldwide: 1.2M cases per year UK: 43K cases per year Activating mutations
First-line treatment of EGFR-mutated nonsmall cell lung cancer: critical review on study methodology
 REVIEW NONSMALL CELL LUNG CANCER First-line treatment of EGFR-mutated nonsmall cell lung cancer: critical review on study methodology Martin Sebastian 1, Alexander Schmittel 2 and Martin Reck 3 Affiliations:
REVIEW NONSMALL CELL LUNG CANCER First-line treatment of EGFR-mutated nonsmall cell lung cancer: critical review on study methodology Martin Sebastian 1, Alexander Schmittel 2 and Martin Reck 3 Affiliations:
Second-line treatment for advanced NSCLC
 UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Second-line treatment for advanced NSCLC Silvia Novello silvia.novello@unito.it UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Life was so simple back in 2008 Di
UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Second-line treatment for advanced NSCLC Silvia Novello silvia.novello@unito.it UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Life was so simple back in 2008 Di
Antiangiogenici in combinazione a chemioterapia in prima linea: bevacizumab
 Micro-ambiente tumorale. Antiangiogenici e immunoterapia: miti e realtà Milano, 11 Ottobre 2016 Antiangiogenici in combinazione a chemioterapia in prima linea: bevacizumab Francesco Grossi U.O.S. Tumori
Micro-ambiente tumorale. Antiangiogenici e immunoterapia: miti e realtà Milano, 11 Ottobre 2016 Antiangiogenici in combinazione a chemioterapia in prima linea: bevacizumab Francesco Grossi U.O.S. Tumori
Next-Generation Covalent Irreversible Kinase Inhibitors in NSCLC: Focus on Afatinib
 BioDrugs (2015) 29:167 183 DOI 10.1007/s40259-015-0130-9 REVIEW ARTICLE Next-Generation Covalent Irreversible Kinase Inhibitors in NSCLC: Focus on Afatinib Vera Hirsh 1 Published online: 30 June 2015 The
BioDrugs (2015) 29:167 183 DOI 10.1007/s40259-015-0130-9 REVIEW ARTICLE Next-Generation Covalent Irreversible Kinase Inhibitors in NSCLC: Focus on Afatinib Vera Hirsh 1 Published online: 30 June 2015 The
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
EGFR Tyrosine Kinase Inhibitors Prolong Overall Survival in EGFR Mutated Non-Small-Cell Lung Cancer Patients with Postsurgical Recurrence
 102 Journal of Cancer Research Updates, 2012, 1, 102-107 EGFR Tyrosine Kinase Inhibitors Prolong Overall Survival in EGFR Mutated Non-Small-Cell Lung Cancer Patients with Postsurgical Recurrence Kenichi
102 Journal of Cancer Research Updates, 2012, 1, 102-107 EGFR Tyrosine Kinase Inhibitors Prolong Overall Survival in EGFR Mutated Non-Small-Cell Lung Cancer Patients with Postsurgical Recurrence Kenichi
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We
 Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
11/21/2009. Erlotinib in KRAS Mt patients. Bevacizumab in Squamous patients
 Decision-Making in Non-Small Cell Lung Cancer (NSCLC): Moving from Empiric to Personalized & Molecular-based Therapy David R. Gandara, MD University of California Davis Cancer Center Disclosures Research
Decision-Making in Non-Small Cell Lung Cancer (NSCLC): Moving from Empiric to Personalized & Molecular-based Therapy David R. Gandara, MD University of California Davis Cancer Center Disclosures Research
Management of EGFR-mutant NSCLC. Jonathan Riess, MD, MS Assistant Professor UC Davis Comprehensive Cancer Center
 Management of EGFR-mutant NSCLC Jonathan Riess, MD, MS Assistant Professor UC Davis Comprehensive Cancer Center Disclosures Research Funding: Merck, Novartis, AstraZeneca, Millenium Consulting: AbbVie,
Management of EGFR-mutant NSCLC Jonathan Riess, MD, MS Assistant Professor UC Davis Comprehensive Cancer Center Disclosures Research Funding: Merck, Novartis, AstraZeneca, Millenium Consulting: AbbVie,
Targeted therapy in lung cancer : experience of NIO-RABAT
 Targeted therapy in lung cancer : experience of NIO-RABAT I.ELGHISSASSI, H.ERRIHANI Medical oncology department, NIO- RABAT 02-05- 2012, FEZ In Morocco, lung cancer is the most common tumor among men At
Targeted therapy in lung cancer : experience of NIO-RABAT I.ELGHISSASSI, H.ERRIHANI Medical oncology department, NIO- RABAT 02-05- 2012, FEZ In Morocco, lung cancer is the most common tumor among men At