CURRENT GUIDELINES FOR SEPSIS MANAGEMENT
|
|
|
- Emmeline Sims
- 5 years ago
- Views:
Transcription





1 HELLENIC SEPSIS STUDY GROUP CURRENT GUIDELINES FOR SEPSIS MANAGEMENT Evangelos J. Giamarellos-Bourboulis, MD, PhD Associate Professor of Medicine 4 th Department of Internal Medicine, National and Kapodistrian University of Athens, Medical School, Greece Guest Professor, Center for Sepsis Control and Care, Jena University Hospital, Germany
2 CONFLICT OF INTEREST DISCLOSURE None for this presentation Honoraria (paid to the University of Athens): AbbVie USA, Astellas Greece, Biotest Germany, Brahms GmbH, InflaRx GmbH Germany, MSD Greece, Novartis Greece SA, Pfizer Greece Consultant: Astellas Greece, InflaRx GmbH, Germany, Roche CH, Xbiotech USA Independent educational grants: AbbVie USA, Abbott CH, Axis Shield, UK, Inflammatix USA, InflaRx GmbH Germany, Xbiotech USA European Grants: FrameWork 7 program HemoSpec, Horizon2020 Marie-Curie Grant European Sepsis Academy.


3 Rhodes A, et al. Crit Care Med 2017; 45: 486 PILLARS OF SEPSIS MANAGEMENT Sepsis management Haemodynamic therapy Source control Antimicrobials ADJUNCTIVE THERAPY
4 % patients EARLY START OF ANTIMICROBIALS: MAIN GOAL (Kumar A, et al. Crit Care Med 2006; 34: 1589) Time (hours) from start of hypotension
 A")

5 SEPSIS-3 DEFINITION (Singer M, et al. JAMA 2016; 315: 801) A life-threatening organ dysfunction caused by a dysregulated host response to infection.
6 SEQUENTIAL ORGAN FAILURE ASSESSMENT SOFA score po 2 /FiO <400 <300 <200 <100 Platelets (x10 3 mm 3 ) 150 <150 <100 <50 <20 Bilirubin (mg/dl) < Cardiovascular MAP 70mmHg MAP < 70mmHg <5* 1** >1** Glasgow Coma Scale <6 Creatinine (mg/dl) (or urine/day) < (<500) 5.0 (<200) *μg/kg/min of dopamine **μg/kg/min of noerpinephrine
7 INFECTION SUSPICION qsofa (quick SOFA) 2 qsofa Altered mental status 22 breaths/minute Systolic blood pressure<100 mmηg EVALUATE ORGAN DYSFUNCTION SOFA 2 admitted in the ER or increase from the baseline SEPSIS SEPTIC SHOCK Despite fluid resuscitation Mean arterial pressure <65mmHg Lactate 2 mmol/l NEED for vasopressors ER: emergency department
 100 Survival Cumulative")

8 % patients THE OTHER READ-OUT (Kumar A, et al. Crit Care Med 2006; 34: 1589) 100 Survival Cumulative effective antimicrobial therapy Time (hours) from start of hypotension
9 RESISTANCE PATTERNS: ER ADMISSION (Koupetori M, et al. BMC Infect Dis 2014; 14: 272) *p< 0.05 between the two periods
10 EPIDEMIOLOGY AS A GUIDING TOOL (Koupetori M, et al. BMC Infect Dis 2014; 14: 272) OR 95%CI p APACHE II> History of COPD Pigtail ureter catheterization Chronic hemodialysis Intake of antibiotics 3 months Residence in long-term care facility <0.0001


11 A MULTI-CENTER SIMULATION: THE HELLENIC SEPSIS STUDY GROUP : 32 CENTERS : 3 CENTERS : 2 CENTERS : 1 CENTER

12 EMPIRICAL ANTIMICROBIALS OUTSIDE THE ICU WITH SOFA 7 3 rd gen. cephalosporin +/- metronidazole Piperacillin/tazobactam Carbapanem EMPIRICAL ANTIMICROBIALS OUTSIDE THE ICU WITH SOFA >8 Piperacillin/tazobactam +/- colistin +/- glycopeptide Carbapanem +/- colistin +/- glycopeptide
13 Serum concentration Serum concentration Serum concentration INCREASE T>MIC FOR B-LACTAMS (MacVane SH, et al. Int J Antimicrob Agents 2014; 43: 105) INCREASE THE DOSE 1g q8h 2g q8h PROLONG INFUSION 1g 0.5H 2g 3H 25% MIC 25% MIC Time (hours) 1g q8h (0.5H) 2g q8h (3H) Time (hours) 50% BOTH!!! MIC Time (hours)
14 HOW ABOUT COLISTIN? (Plachouras D, et al. Antimicrob Agents Chemother 2009; 53: 3430) Colistin methasulfonate is an inactive pro-drug Hydrolyzed into active colistin A and colistin B MIC breakpoint 2μg/ml ( 4μg/ml for P.aeruginosa) 3MU (240mg) q8h in 18 critically ill patients Serum concentrations after 1 st dose Serum concentrations after 4 th dose (24h)
15 NEED FOR INITIAL LOADING DOSE OF 9MU (Mohamed AF, et al. Antimicrob Agents Chemother 2012; 56: 4241)
16 UPDATED DOSING REGIMENS TO ACHIEVE PLASMA COLISTIN C ss 2 mg/l (Nation RL, et al. Clin Infect Dis 2017; 64: 565) 9 million units loading dose to all patients CrCl (ml/min) Daily dose (millions divided into two) to < to < to < to < to < to < to < to < to <
17 OPTIONS FOR ADJUNCTIVE THERAPIES IN SEVERE INFECTIONS: SSC 2016 INTERVENTION COMMENT Low-dose hydrocortisone replacement in septic shock Only if hemodynamic stability cannot be achieved (weak recommendation) Treatment with IV Igs AGAINST preparations of only IgGs Weak recommendation of IgM-enriched preparations Rhodes A, et al. Crit Care Med 2017; 45: 486
18 THE FRENCH STUDY (JAMA 2002; 288: 862) (START hydrocortisone replacement 3-8 h from onset of hypotension) CORTICUS TRIAL (N Engl J Med 2008; 358: 111 (START hydrocortisone replacement <72 h from onset of hypotension)
19 THE APPROACH OF THE HELLENIC SEPSIS STUDY GROUP (1) (Katsenos C, et al. Crit Care Med 2014; 42: 1651) Late: >9hrs from vasopressors (n= 124) Early: <9hrs from vasopressors (n= 46) log-rank: p: 0.018
20 THE APPROACH OF THE HELLENIC SEPSIS STUDY GROUP (2) (Katsenos C, et al. Crit Care Med 2014; 42: 1651) Late: >9hrs from vasopressors (n= 124) Early: <9hrs from vasopressors (n= 46) log-rank: p:
21 Giamarellos-Bourboulis EJ, et al. Crit Care 2013; 17: R247 SEVERE SEPSIS TO SEPTIC SHOCK: 28-DAY MORTALITY AUC SURVIVORS : mg.day/dl AUC NON-SURVIVORS : mg.day/dl p: 0.037
22 ARE THERE ALARMING Ig LEVELS? IMMUNOSCORING (Bermejo-Martín JF, et al. J Intern Med 2014; 276: 404) IgG1 >300 mg/dl IgM >35 mg/dl IgA >150mg/dl IgG1 300 mg/dl IgM 35 mg/dl IgA 150mg/dl
23 RR: relative risk META-ANALYSIS OF CLINICAL TRIALS (Kreymann KG, et al. Crit Care Med 2007; 35: 2677) IgM-enriched IV polyvalent (IgGAM) (12% IgM, 12% IgA, 76% IgG) RR: % risk for death IgG IV polyvalent RR: % risk for death
24 TOTAL NUMBER OF PATIENTS WITH CLINICAL DATA IN THE REGISTRY= 5,143 Step 1: ICU-ACQUIRED INFECTIONS= 1,299 COMPARATORS (from the same hospitals)= 1,077 Excluded from matching (n=2 neutropenia) IgGAM= 232 (ALL Severe sepsis/shock) Step 2: Severe sepsis/shock= 622 Step 3: MDR Gram-negative= 213 Step 4: Case control matching 1:1 matching for sepsis severity 1:1 matching for appropriateness of empirical antimicrobial treatment Fuzzy matching for source of infection Fuzzy matching for CCI EXCLUDED= 132 Lack of microbiology= 72 Incomplete data= 33 Catheter-related infections= 20 Neutropenia= 4 Gram-positive infections= 2 Primary immunodeficiency= 1 ANALYZED= 100 MDR: multidrug-resistant ANALYZED= 100 Giamarellos-Bourboulis EJ, et al. Clin Microbiol Infect 2016; 22: 499
25 Giamarellos-Bourboulis EJ, et al. Clin Microbiol Infect 2016; 22: 499 MATCHED BASELINE DEMOGRAPHICS Comparators (n= 100) IgGAM (n= 100) Age 54.2 ± ± Severe sepsis/shock 14/86 14/ APACHE II score 20.7 ± ± SOFA score 8.9 ± ± Appropriateness of empirically prescribed antimicrobials 51/49 51/ Primary bacteremia Ventilator-associated pneumonia Ventilator-associated pneumonia + bacteremia Intrabdominal + bacteremia 2 2 Charlson s comorbidity index 2.86 ± ± p
26 PRIMARY ENDPOINT: 28-DAY MORTALITY (Giamarellos-Bourboulis EJ, et al. Clin Microbiol Infect 2016; 22: 499) Mortality= 39% OR death under IgGAM Mortality= 58% 0.37 (95%CIs: ) log-rank: 6.88 p: 0.009
27 SECONDARY ENDPOINT 2: EFFECT ON TIME TO BREAKTHROUGH BACTEREMIA* (Giamarellos-Bourboulis EJ, et al. Clin Microbiol Infect 2016; 22: 499) 50%= 4 days 50%= 10 days log-rank: *A new episode of bloodstream infection in a patient having sterile blood cultures for 72 hours. p<
28 SURVIVING SEPSIS CAMPAIGN 2016 (Rhodes A, et al. Crit Care Med 2017; 45: 486) Addition of a macrolide for patients with septic shock after Streptococcus pneumoniae bacteremia Weak recommendation, low quality of evidence
29 META-ANALYSIS OF 16 OBSERVATIONAL STUDIES (Nie W, et al. J Antimicrob Chemother 2014; 69: 1441)
30 PROSPECTIVE, RANDOMIZED APPROACH (Garin N, et al. JAMA Intern Med 2014; 174: 1894) Community-acquired pneumonia Cefuroxime or amoxycillin/clavulanate Clarithromycin 500mg bid iv or po Monotherapy β-lactam / β-lactam + clarithromycin combination Primary endpoint: patients not reaching clinical stability on day 7 Powered for non-inferiority
31 % of patients BENEFITS OF ADDING CLARITHROMYCIN (Garin N, et al. JAMA Intern Med 2014; 174: 1894) Monotherapy (n= 291) Combination (n= 289) p: % 33.6% p: % 3.1% Instability Day 7 30-day readmission
32 200 patients with VAP + Sepsis/ Severe Sepsis/Septic Shock (ACCP/SCCM 1992) 100 iv PLACEBO + ANTIBIOTICS** 100 iv CLARITHROMYCIN* + ANTIBIOTICS** *1000mg iv daily within one hour x 3 days **Standard of Care VAP: ventilator-associated pneumonia (NCT ) Giamarellos-Bourboulis EJ, et al. Clin Infect Dis 2008; 46; 1157
33 % resolved cases EFFECT ON RESOLUTION OF VAP 80% 60% 40% p: Placebo Clarithromycin 20% 50%: 10 days 50%: 15.5 days 0% Days (NCT ) Giamarellos-Bourboulis EJ, et al. Clin Infect Dis 2008; 46; 1157
34 FINAL OUTCOME!!! (Tsaganos T, et al. Antimicrob Agents Chemother 2016; 60: 3640) 57% log-rank: % MORTALITY DAYS (%) p: p: Placebo Clarithromycin
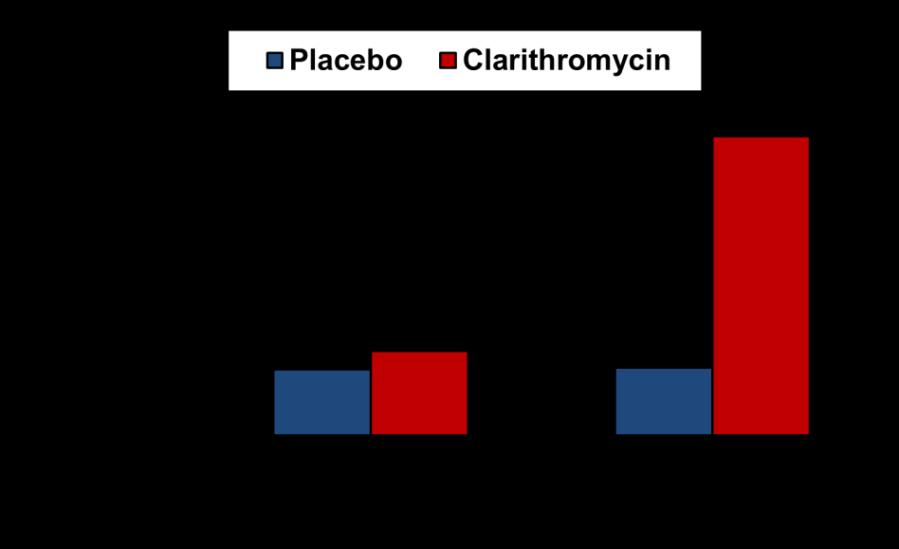

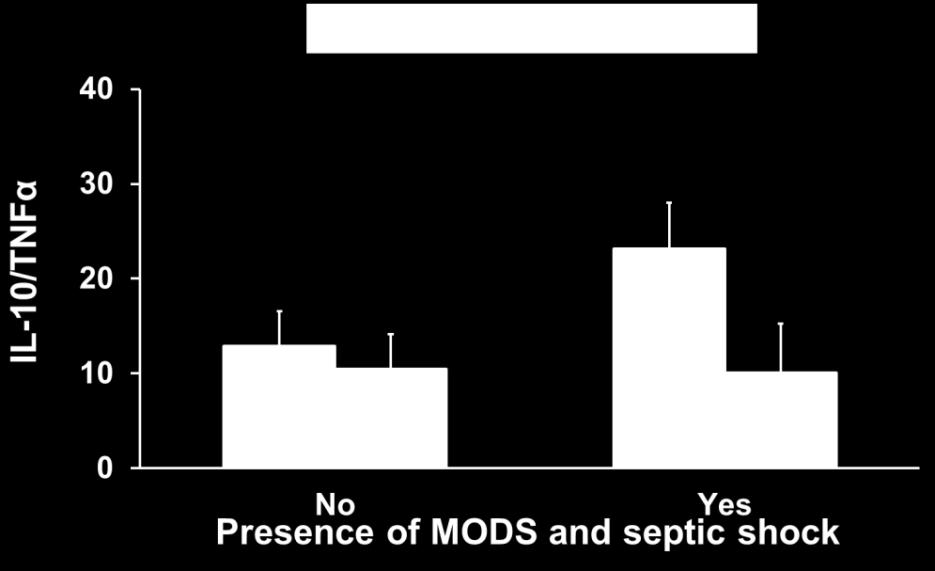
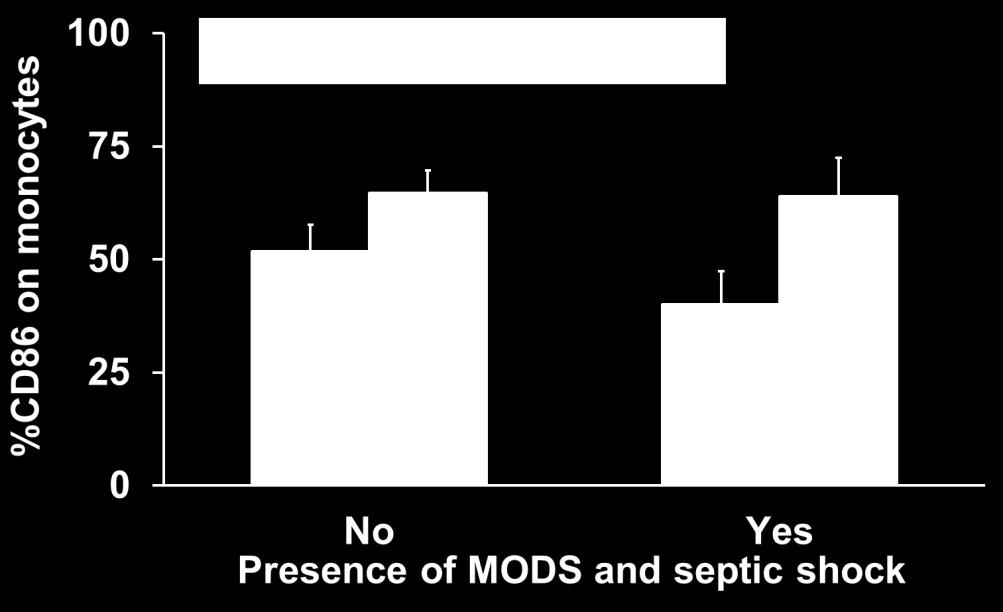
35 REVERSAL OF IMMUNOPARALYSIS (Spyridaki A, et al. Antimicrob Agents Chemother 2012; 56: 3819) p: p: p: 0.024
36 HOW TO DEAL WITH IN 2018? Early broad-spectrum antimicrobials Decision based on epidemiology and SOFA scoring Intense work-up for hemodynamic stability (fluids + vasopressors) Adjunctive approches

37
Educational Workshop
 Educational Workshop EW02: Management of severe sepsis and septic shock anno 2015 Arranged with ESGBIS & International Sepsis Forum (ISF) Convenors: W. Joost Wiersinga, Amsterdam, NL Tom van der Poll,
Educational Workshop EW02: Management of severe sepsis and septic shock anno 2015 Arranged with ESGBIS & International Sepsis Forum (ISF) Convenors: W. Joost Wiersinga, Amsterdam, NL Tom van der Poll,
Evangelos J. Giamarellos-Bourboulis 1, Maria Argyropoulou 1, Theodora Kanni 1, Isabell Kopka 2, Othmar Zenker 2
 EFFICACY AND SAFETY OF IFX-1, AN ANTI-C5A MONOCLONAL ANTIBODY, IN AN OPEN-LABEL, PHASE 2A STUDY IN PATIENTS WITH SEVERE HIDRADENITIS SUPPURATIVA NOT ELIGIBLE FOR ADALIMUMAB Evangelos J. Giamarellos-Bourboulis
EFFICACY AND SAFETY OF IFX-1, AN ANTI-C5A MONOCLONAL ANTIBODY, IN AN OPEN-LABEL, PHASE 2A STUDY IN PATIENTS WITH SEVERE HIDRADENITIS SUPPURATIVA NOT ELIGIBLE FOR ADALIMUMAB Evangelos J. Giamarellos-Bourboulis
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
SEPSIS & SEPTIC SHOCK
 SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions
 Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
JAMA. 2016;315(8): doi: /jama
: doi: /jama") JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
Lessons from recent studies. João Gonçalves Pereira UCIP DALI
 Lessons from recent studies João Gonçalves Pereira UCIP DALI 1 Patterns of Antimicrobial Activity Concentration C max Aminoglycosides Cmax/MIC>10 Metronidazol Area under the concentration curve Azithromycin
Lessons from recent studies João Gonçalves Pereira UCIP DALI 1 Patterns of Antimicrobial Activity Concentration C max Aminoglycosides Cmax/MIC>10 Metronidazol Area under the concentration curve Azithromycin
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
What the ED clinician needs to know about SEPSIS - 3. Anna Morgan Consultant EM Barts Health
 What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Andrea Blotsky MDCM FRCPC General Internal Medicine, McGill University Thursday, October 15, 2015
 The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
A Snapshot of Colistin Use in South-East Europe and Particularly in Greece
 A Snapshot of Colistin Use in South-East Europe and Particularly in Greece Helen Giamarellou 02.05.2013 When Greek Physicians Prescribe Colistin? It is mainly prescribed in the ICU for VAP, bacteremia
A Snapshot of Colistin Use in South-East Europe and Particularly in Greece Helen Giamarellou 02.05.2013 When Greek Physicians Prescribe Colistin? It is mainly prescribed in the ICU for VAP, bacteremia
MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES
 MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES 1 Marin H. Kollef, MD Professor of Medicine Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Washington University School of
MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES 1 Marin H. Kollef, MD Professor of Medicine Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Washington University School of
Is nosocomial infection the major cause of death in sepsis?
 Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
Sepsi: nuove definizioni, approccio diagnostico e terapia
 GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Advancements in Sepsis
 Objectives Advancements in Sepsis Brian Gilbert, PharmD PGY-1 Pharmacy Resident Jackson Memorial Hospital 3/13/2016 www.fshp.org Pharmacist objectives Review recent updates in resuscitation strategies
Objectives Advancements in Sepsis Brian Gilbert, PharmD PGY-1 Pharmacy Resident Jackson Memorial Hospital 3/13/2016 www.fshp.org Pharmacist objectives Review recent updates in resuscitation strategies
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
SEPSIS-3: THE NEW DEFINITIONS
 SEPSIS-3: THE NEW DEFINITIONS WHAT THEY SHOULD MEAN TO YOU MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK https://www.youtube.com/watch?v=1s8l5d2xr6w IN THE
SEPSIS-3: THE NEW DEFINITIONS WHAT THEY SHOULD MEAN TO YOU MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK https://www.youtube.com/watch?v=1s8l5d2xr6w IN THE
Sepsis-3: clarity or confusion
 Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Augmented Renal Clearance: Let s Get the Discussion Flowing
 Augmented Renal Clearance: Let s Get the Discussion Flowing Terry Makhoul, PharmD PGY-2 Emergency Medicine Pharmacy Resident University of Rochester Medical Center Strong Memorial Hospital Disclosures
Augmented Renal Clearance: Let s Get the Discussion Flowing Terry Makhoul, PharmD PGY-2 Emergency Medicine Pharmacy Resident University of Rochester Medical Center Strong Memorial Hospital Disclosures
Guess or get it right?
 Guess or get it right? Antimicrobial prescribing in the 21 st century Robert Masterton Traditional Treatment Paradigm Conservative start with workhorse antibiotics Reserve more potent drugs for non-responders
Guess or get it right? Antimicrobial prescribing in the 21 st century Robert Masterton Traditional Treatment Paradigm Conservative start with workhorse antibiotics Reserve more potent drugs for non-responders
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Sepsis and Septic Shock: New Definitions for Adults
 PL Detail-Document #320424 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER April 2016 Sepsis and Septic
PL Detail-Document #320424 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER April 2016 Sepsis and Septic
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
6-horas 24 horas Coleta de lactato Hemoculturas. Corticosteróides. Controle glicêmico. Fluidos/vasopressores. Otimização de SvO 2
 Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Superhero or Superzero? Vancomycin vs. Linezolid for MRSA Pneumonia
 Superhero or Superzero? Vancomycin vs. Linezolid for MRSA Pneumonia Brandon Dionne, PharmD, BCPS, AAHIVP Assistant Clinical Professor Northeastern University Seth Housman, PharmD, MPA Clinical Assistant
Superhero or Superzero? Vancomycin vs. Linezolid for MRSA Pneumonia Brandon Dionne, PharmD, BCPS, AAHIVP Assistant Clinical Professor Northeastern University Seth Housman, PharmD, MPA Clinical Assistant
Potenzialità Terapeutiche delle Immunoglobuline
 Potenzialità Terapeutiche delle Immunoglobuline AGENDA # Guidelines and Evidences # Ig and Pathobiology of Sepsis # Ideas and Data slides and discussion girardis.massimo@unimo.it Disclosures POTENTIAL
Potenzialità Terapeutiche delle Immunoglobuline AGENDA # Guidelines and Evidences # Ig and Pathobiology of Sepsis # Ideas and Data slides and discussion girardis.massimo@unimo.it Disclosures POTENTIAL
Presented at the annual meeting of the American Society of Microbiology, June 1-5, 2017, New Orleans, LA, USA
 Is Associated With Improved Survival and Safety Compared to Colistin in Serious Carbapenemresistant Enterobacteriaceae (CRE) Infections: Results of the CARE Study Lynn E. Connolly 1, Adrian M. Jubb 1,
Is Associated With Improved Survival and Safety Compared to Colistin in Serious Carbapenemresistant Enterobacteriaceae (CRE) Infections: Results of the CARE Study Lynn E. Connolly 1, Adrian M. Jubb 1,
Is the package insert correct? PK considerations
 Is the package insert correct? PK considerations Jason A Roberts B Pharm (Hons), PhD, FSHP Professor of Medicine and Pharmacy The University of Queensland, Australia Royal Brisbane and Women s Hospital,
Is the package insert correct? PK considerations Jason A Roberts B Pharm (Hons), PhD, FSHP Professor of Medicine and Pharmacy The University of Queensland, Australia Royal Brisbane and Women s Hospital,
Infections In Cirrhotic patients. Dr Abid Suddle Institute of Liver Studies King s College Hospital
 Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of
 Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Anti-inflammatory and immunomodulatory strategies in VAP - Lessons from adult Intensive Care
 Anti-inflammatory and immunomodulatory strategies in VAP - Lessons from adult Intensive Care Charles Feldman Professor of Pulmonology Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand
Anti-inflammatory and immunomodulatory strategies in VAP - Lessons from adult Intensive Care Charles Feldman Professor of Pulmonology Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Steroid in Paediatric Sepsis. Dr Pon Kah Min Hospital Pulau Pinang
 Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Sepsis 3.0: The Impact on Quality Improvement Programs
 Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Guidelines are the Future of Sepsis Management Pro
 Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Vasopressors in Septic Shock. Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada
 Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX
 Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Pharmacologyonline 1: (2010) ewsletter Singh and Kochbar. Optimizing Pharmacokinetic/Pharmacodynamics Principles & Role of
 ewsletter Singh and Kochbar. Optimizing Pharmacokinetic/Pharmacodynamics Principles & Role of") Optimizing Pharmacokinetic/Pharmacodynamics Principles & Role of Cefoperazone Sulbactam Singh M*, Kochhar P* Medical & Research Division, Pfizer India. Summary Antimicrobial resistance is associated with
Optimizing Pharmacokinetic/Pharmacodynamics Principles & Role of Cefoperazone Sulbactam Singh M*, Kochhar P* Medical & Research Division, Pfizer India. Summary Antimicrobial resistance is associated with
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Sepsis: What Is It Really?
 Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Updates in Emergency Department Management of Sepsis
 Resident Journal Review Updates in Emergency Department Management of Sepsis Authors: Eli Brown, MD; Allison Regan, MD; Kaycie Corburn, MD; Jacqueline Shibata, MD Edited by: Jay Khadpe, MD FAAEM; Michael
Resident Journal Review Updates in Emergency Department Management of Sepsis Authors: Eli Brown, MD; Allison Regan, MD; Kaycie Corburn, MD; Jacqueline Shibata, MD Edited by: Jay Khadpe, MD FAAEM; Michael
3 papers from ED. counting sepsis sepsis 3 wet or dry?
 3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Effectively Managing Sepsis Denials
 Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
ESCMID Online Lecture Library. by author
 Novel PK/PD data on the optimisation of colistin and the carbapenems Diamantis Plachouras Athens, Greece Hot Topics on Infections in the Critically Ill Patient, ESCMID Postgraduate Education Course, 31
Novel PK/PD data on the optimisation of colistin and the carbapenems Diamantis Plachouras Athens, Greece Hot Topics on Infections in the Critically Ill Patient, ESCMID Postgraduate Education Course, 31
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Optimizing Antibiotic Therapy in the ICU For Pneumonia Current and Future Approaches
 Optimizing Antibiotic Therapy in the ICU For Pneumonia Current and Future Approaches Andrew F. Shorr, MD, MPH Washington Hospital Center Georgetown Univ. Disclosures I have served as a consultant to, researcher/investigator
Optimizing Antibiotic Therapy in the ICU For Pneumonia Current and Future Approaches Andrew F. Shorr, MD, MPH Washington Hospital Center Georgetown Univ. Disclosures I have served as a consultant to, researcher/investigator
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Objectives. Pathophysiology of Steroids. Question 1. Pathophysiology 3/1/2010. Steroids in Septic Shock: An Update
 Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
A BRIEF HISTORY OF SEPSIS. Euan Mackay
 A BRIEF HISTORY OF SEPSIS Euan Mackay Aims History of sepsis definition Validity of new definition Hippocrates 4 th century BC Hippocrates introduced the term "σήψις the process of decay or decomposition
A BRIEF HISTORY OF SEPSIS Euan Mackay Aims History of sepsis definition Validity of new definition Hippocrates 4 th century BC Hippocrates introduced the term "σήψις the process of decay or decomposition
Early lactate clearance rate is an indicator of Outcome in severe sepsis and septic shock
 Early lactate clearance rate is an indicator of Outcome in severe sepsis and septic shock Sultana R, Ahsan ASMA, Fatema K, Ahmed F, Hamid T, Saha DK, Saha M, Nazneen S, Dr. Rozina Sultana FCPS (Medicine)
Early lactate clearance rate is an indicator of Outcome in severe sepsis and septic shock Sultana R, Ahsan ASMA, Fatema K, Ahmed F, Hamid T, Saha DK, Saha M, Nazneen S, Dr. Rozina Sultana FCPS (Medicine)
CLINICAL USE OF GLYCOPEPTIDES. Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel
 CLINICAL USE OF GLYCOPEPTIDES Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel Glycopeptides Natural Vancomycin introduced in 1958 Teicoplanin introduced in Europe
CLINICAL USE OF GLYCOPEPTIDES Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel Glycopeptides Natural Vancomycin introduced in 1958 Teicoplanin introduced in Europe
Supplementary Online Content
 Supplementary Online Content Uranga A, España, Bilbao A, et al. Duration of antibiotic treatment in communityacquired pneumonia: a multicenter randomized clinical trial. JAMA Intern Med. ublished online
Supplementary Online Content Uranga A, España, Bilbao A, et al. Duration of antibiotic treatment in communityacquired pneumonia: a multicenter randomized clinical trial. JAMA Intern Med. ublished online
Sepsis. Reliability- can we achieve Dr Ron Daniels
 Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Impact of timely antibiotic administration on outcomes in patients with severe sepsis and septic shock in the emergency department
 Clin Exp Emerg Med 2014;1(1):35-40 http://dx.doi.org/10.15441/ceem.14.012 Impact of timely antibiotic administration on outcomes in patients with severe sepsis and septic shock in the emergency department
Clin Exp Emerg Med 2014;1(1):35-40 http://dx.doi.org/10.15441/ceem.14.012 Impact of timely antibiotic administration on outcomes in patients with severe sepsis and septic shock in the emergency department
Basics from anatomy and physiology classes Local tissue reactions
 Septicaemia & SIRS Septicaemia is a life-threatening condition that arises when the physical reaction to an infection, causes damage to tissue and organs Basics from anatomy and physiology classes Local
Septicaemia & SIRS Septicaemia is a life-threatening condition that arises when the physical reaction to an infection, causes damage to tissue and organs Basics from anatomy and physiology classes Local
PHARMACOKINETIC & PHARMACODYNAMIC OF ANTIBIOTICS
 PHARMACOKINETIC & PHARMACODYNAMIC OF ANTIBIOTICS SITI HIR HURAIZAH MD TAHIR Bpharm (UKM), MSc (Clinical Microbiology) (UoN) CLINICAL PHARMACIST HOSPITAL MELAKA WHY STUDY PHARMACOKINETICS (PK) AND PHARMACODYNAMICS
PHARMACOKINETIC & PHARMACODYNAMIC OF ANTIBIOTICS SITI HIR HURAIZAH MD TAHIR Bpharm (UKM), MSc (Clinical Microbiology) (UoN) CLINICAL PHARMACIST HOSPITAL MELAKA WHY STUDY PHARMACOKINETICS (PK) AND PHARMACODYNAMICS
Continuous vs Intermittent Dosing of Antibiotics in Critically-Ill Patients
 Continuous vs Intermittent Dosing of Antibiotics in Critically-Ill Patients Jan O Friedrich, MD DPhil Associate Professor of Medicine, University of Toronto Medical Director, MSICU St. Michael s Hospital,
Continuous vs Intermittent Dosing of Antibiotics in Critically-Ill Patients Jan O Friedrich, MD DPhil Associate Professor of Medicine, University of Toronto Medical Director, MSICU St. Michael s Hospital,
HAP/VAP care bundle interventions - a UK approach. Dr R G Masterton NHS Ayrshire & Arran
 HAP/VAP care bundle interventions - a UK approach Dr R G Masterton NHS Ayrshire & Arran How Hazardous Is Health Care? (Leape and Amalberti) Total lives lost per year 100,000 10,000 1,000 100 10 1 HAZARDOUS
HAP/VAP care bundle interventions - a UK approach Dr R G Masterton NHS Ayrshire & Arran How Hazardous Is Health Care? (Leape and Amalberti) Total lives lost per year 100,000 10,000 1,000 100 10 1 HAZARDOUS
The Use of Metabolic Resuscitation in Sepsis
 The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
without the permission of the author Not to be copied and distributed to others
 Emperor s Castle interior-prato What is the Role of Inhaled Polymyxins for Treatment of Respiratory Tract Infections? Helen Giamarellou CONCLUSIONS: Patients with Pseudomonas and Acinetobacter VAP may
Emperor s Castle interior-prato What is the Role of Inhaled Polymyxins for Treatment of Respiratory Tract Infections? Helen Giamarellou CONCLUSIONS: Patients with Pseudomonas and Acinetobacter VAP may