Evidence-Based. Management of Severe Sepsis. What is the BP Target?
|
|
|
- Noel Booker
- 5 years ago
- Views:
Transcription
1 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco USA Management of Severe Sepsis Resuscitation Endpoints Early Goal Directed Therapy Use of Activated Protein C Replacement Dose Steroids Putting it all together What is the BP Target? BP targets are arbitrary Autoregulation is lost below MAP mmhg What is the data that we should target a MAP of 65 mmhg? 1

2 What is the BP Target? BP targets are arbitrary Autoregulation is lost below MAP mmhg What is the data that we should target a MAP of 65 mmhg? Crit Care Med 2005; 33: How Much BP is Enough? Blood Lactate (meq/l) Oxygen Consumption (ml/min/m 2 ) Oxygen Delivery (ml/min/m 2 ) Oxygen Extraction Ratio (%) 2

3 How Much BP is Enough? Urine Output (ml/h) Creatinine Clearance (ml/min) Crit Care Med 2005; 33: DOPAMINE Best Pressor: Dopamine? No evidence of increased renal perfusion at low doses Tachycardia more common than with norepinephrine May impair splanchnic blood flow Stimulates vasopressin secretion Does not confer clinically significant protection against renal dysfunction 3

4 Multicenter European observational study 198 European ICU s All patients admitted over 2 week period in 2002 Sakr et al, CCM 2006 Sakr et al, CCM 2006 Dopamine Dobutamine Epinephrine Norepinephrine Sakr et al, CCM
5 Best Pressor: Norepinephrine? No evidence of worsening renal function Less tachycardia than dopamine More rapid and effective BP control May increase splanchnic perfusion Best Pressor: Norepinephrine? Effect of norepinephrine compared with high dose dopamine and/or epinephrine on the outcome of septic shock Prospective, observational cohort N=97 Norepinephrine mortality 62% vs 82% P<0.001 RR= % CI, Martin et al, CCM 2000 Best Pressor: Epinephrine? 30 adult patients with septic shock MAP 60 mm Hg Norepinephrine and dobutamine vs epinephrine to MAP >80 mm Hg Results Similar effect on hemodynamics Epinephrine Lactate Lactate/pyruvate ratio Gastric phi Levy et al, Intens Care Med,

6 Best Pressor: Phenylephrine? 13 patients with septic shock Treated with fluids and either low-dose dopamine or dobutamine, but remained hypotensive Phenylephrine added 0.5 to 9 μg/kg/min MAP >70 mm Hg Results Increased MAP, SVR, CI, stroke index, DO 2, VO 2 and urine output No change in HR Dose 3.7 ( ) μg/kg/min Mean duration 65 hours Gregory et al, CCM, 1991 Vasopressin mechanism of action 6


7 Vasopressin in Shock Luckner et al, CCM Prospective trial in 316 patients Vasopressin infusion at 4 units/hour Measured hemodynamics, lab parameters Adverse Effects of Vasopressin Luckner et al, CCM Pressor Dose vs Mortality Luckner et al, CCM

8 Watch for side effects! VASST Trial 779 patients in septic shock requiring vasopressors for at least 6 hours and having at least 1 additional dysfunctional organ system randomized to receive AVP or norepinephrine No difference in 28-day survival between groups (35.4% vs 39.3%, P =.27). Stratified according to severity of hypotension (requiring > 15 mcg/min or < 15 mcg/min of NE at enrollment), and the patients taking lower-dose NE had improved survival with AVP (26.5% vs 35.7%, P =.05). Digital ischemia was somewhat more common in the AVP group (P =.06), while cardiac arrest was slightly more common in the NE group (P =.11). Oxygen Delivery and Consumption 8


9 Shah et al, JAMA Shah et al, JAMA


10 PAC-Man Results Venous Oximetry Measurement of the balance between systemic oxygen delivery and consumption Proven in one study (Rivers) to improve outcome 10

11 Venous oxygen saturation varies in different vascular beds Sampling needs to be well mixed: PA Oximetry Slow sampling SvO 2 vs ScvO 2 Studies are in disagreement about accuracy of ScvO 2 Most agree that the trend is accurate Early Goal Directed Therapy Hypothesis: Early in sepsis, there is inadequate oxygen delivery, manifested by low mixed-venous oxygen saturation. Early resuscitation can save these cells and prevent multi-system organ failure. 11

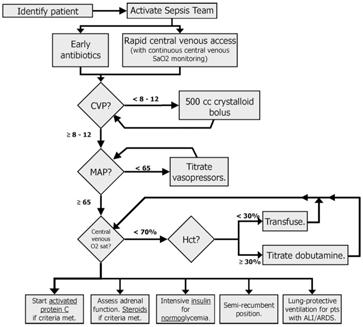
12 Randomized, prospective trial of early, goal-directed resuscitation of patients with severe sepsis Patients randomized to 6 hours of goal-directed therapy vs standard therapy 260 patients randomized In-hospital mortality was 30.5% with goal-directed therapy vs 46.5% with standard therapy Rivers et al, NEJM, 2001;345: Supplemental oxygen + endotracheal intubation and mechanical ventilation CVP < 8 mmhg Crystalloid Central venous and arterial catheterization 8-12 mmhg Colloid MAP < 65 mmhg >90 mmhg Vasoactive agents Sedation, paralysis (if intubated), or both >65 and <90 mmhg ScvO 2 <70% Transfusion of red cells Until hematocrit > 30% >70% Hospital admission Yes No >70% Goals Achieved Inotropic agents <70% Rivers et al, NEJM, 2001;345: Evidence: The Importance of Early Goal Directed Therapy Early goal-directed therapy in patients with severe sepsis produced: 42% in relative risk of in-hospital and 28-day mortality (P=0.009, =0.01) 33% in relative risk of death at 60 days (P=0.03) NNT to prevent 1 event (death) = 6 to Standard Therapy Early goal-directed therapy In-hospital mortality (all patients) 28-day mortality 60-day mortality Rivers E, et al. N Engl J Med 2001;345:
13 Maybe it was the volume Orthogonal Polarization Spectral Imaging Sakr et al, CCM,

14 Pathophysiology of Sepsis Coagulation fibrinolysis Endothelial injury inflammation Organ failure Phase III Trial of Drotrecogin Alfa (Activated): PROWESS PROWESS study group Randomized, double blind, placebo controlled trial 1690 Patients with sepsis were given infusion of activated PC or placebo for 96 hours Primary end point was death by 28 days Also monitored complications and coagulation activation PROWESS: Bleeding Events 14




15 Mortality Reduction in PROWESS Hospital Mortality by Subgroup 15
 n (%) 75 (5.7) 182 (13.8) 31 (2.4) 51 (3.9) 46 (3.5) 143 (10.9) 4 (0.3) 6 (0.5) Treatment Group Placebo (N=1293) n (%) 78 (6.0) 183 (14.2) 15 (1.")
16 ADDRESS Trial Parameter ADDRESS: Serious Adverse Events Serious adverse event rate: Days days Serious bleeding event rate: Days days Serious non-bleeding event rate: Days days CNS bleeding events: Days days DrotAA (N=1317) n (%) 75 (5.7) 182 (13.8) 31 (2.4) 51 (3.9) 46 (3.5) 143 (10.9) 4 (0.3) 6 (0.5) Treatment Group Placebo (N=1293) n (%) 78 (6.0) 183 (14.2) 15 (1.2) 28 (2.2) 66 (5.1) 168 (13.0) 3 (0.2) 5 (0.4) P-value Observational cohort study of 312 pts with estimated ICU LOS>48hrs Measured plasma protein C and measures of organ dysfunction Brunkhorst et al, Anesthesiology,
17 Protein C and Outcomes Brunkhorst et al, Anesthesiology, Protein C and Outcomes Brunkhorst et al, Anesthesiology, Protein C and Outcomes Brunkhorst et al, Anesthesiology,

18 Hypothesis: Patients with septic shock have functional adrenal insufficiency, which contributes to their hypotension and subsequent multi-organ failure. Low dose steroids in septic shock Onset of shock Time 0 Eligibility and ACTH test Randomization At 8 hours Hydrocortisone IV 50 mg QID + Fludrocortisone 50 mcg/d for 7 d Placebo for 7 days 18
19 Low Dose Steroid Treatment in Septic Shock: 28 Day Mortality All Patients 28-day Mortality 100% 80% 60% 40% 20% 0% P= % 55% N=150 N=149 Low-dose Steroids Placebo Annane, D. JAMA, 2002; 288 (7): 868. Low Dose Steroid Treatment in Septic Shock: 28 Day Mortality (Non-responders vs. Responders) 100% Patients with Relative Adrenal Insuffiency (ACTH Test Nonresponders) (77%) 100% Patients Without Relative Adrenal Insufficiency (ACTH Test Responders) (23%) 28-day Mortality 80% 60% 40% P=0.04 P= % 63% 61% 60% 53% 53% 40% N=114 N=115 N=36 N=34 20% 20% 0% 0% Low-dose Steroids Placebo Annane, D. JAMA, 2002; 288 (7): 868. CORTICUS STUDY 19
20 Low Dose Steroid Treatment in Septic Shock : CORTICUS Study Design Objective: To assess whether low doses of corticosteroids improve 28-day survival in patients with septic shock and relative adrenal insufficiency. Primary Objective: 28-day mortality in non-responders to ACTH stimulation test Design: Placebo-controlled, randomized, double-blind, multinational European study. Setting: 52 intensive care units in multiple European countries from March 2002 to November Entry criteria similar (less sick) to Annane. Low Dose Steroid Treatment in Septic Shock : Study Design Onset of shock Randomization Eligibility and ACTH test Hydrocortisone IV 50-mg every 6 hours x 5 days Hydrocortisone IV 50-mg every 12 hours x 3 days Hydrocortisone IV 50-mg every 24 hours x 3 days Placebo X 11 days Main Outcome: 28-day survival Low Dose Steroid Treatment in Septic Shock: 28 Day Mortality All Patients 100% P= day Mortality 80% 60% 40% 20% 34% N=251 31% N=248 0% Low-dose Steroids Placebo Sprung, ESICM September
 28-day Mortality 100% 80% 60% 40% 20% Patients with Relative Adrenal Insuffiency (ACTH Test Nonresponders) (~51%) 38%")

21 Low Dose Steroid Treatment in Septic Shock: 28 Day Mortality (Non-responders vs. Responders) 28-day Mortality 100% 80% 60% 40% 20% Patients with Relative Adrenal Insuffiency (ACTH Test Nonresponders) (~51%) 38% P=0.8 35% 100% 80% 60% 40% 20% Patients Without Relative Adrenal Insufficiency (ACTH Test Responders) (~47%) P=1.0 29% 29% 0% Low-dose Steroids 0% Placebo Sprung, ESICM September 2006 Retrospective multicenter study 477 patients with severe sepsis, shock All had ACTH stimulation testing Corticus Cohort Study CCM

22 Corticus Cohort Study CCM 2007 Predictors of Mortality Sepsis Bundle Implementation Kortgen et al, CCM Retrospective cohort study 30 consecutive patients meeting criteria for severe sepsis after implementation of a standard operating procedure Historical control 22

23 Interventions Early goal directed therapy Intensive insulin therapy Hydrocortisone supplementation If shock progressed Administration of rhapc Kortgen et al, CCM Results Kortgen et al, CCM


24 Survival: 30 Pts each group 24
25 25


26 Conclusions Develop standard guidelines for sepsis treatment If pressors necessary, use norepinephrine EGDT is likely effective in reducing mortality Future resuscitation monitoring may use technology such as OPS Consider APC for patients with refractory septic shock Low dose steroids do not improve outcome in patients with septic shock 26
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Sepsis: Update on Diagnosis, Evaluation and Management
 Sepsis: Epidemiology Sepsis: Update on Diagnosis, Evaluation and Management Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per
Sepsis: Epidemiology Sepsis: Update on Diagnosis, Evaluation and Management Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Vasopressors in Septic Shock. Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada
 Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Vasopressors for shock
 Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
What works in sepsis. Topics. EGDT: Severe Sepsis/ Shock. Sepsis
 What works in sepsis Eric Schmidt, MD Denver Health Medical Center University of Colorado School of Medicine Topics Understanding and implemen@ng early goal directed therapy (EGDT) Ac@vated Protein C should
What works in sepsis Eric Schmidt, MD Denver Health Medical Center University of Colorado School of Medicine Topics Understanding and implemen@ng early goal directed therapy (EGDT) Ac@vated Protein C should
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
Sepsis New Management Strategies
 Sepsis: Epidemiology Sepsis 2013- New Management Strategies Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per year ~200,000 deaths
Sepsis: Epidemiology Sepsis 2013- New Management Strategies Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per year ~200,000 deaths
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Billion
 Surviving : Are we? The 7th National Emergency Medicine Congress Antalya, Turkey Alexander L. Eastman, MD, MPH Department of Surgery UTSW Severe : A Significant Healthcare Challenge Major cause of morbidity
Surviving : Are we? The 7th National Emergency Medicine Congress Antalya, Turkey Alexander L. Eastman, MD, MPH Department of Surgery UTSW Severe : A Significant Healthcare Challenge Major cause of morbidity
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Endpoints of Resuscitation for Circulatory Shock: When Enough is Enough?
 Endpoints of Resuscitation for Circulatory Shock: When Enough is Enough? Emanuel P. Rivers, MD, MPH, IOM Vice Chairman and Research Director Departments of Emergency Medicine and Surgery Henry Ford Hospital
Endpoints of Resuscitation for Circulatory Shock: When Enough is Enough? Emanuel P. Rivers, MD, MPH, IOM Vice Chairman and Research Director Departments of Emergency Medicine and Surgery Henry Ford Hospital
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Actualités de la prise en charge hémodynamique initiale Daniel De Backer
 Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
SEPSIS 2015 DISCLOSURES FINANCIAL DISCLOSURES 9/1/2015. William M. Johnson, MD Nebraska Pulmonary Specialties. William Johnson
 SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
Goal-directed resuscitation in sepsis; a case-based approach
 Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
UTILITY of ScvO 2 and LACTATE
 UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX
 Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Looking for sepsis. Sepsis: Update. Prevalence of High Profile Dzs. Screening and risk stratification. Mortality of High Profile Diseases
 Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Full Disclosure. The case for why it matters. Goal-directed Fluid Resuscitation
 Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Obligatory joke. The case for why it matters. Sepsis: More is more. Goal-Directed Fluid Resuscitation 6/1/2013
 Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Inflammation. Sepsis Ladder
 Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing Pathophysiology of sepsis and septic shock How sepsis affects the endocrine system Pathophysiology of adrenal insufficiency Clinical manifestations
Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing Pathophysiology of sepsis and septic shock How sepsis affects the endocrine system Pathophysiology of adrenal insufficiency Clinical manifestations
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Subclinical Problems in the ICU:
 Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Sepsis Combine experience and Evidence. Eran Segal, MD Director General ICU, Sheba Medical Center, Israel
 Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Steroid in Paediatric Sepsis. Dr Pon Kah Min Hospital Pulau Pinang
 Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Management of Severe Sepsis:
 Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Epidemiology of Severe Sepsis
 Dellinger et al Crit Care Med 2008 Surviving Sepsis Phase I: the Barcelona Declaration Phase II: development and publication of guidelines 2004, updated in 2008 Phase III: operationalize the guidelines,
Dellinger et al Crit Care Med 2008 Surviving Sepsis Phase I: the Barcelona Declaration Phase II: development and publication of guidelines 2004, updated in 2008 Phase III: operationalize the guidelines,
The Use of Metabolic Resuscitation in Sepsis
 The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
Should we use steroids in sepsis? J.G. van der Hoeven
 Should we use steroids in sepsis? J.G. van der Hoeven Why I don t like it It is boring.. It usually results in emotional outcries in the audience If any, the effects on outcome are very small You are not
Should we use steroids in sepsis? J.G. van der Hoeven Why I don t like it It is boring.. It usually results in emotional outcries in the audience If any, the effects on outcome are very small You are not
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Objectives. Pathophysiology of Steroids. Question 1. Pathophysiology 3/1/2010. Steroids in Septic Shock: An Update
 Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
F. BLOOS, K. REINHART Dep. of Anaesthesiology and Intensive Care Medicine, Klinikum der Friedrich-Schiller-Universität Jena, Jena, Germany
 European Society of Anaesthesiologists Refresher Course MANAGEMENT OF SEPSIS 12 RC 5 F. BLOOS, K. REINHART Dep. of Anaesthesiology and Intensive Care Medicine, Klinikum der Friedrich-Schiller-Universität
European Society of Anaesthesiologists Refresher Course MANAGEMENT OF SEPSIS 12 RC 5 F. BLOOS, K. REINHART Dep. of Anaesthesiology and Intensive Care Medicine, Klinikum der Friedrich-Schiller-Universität
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
How can the PiCCO improve protocolized care?
 How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
Objectives. Outline. Sepsis Incidence and Outcomes. Definitions
 Objectives Evaluate recent literature on the management of sepsis Apply new and potentially controversial recommendations from the Surviving Sepsis Guidelines to patient cases. Surviving Sepsis Campaign
Objectives Evaluate recent literature on the management of sepsis Apply new and potentially controversial recommendations from the Surviving Sepsis Guidelines to patient cases. Surviving Sepsis Campaign
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Top Sepsis Studies
 A75M233/A75M529 Monday 08:00-09:15 Wednesday 14:45-16:00 Maureen A Seckel APRN, ACNS-BC, CCRN, CCNS, FCCM Critical Care CNS and Sepsis Leader Christiana Care Health Services, Newark, DE Top Sepsis Studies
A75M233/A75M529 Monday 08:00-09:15 Wednesday 14:45-16:00 Maureen A Seckel APRN, ACNS-BC, CCRN, CCNS, FCCM Critical Care CNS and Sepsis Leader Christiana Care Health Services, Newark, DE Top Sepsis Studies
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Sepsis Learning Collaborative: Sepsis New Definitions
 Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Endocrine and Metabolic Complications in the ICU
 Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
4/4/2014. Of patients diagnosed with sepsis 50% will develop severe sepsis 25% will develop shock. SIRS Sepsis Severe Septic Sepsis Shock.
 A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
VOLUME RESPONSIVENESS IS DIFFERENT FROM NEED FOR FLUIDS BLOOD PRESSURE TARGETS IN SEPSIS
 Department of Intensive Care Medicine VOLUME RESPONSIVENESS IS DIFFERENT FROM NEED FOR FLUIDS BLOOD PRESSURE TARGETS IN SEPSIS SEPTIC SHOCK : THE CLINICAL SCENARIO HYPOTENSION DESPITE ADEQUATE VOLUME RESUSCITATION
Department of Intensive Care Medicine VOLUME RESPONSIVENESS IS DIFFERENT FROM NEED FOR FLUIDS BLOOD PRESSURE TARGETS IN SEPSIS SEPTIC SHOCK : THE CLINICAL SCENARIO HYPOTENSION DESPITE ADEQUATE VOLUME RESUSCITATION
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Dr. İsa KILIÇASLAN Gazi University School of Medicine
 Dr. İsa KILIÇASLAN Gazi University School of Medicine ystemic Inflammatory Response Syndrome (SIRS) Temp > 38.3 C or < 36 C HR > 90/min RR > 20 or PaCO2 < 32 WBC > 12 or < 4 or Bands > 10% TWO out of four
Dr. İsa KILIÇASLAN Gazi University School of Medicine ystemic Inflammatory Response Syndrome (SIRS) Temp > 38.3 C or < 36 C HR > 90/min RR > 20 or PaCO2 < 32 WBC > 12 or < 4 or Bands > 10% TWO out of four