Breast Cancer Staging. Physiology Trumps Anatomy Author: Maxine Jochelson, MD, FSBI
|
|
|
- Duane Young
- 5 years ago
- Views:
Transcription
1 Breast Cancer Staging. Physiology Trumps Anatomy Author: Maxine Jochelson, MD, FSBI The purpose of this paper is to address the importance of physiologic imaging for the staging and follow up of patients with breast cancer according to the principles of precision medicine. Precision medicine is the tailoring of medical treatment to the individual characteristics, needs and preferences of a patient during all stages of care, including prevention, diagnosis, treatment and follow-up. Currently, physiologic imaging is primarily performed with 18F FDG- PET/CT, but other tracers are increasingly being used towards the goal of more specific tumor targeting. Staging Once breast cancer is diagnosed, staging of the axilla must be performed. However, at present, imaging of the clinically negative axilla is not accurate enough to obviate histologic sampling, which is most frequently performed with sentinel lymph node biopsy. Houssami et al. reported in a meta-analysis of 31 studies that axillary ultrasound had a sensitivity of only 61.4% 1. PET/CT provides similar limited sensitivity in the general breast cancer population 2 ; however, in patients with larger primary tumors who may undergo neoadjuvant chemotherapy, sensitivity is 82% for the detection of regional lymphadenopathy reflecting a higher likelihood of nodal metastases in women with larger cancers 3. Based on these data Koolet et al recommend that all patients who will be undergoing neoadjuvant chemotherapy have an FDG PET/CT scan for locoregional staging. Current National Comprehensive Cancer Network (NCCN) guidelines recommend against routine staging of women with Stage I or II disease and primarily recommend CT or MRI in addition to a bone scan for staging women with Stage III or IV breast cancer with the following caveat: The use of FDG PET/CT should generally be discouraged for the evaluation of metastatic disease except in those clinical situations where other staging studies are equivocal or suspicious. Even in those situations biopsy may be more useful. However, there are
2 multiple studies all demonstrating more accurate breast cancer staging with FDG PET/CT as will be briefly described below. In breast cancer detection, it is already well established that physiologic imaging of the breast (with breast MRI, Positron Emission Mammography, Molecular Breast Imaging, and Contrast Enhanced Mammography) has a higher sensitivity than purely anatomic modalities (including Full Field Digital Mammography, Digital Breast Tomosynthesis, and ultrasound). Groheux et al. evaluated 254 women with Stage IIA through IIIC breast cancer and found that FDG PET/CT imaging changed the clinical stage in 30% of the women. Most strikingly, 21% of those women had unsuspected metastatic disease, with an upgrade rate of 10.7% in women with Stage IIB disease 4. In a retrospective study of breast cancer patients younger than 40 years of age, Riedl et al. demonstrated a 17% upstaging rate in women with IIB disease 5. Every study comparing FDG PET/CT to standard imaging with CT and bone scan has demonstrated the superiority of PET/CT with accuracies of 86-90% 6,7. Constantinidou et al. 8 compared FDG PET/CT to CT and bone scan and showed more disease in over 30% of patients. Although the finding of additional metastases when a patient clearly has extensive metastatic disease may not always be clinically relevant, there are times when PET/CT detects a single metastases when all other exams are negative changing treatment and prognosis. It should be stressed that in these cases biopsy confirmation is required when possible to avoid overtreatment of a false positive PET/CT finding. Figure 1 shows PET/CT imaging of a 35-year-old Asian woman presenting with Stage IIB breast cancer who was waiting for the results of BRCA testing to determine if she were to have bilateral mastectomy and

.")
3 reconstruction. PET/CT showed a 6 mm mediastinal node (normal by CT criteria) which was FDG avid. Biopsy proved metastatic disease. Treatment plan was changed from mastectomy to chemotherapy alone. Figure 1 Despite the overall excellent results obtained with PET/CT for staging, however, its utility is not uniform among all types of breast cancer. Dashevsky et al. evaluated FDG PET/CT for its ability to detect bone metastases in 95 women with invasive lobular carcinoma (ILC). They found that ILC bone metastases were more commonly sclerotic on CT than patients with infiltrating ductal carcinoma (IDC) and infiltrating
4 mammary carcinoma (IMC). The standardized uptake value (SUV) max in patients with ILC was lower than in patients with IDC and in fact only 3 of 7 ILC patients with sclerotic bone metastases had a FDG-positive PET scan 9. In another study, Hogan et al. evaluated 87 patients with ILC and found that PET/CT did not reveal unsuspected extra-axillary nodes in any patient 10. Follow up 1. Treatment Response Besides being the most accurate modality for locoregional and systemic staging in breast cancer, 18 F-FDG PET/CT accurately predicts treatment response. As far back as 1993, Wahl et al. reported that patients who ultimately responded to chemotherapy showed a 50% decrease in uptake two months into chemotherapy compared to nonresponders, and this change in uptake was independent of change in size 11. Vranjesevic et al. compared the predictive ability of PET/CT to that of conventional imaging in 61 patients and showed that the positive predictive value (PPV) of PET/CT was 93% compared to 85% for conventional imaging, and that the negative predictive value (NPV) was 84% for PET/CT compared to 59% for conventional imaging 12. Other (non- FDA approved) PET tracers have also been demonstrated to predict response at an early time point, allowing for potential earlier treatment change (risk adaptive treatment). Kenny et al. used 18F-fluorothymidine (FLT) PET which assesses tumor proliferation and showed that a decrease in SUV at 1 week discriminated between clinical response and stable disease 13. Theoretically, if the oncologists can determine that a certain drug combination is not working at an earlier time point, the treatment course may be altered and the patient could benefit from a different treatment before an increase in disease burden which may render the disease
5 more difficult to treat, and avoid unnecessary morbidity of ineffectual therapy. This risk adaptive approach has been successful in treating patients with lymphoma and hopefully can be adopted in breast cancer as well. Once a patient has been treated for breast cancer, accurate assessment of treatment response is vital for both clinical trials as well as for patient care. Currently, for clinical trials and in many practices, follow up assessments of patients are often made using purely anatomic imaging, most often with CT scanning. Decrease in the size of the tumor after treatment is the measure of response. This approach is particularly problematic in women with breast cancer since bone is the most common site of metastatic disease and bone metastases cannot be reliably measured unless there is an extraosseous soft tissue mass associated with the bone lesion. Otherwise, it is difficult to determine treatment response. Development of or increase in sclerosis can be due to either healing or progressive disease. Likewise, a bone scan may show increased uptake caused by a metabolic flare, progression, or disease healing. If PET/CT is employed, physicians will be able to measure the change in SUV reflecting change in metabolic activity and thus determine response to treatment. Figure 2 shows PET/CT imaging in a patient with known hypermetabolic sclerotic metastasis to L3. After treatment, there were no changes in the appearance on CT imaging; the patient would be considered as having a stable disease. However, on PET/CT imaging, there is a significant reduction in FDG activity, confirming treatment response.
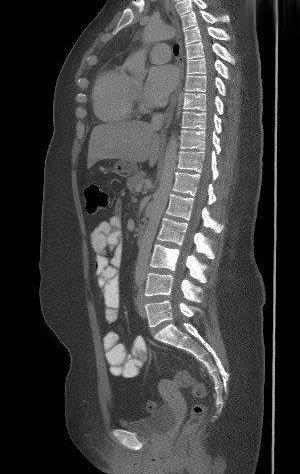



6 Figure 2



7 Figure 3 shows PET/CT imaging in a patient with bone only metastases at presentation and who had a good response to chemotherapy in her bone metastases. However, at the same time as the response in the bone, the patient developed a liver metastasis, which was only seen on FDG PET/CT. Figure 3 Another source of difficulty when assessing treatment response is that patients often have a heterogeneous response within the various tumor sites. This is of particular concern in women presenting with bone metastases. It is well recognized that even within the same patient, there is tumor heterogeneity 14. Huyge et al. demonstrated that in 46 women with bone dominant metastatic breast cancer, the women had heterogeneous response in 43% of the treatment phases; in the subset with both bone and extra-bone metastases, PET/CT showed discordant responses between bone and extra-bone metastases in 30% of treatment phases. 15. In a
8 study that did not include FDG PET Lorincz 16 evaluated 48 women with metastatic breast cancer and showed that half of those with HER 2+ disease lost the genotype in their bone metastases. 2. Clinical trial evaluation The treatment response of patients in clinical trials is most often evaluated by CT using the RECIST (Response Evaluation Criteria in Solid Tumors) 1.1 criteria and is therefore purely anatomic. Five lesions are chosen per patient and except for lymph nodes, a single measurement of the longest diameter of the metastasis is followed. For lymph nodes, a measurement of the short axis, which must be at least 1.5 cm, is followed. Reliability of measurements has been called into question. PERCIST (Positron Emission Tomography Response Criteria in Solid Tumors adds physiology to anatomy. FDG PET/CT is performed >10 days after chemotherapy with measurement of up to five lesions with the most intense uptake. Response is defined as the % change in SUL (SUV corrected for lean body mass). The following case demonstrates the superiority of PERSIST: Figure 4 shows FDG PET/CT in a 35-year-old woman who presented with lung and liver metastases. As a baseline (Figure 4A) for a clinical trial, she had CT chest, abdomen, and pelvis with contrast as required by protocol which used RECIST 1.1 criteria to assess response. She also had a PET/CT. After the first 3 months of chemotherapy she was re-imaged (4B) as per protocol and demonstrated complete response in the lung and near complete response in the liver on both CT and PET/CT with a residual small, mildly FDG avid lesion in the posterior right lobe. She therefore qualified for more chemotherapy after which CT was stable by RECIST
9 which meant that she would undergo another 2 cycles of chemotherapy even though the residual liver lesion had become more hypermetabolic and a new area of FDG avidity had developed in another part of the liver. After the next 2 cycles of this experimental regimen which was clearly not working by PET criteria, she also demonstrated progression on CT. At that point she was considered to have disease progression and taken off the initial protocol and switched to a different chemotherapy combination:

10 4A

11 4B
12 4C

13 4D
14 There are several reasons why this case is an important example. To begin with, this patient underwent two additional cycles of chemotherapy that was not working. This is not only burdensome for the patient; these drugs can be very expensive--far more costly than the additional cost of a PET scan, and can result in additional side effects. Additionally, since this was done on a clinical trial which evaluated the ability of the drug to improve freedom from progression--an endpoint measured in weeks or months in patients with metastatic breast cancer--the results demonstrated 2 additional months of freedom from progression by using the CT results which suggested that the chemotherapy regimen being tested had performed better than it actually had, instead of the more accurate PET/CT results which indicated its lack of efficacy. In a retrospective study, Riedl et al. compared RECIST to PERSIST for their ability to predict progression free survival (PFS) and disease specific survival (DSS) in 71 stage IV patients. PET demonstrated response in patients who had stable CTs and was significantly better at predicting PFS and DSS in these patients 17. Looking forward Targeted therapy is increasingly being used for various subtypes of breast cancer. At the same time, tumorspecific tracers are being developed including 18F-fluoroestradiol (FES) which targets estradiol and may be superior in some estrogen receptor positive tumors 18 and 89Zr-trastuzumab which targets HER 2+ cancers. Although discussion of these tracers is beyond the scope of this paper, it should be noted that the use of new and different tracers should enhance the ability to stage cancer, predict for and assess treatment response beyond the standard imaging with -FDG PET/CT.
15 Conclusion In conclusion, physiologic imaging trumps anatomic imaging not only in the detection of breast cancer but also in the staging of breast cancer and evaluation of response to treatment. As we aim to develop more successful and targeted personalized treatment, targeted personalized imaging will play a critical role in optimizing patient care as well as clinical trial evaluation.
16 References 1. Houssami N, Ciatto S, Turner RM, Cody HS, 3rd, Macaskill P. Preoperative ultrasound-guided needle biopsy of axillary nodes in invasive breast cancer: meta-analysis of its accuracy and utility in staging the axilla. Annals of surgery. Aug 2011;254(2): Heusner TA, Kuemmel S, Hahn S, et al. Diagnostic value of full-dose FDG PET/CT for axillary lymph node staging in breast cancer patients. European journal of nuclear medicine and molecular imaging. Oct 2009;36(10): Koolen BB, Vrancken Peeters MJ, Aukema TS, et al. 18F-FDG PET/CT as a staging procedure in primary stage II and III breast cancer: comparison with conventional imaging techniques. Breast cancer research and treatment. Jan 2012;131(1): Groheux D, Hindie E, Delord M, et al. Prognostic impact of (18)FDG-PET-CT findings in clinical stage III and IIB breast cancer. Journal of the National Cancer Institute. Dec ;104(24): Riedl CC, Slobod E, Jochelson M, et al. Retrospective analysis of 18F-FDG PET/CT for staging asymptomatic breast cancer patients younger than 40 years. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. Oct 2014;55(10): Tatsumi M, Cohade C, Mourtzikos KA, Fishman EK, Wahl RL. Initial experience with FDG-PET/CT in the evaluation of breast cancer. European journal of nuclear medicine and molecular imaging. Mar 2006;33(3): Fuster D, Duch J, Paredes P, et al. Preoperative staging of large primary breast cancer with [18F]fluorodeoxyglucose positron emission tomography/computed tomography compared with conventional imaging procedures. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. Oct ;26(29): Constantinidou A, Martin A, Sharma B, Johnston SR. Positron emission tomography/computed tomography in the management of recurrent/metastatic breast cancer: a large retrospective study from the Royal Marsden Hospital. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO. Feb 2011;22(2): Dashevsky BZ, Goldman DA, Parsons M, et al. Appearance of untreated bone metastases from breast cancer on FDG PET/CT: importance of histologic subtype. European journal of nuclear medicine and molecular imaging. Oct 2015;42(11): Hogan MP, Goldman DA, Dashevsky B, et al. Comparison of 18F-FDG PET/CT for Systemic Staging of Newly Diagnosed Invasive Lobular Carcinoma Versus Invasive Ductal Carcinoma. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. Nov 2015;56(11): Wahl RL, Zasadny K, Helvie M, Hutchins GD, Weber B, Cody R. Metabolic monitoring of breast cancer chemohormonotherapy using positron emission tomography: initial evaluation. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. Nov 1993;11(11):
17 12. Vranjesevic D, Filmont JE, Meta J, et al. Whole-body (18)F-FDG PET and conventional imaging for predicting outcome in previously treated breast cancer patients. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. Mar 2002;43(3): Kenny L, Coombes RC, Vigushin DM, Al-Nahhas A, Shousha S, Aboagye EO. Imaging early changes in proliferation at 1 week post chemotherapy: a pilot study in breast cancer patients with 3'-deoxy-3'- [18F]fluorothymidine positron emission tomography. European journal of nuclear medicine and molecular imaging. Sep 2007;34(9): Gerlinger M, Rowan AJ, Horswell S, et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. The New England journal of medicine. Mar ;366(10): Huyge V, Garcia C, Alexiou J, et al. Heterogeneity of metabolic response to systemic therapy in metastatic breast cancer patients. Clinical oncology. Dec 2010;22(10): Lorincz T, Toth J, Badalian G, Timar J, Szendroi M. HER-2/neu genotype of breast cancer may change in bone metastasis. Pathology oncology research : POR. 2006;12(3): Riedl CC. American Society of Clinical Oncology; 2015; Chicago. 18. Dehdashti F, Mortimer JE, Trinkaus K, et al. PET-based estradiol challenge as a predictive biomarker of response to endocrine therapy in women with estrogen-receptor-positive breast cancer. Breast cancer research and treatment. Feb 2009;113(3):
PET/CT in breast cancer staging
 PET/CT in breast cancer staging Anni Morsing Consultant, PhD, DMSc Rigshospitalet 1 18F- FDG PET/CT for breastcancer staging Where is the clinical impact? To which women should 18F- FDG PET/CT be offered?
PET/CT in breast cancer staging Anni Morsing Consultant, PhD, DMSc Rigshospitalet 1 18F- FDG PET/CT for breastcancer staging Where is the clinical impact? To which women should 18F- FDG PET/CT be offered?
ROLE OF PET-CT IN BREAST CANCER, GUIDELINES AND BEYOND. Prof Jamshed B. Bomanji Institute of Nuclear Medicine UCL Hospitals London
 ROLE OF PET-CT IN BREAST CANCER, GUIDELINES AND BEYOND Prof Jamshed B. Bomanji Institute of Nuclear Medicine UCL Hospitals London CANCER Key facts Estimated 15.2 million new cases per year in 2015 worldwide
ROLE OF PET-CT IN BREAST CANCER, GUIDELINES AND BEYOND Prof Jamshed B. Bomanji Institute of Nuclear Medicine UCL Hospitals London CANCER Key facts Estimated 15.2 million new cases per year in 2015 worldwide
PET/CT in Breast Cancer
 PET/CT in Breast Cancer Rodolfo Núñez Miller, M.D. Nuclear Medicine and Diagnostic Imaging Section Division of Human Health International Atomic Energy Agency Vienna, Austria Overview Introduction Locorregional
PET/CT in Breast Cancer Rodolfo Núñez Miller, M.D. Nuclear Medicine and Diagnostic Imaging Section Division of Human Health International Atomic Energy Agency Vienna, Austria Overview Introduction Locorregional
When do you need PET/CT or MRI in early breast cancer?
 When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
Radiological assessment of neoadjuvent chemotherapy for breast cancer
 XV th Balkan Congress of Radiology Budapest, Hungary, October 12 15, 2017 Radiological assessment of neoadjuvent chemotherapy for breast cancer V. Bešlagić C l i n i c o f R a d i o l o g y, U n i v e
XV th Balkan Congress of Radiology Budapest, Hungary, October 12 15, 2017 Radiological assessment of neoadjuvent chemotherapy for breast cancer V. Bešlagić C l i n i c o f R a d i o l o g y, U n i v e
Detection of Internal Mammary Adenopathy in Patients With Breast Cancer by PET/CT and MRI
 Women s Imaging Original Research Jochelson et al. PET/CT and MRI for Internal Mammary Adenopathy Women s Imaging Original Research Maxine S. Jochelson 1 Lizza Lebron Stefanie S. Jacobs Junting Zheng Chaya
Women s Imaging Original Research Jochelson et al. PET/CT and MRI for Internal Mammary Adenopathy Women s Imaging Original Research Maxine S. Jochelson 1 Lizza Lebron Stefanie S. Jacobs Junting Zheng Chaya
Dr Sneha Shah Tata Memorial Hospital, Mumbai.
 Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
Breast cancer is accurately detected, staged, and restaged
 Whole-Body 18 F-FDG PET and Conventional Imaging for Predicting Outcome in Previously Treated Breast Cancer Patients Duska Vranjesevic, MD 1 ; Jean Emmanuel Filmont, MD 1 ; Joubin Meta, MS 1 ; Daniel H.
Whole-Body 18 F-FDG PET and Conventional Imaging for Predicting Outcome in Previously Treated Breast Cancer Patients Duska Vranjesevic, MD 1 ; Jean Emmanuel Filmont, MD 1 ; Joubin Meta, MS 1 ; Daniel H.
Molecular Imaging and Cancer
 Molecular Imaging and Cancer Cancer causes one in every four deaths in the United States, second only to heart disease. According to the U.S. Department of Health and Human Services, more than 512,000
Molecular Imaging and Cancer Cancer causes one in every four deaths in the United States, second only to heart disease. According to the U.S. Department of Health and Human Services, more than 512,000
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
Prediction of Postoperative Tumor Size in Breast Cancer Patients by Clinical Assessment, Mammography and Ultrasonography
 Prediction of Postoperative Tumor Size in Breast Cancer Patients by Clinical Assessment, Mammography and Ultrasonography Eyad Fawzi AlSaeed 1 and Mutahir A. Tunio 2* 1 Consultant Radiation Oncology, Chairman
Prediction of Postoperative Tumor Size in Breast Cancer Patients by Clinical Assessment, Mammography and Ultrasonography Eyad Fawzi AlSaeed 1 and Mutahir A. Tunio 2* 1 Consultant Radiation Oncology, Chairman
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
An Introduction to PET Imaging in Oncology
 January 2002 An Introduction to PET Imaging in Oncology Janet McLaren, Harvard Medical School Year III Basics of PET Principle of Physiologic Imaging: Allows in vivo visualization of structures by their
January 2002 An Introduction to PET Imaging in Oncology Janet McLaren, Harvard Medical School Year III Basics of PET Principle of Physiologic Imaging: Allows in vivo visualization of structures by their
FDG-PET/CT in Gynaecologic Cancers
 Friday, August 31, 2012 Session 6, 9:00-9:30 FDG-PET/CT in Gynaecologic Cancers (Uterine) cervical cancer Endometrial cancer & Uterine sarcomas Ovarian cancer Little mermaid (Edvard Eriksen 1913) honoring
Friday, August 31, 2012 Session 6, 9:00-9:30 FDG-PET/CT in Gynaecologic Cancers (Uterine) cervical cancer Endometrial cancer & Uterine sarcomas Ovarian cancer Little mermaid (Edvard Eriksen 1913) honoring
Clinical Utility of Positron Emission Tomography Scanning in Breast Cancer Management
 Clinical Utility of Positron Emission Tomography Scanning in Breast Cancer Management David Schuster, MD Director, Division of Nuclear Medicine and Molecular Imaging U N I V E R S I T Y S C H O O L O F
Clinical Utility of Positron Emission Tomography Scanning in Breast Cancer Management David Schuster, MD Director, Division of Nuclear Medicine and Molecular Imaging U N I V E R S I T Y S C H O O L O F
SBI/ACR Breast Imaging Symposium April 7-10, 2016 Austin, TX
 SBI/ACR Breast Imaging Symposium April 7-10, 2016 Austin, TX SAM Session 2 Friday, April 8 2.5 SAM Credits Thank you for completing this SAM activity. Below you will find correct responses, rationales,
SBI/ACR Breast Imaging Symposium April 7-10, 2016 Austin, TX SAM Session 2 Friday, April 8 2.5 SAM Credits Thank you for completing this SAM activity. Below you will find correct responses, rationales,
Clinical Utility of Positron Emission Tomography Scanning in Breast Cancer Management
 Clinical Utility of Positron Emission Tomography Scanning in Breast Cancer Management David Schuster, MD Director, Division of Nuclear Medicine and Molecular Imaging Department of Radiology and Imaging
Clinical Utility of Positron Emission Tomography Scanning in Breast Cancer Management David Schuster, MD Director, Division of Nuclear Medicine and Molecular Imaging Department of Radiology and Imaging
ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER. B.Zandi Professor of Radiology
 ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER B.Zandi Professor of Radiology Introduction In the USA, Breast Cancer is : The Most Common Non-Skin Cancer The Second Leading cause of
ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER B.Zandi Professor of Radiology Introduction In the USA, Breast Cancer is : The Most Common Non-Skin Cancer The Second Leading cause of
Evaluation of Lung Cancer Response: Current Practice and Advances
 Evaluation of Lung Cancer Response: Current Practice and Advances Jeremy J. Erasmus I have no financial relationships, arrangements or affiliations and this presentation will not include discussion of
Evaluation of Lung Cancer Response: Current Practice and Advances Jeremy J. Erasmus I have no financial relationships, arrangements or affiliations and this presentation will not include discussion of
Molecular Imaging and Breast Cancer
 Molecular Imaging and Breast Cancer Breast cancer forms in tissues of the breast usually in the ducts, tubes that carry milk to the nipple, and lobules, the glands that make milk. It occurs in both men
Molecular Imaging and Breast Cancer Breast cancer forms in tissues of the breast usually in the ducts, tubes that carry milk to the nipple, and lobules, the glands that make milk. It occurs in both men
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C.
 Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
The prognosis of patients with locally advanced breast
 F-FDG PET/CT in Staging Patients with Locally Advanced or Inflammatory Breast Cancer: Comparison to Conventional Staging David Groheux 1,2, Sylvie Giacchetti 3, Marc Delord 4, Elif Hindié 2,5, Laetitia
F-FDG PET/CT in Staging Patients with Locally Advanced or Inflammatory Breast Cancer: Comparison to Conventional Staging David Groheux 1,2, Sylvie Giacchetti 3, Marc Delord 4, Elif Hindié 2,5, Laetitia
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Maria João Cardoso, MD, PhD
 Locally Advanced Breast Cancer Specific Issues in LocorregionalTreatment Surgery, MD, PhD Head Breast Surgeon Breast Unit, Champalimaud Foundation Lisbon, Portugal 1 Conflict of Interest Disclosure No
Locally Advanced Breast Cancer Specific Issues in LocorregionalTreatment Surgery, MD, PhD Head Breast Surgeon Breast Unit, Champalimaud Foundation Lisbon, Portugal 1 Conflict of Interest Disclosure No
Expert Review The Role of Molecular Imaging in Response Prediction in Metastatic Breast Cancer
 Expert Review The Role of Molecular Imaging in Response Prediction in Metastatic Breast Cancer Geraldine Gebhart, MD Institut Jules Bordet Brussels, Belgium Discussants Moderator Lee Lokey, MD prime Oncology
Expert Review The Role of Molecular Imaging in Response Prediction in Metastatic Breast Cancer Geraldine Gebhart, MD Institut Jules Bordet Brussels, Belgium Discussants Moderator Lee Lokey, MD prime Oncology
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010
 Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Positron emission tomography/computer tomography in the evaluation of head and neck cancer treatment
 Positron emission tomography/computer tomography in the evaluation of head and neck cancer treatment Severina Šedienė 1, Ilona Kulakienė 1, Viktoras Rudžianskas 2 1 Lithuanian University of Health Sciences,
Positron emission tomography/computer tomography in the evaluation of head and neck cancer treatment Severina Šedienė 1, Ilona Kulakienė 1, Viktoras Rudžianskas 2 1 Lithuanian University of Health Sciences,
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
ASPS Recommended Insurance Coverage Criteria for Third- Party Payers
 ASPS Recommended Insurance Coverage Criteria for Third- Party Payers Breast Implant Associated Anaplastic Large Cell Lymphoma BACKGROUND Anaplastic Large Cell Lymphoma (ALCL) is a rare type of cancer of
ASPS Recommended Insurance Coverage Criteria for Third- Party Payers Breast Implant Associated Anaplastic Large Cell Lymphoma BACKGROUND Anaplastic Large Cell Lymphoma (ALCL) is a rare type of cancer of
Diagnosis and staging of breast cancer and multidisciplinary team working
 1 Diagnosis and staging of breast cancer and multidisciplinary team working Common symptoms and signs Over 90% of breast cancers (BCs) are local or regional when first detected. At least 60% of patients
1 Diagnosis and staging of breast cancer and multidisciplinary team working Common symptoms and signs Over 90% of breast cancers (BCs) are local or regional when first detected. At least 60% of patients
Citation for published version (APA): van Kruchten, M. (2015). Molecular imaging of estrogen receptors [Groningen]: University of Groningen
![Citation for published version (APA): van Kruchten, M. (2015). Molecular imaging of estrogen receptors [Groningen]: University of Groningen](/thumbs/89/99843822.jpg "Citation for published version (APA): van Kruchten, M. (2015). Molecular imaging of estrogen receptors [Groningen]: University of Groningen") University of Groningen Molecular imaging of estrogen receptors van Kruchten, Michel IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please
University of Groningen Molecular imaging of estrogen receptors van Kruchten, Michel IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please
Breast Cancer Imaging
 Breast Cancer Imaging I. Policy University Health Alliance (UHA) will cover breast imaging when such services meet the medical criteria guidelines (subject to limitations and exclusions) indicated below.
Breast Cancer Imaging I. Policy University Health Alliance (UHA) will cover breast imaging when such services meet the medical criteria guidelines (subject to limitations and exclusions) indicated below.
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine
 What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
Innovations in Breast Molecular Imaging and Targeted Therapy
 Innovations in Breast Molecular Imaging and Targeted Therapy Professor Jason S. Lewis, PhD Emily Tow Jackson Endowed Chair in Oncology Memorial Sloan Kettering Cancer Center Disclosure No relevant financial
Innovations in Breast Molecular Imaging and Targeted Therapy Professor Jason S. Lewis, PhD Emily Tow Jackson Endowed Chair in Oncology Memorial Sloan Kettering Cancer Center Disclosure No relevant financial
Role of positron emission mammography (PEM) for assessment of axillary lymph node status in patients with breast cancer
 for assessment of axillary lymph node status in patients with breast cancer") Role of positron emission mammography (PEM) for assessment of axillary lymph node status in patients with breast cancer Poster No.: C-1260 Congress: ECR 2011 Type: Scientific Paper Authors: K. M. Kulkarni,
Role of positron emission mammography (PEM) for assessment of axillary lymph node status in patients with breast cancer Poster No.: C-1260 Congress: ECR 2011 Type: Scientific Paper Authors: K. M. Kulkarni,
Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study
 [ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
[ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
Esophageal Cancer. What is the value of performing PET scan routinely for staging of esophageal cancers
 Esophageal Cancer What is the value of performing PET scan routinely for staging of esophageal cancers What is the sensitivity and specificity of PET scan for metastatic lesions When should PET scan be
Esophageal Cancer What is the value of performing PET scan routinely for staging of esophageal cancers What is the sensitivity and specificity of PET scan for metastatic lesions When should PET scan be
Page: 1 of 29. For this policy, PET scanning is discussed for the following 4 applications in oncology:
 Emission Tomography Scanning Page: 1 of 29 Last Review Status/Date: June 2015 Description Positron emission tomography (PET) scans are based on the use of positron-emitting radionuclide tracers coupled
Emission Tomography Scanning Page: 1 of 29 Last Review Status/Date: June 2015 Description Positron emission tomography (PET) scans are based on the use of positron-emitting radionuclide tracers coupled
PET/CT for Therapy Assessment in Oncology
 PET/CT for Therapy Assessment in Oncology Rodolfo Núñez Miller, M.D. Nuclear Medicine Section Division of Human Health International Atomic Energy Agency Vienna, Austria Clinical Applications of PET/CT
PET/CT for Therapy Assessment in Oncology Rodolfo Núñez Miller, M.D. Nuclear Medicine Section Division of Human Health International Atomic Energy Agency Vienna, Austria Clinical Applications of PET/CT
Utility of PET-CT for detection of N2 or N3 nodal mestastases in the mediastinum in patients with non-small cell lung cancer (NSCLC)
") Utility of PET-CT for detection of N2 or N3 nodal mestastases in the mediastinum in patients with non-small cell lung cancer (NSCLC) Poster No.: C-1360 Congress: ECR 2015 Type: Scientific Exhibit Authors:
Utility of PET-CT for detection of N2 or N3 nodal mestastases in the mediastinum in patients with non-small cell lung cancer (NSCLC) Poster No.: C-1360 Congress: ECR 2015 Type: Scientific Exhibit Authors:
Utility of 18 F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer
 Utility of F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer Ngoc Ha Le 1*, Hong Son Mai 1, Van Nguyen Le 2, Quang Bieu Bui 2 1 Department
Utility of F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer Ngoc Ha Le 1*, Hong Son Mai 1, Van Nguyen Le 2, Quang Bieu Bui 2 1 Department
Minimizing Errors in Diagnostic Pathology
 Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville Medical Director, Shands Jacksonville Breast Health Center
Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville Medical Director, Shands Jacksonville Breast Health Center
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
It is a malignancy originating from breast tissue
 59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
PET-imaging: when can it be used to direct lymphoma treatment?
 PET-imaging: when can it be used to direct lymphoma treatment? Luca Ceriani Nuclear Medicine and PET-CT centre Oncology Institute of Southern Switzerland Bellinzona Disclosure slide I declare no conflict
PET-imaging: when can it be used to direct lymphoma treatment? Luca Ceriani Nuclear Medicine and PET-CT centre Oncology Institute of Southern Switzerland Bellinzona Disclosure slide I declare no conflict
Advances in Breast Surgery. Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015
 Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
16/09/2015. ACOSOG Z011 changing practice. Presentation outline. Nodal mets #1 prognostic tool. Less surgery no change in oncologic outcomes
 ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
PET CT for Staging Lung Cancer
 PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
Radiographic Assessment of Response An Overview of RECIST v1.1
 Radiographic Assessment of Response An Overview of RECIST v1.1 Stephen Liu, MD Georgetown University May 15 th, 2015 Presentation Objectives To understand the purpose of RECIST guidelines To describe the
Radiographic Assessment of Response An Overview of RECIST v1.1 Stephen Liu, MD Georgetown University May 15 th, 2015 Presentation Objectives To understand the purpose of RECIST guidelines To describe the
MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES
 MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES Although response is not the primary endpoint of this trial, subjects with measurable disease will be assessed by standard criteria. For the purposes of this
MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES Although response is not the primary endpoint of this trial, subjects with measurable disease will be assessed by standard criteria. For the purposes of this
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Lugano classification: Role of PET-CT in lymphoma follow-up
 CAR Educational Exhibit: ID 084 Lugano classification: Role of PET-CT in lymphoma follow-up Charles Nhan 4 Kevin Lian MD Charlotte J. Yong-Hing MD FRCPC Pete Tonseth 3 MD FRCPC Department of Diagnostic
CAR Educational Exhibit: ID 084 Lugano classification: Role of PET-CT in lymphoma follow-up Charles Nhan 4 Kevin Lian MD Charlotte J. Yong-Hing MD FRCPC Pete Tonseth 3 MD FRCPC Department of Diagnostic
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 PET Scanning: Oncologic Applications Page 1 of 42 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Positron Emission Tomography (PET) Scanning: Oncologic
PET Scanning: Oncologic Applications Page 1 of 42 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Positron Emission Tomography (PET) Scanning: Oncologic
Types of Breast Cancer
 IOWA RADIOLOGY 1 Types of Breast Cancer 515-226-9810 Ankeny Clive Downtown Des Moines IOWA RADIOLOGY 1 Table of Contents Introduction... 1 Ductal Carcinoma... 2 Paget s Disease of the Nipple... 8 Lobular
IOWA RADIOLOGY 1 Types of Breast Cancer 515-226-9810 Ankeny Clive Downtown Des Moines IOWA RADIOLOGY 1 Table of Contents Introduction... 1 Ductal Carcinoma... 2 Paget s Disease of the Nipple... 8 Lobular
Bone and CT Scans Are Complementary for Diagnoses of Bone Metastases in Breast Cancer When PET Scans Findings Are Equivocal: A Case Report
 Bone and CT Scans Are Complementary for Diagnoses of Bone Metastases in Breast Cancer When Scans Findings Are Equivocal: A Case Report Yuk-Wah Tsang 1, Jyh-Gang Leu 2, Yen-Kung Chen 3, Kwan-Hwa Chi 1,4
Bone and CT Scans Are Complementary for Diagnoses of Bone Metastases in Breast Cancer When Scans Findings Are Equivocal: A Case Report Yuk-Wah Tsang 1, Jyh-Gang Leu 2, Yen-Kung Chen 3, Kwan-Hwa Chi 1,4
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY
 EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY AXILLARY LYMPH NODE METASTASIS Axillary lymph node metastasis is one of the most
EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY AXILLARY LYMPH NODE METASTASIS Axillary lymph node metastasis is one of the most
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Lymphoma Read with the experts
 Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Breast Cancer Basics. Clinical Oncology for Public Health Professionals. Ben Ho Park, MD, PhD
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Case Scenario 1: Breast
 Case Scenario 1: Breast A 63 year old white female presents with a large mass in her left breast. 4/15/13 Mammogram/US: 1. Left breast mammographic and sonographic at 3:00 measuring 7.1 cm highly suggestive
Case Scenario 1: Breast A 63 year old white female presents with a large mass in her left breast. 4/15/13 Mammogram/US: 1. Left breast mammographic and sonographic at 3:00 measuring 7.1 cm highly suggestive
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Oncologic Applications of PET Scanning
 6.01.26 Oncologic Applications of PET Scanning Section 6.0 Radiology Subsection Effective Date February 15, 2015 Original Policy Date January 26, 2009 Next Review Date December 2015 Description Positron
6.01.26 Oncologic Applications of PET Scanning Section 6.0 Radiology Subsection Effective Date February 15, 2015 Original Policy Date January 26, 2009 Next Review Date December 2015 Description Positron
8/10/2016. PET/CT for Tumor Response. Staging and restaging Early treatment response evaluation Guiding biopsy
 PET/CT for Tumor Response Evaluation August 4, 2016 Wei Lu, PhD Department of Medical Physics www.mskcc.org Department of Radiation Oncology www.umaryland.edu FDG PET/CT for Cancer Imaging Staging and
PET/CT for Tumor Response Evaluation August 4, 2016 Wei Lu, PhD Department of Medical Physics www.mskcc.org Department of Radiation Oncology www.umaryland.edu FDG PET/CT for Cancer Imaging Staging and
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Welcome to the RECIST 1.1 Quick Reference
 Welcome to the RECIST 1.1 Quick Reference *Eisenhauer, E. A., et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer 2009;45:228-47. Subject Eligibility
Welcome to the RECIST 1.1 Quick Reference *Eisenhauer, E. A., et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer 2009;45:228-47. Subject Eligibility
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Recommendations for cross-sectional imaging in cancer management, Second edition
 www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Carcinoma of unknown primary origin (CUP) Faculty of Clinical Radiology www.rcr.ac.uk Contents Carcinoma of
www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Carcinoma of unknown primary origin (CUP) Faculty of Clinical Radiology www.rcr.ac.uk Contents Carcinoma of
8/2/2017. Imaging in Clinical Trials: An Overview. Outline. Introduction: Clinical Trials
 Imaging in Clinical Trials: An Overview Keyvan Farahani, PhD Cancer Imaging Program, NCI AAPM Beyond Clinical Imaging Aug 2, 2017 Outline Introduction to Oncology Clinical Trials Role of Imaging in Oncology
Imaging in Clinical Trials: An Overview Keyvan Farahani, PhD Cancer Imaging Program, NCI AAPM Beyond Clinical Imaging Aug 2, 2017 Outline Introduction to Oncology Clinical Trials Role of Imaging in Oncology
New Visions in PET: Surgical Decision Making and PET/CT
 New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
Staging and restaging for distant metastatic disease in breast cancer: Has anything changed?
 Staging and restaging for distant metastatic disease in breast cancer: Has anything changed? Sarah J Vinnicombe Clinical Senior Lecturer in Cancer Imaging Dundee Cancer Centre s.vinnicombe@dundee.ac.uk
Staging and restaging for distant metastatic disease in breast cancer: Has anything changed? Sarah J Vinnicombe Clinical Senior Lecturer in Cancer Imaging Dundee Cancer Centre s.vinnicombe@dundee.ac.uk
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
The treatment of newly diagnosed breast cancer is
 Downloaded from jnm.snmjournals.org by on April 17, 20. For personal use only. Response to Therapy in Breast Cancer Norbert Avril 1, Stefanie Sassen 2, and Rebecca Roylance 3 1 Department of Nuclear Medicine,
Downloaded from jnm.snmjournals.org by on April 17, 20. For personal use only. Response to Therapy in Breast Cancer Norbert Avril 1, Stefanie Sassen 2, and Rebecca Roylance 3 1 Department of Nuclear Medicine,
A case of a BRCA2-mutated ER+/HER2 breast cancer during pregnancy
 ESMO Preceptorship Programme Breast Cancer Lisbon 16,17 September 2016 Emanuela Risi Sandro Pitigliani Medical Oncology Department Hospital of Prato, Istituto Toscano Tumori, Prato, Italy A case of a BRCA2-mutated
ESMO Preceptorship Programme Breast Cancer Lisbon 16,17 September 2016 Emanuela Risi Sandro Pitigliani Medical Oncology Department Hospital of Prato, Istituto Toscano Tumori, Prato, Italy A case of a BRCA2-mutated
Imaging Surveillance in Women with a History of Treated Breast Cancer. Wei Tse Yang, M.D.
 Imaging Surveillance in Women with a History of Treated Breast Cancer Wei Tse Yang, M.D. Breast Cancer 1. Extent 2. Response 3. Recurrence Surveillance Breast Cancer 1. Extent 2. Response Surveillance
Imaging Surveillance in Women with a History of Treated Breast Cancer Wei Tse Yang, M.D. Breast Cancer 1. Extent 2. Response 3. Recurrence Surveillance Breast Cancer 1. Extent 2. Response Surveillance
Department of Breast Oncology, National Hospital Organization Shikoku Cancer Center, Matsuyama, Japan
 Predictive Ability of 18 F-fluorodeoxyglucose Positron Emission Tomography/computed Tomography for Pathological Complete Response and Prognosis after Neoadjuvant Chemotherapy in Triplenegative Breast Cancer
Predictive Ability of 18 F-fluorodeoxyglucose Positron Emission Tomography/computed Tomography for Pathological Complete Response and Prognosis after Neoadjuvant Chemotherapy in Triplenegative Breast Cancer
Update in Lymphoma Imaging
 Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
Detailed Program of the second BREAST IMAGING AND INTERVENTIONS PROGRAM am am : Clinician s requirements from breast imaging
 Detailed Program of the second BREAST IMAGING AND INTERVENTIONS PROGRAM 2012 Day one, 2 nd November BREAST IMAGING AND INTERVENTIONS PROGRAM 2012 9.00 AM 9.10 am Introduction 9.10 am - 9.30 am : Clinician
Detailed Program of the second BREAST IMAGING AND INTERVENTIONS PROGRAM 2012 Day one, 2 nd November BREAST IMAGING AND INTERVENTIONS PROGRAM 2012 9.00 AM 9.10 am Introduction 9.10 am - 9.30 am : Clinician
Cancer Program Report 2014
 Cancer Program Report 2014 Queen of the Valley Hospital St Joseph Health Queen of the Valley Hospital - 2014 Site Table Site Total Class Sex Group Cases Analytic NonAn M F 0 I II ALL SITES 661 494 167
Cancer Program Report 2014 Queen of the Valley Hospital St Joseph Health Queen of the Valley Hospital - 2014 Site Table Site Total Class Sex Group Cases Analytic NonAn M F 0 I II ALL SITES 661 494 167
Mammographic imaging of nonpalpable breast lesions. Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand
 Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
F NaF PET/CT in the Evaluation of Skeletal Malignancy
 F NaF PET/CT in the Evaluation of Skeletal Malignancy Andrei Iagaru, MD September 26, 2013 School of of Medicine Ø Introduction Ø F NaF PET/CT in Primary Bone Cancers Ø F NaF PET/CT in Bone Metastases
F NaF PET/CT in the Evaluation of Skeletal Malignancy Andrei Iagaru, MD September 26, 2013 School of of Medicine Ø Introduction Ø F NaF PET/CT in Primary Bone Cancers Ø F NaF PET/CT in Bone Metastases
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 PET Scanning: Oncologic Applications Page 1 of 88 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Positron Emission Tomography (PET) Scanning: Oncologic Applications
PET Scanning: Oncologic Applications Page 1 of 88 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Positron Emission Tomography (PET) Scanning: Oncologic Applications
Contemporary Classification of Breast Cancer
 Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
WHAT DOES PET IMAGING ADD TO CONVENTIONAL STAGING OF HEAD AND NECK CANCER PATIENTS?
 doi:10.1016/j.ijrobp.2006.12.044 Int. J. Radiation Oncology Biol. Phys., Vol. 68, No. 2, pp. 383 387, 2007 Copyright 2007 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/07/$ see front
doi:10.1016/j.ijrobp.2006.12.044 Int. J. Radiation Oncology Biol. Phys., Vol. 68, No. 2, pp. 383 387, 2007 Copyright 2007 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/07/$ see front
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Targeting Surgery for Known Axillary Disease. Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center
 Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
ARROCase - April 2017
 ARROCase - April 2017 Radiation Indications in the setting of Neoadjuvant chemotherapy for Breast Cancer Lauren Colbert, MD, MSCR Faculty Mentor: Benjamin Smith, MD UT MD Anderson Cancer Center 37 year
ARROCase - April 2017 Radiation Indications in the setting of Neoadjuvant chemotherapy for Breast Cancer Lauren Colbert, MD, MSCR Faculty Mentor: Benjamin Smith, MD UT MD Anderson Cancer Center 37 year
Theranostics in Nuclear Medicine
 Theranostics in Nuclear Medicine Patrick FLAMEN, MD, PhD Head Nuclear Medicine Institut Jules Bordet Université Libre de Bruxelles (U.L.B.) n Theranostics in Nuclear Medicine n A form of (nuclear) diagnostic
Theranostics in Nuclear Medicine Patrick FLAMEN, MD, PhD Head Nuclear Medicine Institut Jules Bordet Université Libre de Bruxelles (U.L.B.) n Theranostics in Nuclear Medicine n A form of (nuclear) diagnostic
Here are examples of bilateral analog mammograms from the same patient including CC and MLO projections.
 Good afternoon. It s my pleasure to be discussing Diagnostic Breast Imaging over the next half hour. I m Wei Yang, Professor of Diagnostic Radiology and Chief, the Section of Breast Imaging as well as
Good afternoon. It s my pleasure to be discussing Diagnostic Breast Imaging over the next half hour. I m Wei Yang, Professor of Diagnostic Radiology and Chief, the Section of Breast Imaging as well as