Personalized ADT. Thomas Keane MD
|
|
|
- Hilda Pearson
- 5 years ago
- Views:
Transcription
1 Personalized ADT Thomas Keane MD
2 Conflicts Ferring Tolemar Bayer Astellas myriad
3 Personalized ADT for the Specific Cardiac Obesity and testosterone Fsh High volume disease Docetaxol Significant LUTS
4 Cardiovascular risk profile and ADT Is there a difference?
5 Degarelix belongs to a class of synthe@c drug, GnRH antagonist (blocker) GnRH pglu His Trp Ser Tyr Gly Leu Arg Pro Gly NH 2 Leuprolide D- Leu NEt Goserelin Triptorelin D- Ser NH 2 D- Trp NH 2 LHRH agonists Buserelin D- Ser NEt Degarelix Abarelix Cetrorelix Ganirelix D- NaI D- Cpa D- PaI Aph D-Aph D- Ala NH 2 D- NaI D- Cpa D- PaI N- Me Tyr D- Asn Lys D- Ala NH 2 D- NaI D- Cpa D- PaI D- Cit D- Ala NH 2 D- NaI D- CPa D- PaI D- harg D- harg D- Ala NH 2 GnRH antagonists Millar RP, et al. Endocr Rev 2004;25:235 75

6 Most acute CVD events are caused by rupture of a vulnerable atherosclero@c plaque


7 The vulnerable plaque thin cap with Inflammation
8 Plaque instability is at the heart of cardiovascular disease Stable plaque Vulnerable plaque Fibrous cap Lumen Lipid core Lumen Fibrous cap Lipid core Thick Cap Thin Rich in SMC and matrix Composi,on Rich in inflammatory cells: Poor Lipid Rich Inflammatory Inflammatory state Highly inflammatory Libby P. 1995;91:
9 Incidence of both prostate cancer and CV events is highest in older men Prostate cancer CV events 3500 Prostate cancer 3500 All CV disease Major CV events Age- specific incidence per 100,000 person- years CV, cardiovascular Major CV events = myocardial infarc@on, stroke, or death due to CV disease All CV disease = major CV events + self- reported angina or revascularisa@on procedures Driver, et al. BMJ 2008;337:a2467
10 Men with prostate cancer and pre- CVD have an increased risk of death Popula,on n (%) Cumula,ve survival (%) 1- year 5- years Adjusted HR (95% CI) Overall 30,721 (100) No IHD or stroke 25,114 (82) (ref) IHD 4,276 (14) ( ) Stroke 1,331 (4) ( ) *HR adjusted for age, stage, calendar period and comorbidity (excluding IHD and stroke) Influence of prostate cancer therapy on mortality rates not assessed CVD, cardiovascular disease IHD, ischaemic heart disease Jespersen CG, et al. BMC Cancer 2012;11:519
11 Oestrogen therapy increases risk of CV- related side effects 2,052 with stage I IV prostate cancer treated using radical prostatectomy or orchiectomy with or without oestrogen Survival significantly shorter in pa@ents with stage I III prostate cancer receiving oestrogens, but incidence of prostate cancer- related death reduced Significant increase in deaths due to CV disease in pa@ents treated with oestrogen Cause of death No oestrogen therapy (n=1,035) Received oestrogen therapy (1,017) Prostate cancer 149 (14.4%) 107 (10.5%) CV 90 (8.7%) 149 (14.7%) Pulmonary embolus 10 (1%) 11 (1.1%) Other 85 (8%) 91 (9.0%) Veterans Administra@on Co- opera@ve Urological Research Group. Surg Gynecol Obstet 1967;124:1011-7
12 This has been confirmed with other types of ADT Incident CHD Myocardial infarction Sudden cardiac death Stroke Treatment Adjusted HR (95% CI) Adjusted HR (95% CI) Adjusted HR (95% CI) Adjusted HR (95% CI) No ADT Ref Ref Ref Ref GnRH agonist 1.19* ( ) 1.28* ( ) 1.35* ( ) 1.21* ( ) Orchiectomy 1.40* ( ) 2.11* ( ) 1.29 ( ) 1.49 ( ) CAB 1.27* ( ) 1.03 ( ) 1.22 ( ) 0.93 ( ) Antiandrogen 1.10 ( ) 1.05 ( ) 1.06 ( ) 0.86 ( ) study of 37,443 men with prostate cancer 39% received some form of ADT during follow- up, primarily GnRH agonists (37.5%) *p<0.05 Few were treated with orchiectomy (0.8%) or oral monotherapy (3.3%) at or CAB (4.9%) for >6 weeks at the start of GnRH agonist therapy ADT, androgen therapy CAB, combined androgen blockade CHD, coronary heart disease; ref, reference NL, et al. J Natl Can Inst 2010;102:39 46
13 The risk has been shown to be increased in older men and those with Men aged 65 years receiving 6 months of ADT had to fatal myocardial infarc@on compared with RT alone (p=0.017) 1 Pa@ents with moderate or severe comorbidi@es* had a greater risk of a fatal myocardial infarc@on when receiving RT + ADT compared with RT alone 2 ADT, androgen depriva@on therapy RT, radiotherapy *Based on Adult Comorbidity Evalua@on 27 (ACE- 27) 1. D Amico AV, et al. J Clin Oncol 2007;25: D Amico AV, et al. JAMA 2008;299:289 95
14 as well as those with pre- cardiac disease Significant increase in CV morbidity during oestrogen treatment in with a history of CVD (p<0.001) 33% of these pa@ents had a CV event during PEP treatment Oestrogen treatment was the greatest risk factor for CV events in a mul@variate analysis (p=0.029) CVD, cardiovascular disease PEP, polyestradiol phosphate Hedlund PO, et al. Scand J Urol Nephrol 2011;45:346 53
15 Based on the studies shown The increase in risk of CV disease in men treated with ADT (orchiectomy, oestrogen or GnRH agonist) appears to be 20 25% In comparison, known major risk factors for CV disease increase risk as follows: Smoking vs no smoking: 22% Hypertension vs no hypertension: 20-93% Low vs not low HDL cholesterol: 44% High vs low total cholesterol: 73% Diabetes vs no diabetes: 122% Lloyd- Jones, et al. 2006;113:791-8
16 CVD is the second most common cause of death in men with prostate cancer Prostate cancer n (%) CVD n (%) Other n (%) EORTC Immediate ADT Delayed ADT Total 94 (37) 99 (35) 193 (36) 88 (34) 97 (34) 185 (34) 75 (29) 88 (31) 163 (30) SEUG Intermirent ADT Con@nuous ADT Total 74 (44) 65 (39) 139 (41) 41 (24) 52 (31) 93 (27) 55 (32) 52 (31) 107 (32) 1. Studer UE, et al. J Clin Oncol 2006;24: Calais da Silva F, et al. Eur Urol 2009;55:
17 Pooled data from randomized phase III/IIIb Study trials of degarelix vs GnRH agonists CS21 Pivotal phase III, monthly dose CS35 3- month depot CS37 Intermirent dosing CS28 LUTS relief CS30 Neoadjuvant to radical RT CS31 TPV Dura,on (months) Comparator Publica,on 12 Leuprolide Klotz et al. BJU Int Goserelin Shore et al. SIU Leuprolide Crawford et al. SUO 2013 *All patients on goserelin also received antiandrogen flare protection 3 Goserelin* Anderson et al. Urol Int Goserelin* Mason et al. Clin Oncol Goserelin* Axcona et al. BJU Int 2012 LUTS, lower urinary tract symptoms RT, radiotherapy TPV, total prostate volume
18 Pooled analysis: Treatment groups Degarelix 463 (31%) CVD history 837 GnRH agonist 245 (29%) 458 Goserelin 379 Leuprolide CVD, cardiovascular disease Albertsen PC, et al. Eur Urol 2014:65;565-73
19 Selected baseline demographics to CV risk Variable Degarelix n=1491 GnRH agonist n=837 Age (yrs) Body mass index >30, n (%) (22) (24) History of CVD, n (%) 463 (31) 245 (29) History of smoking, n (%) 707 (47) 432 (52) History of alcohol use, n (%) 889 (60) 475 (57) History of hypertension, n (%) 1117 (75) 615 (74) Serum cholesterol >6.2 mmol/l, n (%) 399 (27) 247 (30) Sta@n medica@on use, n (%) 400 (27) 234 (28) History of diabetes, n (%) 221 (15) 128 (15) CVD, cardiovascular disease Albertsen PC, et al. Eur Urol 2014:65;565-73
20 Results: Overall incidence of CV events* Degarelix, n (%) n=1491 GnRH agonist, n (%) n=837 Any CV event 37 (2.5) 40 (4.7) Serious CV event 25 (1.7) 24 (2.9) A serious CV event was an event considered life-threatening or that required hospitalization *Data classified according to the MedDRA system Albertsen PC, et al. Eur Urol 2014:65; Tombal B, et al. EAU 2013;Poster 677
21 Lower risk of CV event or death with degarelix (all HR=0.60 (95% CI ) p=0.008 HR adjusted for common CV risk factors including age, use, hypertension and serum cholesterol by Cox regression Albertsen PC, et al. Eur Urol 2014:65; Tombal B, et al. EAU 2013;Poster 677
22 Lower risk of CV event or death with degarelix in men with baseline CVD HR=0.44 (95% CI ) p=0.002 There is a >60% lower risk of serious CV event for men with CVD history receiving degarelix (HR=0.367, 95% Cl , p=0.0086) HR adjusted for common CV risk factors including age, sta@n use, hypertension and serum cholesterol by Cox regression CVD, cardiovascular disease Albertsen PC, et al. Eur Urol 2014:65; Tombal B, et al. EAU 2013;Poster 677
23 Overall survival HR=0.47 (95% CI ) p=0.022 Prostate cancer was not the cause of death in the majority of these CVD, cardiovascular disease Miller K, et al. EAU 2013; Poster 678
24 Effect of degarelix remains when adjusted for common CVD variables Covariate HR es,mate 95% CI p- value Degarelix treatment use Alcohol Hypertension* Cigarere smoking Serum cholesterol >6.2 mmol/l Treated type 2 diabetes Treated hypertension Age at baseline Baseline testosterone Baseline body mass index *Diastolic >90 or systolic >140 mmhg CVD, cardiovascular disease Albertsen PC, et al. Eur Urol 2014:65;565-73
25 Pooled analysis: Summary When treated with degarelix compared with a GnRH agonist, pa@ents with pre- exis@ng CVD: Had significantly fewer CV events during the first year of treatment Had a rela@ve risk reduc@on of >50% (absolute risk reduc@on 8.2%) CVD, cardiovascular disease Albertsen PC, et al. Eur Urol 2014:65;565-73
26 Plaque instability is at the heart of cardiovascular disease Stable plaque Vulnerable plaque Fibrous cap Lumen Lipid core Lumen Fibrous cap Lipid core Thick Cap Thin Rich in SMC and matrix Composi,on Rich in inflammatory cells: Poor Lipid Rich inflammatory Inflammatory state More Libby P. 1995;91:


27 GnRH receptors are expressed by smooth muscle cells in plaques Hultgårdh, Nilsson et al, unpublished



28 plaques induced by different types of shear stress Unstable plaque (low shear) Stable plaque (oscillatory shear)

29 Leuprolide induces necrosis in stable oscillatory shear stress- induced plaques 16 weeks 18 weeks 26 weeks 30 weeks Cholesterol -rich diet Shear stressmodifier Degarelix Leuprolide Untreated End point % necrosis * Untreated Degarelix Leuprolide Enanton Untreated Degarelix Leuprolide Hultgårdh, Nilsson et al, unpublished

30 T lymphocytes are key drivers of collagen metabolism in plaques of the cap Plaque instability T Ly Increased risk of thrombo- embolic complica@ons and cardiovascular disease Libby P J. Lipid Res 2009;50:S352- S357
31 T cells express GnRH receptors: Agonists and antagonists have different effects GnRH or GnRH agonist GnRH-R GnRH antagonist GnRH-R T cells T cells Increased proliferation and activity Complete blockade of receptors with no signal transduction Fibrotic cap disruption and plaque instability Inhibition of stimulated responses IFN, interferon Chen HF, et al. J Clin Endocrinol Metab 1999;84: Tanriverdi F, et al. Clin Exp Immunol 2005;142: Grasso G, et al. Life Sci 1998;62: ; Jacobson JD, et al. Endocrinol 1994;134:
32 mechanisms for differences in CV risk with different forms of ADT Differences in CV risk could be due to differences in the effect of different ADTs on: 1. Metabolic changes 2. GnRH receptor 3. FSH levels
33 Personalized ADT for the Specific Cardiac Obesity and testosterone FSH High volume disease Docetaxol Significant LUTS
34 ADT has been associated with metabolic changes Metabolic syndrome is a disorder of energy u@lisa@on and storage, diagnosed by co- occurrence of any 3 of: Abdominal (central) obesity Elevated blood pressure Elevated fas@ng plasma glucose High serum triglycerides Low high- density (HDL) cholesterol levels Metabolic syndrome increases the risk of developing CVD ADT leads to: Insulin resistance Accumula@on of subcutaneous fat and decreased lean body mass Increased glucose levels Abnormali@es in lipid levels Kelly DM, Jones TH. J Endocrinol 2013;217:R25-45
35 Metabolic syndrome and metabolic changes induced by ADT are different Metabolic syndrome Increased triglycerides Increased visceral fat Reduced HDL Hypertension Increased glucose Decreased Increased C- protein Metabolic changes with ADT Increased triglycerides Increased subcutaneous fat Increased HDL Hypertension Increased glucose Increased Normal C- protein Saylor PJ, Smith MR. J Urol 2009;181:
36 FSH and adipogenesis of FSH receptors possibly alters endothelial cell lipid metabolism and fat Preclinical studies have shown: 1 Mice treated with degarelix have lower FSH levels than those treated with LHRH agonist or orchiectomy Degarelix- treated mice gain less weight and visceral fat than mice treated with LHRH agonists 1. Hopmans SN, et al. Urol Oncol 2014; In press
37 Personalized ADT for the Specific Cardiac Obesity and testosterone FSH High volume disease Docetaxol Significant LUTS

38 ADT: mechanism of in to CV risk Degarelix Rapid suppression of FSH, LH and testosterone LHRH agonists Initial surge in FSH, LH and testosterone GnRH antagonist LHRH agonist X X No microsurges Inhibition of GnRH receptors Microsurges on repeat injection Unlikely that testosterone suppression can explain differences in risk Stimulation of GnRH receptors Potential for agonists to have a plaque destabilising effect due to induction of necrosis and T cell stimulation Prolonged suppression of FSH, LH and testosterone FSH suppression not maintained long term Increased potential for metabolic syndrome and atherogenesis with agonist therapy FSH, follicle-stimulating hormone LH, luteinising hormone
39 FSH and LUTS LHRH Antagonist Cetrorelix Reduces Prostate Size and Gene Expression of Proinflammatory Cytokines and Growth Factors in a Rat Model of BPH. Ferenc G Rick et al. Andrew V schally, NormanL.Block. et al. The Prostate 71: (2011) Rela,onship between serum sex hormones levels and degree of benign prostate hyperplasia in Chinese aging men. Zeng QS, Xu CL, Liu ZY. et al. Asian Journal of Andrology (2012) 14, Degarelix versus Goserelin plus Bicalutamide Therapy for Lower Urinary Tract Symptom Relief, Prostate Volume Reduc,on and Quality of life Improvement in Men with ProstateCancer: A Systema,c Reviewand Meta- Analysis. Cui Y, Zong H, Yan H et al. Urol Int 2014; 93: Disease Control Outcomes from Analysis of Pooled Individual Pa,ent Data from Five Compara,ve Randomized Clinical Trials of Degarelix Versus Luteinising Hormone- releasing Hormone Agonists. Klotz L, Miller K. Crawford E.D. et al. European Urology 66 (2014) In Search of the Molecular Mechanisms Media,ng the Inhibitory Effect of the GnRH Antagonist Degarelix on Human Prostate Cell Growth. Sakai M, Mar@nez- Arguelles D, Parerson N. et al. PLOS ONE / DOI: /journal.pone March 26, 2015.


40

41
42 Literature review performed of all published RCTs that used degarelix vs. GnRH agonists + an@androgens for treatment of Pca Degarelix vs. GnRH + Bicalutamide Berer IPSS reduc@on Decreases in IPSS greater in pa@ents with ini@al IPSS score >13 Prostate volume reduc@on similar for both groups Quality of life related to urinary symptoms similar for both groups
43
44 Forest plots showing changes in IPSS, IPSS >= 13, TPC and QoL related to urinary symptoms in the treatment studies. SD = standard devia@on; IV = inverse variance No heterogeneity among trials, pooled es@mate of standardized mean difference is , 95% CI ( to ) (p=0.001). Results suggest decreases in IPSS greater in degarelix. Pa@ents with baseline IPSS >= 13 larger benefit in degarelix group
45 Forest plots showing changes in treatment- emergent adverse events, site and hot flushes in the treatment studies. M- H = Mantel- Haenszel

46

47 No evidence of bias was found
48 Conclusion Meta- analysis indicates that compared to goserelin plus bicalutamide, degarelix has significantly more pronounced effects on LUTS

49

50 Randomized phase 3 trials of degarelix and luteinizing hormone- releasing hormone agonists included in the pooled analysis (safety analysis set)

51 Treatment- emergent adverse events (>5% in either group)
52 Probability of experiencing renal or urinary tract- related adverse event
53 Conclusion Data indicate clinical benefits with degarelix including a significant improvement in PSA PFS and OS as well as reduced incidence of joint, musculoskeletal and urinary tract events compared with LHRH agonists.
 mass spec Inves@gated cell lines express GNRHR1 and")
54 Normal prostate myofibroblast WPMY- 1 and epithelial WPE1- NA22 cells, BPH- 1 cells, androgen independent and dependent (PC- 3 and LNCAP) cells and VCaP cells from (CRPC) pa@ent were used Discriminatory protein and lipid fingerprints of Normal, hyperplas@c and Ca cells generated by matrix assisted laser desorp@on/ioniza@on (MALDI) mass spec Inves@gated cell lines express GNRHR1 and GNRHR2 and their endogenous ligands Treatment with Degarelix reduced cell viability in all cell lines tested, except PC- 3 cells, by increased apoptosis (increased caspase 3/7, 8 and 9 levels) Cell viability was not affected by treatment with GnRH agonists Leuprolide and Goserelin MALDI MS detected changes in m/z signals robust enough to create a complete discriminatory profile induced by Degarelix Transcriptomic analysis of BPH- 1 cells provided a global map of genes affected by Degarelix, indica@ng the biological processes affected were related to cell growth, G- coupled receptors, the MAPK pathway, angiogenesis, and cell adhesion
55 Protein spectra of human prostate cells. (A) MALDI MS protein mass spectra showing expression of protein signals between the 3 cell types. (B) principal component analysis (PCA) score plot, and (C) comparison of the two most discriminant peaks across samples. These analysis iden@fy unique protein signatures for each cell line.
56 Gene expression of prostate human cell lines for GnRH and its receptor subtypes 1 and 2. (A) GNRH1, (B) GNRHR1, (C) GNRH2, and (D) GNRHR2. The white bars show normal cells and the black bars show hyperplasia or cancer cells. Results are presented as a ra@o between the target gene rela@ve to the reference gene normalized to the levels of the control. Results shown are means +/- standard error from 3 independent experiments performed in triplicates. Results indicate significant differences between the various cell lines.
57 MTT assay showing the viability of prostate cell lines following treatment with the GnRH antagonist, degarelix. (A) WPMY- 1, (B) WPE1- NA22, (C) BPH- 1, (D) PC- 3, and (E) LNCaP. Data are expressed as the percentage of the controls and the average +/- standard error. Each assay was done in triplicate in at least 3 independent experiments for each cell line. Two- way ANOVA indicated there was a significant difference overall for degarelix treatment (p<0.001), and the posrest indicated that there were differences against each control, as displayed in each graph (***p<0.001). For PC- 3 cells only Time
58 MTT assay showing the viability of WPE1- NA22, BPH- 1, and LNCaP cell lines following treatment with GnRH agonists. (A- C) Leuprolide and (D- E) goserelin. Note that the different cell lines are displayed in each column. The data are expressed in terms of the percentage of the control and the average +/- standard error. Each assay was done in triplicate with at least n=3 independent experiments for each cell line. Two- way ANOVA displayed p>0.05; there was no difference overall for the treatments.
59 MTT assay showing the viability of the VCaP cell line ader treatment with the GnRH antagonist or agonists. (A) Degarelix, (B) leuprolide, and (C) goserelin. The data are expressed in terms of the percentage of the control and the average +/- standard error. Each assay was done in triplicate with at least n=3 independent experiments for each cell line. Two- way ANOVA indicates that there was a significant difference overall for degarelix treatment (p<0.001), and the posrest indicated that there were differences against each control, as displayed in each graph (*p<0.05). ANOVA displayed p>0.05; for the leuprolide and goserelin groups, there was no difference overall for the treatments.
 of Degarelix- deregulated Genes on BPH- 1")
60 Gene Ontology (Based on Biological Processes) of Degarelix- deregulated Genes on BPH- 1 Cells
 of degarelix- deregulated genes on BPH- 1 cells.")

61 Gene Ontology (Based on Biological Processes) of Degarelix- deregulated Genes on BPH- 1 Cells Gene ontology classifica,on (based on biological processes) of degarelix- deregulated genes on BPH- 1 cells. (A- B) The number of genes deregulated by degarelix in various biological processes azer 6 and 24h, respec@vely. The arrows point to poten@al interes@ng processes in the BPH and degarelix context. (C) Venn diagram illustra@ng the number of genes deregulated by degarelix at 6 and 24h.
62 These data demonstrate 1. Degarelix exerts a direct effect on prostate cell growth through apoptosis 2. MALDI MS analysis provides a basis to fingerprint Degarelix- treated prostate cells 3. Clusters of genes affected by Degarelix suggest that in addi@on to use in prostate cancer, it may be efficacious in BPH
63 Conclusions Different types of human prostate cell lines (normal, hyperplasia and cancer are to the effect of Degarelix. Prostate cell growth was directly inhibited possibly involving a cell cycle related mechanism and leading to apoptosis. Gene Array results indicate a few interes@ng early molecular changes induced by degarelix that could have an impact in the prostate context,mainly controlling BPH growth. A maldi analysis provided the basis to discriminate between the specific proteins and lipids found following degarelix treatment. These findings suggest that GNRHR signaling within the prostate environment should be taken into considera@on when designing therapies for the treatment of prostate diseases.
 percentage change from baseline FSH, follicle- s@mula@ng hormone Crawford ED, et al.")
64 a Further FSH suppression after crossover from leuprolide to degarelix CS21: degarelix or leuprolide CS21A: all degarelix a Median (quar@les) percentage change from baseline FSH, follicle- s@mula@ng hormone Crawford ED, et al. J Urol 2011;186:889 97
65 Median of FSH azer Abarelix and azer GnRH- agonist with 40 Median FSH concentration Median FSH Level (IU/L) GnRH agonist ± antiandrogen Abarelix Garnick MB et al. Mol Urol. 2000;4: Time (Days)


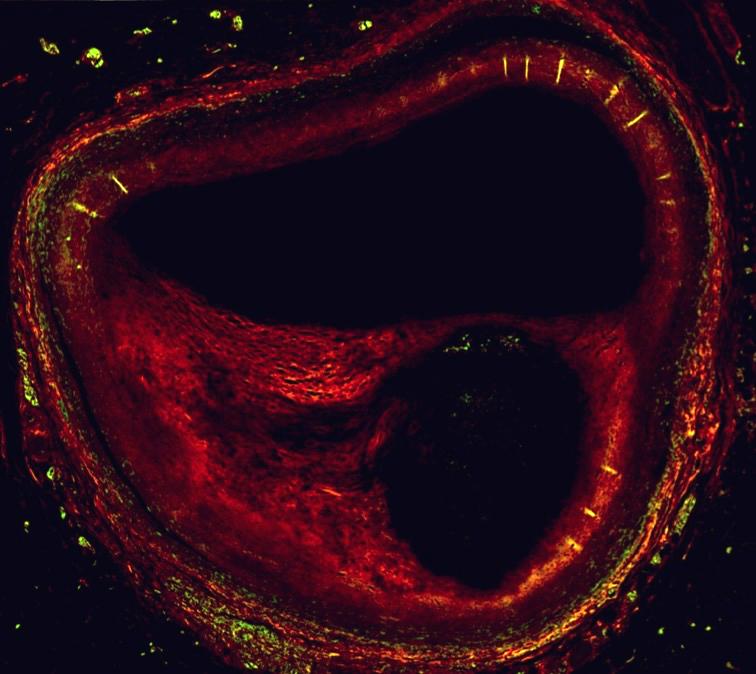
66 FSH receptor is strongly expressed by human prostate tumor blood vessels Analysis of samples from 773 patients with PCa; all samples expressed FSH receptor, whereas normal tissue had no receptor expression Human prostate tumor labeled for FSH receptor and vascular endothelial cell marker Red = FSH- R immunostaining Green = Vascular endothelial cell marker Yellow = Colocaliza@on of markers Vessels Expressing FSH Receptor, % FSH- expressing vessels Tumor No. of vessels Normal Tissue Distance From Tumor Border, mm A higher More density FSH-R of blood expressing vessels vessels is present are present in the tumor compared at or near the to normal tumor border tissue No. of Vessels per mm 2 FSH, follicle-stimulating hormone; PCa, prostate cancer Radu A. New Engl J Med. 2010;363:
67 Personalized ADT for the Specific Cardiac Obesity and testosterone FSH High volume metasta,c disease Docetaxol Significant LUTS
68 High Volume Disease Rapidity of and PSA suppression Lack of flare and miniflare Berer FSH suppression Berer suppression of S- ALP Less SREs Longer of HSPCa state
69 Docetaxel PK varies with State 10 non- castrate and 20 castrate men with similar demographics Clearance of docetaxel in castrate men was 100% increased with 2 fold reduc@on in AUC Erythromycin breath test indicated hepa@c CYP3A4 ac@vity, for docetaxel metabolism, was not different Castrate rats have higher AUC of docetaxel in liver compared to intact animals 50% decrease in docetaxel clearance associated with >430% increase in odds of grade ¾ neutropenia* Franke RM et al. J Clin Oncol 2010; 28: ; *Bruno R et al. J Clin Oncol 1998; 16:
70 What are the of these PK Differences? Between Different Trials May explain some of the greater hematologic toxicity but also survival benefit observed in compared to resistant trials Why was there greater hematologic toxicity in GETUG- AFU 15 compared to CHAARTED? How many were non- castrate vs. castrate in each trial? GETUG- AFU 15: 47% ADT within 15 days of enrollment CHAARTED: ADT median 1.1 months to enrollment How much GCSF was used in each trial? For the Prac,cing Clinician Consider azer 1-2 months of ADT or castrate testosterone levels have been reached before docetaxel? Use GCSF, at least for the first couple cycles, castrate
71 Clinical for the use of ADT: A hormonal therapy algorithm History of CVD? Coronary artery disease Myocardial ischaemia and infarc@on Cerebrovascular accident Angina pectoris Coronary artery bypass YES Degarelix >50% lower CVD risk over one year 1 NO PSA >20 ng/ml or metastases? YES Degarelix Longer PSA PFS 2 No clinical flare 3 Berer S- ALP control 4 Berer bone pain control 5 NO Pa@ents with LUTS: IPSS >12? YES NO Degarelix Berer relief of LUTS 6-8 Degarelix or LHRH agonist 1. Albertsen PC, et al. Eur Urol 2014;65:565 73; 2. Boccon- Gibod L, et al. Therap Adv Urol 2011;3:127 40; 3. Klotz L, et al. BJU Int 2008; 102:1531 8; 4. Schroder FH, et al. BJU Int 2010;106:182 7; 5. Shore N, et al. Presented at SUO 2012;Poster 84; 6. Anderson J, et al. Urol Int 2013;90:321 8; 7. Mason M, et al. Clin Oncol 2013;25:190 6; 8. Axcona K, et al. BJU Int 2012;110:1721 8
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes
 Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Per$nent ques$ons. Is ADT promo+ng CVD? Why ADT may promote CVD? What can we do about it?
 Per$nent ques$ons Is ADT promo+ng CVD? Why ADT may promote CVD? What can we do about it? PC pa$ents are at high risk of CVD Ø Risk of MI, stroke, or CV death in PC pa+ents >2% per year 1, 2 Ø Risk of MI,
Per$nent ques$ons Is ADT promo+ng CVD? Why ADT may promote CVD? What can we do about it? PC pa$ents are at high risk of CVD Ø Risk of MI, stroke, or CV death in PC pa+ents >2% per year 1, 2 Ø Risk of MI,
ADT AND CARDIOVASCULAR RISK: should Antagonists be the primary choice for ADT?
 ADT AND CARDIOVASCULAR RISK: should Antagonists be the primary choice for ADT? Igor Tsaur University Medicine Mainz COI Urologische Klinik und Poliklinik Off-label use of drugs, devices, or other agents:
ADT AND CARDIOVASCULAR RISK: should Antagonists be the primary choice for ADT? Igor Tsaur University Medicine Mainz COI Urologische Klinik und Poliklinik Off-label use of drugs, devices, or other agents:
Risk of renal side effects with ADT. E. David Crawford University of Colorado, Aurora, CO, USA
 Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Mechanism: How ADT accelerates CVD?
 Mechanism: How ADT accelerates CVD? Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials and conflict of interests Professor
Mechanism: How ADT accelerates CVD? Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials and conflict of interests Professor
Cardiovascular Effects of ADT in
 Cardiovascular Effects of ADT in Click to edit Prostate Master Cancer /tle style Pa/ents Chris Plummer Freeman Hospital, Newcastle upon Tyne, UK Newcastle University Bri/sh Cardio- Oncology Society Click
Cardiovascular Effects of ADT in Click to edit Prostate Master Cancer /tle style Pa/ents Chris Plummer Freeman Hospital, Newcastle upon Tyne, UK Newcastle University Bri/sh Cardio- Oncology Society Click
Metastatic prostate carcinoma. Lee Say Bob July 2017
 Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Metasta&c prostate cancer. Walid Obeid PGY IV SGHUMC
 Metasta&c prostate cancer Walid Obeid PGY IV SGHUMC Defini&on Stage IV prostate cancer : is defined by the American Joint CommiEee on Cancer's TNM classifica&on system: T4, N0, M0, any prostate- specific
Metasta&c prostate cancer Walid Obeid PGY IV SGHUMC Defini&on Stage IV prostate cancer : is defined by the American Joint CommiEee on Cancer's TNM classifica&on system: T4, N0, M0, any prostate- specific
Androgen deprivation therapy: New concepts. Laurence Klotz Professor of Surgery Sunnybrook HSC University of Toronto
 Androgen deprivation therapy: New concepts Laurence Klotz Professor of Surgery Sunnybrook HSC University of Toronto Clinical Research funding: 1. Bayer/Algeta 2. Ferring 3. Abbott 4. GSK 5. EMD Serono
Androgen deprivation therapy: New concepts Laurence Klotz Professor of Surgery Sunnybrook HSC University of Toronto Clinical Research funding: 1. Bayer/Algeta 2. Ferring 3. Abbott 4. GSK 5. EMD Serono
Cardiovascular Complica/ons of ADT: Reviewing Pre- clincal and Clinical Data and Introducing the RADICAL- PC Trial
 Cardiovascular Complica/ons of ADT: Reviewing Pre- clincal and Clinical Data and Introducing the RADICAL- PC Trial Jehonathan H. Pinthus MD, Ph.D. Associate professor Department of Surgery- Urology McMaster
Cardiovascular Complica/ons of ADT: Reviewing Pre- clincal and Clinical Data and Introducing the RADICAL- PC Trial Jehonathan H. Pinthus MD, Ph.D. Associate professor Department of Surgery- Urology McMaster
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Francesco Bertoldo. Metabolic Bone Diseases and Osteoncology Unit DRUG INDUCED S OSTEOPOROSIS: ANDROGEN DEPRIVATION THERAPY
 DRUG INDUCED S OSTEOPOROSIS: ANDROGEN DEPRIVATION THERAPY Francesco Bertoldo Metabolic Bone Diseases and Osteoncology Unit Department of Medicine University di Verona EPIDEMIOLGY OF PROSTATE CANCER Prostate
DRUG INDUCED S OSTEOPOROSIS: ANDROGEN DEPRIVATION THERAPY Francesco Bertoldo Metabolic Bone Diseases and Osteoncology Unit Department of Medicine University di Verona EPIDEMIOLGY OF PROSTATE CANCER Prostate
FIRMAGON/DEGARELIX. Compiled by Charles (Chuck) Maack Prostate Cancer Activist/Mentor
 Maack Prostate Cancer Activist/Mentor") FIRMAGON/DEGARELIX The Advantage of this GnRH/LHRH antagonist over that of GnRH/LHRH agonists particularly when administered to patients with known prostate cancer metastases Compiled by Charles (Chuck)
FIRMAGON/DEGARELIX The Advantage of this GnRH/LHRH antagonist over that of GnRH/LHRH agonists particularly when administered to patients with known prostate cancer metastases Compiled by Charles (Chuck)
Degarelix (Firmagon) induction and maintenance for advanced hormone-dependent prostate cancer
 induction and maintenance for advanced hormone-dependent prostate cancer") LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Degarelix (Firmagon) induction and maintenance for advanced hormone-dependent prostate cancer Degarelix (Firmagon) induction and maintenance for advanced hormone-dependent
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Degarelix (Firmagon) induction and maintenance for advanced hormone-dependent prostate cancer Degarelix (Firmagon) induction and maintenance for advanced hormone-dependent
Initial hormone therapy (and more) for metastatic prostate cancer
 for metastatic prostate cancer") Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Cardiovascular Complica/ons of ADT: Reviewing Pre- clincal and Clinical Data and Introducing the RADICAL- PC Trial
 Cardiovascular Complica/ons of ADT: Reviewing Pre- clincal and Clinical Data and Introducing the RADICAL- PC Trial Jehonathan H. Pinthus MD, Ph.D. Associate professor Department of Surgery- Urology McMaster
Cardiovascular Complica/ons of ADT: Reviewing Pre- clincal and Clinical Data and Introducing the RADICAL- PC Trial Jehonathan H. Pinthus MD, Ph.D. Associate professor Department of Surgery- Urology McMaster
Prostate cancer is now the most
 : a new hormonal treatment for prostate cancer Professor Malcolm Mason, School of Medicine, Cardiff University, Velindre Hospital, Whitchurch, Cardiff - hypothalamus According to NICE, prostate cancer
: a new hormonal treatment for prostate cancer Professor Malcolm Mason, School of Medicine, Cardiff University, Velindre Hospital, Whitchurch, Cardiff - hypothalamus According to NICE, prostate cancer
Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer*
 Chinese-German J Clin Oncol DOI 10.1007/s10330-014-0037-9 September 2014, Vol. 13, No. 9, P417 P421 Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer* Abeer
Chinese-German J Clin Oncol DOI 10.1007/s10330-014-0037-9 September 2014, Vol. 13, No. 9, P417 P421 Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer* Abeer
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
majority of the patients. And taking an aggregate of all trials, very possibly has a modest effect on improved survival.
 Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
MEETING REVIEW. Jack Barkin, MD University of Toronto, Humber River Hospital, Toronto, Ontario, Canada. Background
 MEETING REVIEW Risks, benefits, and approaches to hormonal blockade in prostate cancer Highlights from the European Association of Urology Meeting, March 20-24, 2015, Madrid, Spain Jack Barkin, MD University
MEETING REVIEW Risks, benefits, and approaches to hormonal blockade in prostate cancer Highlights from the European Association of Urology Meeting, March 20-24, 2015, Madrid, Spain Jack Barkin, MD University
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Philip Kantoff, MD Dana-Farber Cancer Institute
 CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
Androgen Deprivation Therapy Its impact and the nursing role. Jane Thacker Uro-Oncology Nurse Specialist
 Androgen Deprivation Therapy Its impact and the nursing role Jane Thacker Uro-Oncology Nurse Specialist Overview of content To gain an understanding of ADT (androgendeprivation therapy) and why and how
Androgen Deprivation Therapy Its impact and the nursing role Jane Thacker Uro-Oncology Nurse Specialist Overview of content To gain an understanding of ADT (androgendeprivation therapy) and why and how
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
PCa Commentary. Volume 79 May June 2014
 1221 Madison Street, 1 st Floor Seattle, WA 98104 P 206-215-2480 www.seattleprostate.com PCa Commentary Volume 79 May June 2014 CONTENT: Active Surveillance Page 1 Firmagon and Lupron Page 5 ACTIVE SURVEILLANCE:
1221 Madison Street, 1 st Floor Seattle, WA 98104 P 206-215-2480 www.seattleprostate.com PCa Commentary Volume 79 May June 2014 CONTENT: Active Surveillance Page 1 Firmagon and Lupron Page 5 ACTIVE SURVEILLANCE:
Degarelix Subcutaneous Injection (Firmagon ) Treatment Guideline
 Treatment Guideline") Mid Essex Locality Degarelix Subcutaneous Injection (Firmagon ) Treatment Guideline Contents FlowChart 2 Summary... 3 Key points... 3 Introduction... 3 Pharmacology... 3 Product information... 4 Place
Mid Essex Locality Degarelix Subcutaneous Injection (Firmagon ) Treatment Guideline Contents FlowChart 2 Summary... 3 Key points... 3 Introduction... 3 Pharmacology... 3 Product information... 4 Place
and Sayo Suda Takeshi Kashiwabara *
 Kashiwabara and Suda BMC Cancer (2018) 18:619 https://doi.org/10.1186/s12885-018-4541-0 RESEARCH ARTICLE Open Access Usefulness of combined androgen blockade therapy with gonadotropinreleasing hormone
Kashiwabara and Suda BMC Cancer (2018) 18:619 https://doi.org/10.1186/s12885-018-4541-0 RESEARCH ARTICLE Open Access Usefulness of combined androgen blockade therapy with gonadotropinreleasing hormone
A large database study in the general population in England
 Time-dependent markers of comorbidity severity and change are associated with increased risk of mortality in heart failure: A large database study in the general population in England Claire A. Rushton,
Time-dependent markers of comorbidity severity and change are associated with increased risk of mortality in heart failure: A large database study in the general population in England Claire A. Rushton,
mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE
 mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE IL CARCINOMA PROSTATICO, UNA MALATTIA ETEROGENEA? RAZIONALE E RISULTATI DEL TRATTAMENTO CHEMIOTERAPICO ASSOCIATO ALL
mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE IL CARCINOMA PROSTATICO, UNA MALATTIA ETEROGENEA? RAZIONALE E RISULTATI DEL TRATTAMENTO CHEMIOTERAPICO ASSOCIATO ALL
Complications of Diabetes mellitus. Dr Bill Young 16 March 2015
 Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Efficacy and safety of androgen deprivation therapy after switching from monthly leuprolide to monthly degarelix in patients with prostate cancer
 Efficacy and safety of androgen deprivation therapy after switching from monthly leuprolide to monthly degarelix in patients with prostate cancer Jean De La Rosette, Ronald Davis Iii, David Frankel, Tine
Efficacy and safety of androgen deprivation therapy after switching from monthly leuprolide to monthly degarelix in patients with prostate cancer Jean De La Rosette, Ronald Davis Iii, David Frankel, Tine
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Therapeutic Advances in Urology. Original Research
 621471TAU0010.1177/1756287215621471Therapeutic Advances in UrologyP Iversen, J Damber research-article2015 Therapeutic Advances in Urology Original Research Degarelix monotherapy compared with luteinizing
621471TAU0010.1177/1756287215621471Therapeutic Advances in UrologyP Iversen, J Damber research-article2015 Therapeutic Advances in Urology Original Research Degarelix monotherapy compared with luteinizing
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Bones, Hot Flashes, and ADT Use with Chemotherapy and Timing
 Bones, Hot Flashes, and ADT Use with Chemotherapy and Timing Thomas E. Keane, MD Professor and Chairman Department of Urology Medical University of South Carolina Common Adverse Events Associated with
Bones, Hot Flashes, and ADT Use with Chemotherapy and Timing Thomas E. Keane, MD Professor and Chairman Department of Urology Medical University of South Carolina Common Adverse Events Associated with
Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer
 Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer Daisaku Hirano, MD Department of Urology Higashi- matsuyama Municipal Hospital, Higashi- matsuyama- city, Saitama- prefecture,
Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer Daisaku Hirano, MD Department of Urology Higashi- matsuyama Municipal Hospital, Higashi- matsuyama- city, Saitama- prefecture,
TITLE: Chemical Or Surgical Castration? Is This Still An Important Question?
 TITLE: Chemical Or Surgical Castration? Is This Still An Important Question? SUBTITLE: Chemical Or Surgical Castration? AUTHORS: Michael Kolinsky BSc, MD 1,2, Pasquale Rescigno MD 1,2, Johann S. de Bono
TITLE: Chemical Or Surgical Castration? Is This Still An Important Question? SUBTITLE: Chemical Or Surgical Castration? AUTHORS: Michael Kolinsky BSc, MD 1,2, Pasquale Rescigno MD 1,2, Johann S. de Bono
Central pressures and prediction of cardiovascular events in erectile dysfunction patients
 Central pressures and prediction of cardiovascular events in erectile dysfunction patients N. Ioakeimidis, K. Rokkas, A. Angelis, Z. Kratiras, M. Abdelrasoul, C. Georgakopoulos, D. Terentes-Printzios,
Central pressures and prediction of cardiovascular events in erectile dysfunction patients N. Ioakeimidis, K. Rokkas, A. Angelis, Z. Kratiras, M. Abdelrasoul, C. Georgakopoulos, D. Terentes-Printzios,
Clinical Management Guideline for Planning and Treatment. The process to be followed when a course of chemotherapy is required to treat:
 Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Current role of chemotherapy in hormone-naïve patients Elena Castro
 Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Intermittent Androgen Suppression - A standard of care or a good second choice?
 Intermittent Androgen Suppression - A standard of care or a good second choice? Dr Nicholas Buchan Uro-oncology Fellow Olympic Medal Standings Gold Silver Bronze USA 9 15 13 Germany 10 13 7 Canada 14 7
Intermittent Androgen Suppression - A standard of care or a good second choice? Dr Nicholas Buchan Uro-oncology Fellow Olympic Medal Standings Gold Silver Bronze USA 9 15 13 Germany 10 13 7 Canada 14 7
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
Miyazawa et al. Basic and Clinical Andrology (2015) 25:7 DOI /s
 25:7 DOI /s") Miyazawa et al. Basic and Clinical Andrology (2015) 25:7 DOI 10.1186/s12610-015-0023-2 RESEARCH ARTICLE Open Access Clinical endocrinological evaluation of the gonadal axis (testosterone, LH and FSH) in
Miyazawa et al. Basic and Clinical Andrology (2015) 25:7 DOI 10.1186/s12610-015-0023-2 RESEARCH ARTICLE Open Access Clinical endocrinological evaluation of the gonadal axis (testosterone, LH and FSH) in
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer 2009 MDV Anti-Angiogenesis. Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy. Docetaxel/Epothilone
 Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD
 Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Hormone Replacement Therapy
 Hormone Replacement Therapy What Role Should It Play With Our Patients? Noel R. Williams MD, FACOG TESTOSTERONE FOR MEN: SALVATION OR SNAKE OIL? Definition Male hypogonadism means the testicles don't produce
Hormone Replacement Therapy What Role Should It Play With Our Patients? Noel R. Williams MD, FACOG TESTOSTERONE FOR MEN: SALVATION OR SNAKE OIL? Definition Male hypogonadism means the testicles don't produce
Götz Geiges 1*, Thomas Harms 2, Gerald Rodemer 3, Ralf Eckert 4, Frank König 5, Rolf Eichenauer 6 and Jörg Schroder 5
 Geiges et al. BMC Urology (2015) 15:122 DOI 10.1186/s12894-015-0116-4 RESEARCH ARTICLE Open Access Degarelix therapy for prostate cancer in a real-world setting: experience from the German IQUO (Association
Geiges et al. BMC Urology (2015) 15:122 DOI 10.1186/s12894-015-0116-4 RESEARCH ARTICLE Open Access Degarelix therapy for prostate cancer in a real-world setting: experience from the German IQUO (Association
Treatment of Advanced Prostate Cancer
 Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924
 EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Luteinising hormone-releasing hormone (LHRH) agonists in prostate cancer
 agonists in prostate cancer") B88 April 2015 2.1 Community Interest Company Luteinising hormone-releasing hormone (LHRH) agonists in prostate cancer This bulletin focuses on luteinising hormone-releasing hormone (LHRH) agonists. Currently
B88 April 2015 2.1 Community Interest Company Luteinising hormone-releasing hormone (LHRH) agonists in prostate cancer This bulletin focuses on luteinising hormone-releasing hormone (LHRH) agonists. Currently
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일
 New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
John C. Kim, RPh, JD Senior Director, Regulatory Affairs Ferring Pharmaceuticals Inc. 4 Gatehall Drive 3 rd Floor Parsippany, NJ 07054
 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration Silver Spring, MD 20993 John C. Kim, RPh, JD Senior Director, Regulatory Affairs Ferring Pharmaceuticals Inc. 4
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration Silver Spring, MD 20993 John C. Kim, RPh, JD Senior Director, Regulatory Affairs Ferring Pharmaceuticals Inc. 4
PACKAGE LEAFLET TEXT ZOLADEX LA 10.8MG. (goserelin)
") ONC.000-092-861.10.0 PACKAGE LEAFLET TEXT ZOLADEX LA 10.8MG (goserelin) Name of the medicinal product Zoladex LA 10.8mg depot Qualitative and quantitative composition Goserelin acetate (equivalent to 10.8
ONC.000-092-861.10.0 PACKAGE LEAFLET TEXT ZOLADEX LA 10.8MG (goserelin) Name of the medicinal product Zoladex LA 10.8mg depot Qualitative and quantitative composition Goserelin acetate (equivalent to 10.8
Timing of Androgen Deprivation: The Modern Debate Must be conducted in the following Contexts: 1. Clinical States Model
 Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Does TRT Induce Prostate Cancer?
 Does TRT Induce Prostate Cancer? Prism VI, Bruges, Belgium 21-22November 2014 Herman Leliefeld, Urologist, Utrecht The Netherlands Does TRT Induce Prostate Cancer? Why is it a controversial topic? Is there
Does TRT Induce Prostate Cancer? Prism VI, Bruges, Belgium 21-22November 2014 Herman Leliefeld, Urologist, Utrecht The Netherlands Does TRT Induce Prostate Cancer? Why is it a controversial topic? Is there
METABOLIC SYNDROME DONALD FELITTO, M.D.
 METABOLIC SYNDROME DONALD FELITTO, M.D. DEFINITIONS WHO Defini:on 1999 Diabetes or impaired fas/ng glycemia or IGT or insulin resistance Plus any two: Obesity: BMI > 30, WTH ra/o>0.9 male or >0.85 female.
METABOLIC SYNDROME DONALD FELITTO, M.D. DEFINITIONS WHO Defini:on 1999 Diabetes or impaired fas/ng glycemia or IGT or insulin resistance Plus any two: Obesity: BMI > 30, WTH ra/o>0.9 male or >0.85 female.
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer
 Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
NCCN Guidelines for Prostate Cancer V Web teleconference 06/17/16 and 06/30/17
 Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Point-Counterpoint: Late Onset Hypogonadism (LOH)
") Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
What is New in Hormone Therapy for Prostate Cancer in 2007?
 european urology supplements 7 (2008) 477 483 available at www.sciencedirect.com journal homepage: www.europeanurology.com What is New in Hormone Therapy for Prostate Cancer in 2007? Bertrand Tombal *
european urology supplements 7 (2008) 477 483 available at www.sciencedirect.com journal homepage: www.europeanurology.com What is New in Hormone Therapy for Prostate Cancer in 2007? Bertrand Tombal *
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY. Harvey D White on behalf of The STABILITY Investigators
 STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY Harvey D White on behalf of The STABILITY Investigators Lipoprotein- associated Phospholipase A 2 (Lp-PLA 2 ) activity:
STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY Harvey D White on behalf of The STABILITY Investigators Lipoprotein- associated Phospholipase A 2 (Lp-PLA 2 ) activity:
UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS
 UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS Dr. Neal Shore, Carolina Urologic Research Centre, USA Assoc. Prof. Neeraj Agarwal, Huntsman Cancer Institute,
UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS Dr. Neal Shore, Carolina Urologic Research Centre, USA Assoc. Prof. Neeraj Agarwal, Huntsman Cancer Institute,
MMM. Topic The use of Tadalafil 5mg daily for the treatment of BPH-LUTS
 Dr Tan & Partners MMM Vol. 1 No. 1 Morbidity & Mortality Meeting 14 th November 2014 Introduction Topic The use of Tadalafil 5mg daily for the treatment of BPH-LUTS Tadalafil 5mg daily is a well established
Dr Tan & Partners MMM Vol. 1 No. 1 Morbidity & Mortality Meeting 14 th November 2014 Introduction Topic The use of Tadalafil 5mg daily for the treatment of BPH-LUTS Tadalafil 5mg daily is a well established
Obesity Comorbidi.es: It s About Your Health, Not Your Weight. Elizabeth Estrada, MD Pediatric Endocrinology
 Obesity Comorbidi.es: It s About Your Health, Not Your Weight Elizabeth Estrada, MD Pediatric Endocrinology Conflict of Interest NOTHING TO DISCLOSE Objec.ves 1. Recognize the most common comorbidi.es
Obesity Comorbidi.es: It s About Your Health, Not Your Weight Elizabeth Estrada, MD Pediatric Endocrinology Conflict of Interest NOTHING TO DISCLOSE Objec.ves 1. Recognize the most common comorbidi.es
BJUI. Study Type Therapy (RCT) Level of Evidence 1b OBJECTIVE CONCLUSION
 Level of Evidence 1b OBJECTIVE CONCLUSION") . JOURNAL COMPILATION 9 BJU INTERNATIONAL Urological Oncology SCHRÖDER ET AL. BJUI BJU INTERNATIONAL Changes in alkaline phosphatase levels in patients with prostate cancer receiving degarelix or leuprolide:
. JOURNAL COMPILATION 9 BJU INTERNATIONAL Urological Oncology SCHRÖDER ET AL. BJUI BJU INTERNATIONAL Changes in alkaline phosphatase levels in patients with prostate cancer receiving degarelix or leuprolide:
Resolving the PSA testing controversy. Professor Villis Marshall AC Professor Bruce Armstrong AM Professor Mark Frydenberg
 Resolving the PSA testing controversy Professor Villis Marshall AC Professor Bruce Armstrong AM Professor Mark Frydenberg Professor Villis Marshall AC Introduc)on Guidelines aim to inform tes)ng for the
Resolving the PSA testing controversy Professor Villis Marshall AC Professor Bruce Armstrong AM Professor Mark Frydenberg Professor Villis Marshall AC Introduc)on Guidelines aim to inform tes)ng for the
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Pathology of Coronary Artery Disease
 Pathology of Coronary Artery Disease Seth J. Kligerman, MD Pathology of Coronary Artery Disease Seth Kligerman, MD Assistant Professor Medical Director of MRI University of Maryland Department of Radiology
Pathology of Coronary Artery Disease Seth J. Kligerman, MD Pathology of Coronary Artery Disease Seth Kligerman, MD Assistant Professor Medical Director of MRI University of Maryland Department of Radiology
Testosterone Therapy and the Prostate. Frans M.J. Debruyne Professor of Urology The Netherlands
 Testosterone Therapy and the Prostate Frans M.J. Debruyne Professor of Urology The Netherlands TRT- Risks Prostate ( Cancer, BPH )? Cardiac? Lipids? Polycythemia Sleep apnea Gynecomastia Edema Testosterone
Testosterone Therapy and the Prostate Frans M.J. Debruyne Professor of Urology The Netherlands TRT- Risks Prostate ( Cancer, BPH )? Cardiac? Lipids? Polycythemia Sleep apnea Gynecomastia Edema Testosterone
2. The effectiveness of combined androgen blockade versus monotherapy.
 Relative effectiveness and cost-effectiveness of methods of androgen suppression in the treatment of advanced prostate cancer Blue Cross and Blue Shield Association, Aronson N, Seidenfeld J Authors' objectives
Relative effectiveness and cost-effectiveness of methods of androgen suppression in the treatment of advanced prostate cancer Blue Cross and Blue Shield Association, Aronson N, Seidenfeld J Authors' objectives
ADT vs chemo + ADT as initial treatment for advanced prostate cancer
 ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
Review of the Stampede Results. Charles Ryan MD University of California San Francisco
 Review of the Stampede Results Charles Ryan MD University of California San Francisco Se#ng and hypothesis Se
Review of the Stampede Results Charles Ryan MD University of California San Francisco Se#ng and hypothesis Se
9/3/ AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis. Disclosure
 2013 AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis Robert Gleeson MD Preven5ve Cardiology and Lipid Management Froedtert and The Medical College of Wisconsin Disclosure
2013 AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis Robert Gleeson MD Preven5ve Cardiology and Lipid Management Froedtert and The Medical College of Wisconsin Disclosure
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Final Appraisal Report. Ferring Pharmaceuticals Ltd. Advice No: 2109 December Recommendation of AWMSG
 Final Appraisal Report Degarelix (Firmagon ) for the treatment of advanced hormone-dependent prostate cancer Ferring Pharmaceuticals Ltd Advice No: 2109 December 2009 Recommendation of AWMSG Degarelix
Final Appraisal Report Degarelix (Firmagon ) for the treatment of advanced hormone-dependent prostate cancer Ferring Pharmaceuticals Ltd Advice No: 2109 December 2009 Recommendation of AWMSG Degarelix
Testosterone and the Prostate
 Testosterone and the Prostate E. David Crawford, MD Professor of Surgery (Urology) and Radiation Oncology Head, Urologic Oncology E. David and Vicki M. Crawford Endowed Chair in Urologic Oncology University
Testosterone and the Prostate E. David Crawford, MD Professor of Surgery (Urology) and Radiation Oncology Head, Urologic Oncology E. David and Vicki M. Crawford Endowed Chair in Urologic Oncology University
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
The Spa Hotel, Tunbridge Wells Friday 23 rd March Platinum sponsor
 The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
Guidelines for the Shared Care of Patients on hormonal therapy for Prostate Cancer
 Peterborough City Hospital Department of Urology Guidelines for the Shared Care of Patients on hormonal therapy for Prostate Cancer Hormonal Therapy - How does it work? Prostate Cancer relies on the presence
Peterborough City Hospital Department of Urology Guidelines for the Shared Care of Patients on hormonal therapy for Prostate Cancer Hormonal Therapy - How does it work? Prostate Cancer relies on the presence
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Clinical Trial Synopsis TL-OPI-518, NCT#
 Clinical Trial Synopsis, NCT# 00225264 Title of Study: A Double-Blind, Randomized, Comparator-Controlled Study in Subjects With Type 2 Diabetes Mellitus Comparing the Effects of Pioglitazone HCl vs Glimepiride
Clinical Trial Synopsis, NCT# 00225264 Title of Study: A Double-Blind, Randomized, Comparator-Controlled Study in Subjects With Type 2 Diabetes Mellitus Comparing the Effects of Pioglitazone HCl vs Glimepiride
Cardiac Pathology 2: Heart Failure, Ischemic Heart Disease and other assorted stuff. Kris=ne Kra>s, M.D.
 Cardiac Pathology 2: Heart Failure, Ischemic Heart Disease and other assorted stuff Kris=ne Kra>s, M.D. Cardiac Pathology Outline Blood Vessels Heart I Heart II Cardiac Pathology Outline Blood Vessels
Cardiac Pathology 2: Heart Failure, Ischemic Heart Disease and other assorted stuff Kris=ne Kra>s, M.D. Cardiac Pathology Outline Blood Vessels Heart I Heart II Cardiac Pathology Outline Blood Vessels