METABOLIC SYNDROME DONALD FELITTO, M.D.
|
|
|
- Jasmine Lloyd
- 5 years ago
- Views:
Transcription
1 METABOLIC SYNDROME DONALD FELITTO, M.D.
2 DEFINITIONS
3 WHO Defini:on 1999 Diabetes or impaired fas/ng glycemia or IGT or insulin resistance Plus any two: Obesity: BMI > 30, WTH ra/o>0.9 male or >0.85 female. Dyslipidemia: TG >or= 1.7mmol/liter or HDL cholesterol <0.9 mmol/l male or <1.0mmol/l female. Hypertension: BP > 140/90 mmhg Microalbuminuria: albumin excre/on >20mcg/min
4 European Group for the Study of Insulin Resistance 1999 Insulin Resistance: hyperinsulinemia: top 25% of the fas/ng insulin values from the non- diabe/c popula/on. Plus 2 or more of the following: Central obesity: waist circumference > or = to 94 cm for male and 84 cm female Dyslipidemia: TG > 2.0mmol/L or HDL cholesterol > 1.0mmol/L Hypertension: BP 140/90 and/or medica/on Fas/ng plasma glucose > 6.1mmol/l
5 Na:onal Cholesterol Educa:on Program s Adult Treatment Panel III (2001) Three or more of the following: Central Obesity: waist > 40 in. male and waist > 34 in. female. TG > or = to 150 Low HDL cholesterol: < 40 male and less than 50 female. Hypertension: BP > or = 135/85mm/Hg Fas/ng plasma glucose > 110
6 American Associa:on of Endocrinology - Statement Insulin Resistance Syndrome (2002) Four Iden/fying Abnormali/es: High Triglycerides Low HDL cholesterol Hypertension Elevated fas/ng or post load (75g) glucose. OBESITY is not a component of the defini/on.
 IR,")



")
 BS>/=100 or DM")
7 Comparison of Defini:ons WHO 1999 Risk Factor Impaired glucose regula/on (+2 other risks,) IR, IGT, DM Central Obesity BP > 140/90 TG >150 or HDL. M <35, F <39 Mcroalbuminuria ATP III 2001 Risk Factor (any 3 of 5 risk factors) Blood Sugar >/= 100 Central obesity BPS >/=130, BPD >/= 85 Triglyceride >/= 150 HDL <40M, <50F Am. Assoc. of Endo 2002 Risk factor Elevated fas/ng or post load (75g) glucose Hypertension Elevated Triglycerides Low HDL (no men/on of obesity) Interna/onal Diabetes Federa/on 2005 Risk Factor Central Obesity (plus >/= 2 factors) BS>/=100 or DM BPS>/=135, BPD >/ =85 TG > 150 HDL <40M,,50F

8

9 Table 2: AHA/NHLBI criteria for diagnosis of metabolic syndrome
10 Commonali:es A large waistline: Central Obesity/ Visceral Obesity For women a waistline > 35 and for men >40 Dyslipidemia: High Triglyceride and low HDL in the blood Hypertension: 135/85 or 140/90 Some form of insulin resistance
11 Case Report Mr. B. is a 63 year old man with a past medical history for Hypertension, Dyslipidemia, Obesity and family history of Type 2 Diabetes Mellitus was evaluated for weight loss. The BMI was 36 kg/m2, BP was 144/84, fas/ng blood sugar was 125, TC was 183, LDL cholesterol 112, TG 171, HDL cholesterol 37. The EKG showed old MI.
12 Prevalence of Metabolic Syndrome USA Na/ve Americans 45-49y/o: (58% women and 45% men) USA Filipina- Americans: 50-69y/o (35%) USA 30-79y/o: 25+% (>60y/o 40+%) USA non- Hispanic white:30-79y/o (25%) USA Mexican American 30-79y/o (30%)
13 Prevalence of Metabolic Syndrome Weiss et al. (2004) Severely obese children/adolescents, the prevalence is 50%! NHANES III 12-19y/o using ATPIII criteria for metabolic syndrome the prevalence is 4.2%.
14 Risk factors for developing Metabolic Syndrome Overweight Obesity Lack of physical ac/vity (sedentary lifestyle) Insulin resistance Gene/cs Older age NHLBI 2007
15 Condi:ons that may play a role Fajy Liver (NASH) Polycys/c Ovarian Syndrome Gallstones Sleep Apnea NHLBI 2007
16 The diagnosis of metabolic syndrome requires a tape measure or accurate eye; fasting lipogram and plasma glucose measurements; and BP measurements. Opie L H Circulation. 2007;115:e32-e35 Copyright American Heart Association, Inc. All rights reserved.
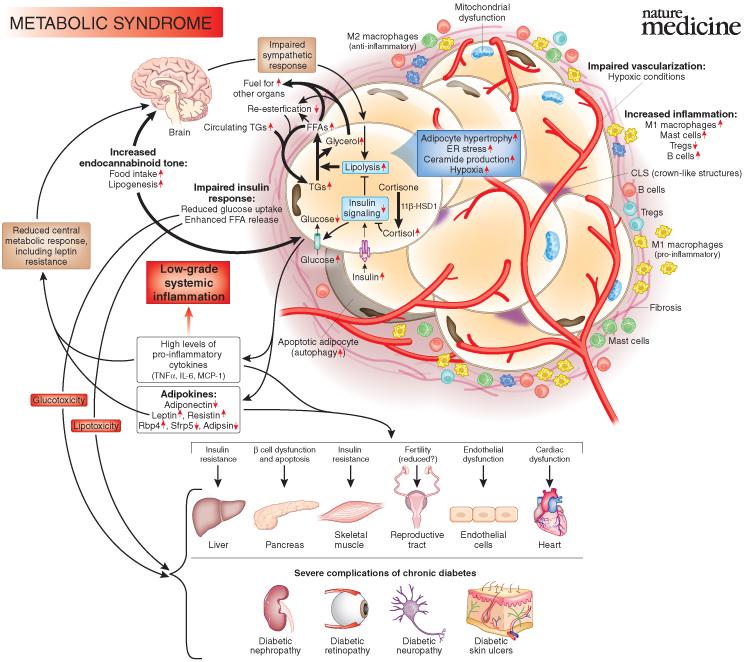
17 Mechanisms Abdominal adipose /ssue is an endocrine organ which releases into circula/on FFA, Angiotensin II and adipokines. Increased FFA in the blood inhibit uptake of glucose by muscle. Excess FFA and AT II damage the pancreas. The pancreas makes extra insulin, it is an insufficient to counter hyperglycemia So, there is increased insulin levels and increased glucose. This is insulin resistance. AT II increases BP through vasoconstric/on. Inflammatory cytokines are responsible IR and Hypertension Hyperglycemia and increased circula/ng FFA contribute to increased manufacture of TG by the liver. Circula/ng TG increase so that lipoproteins carry more TG and less HDL. Circulation 2007;115:e32-e35
18 Mechanisms Insulin resistance: Increased postprandial insulin to maintain euglycemia. Increased fas/ng insulin secre/on to maintain euglycemia. Eventually, hyperglycemia in many. Hyperglycemia and increased FFA will increase insulin levels further. Beta cell dysfunc/on, defec/ve insulin secre/on
19 Pathophysiology AT II increases Blood Pressure The adipose /ssue liberates Tumor Necrosis Factor alpha and interleukins that provoke an inflammatory reac/on which promotes insulin resistance and promotes and promotes hypertension. Hyperglycemia and elevated levels of circula/ng FFA foster the manufacture of triglycerides by the liver. Lipoproteins carry triglyceride and TG level rises. HDL molecules are small and they are easily secreted. These physiologic reac/ons cause the high TG: HDL lipid abnormality. Opie L H Circulation. 2007;115:e32-e35
20 Inflama:on Inflamma/on associated with Insulin resistance: IL 6, TNF a, CRP, are increased. IL 6 and other cytokines increase hepa/c glucose produc/on, inc. hepa/c produc/on of VLDL and increase insulin resistance in muscle /ssue. Cytokines plus FFA increase fibrinogen and plasminogen ac/vator inhibitor 1 (from the liver) promote a prothrombo/c state.
21 Adiponec:n Adiponec/n: An/- inflammatory cytokine produced by adipose /ssue. Enhances insulin sensi/vity and inhibits the inflammatory process. Inhibits hepa/c glucose produc/on. Enhances glucose transport to muscle. It is reduced with insulin resistance. Some associate low concentra/ons with progression of subclinical CAD and MI.
22 The diagnosis of metabolic syndrome requires a tape measure or accurate eye; fasting lipogram and plasma glucose measurements; and BP measurements. Opie L H Circulation. 2007;115:e32-e35 Copyright American Heart Association, Inc. All rights reserved.
23
24 Manifesta:ons Obesity and Physical Inac/vity Dyslipidemia Insulin Resistance/IGT/Hyperinsulinemia (Na reten/on, SNS s/mula/on, HTN, increased circula/ng FFA). Prothrombo/c state Pro- inflammatory state Hyperuricemia defects in insulin ac/on on the renal tubular reabsorp/on of uric acid. Asymmetric dimethylarginine (endothelial dysfunc/on) Homocysteinemia Microalbuminuria Non- alcoholic fajy liver OSA? Lep/n deficiency/dysfunc/on (TG accumula/on and?hyperinsulinism) NHLBI 2007
25 Diagnosis of Metabolic Syndrome Large waistline High TG and low HDL (3:1) Blood Pressure >130/85 High FBS About 85% of people with Type 2 Diabetes Mellitus have Metabolic Syndrome NHLBI 2007
26 Case Report A 45 year old man with a PHx significant for MCD, Obesity, Hyperlipidemia, HTN who despite counseling developed Type 2 DM. BP controlled with ACEI. Total cholesterol 303, TG 1498, Abnormal LFT s, TC/HDL cholesterol 9.2
27 A pa:ent is found to have Metabolic Syndrome; so what?





28 Metabolic Syndrome Lifestyle High Sodium Intake High Caloric Intake Atherogenic diet Carbohydrate abuse Sedentary living plus Predisposi/on Tobacco Abuse Hypertension Obesity Insulin Resistance Premature Coronary Heart Disease Hyperlipidemia Metabolic Syndrome Type 2 Diabetes Mellitus Neuropathy Nephropathy Retinopathy Vasculopathy
29 Metabolic Syndrome is associated with risk of cardiovascular disease The risk of vascular complica/ons (CHD, Type 2 Diabetes Mellitus and Stroke) increase with the number of risk factors. People with Metabolic Syndrome are twice as likely to develop CHD and 5 /mes as likely to develop Type 2 Diabetes Mellitus when compared to pa/ents who do not have Metabolic Syndrome. Coagulopathy (propensity for blood clonng) and inflamma/on (elevated C- Reac/ve Protein) The risk must be added to finding of high LDL and smoking NHLBI 2007
30 Risk of Metabolic Syndrome Although the metabolic syndrome unequivocally predisposes to type 2 diabetes mellitus, 48,58 62 many inves/gators of cardiovascular diseases consider this syndrome to be a mul/dimensional risk factor for ASCVD. 1,58 Several recent reports show that the metabolic syndrome is associated with greater risk for cardiovascular disease, but once type 2 diabetes mellitus emerges, cardiovascular risk increases even more. Ann Intern Med. doi: /m
31 Metabolic Syndrome- Risk Other metabolic risk factors likewise appear individually to be: atherogenic diet Hypertension Elevated blood glucose prothrombo:c state proinflammatory state. Indeed, 3 of the metabolic risk factors elevated apob- containing lipoproteins, 1 low HDL- C levels, 1 and hypertension 91 are well established, major risk factors. Each imparts increased risk even when only marginally abnormal. Ann Intern Med. doi: /m
32 THERAPY
33 Treatments Healthy Lifestyle Ea/ng a healthy diet/losing weight Increasing physical ac/vity Quinng the cigareje smoking habit
34 The Diabetes Preven:on Program A randomized clinical trial tes/ng strategies to prevent Type 2 Diabetes Mellitus. High risk individuals with elevated fas/ng glucose and impaired glucose tolerance. 3,234 par/cipants 27 centers in the U.S.- 20% of whom were over 65y/o. Mean age 51y/o, BMI 34m/kg2. Three interven/ons: intensive lifestyle interven/on, Merormin, Placebo.
35 Diabetes Preven:on Program Primary outcome was development of Type 2 DM Secondary outcomes: CVD, changes in glycemia, Beta cell func/on, insulin sensi/vity, obesity, diet, physical ac/vity, health related QOL, occurrence of adverse events.
36 Diabetes Preven:on Program Inclusion Criteria: Age greater than or equal to 25y/o. BMI >/= 24kg/m2. IGT 2h plasma glucose Elevated FPG (95-125mg/dl)
37 Diabetes Preven:on Program ILS reduced the incidence of Type 2 DM by 58%. Merormin reduced the incidence of Type 2 DM by 31% over 2.8 years. 6.9 par/cipants with IGT would need to be treated with ILS for 3 years to prevent one case of Type 2 DM. For Merormin 14.3 par/cipants for 3 yrs to prevent one case Type 2 DM. Cost analysis shows both therapies to be cost effec/ve. Diabetes Care 9/03
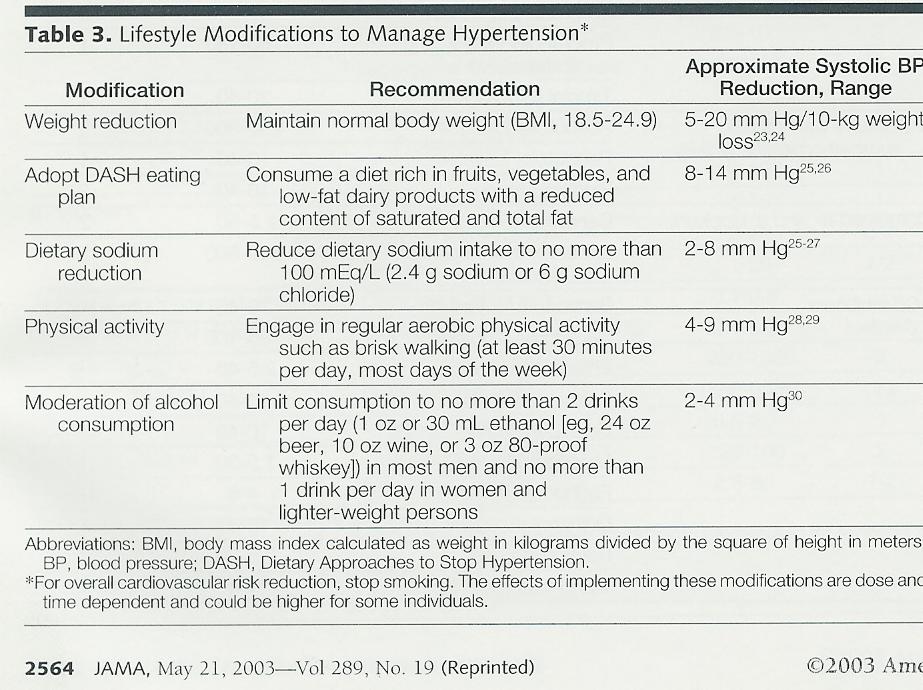
38 Lifestyle changes Losing weight Reduce salt in the diet DASH diet (Dietary Approaches to Stop Hypertension) Increase ac/vity/fitness
39
40 Therapy: Finnish Study Study design: Reduce fat intake Reduce saturated fat Increase Fiber Increase exercise Yield was a 60% reduc/on of Type II Diabetes. Finnish Diabetes Preven/on Study Group. Preven/on of type- 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance.tuomilehto et al. N Engl J Med. 2001;344:
41 Treatment of Metabolic Syndrome Therapeu/c Strategies: 1. Lifestyle changes, exercise, adherence to the Mediterranean diet, and weight loss less new diabetes 2. Merormin (less new diabetes, not as good as lifestyle changes) 3. Glitazones, for non- diabe/cs with high cardiovascular risk: reduce fajy free acids, reduce insulin resistance, Increase HDL, must balance these against possible weight gain and heart failure 4. Choice of an/hypertensives: - blocker/diure/c much more likely to cause metabolic syndrome than calcium channel blockers/angiotensin- conver/ng enzyme inhibitors32 Opie L H Circulation. 2007;115:e32-e35
42 BEHAVIORAL COUNSELING TO PROMOTE A HEALTHFUL DIET AND PHYSICAL ACTIVITY FOR CARDIOVASCULAR DISEASE PREVENTION IN ADULTS WITH CARDIOVASCULAR RISK FACTORS CLINICAL SUMMARY OF U.S. PREVENTIVE SERVICES TASK FORCE RECOMMENDATION Ann Intern Med. doi: /m
43 Importance of the Recommenda:ons 1. Obesity is associated with increased CVD mortality 2. Adults who adhere to na/onal guidelines for a healthy diet and physical ac/vity have a lower cardiovascular morbidity and mortality than those who do not 3. All persons, regardless of CVD risk status, can accrue the health of improved nutri/on, healthy ea/ng behaviors and increased physical ac/vity. AnnInternMed.doi: /M
44 Proof of Efficacy The task force found adequate evidence that intensive behavioral counseling interven/ons have moderate benefits for CVD risk in overweight or obese adults who are at increased risk for CVD, including: Ø Decreases in blood pressure, lipid and fas/ng glucose levels, and body mass index (BMI). Ø Increases in levels of physical ac/vity. Ø The reduc/on in glucose levels was large enough to decrease the incidence of a diabetes diagnosis. Ann Intern Med. doi: /m

45
46 Case Report A 45 year old man with a PHx significant for MCD, Obesity, Hyperlipidemia, HTN who despite counseling developed Type 2 DM. BP controlled with ACEI. Total cholesterol 303, TG 1498, Abnormal LFT s, TC/HDL cholesterol 9.2
47 Case Report: 57lb. Weight Loss Total Protein 1.6g/ 24h Cholesterol 303mg/ dl HDL 32.9 Tc/HDL 9.2 LDL CNC TG mg/24h Cholesterol 191mg/ dl HDL 49mg/dl Tc/HDL 3.89 LDL 95mg/dl TG 236mg/dl
48 Treatments/Medica:ons If lifestyle changes are inadequate; medica/on may be necessary: Hypertension (Ace Inhibitors/Angiotensin Receptor Blockers) Dyslipidemia (Sta/ns and fibrates) High Blood Sugar (Merormin) Excessive blood clonng (ASA may be indicated) Ann Intern Med. doi: /m
49 Disease Burden Cardiovascular disease is the leading cause of death in the US CVD risk factors are common in adults Ann Intern Med. doi: /m
50 Disease Burden The Center for Disease Control and Preven/on es/mates that nearly half of all U.S. adults aged 20 years or older have at least of the following CVD risk factors: Uncontrolled hypertension Elevated low density lipoprotein Current smoking Ø Nearly 70% of U.S. adults are either overweight or obese Ann Intern Med. doi: /m
51 Low carbohydrate vs. Low fat diet 1.Foster GD, et al. A randomized trial of a low- carbohydrate diet for obesity. New England Journal of Medicine, Details: 63 individuals were randomized to either a low- fat diet group, or a low- carb diet group. The low- fat group was calorie restricted. This study went on for 12 months. Weight Loss: The low- carb group lost more weight, 7.3% of total body weight, compared to the low- fat group, which lost 4.5%. The difference was sta/s/cally significant at 3 and 6 months, but not 12 months. Conclusion: There was more weight loss in the low- carb group, significant at 3 and 6 months, but not 12. The low- carb group had greater improvements in blood triglycerides and HDL, but other biomarkers were similar between groups. authoritynutrition.com
52 Low carbohydrate vs. Low fat diet 2. Samaha FF, et al. A low- carbohydrate as compared with a low- fat diet in severe obesity. New England Journal of Medicine, Details: 132 individuals with severe obesity (mean BMI of 43) were randomized to either a low- fat or a low- carb diet. Many of the subjects had metabolic syndrome or type II diabetes. The low- fat dieters were calorie restricted. Study dura/on was 6 months. Weight Loss: The low- carb group lost an average of 5.8 kg (12.8 lbs) while the low- fat group lost only 1.9 kg (4.2 lbs). The difference was sta/s/cally significant. authoritynutrition.com
53 Low carbohydrate vs. Low carbohydrate diet Conclusion: The low- carb group lost significantly more weight (about 3 /mes as much). There was also a sta/s/cally significant difference in several biomarkers: Triglycerides went down by 38 mg/dl in the LC group, compared to 7 mg/dl in the LF group. Insulin sensi/vity improved on LC, got slightly worse on LF. Fas/ng blood glucose levels went down by 26 mg/dl in the LC group, only 5 mg/dl in the LF group. Insulin levels went down by 27% in the LC group, but increased slightly in the LF group. Overall, the low- carb diet had significantly more beneficial effects on weight and key biomarkers in this group of severely obese individuals. authoritynutrition.com
54 Low carbohydrate vs. Low fat diet 8. Meckling KA, et al. Comparison of a low- fat diet to a low- carbohydrate diet on weight loss, body composi/on, and risk factors for diabetes and cardiovascular disease in free- living, overweight men and women. The Journal of Clinical Endocrinology & Metabolism, Details: 40 overweight individuals were randomized to a low- carb and a low- fat diet for 10 weeks. The calories were matched between groups. Weight Loss: The low- carb group lost 7.0 kg (15.4 lbs) and the low- fat group lost 6.8 kg (14.9 lbs). The difference was not sta/s/cally significant. authoritynutrition.com
55 Low carbohydrate vs. Low fat diet Conclusion: Both groups lost a similar amount of weight. A few other notable differences in biomarkers: Blood pressure decreased in both groups, both systolic and diastolic. Total and LDL cholesterol decreased in the LF group only. Triglycerides decreased in both groups. HDL cholesterol went up in the LC group, but decreased in the LF group. Blood sugar went down in both groups, but only the LC group had decreases in insulin levels, indica/ng improved insulin sensi/vity. authoritynutrition.com
56 Low carbohydrate vs. Low Carbohydrate diet 19. Volek JS, et al. Carbohydrate restric/on has a more favorable impact on the metabolic syndrome than a low fat diet. Lipids, Details: 40 subjects with elevated risk factors for cardiovascular disease were randomized to a low- carb or a low- fat diet for 12 weeks. Both groups were calorie restricted. Weight Loss: The low- carb group lost 10.1 kg (22.3), while the low- fat group lost 5.2 kg (11.5 lbs). authoritynutrition.com
57 Low carbohydrate vs. Low fat diet Conclusion: The low- carb group lost almost twice the amount of weight as the low- fat group, despite ea/ng the same amount of calories. This study is par/cularly interes/ng because it matched calories between groups and measured so- called advanced lipid markers. Several things are worth no/ng: Triglycerides went down by 107 mg/dl on LC, but 36 mg/dl on the LF diet. HDL cholesterol increased by 4 mg/dl on LC, but went down by 1 mg/dl on LF. Apolipoprotein B went down by 11 points on LC, but only 2 points on LF. LDL size increased on LC, but stayed the same on LF. On the LC diet, the LDL par/cles partly shixed from small to large (good), while they partly shixed from large to small on LF (bad). authoritynutrition.com
58 Case Report Mrs. D. is a 46 year old woman with a PMH significant for Type 2 Diabetes Mellitus, Hypertension, Dyslipidemia, microalbuminuria, and morbid obesity who was seen in the clinic for weight loss management. BP was 126/80, BMI 54.3kg/m2, : HbA1C : TC 163, LDL 89, HDL 56, TG : weight 356 lbs Axer weight loss of 60lbs, 70/30 insulin requirement has dropped. From 70/ units bid to 30 units bid : HbA1C has likewise dropped to 6.4
59 Physical Ac:vity
, parental history of CHD, postmenopausal status and hormone use (never-use, past, current), physical activity (5 categories), aspirin use")
60 Figure 1. A, Joint associations of waist circumference and physical activity with CHD, the Nurses Health Study 1986 to *Adjusted for age (<50, 50 to 54, 55 to 59, 60 to 64, 65), parental history of CHD, postmenopausal status and hormone use (never-use, past, current), physical activity (5 categories), aspirin use (<1, 1 to 2, 3 to 6, 7 to 14, 15+/wk), BMI (<25, 25 to 29.9, 30 kg/m2), and alcohol consumption (0, 0.1 to 4.9, 5 to 14.9, 15 g/d). Li T Y et al. Circulation. 2006;113: Copyright American Heart Association, Inc. All rights reserved.
, parental history of CHD, postmenopausal status and hormone use (never-use, past, current), physical activity (5 categories), aspirin use")
61 Figure 2. Joint associations of WHR and BMI and CHD, the Nurses Health Study 1986 to *Adjusted for age (<50, 50 to 54, 55 to 59, 60 to 64, 65), parental history of CHD, postmenopausal status and hormone use (never-use, past, current), physical activity (5 categories), aspirin use (<1, 1 to 2, 3 to 6, 7 to 14, 15+/wk), and alcohol consumption (0, 0.1 to 4.9, 5 to 14.9, 15 g/d). Li T Y et al. Circulation. 2006;113: Copyright American Heart Association, Inc. All rights reserved.
62 Goals of Therapy Prevent risk of heart disease Prevent Type 2 Diabetes Mellitus Manage risk factors that can be controlled (weight and sedentary lifestyle) and smoking Ann Intern Med. doi: /m
63 Preven:on and Delay of Metabolic Syndrome Regular follow up with the primary care physician A lifelong commitment to a healthy lifestyle (ea/ng habits and exercise) Long- term effort Because of the rise in the prevalence of obesity, Metabolic Syndrome may overtake smoking as the leading cause of Coronary Heart Disease. Ann Intern Med. doi: /m
64 Summary Onset of Type 2 DM can be delayed. The results have been replicated in Finland and China. Assess CVD risks in each pa/ent Managing each cardiac risk factor with ILS interven/ons and the appropriate medica/ons can reduce CVD morbidity and mortality.
65 Thank you.
66 Pathophysiology Adipose /ssue is an endocrine organ. It liberates excess FFA, AT II and adipokines The rise of FFA in the blood inhibit uptake of glucose by muscle. Excess FFA + AT II damage the pancreas (Lipotoxicity) Pancreas increases insulin but not enough to counter the rise of blood sugar, therefore; both insulin and blood sugar rise. Opie L H Circulation. 2007;115:e32-e35
Obesity Comorbidi.es: It s About Your Health, Not Your Weight. Elizabeth Estrada, MD Pediatric Endocrinology
 Obesity Comorbidi.es: It s About Your Health, Not Your Weight Elizabeth Estrada, MD Pediatric Endocrinology Conflict of Interest NOTHING TO DISCLOSE Objec.ves 1. Recognize the most common comorbidi.es
Obesity Comorbidi.es: It s About Your Health, Not Your Weight Elizabeth Estrada, MD Pediatric Endocrinology Conflict of Interest NOTHING TO DISCLOSE Objec.ves 1. Recognize the most common comorbidi.es
Objectives. Objectives. Alejandro J. de la Torre, MD Cook Children s Hospital May 30, 2015
 Alejandro J. de la Torre, MD Cook Children s Hospital May 30, 2015 Presentation downloaded from http://ce.unthsc.edu Objectives Understand that the obesity epidemic is also affecting children and adolescents
Alejandro J. de la Torre, MD Cook Children s Hospital May 30, 2015 Presentation downloaded from http://ce.unthsc.edu Objectives Understand that the obesity epidemic is also affecting children and adolescents
3/20/2011. Body Mass Index (kg/[m 2 ]) Age at Issue (*BMI > 30, or ~ 30 lbs overweight for 5 4 woman) Mokdad A.H.
![3/20/2011. Body Mass Index (kg/[m 2 ]) Age at Issue (*BMI > 30, or ~ 30 lbs overweight for 5 4 woman) Mokdad A.H.](/thumbs/82/84935173.jpg "3/20/2011. Body Mass Index (kg/[m 2 ]) Age at Issue (*BMI > 30, or ~ 30 lbs overweight for 5 4 woman) Mokdad A.H.") U.S. Adults: 1988 Nineteen states with 10-14% 14% Prevalence of Obesity (*BMI > 30, or ~ 30 lbs overweight for 5 4 woman) Metabolic John P. Cello, MD Professor of Medicine and Surgery, University of California,
U.S. Adults: 1988 Nineteen states with 10-14% 14% Prevalence of Obesity (*BMI > 30, or ~ 30 lbs overweight for 5 4 woman) Metabolic John P. Cello, MD Professor of Medicine and Surgery, University of California,
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
Metabolic Syndrome. Shon Meek MD, PhD Mayo Clinic Florida Endocrinology
 Metabolic Syndrome Shon Meek MD, PhD Mayo Clinic Florida Endocrinology Disclosure No conflict of interest No financial disclosure Does This Patient Have Metabolic Syndrome? 1. Yes 2. No Does This Patient
Metabolic Syndrome Shon Meek MD, PhD Mayo Clinic Florida Endocrinology Disclosure No conflict of interest No financial disclosure Does This Patient Have Metabolic Syndrome? 1. Yes 2. No Does This Patient
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Established Risk Factors for Coronary Heart Disease (CHD)
") Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Diabetes and Heart Disease
 Diabetes and Heart Disease Sarah Alexander, MD Assistant Professor of Medicine Division of Cardiology Rush University Medical Center 2/8/2017 Rush is a not-for-profit health care, education and research
Diabetes and Heart Disease Sarah Alexander, MD Assistant Professor of Medicine Division of Cardiology Rush University Medical Center 2/8/2017 Rush is a not-for-profit health care, education and research
Hypertension with Comorbidities Treatment of Metabolic Risk Factors in Children and Adolescents
 Hypertension with Comorbidities Treatment of Metabolic Risk Factors in Children and Adolescents Stella Stabouli Ass. Professor Pediatrics 1 st Department of Pediatrics Hippocratio Hospital Evaluation of
Hypertension with Comorbidities Treatment of Metabolic Risk Factors in Children and Adolescents Stella Stabouli Ass. Professor Pediatrics 1 st Department of Pediatrics Hippocratio Hospital Evaluation of
Metabolic Syndrome. Bill Roberts, M.D., Ph.D. Professor of Pathology University of Utah
 Metabolic Syndrome Bill Roberts, M.D., Ph.D. Professor of Pathology University of Utah Objectives Be able to outline the pathophysiology of the metabolic syndrome Be able to list diagnostic criteria for
Metabolic Syndrome Bill Roberts, M.D., Ph.D. Professor of Pathology University of Utah Objectives Be able to outline the pathophysiology of the metabolic syndrome Be able to list diagnostic criteria for
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Dietary recommendations in Obesity, Hypertension, Hyperlipidemia, and Diabetes. Stephen D. Sisson MD
 Dietary recommendations in Obesity, Hypertension, Hyperlipidemia, and Diabetes Stephen D. Sisson MD Objectives To review dietary recommendations in the following conditions: Obesity Hypertension Diabetes
Dietary recommendations in Obesity, Hypertension, Hyperlipidemia, and Diabetes Stephen D. Sisson MD Objectives To review dietary recommendations in the following conditions: Obesity Hypertension Diabetes
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
Part 1: Obesity. Dietary recommendations in Obesity, Hypertension, Hyperlipidemia, and Diabetes 10/15/2018. Objectives.
 Dietary recommendations in Obesity, Hypertension, Hyperlipidemia, and Diabetes Stephen D. Sisson MD Objectives To review dietary recommendations in the following conditions: Obesity Hypertension Diabetes
Dietary recommendations in Obesity, Hypertension, Hyperlipidemia, and Diabetes Stephen D. Sisson MD Objectives To review dietary recommendations in the following conditions: Obesity Hypertension Diabetes
Cardiovascular Disease After Spinal Cord Injury: Achieving Best Practice. Suzanne Groah, MD, MSPH Walter Reed Army Medical Center February 12, 2010
 Cardiovascular Disease After Spinal Cord Injury: Achieving Best Practice Suzanne Groah, MD, MSPH Walter Reed Army Medical Center February 12, 2010 CAVEAT LECTOR 2 CVD-related Mortality in Aging SCI GU
Cardiovascular Disease After Spinal Cord Injury: Achieving Best Practice Suzanne Groah, MD, MSPH Walter Reed Army Medical Center February 12, 2010 CAVEAT LECTOR 2 CVD-related Mortality in Aging SCI GU
Metabolic Syndrome.
 www.bmiweightloss.com.au What is the metabolic syndrome? The was first described in 1988 by Gerald Reavson It was originally described as the clustering of four conditions These conditions when present
www.bmiweightloss.com.au What is the metabolic syndrome? The was first described in 1988 by Gerald Reavson It was originally described as the clustering of four conditions These conditions when present
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Risk Factors for Heart Disease
 Risk Factors for Heart Disease Risk Factors we cannot change (Age, Gender, Family History) Risk Factors we can change (modifiable) Smoking Blood pressure Cholesterol Diabetes Inactivity Overweight Stress
Risk Factors for Heart Disease Risk Factors we cannot change (Age, Gender, Family History) Risk Factors we can change (modifiable) Smoking Blood pressure Cholesterol Diabetes Inactivity Overweight Stress
Know Your Number Aggregate Report Single Analysis Compared to National Averages
 Know Your Number Aggregate Report Single Analysis Compared to National s Client: Study Population: 2242 Population: 3,000 Date Range: 04/20/07-08/08/07 Version of Report: V6.2 Page 2 Study Population Demographics
Know Your Number Aggregate Report Single Analysis Compared to National s Client: Study Population: 2242 Population: 3,000 Date Range: 04/20/07-08/08/07 Version of Report: V6.2 Page 2 Study Population Demographics
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Standards of Medical Care in Diabetes 2016
 Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Total risk management of Cardiovascular diseases Nobuhiro Yamada
 Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
Primary and Secondary Prevention of Cardiovascular Disease. Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group
 Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
The Metabolic Syndrome Update The Metabolic Syndrome: Overview. Global Cardiometabolic Risk
 Update 2013 Marc Cornier, M.D. Associate Professor of Medicine Division of Endocrinology, Metabolism & Diabetes Anschutz Health and Wellness Center University of Colorado School of Medicine Denver Health
Update 2013 Marc Cornier, M.D. Associate Professor of Medicine Division of Endocrinology, Metabolism & Diabetes Anschutz Health and Wellness Center University of Colorado School of Medicine Denver Health
2/11/2017. Weighing the Heavy Cardiovascular Burden of Obesity and the Obesity Paradox. Disclosures. Carl J. Lavie, MD, FACC, FACP, FCCP
 Weighing the Heavy Cardiovascular Burden of Obesity and the Obesity Paradox Carl J. Lavie, MD, FACC, FACP, FCCP Professor of Medicine Medical Director, Cardiac Rehabilitation and Preventive Cardiology
Weighing the Heavy Cardiovascular Burden of Obesity and the Obesity Paradox Carl J. Lavie, MD, FACC, FACP, FCCP Professor of Medicine Medical Director, Cardiac Rehabilitation and Preventive Cardiology
Metabolic Syndrome: An overview. Kevin Niswender MD, PhD Vanderbilt University School of Medicine
 Metabolic Syndrome: An overview. Kevin Niswender MD, PhD Vanderbilt University School of Medicine Setting the scene GB, 43 yo AA man followed for hypothyroidism returns on LT4 125 mcg/d and has a TSH=1.1
Metabolic Syndrome: An overview. Kevin Niswender MD, PhD Vanderbilt University School of Medicine Setting the scene GB, 43 yo AA man followed for hypothyroidism returns on LT4 125 mcg/d and has a TSH=1.1
Diabetes and Concomitant Cardiovascular Disease: Guideline Recommendations and Future Directions
 Diabetes and Concomitant Cardiovascular Disease: Guideline Recommendations and Future Directions Diabetes is one of the largest global health emergencies of 21 st century, with the number of people with
Diabetes and Concomitant Cardiovascular Disease: Guideline Recommendations and Future Directions Diabetes is one of the largest global health emergencies of 21 st century, with the number of people with
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
Rick Fox M.A Health and Wellness Specialist
 Metabolic Diseases Rick Fox M.A Health and Wellness Specialist Metabolic Diseases Metabolism is the process your body uses to get or make energy from the food you eat. Food is made up of proteins, carbohydrates
Metabolic Diseases Rick Fox M.A Health and Wellness Specialist Metabolic Diseases Metabolism is the process your body uses to get or make energy from the food you eat. Food is made up of proteins, carbohydrates
Session 21: Heart Health
 Session 21: Heart Health Heart disease and stroke are the leading causes of death in the world for both men and women. People with pre-diabetes, diabetes, and/or the metabolic syndrome are at higher risk
Session 21: Heart Health Heart disease and stroke are the leading causes of death in the world for both men and women. People with pre-diabetes, diabetes, and/or the metabolic syndrome are at higher risk
The Metabolic Syndrome Update The Metabolic Syndrome Update. Global Cardiometabolic Risk
 The Metabolic Syndrome Update 2018 Marc Cornier, M.D. Professor of Medicine Division of Endocrinology, Metabolism & Diabetes Anschutz Health and Wellness Center University of Colorado School of Medicine
The Metabolic Syndrome Update 2018 Marc Cornier, M.D. Professor of Medicine Division of Endocrinology, Metabolism & Diabetes Anschutz Health and Wellness Center University of Colorado School of Medicine
Chapter 2 The Metabolic Syndrome
 Chapter 2 The Metabolic Syndrome Matthew J. Sorrentino Keywords Waist circumference Abdominal obesity Impaired fasting glucose HDL-cholesterol Triglycerides Metabolic syndrome is the designation given
Chapter 2 The Metabolic Syndrome Matthew J. Sorrentino Keywords Waist circumference Abdominal obesity Impaired fasting glucose HDL-cholesterol Triglycerides Metabolic syndrome is the designation given
Diabetes and Heart Disease. Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center
 Diabetes and Heart Disease Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center No conflicts of interest or financial relationships to disclose. 2 What s the problem??
Diabetes and Heart Disease Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center No conflicts of interest or financial relationships to disclose. 2 What s the problem??
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY
 MCC-006 POST GRADUATE DIPLOMA IN CLINICAL CARDIOLOGY (PGDCC) 00269 Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY Time : 2 hours Maximum Marks : 60 Note : There will be multiple
MCC-006 POST GRADUATE DIPLOMA IN CLINICAL CARDIOLOGY (PGDCC) 00269 Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY Time : 2 hours Maximum Marks : 60 Note : There will be multiple
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
THE CLINICAL BIOCHEMISTRY OF LIPID DISORDERS
 THE CLINICAL BIOCHEMISTRY OF LIPID DISORDERS Hormonal regulation INSULIN lipid synthesis, lipolysis CORTISOL lipolysis GLUCAGON lipolysis GROWTH HORMONE lipolysis CATECHOLAMINES lipolysis LEPTIN catabolism
THE CLINICAL BIOCHEMISTRY OF LIPID DISORDERS Hormonal regulation INSULIN lipid synthesis, lipolysis CORTISOL lipolysis GLUCAGON lipolysis GROWTH HORMONE lipolysis CATECHOLAMINES lipolysis LEPTIN catabolism
Pre-diabetes. Pharmacological Approaches to Delay Progression to Diabetes
 Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
13/09/2012. Dietary fatty acids. Triglyceride. Phospholipids:
 CARDIOVASCULAR DISEASES (CVD) and NUTRITION Major cause of morbidity & mortality in Canada & other developed countries e.g., majority of approved health claims on food labels relate to lowering CVD Relation
CARDIOVASCULAR DISEASES (CVD) and NUTRITION Major cause of morbidity & mortality in Canada & other developed countries e.g., majority of approved health claims on food labels relate to lowering CVD Relation
The metabolic syndrome has received increased attention
 AHA/NHLBI Scientific Statement Diagnosis and Management of the Metabolic Syndrome An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement Scott M. Grundy, MD, PhD,
AHA/NHLBI Scientific Statement Diagnosis and Management of the Metabolic Syndrome An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement Scott M. Grundy, MD, PhD,
Complications of Diabetes mellitus. Dr Bill Young 16 March 2015
 Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Metabolic Syndrome in Asians
 Metabolic Syndrome in Asians Alka Kanaya, MD Asst. Professor of Medicine, UCSF Asian CV Symposium, November 17, 2007 The Metabolic Syndrome Also known as: Syndrome X Insulin Resistance Syndrome The Deadly
Metabolic Syndrome in Asians Alka Kanaya, MD Asst. Professor of Medicine, UCSF Asian CV Symposium, November 17, 2007 The Metabolic Syndrome Also known as: Syndrome X Insulin Resistance Syndrome The Deadly
Fructose in diabetes: Friend or Foe. Kim Chong Hwa MD,PhD Sejong general hospital, Division of Endocrinology & Metabolism
 Fructose in diabetes: Friend or Foe Kim Chong Hwa MD,PhD Sejong general hospital, Division of Endocrinology & Metabolism Contents What is Fructose? Why is Fructose of Concern? Effects of Fructose on glycemic
Fructose in diabetes: Friend or Foe Kim Chong Hwa MD,PhD Sejong general hospital, Division of Endocrinology & Metabolism Contents What is Fructose? Why is Fructose of Concern? Effects of Fructose on glycemic
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES
 RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
Also, some risk factors, such as smoking and diabetes, put you at greater risk for CHD and heart attack than others.
 Who is at Risk for Heart Disease? Certain traits, conditions, or habits may raise your risk for coronary heart disease (CHD). These conditions are known as risk factors. Risk factors also increase the
Who is at Risk for Heart Disease? Certain traits, conditions, or habits may raise your risk for coronary heart disease (CHD). These conditions are known as risk factors. Risk factors also increase the
Pathophysiology of Lipid Disorders
 Pathophysiology of Lipid Disorders Henry Ginsberg, M.D. Division of Preventive Medicine and Nutrition CHD in the United States CHD is the single largest killer of men and women 12 million have history
Pathophysiology of Lipid Disorders Henry Ginsberg, M.D. Division of Preventive Medicine and Nutrition CHD in the United States CHD is the single largest killer of men and women 12 million have history
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
9/3/ AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis. Disclosure
 2013 AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis Robert Gleeson MD Preven5ve Cardiology and Lipid Management Froedtert and The Medical College of Wisconsin Disclosure
2013 AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis Robert Gleeson MD Preven5ve Cardiology and Lipid Management Froedtert and The Medical College of Wisconsin Disclosure
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
DYSLIPIDEMIA RECOMMENDATIONS
 DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
Implications of The LookAHEAD Trial: Is Weight Loss Beneficial for Patients with Diabetes?
 Implications of The LookAHEAD Trial: Is Weight Loss Beneficial for Patients with Diabetes? Boston, MA November 7, 213 Edward S. Horton, MD Professor of Medicine Harvard Medical School Senior Investigator
Implications of The LookAHEAD Trial: Is Weight Loss Beneficial for Patients with Diabetes? Boston, MA November 7, 213 Edward S. Horton, MD Professor of Medicine Harvard Medical School Senior Investigator
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Metabolic Syndrome Update The Metabolic Syndrome: Overview. Global Cardiometabolic Risk
 Metabolic Syndrome Update 21 Marc Cornier, M.D. Associate Professor of Medicine Division of Endocrinology, Metabolism & Diabetes University of Colorado Denver Denver Health Medical Center The Metabolic
Metabolic Syndrome Update 21 Marc Cornier, M.D. Associate Professor of Medicine Division of Endocrinology, Metabolism & Diabetes University of Colorado Denver Denver Health Medical Center The Metabolic
Cardiovascular disease, studies at the cellular and molecular level. Linda Lowe Krentz Bioscience in the 21 st Century September 23, 2009
 Cardiovascular disease, studies at the cellular and molecular level Linda Lowe Krentz Bioscience in the 21 st Century September 23, 2009 Content Introduction The number 1 killer in America Some statistics
Cardiovascular disease, studies at the cellular and molecular level Linda Lowe Krentz Bioscience in the 21 st Century September 23, 2009 Content Introduction The number 1 killer in America Some statistics
Comprehensive Treatment for Dyslipidemias. Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium
 Comprehensive Treatment for Dyslipidemias Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium Primary Prevention 41 y/o healthy male No Medications Normal BP, Glucose and BMI Social History:
Comprehensive Treatment for Dyslipidemias Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium Primary Prevention 41 y/o healthy male No Medications Normal BP, Glucose and BMI Social History:
OBESITY IN PRIMARY CARE
 OBESITY IN PRIMARY CARE Obesity- definition Is a chronic disease In ICD 10 E66 Overweight and obesity are defined as abnormal or excessive fat accumulation that may impair health. Obesity is a leading
OBESITY IN PRIMARY CARE Obesity- definition Is a chronic disease In ICD 10 E66 Overweight and obesity are defined as abnormal or excessive fat accumulation that may impair health. Obesity is a leading
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Metabolic Syndrome: Why Should We Look For It?
 021-CardioCase 29/05/06 15:04 Page 21 Metabolic Syndrome: Why Should We Look For It? Dafna Rippel, MD, MHA and Andrew Ignaszewski, MD, FRCPC CardioCase presentation Andy s fatigue Andy, 47, comes to you
021-CardioCase 29/05/06 15:04 Page 21 Metabolic Syndrome: Why Should We Look For It? Dafna Rippel, MD, MHA and Andrew Ignaszewski, MD, FRCPC CardioCase presentation Andy s fatigue Andy, 47, comes to you
Cardiovascular Disease Risk Factors:
 Cardiovascular Disease Risk Factors: Risk factors are traits or habits that increase a person's chances of having cardiovascular disease. Some risk factors can be changed. These risk factors are high blood
Cardiovascular Disease Risk Factors: Risk factors are traits or habits that increase a person's chances of having cardiovascular disease. Some risk factors can be changed. These risk factors are high blood
Know Your Number Aggregate Report Comparison Analysis Between Baseline & Follow-up
 Know Your Number Aggregate Report Comparison Analysis Between Baseline & Follow-up... Study Population: 340... Total Population: 500... Time Window of Baseline: 09/01/13 to 12/20/13... Time Window of Follow-up:
Know Your Number Aggregate Report Comparison Analysis Between Baseline & Follow-up... Study Population: 340... Total Population: 500... Time Window of Baseline: 09/01/13 to 12/20/13... Time Window of Follow-up:
Statistical Fact Sheet Populations
 Statistical Fact Sheet Populations At-a-Glance Summary Tables Men and Cardiovascular Diseases Mexican- American Males Diseases and Risk Factors Total Population Total Males White Males Black Males Total
Statistical Fact Sheet Populations At-a-Glance Summary Tables Men and Cardiovascular Diseases Mexican- American Males Diseases and Risk Factors Total Population Total Males White Males Black Males Total
1Why lipids cannot be transported in blood alone? 2How we transport Fatty acids and steroid hormones?
 1Why lipids cannot be transported in blood alone? 2How we transport Fatty acids and steroid hormones? 3How are dietary lipids transported? 4How lipids synthesized in the liver are transported? 5 Lipoprotien
1Why lipids cannot be transported in blood alone? 2How we transport Fatty acids and steroid hormones? 3How are dietary lipids transported? 4How lipids synthesized in the liver are transported? 5 Lipoprotien
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Hypertension and obesity. Dr Wilson Sugut Moi teaching and referral hospital
 Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Know Your Numbers. Your guide to maintaining good health. Helpful information from Providence Medical Center and Saint John Hospital
 Know Your Numbers Your guide to maintaining good health Helpful information from Providence Medical Center and Saint John Hospital If it has been awhile since your last check up and you are searching for
Know Your Numbers Your guide to maintaining good health Helpful information from Providence Medical Center and Saint John Hospital If it has been awhile since your last check up and you are searching for
Key Nutritional Considerations & Lab Markers as Adjuncts in Effective Lipid Management. Carmen Ritz, MS Clinical Physiologist
 Key Nutritional Considerations & Lab Markers as Adjuncts in Effective Lipid Management Carmen Ritz, MS Clinical Physiologist The Ideal Biomarker to identify risk for CVD Specific accurately identifies
Key Nutritional Considerations & Lab Markers as Adjuncts in Effective Lipid Management Carmen Ritz, MS Clinical Physiologist The Ideal Biomarker to identify risk for CVD Specific accurately identifies
Roadmap. Diabetes and the Metabolic Syndrome in the Asian Population. Asian. subgroups 8.9. in U.S. (% of total
 Diabetes and the Metabolic Syndrome in the Asian Population Alka Kanaya, MD Associate Professor of Medicine, UCSF Feb 26, 2010 Roadmap 1. Diabetes in Asian Americans Prevalence in the U.S. Risk factors
Diabetes and the Metabolic Syndrome in the Asian Population Alka Kanaya, MD Associate Professor of Medicine, UCSF Feb 26, 2010 Roadmap 1. Diabetes in Asian Americans Prevalence in the U.S. Risk factors
Figure S1. Comparison of fasting plasma lipoprotein levels between males (n=108) and females (n=130). Box plots represent the quartiles distribution
 and females (n=130). Box plots represent the quartiles distribution") Figure S1. Comparison of fasting plasma lipoprotein levels between males (n=108) and females (n=130). Box plots represent the quartiles distribution of A: total cholesterol (TC); B: low-density lipoprotein
Figure S1. Comparison of fasting plasma lipoprotein levels between males (n=108) and females (n=130). Box plots represent the quartiles distribution of A: total cholesterol (TC); B: low-density lipoprotein
Establishment of Efficacy of Intervention in those with Metabolic Syndrome. Dr Wendy Russell - ILSI Europe Expert Group
 Establishment of Efficacy of Intervention in those with Metabolic Syndrome Dr Wendy Russell - ILSI Europe Expert Group Conflict of interest regarding this presentation: I have no conflict of interest to
Establishment of Efficacy of Intervention in those with Metabolic Syndrome Dr Wendy Russell - ILSI Europe Expert Group Conflict of interest regarding this presentation: I have no conflict of interest to
... REPORT... The Metabolic Syndrome, Type 2 Diabetes, and Cardiovascular Disease: Understanding the Role of Insulin Resistance
 ... REPORT... The Metabolic Syndrome, Type 2 Diabetes, and Cardiovascular Disease: Understanding the Role of Insulin Resistance David M. Kendall, MD; Anne Peters Harmel, MD Abstract The most common and
... REPORT... The Metabolic Syndrome, Type 2 Diabetes, and Cardiovascular Disease: Understanding the Role of Insulin Resistance David M. Kendall, MD; Anne Peters Harmel, MD Abstract The most common and
Plasma fibrinogen level, BMI and lipid profile in type 2 diabetes mellitus with hypertension
 World Journal of Pharmaceutical Sciences ISSN (Print): 2321-3310; ISSN (Online): 2321-3086 Published by Atom and Cell Publishers All Rights Reserved Available online at: http://www.wjpsonline.org/ Original
World Journal of Pharmaceutical Sciences ISSN (Print): 2321-3310; ISSN (Online): 2321-3086 Published by Atom and Cell Publishers All Rights Reserved Available online at: http://www.wjpsonline.org/ Original
Diabetes Mellitus: Evaluation and Care Management
 Diabetes Mellitus: Evaluation and Care Management Michael King, MD Assistant Professor Residency Program Director University of Kentucky Dept. of Family & Community Medicine Learning Objectives 1. Review
Diabetes Mellitus: Evaluation and Care Management Michael King, MD Assistant Professor Residency Program Director University of Kentucky Dept. of Family & Community Medicine Learning Objectives 1. Review
Clinical Care Performance. Financial Year 2012 to 2018
 Clinical Care Performance Financial Year 2012 to 2018 SHP Clinical Care Performance Diabetes Mellitus Hyperlipidemia Hypertension Diabetes Mellitus Find out how our patients are doing for: HbA1C HbA1c
Clinical Care Performance Financial Year 2012 to 2018 SHP Clinical Care Performance Diabetes Mellitus Hyperlipidemia Hypertension Diabetes Mellitus Find out how our patients are doing for: HbA1C HbA1c
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
ASSeSSing the risk of fatal cardiovascular disease
 ASSeSSing the risk of fatal cardiovascular disease «Systematic Cerebrovascular and coronary Risk Evaluation» think total vascular risk Assess the risk Set the targets Act to get to goal revised; aupril
ASSeSSing the risk of fatal cardiovascular disease «Systematic Cerebrovascular and coronary Risk Evaluation» think total vascular risk Assess the risk Set the targets Act to get to goal revised; aupril
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Controversies in Preventative Cardiology
 Controversies in Preventative Cardiology Francisco Lopez-Jimenez, M.D., M.Sc, FACC, FAHA Professor of Medicine, Mayo Medical School Chair, Division of Preventive Cardiology Co-Director, Artificial Intelligence
Controversies in Preventative Cardiology Francisco Lopez-Jimenez, M.D., M.Sc, FACC, FAHA Professor of Medicine, Mayo Medical School Chair, Division of Preventive Cardiology Co-Director, Artificial Intelligence
Module 2: Metabolic Syndrome & Sarcopenia. Lori Kennedy Inc & Beyond
 Module 2: Metabolic Syndrome & Sarcopenia 1 What You Will Learn Sarcopenia Metabolic Syndrome 2 Sarcopenia Term utilized to define the loss of muscle mass and strength that occurs with aging Progressive
Module 2: Metabolic Syndrome & Sarcopenia 1 What You Will Learn Sarcopenia Metabolic Syndrome 2 Sarcopenia Term utilized to define the loss of muscle mass and strength that occurs with aging Progressive
Before the Pre. PREDIABETES Diagnosis, Management, Treatment. A few thoughts on diabetes.
 PREDIABETES Diagnosis, Management, Treatment Before the Pre A few thoughts on diabetes. James Lenhard, MD Director, Diabetes and Metabolic Diseases Center Christiana Care Health System JLenhard@ChristianaCare.org
PREDIABETES Diagnosis, Management, Treatment Before the Pre A few thoughts on diabetes. James Lenhard, MD Director, Diabetes and Metabolic Diseases Center Christiana Care Health System JLenhard@ChristianaCare.org
 Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
«Πατσζαρκία και Καρδιαγγειακή Νόζος»
 «Πατσζαρκία και Καρδιαγγειακή Νόζος» Δημήτρης Π. Παπαδόπουλος-FESC Clinical Assist. Professor George Washington University USA Επιμελητής Καρδιολογικής Κλινικής Π.Γ.Ν.Α. «ΛΑΪΚΟ» Υπεύθυνος Αντιυπερτασικού
«Πατσζαρκία και Καρδιαγγειακή Νόζος» Δημήτρης Π. Παπαδόπουλος-FESC Clinical Assist. Professor George Washington University USA Επιμελητής Καρδιολογικής Κλινικής Π.Γ.Ν.Α. «ΛΑΪΚΟ» Υπεύθυνος Αντιυπερτασικού
Your Name & Phone Number Here! Longevity Index
 Your Name & Phone Number Here! Longevity Index Your Health Risk Analysis is based on a variety of medical and scientific data from organizations such as the American Heart Association, American Dietetic
Your Name & Phone Number Here! Longevity Index Your Health Risk Analysis is based on a variety of medical and scientific data from organizations such as the American Heart Association, American Dietetic
Metabolic syndrome. Metabolic syndrome and prediabetes appear to be the same disorder, just diagnosed by a different set of biomarkers.
 Metabolic syndrome Metabolic syndrome is a disorder of energy utilization and storage, diagnosed by a co-occurrence of three out of five of the following medical conditions: abdominal (central) obesity,
Metabolic syndrome Metabolic syndrome is a disorder of energy utilization and storage, diagnosed by a co-occurrence of three out of five of the following medical conditions: abdominal (central) obesity,
Sugar-Loaded Beverages and the Impact on Cardiovascular Health. Christina M. Shay, PhD, MA
 Sugar-Loaded Beverages and the Impact on Cardiovascular Health Christina M. Shay, PhD, MA 1 Presenter Disclosure Information Christina M. Shay, PhD, MA Sugar-Loaded Beverages and the Impact on Cardiovascular
Sugar-Loaded Beverages and the Impact on Cardiovascular Health Christina M. Shay, PhD, MA 1 Presenter Disclosure Information Christina M. Shay, PhD, MA Sugar-Loaded Beverages and the Impact on Cardiovascular
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden
 Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Cardiovascular disease physiology. Linda Lowe-Krentz Bioscience in the 21 st Century November 2, 2016
 Cardiovascular disease physiology Linda Lowe-Krentz Bioscience in the 21 st Century November 2, 2016 Content Introduction The number 1 killer in America Some statistics Recommendations The disease process
Cardiovascular disease physiology Linda Lowe-Krentz Bioscience in the 21 st Century November 2, 2016 Content Introduction The number 1 killer in America Some statistics Recommendations The disease process
Low carbohydrate diets- do they have a place?
 Low carbohydrate diets- do they have a place? Grant Schofield Professor of Public Health AUT University, Auckland NZ @grantsnz www.facebook.com/profgrant www.profgrant.com Atherogenic dyslipidemia is [primarily]
Low carbohydrate diets- do they have a place? Grant Schofield Professor of Public Health AUT University, Auckland NZ @grantsnz www.facebook.com/profgrant www.profgrant.com Atherogenic dyslipidemia is [primarily]
HSN301 REVISION NOTES TOPIC 1 METABOLIC SYNDROME
 HSN301 REVISION NOTES TOPIC 1 METABOLIC SYNDROME What does the term Metabolic Syndrome describe? Metabolic syndrome describes a cluster of cardio-metabolic conditions that increase one's risk of developing
HSN301 REVISION NOTES TOPIC 1 METABOLIC SYNDROME What does the term Metabolic Syndrome describe? Metabolic syndrome describes a cluster of cardio-metabolic conditions that increase one's risk of developing
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
overweight you are part of it!... Healthier, fitter, safer... Seafarers Health Information Programme ICSW S.H.I.P.
 overweight you are part of it!... Seafarers Health Information Programme Healthier, fitter, safer... S.H.I.P. ICSW BROCHUREA5_COR1.indd 1 24/08/2007 19:38:40 Overweight prevention, you are part of it!...
overweight you are part of it!... Seafarers Health Information Programme Healthier, fitter, safer... S.H.I.P. ICSW BROCHUREA5_COR1.indd 1 24/08/2007 19:38:40 Overweight prevention, you are part of it!...
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Misperceptions still exist that cardiovascular disease is not a real problem for women.
 Management of Cardiovascular Risk Factors in the Cynthia A., MD University of California, San Diego ARHP 9/19/08 Disclosures Research support Wyeth, Lilly, Organon, Novo Nordisk, Pfizer Consultant fees
Management of Cardiovascular Risk Factors in the Cynthia A., MD University of California, San Diego ARHP 9/19/08 Disclosures Research support Wyeth, Lilly, Organon, Novo Nordisk, Pfizer Consultant fees