Metasta&c prostate cancer. Walid Obeid PGY IV SGHUMC
|
|
|
- Angelina Warner
- 5 years ago
- Views:
Transcription
1 Metasta&c prostate cancer Walid Obeid PGY IV SGHUMC
2 Defini&on Stage IV prostate cancer : is defined by the American Joint CommiEee on Cancer's TNM classifica&on system: T4, N0, M0, any prostate- specific an&gen (PSA), any Gleason. Any T, N1, M0, any PSA, any Gleason. Any T, any N, M1, any PSA, any Gleason
3 Incidence Approximately 10-20% of newly diagnosed prostate cancer cases involve locally advanced disease. Advanced disease is comparably less common, because more early stage cancer is being discovered with availability of PSA screening
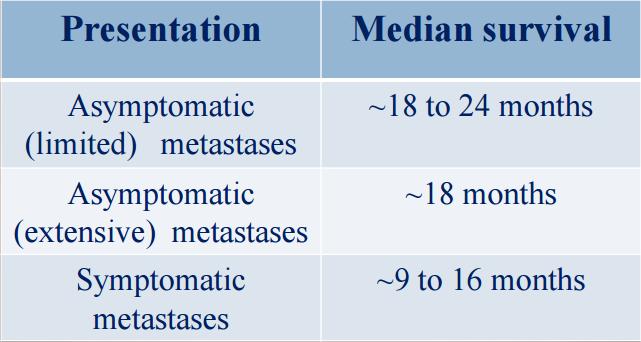
4 Prognosis
5 Presenta&on Anemia Bone marrow suppression Weight loss Pathologic fractures Spinal cord compression Pain Hematuria Ureteral and/or bladder outlet obstruc&on Urinary reten&on Chronic renal failure Urinary incon&nence Symptoms related to bony or soz- &ssue metastases
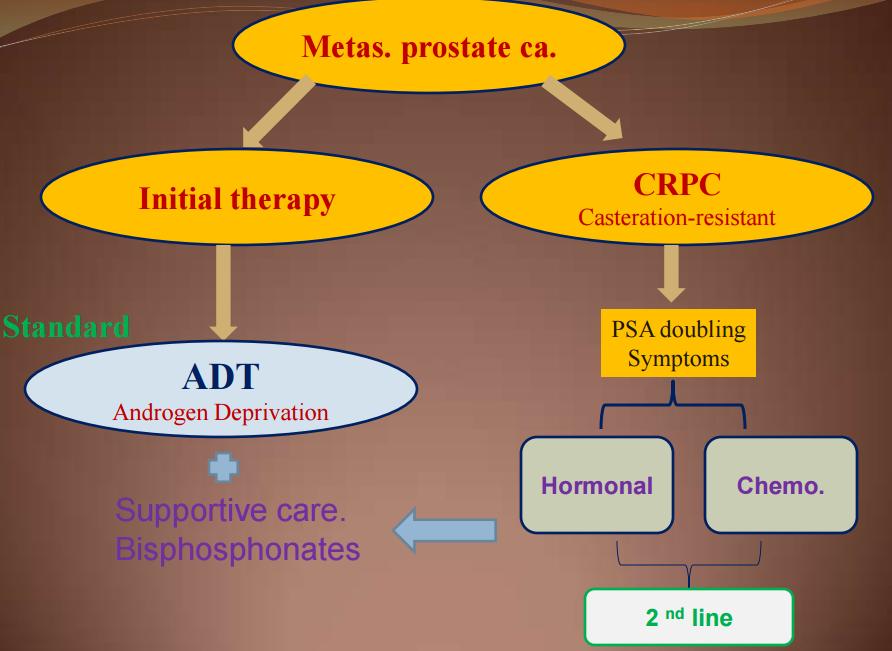
6 Treatment Mainstay: androgen suppression. It is a pallia&ve tool, no cure. Results of treatment: median progression- free survival = months overall survival = months All pa&ents develop hormone- refractory disease. Take in considera&on the toxic effects of treatment.
7
8 Androgen depriva&on therapy Aim à Testosterone < 50 ng/dl Surgical castra&on by Bilateral orchiectomy Medical castra&on 1. LHRH agonist: (e.g. goserelin, leuprolide) ( + oral an&androgen 7 days to avoid testosterone flare) 2. LHRH antagonist. (e.g. degarelix ) 3. CAB: combined androgen blockade: LHRH agonist + oral an&androgen
9 Androgen depriva&on therapy Pa&ents who do not show an adequate suppression of serum testosterone (< 50 ng/dl) may be considered for CAB Monotherapy of nonsteroidal an&androgens are less effec&ve but are associated with fewer hot flashes and fa&gue and do not impair libido If hormone therapy fails, that therapy should be con&nued into and through the next hormone manipula&on. Recent data showed that CAB is not superior to LHRH agonists alone in treatment of metasta&c PCa.
10 Luteneising- hormone- releasing hormone agonists: Therapy with LHRH analogs may induce medical castra&on by suppressing LH produc&on These agonists can poten&ally cause a transient surge of LH when therapy is ini&ated before the LH levels fall (flare phenomenon) LHRH agonists are offered in 1mo, 3mo, and once- yearly depots; it is necessary to pre- medicate with an&androgen to prevent flare up phenomenon Leuprolide: 7.5 mg IM monthly or 22.5 mg IM every 3ms or 30 mg IM every 4ms or 45 mg IV every 6ms. Histrelin: one 50mg implant SC every 12ms ; con&nue therapy un&l disease progression. Goserelin: 3.6 mg implant SC monthly or a 10.8 mg implant SC every 3ms. Triptorelin: 3.75 mg IM monthly or mg IM every 3mo or 22.5 mg IM every 6ms.
11 Luteneising- hormone- releasing hormone antagonists: Pure LHRH antagonists suppress testosterone and avoid the flare phenomenon associated with GnRH agonists. Degarelix: 120 mg SC x 2 doses (i.e. 2 separate injec&ons totaling 240 mg), and then, azer 28 days, begin monthly maintenance dose of 80mg SC.
12 Nonsteroidal an&androgens: An&androgens bind to androgen receptors and compe&&vely inhibit their interac&on with testosterone and dihydrotestosterone These agents do not decrease LH levels and androgen produc&on An&androgens are usually used in combina&on with a GnRH agonist in order to prevent a disease flare caused by the transient increase in testosterone levels. Flutamide 250 mg PO TID. Bicalutamide 50 mg PO daily; pa&ents refractory to other an&androgen agents may start with 150 mg PO daily. Nilutamide 300 mg PO daily for 30 days, and then 150 mg PO daily.
13 IntermiEent vs con&nuous ADT SWOG TRIAL, negm 2013 Metasta&c PCa 7 months induc&on ADT PSA 4 IntermiEent vs con&nuous SURVIVAL RESULTS ARE INCONCLUSIVE According to NCCN guidelines: You can consider intermieent ADT when the adverse effects of ADT is a maeer
14 Adverse effect of ADT Hot flushes Osteoporosis Fractures Obesity Insulin resistance DM Altera&on in lipids Cardiovascular dis.

15 Castrate resistant prostate cancer CRPC
16 Castrate resistant prostate cancer CRPC
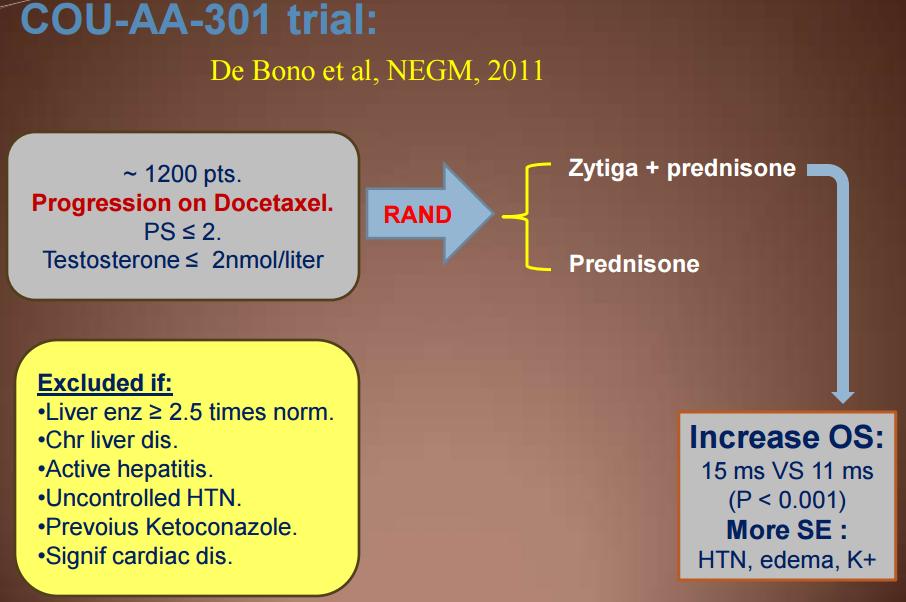
17 Secondary hormonal therapy Abiraterone Acetate ( Zy&ga 250 mg tab) Enzalutamide ( Xtandi 40 mg caps)

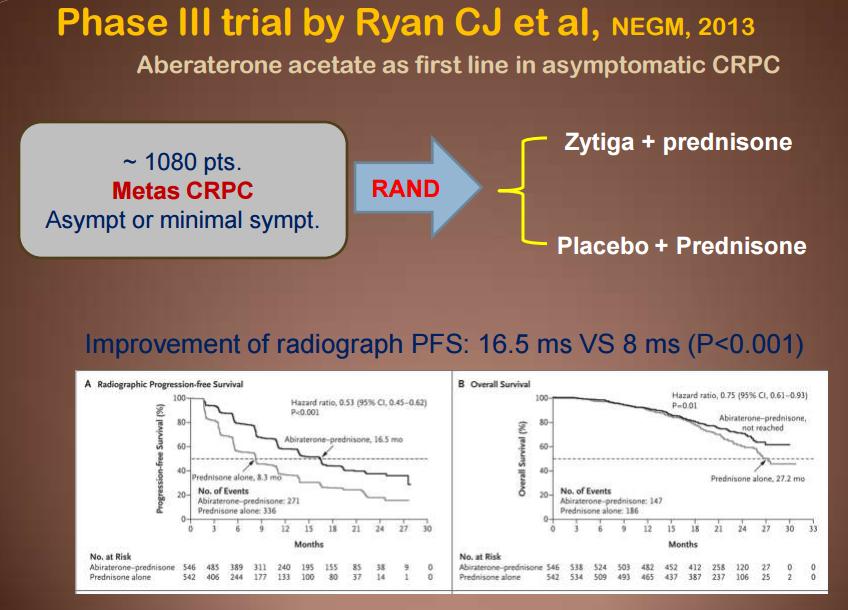
18 Abiraterone acetate 4 tabs once daily, on empty stomach. Androgen synthesis inhibitor To be taken with prednisone tab (5mg 1 x 2). FDA approval as first line therapy in asympto&c CRPC and as second line therapy azer failure of Docetaxel. Precau&ons: Monitor liver func.ons, K+, Phosphorus / month Monitor Bld pressure / month. Most common S.E: Fa&gue, back/joint pain, peripheral edema., HTN Serious S.E: hepa&c, cardiac and electrolytes
19

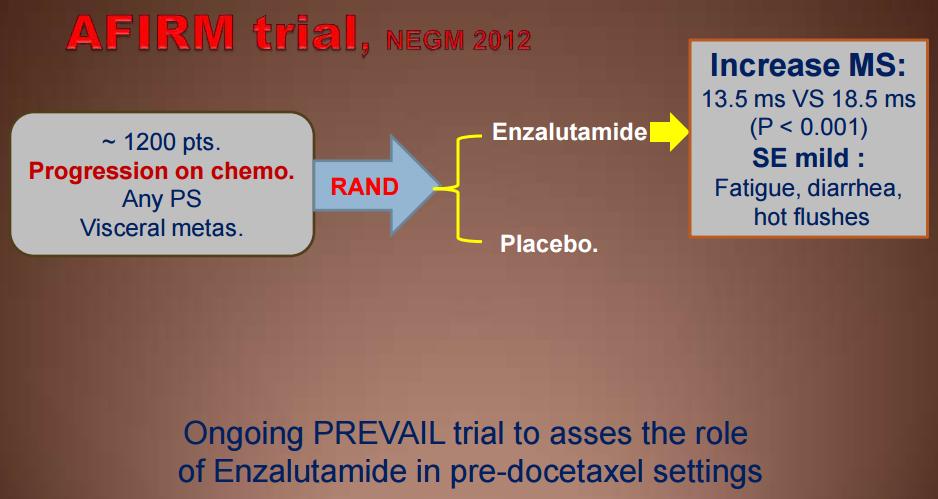
20 Enzalutamide An&- androgen: Inhibit signaling of androgen receptor at mul&ple levels. Dose: 4 caps once daily, +/- food. Not necessary to take prednisone with it. Could be used in pts with poor PS. Less S.E than Abiraterone. Given with GnRH agonists. Seroius S.E: Seizures. (0.6 %)
21 Sipuleucel- T Immunotherapy Provenge : IV over 60 min / 2 weeks x 3 cycles. Autologous cancer vaccine 1) Collect blood from pt. 2) Separate APC (Ag- presen&ng cells) 3) Exposure to (PAP- GM- CSF recombinant fusion gene) ; prosta&c acid phosphatase 4) Re- infuse in the same pa&ent.
22
23 Who are the candidates to Sipuleucel- T Metasta&c CRPC. First line in asymptoma&c or minimally symptoma&c pts. Good PS. Life expectancy > 6 months. No visceral metastasis. Resulted in 22% reduc&on in mortality when compared to placebo in a phase III trial, which was published by Kantoff PW et al, NEGM Common S.E: chills. pyrexia and headache.

24 RADIUM- 223 Xofigo alpha par&cle- emixng radioac&ve therapeu&c agent (half life~11 day) I.V injec&on over 1 min. Every 4 weeks X 6 cycles. Dose: 1.35 micro- curie/ Kg. Given for symptoma&c CRPC + bone mets without visceral mets S.E: ( 10%) were nausea/vomi&ng and peripheral edema Hematologic laboratory abnormali&es ( 10%) were anemia, lymphocytopenia, leukopenia, thrombocytopenia, and neutropenia


25 ALSYMPCA, NEGM 2013
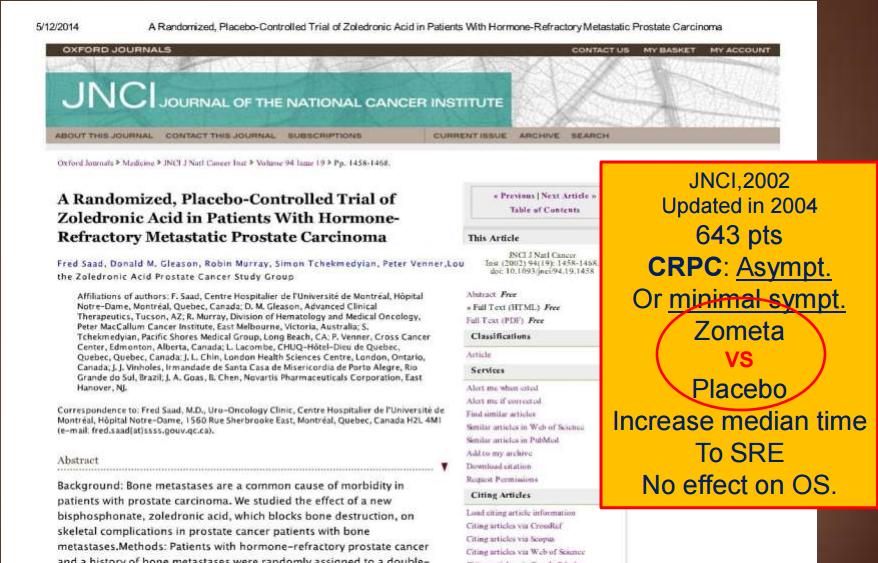
26 Bone health in metasta&c PCa ADT associated with 20-50% rela&ve increase of fracture risk. ADT decrease bone menial density. Longer treatment dura&on greater fracture risk. NCCN recommenda,ons: (with ADT) Supplemental Calcium (1200 mg daily) + vit- D (1000 IU daily). Base line DEXA scan then annually. Denosumab: 60 mg / 6 months : phase III trial in non- metasta&c PCa showed that Denosumab increase bone mineral density by 6.7% and reduces the risk of fracture ( from 3.9% to 1.5%); Smith MR et al, NEGM 2009; 361(8): Or Zoledronic acid (5mg/12 ms).
27
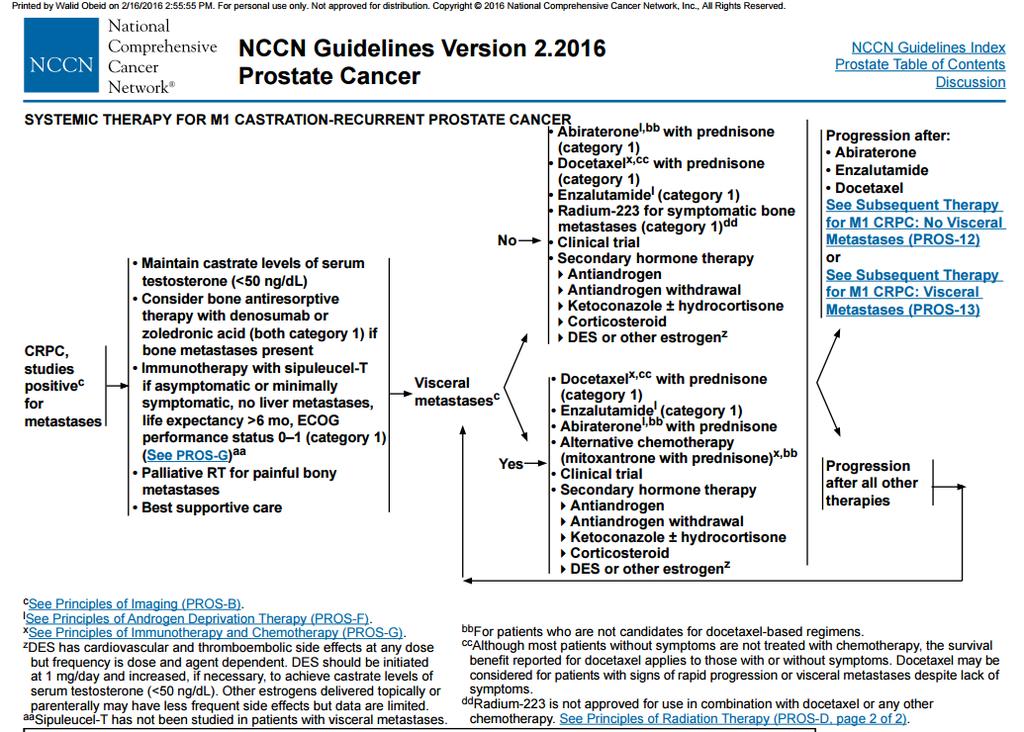
28 Algorithm in mcrpc

29 Cross resistance between new therapies
30 Treatment Sequencing: Post STAMPEDE results
31 Art of sequencing Based on the concept that more treatments => increased survival 2 philosophical approaches: Give the less toxic agent first Give the more toxic agent first
32 Tenta&ve decision tree Metasta&c CRPC Short response (<1 year) to 1st- line ADT High Gleason score (>=8) High Volume mets Or rapidly progressive/aggressive disease Or previous Abiraterone/Enzalutamide Or AR- V7 posi&ve (if available) Poor predicted response to further hormonal therapy (including abiraterone/enzalutamide) Indica&on for chemotherapy (Docetaxelà Cabazitaxel)

33 Mul& disciplinary approach
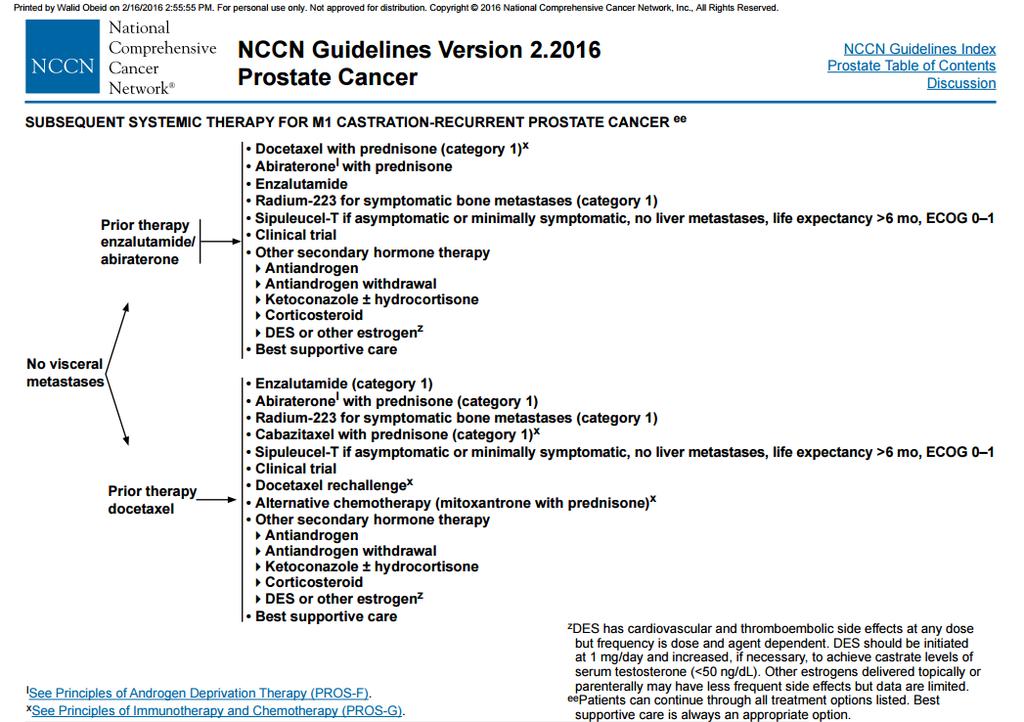
34 Second Line Therapy Definitely depends on previous treatments
35
36


37 Cabazitaxel Marketed as JEVTANA Semi- synthe&c taxane deriva&ve Dose: 25 mg/m2 over 1 hour / 3weeks. AZer failure of Docetaxel.
38 Meta- analysis of 10 retrospec&ve studies
39 Conclusions Management of metasta&c prostate cancer is rapidly evolving..poten&al change in paradigm New drugs in development: need to move to a tailored therapy The most appropriate sequencing of these new agents remains to be determined and chemotherapy remains a valid treatment op&on in mcrpc
40
41
42
43
44
45 RESOURCES AUA GUIDELINES 2015 EAU GUIDELINES 2016 NCNN GUIDELINES 2016 NEJM
46 Ques&on 1 The desired Castrate testosterone levels is 1. Less than 10 ng/dl 2. Less than 20 ng/dl 3. Less than 50 ng/dl 4. More than 20 ng/dl 5. More than 50 ng/dl
47 Ques&on 2 All these are side effects of ADT but one 1. Hot flashes 2. Osteoporosis 3. Obesity 4. Headache 5. Insulin resistance
48 Ques&on 3 Enzalutamide is a : hydroxylase inhibitor lyase inhibitor 3. Novel an,- androgen 4. Type of chemotherapy 5. Given intravenously
49 Ques&on 4 Sipuleucel- T is given to pa&ents with all the above except: 1. Metasta&c CRPC. 2. First line in asympto&c or minimally symptoma&c pts. 3. Poor PS. 4. Life expectancy > 6 months. 5. No visceral metastasis.
50 Ques&on 5 According to EAU guidelines, in M1 pa&ents an&- androgen short- term administra&on is recommended 1. Started prior to LHRH agonist treatment ini&a&on 2. Started with LHRH agonist treatment ini,a,on 3. Started 1 week post LHRH agonist ini&a&on 4. Not necessary with LHRH agonists
51 Ques&on 6 Which of these products was shown to improve OS in pa&ents with CRPC: 1. Zoledronic acid 2. Denosumab 3. Radium Steroids
52 Ques&on 7 Radiographic progression in prostate cancer: 1. More than 1 new lesion on follow up bone scan 2. More than 2 new lesions on follow up bone scan 3. More than 3 new lesions on follow up bone scan 4. More than 4 new lesions on follow up bone scan
53 Ques&on 8 Concerning con&nuous vs intermieent ADT- pick the correct answer 1. Survival results are inconclusive 2. IntermiEent ADT showed improved survival 3. Con&nuous ADT showed improved survival 4. Side effects increase with intermieent therapy
54 Ques&on 9 STAMPEDE trial: Docetaxel plus standard therapy improved overall survival by an average of 10 months in men with newly diagnosed, hormone- naive, advanced prostate cancer. 1. TRUE 2. FALSE
55 Ques&on 10 Factors favoring early chemotherapy with docetaxel 1. High volume disease 2. Gleason <8 3. PSA- DT >10 months 4. Response to ADT for more than 12 months
56 THANK YOU
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD
 Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Metastatic prostate carcinoma. Lee Say Bob July 2017
 Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
LUNCH AND LEARN. April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology
 LUNCH AND LEARN April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology Medical Therapy for Prostate Cancer Androgen (testosterone) is required for the growth of both normal prostate and prostate cancers
LUNCH AND LEARN April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology Medical Therapy for Prostate Cancer Androgen (testosterone) is required for the growth of both normal prostate and prostate cancers
Con$nuing Care for Your Pa$ents with Metasta$c CRPC
 27 th Annual InternaAonal Prostate Cancer Symposium Update January 26, 2017 Con$nuing Care for Your Pa$ents with Metasta$c CRPC Michael S. Cookson, MD, MMHC Professor and Chair Department of Urology University
27 th Annual InternaAonal Prostate Cancer Symposium Update January 26, 2017 Con$nuing Care for Your Pa$ents with Metasta$c CRPC Michael S. Cookson, MD, MMHC Professor and Chair Department of Urology University
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
 www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC)
") Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
ERLEADA (apalutamide) oral tablet
 oral tablet") ERLEADA (apalutamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ERLEADA (apalutamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy).
.") Thanks to: The Medical Educator Consortium Luis Raez, MD, Florida International University 15th ed. Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy). Mayer Fishman,
Thanks to: The Medical Educator Consortium Luis Raez, MD, Florida International University 15th ed. Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy). Mayer Fishman,
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일
 New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Advanced Prostate Cancer
 Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Prostate Cancer 2009 MDV Anti-Angiogenesis. Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy. Docetaxel/Epothilone
 Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Francesco Bertoldo. Metabolic Bone Diseases and Osteoncology Unit DRUG INDUCED S OSTEOPOROSIS: ANDROGEN DEPRIVATION THERAPY
 DRUG INDUCED S OSTEOPOROSIS: ANDROGEN DEPRIVATION THERAPY Francesco Bertoldo Metabolic Bone Diseases and Osteoncology Unit Department of Medicine University di Verona EPIDEMIOLGY OF PROSTATE CANCER Prostate
DRUG INDUCED S OSTEOPOROSIS: ANDROGEN DEPRIVATION THERAPY Francesco Bertoldo Metabolic Bone Diseases and Osteoncology Unit Department of Medicine University di Verona EPIDEMIOLGY OF PROSTATE CANCER Prostate
SAMPLE ONLY. Your Health Matters. Advanced Prostate Cancer and its Treatment A Patient Guide. Please order from Documents and Media: 415/
 Your Health Matters Advanced Prostate Cancer and its Treatment A Patient Guide UCSF Genitourinary Medical Oncology Program Charles Ryan, MD, UCSF Patient Advocates Please order from Documents and Media:
Your Health Matters Advanced Prostate Cancer and its Treatment A Patient Guide UCSF Genitourinary Medical Oncology Program Charles Ryan, MD, UCSF Patient Advocates Please order from Documents and Media:
Summary of Phase 3 IMPACT Trial Results Presented at AUA Meeting Webcast Conference Call April 28, Nasdaq: DNDN
 Summary of Phase 3 IMPACT Trial Results Presented at AUA Meeting Webcast Conference Call April 28, 2009 Nasdaq: DNDN PROVENGE sipuleucel-t is an autologous active cellular immunotherapy that activates
Summary of Phase 3 IMPACT Trial Results Presented at AUA Meeting Webcast Conference Call April 28, 2009 Nasdaq: DNDN PROVENGE sipuleucel-t is an autologous active cellular immunotherapy that activates
Clinical Management Guideline for Planning and Treatment. The process to be followed when a course of chemotherapy is required to treat:
 Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Cardiovascular Effects of ADT in
 Cardiovascular Effects of ADT in Click to edit Prostate Master Cancer /tle style Pa/ents Chris Plummer Freeman Hospital, Newcastle upon Tyne, UK Newcastle University Bri/sh Cardio- Oncology Society Click
Cardiovascular Effects of ADT in Click to edit Prostate Master Cancer /tle style Pa/ents Chris Plummer Freeman Hospital, Newcastle upon Tyne, UK Newcastle University Bri/sh Cardio- Oncology Society Click
Philip Kantoff, MD Dana-Farber Cancer Institute
 CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
Strategic decisions for systemic treatment. metastatic castration resistant prostate cancer (mcrpc)
") Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Initial hormone therapy (and more) for metastatic prostate cancer
 for metastatic prostate cancer") Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
PROSTATE CANCER HORMONE THERAPY AND BEYOND. Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute
 PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
The Role of the Medical Oncologist in the Treatment of Prostate Cancer. Alireza saadat hematologist and oncologist
 The Role of the Medical Oncologist in the Treatment of Prostate Cancer Alireza saadat hematologist and oncologist When should you see an oncologist? High risk localized disease Rising PSA after local therapy
The Role of the Medical Oncologist in the Treatment of Prostate Cancer Alireza saadat hematologist and oncologist When should you see an oncologist? High risk localized disease Rising PSA after local therapy
NCCN Guidelines for Prostate Cancer V Web teleconference 06/17/16 and 06/30/17
 Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Clinical Policy: Enzalutamide (Xtandi) Reference Number: CP.CPA.203 Effective Date: Last Review Date: 02.19
 Reference Number: CP.CPA.203 Effective Date: Last Review Date: 02.19") Clinical Policy: (Xtandi) Reference Number: CP.CPA.203 Effective Date: 11.16.16 Last Review Date: 02.19 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Xtandi) Reference Number: CP.CPA.203 Effective Date: 11.16.16 Last Review Date: 02.19 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Patients Living Longer: The Promise of Newer Therapies
 Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
Review of the Stampede Results. Charles Ryan MD University of California San Francisco
 Review of the Stampede Results Charles Ryan MD University of California San Francisco Se#ng and hypothesis Se
Review of the Stampede Results Charles Ryan MD University of California San Francisco Se#ng and hypothesis Se
Index Patients 3& 4. Guideline Statements 10/11/2014. Enzalutamide Reduced the Risk of Death
 //4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
//4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
17/07/2014. Prostate Cancer Watchful Waiting New Treatments Andrew Williams Urologist and Urological Oncologist ADHB, CMDHB and 161 Gillies Ave, Epsom
 My Biases Prostate Cancer Watchful Waiting New Treatments Andrew Williams Urologist and Urological Oncologist ADHB, CMDHB and 161 Gillies Ave, Epsom I am a member of the specialist group of the Prostate
My Biases Prostate Cancer Watchful Waiting New Treatments Andrew Williams Urologist and Urological Oncologist ADHB, CMDHB and 161 Gillies Ave, Epsom I am a member of the specialist group of the Prostate
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer
 Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Treatment of Advanced Prostate Cancer
 Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer. Dr. Simon Yu Nov 18, 2017
 GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
New Treatment Options for Prostate Cancer
 New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
Cancer de la prostate métastatique: prise en charge précoce
 Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy
 Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Second line hormone therapies. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
8/31/ ) Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases
 Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases") Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
ASCO 2012 Genitourinary tumors
 ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223
 SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia
 Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia 5-year prostate cancer specific survival rates have improved from 67% to 99% between 1974 and 2000 Excellent survival
Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia 5-year prostate cancer specific survival rates have improved from 67% to 99% between 1974 and 2000 Excellent survival
Management of Prostate Cancer
 Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Lower Baseline PSA Predicts Greater Benefit From Sipuleucel-T
 Lower Baseline PSA Predicts Greater Benefit From Sipuleucel-T Schelhammer PF, Chodak G, Whitmore JB, Sims R, Frohlich MW, Kantoff PW. Lower baseline prostate-specific antigen is associated with a greater
Lower Baseline PSA Predicts Greater Benefit From Sipuleucel-T Schelhammer PF, Chodak G, Whitmore JB, Sims R, Frohlich MW, Kantoff PW. Lower baseline prostate-specific antigen is associated with a greater
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey
 Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC
 Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Suthan Chanthawong. B. Pharm, BCP, BCOP. Faculty of Pharmaceutical Sciences, Khon Kaen University
 Suthan Chanthawong B. Pharm, BCP, BCOP Faculty of Pharmaceutical Sciences, Khon Kaen University Objectives 1) Outline appropriate screening and prevention strategy. 2) Describe appropriate patient-specific
Suthan Chanthawong B. Pharm, BCP, BCOP Faculty of Pharmaceutical Sciences, Khon Kaen University Objectives 1) Outline appropriate screening and prevention strategy. 2) Describe appropriate patient-specific
Medical management in locally advanced and metastatic prostate cancer: Does changes in treatment policy have any specific effect on PSA levels?
 ORIGINAL PAPER DOI: 10.4081/aiua.2017.4.282 Medical management in locally advanced and metastatic prostate cancer: Does changes in treatment policy have any specific effect on PSA levels? Murat Bagcioglu
ORIGINAL PAPER DOI: 10.4081/aiua.2017.4.282 Medical management in locally advanced and metastatic prostate cancer: Does changes in treatment policy have any specific effect on PSA levels? Murat Bagcioglu
majority of the patients. And taking an aggregate of all trials, very possibly has a modest effect on improved survival.
 Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes
 Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Prostate Cancer: Vision of the Future By: H.R.Jalalian
 1 H. R. Jalalian Hematologist&Oncologist Baqiyatallah University of Medical Sciences 2 State of the art: vision on the future Diagnosis Surgery Radiotherapy Medical Oncology 3 Early Detection PSA sensitivity
1 H. R. Jalalian Hematologist&Oncologist Baqiyatallah University of Medical Sciences 2 State of the art: vision on the future Diagnosis Surgery Radiotherapy Medical Oncology 3 Early Detection PSA sensitivity
Androgen Deprivation Therapy Its impact and the nursing role. Jane Thacker Uro-Oncology Nurse Specialist
 Androgen Deprivation Therapy Its impact and the nursing role Jane Thacker Uro-Oncology Nurse Specialist Overview of content To gain an understanding of ADT (androgendeprivation therapy) and why and how
Androgen Deprivation Therapy Its impact and the nursing role Jane Thacker Uro-Oncology Nurse Specialist Overview of content To gain an understanding of ADT (androgendeprivation therapy) and why and how
Sequencing treatment for metastatic prostate cancer
 11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
MAMTA PARIKH, MD, MS CHALLENGING CASE #2: GU CANCER & STATE OF THE ART: CASTRATION RESISTANT PROSTATE CANCER
 MAMTA PARIKH, MD, MS CHALLENGING CASE #2: GU CANCER & STATE OF THE ART: CASTRATION RESISTANT PROSTATE CANCER NO RELEVANT FINANCIAL RELATIONSHIPS IN THE PAST TWELVE MONTHS BY PRESENTER OR SPOUSE/PARTNER.
MAMTA PARIKH, MD, MS CHALLENGING CASE #2: GU CANCER & STATE OF THE ART: CASTRATION RESISTANT PROSTATE CANCER NO RELEVANT FINANCIAL RELATIONSHIPS IN THE PAST TWELVE MONTHS BY PRESENTER OR SPOUSE/PARTNER.
Joelle Hamilton, M.D.
 Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Management Options in Advanced Prostate Cancer: What is the Role for Sipuleucel-T?
 Clinical Medicine Insights: Oncology Consise Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Management Options in Advanced Prostate Cancer: What is
Clinical Medicine Insights: Oncology Consise Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Management Options in Advanced Prostate Cancer: What is
ADT vs chemo + ADT as initial treatment for advanced prostate cancer
 ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
Castrate resistant prostate cancer: the future of anti-androgens.
 Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
Updates on Use of Radiopharmaceu3cals in Clinical Trials August 22, 2017
 Updates on Use of Radiopharmaceu3cals in Clinical Trials August 22, 2017 Evan Y. Yu, M.D. Professor of Medicine (Oncology) University of Washington Fred Hutchinson Cancer Research Center Discussion Topics
Updates on Use of Radiopharmaceu3cals in Clinical Trials August 22, 2017 Evan Y. Yu, M.D. Professor of Medicine (Oncology) University of Washington Fred Hutchinson Cancer Research Center Discussion Topics
Bone Metastases and Mortality: Can We Be Doing More?
 Bone Metastases and Mortality: Can We Be Doing More? Leonard G. Gomella, MD Chairman, Department of Urology President Society of Urologic Oncology Sidney Kimmel Cancer Center Thomas Jefferson University
Bone Metastases and Mortality: Can We Be Doing More? Leonard G. Gomella, MD Chairman, Department of Urology President Society of Urologic Oncology Sidney Kimmel Cancer Center Thomas Jefferson University
Marketing Authorisation Holder Applicant Invented name. Route of administration. Content (concentration) Member State. l form
 Member State. l form") ANNEX I LIST OF THE NAMES, PHARMACEUTICAL FORM, STRENGTH OF THE MEDICINAL PRODUCT, ROUTE OF ADMINISTRATION, APPLICANT AND MARKETING AUTHORISATION HOLDER IN THE MEMBER STATES 1 Member State Marketing Authorisation
ANNEX I LIST OF THE NAMES, PHARMACEUTICAL FORM, STRENGTH OF THE MEDICINAL PRODUCT, ROUTE OF ADMINISTRATION, APPLICANT AND MARKETING AUTHORISATION HOLDER IN THE MEMBER STATES 1 Member State Marketing Authorisation
Saad et al [12] Metastatic CRPC. Bhoopalam et al [14] M0 PCa on ADT <1 yr vs >1 yr ADT
![Saad et al [12] Metastatic CRPC. Bhoopalam et al [14] M0 PCa on ADT <1 yr vs >1 yr ADT](/thumbs/71/65630457.jpg "Saad et al [12] Metastatic CRPC. Bhoopalam et al [14] M0 PCa on ADT <1 yr vs >1 yr ADT") Evolution of Treatment Options for Patients with and Bone Metastases Trials of Treatments for Castration-Resistant Prostrate Cancer Mentioned in This Review Bisphosphonates (Zometa) 4 mg IV 8 mg IV ( to
Evolution of Treatment Options for Patients with and Bone Metastases Trials of Treatments for Castration-Resistant Prostrate Cancer Mentioned in This Review Bisphosphonates (Zometa) 4 mg IV 8 mg IV ( to
The Role of Immunotherapy in Prostate Cancer: What s Trending?
 The Role of Immunotherapy in Prostate Cancer: What s Trending? Douglas G. McNeel, MD, PhD University of Wisconsin Carbone Cancer Center Madison, Wisconsin Prostate cancer rationale for immune therapies
The Role of Immunotherapy in Prostate Cancer: What s Trending? Douglas G. McNeel, MD, PhD University of Wisconsin Carbone Cancer Center Madison, Wisconsin Prostate cancer rationale for immune therapies
New Pharmacotherapies in the Treatment of Advanced Prostate Cancer
 Clinical Medicine Insights: Urology Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. New Pharmacotherapies in the Treatment of Advanced Prostate Cancer
Clinical Medicine Insights: Urology Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. New Pharmacotherapies in the Treatment of Advanced Prostate Cancer
PCa Commentary. " Clinical Update New Information on Topics Presented in Earlier. Volume 78 November December 2012 CLINICAL UPDATE: ALPHARADIN
 1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2480 www.seattleprostate.com PCa Commentary Volume 78 November December 2012 Content Page Alpharadin 1 Degarelix 2 MDV3100 4 MRI 4 Aspirin 6 "
1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2480 www.seattleprostate.com PCa Commentary Volume 78 November December 2012 Content Page Alpharadin 1 Degarelix 2 MDV3100 4 MRI 4 Aspirin 6 "
Risk of renal side effects with ADT. E. David Crawford University of Colorado, Aurora, CO, USA
 Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer*
 Chinese-German J Clin Oncol DOI 10.1007/s10330-014-0037-9 September 2014, Vol. 13, No. 9, P417 P421 Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer* Abeer
Chinese-German J Clin Oncol DOI 10.1007/s10330-014-0037-9 September 2014, Vol. 13, No. 9, P417 P421 Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer* Abeer
C. Stephen Farmer, II MD Urology Associates
 C. Stephen Farmer, II MD Urology Associates Benign Prostate Hypertrophy Benign Prostate Hypertrophy Symptoms Hesitancy Intermittency Nocturia Post-void dribbling Dysuria Urgency Frequency Hematuria Benign
C. Stephen Farmer, II MD Urology Associates Benign Prostate Hypertrophy Benign Prostate Hypertrophy Symptoms Hesitancy Intermittency Nocturia Post-void dribbling Dysuria Urgency Frequency Hematuria Benign
This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository:
 This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: http://orca.cf.ac.uk/103187/ This is the author s version of a work that was submitted to / accepted
This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: http://orca.cf.ac.uk/103187/ This is the author s version of a work that was submitted to / accepted
Two late stage clinical programs
 Safe harbor This presentation and our remarks based upon it, including responses to questions made during and following the presentation, may include forward-looking statements. Such statements are subject
Safe harbor This presentation and our remarks based upon it, including responses to questions made during and following the presentation, may include forward-looking statements. Such statements are subject
פ א ר מ ה P H A R x M A
 פ א ר מ ה P H A R x M A הביטאון לענייני תרופות ותראפיה ISRAEL DRUG BULLETIN Vol. 19, Bulletin No. 107 June-July 2012 Also in the Bulletin: Degarelix for Advanced Hormone-Dependent Prostate Cancer NEW TREATMENT
פ א ר מ ה P H A R x M A הביטאון לענייני תרופות ותראפיה ISRAEL DRUG BULLETIN Vol. 19, Bulletin No. 107 June-July 2012 Also in the Bulletin: Degarelix for Advanced Hormone-Dependent Prostate Cancer NEW TREATMENT
Personalized ADT. Thomas Keane MD
 Personalized ADT Thomas Keane MD Conflicts Ferring Tolemar Bayer Astellas myriad Personalized ADT for the Specific Pa@ent Cardiac Obesity and testosterone Fsh High volume metasta@c disease Docetaxol Significant
Personalized ADT Thomas Keane MD Conflicts Ferring Tolemar Bayer Astellas myriad Personalized ADT for the Specific Pa@ent Cardiac Obesity and testosterone Fsh High volume metasta@c disease Docetaxol Significant
Novel treatment for castration-resistant prostate cancer
 Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
CME Baseline Curriculum Report
 CME Baseline Curriculum Report October 14, 2010 For CME Activity: Managing Advanced Prostate Cancer in the Community Setting: A Case-based Curriculum Supported by an independent educational grant from
CME Baseline Curriculum Report October 14, 2010 For CME Activity: Managing Advanced Prostate Cancer in the Community Setting: A Case-based Curriculum Supported by an independent educational grant from
Perspective on endocrine and chemotherapy agents. Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
PRO STATE of the art. METASTATIC HORMONE SENSITIVE PROSTATE CANCER Clinical case and evidences from literature
 PRO STATE of the art METASTATIC HORMONE SENSITIVE PROSTATE CANCER Clinical case and evidences from literature Marcello Tucci, MD Department of Oncology San Luigi Gonzaga Hospital Orbassano, Turin 30 MAY
PRO STATE of the art METASTATIC HORMONE SENSITIVE PROSTATE CANCER Clinical case and evidences from literature Marcello Tucci, MD Department of Oncology San Luigi Gonzaga Hospital Orbassano, Turin 30 MAY
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC
 Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Advanced Therapeutic Strategies in the Successful Management of Patients with Castrate Resistant Prostate Cancer (CRCP)
") Advanced Therapeutic Strategies in the Successful Management of Patients with Castrate Resistant Prostate Cancer (CRCP) Pamela Ellsworth, MD Professor of Urology Vice Chair Department of Urology UMassMemorial
Advanced Therapeutic Strategies in the Successful Management of Patients with Castrate Resistant Prostate Cancer (CRCP) Pamela Ellsworth, MD Professor of Urology Vice Chair Department of Urology UMassMemorial