Pancreatic intraglandular metastasis predicts poorer outcome in postoperative patients with pancreatic
|
|
|
- Rosamond Victoria Woods
- 5 years ago
- Views:
Transcription
1 Pancreatic intraglandular metastasis predicts poorer outcome in postoperative patients with pancreatic ductal carcinoma Seiji Oguro, MD * +, Kazuaki Shimada, MD, PhD, Yoshinori Ino, PhD *, Minoru Esaki, MD, PhD, Satoshi Nara, MD, Yoji Kishi, MD, PhD, Tomoo Kosuge, MD, PhD +, Yae Kanai, MD, PhD *, Nobuyoshi Hiraoka, MD, PhD * *Division of Molecular Pathology, National Cancer Center Research Institute, Tokyo, Hepatobiliary and Pancreatic Surgery Division, National Cancer Center Hospital, Tokyo +Juntendo University Graduate School of Medicine, Tokyo Correspondence to: Nobuyoshi Hiraoka, MD, PhD Division of Molecular Pathology, National Cancer Center Research Institute Tsukiji, Chuo-ku, Tokyo , Japan TEL: FAX: nhiraoka@ncc.go.jp Conflicts of interest and source of funding: This work was supported by a Grant-in-Aid for Third Term Comprehensive 10-year Strategy for Cancer Control from the Ministry of Health, Labor and Welfare of Japan (NH) and the National Cancer Center Research and Development Fund (NH). All authors have nothing to disclose any potential conflicts (financial, professional, or personal). 1
2 Abstract: Intra-organ metastasis of a primary cancer within the organ of origin, such as intrahepatic metastasis of hepatocellular carcinoma, is one of the key features for clinicopathological staging of the cancer. Pancreatic intraglandular metastasis (P-IM) of pancreatic ductal carcinoma (PDC) is encountered occasionally, but has not yet been evaluated. The aim of this study was to investigate the clinicopathological characteristics and prognostic value of P-IM in patients with PDC. The histopathological features of 393 consecutive patients with PDC who had undergone pancreatic resection at the National Cancer Center Hospital, Tokyo, between 2003 and 2010 were reviewed. For the purposes of the study, P-IM was defined as an independent tumor showing histopathological features similar to those of the primary one. Twenty-six cases of P-IM were identified in 21 (5.3%) of the reviewed patients. The incidence of P-IM at each stages of the TNM classification was 0% (0/7) at stage IA, 17% (1/6) at stage IB, 5% (5/92) at stage IIA, 4% (11/252) at stage IIB, 0% (0/1) at stage III, and 11% (4/35) at stage IV. Univariate survival analysis showed that both overall survival (OS) and disease-free survival (DFS) for patients with P-IM were significantly shorter than for those without P-IM (P <0.001 and P = 0.019, respectively). Multivariate survival analysis showed that P-IM was significantly correlated with shorter OS (P = 0.002; HR = 2.239; 95% CI: ). Our findings suggest that the presence of P-IM in patients with PDC is an independent prognosticator and may represent aggressive tumor behavior. Keywords: intraglandular metastasis, pancreas, ductal carcinoma, prognosis 2
3 Introduction Pancreatic cancer is the fourth and fifth leading cause of cancer death in the United States(1) and Japan,(2) respectively. Most patients with pancreatic ductal carcinoma (PDC) present late with locoregional advanced disease or metastatic dissemination, and the overall 5-year survival rate for such patients is <5%.(1) Even for patients whose tumors are resectable and who receive adjuvant chemotherapy, the 5-year survival rate is still as low as 20%.(3) This is partly because of a high incidence of subclinical metastasis, which is not detectable by radiological imaging, at the time of diagnosis and surgery. Multiplicity of a malignant tumor in any organ is caused by intra-organ metastasis and/or multiple primary tumors. A malignant tumor with intra-organ metastasis is likely to be at an advanced stage. For example, in lung cancer, an additional tumor nodule with a histological appearance identical to that of the dominant, primary tumor is regarded as intrapulmonary metastasis, which indicates poorer prognosis and is a determinant of T factor and M factor in the Union for International Cancer Control (UICC) TNM classification.(4) Likewise, liver cancer with intrahepatic metastasis is classified as multiple tumors and assigned a higher T factor.(4) Among patients with hepatocellular carcinoma (HCC), it has been reported that those with intrahepatic metastasis have significantly poorer survival than those with multicentric occurrence.(5) Sometimes such additional tumor nodules in the pancreas are revealed by histopathological examination in cases of pancreatic ductal carcinoma (PDC), a feature known as pancreatic intraglandular metastasis (P-IM).(6) Similarly to intrahepatic metastasis of HCC and intrapulmonary metastasis of lung cancer, P-IM is assumed to be of clinicopathological importance in patients with PDC. However, no study has yet assessed the characteristics and clinicopathological significance of P-IM, and its incidence, pathogenesis, and impact on prognosis remain unknown. The aim of the present study was to investigate the clinicopathological characteristics and prognostic impact of P-IM, for which purpose we reviewed the histopathological features of 393 consecutive cases of PDC with reference to the corresponding clinicopathological data. 3
4 Materials and methods Study population Clinical and pathological data were obtained through a detailed retrospective review of the medical records of all 393 consecutive patients with PDC who had undergone initial surgical resection between January 2003 and December 2010 at the National Cancer Center Hospital, Japan. None of the patients had received any previous therapy. The surgical procedures for pancreatic resection comprised 258 pancreatoduodenectomies with or without resection of the pylorus ring, 117 distal pancreatectomies, and 18 total pancreatectomies; regional lymph node dissection was performed in all cases. All of the patients included in this study underwent macroscopic curative resection, which was defined as the macroscopic removal of all gross tumors without liver metastases, macroscopic peritoneal dissemination, bulky lymph node involvement, or apparent tumor invasion around the common hepatic or superior mesenteric arteries. Peritoneal washing cytology was routinely performed just after laparotomy, though positive peritoneal cytology was not regarded as a contraindication for surgery. Ninety-three patients (24%) received intraoperative radiotherapy. All of the cases were conventional PDC; adenocarcinomas originating in intraductal papillary mucinous neoplasms or mucinous cystic neoplasms were excluded, as were secondary tumors and post-neoadjuvant cases. Tumors were staged according to the UICC TNM classification(4) as follows: stage IA (n = 7, 1.8%), IB (n = 6, 1.5%), IIA (n = 92, 23.4%), IIB (n = 252, 64.1%), III (n=1, 0.3%), and IV (n = 35, 8.9%). One patient with stage III disease had PDC involving the celiac artery and underwent distal pancreatectomy with celiac axis resection. All patients with Stage IV disease were diagnosed on the basis of paraaortic lymph node involvement. Patients were closely followed up every 1 to 2 months during the first year after surgery. Each follow-up visit included a physical examination, blood chemistry tests, and measurement of serum carbohydrate antigen 19-9 (CA19-9) and carcinoembryonic antigen. Ultrasonography and enhanced computed tomography were performed every 3 4
5 months. Recurrence was diagnosed when a new local or distant metastatic lesion was found on imaging studies or an increase in tumor marker levels with deterioration of the patient's general condition was recognized. The follow-up period was calculated from the date of surgery to the last day of follow-up. The median follow-up period was 20.5 ( ) months for the patients overall: 164 patients (41.7%) were alive, 197 (50.1%) died because of pancreatic cancer and 32 (8.2%) died of other causes. During the study period, adjuvant chemotherapy was not performed routinely. One hundred twenty four patients received adjuvant chemotherapy in a randomized clinical trial setting or at the discretion of the attending physician. This study was approved by the Institutional Review Board of the National Cancer Center, Tokyo. Written informed consent was obtained from all participants involved in this study and all clinical investigations were conducted according to the principles expressed in the Declaration of Helsinki. Pathological examination All of the ductal carcinomas were reexamined pathologically and classified according to the World Health Organization classification,(7) the UICC TNM classification(4) and the Japan Pancreas Society (JPS) Classification of Pancreatic Carcinoma.(8) Surgically resected specimens were fixed in 10% formalin and cut into serial slices 5 mm thick, horizontally in the pancreas head, and sagittally in the pancreas body and tail. All of these sections were then subjected to detailed pathological examination after staining with hematoxylin and eosin. The following histopathological variables were evaluated according to the JPS classification:(8) tumor margin status, nerve plexus invasion, and lymphatic, venous, and intrapancreatic neural invasion. The grading of the latter four factors is as follows: 0; no invasion, 1; slight invasion, 2; moderate invasion, and 3; marked invasion. For evaluation of venous invasion and intraductal tumor spread, tissue sections were stained for elastic fibers. To investigate lymphatic invasion, we also performed immunohistochemistry for podoplanin, 5
6 which is a specific marker of lymphatic vessels. Immunohistochemical analysis was performed on formalin-fixed, paraffin-embedded tissue sections as mentioned previously,(9) using an antibody against podoplanin (D2-40, 1:100, DAKO, Glostrup, Denmark). The size of the P-IM and its distance from the primary tumor to the P-IM were measured. Pancreatic intraepithelial neoplasm (PanIN)-3 is sometimes difficult to distinguish from intraepithelial spread of invasive carcinoma in pancreatic ducts or ductules. In order to detect multicentric tumors with certainty, we defined solitary PanIN-3 as a PanIN-3 lesion separated from any invasive carcinoma and located within the pancreas in each case, the size of the lesion was measured, as well as its distance from the dominant, primary invasive carcinoma. Criteria for identifying P-IM We defined P-IM with reference to the definitions of intrahepatic metastasis of HCC(10) and intrapulmonary metastasis of lung cancer.(11) When multiple invasive PDCs were detected in the specimen, we defined as P-IM those additional tumors that met all of the following conditions: (i) located within the pancreatic parenchyma and separated from the dominant, primary tumor by a distance of 5 mm or more; (ii) showing a histological appearances identical to that of the dominant, primary tumor; (iii) differentiated to the same degree or less than the dominant, primary tumor; (iv) unaccompanied by premalignant lesions of PDC such as PanIN and intraductal papillary-mucinous neoplasm, implying that the tumors might be other primaries arising through multicentric carcinogenesis. To confirm discontinuity between P-IM and the premalignant lesions, we considered an invasive lesion to be separated from PanIN-3 or non-invasive IPMN with high-grade dysplasia by a distance of 5 mm or more. Intraepithelial spread of the invasive carcinoma in pancreatic ducts or ductules, i.e. so-called cancerization of ducts, was also excluded. Because at our institution resected specimens are cut into serial slices 5 mm thick, a distance of 5 mm from the main lesion was employed in order to confirm discontinuity. A representative 6
7 case of P-IM is shown in Figure 1. Statistical analysis Chi-squared analysis or the Fisher exact test was used to compare categorical data. The postoperative overall survival (OS) rate and disease-free survival (DFS) rate were calculated by the Kaplan Meier method. Univariate analysis was performed for prognostic factors using the log-rank test. The factors found to be significant by univariate analysis were subjected to multivariate analysis using the Cox proportional hazards model (backward elimination method). Differences at P <0.05 were considered statistically significant. Statistical analyses were performed using the Statistical Package for the Social Sciences (version 20.0, SPSS Inc., Chicago, IL, USA). Results Characteristics of P-IM Twenty-six P-IMs were identified in 21 (5.3%) of the 393 patients. None of the P-IMs had been detected by preoperative radiological imaging or intraoperative examination using ultrasonography, and was identified postoperatively for the first time by microscopic examination. Table 1 shows the pathological features of the P-IMs and the primary tumors. The incidence of P-IM at each stages of the TNM classification was 0% (0/7) at stage IA, 17% (1/6) at stage IB, 5% (5/92) at stage IIA, 4% (11/252) at stage IIB, 0% (0/1) at stage III, and 11% (4/35) at stage IV. One patient had 3 P-IM lesions, 3 patients had 2, and the other patients had 1 P-IM lesion each. The maximum size of the P-IM ranged from 1 to 10 mm with a median of 3.0 mm and an average of 3.4 mm, and the distance from the primary tumor to the P-IM ranged from 5 to 25 mm with a median of 10.5 mm and an average of 12.3 mm. Lymphatic invasion, venous invasion, and intrapancreatic neural invasion within the P-IM were detected in 35% (9/26), 62% (16/26), and 12% (3/26) of the lesions, respectively. 7
8 Forty-one of the solitary PanIN-3 lesions were identified in 24 (6.1%) of the patients. One solitary PanIN-3 lesion was detected in 18 of the patients, two lesions in two, three lesions in two, five lesions in one, and eight lesions in one. The average, median, and range of lesion size were 4.58 mm, 2 mm, and <1 to 20 mm, respectively. The average, mean and range of distance between the solitary PanIN-3 and the dominant invasive carcinoma was 19.5 mm, 15 mm, and 5 to 60 mm, respectively. One case involving two overt invasive primary PDCs was found at surgery. Correlation of P-IM with clinicopathological parameters Table 2 shows the correlation of P-IM with clinicopathological characteristics of the patients with PDC. No significant relationship was found. Prognostic significance of the presence of P-IM The median survival time for patients having PDC with and without P-IM was 16 months and 29 months, respectively. The one-year survival rates for patients having PDC with and without P-IM were 59% and 83%, respectively; the 2-year rates were 18% and 57%, and the 5-year rates were 0% and 27%, respectively. Univariate survival analysis demonstrated an association between the presence of P-IM and shorter OS (P <0.001; HR = 2.427; 95% CI: ) and DFS (P = 0.019; HR = 1.762; 95% CI: ) (Figures 2 A and 2B). For stages IA/IB/IIA and stage IIB, OS for patients with P-IM was significantly shorter than for those without P-IM (P = and P = 0.019, respectively) (Figure 3). All the recurrences (n = 18) in patients having P-IM involved peritoneal dissemination or distant metastasis, rather than local recurrence in the remnant pancreas. Multivariate Cox regression analysis showed that P-IM (P = 0.002; HR = 2.239; 95% CI: ), tumor size, pathologic node status, histological grade, intrapancreatic neural invasion, peritoneal 8
9 cytology, and adjuvant chemotherapy were independent predictors of OS, and that preoperative CA 19-9 level, tumor size, pathologic node status, pathologic metastasis status, histological grade, venous invasion, intrapancreatic neural invasion, and peritoneal cytology were independent predictors of DFS (Table 3). In addition, the relationship between P-IM size and survival was analyzed among the patients with P-IM, but no significant correlation was found. Similarly, there was no significant correlation between survival and the distance from the primary tumor to P-IM. There were no significant differences in the proportions of patients undergoing intraoperative radiotherapy and adjuvant chemotherapy between those with P-IM and those without P-IM. Four (19%) of 21 patients with P-IM underwent intraoperative radiotherapy, while 89 (24%) of 372 patients without P-IM did so (P = 0.609). Nine (43%) of 21 patients with P-IM underwent adjuvant chemotherapy, while 115 (31%) of 372 patients without P-IM did so (P = 0.252). In addition, among the patients with P-IM, there was no significant difference in OS and DFS between those who underwent intraoperative radiotherapy and those who did not, as well as between those who underwent adjuvant chemotherapy and those who did not. Discussion When multiple tumors are detected in a single organ in the absence of any primary tumors in other organs, two possibilities can be considered. One is a primary tumor with intra-organ metastatic lesions, and the other is the development of multiple primary tumors in the organ. Although some types of tumor often show intra-organ metastasis, details of its clinicopathological characteristics have been investigated only for lung cancer and HCC. Such studies have revealed that patients with intra-organ metastases have poorer prognosis,(12-14) and the presence of intra-organ metastasis has been used as one of the critical factors for estimation of disease stage.(4, 10) However, no reported study has yet assessed intraglandular metastasis in patients with PDC. In the present study, we defined P-IM in patients with PDC and 9
10 evaluated its characteristics and prognostic significance. We found that P-IM was a prognostic factor indicative of shorter OS (P = 0.002; HR = 2.239; 95% CI: ) in patients with PDC (Table 3). P-IM was found not only at an advanced disease stage, but also at relatively early stages, the incidence of P-IM being 17% (1/6) at stage IB, 5% (5/92) at stage IIA, 4% (11/252) at stage IIB, and 11% (4/35) at stage IV (Table 1). Moreover, the patients in stages IA/IB/IIA and stage IIB with P-IM had significantly shorter survival than those without (Figure 3). The outcome of patients with P-IM at stages IIB and IV was dismal, and among them, no patient surviving for more than 3 years has yet been confirmed. These findings suggest that PDC with P-IM has an aggressive nature. P-IMs were found in 21 (5.3%) of the 393 cases of PDC we studied; 24 (6.1%) of the cases involved solitary PanIN-3. In our series, multicentric tumors other than the dominant, primary invasive tumor were P-IM or solitary PanIN-3, showing almost the same incidence. The incidence of P-IM in this study may have been underestimated for two reasons. One was that P-IM located within 5 mm from the primary tumor was excluded on the basis of our criteria because continuity between the primary tumor and P-IM could not be assessed with certainty. The other was that most of the surgical procedures employed were not total pancreatectomy, but pancreaticoduodenectomy or distal pancreatectomy, meaning that any P-IM located in the remnant pancreas could not be assessed. Several studies have reported that the incidence of multiple pancreatic cancers in resected specimens ranges from 5% to 20%.(15-17) However, they did not mention whether the entire specimen was examined histopathologically, whether the multiple tumors were invasive, or whether the multiple tumors were P-IM or multicentric primary tumors. The present study has provided some insight into how P-IM forms. For intrapulmonary metastasis of lung cancer, three possible mechanisms have been postulated: tumor cells spread via the lymphatic vessels, via blood vessels, or via the airway.(12) Intrahepatic metastasis of HCC is thought to develop through tumor cell dispersal via the portal vein or systemic circulation.(13, 14) Two routes for the formation of P-IM are possible: lymphatic and venous. PDC can spread via both of these two routes to form 10
11 P-IM, since venous and lymphatic invasion in the area of P-IM were observed in 62% and 35% of cases with P-IM, respectively. In conclusion, our findings indicate that the presence of P-IM in patients with PDC is an independent prognosticator and could represent aggressive tumor behavior. Acknowledgments The authors thank Dr. Hidenori Ojima for useful discussion and Ms. Rie Yamazaki-Itoh and Ms. Keiko Gomisawa for technical assistance. 11
12 References 1. Siegel R, Ward E, Brawley O, et al. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin. 2011;61: Ministry of Health Labour and Welfare. Vital Statistics Japan Neoptolemos JP, Stocken DD, Friess H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med. 2004;350: Sobin LH, Gospodarowicz MK, Wittekind C. TNM Classification of Malignant Tumors. New York: Wiley-Blackwell; Arii S, Monden K, Niwano M, et al. Results of surgical treatment for recurrent hepatocellular carcinoma; comparison of outcome among patients with multicentric carcinogenesis, intrahepatic metastasis, and extrahepatic recurrence. J Hepatobiliary Pancreat Surg. 1998;5: Hruban RH, Pitman MB, Klimstra DS, et al. Tumors of the pancreas. Washington, D.C. : American Registry of Pathology in collaboration with the Armed Forces Institute of Pathology; Hruban RH, Boffetta P, Hiraoka N. Pancreas. In: Bosman FT, Carneiro F, Hruban RH, et al., eds. WHO Classification of Tumours of the Digestive System. Lyon: IARC Press; 2010: Japan Pancreas Society. Classification of Pancreatic Cancer. Tokyo, Japan: Kanehara; Takahashi Y, Akishima-Fukasawa Y, Kobayashi N, et al. Prognostic value of tumor architecture, tumor-associated vascular characteristics, and expression of angiogenic molecules in pancreatic endocrine tumors. Clin Cancer Res. 2007;13: Liver Cancer Study Group of Japan. General Rules for the Clinical and Pathological Study of Primary Liver Cancer. Tokyo, Japan: Kanehara; Wittekind C. TNM Supplement: A commentary on uniform use. Oxford: Wiley-Blackwell; Urschel JD, Urschel DM, Anderson TM, et al. Prognostic implications of pulmonary satellite nodules: are the 1997 staging revisions appropriate? Lung Cancer. Ireland; 1998:83-87; discussion
13 13. Sakon M, Nagano H, Nakamori S, et al. Intrahepatic recurrences of hepatocellular carcinoma after hepatectomy: analysis based on tumor hemodynamics. Arch Surg. 2002;137: Mitsunobu M, Toyosaka A, Oriyama T, et al. Intrahepatic metastases in hepatocellular carcinoma: the role of the portal vein as an efferent vessel. Clin Exp Metastasis. 1996;14: Tanaka M. Pancreatic Cancer Registry Report Suizo. 2007;22:e Tryka AF, Brooks JR. Histopathology in the evaluation of total pancreatectomy for ductal carcinoma. Ann Surg. 1979;190: Ihse I, Lilja P, Arnesjo B, et al. Total pancreatectomy for cancer. An appraisal of 65 cases. Ann Surg. 1977;186:
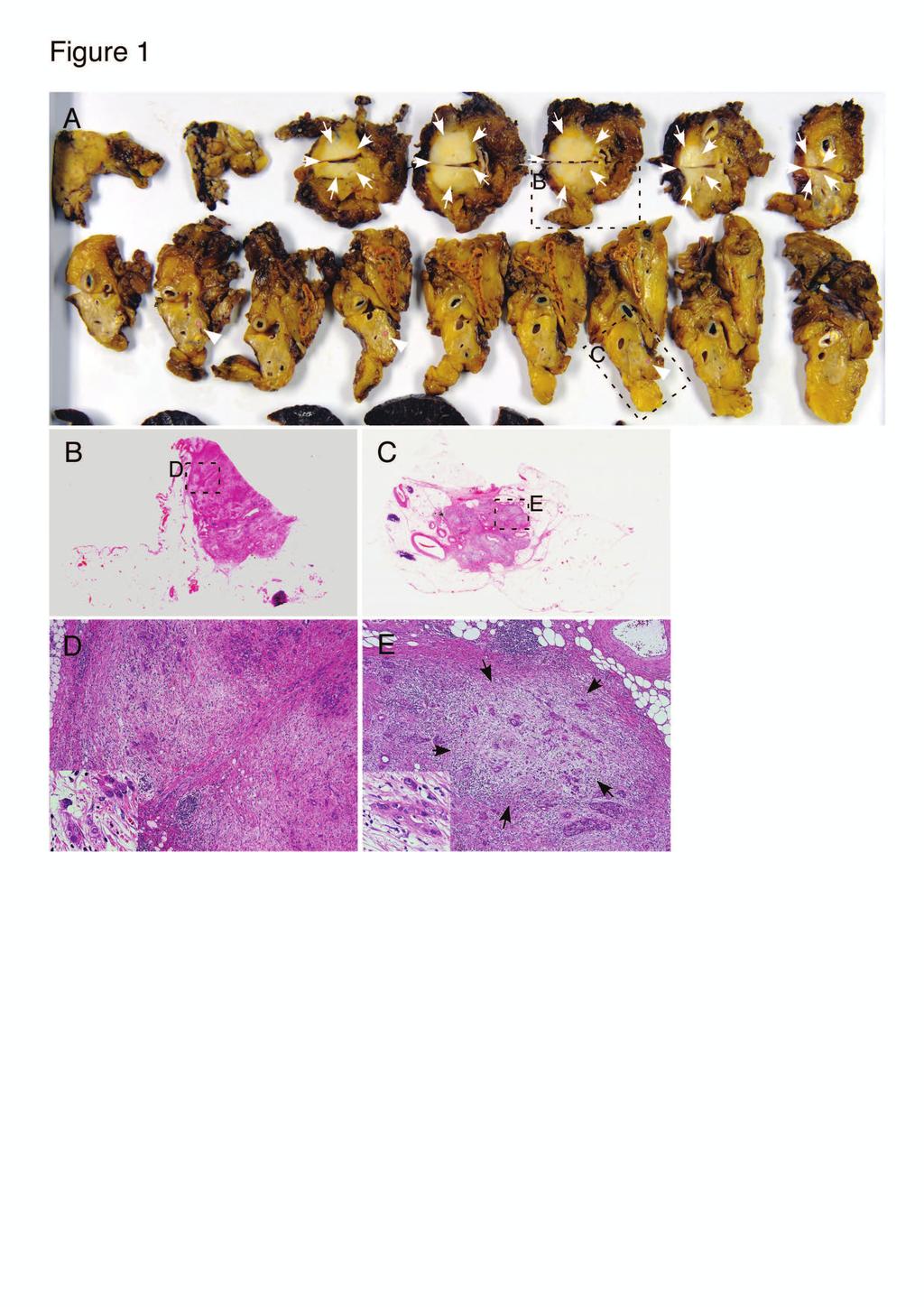
14 Figure legends Figure 1 A representative case of P-IM with the primary tumor (case 4). A, Cut surface of a formalin-fixed specimen. The specimen resected by distal pancreatectomy was cut sagittally into serial slices 5 mm thick and each of the sections are lined in order from the pancreatic body to the tail from the left to lower right of the figure. Three lesions of P-IM (lower column, red circle indicated by arrow heads) are separated from a primary ductal adenocarcinoma of the pancreas body (white arrows). B and C, Loupe view of the primary tumor (B) and P-IM (C). B and C correspond to the rectangle in A, respectively. D and E, Histological features of the primary tumor (D) and P-IM (E). Poorly differentiated adenocarcinoma infiltrated into the pancreatic parenchyma with a marked desmoplastic reaction. The similar features are evident in both the primary tumor and the P-IM. D and E correspond to the rectangles in B and C, respectively. Black arrows indicate the P-IM in E. D and E are low-power views and insets in D and E are high-power views. Figure 2 Kaplan-Meier survival curves showing a comparison of overall survival (A) and disease-free survival (B) between patients with and without P-IM. P-values were obtained by log-rank test. Figure 3 Kaplan-Meier survival curves showing a comparison of overall survival (left column) and disease-free survival (right column) between patients with and without P-IM at each of the TNM stages. The total numbers of patients at stage IA/IB/IIA, IIB, and IV were 105, 252, and 35, respectively. P-values were obtained by log-rank test. 14
15 Table1. Pathological findings of P-IM with the primary tumor Primary tumor P-IM Case Age Sex Stage * Location Size (mm) Histological grade ly à v à ne à Number of P-IM Size (mm) Distance from the primary tumor (mm) Direction from the primary tumor Histological grade ly v ne 1 82 M IB Ph 44 G cranial G F IIA Ph 15 G caudal G M IIA Ph 34 G left G M IIA Pb 25 G left G left G left G M IIA Pb 35 G left G F IIA Pb 30 G left G M IIB Ph 18 G cranial G caudal G M IIB Ph 32 G caudal G caudal G M IIB Ph 35 G caudal G M IIB Ph 20 G caudal G M IIB Ph 30 G caudal G M IIB Ph 35 G ventral G M IIB Ph 114 G left G M IIB Ph 37 G left G M IIB Ph 30 G left G F IIB Phb 78 G left G M IIB Pb 35 G left G M IV Ph 50 G caudal G caudal G F IV Ph 40 G caudal G M IV Ph 28 G caudal G F IV Pb 31 G left G * Classified according to UICC TNM classification Classified according to the World Health Organization classification ly: Lymphatic invasion, v: Venous invasion, ne: intrapancreatic neural invasion à Classified according to the classification of the pancreatic carcinoma of Japan Pancreas Society (0: no invasion, 1: slight invasion, 2: moderate invasion, 3: marked invasion) Classified as presence (+) or absence (-) of tumor invasion.
16 Table 2. Correlation of P-IM with clinicopathological variables in patients with PDC Characteristics P-IM Presence Absence Age (years) < Sex Male Female Location Pancreas head Pancreas body or tail Preoperative CA 19-9 level (median 138 U/ml) No. of Patients <138 U/ml U/ml Tumor size (mm) < Pathologic tumor status T1, T T3, T Pathologic node status N N Pathologic metastasis status M M Stage IA, IB, IIA IIB, III, IV Tumor histological grade G G2 or G Nerve plexus invasion* 0, , Lymphatic invasion* 0, , Venous invasion* 0, , Intrapancreatic neural invasion* 0, , Surgical margin status Negative Positive Peritoneal cytology Negative Positive *Classified according to the classification of pancreatic carcinoma of Japan Pancreas Society. (0: no invasion, 1: slight invasion, 2: moderate invasion, 3: marked invasion) P- value
17 Table 3. Univariate and multivariate analysis of P-IM as a prognostic factor associated with overall survival in patients with pancreatic ductal carcinoma (n=393) Variables Univariate analysis Multivariate analysis HR(95% CI) P- value HR(95% CI) P- value Age ( 65 years/ <65 years) 0.978( ) Gender (male/ female) ( ) Location (pancreas head/ body, tail) ( ) Preoperative CA 19-9 level ( 138/ <138 U/ml) ( ) <0.001 Size ( 30 mm/ <30 mm) ( ) < ( ) <0.001 Pathologic tumor status (T3, T4/ T1, T2) ( ) Pathologic node status (N1/ N0) ( ) < ( ) Pathologic metastasis status (M1/ M0) ( ) Histological grade (G2, G3/ G1) ( ) ( ) Nerve plexus invasion (2, 3/ 0, 1)* ( ) <0.001 Lymphatic invasion (2, 3/ 0, 1)* ( ) Venous invasion (2, 3/ 0, 1)* ( ) <0.001 Intrapancreatic neural invasion (2, 3/ 0, 1)* ( ) < ( ) Surgical margin status (positive/ negative) ( ) <0.001 Peritoneal cytology (positive/ negative) ( ) < ( ) <0.001 Adjuvant chemotherapy (performed/ not performed) ( ) ( ) P-IM (presence/ absence) ( ) < ( ) Univariate and multivariate analysis of P-IM as a prognostic factor associated with disease-free survival in patients with pancreatic ductal carcinoma (n=393) Variables Univariate analysis Multivariate analysis HR(95% CI) P- value HR(95% CI) P- value Age ( 65 years/ <65 years) ( ) Gender (male/ female) ( ) Location (pancreas head/ body, tail) ( ) 0.03 Preoperative CA 19-9 level ( 138/ <138 U/ml) ( ) < ( ) <0.001 Size ( 30 mm/ <30 mm) ( ) < ( ) Pathologic tumor status (T3, T4/ T1, T2) ( ) Pathologic node status (N1/ N0) ( ) < ( ) Pathologic metastasis status (M1/ M0) ( ) < ( ) Histological grade (G2, G3/ G1) ( ) ( ) Nerve plexus invasion (2, 3/ 0, 1)* ( ) <0.001 Lymphatic invasion (2, 3/ 0, 1)* ( ) <0.001 Venous invasion (2, 3/ 0, 1)* ( ) < ( ) Intrapancreatic neural invasion (2, 3/ 0, 1)* ( ) < ( ) <0.001 Surgical margin status (positive/ negative) ( ) <0.001 Peritoneal cytology (positive/ negative) ( ) < ( ) <0.001 Adjuvant chemotherapy (performed/ not performed) ( ) P-IM (presence/ absence) ( ) *Classified according to the classification of pancreatic carcinoma of Japan Pancreas Society. Statistically significant in bold values.
18
19
20
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study
 Original article Annals of Gastroenterology (2013) 26, 346-352 Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study Subhankar Chakraborty
Original article Annals of Gastroenterology (2013) 26, 346-352 Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study Subhankar Chakraborty
Topics: Staging and treatment for pancreatic cancer. Staging systems for pancreatic cancer: Differences between the Japanese and UICC systems
 M. J Hep Kobari Bil Pancr and S. Surg Matsuno: (1998) Staging 5:121 127 system for pancreatic cancer 121 Topics: Staging and treatment for pancreatic cancer Staging systems for pancreatic cancer: Differences
M. J Hep Kobari Bil Pancr and S. Surg Matsuno: (1998) Staging 5:121 127 system for pancreatic cancer 121 Topics: Staging and treatment for pancreatic cancer Staging systems for pancreatic cancer: Differences
p53 expression in invasive pancreatic adenocarcinoma and precursor lesions
 Malaysian J Pathol 2011; 33(2) : 89 94 ORIGINAL ARTICLE p53 expression in invasive pancreatic adenocarcinoma and precursor lesions NORFADZILAH MY MBBCH,* Jayalakshmi PAILOOR MPath, FRCPath,* RETNESWARI
Malaysian J Pathol 2011; 33(2) : 89 94 ORIGINAL ARTICLE p53 expression in invasive pancreatic adenocarcinoma and precursor lesions NORFADZILAH MY MBBCH,* Jayalakshmi PAILOOR MPath, FRCPath,* RETNESWARI
Peritoneal Involvement in Stage II Colon Cancer
 Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
ORIGINAL ARTICLE. Helical Computed Tomography in the Diagnosis of Portal Vein Invasion by Pancreatic Head Carcinoma
 ORIGINAL ARTICLE Helical Computed Tomography in the Diagnosis of Portal Vein Invasion by Pancreatic Head Carcinoma Usefulness for Selecting Surgical Procedures and Predicting the Outcome Hiroyoshi Furukawa,
ORIGINAL ARTICLE Helical Computed Tomography in the Diagnosis of Portal Vein Invasion by Pancreatic Head Carcinoma Usefulness for Selecting Surgical Procedures and Predicting the Outcome Hiroyoshi Furukawa,
Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers
 日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
Citation American Journal of Surgery, 196(5)
") NAOSITE: Nagasaki University's Ac Title Author(s) Multifocal branch-duct pancreatic i neoplasms Tajima, Yoshitsugu; Kuroki, Tamotsu Amane; Adachi, Tomohiko; Mishima, T Kanematsu, Takashi Citation American
NAOSITE: Nagasaki University's Ac Title Author(s) Multifocal branch-duct pancreatic i neoplasms Tajima, Yoshitsugu; Kuroki, Tamotsu Amane; Adachi, Tomohiko; Mishima, T Kanematsu, Takashi Citation American
Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules
 Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules YASUHIRO ITO, TAKUYA HIGASHIYAMA, YUUKI TAKAMURA, AKIHIRO MIYA, KAORU KOBAYASHI, FUMIO MATSUZUKA, KANJI KUMA
Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules YASUHIRO ITO, TAKUYA HIGASHIYAMA, YUUKI TAKAMURA, AKIHIRO MIYA, KAORU KOBAYASHI, FUMIO MATSUZUKA, KANJI KUMA
Enrollment Form: Pancreas
 Tissue Source Site (TSS) Name: TSS Identifier: _ TSS Unique Patient #: Completed By: Completion Date (MM/DD/YYYY): Form Notes: An Enrollment Form should be completed for each TCGA qualified case upon qualification
Tissue Source Site (TSS) Name: TSS Identifier: _ TSS Unique Patient #: Completed By: Completion Date (MM/DD/YYYY): Form Notes: An Enrollment Form should be completed for each TCGA qualified case upon qualification
PAPER. Experience With 208 Resections for Intraductal Papillary Mucinous Neoplasm of the Pancreas
 PAPER Experience With 0 Resections for Intraductal Papillary Mucinous Neoplasm of the Pancreas Thomas Schnelldorfer, MD; Michael G. Sarr, MD; David M. Nagorney, MD; Lizhi Zhang, MD; Thomas C. Smyrk, MD;
PAPER Experience With 0 Resections for Intraductal Papillary Mucinous Neoplasm of the Pancreas Thomas Schnelldorfer, MD; Michael G. Sarr, MD; David M. Nagorney, MD; Lizhi Zhang, MD; Thomas C. Smyrk, MD;
Histologic Characteristics Enhance Predictive Value of American Joint Committee on Cancer Staging in Resectable Pancreas Cancer
 Original Article Histologic Characteristics Enhance Predictive Value of American Joint Committee on Cancer Staging in Resectable Pancreas Cancer James Helm, MD, PhD 1,2,3,4,5 ; Barbara A. Centeno, MD 3,6,7
Original Article Histologic Characteristics Enhance Predictive Value of American Joint Committee on Cancer Staging in Resectable Pancreas Cancer James Helm, MD, PhD 1,2,3,4,5 ; Barbara A. Centeno, MD 3,6,7
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas.
 Protocol applies to all carcinomas of the exocrine pancreas.") Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Lung cancer pleural invasion was recognized as a poor prognostic
 Visceral pleural invasion classification in non small cell lung cancer: A proposal on the basis of outcome assessment Kimihiro Shimizu, MD a Junji Yoshida, MD a Kanji Nagai, MD a Mitsuyo Nishimura, MD
Visceral pleural invasion classification in non small cell lung cancer: A proposal on the basis of outcome assessment Kimihiro Shimizu, MD a Junji Yoshida, MD a Kanji Nagai, MD a Mitsuyo Nishimura, MD
Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer?
 Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer? Lee H, Park JY, Youn S, Kwon W, Heo JS, Choi SH, Choi DW Department of Surgery, Samsung Medical Center Sungkyunkwan
Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer? Lee H, Park JY, Youn S, Kwon W, Heo JS, Choi SH, Choi DW Department of Surgery, Samsung Medical Center Sungkyunkwan
Significance of the lymph nodes in the 7th station in rational dissection for metastasis of distal gastric cancer with different T categories
 Original Article Significance of the lymph nodes in the 7th station in rational dissection for metastasis of distal gastric cancer with different T categories Wu Song, Yulong He, Shaochuan Wang, Weiling
Original Article Significance of the lymph nodes in the 7th station in rational dissection for metastasis of distal gastric cancer with different T categories Wu Song, Yulong He, Shaochuan Wang, Weiling
Predictive factors for invasive intraductal papillary mucinous neoplasm of the pancreas
 Korean J Hepatobiliary Pancreat Surg 2011;15:27-22 Original Article Predictive factors for invasive intraductal papillary mucinous neoplasm of the pancreas Dae Young Jun 1, Hyung Jun Kwon 2, Sang Geol
Korean J Hepatobiliary Pancreat Surg 2011;15:27-22 Original Article Predictive factors for invasive intraductal papillary mucinous neoplasm of the pancreas Dae Young Jun 1, Hyung Jun Kwon 2, Sang Geol
Visceral pleural involvement (VPI) of lung cancer has
 of lung cancer has") Visceral Pleural Involvement in Nonsmall Cell Lung Cancer: Prognostic Significance Toshihiro Osaki, MD, PhD, Akira Nagashima, MD, PhD, Takashi Yoshimatsu, MD, PhD, Sosuke Yamada, MD, and Kosei Yasumoto,
Visceral Pleural Involvement in Nonsmall Cell Lung Cancer: Prognostic Significance Toshihiro Osaki, MD, PhD, Akira Nagashima, MD, PhD, Takashi Yoshimatsu, MD, PhD, Sosuke Yamada, MD, and Kosei Yasumoto,
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Modified primary tumour/vessel tumour/nodal tumour classification for patients with invasive ductal carcinoma of the breast
 British Journal of Cancer (2011) 105, 698 708 All rights reserved 0007 0920/11 www.bjcancer.com Modified primary tumour/vessel tumour/nodal tumour classification for patients with invasive ductal carcinoma
British Journal of Cancer (2011) 105, 698 708 All rights reserved 0007 0920/11 www.bjcancer.com Modified primary tumour/vessel tumour/nodal tumour classification for patients with invasive ductal carcinoma
Concurrent Analysis of Human Equilibrative Nucleoside Transporter 1 and Ribonucleotide
 1 ORIGINAL ARTICLE Concurrent Analysis of Human Equilibrative Nucleoside Transporter 1 and Ribonucleotide Reductase Subunit 1 Expression Increases Predictive Value for Prognosis in Cholangiocarcinoma Patients
1 ORIGINAL ARTICLE Concurrent Analysis of Human Equilibrative Nucleoside Transporter 1 and Ribonucleotide Reductase Subunit 1 Expression Increases Predictive Value for Prognosis in Cholangiocarcinoma Patients
Objectives. Intraoperative Consultation of the Whipple Resection Specimen. Pancreas Anatomy. Pancreatic ductal carcinoma 11/10/2014
 Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Pulmonary resection for lung cancer with malignant pleural disease first detected at thoracotomy
 European Journal of Cardio-Thoracic Surgery 41 (2012) 25 30 doi:10.1016/j.ejcts.2011.04.010 ORIGINAL ARTICLE Pulmonary resection for lung cancer with malignant pleural disease first detected at thoracotomy
European Journal of Cardio-Thoracic Surgery 41 (2012) 25 30 doi:10.1016/j.ejcts.2011.04.010 ORIGINAL ARTICLE Pulmonary resection for lung cancer with malignant pleural disease first detected at thoracotomy
ORIGINAL PAPER. Marginal pulmonary function is associated with poor short- and long-term outcomes in lung cancer surgery
 Nagoya J. Med. Sci. 79. 37 ~ 42, 2017 doi:10.18999/nagjms.79.1.37 ORIGINAL PAPER Marginal pulmonary function is associated with poor short- and long-term outcomes in lung cancer surgery Naoki Ozeki, Koji
Nagoya J. Med. Sci. 79. 37 ~ 42, 2017 doi:10.18999/nagjms.79.1.37 ORIGINAL PAPER Marginal pulmonary function is associated with poor short- and long-term outcomes in lung cancer surgery Naoki Ozeki, Koji
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Characteristics of intramural metastasis in gastric cancer. Tatsuya Hashimoto Kuniyoshi Arai Yuichi Yamashita Yoshiaki Iwasaki Tsunekazu
 ORIGINAL ARTICLE Characteristics of intramural metastasis in gastric cancer Tatsuya Hashimoto Kuniyoshi Arai Yuichi Yamashita Yoshiaki Iwasaki Tsunekazu Hishima Author for correspondence: T. Hashimoto
ORIGINAL ARTICLE Characteristics of intramural metastasis in gastric cancer Tatsuya Hashimoto Kuniyoshi Arai Yuichi Yamashita Yoshiaki Iwasaki Tsunekazu Hishima Author for correspondence: T. Hashimoto
Although the international TNM classification system
 Prognostic Significance of Perioperative Serum Carcinoembryonic Antigen in Non-Small Cell Lung Cancer: Analysis of 1,000 Consecutive Resections for Clinical Stage I Disease Morihito Okada, MD, PhD, Wataru
Prognostic Significance of Perioperative Serum Carcinoembryonic Antigen in Non-Small Cell Lung Cancer: Analysis of 1,000 Consecutive Resections for Clinical Stage I Disease Morihito Okada, MD, PhD, Wataru
Prognostic Role of Gastrectomy in Patients With Gastric Cancer With Positive Peritoneal Cytology
 Int Surg 2014;99:830 834 DOI: 10.9738/INTSURG-D-14-00119.1 Prognostic Role of Gastrectomy in Patients With Gastric Cancer With Positive Peritoneal Cytology Okihide Suzuki, Minoru Fukuchi, Erito Mochiki,
Int Surg 2014;99:830 834 DOI: 10.9738/INTSURG-D-14-00119.1 Prognostic Role of Gastrectomy in Patients With Gastric Cancer With Positive Peritoneal Cytology Okihide Suzuki, Minoru Fukuchi, Erito Mochiki,
Prognostic value of the 8 th tumor-node-metastasis classification for follicular carcinoma and poorly differentiated carcinoma of the thyroid in Japan
 2018, 65 (6), 621-627 ORIGINAL Prognostic value of the 8 th tumor-node-metastasis classification for follicular carcinoma and poorly differentiated carcinoma of the thyroid in Japan Yasuhiro Ito 1), Akira
2018, 65 (6), 621-627 ORIGINAL Prognostic value of the 8 th tumor-node-metastasis classification for follicular carcinoma and poorly differentiated carcinoma of the thyroid in Japan Yasuhiro Ito 1), Akira
Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases
 J Rural Med 2014; 9(1): 20 26 Original article Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases Eiichi Yabata, Masaru Udagawa and Hiroyuki
J Rural Med 2014; 9(1): 20 26 Original article Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases Eiichi Yabata, Masaru Udagawa and Hiroyuki
Lung cancer is a major cause of cancer deaths worldwide.
 ORIGINAL ARTICLE Prognostic Factors in 3315 Completely Resected Cases of Clinical Stage I Non-small Cell Lung Cancer in Japan Teruaki Koike, MD,* Ryosuke Tsuchiya, MD, Tomoyuki Goya, MD, Yasunori Sohara,
ORIGINAL ARTICLE Prognostic Factors in 3315 Completely Resected Cases of Clinical Stage I Non-small Cell Lung Cancer in Japan Teruaki Koike, MD,* Ryosuke Tsuchiya, MD, Tomoyuki Goya, MD, Yasunori Sohara,
Extent of visceral pleural invasion and the prognosis of surgically resected node-negative non-small cell lung cancer
 Thoracic Cancer ISSN 1759-7706 ORIGINAL ARTICLE Extent of visceral pleural invasion and the prognosis of surgically resected node-negative non-small cell lung cancer Yangki Seok 1, Ji Yun Jeong 2 & Eungbae
Thoracic Cancer ISSN 1759-7706 ORIGINAL ARTICLE Extent of visceral pleural invasion and the prognosis of surgically resected node-negative non-small cell lung cancer Yangki Seok 1, Ji Yun Jeong 2 & Eungbae
Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer
 Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Clinicopathologic Characteristics and Prognosis of Gastric Cancer in Young Patients
 Yonago Acta medica 2012;55:57 61 Clinicopathologic Characteristics and Prognosis of Gastric Cancer in Young Patients Hiroaki Saito, Seigo Takaya, Yoji Fukumoto, Tomohiro Osaki, Shigeru Tatebe and Masahide
Yonago Acta medica 2012;55:57 61 Clinicopathologic Characteristics and Prognosis of Gastric Cancer in Young Patients Hiroaki Saito, Seigo Takaya, Yoji Fukumoto, Tomohiro Osaki, Shigeru Tatebe and Masahide
Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer
 498 Original article Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer Authors C. Kunisaki 1, M. Takahashi 2, Y. Nagahori 3, T. Fukushima 3, H. Makino
498 Original article Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer Authors C. Kunisaki 1, M. Takahashi 2, Y. Nagahori 3, T. Fukushima 3, H. Makino
Natural History and Treatment Trends in Hepatocellular Carcinoma Subtypes: Insights From a National Cancer Registry
 2015;112:872 876 Natural History and Treatment Trends in Hepatocellular Carcinoma Subtypes: Insights From a National Cancer Registry PETER L. JERNIGAN, MD, KOFFI WIMA, MS, DENNIS J. HANSEMAN, PhD, RICHARD
2015;112:872 876 Natural History and Treatment Trends in Hepatocellular Carcinoma Subtypes: Insights From a National Cancer Registry PETER L. JERNIGAN, MD, KOFFI WIMA, MS, DENNIS J. HANSEMAN, PhD, RICHARD
Xiang Hu*, Liang Cao*, Yi Yu. Introduction
 Original Article Prognostic prediction in gastric cancer patients without serosal invasion: comparative study between UICC 7 th edition and JCGS 13 th edition N-classification systems Xiang Hu*, Liang
Original Article Prognostic prediction in gastric cancer patients without serosal invasion: comparative study between UICC 7 th edition and JCGS 13 th edition N-classification systems Xiang Hu*, Liang
Pancreatic Cancer. BIOLOGY: Not well defined (genetic and enviromental factors) CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.
 CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.") EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy
 Original Article Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy Shupeng Zhang 1, Liangliang Wu 2, Xiaona Wang 2, Xuewei Ding 2, Han Liang 2 1 Department of General
Original Article Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy Shupeng Zhang 1, Liangliang Wu 2, Xiaona Wang 2, Xuewei Ding 2, Han Liang 2 1 Department of General
Clinicopathological and prognostic differences between mucinous gastric carcinoma and signet-ring cell carcinoma
 Original Article Clinicopathological and prognostic differences between mucinous gastric carcinoma and signet-ring cell carcinoma Zhaode Bu, Zhixue Zheng, Ziyu Li, Xiaojiang Wu, Lianhai Zhang, Aiwen Wu,
Original Article Clinicopathological and prognostic differences between mucinous gastric carcinoma and signet-ring cell carcinoma Zhaode Bu, Zhixue Zheng, Ziyu Li, Xiaojiang Wu, Lianhai Zhang, Aiwen Wu,
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Metastatic mechanism of spermatic cord tumor from stomach cancer
 Int Canc Conf J (2013) 2:191 195 DOI 10.1007/s13691-013-0-9 CANCER BOARD CONFERENCE Metastatic mechanism of spermatic cord tumor from stomach cancer Masahiro Seike Yoshikazu Kanazawa Ryuji Ohashi Tadashi
Int Canc Conf J (2013) 2:191 195 DOI 10.1007/s13691-013-0-9 CANCER BOARD CONFERENCE Metastatic mechanism of spermatic cord tumor from stomach cancer Masahiro Seike Yoshikazu Kanazawa Ryuji Ohashi Tadashi
The prognostic significance of central fibrosis of adenocarcinoma
 Prognostic Significance of the Size of Central Fibrosis in Peripheral Adenocarcinoma of the Lung Kenji Suzuki, MD, Tomoyuki Yokose, MD, Junji Yoshida, MD, Mitsuyo Nishimura, MD, Kenro Takahashi, MD, Kanji
Prognostic Significance of the Size of Central Fibrosis in Peripheral Adenocarcinoma of the Lung Kenji Suzuki, MD, Tomoyuki Yokose, MD, Junji Yoshida, MD, Mitsuyo Nishimura, MD, Kenro Takahashi, MD, Kanji
Lung cancer is now a major cause of death in developed
 Original Article New IASLC/ATS/ERS Classification and Invasive Tumor Size are Predictive of Disease Recurrence in Stage I Lung Adenocarcinoma Naoki Yanagawa, MD, PhD,* Satoshi Shiono, MD, PhD, Masami Abiko,
Original Article New IASLC/ATS/ERS Classification and Invasive Tumor Size are Predictive of Disease Recurrence in Stage I Lung Adenocarcinoma Naoki Yanagawa, MD, PhD,* Satoshi Shiono, MD, PhD, Masami Abiko,
Does Preoperative Biliary Drainage Compromise the Long-Term Survival of Patients With Pancreatic Head Carcinoma?
 2015;111:270 276 Does Preoperative Biliary Drainage Compromise the Long-Term Survival of Patients With Pancreatic Head Carcinoma? YOSHIAKI MURAKAMI, MD,* KENICHIRO UEMURA, MD, YASUSHI HASHIMOTO, MD, NARU
2015;111:270 276 Does Preoperative Biliary Drainage Compromise the Long-Term Survival of Patients With Pancreatic Head Carcinoma? YOSHIAKI MURAKAMI, MD,* KENICHIRO UEMURA, MD, YASUSHI HASHIMOTO, MD, NARU
Effectiveness of additional resection of the invasive cancer-positive proximal bile duct margin in cases of hilar cholangiocarcinoma
 Original Article Effectiveness of additional resection of the invasive cancer-positive proximal bile duct margin in cases of hilar cholangiocarcinoma Wen-Jie Ma 1#, Zhen-Ru Wu 2#, Anuj Shrestha 1,3, Qin
Original Article Effectiveness of additional resection of the invasive cancer-positive proximal bile duct margin in cases of hilar cholangiocarcinoma Wen-Jie Ma 1#, Zhen-Ru Wu 2#, Anuj Shrestha 1,3, Qin
Prognostic Significance of Extranodal Cancer Invasion of Mediastinal Lymph Nodes in Lung Cancer
 Jpn. J. Clin. Oncol. 198, 1 (), 7-1 Prognostic Significance of Extranodal Cancer Invasion of Mediastinal Lymph Nodes in Lung Cancer KEIICHI SUEMASU, M.D. AND TSUGUO NARUKE, M.D. Department of Surgery,
Jpn. J. Clin. Oncol. 198, 1 (), 7-1 Prognostic Significance of Extranodal Cancer Invasion of Mediastinal Lymph Nodes in Lung Cancer KEIICHI SUEMASU, M.D. AND TSUGUO NARUKE, M.D. Department of Surgery,
The role of hepatic artery lymph node in pancreatic adenocarcinoma: prognostic factor or a selection criterion for surgery
 DOI:10.1111/hpb.12306 HPB ORIGINAL ARTICLE The role of hepatic artery lymph node in pancreatic adenocarcinoma: prognostic factor or a selection criterion for surgery Prejesh Philips, Erik Dunki-Jacobs,
DOI:10.1111/hpb.12306 HPB ORIGINAL ARTICLE The role of hepatic artery lymph node in pancreatic adenocarcinoma: prognostic factor or a selection criterion for surgery Prejesh Philips, Erik Dunki-Jacobs,
ORIGINAL ARTICLE. Fate of the Pancreatic Remnant After Resection for an Intraductal Papillary Mucinous Neoplasm
 ONLINE FIRST ORIGINAL ARTICLE Fate of the Pancreatic Remnant After Resection for an Intraductal Papillary Mucinous Neoplasm A Longitudinal Level II Cohort Study Toshiyuki Moriya, MD, PhD; L. William Traverso,
ONLINE FIRST ORIGINAL ARTICLE Fate of the Pancreatic Remnant After Resection for an Intraductal Papillary Mucinous Neoplasm A Longitudinal Level II Cohort Study Toshiyuki Moriya, MD, PhD; L. William Traverso,
In the mid 1970s, visceral pleural invasion (VPI) was included
 was included") ORIGINAL ARTICLE Tumor Invasion of Extralobar Soft Tissue Beyond the Hilar Region Does Not Affect the Prognosis of Surgically Resected Lung Cancer Patients Hajime Otsuka, MD,* Genichiro Ishii, MD, PhD,*
ORIGINAL ARTICLE Tumor Invasion of Extralobar Soft Tissue Beyond the Hilar Region Does Not Affect the Prognosis of Surgically Resected Lung Cancer Patients Hajime Otsuka, MD,* Genichiro Ishii, MD, PhD,*
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Perigastric lymph node metastases in gastric cancer: comparison of different staging systems
 Gastric Cancer (1999) 2: 201 205 Original article 1999 by International and Japanese Gastric Cancer Associations Perigastric lymph node metastases in gastric cancer: comparison of different staging systems
Gastric Cancer (1999) 2: 201 205 Original article 1999 by International and Japanese Gastric Cancer Associations Perigastric lymph node metastases in gastric cancer: comparison of different staging systems
PANCREATECTOMY WITH MESENTERIC AND PORTAL VEIN RESECTION FOR BORDERLINE RESECTABLE PANCREATIC CANCER: MULTICENTER STUDY
 PROPOSAL: PANCREATECTOMY WITH MESENTERIC AND PORTAL VEIN RESECTION FOR BORDERLINE RESECTABLE PANCREATIC CANCER: MULTICENTER STUDY Pancreatic carcinoma represents the fourth-leading cause of cancer-related
PROPOSAL: PANCREATECTOMY WITH MESENTERIC AND PORTAL VEIN RESECTION FOR BORDERLINE RESECTABLE PANCREATIC CANCER: MULTICENTER STUDY Pancreatic carcinoma represents the fourth-leading cause of cancer-related
Surgical outcomes of multifocal branch duct intraductal papillary mucinous neoplasms of pancreas
 Korean J Hepatobiliary Pancreat Surg 2014;18:152-158 http://dx.doi.org/10.14701/kjhbps.2014.18.4.152 Original Article Surgical outcomes of multifocal branch duct intraductal papillary mucinous neoplasms
Korean J Hepatobiliary Pancreat Surg 2014;18:152-158 http://dx.doi.org/10.14701/kjhbps.2014.18.4.152 Original Article Surgical outcomes of multifocal branch duct intraductal papillary mucinous neoplasms
Surgical resection is the first treatment of choice for
 Predictors of Lymph Node and Intrapulmonary Metastasis in Clinical Stage IA Non Small Cell Lung Carcinoma Kenji Suzuki, MD, Kanji Nagai, MD, Junji Yoshida, MD, Mitsuyo Nishimura, MD, and Yutaka Nishiwaki,
Predictors of Lymph Node and Intrapulmonary Metastasis in Clinical Stage IA Non Small Cell Lung Carcinoma Kenji Suzuki, MD, Kanji Nagai, MD, Junji Yoshida, MD, Mitsuyo Nishimura, MD, and Yutaka Nishiwaki,
Prognostic value of visceral pleura invasion in non-small cell lung cancer q
 European Journal of Cardio-thoracic Surgery 23 (2003) 865 869 www.elsevier.com/locate/ejcts Prognostic value of visceral pleura invasion in non-small cell lung cancer q Jeong-Han Kang, Kil Dong Kim, Kyung
European Journal of Cardio-thoracic Surgery 23 (2003) 865 869 www.elsevier.com/locate/ejcts Prognostic value of visceral pleura invasion in non-small cell lung cancer q Jeong-Han Kang, Kil Dong Kim, Kyung
Cholangiocarcinoma. Judy Wyatt Dundee November 2010
 Cholangiocarcinoma Judy Wyatt Dundee November 2010 Making sense of cholangiocarcinoma Difficulties with diagnostic criteria How many entities within cholangiocarcinoma? Rapidly evolving Intrahepatic cholangiocarcinoma
Cholangiocarcinoma Judy Wyatt Dundee November 2010 Making sense of cholangiocarcinoma Difficulties with diagnostic criteria How many entities within cholangiocarcinoma? Rapidly evolving Intrahepatic cholangiocarcinoma
Superior and Basal Segment Lung Cancers in the Lower Lobe Have Different Lymph Node Metastatic Pathways and Prognosis
 ORIGINAL ARTICLES: Superior and Basal Segment Lung Cancers in the Lower Lobe Have Different Lymph Node Metastatic Pathways and Prognosis Shun-ichi Watanabe, MD, Kenji Suzuki, MD, and Hisao Asamura, MD
ORIGINAL ARTICLES: Superior and Basal Segment Lung Cancers in the Lower Lobe Have Different Lymph Node Metastatic Pathways and Prognosis Shun-ichi Watanabe, MD, Kenji Suzuki, MD, and Hisao Asamura, MD
Research Article Prognostic Implication of Predominant Histologic Subtypes of Lymph Node Metastases in Surgically Resected Lung Adenocarcinoma
 BioMed Research International, Article ID 64568, 6 pages http://dx.doi.org/.55/24/64568 Research Article Prognostic Implication of Predominant Histologic Subtypes of Lymph Node Metastases in Surgically
BioMed Research International, Article ID 64568, 6 pages http://dx.doi.org/.55/24/64568 Research Article Prognostic Implication of Predominant Histologic Subtypes of Lymph Node Metastases in Surgically
Although ipsilateral intrapulmonary metastasis (PM), Evaluation of TMN Classification for Lung Carcinoma With Ipsilateral Intrapulmonary Metastasis
, Evaluation of TMN Classification for Lung Carcinoma With Ipsilateral Intrapulmonary Metastasis") Evaluation of TMN Classification for Lung Carcinoma With Ipsilateral Intrapulmonary Metastasis Morihito Okada, MD, Noriaki Tsubota, MD, Masahiro Yoshimura, MD, Yoshifumi Miyamoto, MD, and Reiko Nakai,
Evaluation of TMN Classification for Lung Carcinoma With Ipsilateral Intrapulmonary Metastasis Morihito Okada, MD, Noriaki Tsubota, MD, Masahiro Yoshimura, MD, Yoshifumi Miyamoto, MD, and Reiko Nakai,
Outcomes of adjuvant radiotherapy and lymph node resection in elderly patients with pancreatic cancer treated with surgery and chemotherapy
 Original Article Outcomes of adjuvant radiotherapy and lymph node resection in elderly patients with pancreatic cancer treated with surgery and chemotherapy Jessica Frakes 1, Eric A. Mellon 1, Gregory
Original Article Outcomes of adjuvant radiotherapy and lymph node resection in elderly patients with pancreatic cancer treated with surgery and chemotherapy Jessica Frakes 1, Eric A. Mellon 1, Gregory
Prognostic Factors for Survival of Stage IB Upper Lobe Non-small Cell Lung Cancer Patients: A Retrospective Study in Shanghai, China
 www.springerlink.com Chin J Cancer Res 23(4):265 270, 2011 265 Original Article Prognostic Factors for Survival of Stage IB Upper Lobe Non-small Cell Lung Cancer Patients: A Retrospective Study in Shanghai,
www.springerlink.com Chin J Cancer Res 23(4):265 270, 2011 265 Original Article Prognostic Factors for Survival of Stage IB Upper Lobe Non-small Cell Lung Cancer Patients: A Retrospective Study in Shanghai,
Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach
 Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
A new scoring system for peritoneal metastasis in gastric cancer
 Gastric Cancer (2003) 6: 146 152 DOI 10.1007/s10120-003-0243-6 2003 by International and Japanese Gastric Cancer Associations Original article A new scoring system for peritoneal metastasis in gastric
Gastric Cancer (2003) 6: 146 152 DOI 10.1007/s10120-003-0243-6 2003 by International and Japanese Gastric Cancer Associations Original article A new scoring system for peritoneal metastasis in gastric
Visceral pleura invasion (VPI) was adopted as a specific
 was adopted as a specific") ORIGINAL ARTICLE Visceral Pleura Invasion Impact on Non-small Cell Lung Cancer Patient Survival Its Implications for the Forthcoming TNM Staging Based on a Large-Scale Nation-Wide Database Junji Yoshida,
ORIGINAL ARTICLE Visceral Pleura Invasion Impact on Non-small Cell Lung Cancer Patient Survival Its Implications for the Forthcoming TNM Staging Based on a Large-Scale Nation-Wide Database Junji Yoshida,
Lymph node dissection for lung cancer is both an old
 LOBE-SPECIFIC EXTENT OF SYSTEMATIC LYMPH NODE DISSECTION FOR NON SMALL CELL LUNG CARCINOMAS ACCORDING TO A RETROSPECTIVE STUDY OF METASTASIS AND PROGNOSIS Hisao Asamura, MD Haruhiko Nakayama, MD Haruhiko
LOBE-SPECIFIC EXTENT OF SYSTEMATIC LYMPH NODE DISSECTION FOR NON SMALL CELL LUNG CARCINOMAS ACCORDING TO A RETROSPECTIVE STUDY OF METASTASIS AND PROGNOSIS Hisao Asamura, MD Haruhiko Nakayama, MD Haruhiko
Prognostic significance of metastatic lymph node ratio: the lymph node ratio could be a prognostic indicator for patients with gastric cancer
 Hou et al. World Journal of Surgical Oncology (2018) 16:198 https://doi.org/10.1186/s12957-018-1504-5 REVIEW Open Access Prognostic significance of metastatic lymph node ratio: the lymph node ratio could
Hou et al. World Journal of Surgical Oncology (2018) 16:198 https://doi.org/10.1186/s12957-018-1504-5 REVIEW Open Access Prognostic significance of metastatic lymph node ratio: the lymph node ratio could
Treatment outcomes and prognostic factors of gallbladder cancer patients after postoperative radiation therapy
 Korean J Hepatobiliary Pancreat Surg 2011;15:152-156 Original Article Treatment outcomes and prognostic factors of gallbladder cancer patients after postoperative radiation therapy Suzy Kim 1,#, Kyubo
Korean J Hepatobiliary Pancreat Surg 2011;15:152-156 Original Article Treatment outcomes and prognostic factors of gallbladder cancer patients after postoperative radiation therapy Suzy Kim 1,#, Kyubo
Characteristics and prognostic factors of synchronous multiple primary esophageal carcinoma: A report of 52 cases
 Thoracic Cancer ISSN 1759-7706 ORIGINAL ARTICLE Characteristics and prognostic factors of synchronous multiple primary esophageal carcinoma: A report of 52 cases Mei Li & Zhi-xiong Lin Department of Radiation
Thoracic Cancer ISSN 1759-7706 ORIGINAL ARTICLE Characteristics and prognostic factors of synchronous multiple primary esophageal carcinoma: A report of 52 cases Mei Li & Zhi-xiong Lin Department of Radiation
Clinicopathological Characteristics and Outcome Indicators of Stage II Gastric Cancer According to the Japanese Classification of Gastric Cancer
 Clinicopathological Characteristics and Outcome Indicators of Stage II Gastric Cancer According to the Japanese Classification of Gastric Cancer HITOSHI OJIMA 1, KEN-ICHIRO ARAKI 1, TOSHIHIDE KATO 1, KAORI
Clinicopathological Characteristics and Outcome Indicators of Stage II Gastric Cancer According to the Japanese Classification of Gastric Cancer HITOSHI OJIMA 1, KEN-ICHIRO ARAKI 1, TOSHIHIDE KATO 1, KAORI
Citation Hepato-Gastroenterology, 55(86-87),
,") NAOSITE: Nagasaki University's Ac Title Author(s) Combined pancreatic resection and p multiple lesions of the pancreas: i of the pancreas concomitant with du Kuroki, Tamotsu; Tajima, Yoshitsugu Tomohiko;
NAOSITE: Nagasaki University's Ac Title Author(s) Combined pancreatic resection and p multiple lesions of the pancreas: i of the pancreas concomitant with du Kuroki, Tamotsu; Tajima, Yoshitsugu Tomohiko;
Pancreatobiliary Frozen Section Nightmares
 Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
RESEARCH ARTICLE. Normalization of CA19-9 Following Resection for Pancreatic Ductal Adenocarcinoma is not Tantamount to being Cured?
 DOI:http://dx.doi.org/10.7314/APJCP.2015.16.2.661 Normalization of CA19-9 Following Resection for Pancreatic Ductal Adenocarcinoma is not Tantamount to being Cured? RESEARCH ARTICLE Normalization of CA19-9
DOI:http://dx.doi.org/10.7314/APJCP.2015.16.2.661 Normalization of CA19-9 Following Resection for Pancreatic Ductal Adenocarcinoma is not Tantamount to being Cured? RESEARCH ARTICLE Normalization of CA19-9
Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer. Cheol Min Kang 2018/04/05
 Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
ORIGINAL ARTICLE INTRODUCTION METHODS ABSTRACT
 ORIGINAL ARTICLE Patients with Lung Recurrence after Curative Resection for Pancreatic Ductal Adenocarcinoma Have a Better Prognosis than Those with Recurrence at Other Sites Yusuke Watanabe 1, Kazuyoshi
ORIGINAL ARTICLE Patients with Lung Recurrence after Curative Resection for Pancreatic Ductal Adenocarcinoma Have a Better Prognosis than Those with Recurrence at Other Sites Yusuke Watanabe 1, Kazuyoshi
In 1989, Deslauriers et al. 1 described intrapulmonary metastasis
 ORIGINAL ARTICLE Prognosis of Resected Non-Small Cell Lung Cancer Patients with Intrapulmonary Metastases Kanji Nagai, MD,* Yasunori Sohara, MD, Ryosuke Tsuchiya, MD, Tomoyuki Goya, MD, and Etsuo Miyaoka,
ORIGINAL ARTICLE Prognosis of Resected Non-Small Cell Lung Cancer Patients with Intrapulmonary Metastases Kanji Nagai, MD,* Yasunori Sohara, MD, Ryosuke Tsuchiya, MD, Tomoyuki Goya, MD, and Etsuo Miyaoka,
Original Article Prognostic role of neuroendocrine cell differentiation in human gastric carcinoma
 Int J Clin Exp Med 2015;8(5):7837-7842 www.ijcem.com /ISSN:1940-5901/IJCEM0003844 Original Article Prognostic role of neuroendocrine cell differentiation in human gastric carcinoma Tingting Zhang, Dan
Int J Clin Exp Med 2015;8(5):7837-7842 www.ijcem.com /ISSN:1940-5901/IJCEM0003844 Original Article Prognostic role of neuroendocrine cell differentiation in human gastric carcinoma Tingting Zhang, Dan
Intrahepatic Sarcomatoid Cholangiocarcinoma with Portal Vein Thrombosis: A Case Report 1
 Intrahepatic Sarcomatoid Cholangiocarcinoma with Portal Vein Thrombosis: A Case Report 1 Jae-Hoon Lim, M.D., Jin Woong Kim, M.D., Suk Hee Heo, M.D., Yong Yeon Jeong, M.D., Heoung Keun Kang, M.D. A 53-year-old
Intrahepatic Sarcomatoid Cholangiocarcinoma with Portal Vein Thrombosis: A Case Report 1 Jae-Hoon Lim, M.D., Jin Woong Kim, M.D., Suk Hee Heo, M.D., Yong Yeon Jeong, M.D., Heoung Keun Kang, M.D. A 53-year-old
Akt Phosphorylation Is a Risk Factor for Early Disease Recurrence and Poor Prognosis in Hepatocellular Carcinoma
 307 Akt Phosphorylation Is a Risk Factor for Early Disease Recurrence and Poor Prognosis in Hepatocellular Carcinoma Kazuaki Nakanishi, M.D., Ph.D. 1,2 Michiie Sakamoto, M.D., Ph.D. 1,3 Susumu Yamasaki,
307 Akt Phosphorylation Is a Risk Factor for Early Disease Recurrence and Poor Prognosis in Hepatocellular Carcinoma Kazuaki Nakanishi, M.D., Ph.D. 1,2 Michiie Sakamoto, M.D., Ph.D. 1,3 Susumu Yamasaki,
Original Article. Spontaneous Healing of Breast Cancer
 Breast Cancer Vol. 12 No. 2 April 2005 Original Article Rie Horii 1, 3, Futoshi Akiyama 1, Fujio Kasumi 2, Morio Koike 3, and Goi Sakamoto 1 1 Department of Breast Pathology, the Cancer Institute of the
Breast Cancer Vol. 12 No. 2 April 2005 Original Article Rie Horii 1, 3, Futoshi Akiyama 1, Fujio Kasumi 2, Morio Koike 3, and Goi Sakamoto 1 1 Department of Breast Pathology, the Cancer Institute of the
Is it Time to Stop Checking Frozen Section Neck Margins During Pancreaticoduodenectomy?
 Ann Surg Oncol (2013) 20:3626 3633 DOI 10.1245/s10434-013-3080-9 ORIGINAL ARTICLE PANCREATIC TUMORS Is it Time to Stop Checking Frozen Section Neck Margins During Pancreaticoduodenectomy? Neha L. Lad,
Ann Surg Oncol (2013) 20:3626 3633 DOI 10.1245/s10434-013-3080-9 ORIGINAL ARTICLE PANCREATIC TUMORS Is it Time to Stop Checking Frozen Section Neck Margins During Pancreaticoduodenectomy? Neha L. Lad,
A Multicentric Development Of Intraductal Papillary Mucinous Neoplasm Treated By Repeated Pancreatectomy
 ISPUB.COM The Internet Journal of Surgery Volume 7 Number 2 A Multicentric Development Of Intraductal Papillary Mucinous Neoplasm Treated By Repeated T Matsumoto, K Iwaki, H Uchida, K Yada, K Shibata,
ISPUB.COM The Internet Journal of Surgery Volume 7 Number 2 A Multicentric Development Of Intraductal Papillary Mucinous Neoplasm Treated By Repeated T Matsumoto, K Iwaki, H Uchida, K Yada, K Shibata,
Clinical Outcome of Reconstruction With Tissue Expanders for Patients With Breast Cancer and Mastectomy
 Clinical Outcome of Reconstruction With Tissue Expanders for Patients With Breast Cancer and Mastectomy Mitsui Memorial Hospital Department of Breast and Endocine surgery Daisuke Ota No financial support
Clinical Outcome of Reconstruction With Tissue Expanders for Patients With Breast Cancer and Mastectomy Mitsui Memorial Hospital Department of Breast and Endocine surgery Daisuke Ota No financial support
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Key words: recurrence pattern of pancreatic cancer, extended resection for pancreatic cancer, intraoperative radiation therapy. stage I.
 Key words: recurrence pattern of pancreatic cancer, extended resection for pancreatic cancer, intraoperative radiation therapy stage I stage II stage III stage W Ex-TP : Extended Total Pancreatectomy Ex-PD
Key words: recurrence pattern of pancreatic cancer, extended resection for pancreatic cancer, intraoperative radiation therapy stage I stage II stage III stage W Ex-TP : Extended Total Pancreatectomy Ex-PD
Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY
 PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY Jeannelyn S. Estrella, MD Department of Pathology The UT MD Anderson Cancer
PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY Jeannelyn S. Estrella, MD Department of Pathology The UT MD Anderson Cancer
RESEARCH ARTICLE. Qian Liu, Jian-Jun Bi, Yan-Tao Tian, Qiang Feng, Zhao-Xu Zheng, Zheng Wang* Abstract. Introduction. Materials and Methods
 RESEARCH ARTICLE Outcome after Simultaneous Resection of Gastric Primary Tumour and Synchronous Liver Metastases: Survival Analysis of a Single-center Experience in China Qian Liu, Jian-Jun Bi, Yan-Tao
RESEARCH ARTICLE Outcome after Simultaneous Resection of Gastric Primary Tumour and Synchronous Liver Metastases: Survival Analysis of a Single-center Experience in China Qian Liu, Jian-Jun Bi, Yan-Tao
Management of Rare Liver Tumours
 Gian Luca Grazi Hepato-Biliary-Pancreatic Surgery National Cancer Institute Regina Elena Rome Fibrolamellar Carcinoma Mixed Hepato Cholangiocellular Carcinoma Hepatoblastoma Carcinosarcoma Primary Hepatic
Gian Luca Grazi Hepato-Biliary-Pancreatic Surgery National Cancer Institute Regina Elena Rome Fibrolamellar Carcinoma Mixed Hepato Cholangiocellular Carcinoma Hepatoblastoma Carcinosarcoma Primary Hepatic
A Proposed Strategy for Treatment of Superficial Carcinoma. in the Thoracic Esophagus Based on an Analysis. of Lymph Node Metastasis
 Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
THE RELEVANCE OF SOME TUMORAL MARKERS IN PATIENTS WITH PANCREATIC CANCER
 THE RELEVANCE OF SOME TUMORAL MARKERS IN PATIENTS WITH PANCREATIC CANCER DANIEL TIMOFTE 1, RADU DANILA 1*, ALIN CIOBICA 2, CORNELIU DIACONU 1, ROXANA LIVADARIU 3, LIDIA IONESCU 1 Keywords: pancreatic cancer,
THE RELEVANCE OF SOME TUMORAL MARKERS IN PATIENTS WITH PANCREATIC CANCER DANIEL TIMOFTE 1, RADU DANILA 1*, ALIN CIOBICA 2, CORNELIU DIACONU 1, ROXANA LIVADARIU 3, LIDIA IONESCU 1 Keywords: pancreatic cancer,
Treatment of oligometastatic NSCLC
 Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination
 Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Radical nerve dissection for the carcinoma of head of pancreas: report of 30 cases
 Original Article Radical nerve dissection for the carcinoma of head of pancreas: report of 30 cases Qing Lin, Langping Tan, Yu Zhou, Quanbo Zhou, Rufu Chen Department of Biliary and Pancreatic Surgery,
Original Article Radical nerve dissection for the carcinoma of head of pancreas: report of 30 cases Qing Lin, Langping Tan, Yu Zhou, Quanbo Zhou, Rufu Chen Department of Biliary and Pancreatic Surgery,
Branch duct intraductal papillary mucinous neoplasm of the pancreas: single-center experience with 324 patients who underwent surgical resection
 Korean J Hepatobiliary Pancreat Surg 2015;19:113-120 http://dx.doi.org/10.14701/kjhbps.2015.19.3.113 Original Article Branch duct intraductal papillary mucinous neoplasm of the pancreas: single-center
Korean J Hepatobiliary Pancreat Surg 2015;19:113-120 http://dx.doi.org/10.14701/kjhbps.2015.19.3.113 Original Article Branch duct intraductal papillary mucinous neoplasm of the pancreas: single-center
Correlation between expression and significance of δ-catenin, CD31, and VEGF of non-small cell lung cancer
 Correlation between expression and significance of δ-catenin, CD31, and VEGF of non-small cell lung cancer X.L. Liu 1, L.D. Liu 2, S.G. Zhang 1, S.D. Dai 3, W.Y. Li 1 and L. Zhang 1 1 Thoracic Surgery,
Correlation between expression and significance of δ-catenin, CD31, and VEGF of non-small cell lung cancer X.L. Liu 1, L.D. Liu 2, S.G. Zhang 1, S.D. Dai 3, W.Y. Li 1 and L. Zhang 1 1 Thoracic Surgery,