NEUROLOGICAL EXAMINATIONS: LOCALISATION AND GRADING
|
|
|
- Arnold Hicks
- 5 years ago
- Views:
Transcription
1 Vet Times The website for the veterinary profession NEUROLOGICAL EXAMINATIONS: LOCALISATION AND GRADING Author : MARK LOWRIE Categories : Vets Date : June 16, 2014 MARK LOWRIE MA, VetMB, MVM, DipECVN, MRCVS in the second of a three-part article, provides a step-by-step approach to focusing on determining the severity and position of the problem AS described in the previous article (VT44.20), the neurological examination has key aims and questions to answer: Is the problem definitely neurological? What is the location of this lesion in the nervous system? How severe is the disease? What are the main types of disease process that can explain the clinical signs? Whether the problem is definitely neurological was tackled in the first article. Having determined a patient truly is neurological we can embark on a neurological examination. This article will describe how the problem can be further localised and graded based on the other three questions. It will highlight the importance of not skipping the neurological examination and give insights about the important information that can be obtained by refining this skill. A discussion of the common diseases affecting the spinal cord will follow in a future article. 1 / 14
2 What is the location of this lesion? The nervous system can be crudely divided into segments (Figure 1). The idea is to precisely localise the lesion to a progressively smaller area of the nervous system. By the end of the neurological examination it should be possible to locate the lesion in one or more of these areas. The examination can be divided into a series of questions that should be sequentially answered. The neurological examination starts with watching the animal walk and observing how it interacts with its surroundings. Gait assessment is the only way of revealing certain abnormalities (for example, circling or hypermetria) although observation will also allow evaluation of posture (for example, the presence of a head tilt, wide-based stance and so on), mental status (for example, is the patient alert, obtunded, stuporous or comatose) and the presence of any abnormal behaviours and involuntary movements. a) How many limbs are affected? Having understood the nature of the gait abnormality (such as whether the patient is ataxic, lame or paretic) and associated signs, it is important to determine how many limbs are affected. In many cases, particularly in patients that are non-ambulatory, this can be relatively straightforward. However, when managing ambulatory patients it can be very difficult to distinguish subtle neurological signs in potentially affected limbs. Paw positioning and hopping responses do not need to be tested if a patient is obviously dragging a limb. However, if the results of gait observation are equivocal, these procedures are extremely useful to detect subclinical neurological disease. b) How are the reflexes in the affected limbs? Having ascertained which limbs are affected we can slowly narrow down the location of the lesion (Figure 1). For example, a patient with only pelvic limb involvement will have a lesion caudal to T2 but a patient with all four limbs affected will have a lesion cranially to T2 or in the neuromuscular system. To narrow this localisation further we must check the reflexes in the affected limbs and determine whether upper or lower motor neuron reflexes are present (Table 1). The patellar reflex can be considered. It is a monosynaptic reflex that evaluates the femoral nerve (L4 to L6). However, its presence and absence are unreliable, with many older dogs losing this reflex as a normal finding. With this in mind, I tend to use the withdrawal reflex (pedal or flexor reflex) as it evaluates multiple thoracic (C6 to T1) and pelvic (L6 to S1) limb nerves and seems reliable regardless of age. The importance of doing this is to determine whether the reflex is decreased or absent. If lower motor neuron signs are present then the lesion is affecting the reflex arc and hence the 2 / 14
3 lesion will be in the L4 to S3 spinal segments (if only the pelvic limbs are affected) or the C6 to T2 spinal segments (if only the forelimbs are affected). If all four limbs are affected with lower motor neuron signs (decreased tone, decreased reflexes and atrophy) then the lesion is suspected to be involving the neuromuscular system. If upper motor neuron signs are present to all four limbs then the lesion will be cranial to the brachial plexus (cranial to T2). If only the pelvic limbs are affected with upper motor neuron signs then the lesion will be in the T3 to L3 segments. How severe is the disease? The spinal cord is important in the perception of pain (performed via small diameter slow conducting neurons), in enabling voluntary movement (via descending motor fibres), and the transmission of spatial awareness (proprioception; performed via ascending large diameter fast conducting myelinated axons). These functions are lost sequentially as a spinal cord injury progresses. The large diameter fast-conducting myelinated axons are the first to be affected in spinal cord disease followed by the motor fibres. The most resilient neurons are the slowconducting small diameter neurons involved in deep pain perception that are contained deep in the spinal cord white matter. Therefore, the first clinical sign observed in spinal cord injury would be ataxia followed by paresis. Pain perception is the last thing to be lost. Pain perception is, therefore, the most important factor in determining prognosis. Any patient that has voluntary movement (no matter how little) in the affected limb will have retained pain perception and testing this should be reserved only for those cases that have complete paralysis of a limb or limbs. A conscious and positive deep pain perception response is defined as the animal turning around and making some form of behavioural response that indicates they have perceived the painful stimulus, for example, whimpering or trying to bite when a pair of haemostats is applied to a digit. A withdrawal of the limb is not sufficient to declare deep pain present (Panel 1). An absence of deep pain perception should be considered an emergency with a prognosis of 50 per cent to 70 per cent if treatment is administered within 12 hours of losing pain perception. Assessing severity in cervical and lumbosacral disease Patients with cervical lesions will always have intact deep pain perception because a lesion severe enough to diminish this response would also abolish voluntary respiratory movements leading to death. Therefore, deep pain perception is a less useful indicator in cervical spinal disease. A lesion of the lumbosacral spine will not cause paralysis to the pelvic limbs. Instead, it will cause signs compatible with damage to the nerve roots in this region (typically the sacral nerve roots; Figure 2 ). This is because the vertebral canal in this region contains the cauda equina (predominantly the 3 / 14
4 sacral nerve roots) rather than the spinal cord. A lesion to the cauda equina therefore has different implications to lesions involving the spinal cord. The sacral nerve roots supply the tail, anus and perineum. Complete laceration of these nerve roots would cause a flaccid tail with absent deep pain perception, a dilated anus with absent tone and loss of sensation around the perineum. In patients with laceration of these nerve roots the long-term prognosis for a return to normal continence is grave despite having intact deep pain perception. The take-home message is loss of deep pain perception does not carry the same grave prognosis as it would for spinal cord injury because paralysis of the pelvic limbs is not an expected finding (nerve roots supplying the limbs have already exited the spinal column at this level). A traction injury to this region, however, could cause severe weakness to the pelvic limbs (for example, as is seen following tail pull injuries in cats). Furthermore, lumbosacral disease rarely affects the gait and more frequently results in pain alongside tail carriage, anal tone and perineal sensation abnormalities (which may partly manifest as faecal and/or urinary incontinence). Prognosis in these cases is determined by the presence or absence of perineal sensation, anal tone and tail base sensation. Main types of disease process that can explain clinical signs Different spinal cord segments are affected by different diseases. Similarly, the age, breed and speed of onset will also determine the more likely diseases. Each disease process has a typical signalment, onset and progression as well as distribution in the nervous system. For example, a middle-aged dachshund with an acute onset paraparesis is most likely to have an intervertebral disc extrusion while a young beagle with neck pain is most likely to have steroid-responsive meningitis-arteritis. Despite these patterns it is very important not to ignore other less common possibilities. Before examination, a complete history must be taken to establish the onset and progression of the clinical signs. Did the signs occur acutely, chronically or insidiously? Is the disease progressive? This information alone can refine the list of differential diagnoses by considering the sign-time graph (Figure 3) and also allows a prognosis to be considered. For example, a dog presenting with slowly progressive clinical signs suggests a degenerative or neoplastic condition and may be given a poorer prognosis. However, it must be emphasised to the owner that without further investigation the likely diagnoses, and associated prognoses, remain speculative. A list of potential causes can be made using the VITAMIN-D acronym (Table 2). Based on the history, signalment and neurological localisation this list of potential causes can be narrowed further depending on the neurological segments involved (Tables 3 to 6). Therefore, at the end of the examination the clinician should be aware of the potential disease processes involved and hence enable the owner to make an informed decision as to whether further investigation to identify these causes is warranted in light of the likely prognosis. 4 / 14
5 Summary These two articles have given a stepwise approach to the spinal patient. On presentation, a full clinical examination should first be performed to ensure the signs are not due to a non-neurological problem. A neurological assessment can then follow to include observation of the gait to ascertain the number of legs that are affected and the nature of the reflexes in the affected legs. Finally, the severity is established, that is, is movement present or absent? If movement is absent then deep pain perception should be evaluated. Collating this information will allow an accurate neurological localisation to be determined as well as an expected prognosis. Following these simple rules and avoiding the common mistakes ensures spinal cases are managed correctly and appropriately, regardless of costs and facilities. PANEL 1 Deep pain perception is not the same as the withdrawal reflex It is important not to confuse the withdrawal reflex with the conscious perception of pain. The withdrawal reflex is useful only in localising lesions whereas deep pain perception is only useful in establishing a lesion s severity. If a lesion does not affect the reflex arc then the withdrawal reflex may be intact even if deep pain perception is lost due to a spinal cord lesion situated more cranially. Pain perception is tested by pinching the digits. If there is no conscious response then the nail beds and digits are also tested with haemostats. If there is still no response then forceps are applied to the tibia. 5 / 14
6 Figure 1. Schematic representation of the components of the nervous system and how they are divided. Lesions at C6 to T2 and L4 to S3 (and the neuromuscular system) cause lower motor neuron signs. Lesions in the region of C1 to C5 and T3 to L3 cause upper motor neuron signs. 6 / 14

7 Figure 2. A 12-week-old domestic shorthair cat presented after being accidentally trodden on by the owner. The neurological presentation was a flaccid tail with no deep pain perception, and absent anal tone and perineal sensation. The cat was still able to walk, although it exhibited mild paraparesis with no ataxia, most probably due to transient traction of the nerve roots supplying the pelvic limbs at the time of trauma. A displaced fracture of the lumbosacral region is seen on this lateral radiograph. This was causing instability of the lumbosacral region. The fracture was stabilised and, long term, the cat returned to normal mobility (as would be expected) as well as regaining normal tail function, and urinary and faecal continence. 7 / 14

8 Figure 3. A sign-time graph to show the course of different categories of neurological disease over time. 8 / 14

9 Table 1. Clinical signs that may be expected with upper motor neuron and lower motor neuron signs 9 / 14
10 10 / 14

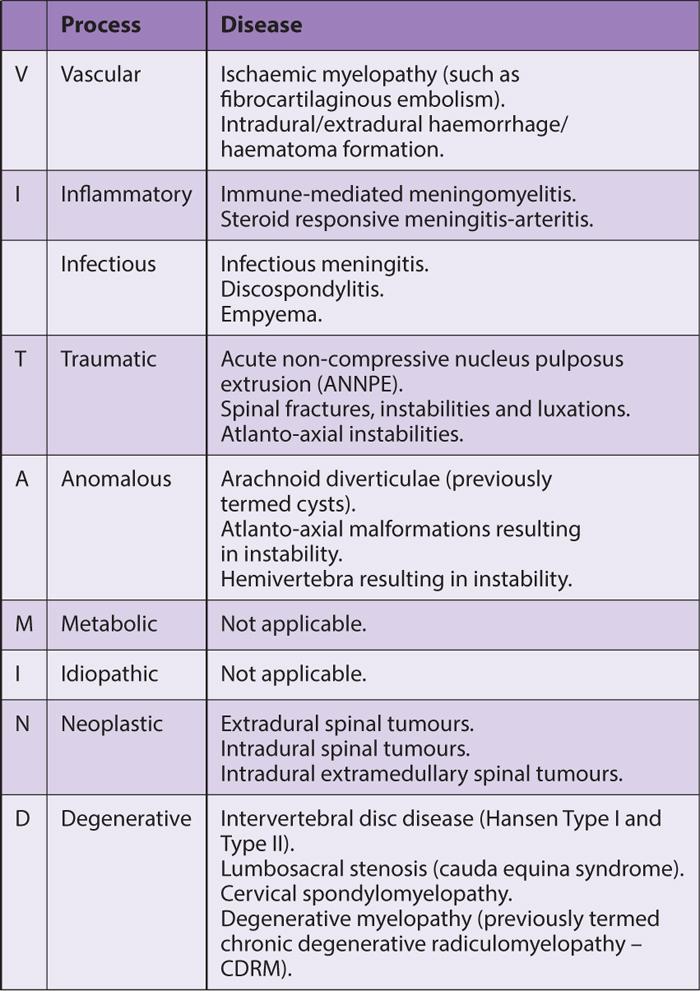
11 Table 2. Some of the more common diseases affecting the spinal cord of the dog classified according to the VITAMIN-D acronym. 11 / 14

12 Table 3. The common diseases affecting the canine cervical spine (C1 to C5 spinal segments) and cervical intumescence (C6 to T2 spinal segments). 12 / 14
.")
13 Table 4. The common diseases affecting the canine thoracolumbar spine (T3 to L3 spinal segments). Table 5. The common diseases affecting the canine caudal lumbar spine (L4 to L7 spinal segments). 13 / 14

14 Table 6. The common diseases affecting the canine lumbosacral spine (L7 to S3 spinal segments). 14 / 14 Powered by TCPDF (
Fecal Incontinence. Inability to retain feces or bowel movements, resulting in involuntary passage of feces or bowel movements
 Fecal Incontinence (Involuntary Passage of Feces or Bowel Movements) Basics OVERVIEW Inability to retain feces or bowel movements, resulting in involuntary passage of feces or bowel movements GENETICS
Fecal Incontinence (Involuntary Passage of Feces or Bowel Movements) Basics OVERVIEW Inability to retain feces or bowel movements, resulting in involuntary passage of feces or bowel movements GENETICS
Spinal disorders in small animals
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Spinal disorders in small animals Author : ROB PETTITT Categories : Vets Date : June 2, 2008 ROB PETTITT discusses conditions
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Spinal disorders in small animals Author : ROB PETTITT Categories : Vets Date : June 2, 2008 ROB PETTITT discusses conditions
The Deconstructed Neurological Examination
 The Deconstructed Neurological Examination Marguerite Knipe, DVM, Diplomate ACVIM (Neurology) I. MENTATION: Normal, Quiet, Obtunded (mild, moderate, severe), Stuporous, Comatose Define stuporous and comatose.
The Deconstructed Neurological Examination Marguerite Knipe, DVM, Diplomate ACVIM (Neurology) I. MENTATION: Normal, Quiet, Obtunded (mild, moderate, severe), Stuporous, Comatose Define stuporous and comatose.
SPINAL CORD DISEASE IN DOGS PART TWO: MOST LIKELY CAUSES
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk SPINAL CORD DISEASE IN DOGS PART TWO: MOST LIKELY CAUSES Author : RITA GONÇALVES Categories : Vets Date : April 7, 2014 RITA
Vet Times The website for the veterinary profession https://www.vettimes.co.uk SPINAL CORD DISEASE IN DOGS PART TWO: MOST LIKELY CAUSES Author : RITA GONÇALVES Categories : Vets Date : April 7, 2014 RITA
examination in Companion Animals
 Peer reviewed The Neurologic examination in Companion Animals Part 2: Interpreting Abnormal Findings Helena Rylander, DVM, Diplomate ACVIM (Neurology) In the January/February issue of Today s Veterinary
Peer reviewed The Neurologic examination in Companion Animals Part 2: Interpreting Abnormal Findings Helena Rylander, DVM, Diplomate ACVIM (Neurology) In the January/February issue of Today s Veterinary
TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION Author : SIMONA T RADAELLI Categories : Vets Date : July
Vet Times The website for the veterinary profession https://www.vettimes.co.uk TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION Author : SIMONA T RADAELLI Categories : Vets Date : July
Nursing the spinal patient
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Nursing the spinal patient Author : Lisa Thompson Categories : RVNs Date : November 1, 2009 Lisa Thompson DipAVN(surg), looks
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Nursing the spinal patient Author : Lisa Thompson Categories : RVNs Date : November 1, 2009 Lisa Thompson DipAVN(surg), looks
Note: Please refer to handout Spinal Plexuses and Representative Spinal Nerves for
 Chapter 13 Outline Note: Please refer to handout Spinal Plexuses and Representative Spinal Nerves for what you need to know from Exhibits 13.1 13.4 I. INTRODUCTION A. The spinal cord and spinal nerves
Chapter 13 Outline Note: Please refer to handout Spinal Plexuses and Representative Spinal Nerves for what you need to know from Exhibits 13.1 13.4 I. INTRODUCTION A. The spinal cord and spinal nerves
Chapter 13. The Spinal Cord & Spinal Nerves. Spinal Cord. Spinal Cord Protection. Meninges. Together with brain forms the CNS Functions
 Spinal Cord Chapter 13 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward
Spinal Cord Chapter 13 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward
APPROACHES TO NEUROLOGICAL EXAMINATION IN RABBITS
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk APPROACHES TO NEUROLOGICAL EXAMINATION IN RABBITS Author : ELISABETTA MANCINELLI Categories : Vets Date : October 6, 2014
Vet Times The website for the veterinary profession https://www.vettimes.co.uk APPROACHES TO NEUROLOGICAL EXAMINATION IN RABBITS Author : ELISABETTA MANCINELLI Categories : Vets Date : October 6, 2014
Thoracolumbar Intervertebral Disk Disease Basics
 Thoracolumbar Intervertebral Disk Disease Basics OVERVIEW The spine is composed of multiple bones (vertebrae) with disks (intervertebral disks) located in between adjacent bones; the disks act as shock
Thoracolumbar Intervertebral Disk Disease Basics OVERVIEW The spine is composed of multiple bones (vertebrae) with disks (intervertebral disks) located in between adjacent bones; the disks act as shock
Human Anatomy. Spinal Cord and Spinal Nerves
 Human Anatomy Spinal Cord and Spinal Nerves 1 The Spinal Cord Link between the brain and the body. Exhibits some functional independence from the brain. The spinal cord and spinal nerves serve two functions:
Human Anatomy Spinal Cord and Spinal Nerves 1 The Spinal Cord Link between the brain and the body. Exhibits some functional independence from the brain. The spinal cord and spinal nerves serve two functions:
Spinal Cord- Medulla Spinalis. Cuneyt Mirzanli Istanbul Gelisim University
 Spinal Cord- Medulla Spinalis Cuneyt Mirzanli Istanbul Gelisim University Spinal Column Supports the skull, pectoral girdle, upper limbs and thoracic cage by way of the pelvic girdle. Transmits body weight
Spinal Cord- Medulla Spinalis Cuneyt Mirzanli Istanbul Gelisim University Spinal Column Supports the skull, pectoral girdle, upper limbs and thoracic cage by way of the pelvic girdle. Transmits body weight
Nervous System: Spinal Cord and Spinal Nerves (Chapter 13)
") Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College Eastern Campus Primary Sources for figures and content: Marieb,
Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College Eastern Campus Primary Sources for figures and content: Marieb,
CANINE LUMBOSACRAL DISEASE
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk CANINE LUMBOSACRAL DISEASE Author : Brent Higgins Categories : Vets Date : April 6, 2009 Brent Higgins discusses differing
Vet Times The website for the veterinary profession https://www.vettimes.co.uk CANINE LUMBOSACRAL DISEASE Author : Brent Higgins Categories : Vets Date : April 6, 2009 Brent Higgins discusses differing
CHAPTER 13 LECTURE OUTLINE
 CHAPTER 13 LECTURE OUTLINE I. INTRODUCTION A. The spinal cord and spinal nerves mediate reactions to environmental changes. B. The spinal cord has several functions. 1. It processes reflexes. 2. It is
CHAPTER 13 LECTURE OUTLINE I. INTRODUCTION A. The spinal cord and spinal nerves mediate reactions to environmental changes. B. The spinal cord has several functions. 1. It processes reflexes. 2. It is
Chapter 13: The Spinal Cord and Spinal Nerves
 Chapter 13: The Spinal Cord and Spinal Nerves Spinal Cord Anatomy Protective structures: Vertebral column and the meninges protect the spinal cord and provide physical stability. a. Dura mater, b. Arachnoid,
Chapter 13: The Spinal Cord and Spinal Nerves Spinal Cord Anatomy Protective structures: Vertebral column and the meninges protect the spinal cord and provide physical stability. a. Dura mater, b. Arachnoid,
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and
 This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution
Chapter 12b. Overview
 Chapter 12b Spinal Cord Overview Spinal cord gross anatomy Spinal meninges Sectional anatomy Sensory pathways Motor pathways Spinal cord pathologies 1 The Adult Spinal Cord About 18 inches (45 cm) long
Chapter 12b Spinal Cord Overview Spinal cord gross anatomy Spinal meninges Sectional anatomy Sensory pathways Motor pathways Spinal cord pathologies 1 The Adult Spinal Cord About 18 inches (45 cm) long
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress ABNORMALITIES OF POSTURE AND APPEARANCE Rodney S. Bagley DVM, Diplomate, American College of Veterinary Internal
Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress ABNORMALITIES OF POSTURE AND APPEARANCE Rodney S. Bagley DVM, Diplomate, American College of Veterinary Internal
Proceedings of the European Veterinary Conference Voorjaarsdagen
 Close this window to return to IVIS www.ivis.org Proceedings of the European Veterinary Conference Voorjaarsdagen Apr. 13-15, 2016 Next Meeting: April 1 -, 201 The Hague, The Netherlands Reprinted in IVIS
Close this window to return to IVIS www.ivis.org Proceedings of the European Veterinary Conference Voorjaarsdagen Apr. 13-15, 2016 Next Meeting: April 1 -, 201 The Hague, The Netherlands Reprinted in IVIS
WHEN IS A SPINAL NOT A DISC PROLAPSE?
 WHEN IS A SPINAL NOT A DISC PROLAPSE? Dr Sara Boyd Johannesburg Specialist Veterinary Centre 63 Kayburne Venue Randpark Ridge Email: sara.boyd@jsvc.co.za ABSTRACT Dogs showing the early signs of spinal
WHEN IS A SPINAL NOT A DISC PROLAPSE? Dr Sara Boyd Johannesburg Specialist Veterinary Centre 63 Kayburne Venue Randpark Ridge Email: sara.boyd@jsvc.co.za ABSTRACT Dogs showing the early signs of spinal
DEGENERATIVE DISC DISEASE
 DEGENERATIVE DISC DISEASE What is a disc, and what is its purpose? The spinal cord is one of the most important and most sensitive organs in the body. If it is damaged the nerve cells do not regenerate
DEGENERATIVE DISC DISEASE What is a disc, and what is its purpose? The spinal cord is one of the most important and most sensitive organs in the body. If it is damaged the nerve cells do not regenerate
Neurologic examination- a practitioner's guide
 Neurologic examination- a practitioner's guide L Snow Department of Veterinary Clinical Sciences, School of Veterinary and Biological Sciences, Murdoch University, Murdoch, Western Australia 6150, Australia;
Neurologic examination- a practitioner's guide L Snow Department of Veterinary Clinical Sciences, School of Veterinary and Biological Sciences, Murdoch University, Murdoch, Western Australia 6150, Australia;
LOOKING AT BLINDNESS FROM NEUROLOGIST S PERSPECTIVE
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk LOOKING AT BLINDNESS FROM NEUROLOGIST S PERSPECTIVE Author : LAURENT S GAROSI Categories : Vets Date : June 23, 2008 LAURENT
Vet Times The website for the veterinary profession https://www.vettimes.co.uk LOOKING AT BLINDNESS FROM NEUROLOGIST S PERSPECTIVE Author : LAURENT S GAROSI Categories : Vets Date : June 23, 2008 LAURENT
The Neurologic Examination
 The Neurologic Examination Cheryl L. Chrisman, DVM, MS, EdS, DACVIM (Neurology) The neurologic examination is a series of observations and tests done to answer the following four questions: h Is a lesion
The Neurologic Examination Cheryl L. Chrisman, DVM, MS, EdS, DACVIM (Neurology) The neurologic examination is a series of observations and tests done to answer the following four questions: h Is a lesion
Arthritis. in dogs & cats
 Arthritis in dogs & cats What is Arthritis? Degenerative joint disease or arthritis is a common problem in dogs and cats as they age. In fact, arthritis affects one in five adult dogs. It is more prevalent
Arthritis in dogs & cats What is Arthritis? Degenerative joint disease or arthritis is a common problem in dogs and cats as they age. In fact, arthritis affects one in five adult dogs. It is more prevalent
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007 Hosted by: Australian Small Animal Veterinary Association (ASAVA) Australian Small Animal Veterinary Association (ASAVA)
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007 Hosted by: Australian Small Animal Veterinary Association (ASAVA) Australian Small Animal Veterinary Association (ASAVA)
3/3/2016. International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI)
") International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
Brain Stem. Nervous System (Part A-3) Module 8 -Chapter 14
 Module 8 -Chapter 14") Nervous System (Part A-3) Module 8 -Chapter 14 Overview Susie Turner, M.D. 1/9/13 Cellular structure of the nervous system Neurons Neuroglia Nervous System Divisions Central nervous system Peripheral nervous
Nervous System (Part A-3) Module 8 -Chapter 14 Overview Susie Turner, M.D. 1/9/13 Cellular structure of the nervous system Neurons Neuroglia Nervous System Divisions Central nervous system Peripheral nervous
Gross Morphology of Spinal Cord
 Gross Morphology of Spinal Cord Done By : Rahmeh Alsukkar ** I did my best and sorry for any mistake ** the sheet does not contain pictures, tables and some slides so please be careful and go back to slides
Gross Morphology of Spinal Cord Done By : Rahmeh Alsukkar ** I did my best and sorry for any mistake ** the sheet does not contain pictures, tables and some slides so please be careful and go back to slides
Making headway: problem-oriented approaches to neurological disease
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Making headway: problem-oriented approaches to neurological disease Author : Mark Lowrie Categories : Vets Date : July 4,
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Making headway: problem-oriented approaches to neurological disease Author : Mark Lowrie Categories : Vets Date : July 4,
Gross Anatomy of Lower Spinal Cord
 Chapter 13 Spinal Cord, Spinal Nerves and Somatic Reflexes Spinal cord Spinal nerves Somatic reflexes Gross Anatomy of Lower Spinal Cord Meninges of Vertebra & Spinal Cord Spina Bifida Congenital defect
Chapter 13 Spinal Cord, Spinal Nerves and Somatic Reflexes Spinal cord Spinal nerves Somatic reflexes Gross Anatomy of Lower Spinal Cord Meninges of Vertebra & Spinal Cord Spina Bifida Congenital defect
CHAPTER 10 THE SOMATOSENSORY SYSTEM
 CHAPTER 10 THE SOMATOSENSORY SYSTEM 10.1. SOMATOSENSORY MODALITIES "Somatosensory" is really a catch-all term to designate senses other than vision, hearing, balance, taste and smell. Receptors that could
CHAPTER 10 THE SOMATOSENSORY SYSTEM 10.1. SOMATOSENSORY MODALITIES "Somatosensory" is really a catch-all term to designate senses other than vision, hearing, balance, taste and smell. Receptors that could
The Nervous System: The
 C h a p t e r 14 The Nervous System: The Spinal Cord and Spinal Nerves PowerPoint Lecture Slides prepared by Jason LaPres North Harris College Houston, Texas Copyright 2009 Pearson Education, Inc., publishing
C h a p t e r 14 The Nervous System: The Spinal Cord and Spinal Nerves PowerPoint Lecture Slides prepared by Jason LaPres North Harris College Houston, Texas Copyright 2009 Pearson Education, Inc., publishing
A review of neurological examinationdifferential. diseases in cats and dogs
 A review of neurological examinationdifferential diagnosis for intracranial diseases in cats and dogs Picture source: https://www.fotolia.com/id/25810320 Authors: Raluca TURBATU, Cristina FERNOAGĂ, Nicolae
A review of neurological examinationdifferential diagnosis for intracranial diseases in cats and dogs Picture source: https://www.fotolia.com/id/25810320 Authors: Raluca TURBATU, Cristina FERNOAGĂ, Nicolae
Intervertebral Disc Disease and Nursing Care of the Down Dog. Deanna M. Swartzfager, RVT
 Intervertebral Disc Disease and Nursing Care of the Down Dog Deanna M. Swartzfager, RVT Intervertebral Disc Disease (IVDD) Syndrome of pain and neurologic deficits, and sometimes complete paralysis, resulting
Intervertebral Disc Disease and Nursing Care of the Down Dog Deanna M. Swartzfager, RVT Intervertebral Disc Disease (IVDD) Syndrome of pain and neurologic deficits, and sometimes complete paralysis, resulting
The Spinal Cord & Spinal Nerves
 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward and downward travel
The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward and downward travel
Study the Strut: Gait Changes in Dogs: Cased Based Analysis Mike Thoesen, DVM, DACVS th Ave NE, Shoreline, WA (206)
") Study the Strut: Gait Changes in Dogs: Cased Based Analysis Mike Thoesen, DVM, DACVS 14810 15th Ave NE, Shoreline, WA 98155 (206) 545-4322 September 17 th, 2017 Copyright 2015 Animal Surgical Clinic of
Study the Strut: Gait Changes in Dogs: Cased Based Analysis Mike Thoesen, DVM, DACVS 14810 15th Ave NE, Shoreline, WA 98155 (206) 545-4322 September 17 th, 2017 Copyright 2015 Animal Surgical Clinic of
Spinal cord. We have extension of the pia mater below L1-L2 called filum terminale
 Spinal cord Part of the CNS extend from foramen magnum to the level of L1-L2 (it is shorter than the vertebral column) it is covered by spinal meninges. It is cylindrical in shape. It s lower end become
Spinal cord Part of the CNS extend from foramen magnum to the level of L1-L2 (it is shorter than the vertebral column) it is covered by spinal meninges. It is cylindrical in shape. It s lower end become
ANATOMY OF SPINAL CORD. Khaleel Alyahya, PhD, MEd King Saud University School of
 ANATOMY OF SPINAL CORD Khaleel Alyahya, PhD, MEd King Saud University School of Medicine @khaleelya OBJECTIVES At the end of the lecture, students should be able to: Describe the external anatomy of the
ANATOMY OF SPINAL CORD Khaleel Alyahya, PhD, MEd King Saud University School of Medicine @khaleelya OBJECTIVES At the end of the lecture, students should be able to: Describe the external anatomy of the
Wildlife brain and spinal cord injuries
 Wildlife brain and spinal cord injuries Author: Georgina Child BVSc DACVIM (Neurology) University of Sydney Veterinary Teaching Hospital, Sydney Small Animal Specialist Hospital, North Ryde Introduction
Wildlife brain and spinal cord injuries Author: Georgina Child BVSc DACVIM (Neurology) University of Sydney Veterinary Teaching Hospital, Sydney Small Animal Specialist Hospital, North Ryde Introduction
Dr. Csébi Péter, Dr. Ipolyi Tamás Sebészeti Tanszék
 Dr. Csébi Péter, Dr. Ipolyi Tamás Sebészeti Tanszék Neurological examination is the most important part of the clinical evaluation of the neurological patient Auxilary examinations: Radiology, MRI, CT,
Dr. Csébi Péter, Dr. Ipolyi Tamás Sebészeti Tanszék Neurological examination is the most important part of the clinical evaluation of the neurological patient Auxilary examinations: Radiology, MRI, CT,
Surgery. Conus medullaris and Cauda Equina Syndromes. Anatomy. See online here
 Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Cranial Nerves and Spinal Cord Flashcards
 1. Name the cranial nerves and their Roman numeral. 2. What is Cranial Nerve I called, and what does it 3. Scientists who are trying to find a way to make neurons divide to heal nerve injuries often study
1. Name the cranial nerves and their Roman numeral. 2. What is Cranial Nerve I called, and what does it 3. Scientists who are trying to find a way to make neurons divide to heal nerve injuries often study
Spinal Cord Protection. Chapter 13 The Spinal Cord & Spinal Nerves. External Anatomy of Spinal Cord. Structures Covering the Spinal Cord
 Spinal Cord Protection Chapter 13 The Spinal Cord & Spinal Nerves We are only going to cover Pages 420-434 and 447 Together with brain forms the CNS Functions spinal cord reflexes integration (summation
Spinal Cord Protection Chapter 13 The Spinal Cord & Spinal Nerves We are only going to cover Pages 420-434 and 447 Together with brain forms the CNS Functions spinal cord reflexes integration (summation
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Properties of Purdue. Anatomy. Positioning AXIAL SKELETAL RADIOLOGY FOR PRIVATE PRACTITIONERS 11/30/2018
 AXIAL SKELETAL RADIOLOGY FOR PRIVATE PRACTITIONERS Anatomy Complex Text book is needed Species Contrast Positioning Painful/ non cooperative Sedation General anesthesia Species Contrast 1 Slightly oblique
AXIAL SKELETAL RADIOLOGY FOR PRIVATE PRACTITIONERS Anatomy Complex Text book is needed Species Contrast Positioning Painful/ non cooperative Sedation General anesthesia Species Contrast 1 Slightly oblique
Human Anatomy - Problem Drill 11: The Spinal Cord and Spinal Nerves
 Human Anatomy - Problem Drill 11: The Spinal Cord and Spinal Nerves Question No. 1 of 10 Instructions: (1) Read the problem statement and answer choices carefully, (2) Work the problems on paper as needed,
Human Anatomy - Problem Drill 11: The Spinal Cord and Spinal Nerves Question No. 1 of 10 Instructions: (1) Read the problem statement and answer choices carefully, (2) Work the problems on paper as needed,
50a A&P: Nervous System -! Peripheral Nervous System
 50a A&P: Nervous System -! Peripheral Nervous System 50a A&P: Nervous System -! Peripheral Nervous System! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:"
50a A&P: Nervous System -! Peripheral Nervous System 50a A&P: Nervous System -! Peripheral Nervous System! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:"
Proceedings of the 33rd World Small Animal Veterinary Congress
 www.ivis.org Proceedings of the 33rd World Small Animal Veterinary Congress Dublin, Ireland - 2008 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers 20 Neurology Com
www.ivis.org Proceedings of the 33rd World Small Animal Veterinary Congress Dublin, Ireland - 2008 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers 20 Neurology Com
Peripheral Nervous System Dr. Gary Mumaugh
 Peripheral Nervous System Dr. Gary Mumaugh Spinal Nerves Overview Thirty-one pairs of spinal nerves are connected to the spinal cord No special names; numbered by level of vertebral column at which they
Peripheral Nervous System Dr. Gary Mumaugh Spinal Nerves Overview Thirty-one pairs of spinal nerves are connected to the spinal cord No special names; numbered by level of vertebral column at which they
Sympathetic Nervous System
 Sympathetic Nervous System Lecture Objectives Review the subdivisions of the nervous system. Review the general arrangement and compare the sympathetic and parasympathetic parts. Describe the following
Sympathetic Nervous System Lecture Objectives Review the subdivisions of the nervous system. Review the general arrangement and compare the sympathetic and parasympathetic parts. Describe the following
The Spinal Cord. The Nervous System. The Spinal Cord. The Spinal Cord 1/2/2016. Continuation of CNS inferior to foramen magnum.
 The Nervous System Spinal Cord Continuation of CNS inferior to foramen magnum Simpler than the brain Conducts impulses to and from brain Two way conduction pathway Reflex actions Passes through vertebral
The Nervous System Spinal Cord Continuation of CNS inferior to foramen magnum Simpler than the brain Conducts impulses to and from brain Two way conduction pathway Reflex actions Passes through vertebral
Sir William Asher ANATOMY
 SPINAL CORD INJURY BASICS RELATED TO LIFE CARE PLANNING Lesson 1 Sir William Asher Picture the pathetic patient lying long abed, the urine leaking from his distended bladder, the lime draining from his
SPINAL CORD INJURY BASICS RELATED TO LIFE CARE PLANNING Lesson 1 Sir William Asher Picture the pathetic patient lying long abed, the urine leaking from his distended bladder, the lime draining from his
Spinal Cord Anatomy. Key Points. What is the spine? Areas of the spine: Spinal Cord Anatomy
 Spinal Cord Anatomy Authors: SCIRE Community Team Reviewed by: Riley Louie, PT Last updated: Sept 21, 2017 This page provides an overview of the structures of the spinal cord and how the spinal cord works.
Spinal Cord Anatomy Authors: SCIRE Community Team Reviewed by: Riley Louie, PT Last updated: Sept 21, 2017 This page provides an overview of the structures of the spinal cord and how the spinal cord works.
Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005
 Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA Laboratory
Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA Laboratory
Lab Activity 13. Spinal Cord. Portland Community College BI 232
 Lab Activity 13 Spinal Cord Portland Community College BI 232 Definitions Tracts: collections of axons in CNS Nerves:collections of axons in PNS Ganglia: collections of neuron cell bodies in PNS Nucleus
Lab Activity 13 Spinal Cord Portland Community College BI 232 Definitions Tracts: collections of axons in CNS Nerves:collections of axons in PNS Ganglia: collections of neuron cell bodies in PNS Nucleus
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Spinal Cord H. Ruth Clemo, Ph.D.
 Spinal Cord H. Ruth Clemo, Ph.D. OBJECTIVES After studying the material of this lecture, the student should be familiar with: 1. Surface anatomy of the spinal cord. 2. Internal structure and organization
Spinal Cord H. Ruth Clemo, Ph.D. OBJECTIVES After studying the material of this lecture, the student should be familiar with: 1. Surface anatomy of the spinal cord. 2. Internal structure and organization
Gross Morphology of Spinal Cord
 Gross Morphology of Spinal Cord Lecture Objectives Describe the gross anatomical features of the spinal cord. Describe the level of the different spinal segments compared to the level of their respective
Gross Morphology of Spinal Cord Lecture Objectives Describe the gross anatomical features of the spinal cord. Describe the level of the different spinal segments compared to the level of their respective
SENSORY (ASCENDING) SPINAL TRACTS
 SPINAL TRACTS") SENSORY (ASCENDING) SPINAL TRACTS Dr. Jamila El-Medany Dr. Essam Eldin Salama OBJECTIVES By the end of the lecture, the student will be able to: Define the meaning of a tract. Distinguish between the different
SENSORY (ASCENDING) SPINAL TRACTS Dr. Jamila El-Medany Dr. Essam Eldin Salama OBJECTIVES By the end of the lecture, the student will be able to: Define the meaning of a tract. Distinguish between the different
Synapse Homework. Back page last question not counted. 4 pts total, each question worth 0.18pts. 26/34 students answered correctly!
 Synapse Homework Back page last question not counted 26/34 students answered correctly! 4 pts total, each question worth 0.18pts Business TASS hours extended! MWF 1-2pm, Willamette 204 T and Th 9:30-10:30am,
Synapse Homework Back page last question not counted 26/34 students answered correctly! 4 pts total, each question worth 0.18pts Business TASS hours extended! MWF 1-2pm, Willamette 204 T and Th 9:30-10:30am,
Lecture 14: The Spinal Cord
 Lecture 14: The Spinal Cord M/O Chapters 16 69. Describe the relationship(s) between the following structures: root, nerve, ramus, plexus, tract, nucleus, and ganglion. 70. Trace the path of information
Lecture 14: The Spinal Cord M/O Chapters 16 69. Describe the relationship(s) between the following structures: root, nerve, ramus, plexus, tract, nucleus, and ganglion. 70. Trace the path of information
Human Nervous System:
 OLLI Brain: Making Sense of Our World: Lecture 3 Human Nervous System: The Motor & Sensory Divisions Copyright 2004 Pearson Education, Inc., publishing as Benjamin Cummings Organization of the Nervous
OLLI Brain: Making Sense of Our World: Lecture 3 Human Nervous System: The Motor & Sensory Divisions Copyright 2004 Pearson Education, Inc., publishing as Benjamin Cummings Organization of the Nervous
Chapter 13 PNS and reflex activity
 Chapter 13 PNS and reflex activity I. Peripheral nervous system A. PNS links CNS to the body B. Sensory: the afferent division C. Motor: the efferent division D. Ganglia: collections of cell bodies in
Chapter 13 PNS and reflex activity I. Peripheral nervous system A. PNS links CNS to the body B. Sensory: the afferent division C. Motor: the efferent division D. Ganglia: collections of cell bodies in
LESION LOCALIZATION AND DIFFERENTIAL DIAGNOSIS OF NEUROLOGICAL DISEASE
 THE NEUROANATOMIC DIAGNOSIS WHERE S THE LESION? Scott J. Schatzberg, DVM, PhD, DACVIM (Neurology) The Animal Neurology & Imaging Center Albuquerque, NM LESION LOCALIZATION AND DIFFERENTIAL DIAGNOSIS OF
THE NEUROANATOMIC DIAGNOSIS WHERE S THE LESION? Scott J. Schatzberg, DVM, PhD, DACVIM (Neurology) The Animal Neurology & Imaging Center Albuquerque, NM LESION LOCALIZATION AND DIFFERENTIAL DIAGNOSIS OF
Overview. Spinal Anatomy Spaces & Meninges Spinal Cord. Anatomy of the dura. Anatomy of the arachnoid. Anatomy of the spinal meninges
 European Course in Neuroradiology Module 1 - Anatomy and Embryology Dubrovnik, October 2018 Spinal Anatomy Spaces & Meninges Spinal Cord Johan Van Goethem Overview spinal meninges & spaces spinal cord
European Course in Neuroradiology Module 1 - Anatomy and Embryology Dubrovnik, October 2018 Spinal Anatomy Spaces & Meninges Spinal Cord Johan Van Goethem Overview spinal meninges & spaces spinal cord
THE BACK. Dr. Ali Mohsin. Spinal Cord
 Spinal Cord THE BACK Dr. Ali Mohsin The spinal cord is the elongated caudal part of the CNS. It starts as the inferior continuation of the medulla oblongata at the level of foramen magnum, & ends as an
Spinal Cord THE BACK Dr. Ali Mohsin The spinal cord is the elongated caudal part of the CNS. It starts as the inferior continuation of the medulla oblongata at the level of foramen magnum, & ends as an
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes
 Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Chapter 13! Chapter 13 Spinal Cord and Spinal Nerves! The Spinal Cord and Spinal Nerves!
 Chapter 13! The Spinal Cord and Spinal Nerves! SECTION 13-1! The brain and spinal cord make up the central nervous system, and the cranial nerves and spinal nerves constitute the peripheral nervous system!
Chapter 13! The Spinal Cord and Spinal Nerves! SECTION 13-1! The brain and spinal cord make up the central nervous system, and the cranial nerves and spinal nerves constitute the peripheral nervous system!
Principles of Anatomy and Physiology
 Principles of Anatomy and Physiology 14 th Edition CHAPTER 15 The Autonomic Nervous System Comparison of Somatic and Autonomic Nervous Systems The somatic nervous system includes both sensory and motor
Principles of Anatomy and Physiology 14 th Edition CHAPTER 15 The Autonomic Nervous System Comparison of Somatic and Autonomic Nervous Systems The somatic nervous system includes both sensory and motor
RETROLISTHESIS. Retrolisthesis. is found mainly in the cervical spine and lumbar region but can also be often seen in the thoracic spine
 RETROLISTHESIS A retrolisthesis is a posterior displacement of one vertebral body with respect to adjacent vertebrae Typically a vertebra is to be in retrolisthesis position when it translates backward
RETROLISTHESIS A retrolisthesis is a posterior displacement of one vertebral body with respect to adjacent vertebrae Typically a vertebra is to be in retrolisthesis position when it translates backward
Nervous System. The Peripheral Nervous System Agenda Review of CNS v. PNS PNS Basics Cranial Nerves Spinal Nerves Reflexes Pathways
 Nervous System Agenda Review of CNS v. PNS PNS Basics Cranial Nerves Spinal Nerves Sensory Motor Review of CNS v. PNS Central nervous system (CNS) Brain Spinal cord Peripheral nervous system (PNS) All
Nervous System Agenda Review of CNS v. PNS PNS Basics Cranial Nerves Spinal Nerves Sensory Motor Review of CNS v. PNS Central nervous system (CNS) Brain Spinal cord Peripheral nervous system (PNS) All
RADICULOPATHY AN INTRODUCTION TO
 AN INTRODUCTION TO RADICULOPATHY This booklet provides general information on radiculopathy. It is not meant to replace any personal conversations that you might wish to have with your physician or other
AN INTRODUCTION TO RADICULOPATHY This booklet provides general information on radiculopathy. It is not meant to replace any personal conversations that you might wish to have with your physician or other
Nervous system. The main regulation mechanism of organism's functions
 Nervous system The main regulation mechanism of organism's functions Questions Neuron The reflex arc The nervous centers Properties of the nervous centers The general principles of coordination Inhibition
Nervous system The main regulation mechanism of organism's functions Questions Neuron The reflex arc The nervous centers Properties of the nervous centers The general principles of coordination Inhibition
HERNIATED DISCS AN INTRODUCTION TO
 AN INTRODUCTION TO HERNIATED S This booklet provides general information on herniated discs. It is not meant to replace any personal conversations that you might wish to have with your physician or other
AN INTRODUCTION TO HERNIATED S This booklet provides general information on herniated discs. It is not meant to replace any personal conversations that you might wish to have with your physician or other
NERVOUS SYSTEM ANATOMY
 INTRODUCTION to NERVOUS SYSTEM ANATOMY M1 - Gross and Developmental Anatomy Dr. Milton M. Sholley Professor of Anatomy and Neurobiology and Dr. Michael H. Peters Professor of Chemical and Life Science
INTRODUCTION to NERVOUS SYSTEM ANATOMY M1 - Gross and Developmental Anatomy Dr. Milton M. Sholley Professor of Anatomy and Neurobiology and Dr. Michael H. Peters Professor of Chemical and Life Science
Reflexes. Dr. Baizer
 Reflexes Dr. Baizer 1 Learning objectives: reflexes Students will be able to describe: 1. The clinical importance of testing reflexes. 2. The essential components of spinal reflexes. 3.The stretch reflex.
Reflexes Dr. Baizer 1 Learning objectives: reflexes Students will be able to describe: 1. The clinical importance of testing reflexes. 2. The essential components of spinal reflexes. 3.The stretch reflex.
Nervous System C H A P T E R 2
 Nervous System C H A P T E R 2 Input Output Neuron 3 Nerve cell Allows information to travel throughout the body to various destinations Receptive Segment Cell Body Dendrites: receive message Myelin sheath
Nervous System C H A P T E R 2 Input Output Neuron 3 Nerve cell Allows information to travel throughout the body to various destinations Receptive Segment Cell Body Dendrites: receive message Myelin sheath
Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc. Copyright 2014, 2011, 2006 by Saunders, an imprint of Elsevier, Inc.
 Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc 1 Spinal Cord Injury Results from fracture and/or dislocation of vertebrae // Compresses, stretches, or tears spinal cord Cervical
Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc 1 Spinal Cord Injury Results from fracture and/or dislocation of vertebrae // Compresses, stretches, or tears spinal cord Cervical
Spinal Cord Organization. January 12, 2011
 Spinal Cord Organization January 12, 2011 Spinal Cord 31 segments terminates at L1-L2 special components - conus medullaris - cauda equina no input from the face Spinal Cord, Roots & Nerves Dorsal root
Spinal Cord Organization January 12, 2011 Spinal Cord 31 segments terminates at L1-L2 special components - conus medullaris - cauda equina no input from the face Spinal Cord, Roots & Nerves Dorsal root
PNS and ANS Flashcards
 1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
Chapter 17 Nervous System
 Chapter 17 Nervous System 1 The Nervous System Two Anatomical Divisions Central Nervous System (CNS) Brain and Spinal Cord Peripheral Nervous System (PNS) Two Types of Cells Neurons Transmit nerve impulses
Chapter 17 Nervous System 1 The Nervous System Two Anatomical Divisions Central Nervous System (CNS) Brain and Spinal Cord Peripheral Nervous System (PNS) Two Types of Cells Neurons Transmit nerve impulses
This article describes the clinically relevant anatomic components
 3 CE Credits Vestibular Disease: Anatomy, Physiology, and Clinical Signs Mark Lowrie, MA VetMB, MVM, DECVN, MRCVS Davies Veterinary Specialists Higham Gobion, Hertfordshire United Kingdom Abstract: The
3 CE Credits Vestibular Disease: Anatomy, Physiology, and Clinical Signs Mark Lowrie, MA VetMB, MVM, DECVN, MRCVS Davies Veterinary Specialists Higham Gobion, Hertfordshire United Kingdom Abstract: The
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Clinical examination of the dog with thoracic limb lameness
 Clinical examination of the dog with thoracic limb lameness Examination of the patient Examination of the patient with musculoskeletal disease should start with a general physical examination. Particular
Clinical examination of the dog with thoracic limb lameness Examination of the patient Examination of the patient with musculoskeletal disease should start with a general physical examination. Particular
Chapter 14. The Nervous System. The Spinal Cord and Spinal Nerves. Lecture Presentation by Steven Bassett Southeast Community College
 Chapter 14 The Nervous System The Spinal Cord and Spinal Nerves Lecture Presentation by Steven Bassett Southeast Community College Introduction The Central Nervous System (CNS) consists of: The spinal
Chapter 14 The Nervous System The Spinal Cord and Spinal Nerves Lecture Presentation by Steven Bassett Southeast Community College Introduction The Central Nervous System (CNS) consists of: The spinal
Tymaa Al-zaben & Amin Al-ajalouni
 Done by: Tymaa Al-zaben & Amin Al-ajalouni ** Hello SERTONIN! SLIDE 3 note:: the slide included within the sheet but make sure back to slide for pictures The Autonomic Nervous System Function : Regulate
Done by: Tymaa Al-zaben & Amin Al-ajalouni ** Hello SERTONIN! SLIDE 3 note:: the slide included within the sheet but make sure back to slide for pictures The Autonomic Nervous System Function : Regulate
Nervous system. Made up of. Peripheral nervous system. Central nervous system. The central nervous system The peripheral nervous system.
 Made up of The central nervous system The peripheral nervous system Nervous system Central nervous system Peripheral nervous system Brain Spinal Cord Cranial nerve Spinal nerve branch from the brain connect
Made up of The central nervous system The peripheral nervous system Nervous system Central nervous system Peripheral nervous system Brain Spinal Cord Cranial nerve Spinal nerve branch from the brain connect
Acute Thoracolumbar IVD Extrusion. Tracy Sutton, DVM, DACVIM (Neurology)
") Acute Thoracolumbar IVD Extrusion Tracy Sutton, DVM, DACVIM (Neurology) CONTACT INFORMATION Austin Veterinary Emergency Specialty Center (AVES) 7300 Ranch Road 2222, Austin, TX 78730 (512) 343-2837 DrSutton@AustinVets.com
Acute Thoracolumbar IVD Extrusion Tracy Sutton, DVM, DACVIM (Neurology) CONTACT INFORMATION Austin Veterinary Emergency Specialty Center (AVES) 7300 Ranch Road 2222, Austin, TX 78730 (512) 343-2837 DrSutton@AustinVets.com
Human Anatomy. Autonomic Nervous System
 Human Anatomy Autonomic Nervous System 1 Autonomic Nervous System ANS complex system of nerves controls involuntary actions. Works with the somatic nervous system (SNS) regulates body organs maintains
Human Anatomy Autonomic Nervous System 1 Autonomic Nervous System ANS complex system of nerves controls involuntary actions. Works with the somatic nervous system (SNS) regulates body organs maintains
Done By: manar aljebreen Abdulrahman alsharidah
 Female Side Male side Done By: manar aljebreen Abdulrahman alsharidah Revised By: Nour Al-Khawajah Mohammed Asiri 2 Slide No.( 1 ) Slide No.( 2 ) 3 Slide No.( 3 ) Slide No.( 4 ) Upper motor neurons are
Female Side Male side Done By: manar aljebreen Abdulrahman alsharidah Revised By: Nour Al-Khawajah Mohammed Asiri 2 Slide No.( 1 ) Slide No.( 2 ) 3 Slide No.( 3 ) Slide No.( 4 ) Upper motor neurons are
Evaluation and Management of Spinal Cord Emergency and Cervical Spondylotic Myelopathy
 Evaluation and Management of Spinal Cord Emergency and Cervical Spondylotic Myelopathy James J. Lehman, DC, MBA, FACO Associate Professor of Clinical Sciences University of Bridgeport College of Chiropractic
Evaluation and Management of Spinal Cord Emergency and Cervical Spondylotic Myelopathy James J. Lehman, DC, MBA, FACO Associate Professor of Clinical Sciences University of Bridgeport College of Chiropractic
Dry Needle Acupuncture In Locomotory Paresis Post Column Trauma In Dog Case Study
 Dry Needle Acupuncture In Locomotory Paresis Post Column Trauma In Dog Case Study C lin I. Hulea, Marius C. Pentea, Romeo T. Cristina, Eugenia Dumitrescu Paresis and paralysis are manifested by total or
Dry Needle Acupuncture In Locomotory Paresis Post Column Trauma In Dog Case Study C lin I. Hulea, Marius C. Pentea, Romeo T. Cristina, Eugenia Dumitrescu Paresis and paralysis are manifested by total or
Nervous system Reflexes and Senses
 Nervous system Reflexes and Senses Physiology Lab-4 Wrood Slaim, MSc Department of Pharmacology and Toxicology University of Al-Mustansyria 2017-2018 Nervous System The nervous system is the part of an
Nervous system Reflexes and Senses Physiology Lab-4 Wrood Slaim, MSc Department of Pharmacology and Toxicology University of Al-Mustansyria 2017-2018 Nervous System The nervous system is the part of an
Neurological examination of the horse
 Neurological examination of the horse Aim of the neurological examination Is there a neurological disease? Anatomical location of the problem? Diagnosis? Are there therapeutic options? What is the prognosis?
Neurological examination of the horse Aim of the neurological examination Is there a neurological disease? Anatomical location of the problem? Diagnosis? Are there therapeutic options? What is the prognosis?
Patient Information MIS TLIF. Transforaminal Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques
 Patient Information MIS TLIF Transforaminal Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques MIS TLIF Table of Contents Anatomy of Spine...2 General Conditions of the Spine...4 6 MIS-TLIF
Patient Information MIS TLIF Transforaminal Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques MIS TLIF Table of Contents Anatomy of Spine...2 General Conditions of the Spine...4 6 MIS-TLIF
CHAPTER 3 THE STRUCTURE OF THE NERVOUS SYSTEM
 CHAPTER 3 THE STRUCTURE OF THE NERVOUS SYSTEM 3.1. THE BASIC STRUCTURE OF THE NERVOUS SYSTEM. The nervous system of all animals is made up of groups of neurons that receive information from sensory systems,
CHAPTER 3 THE STRUCTURE OF THE NERVOUS SYSTEM 3.1. THE BASIC STRUCTURE OF THE NERVOUS SYSTEM. The nervous system of all animals is made up of groups of neurons that receive information from sensory systems,
NERVOUS SYSTEM ANATOMY
 NTRODUCTON to NERVOUS SYSTEM ANATOMY M1 - Gross and Developmental Anatomy Dr. Milton M. Sholley Professor of Anatomy and Neurobiology and Dr. Michael H. Peters Professor of Chemical and Life Science Engineering
NTRODUCTON to NERVOUS SYSTEM ANATOMY M1 - Gross and Developmental Anatomy Dr. Milton M. Sholley Professor of Anatomy and Neurobiology and Dr. Michael H. Peters Professor of Chemical and Life Science Engineering