Dr Charlie Baker Consultant Anaesthetist UHNM. Being a place our f amilies would choose
|
|
|
- Susan McCarthy
- 5 years ago
- Views:
Transcription
1 Dr Charlie Baker Consultant Anaesthetist UHNM Being a place our f amilies would choose
2 The story so far: Anaemia is associated with transfusion. The more anaemic you are pre op the more likely you are to require a transfusion. Anaemia is associated with increased post op morbidity & mortality independent of transfusion. Being a place our f amilies would choose
3
4
5
6
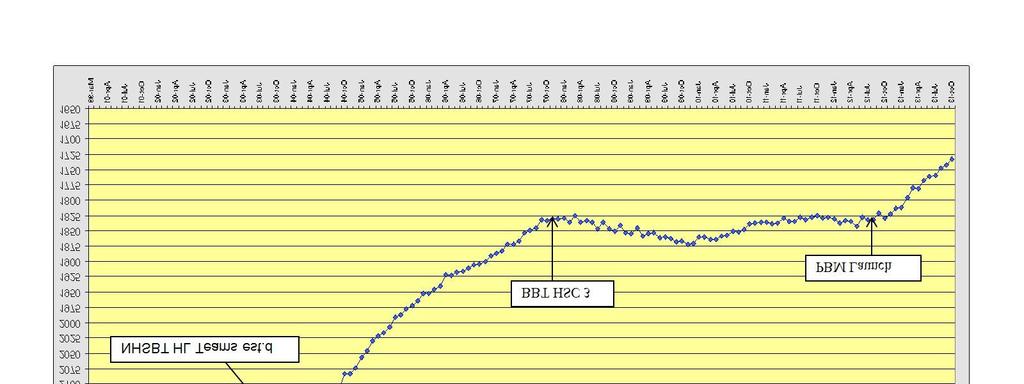
7 Supposition, correcting pre op anaemia will reduce: Requirement for transfusion Reduce morbidity and mortality Reduce length of stay Reduce cost of health care PREVENTT trial (PREoperative intravenous iron To Treat anaemia in major surgery) Being a place our f amilies would choose
8 PREVENTT Major surgery Hb >90g/ litre <120g/ litre Single dose of iv iron Logistical problems Infusion days pre op. Being a place our f amilies would choose
9 PRE-OPERATIVE MANAGEMENT HAEMATOLOGY We already have guidelines: West Mercia clinical guidelines West Midlands RTC guidelines HAEMOGLOBIN Investigate and treat unexpected anaemia. Anaemia is defined by WHO as Hb <13 g/dl in men and Hb <12 g/dl in women. See Algorithm for management of unexpected pre-operative anaemia in patients with shortness of breath or worsening angina caused by anaemia, consider blood transfusion see Chronic anaemia transfusion flowchart in Medical guidelines and postpone operation until asymptomatic Prescribe oral iron for patients with surgical conditions known to predispose to ongoing blood loss from time of diagnosis until condition treated if surgery urgent (cancer surgery) or operation required within 2 weeks, consider preoperative use of intravenous iron, vitamin B12 injections and folate as guided by assays; use blood transfusion only when there has been insufficient response to haematinic agents and patient is symptomatic of anaemia In patients with anaemia associated with chronic diseases, such as chronic renal failure or rheumatoid arthritis with Hb <12 g/dl, consider intravenous iron to treat functional iron deficiency state such patients may subsequently undergo surgery, despite a persistently low Hb, but take into account risk of bleeding during surgery and discuss transfusion requirements with blood bank taking in to account the Maximum surgical blood ordering schedule (MSBOS) guideline and patient s usual haemoglobin level if pre-operative patient has iron deficiency or functional iron deficiency state and is unable to take/tolerate oral iron, treat as soon as possible with IV iron as out-patient after checking with consultant surgeon Algorithm for management of unexpected pre-operative anaemia Female: Hb 12.0 g/dl Male: Hb 13.0 g/dl List for surgery. If major surgery planned, consider up to 4 week course of ferrous sulphate (maximum 200 mg orally 8-hrly) if tolerated, to improve iron stores Female: Hb g/dl Male: Hb g/dl Check MCV Hb <10.0 g/dl Defer operation unless urgent. Take blood for serum ferritin/b12/folate and consider haematology referral via GP Microcytic (MCV <80) Exclude iron deficiency Take blood for serum ferritin and start oral ferrous sulphate up to 200 mg 8-hrly, if tolerated, for 4 weeks pre-op Normocytic (MCV ) or macrocytic (MCV >100) Exclude B12/folate/iron deficiency Take blood for vitamin B12 folate and ferritin. Await results before considering treatment While patient remains on waiting list, Refer back to GP with ferritin result While patient remains on waiting list, Refer back to GP with results GP to review results, adjust medication as necessary and/or initiate investigation if appropriate GP to re-refer for surgery when patient has been fully investigated and treated Even a short course of iron can be effective in raising haemoglobin and reducing the need for blood transfusion Being a place our f amilies would choose
10 Guidelines for the Management W e s t M id la n d s of Anaemia in Pre-operative Assessment Clinics (2007) Some key recommendations: The GP should identify and treat anaemia before referral wherever possible Pre-operative assessment should take place at least 4 weeks prior to surgery, and ideally immediately following the decision to operate All patients who are identified as at risk of requiring a blood transfusion should have FBC assessed at PAC. These patients should also be given information about the possibility of requiring a blood transfusion All FBC results should be reviewed within 2 working days The definition of anaemia should be based on WHO classifications Male Hb <13g/dl / Female Hb <12g/dl Anaemic results should be seen by a member of the clinical team who has sufficient authority to commence treatment, refer for further investigation or delay surgery.

11 Being a place our f amilies would choose

12 Is treatment of anaemia initiated by the POAC 2013 survey results only West Midlands If yes what treatments are initiated? Routinely Regularly Rarely Never Oral Iron IV iron Transfusion
13 Battles to be fought: Availability of suitable iv iron preparation Selection of appropriate treatment once anaemia identified Recognition of anaemia Somewhere to give iv iron Someone to give iv iron Control of the waiting lists Being a place our f amilies would choose
14
15
16 Recognition of anaemia Talk to the pre operative assessment nurses Referrals made to me Treatment initiated Consultants advised Talk on stat & mandatory training to Consultant staff Being a place our f amilies would choose
17 Being a place our f amilies would choose

18 Being a place our f amilies would choose
19 Item Name 24/07/ :58 Ferritin. Haemoglobin 96 White Cell Count 5.7 Platelet Count 359 Red Blood Cell 4.28 Haematocrit 0.32 Mean Cell Volume 74.8 Mean Cell Haemoglobin 22.5 Absolute Neutrophil Count 3.8 Absolute Lymphocyte Count 1.4 Absolute Monocyte Count 0.2 Absolute Eosinphil Count 0.1 Absolute Basophil Count 0 Absolute Large Unstained Cell Count 0.1 ESR. 5 Prothrombin INR. APTT Ratio
20 Item Name 24/07/ :58 19/02/ :15 Ferritin. 4 Haemoglobin White Cell Count Platelet Count Red Blood Cell Haematocrit Mean Cell Volume Mean Cell Haemoglobin Absolute Neutrophil Count Absolute Lymphocyte Count Absolute Monocyte Count Absolute Eosinphil Count Absolute Basophil Count 0 0 Absolute Large Unstained Cell Count ESR. 5 2 Prothrombin INR. APTT Ratio
21 Item Name 24/07/ :58 19/02/ :15 25/07/ :00 Ferritin. 4 5 Haemoglobin White Cell Count Platelet Count Red Blood Cell Haematocrit Mean Cell Volume Mean Cell Haemoglobin Absolute Neutrophil Count Absolute Lymphocyte Count Absolute Monocyte Count Absolute Eosinphil Count Absolute Basophil Count Absolute Large Unstained Cell Count
22 Item Name 24/07/ :58 19/02/ :15 25/07/ :00 29/07/ :10 24/10/ :42 Ferritin Haemoglobin White Cell Count Platelet Count Red Blood Cell Haematocrit Mean Cell Volume Mean Cell Haemoglobin Absolute Neutrophil Count Absolute Lymphocyte Count Absolute Monocyte Count Absolute Eosinphil Count Absolute Basophil Count Absolute Large Unstained Cell Count ESR. 5 2 Prothrombin INR APTT Ratio
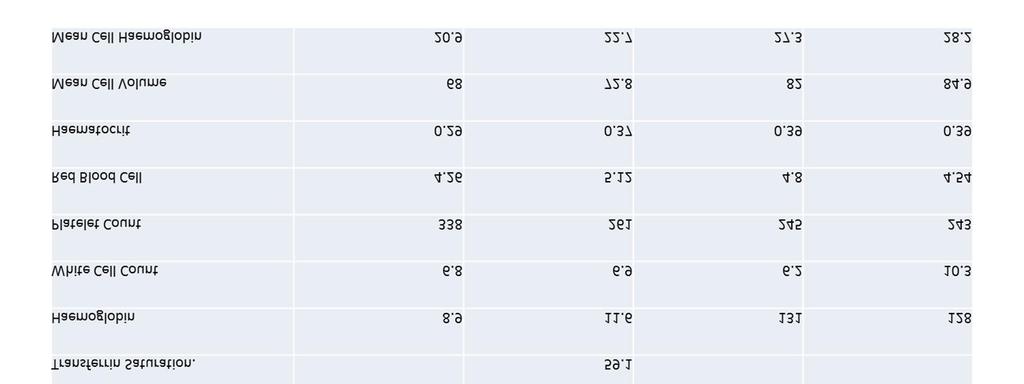
23 Item Name 20/06/ :13 Magnesium. Serum B12. Serum Folate. Ferritin. Transferrin. Serum Iron. Transferrin Saturation. Aspartate Transaminase. CRP - Wide Range. Prothrombin INR. Haemoglobin 107 White Cell Count 7 Platelet Count 240 Red Blood Cell 4.61 Haematocrit 0.33 Mean Cell Volume 71.8 Mean Cell Haemoglobin 23.3 Absolute Neutrophil Count 4.9 Absolute Lymphocyte Count 1.1 Absolute Monocyte Count 0.6 Absolute Eosinphil Count 0.2 Absolute Basophil Count 0.1 Absolute Large Unstained Cell Count 0.2 Percentage Reticulocyte Count Absolute Reticulocyte Count Direct Antiglobulin Test. APTT Ratio
24 Item Name 14/03/ :50 20/06/ :13 Magnesium. Serum B12. Serum Folate. Ferritin. Transferrin. Serum Iron. Transferrin Saturation. Aspartate Transaminase. CRP - Wide Range. Prothrombin INR. Haemoglobin White Cell Count Platelet Count Red Blood Cell Haematocrit Mean Cell Volume Mean Cell Haemoglobin Absolute Neutrophil Count Absolute Lymphocyte Count Absolute Monocyte Count Absolute Eosinphil Count Absolute Basophil Count Absolute Large Unstained Cell Count Percentage Reticulocyte Count Absolute Reticulocyte Count Direct Antiglobulin Test. APTT Ratio
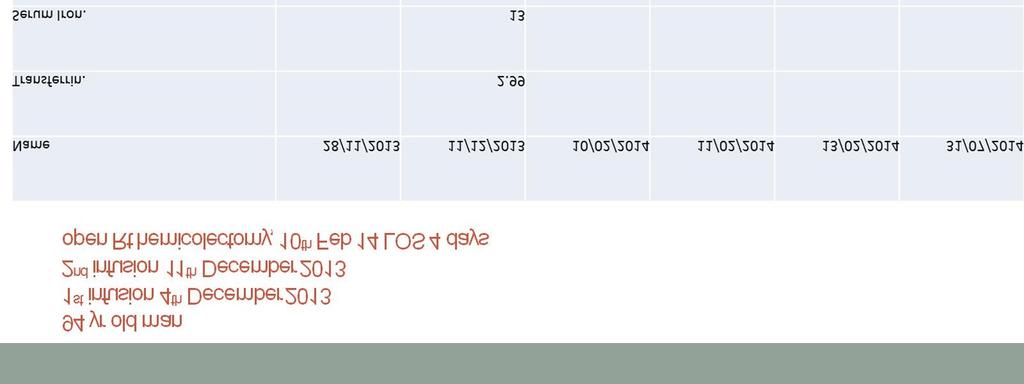
25 Item Name 14/03/ :50 20/06/ :13 14/11/ :30 Magnesium. Serum B Serum Folate. 6.8 Ferritin. Result was 7 ng/ ml 17 days ago Transferrin Serum Iron. 5 Transferrin Saturation. 5.7 Aspartate Transaminase. CRP - Wide Range. Prothrombin INR. Haemoglobin White Cell Count Platelet Count Red Blood Cell Haematocrit Mean Cell Volume Mean Cell Haemoglobin Absolute Neutrophil Count Absolute Lymphocyte Count Absolute Monocyte Count Absolute Eosinphil Count Absolute Basophil Count Absolute Large Unstained Cell Count Percentage Reticulocyte Count Absolute Reticulocyte Count Direct Antiglobulin Test. APTT Ratio
26 Item Name 14/03/ :50 20/06/ :13 14/11/ :30 20/11/ :40 21/11/ :24 27/11/ :12 Magnesium. Serum B Serum Folate. 6.8 Ferritin. Result was 7 ng/ ml 17 days ago Transferrin Serum Iron Transferrin Saturation. 5.7 Aspartate Transaminase. 19 CRP - Wide Range. <4.0 <4.0 Prothrombin INR Haemoglobin White Cell Count Platelet Count Red Blood Cell Haematocrit Mean Cell Volume Mean Cell Haemoglobin Absolute Neutrophil Count Absolute Lymphocyte Count Absolute Monocyte Count Absolute Eosinphil Count Absolute Basophil Count Absolute Large Unstained Cell Count Percentage Reticulocyte Count 3.2 Absolute Reticulocyte Count Direct Antiglobulin Test. Negative APTT Ratio 0.95
27 Failures Time to surgery. CT PET scan but no bloods Last Thursday Control of waiting lists Success Upper GI interested in prehabilitation now Last Friday Being a place our f amilies would choose
28 Achievements to date: Education of PREAMS staff Referrals from them Referrals from some surgeons >50 iv iron infusions to date No adverse reactions even in a patient who had previously reacted to iron dextran iv iron given in PREAMS clinics both in County site and Royal site (by me) Being a place our f amilies would choose
29 SA03D Haemolytic Anaemia with CC , No HRG SA03F Haemolytic Anaemia without CC , No HRG SA04D Iron Deficiency Anaemia with CC , No HRG SA04F Iron Deficiency Anaemia without CC No HRG SA05D Megaloblastic Anaemia with CC , No HRG SA05F Megaloblastic Anaemia without CC Best practice tariff SA03D Haemolytic Anaemia with CC , No HRG SA04D Iron Deficiency Anaemia with CC 2,171 1,929 Anaemia SA04F Iron Deficiency Anaemia without CC 1, Being a place our f amilies would choose 2,828 2,586 SA03F Haemolytic Anaemia without CC 2,050 1,807 SA05D Megaloblastic Anaemia with CC 2,072 1,830 SA05F Megaloblastic Anaemia without CC 1,366 1,124 HRG BP54

30
31
32
 Peer pressure Systems approach")
33 What will improve anaemia management? Editorials and journal articles (BMJ & BJA) Peer pressure Systems approach Being a place our f amilies would choose
34
35 Our mission To be un-noticed To ensure all patients turn up in theatre nonanaemic As a consequence improve outcomes, reduce lengths of stay Let the surgeons take the glory but be self satisfied that we have made the difference! Ensure that blood is transfused appropriately in all specialties 25 unit ptp Being a place our f amilies would choose

36 Being a place our f amilies would choose
Pre-operative Assessment
 Pre-operative Assessment Dr Craig Taylor Andrea Harris On behalf of the WM RTC Audit Group A good example of an audit cycle...... or is it!!?? Identify Better Blood Transfusion 2002 2007 West Midlands
Pre-operative Assessment Dr Craig Taylor Andrea Harris On behalf of the WM RTC Audit Group A good example of an audit cycle...... or is it!!?? Identify Better Blood Transfusion 2002 2007 West Midlands
Managing peri-operative anaemiathe Papworth way. Dr Andrew A Klein Royal Papworth Hospital Cambridge UK
 Managing peri-operative anaemiathe Papworth way Dr Andrew A Klein Royal Papworth Hospital Cambridge UK Conflicts of interest: Unrestricted educational grants/honoraria from CSL Behring, Brightwake Ltd,
Managing peri-operative anaemiathe Papworth way Dr Andrew A Klein Royal Papworth Hospital Cambridge UK Conflicts of interest: Unrestricted educational grants/honoraria from CSL Behring, Brightwake Ltd,
PREOPERATIVE ANAEMIA PATHWAY
 PREOPERATIVE ANAEMIA PATHWAY Surname: Patient ID No. Forename: DOB: / / Age: NHS Number: Likes to be called: Address: Tel. No. Religion/Spirituality: Next of Kin: Name GP Name: GP Practice: Planned Operation:
PREOPERATIVE ANAEMIA PATHWAY Surname: Patient ID No. Forename: DOB: / / Age: NHS Number: Likes to be called: Address: Tel. No. Religion/Spirituality: Next of Kin: Name GP Name: GP Practice: Planned Operation:
Julie Ball SHOT Clinical Incidents Specialist
 Julie Ball SHOT Clinical Incidents Specialist Surveillance procedures from the collection of blood and its components to the follow up of the recipients To collect and assess information on unexpected
Julie Ball SHOT Clinical Incidents Specialist Surveillance procedures from the collection of blood and its components to the follow up of the recipients To collect and assess information on unexpected
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant
 Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include:
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include:
IRON DEFICIENCY / ANAEMIA ANTHONY BEETON
 IRON DEFICIENCY / ANAEMIA ANTHONY BEETON HYPOXIA 1-2 mg IRON Labile iron Body iron ± 3 4 g Liver and the reticuloendothelial system and spleen (approximately 200 300 mg in adult women and 1 g in adult
IRON DEFICIENCY / ANAEMIA ANTHONY BEETON HYPOXIA 1-2 mg IRON Labile iron Body iron ± 3 4 g Liver and the reticuloendothelial system and spleen (approximately 200 300 mg in adult women and 1 g in adult
West Midlands Regional Transfusion Committee (RTC) Guidelines for the management of anaemia in pre-operative assessment clinics
 Guidelines for the management of anaemia in pre-operative assessment clinics") West Midlands West Midlands Regional Transfusion Committee (RTC) Guidelines for the management of anaemia in pre-operative assessment clinics Blest, A. 1, Baker, C. 2, Taylor, C. 3, Brothwood, D. 4, Bramhall,
West Midlands West Midlands Regional Transfusion Committee (RTC) Guidelines for the management of anaemia in pre-operative assessment clinics Blest, A. 1, Baker, C. 2, Taylor, C. 3, Brothwood, D. 4, Bramhall,
Classification of Anaemia
 Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
Pre-operative Anaemia Colorectal and Orthopaedic Surgery
 Pre-operative Anaemia Colorectal and Orthopaedic Surgery Dr Simon Rang Consultant Anaesthetist East Kent Hospitals NHS Trust Dreamland Pre-operative Anaemia Anaemia is a perioperative risk factor Perioperative
Pre-operative Anaemia Colorectal and Orthopaedic Surgery Dr Simon Rang Consultant Anaesthetist East Kent Hospitals NHS Trust Dreamland Pre-operative Anaemia Anaemia is a perioperative risk factor Perioperative
Anaemia Patient information
 Anaemia Patient information What is anaemia? Anaemia is the result of either not having enough red cells to take oxygen around the body, or having faulty red cells that are unable to carry enough oxygen.
Anaemia Patient information What is anaemia? Anaemia is the result of either not having enough red cells to take oxygen around the body, or having faulty red cells that are unable to carry enough oxygen.
DETECTION, INVESTIGATION AND MANAGEMENT OF ANAEMIA
 From the Chief Medical Officer Dr Michael McBride HSS(MD) 22/2012 Circulation list: For Action: Chief Executives of HSC Trusts Medical Directors of HSC Trusts (for onward distribution to All Hospital Doctors)
From the Chief Medical Officer Dr Michael McBride HSS(MD) 22/2012 Circulation list: For Action: Chief Executives of HSC Trusts Medical Directors of HSC Trusts (for onward distribution to All Hospital Doctors)
FBC interpretation. Dr. Gergely Varga
 FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
Gemcitabine & Cisplatin
 Gemcitabine & Cisplatin Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community Burton out-patient Derby out-patient Indication Advanced
Gemcitabine & Cisplatin Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community Burton out-patient Derby out-patient Indication Advanced
CAUTION: You must refer to the intranet for the most recent version of this procedural document.
 Procedure for the use of Intravenous Iron Dextran (CosmoFer ) Sharepoint Location Sharepoint Index Directory Clinical Policies and Guidelines General Policies and Guidelines/ Haematology And blood transfusion
Procedure for the use of Intravenous Iron Dextran (CosmoFer ) Sharepoint Location Sharepoint Index Directory Clinical Policies and Guidelines General Policies and Guidelines/ Haematology And blood transfusion
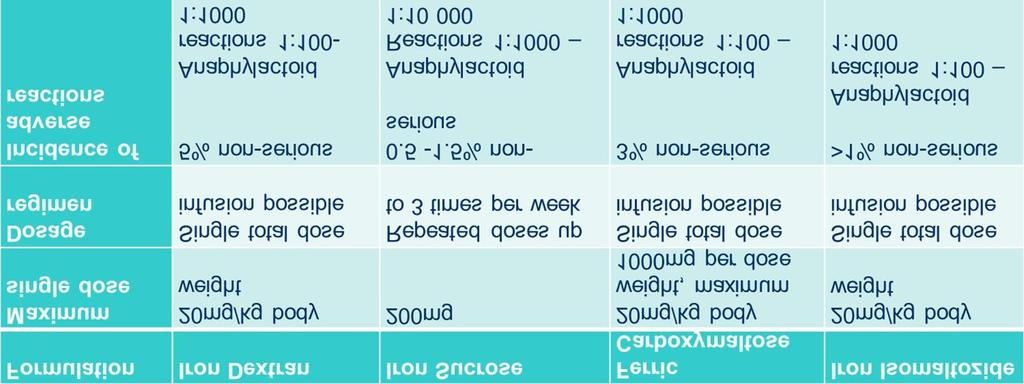
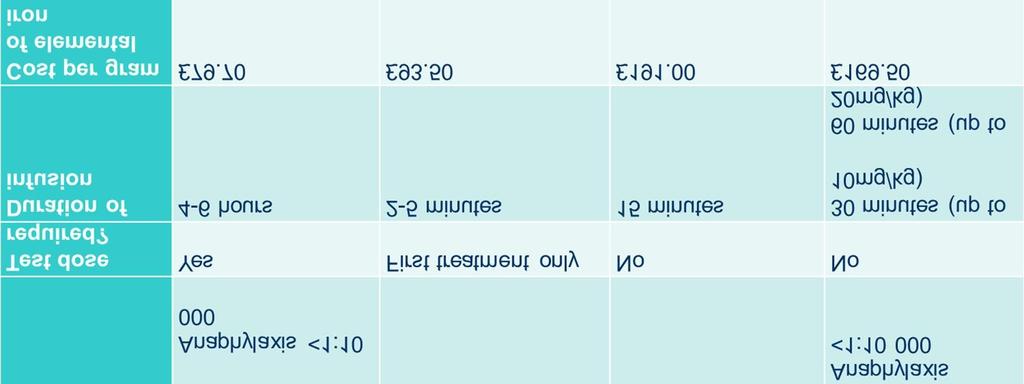
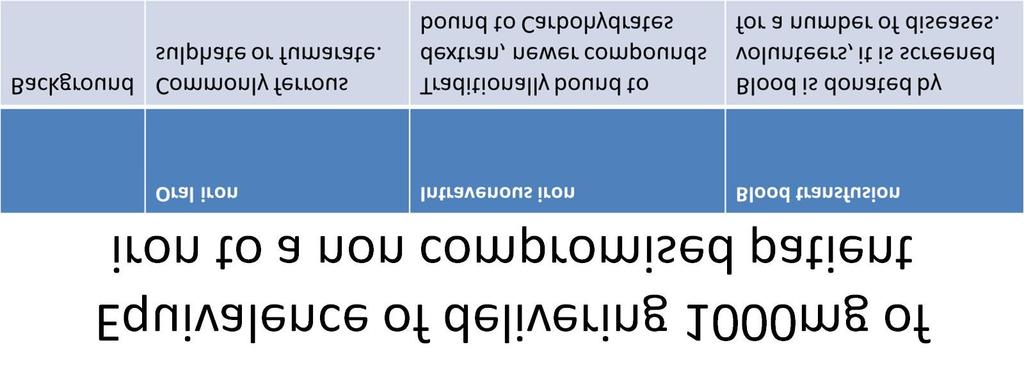
Types of Anaemias and their Management. S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014
 Types of Anaemias and their Management S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014 Objectives At the end of the presentations participants should be able to: 1. Define
Types of Anaemias and their Management S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014 Objectives At the end of the presentations participants should be able to: 1. Define
PREOPERATIVE ANAEMIA PATHWAY
 PREOPERATIVE ANAEMIA PATHWAY Surname: Unit No. Forename: DOB: / / Age: NHS Number: Likes to be called: Address: Tel. No. Religion/Spirituality: GP Name: GP Practice: Planned Operation: Postcode: Mobile
PREOPERATIVE ANAEMIA PATHWAY Surname: Unit No. Forename: DOB: / / Age: NHS Number: Likes to be called: Address: Tel. No. Religion/Spirituality: GP Name: GP Practice: Planned Operation: Postcode: Mobile
Management of Anaemia
 Management of Anaemia Janet Birchall Consultant Haematologist North Bristol Trust and NHS Blood & Transplant Case History - DW age 86 years 14.30 FBC by GP Hb 58 g/l, ferritin 3microg/L. Hospital review
Management of Anaemia Janet Birchall Consultant Haematologist North Bristol Trust and NHS Blood & Transplant Case History - DW age 86 years 14.30 FBC by GP Hb 58 g/l, ferritin 3microg/L. Hospital review
Northern Treatment Advisory Group
 Northern Treatment Advisory Group Ferric Maltol (Feraccru ) for the treatment of iron deficiency Lead author: Daniel Hill Regional Drug & Therapeutics Centre (Newcastle) September 2018 2018 Summary Iron
Northern Treatment Advisory Group Ferric Maltol (Feraccru ) for the treatment of iron deficiency Lead author: Daniel Hill Regional Drug & Therapeutics Centre (Newcastle) September 2018 2018 Summary Iron
Policy for the use of intravenous Iron Dextran (CosmoFer )
") Policy for the use of intravenous Iron Dextran (CosmoFer ) Sharepoint Location Clinical Policies and Guidelines Sharepoint Index Directory General Policies and Guidelines Sub Area Haematology and Blood
Policy for the use of intravenous Iron Dextran (CosmoFer ) Sharepoint Location Clinical Policies and Guidelines Sharepoint Index Directory General Policies and Guidelines Sub Area Haematology and Blood
Laboratory diagnosis of iron deficiency: The interpretation of automated counting parameters. Dr Wayne Thomas Derriford Hospital, Plymouth
 Laboratory diagnosis of iron deficiency: The interpretation of automated counting parameters. Dr Wayne Thomas Derriford Hospital, Plymouth Why does it matter? Over 30% of the Worlds population are anaemic,
Laboratory diagnosis of iron deficiency: The interpretation of automated counting parameters. Dr Wayne Thomas Derriford Hospital, Plymouth Why does it matter? Over 30% of the Worlds population are anaemic,
National Comparative Audit of red cell transfusion in Medical Patients Part Two
 National Comparative Audit of red cell transfusion in Medical Patients Part Two Dr. Kate Pendry, Project Clinical Lead John Grant-Casey, Project Manager August 2013 Part One 9216 cases from 181 sites (90%
National Comparative Audit of red cell transfusion in Medical Patients Part Two Dr. Kate Pendry, Project Clinical Lead John Grant-Casey, Project Manager August 2013 Part One 9216 cases from 181 sites (90%
27/01/2019. Anaemia, Transfusion and TACO Lise Estcourt. Anaemia. What is anaemia?
 Anaemia, Transfusion and TACO Lise Estcourt 1 Anaemia 2 What is anaemia? 3 1 Anaemia according to WHO 4 Anaemia in palliative care Common (77% men 68% women) Symptoms often non-specific Some causes potentially
Anaemia, Transfusion and TACO Lise Estcourt 1 Anaemia 2 What is anaemia? 3 1 Anaemia according to WHO 4 Anaemia in palliative care Common (77% men 68% women) Symptoms often non-specific Some causes potentially
ESM Table 2 Data extraction form and key data from included studies
 ESM Table 2 Data extraction form and key data from included studies Author, year and title Behan, 2006 [21] Cessation of menstruation improves the correlation of FPG to hemoglobin A 1c in Caucasian women
ESM Table 2 Data extraction form and key data from included studies Author, year and title Behan, 2006 [21] Cessation of menstruation improves the correlation of FPG to hemoglobin A 1c in Caucasian women
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS
 GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
Blood Transfusion. Dr William Dooley
 Blood Transfusion Dr William Dooley Plan Cases Blood groups / Indications Procedure Monitoring / Reactions Cases For following cases: - Would you give them a blood transfusion? - How many units you would
Blood Transfusion Dr William Dooley Plan Cases Blood groups / Indications Procedure Monitoring / Reactions Cases For following cases: - Would you give them a blood transfusion? - How many units you would
The Perioperative Care Chain is Only as Strong as its weakest link
 The Perioperative Care Chain is Only as Strong as its weakest link Associate Professor Kerin Fielding The University of Notre Dame, Australia School of Medicine, Sydney Outline The perioperative chain
The Perioperative Care Chain is Only as Strong as its weakest link Associate Professor Kerin Fielding The University of Notre Dame, Australia School of Medicine, Sydney Outline The perioperative chain
Dr Dominic Fleischer
 Dr Tony Smith Intensive Care Specialist Auckland DHB Critical Care Medicine, Auckland, National Medical Director for St John Dr Dominic Fleischer ED Specialist Dr Richard Seigne Specialist Anaesthetist
Dr Tony Smith Intensive Care Specialist Auckland DHB Critical Care Medicine, Auckland, National Medical Director for St John Dr Dominic Fleischer ED Specialist Dr Richard Seigne Specialist Anaesthetist
Patient Blood Management and alternatives to transfusion
 Patient Blood Management and alternatives to transfusion Patient Blood Management and the alternatives to transfusion and when these should be used Learning Outcomes Explain techniques that can be used
Patient Blood Management and alternatives to transfusion Patient Blood Management and the alternatives to transfusion and when these should be used Learning Outcomes Explain techniques that can be used
Summary of Recommendation Statements Kidney International Supplements (2012) 2, ; doi: /kisup
 2, ; doi: /kisup") http://www.kidney-international.org & 2012 KDIGO Summary of Recommendation Statements Kidney International Supplements (2012) 2, 283 287; doi:10.1038/kisup.2012.41 Chapter 1: Diagnosis and evaluation of
http://www.kidney-international.org & 2012 KDIGO Summary of Recommendation Statements Kidney International Supplements (2012) 2, 283 287; doi:10.1038/kisup.2012.41 Chapter 1: Diagnosis and evaluation of
Laboratory Empowerment. Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance
 Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Western Health Specialist Clinics Access & Referral Guidelines
 Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
The LaboratoryMatters
 Laboratory Medicine Newsletter for clinicians, pathologists & clinical laboratory technologists. A Initiative. Complete Blood Count This issue highlights: CBC, while ubiquitous, is an excellent diagnostic
Laboratory Medicine Newsletter for clinicians, pathologists & clinical laboratory technologists. A Initiative. Complete Blood Count This issue highlights: CBC, while ubiquitous, is an excellent diagnostic
Managing Anaemia in IBD
 Oxford Inflammatory Bowel Disease & Hepatology MasterClass Managing Anaemia in IBD Dr Alex Kent Senior Research Fellow Disclosures WHO Classification of Anaemia Normal haemoglobin and haematocrit levels
Oxford Inflammatory Bowel Disease & Hepatology MasterClass Managing Anaemia in IBD Dr Alex Kent Senior Research Fellow Disclosures WHO Classification of Anaemia Normal haemoglobin and haematocrit levels
I. Definitions. V. Evaluation A. History B. Physical Exam C. Laboratory evaluation D. Bone marrow examination E. Specialty referrals
 I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
Mr John Faulds Blood Conservation Co-ordinator Royal Cornwall Hospital
 Mr John Faulds Blood Conservation Co-ordinator Royal Cornwall Hospital Primary aim to reduce the need for red blood cell transfusion, in those patients where transfusion can be avoided, through the use
Mr John Faulds Blood Conservation Co-ordinator Royal Cornwall Hospital Primary aim to reduce the need for red blood cell transfusion, in those patients where transfusion can be avoided, through the use
Audit of Blood Use in Orthopaedic Surgery. Comparative Report
 West Midlands Regional Transfusion Committee Audit of Blood Use in Orthopaedic Surgery Comparative Report West Midlands RTC Audit Group Dr Craig Taylor (Chair), Andrea Blest, Dr Matthew Lumley, Jenny Hartley,
West Midlands Regional Transfusion Committee Audit of Blood Use in Orthopaedic Surgery Comparative Report West Midlands RTC Audit Group Dr Craig Taylor (Chair), Andrea Blest, Dr Matthew Lumley, Jenny Hartley,
NEW RCPCH REFERENCE RANGES-
 s vary between populations and age groups and it is important to always check the reference Haematology: Haemoglobin Male 130 175 g/l 0 6 days 145-220 g/l Female 115 165 g/l 7 days 140-186 g/l 8 days 3
s vary between populations and age groups and it is important to always check the reference Haematology: Haemoglobin Male 130 175 g/l 0 6 days 145-220 g/l Female 115 165 g/l 7 days 140-186 g/l 8 days 3
Guidelines on Anaemia Management in Patients with Chronic Kidney Disease (CKD)
") Guidelines on Anaemia Management in Patients with Chronic Kidney Disease (CKD) This guideline is for use in adult patients with an estimated Glomerular Filtration Rate (egfr) of less than 60ml/min/1.73m
Guidelines on Anaemia Management in Patients with Chronic Kidney Disease (CKD) This guideline is for use in adult patients with an estimated Glomerular Filtration Rate (egfr) of less than 60ml/min/1.73m
Preparing for Patients at High Risk of Transfusion
 18/10/2017 Preparing for Patients at High Risk of Transfusion Jane Ottens. B.Sc., CCP ( Aust) Ashford Hospital, South Australia Preparing for Patients at High Risk of Transfusion Jane Ottens. B.Sc., CCP
18/10/2017 Preparing for Patients at High Risk of Transfusion Jane Ottens. B.Sc., CCP ( Aust) Ashford Hospital, South Australia Preparing for Patients at High Risk of Transfusion Jane Ottens. B.Sc., CCP
Blood Transfusions in Children with Haemoglobinopathies
 Blood Transfusions in Children with Haemoglobinopathies Version: 2 Date: 22 nd April 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/ committees involved in
Blood Transfusions in Children with Haemoglobinopathies Version: 2 Date: 22 nd April 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/ committees involved in
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Preoperative anemia Common, consequential and correctable in non-emergent surgery By Kathrine Frey, MD
 Preoperative anemia Common, consequential and correctable in non-emergent surgery By Kathrine Frey, MD Preoperative anemia is common, especially in patients undergoing nonemergent high-blood-loss surgical
Preoperative anemia Common, consequential and correctable in non-emergent surgery By Kathrine Frey, MD Preoperative anemia is common, especially in patients undergoing nonemergent high-blood-loss surgical
EFFECTIVE SHARE CARE AGREEMENT
 Specialist details Patient identifier Name: Tel: EFFECTIVE SHARE CARE AGREEMENT For the specialist use of Erythropoietin Stimulating Agent (ESA) Therapy (formerly known as EPO) for the correction of Anaemia
Specialist details Patient identifier Name: Tel: EFFECTIVE SHARE CARE AGREEMENT For the specialist use of Erythropoietin Stimulating Agent (ESA) Therapy (formerly known as EPO) for the correction of Anaemia
Anaemia in the ICU: Is there an alternative to using blood transfusion?
 Anaemia in the ICU: Is there an alternative to using blood transfusion? Tim Walsh Professor of Critical Care, Edinburgh University World Health Organisation grading of the severity of anaemia Grade of
Anaemia in the ICU: Is there an alternative to using blood transfusion? Tim Walsh Professor of Critical Care, Edinburgh University World Health Organisation grading of the severity of anaemia Grade of
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
2. Liver blood tests and what they mean p2 Acute and chronic liver screen
 Hepatology referral pathways for GP 1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for hepatology referral 3. Raised
Hepatology referral pathways for GP 1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for hepatology referral 3. Raised
namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES
 namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF BIOMEDICAL SCIENCES QUALIFICATION CODE: SOBBMS LEVEL: 6 COURSE
namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF BIOMEDICAL SCIENCES QUALIFICATION CODE: SOBBMS LEVEL: 6 COURSE
NICE guideline on Suspected cancer: recognition and referral (2015) Education package for GPs and Nurse Practitioners Case scenarios
 Education package for GPs and Nurse Practitioners Case scenarios") NICE guideline on Suspected cancer: recognition and referral (2015) Education package for GPs and Nurse Practitioners Case scenarios How to use the case scenarios The case scenarios can be used in a training
NICE guideline on Suspected cancer: recognition and referral (2015) Education package for GPs and Nurse Practitioners Case scenarios How to use the case scenarios The case scenarios can be used in a training
Avoiding Early Cancer Claims. Presentation #4. Hank George, FALU
 Avoiding Early Cancer Claims Presentation #4 Hank George, FALU Hematology and High Risk of Early Cancer Claims Mild Anemia in elders is underpriced by insurers most likely because of its high prevalence
Avoiding Early Cancer Claims Presentation #4 Hank George, FALU Hematology and High Risk of Early Cancer Claims Mild Anemia in elders is underpriced by insurers most likely because of its high prevalence
Clinical Profile and Etiology of Anaemia in Elderly: A Hospital Based Study at a Tertiary Care in the Sub-Himalayan Region
 Original Article Clinical Profile and Etiology of Anaemia in Elderly: A Hospital Based Study at a Tertiary Care in the Sub-Himalayan Region I Joshi*, S Thakur**, R Bhawani***, V Kaushal**#, A Mahajan #
Original Article Clinical Profile and Etiology of Anaemia in Elderly: A Hospital Based Study at a Tertiary Care in the Sub-Himalayan Region I Joshi*, S Thakur**, R Bhawani***, V Kaushal**#, A Mahajan #
ROYAL WOLVERHAMPTON HOSPITALS NHS TRUST
 ROYAL WOLVERHAMPTON HOSPITALS NHS TRUST SHARED CARE PROTOCOL FOR ERYTHROPOIETIN USE 2016 New Cross Hospital Dr J Odum Dr P B Rylance Dr P Carmichael Dr S Acton Dr B Ramakrishna Walsall Manor Hospital Dr
ROYAL WOLVERHAMPTON HOSPITALS NHS TRUST SHARED CARE PROTOCOL FOR ERYTHROPOIETIN USE 2016 New Cross Hospital Dr J Odum Dr P B Rylance Dr P Carmichael Dr S Acton Dr B Ramakrishna Walsall Manor Hospital Dr
Part 1 examination. Haematology: First paper. Tuesday 20 March Candidates must answer all questions. Each question is worth a total of 25 marks.
 Part 1 examination Haematology: First paper Tuesday 20 March 2018 Candidates must answer all questions. Each question is worth a total of 25 marks. Time allowed: 3 hours Question 1: General Haematology
Part 1 examination Haematology: First paper Tuesday 20 March 2018 Candidates must answer all questions. Each question is worth a total of 25 marks. Time allowed: 3 hours Question 1: General Haematology
An Audit of Poor Response To Erythropoeitin Therapy. September 1998
 1 An Audit of Poor Response To Erythropoeitin Therapy September 1998 Prepared By: Nicola Austerberry Renal Audit Facilitator Phil Kalra Consultant Nephrologist 2 1 Introduction The topic for this audit
1 An Audit of Poor Response To Erythropoeitin Therapy September 1998 Prepared By: Nicola Austerberry Renal Audit Facilitator Phil Kalra Consultant Nephrologist 2 1 Introduction The topic for this audit
Quick Reference Sheet for Guideline Patient Blood Management prior to Surgery CPDI 063, v5.1 Pathway for investigation of anaemia (Flowchart 1)
") Quick Reference Sheet for Guideline Patient Blood Management prior to Surgery CPDI 063, v5.1 Pathway for investigation of anaemia (Flowchart 1) If neutrophils
Quick Reference Sheet for Guideline Patient Blood Management prior to Surgery CPDI 063, v5.1 Pathway for investigation of anaemia (Flowchart 1) If neutrophils
Haematology dilemma s to refer or not to refer?
 Haematology dilemma s to refer or not to refer? NWL Pathology GP Study Day Dr Fatts Chowdhury Consultant Haematologist in Transfusion Medicine NHS Blood and Transplant Senior Honorary Clinical Lecturer
Haematology dilemma s to refer or not to refer? NWL Pathology GP Study Day Dr Fatts Chowdhury Consultant Haematologist in Transfusion Medicine NHS Blood and Transplant Senior Honorary Clinical Lecturer
TACO CASE STUDIES RTC JUNE Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner
 TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust
 Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Guidelines for the management of warfarin reversal in adults
 SharePoint Location Clinical Policies and Guidelines SharePoint Index Directory General Policies and Guidelines Sub Area Haematology and Transfusion Key words (for search purposes) Warfarin, Bleeding Central
SharePoint Location Clinical Policies and Guidelines SharePoint Index Directory General Policies and Guidelines Sub Area Haematology and Transfusion Key words (for search purposes) Warfarin, Bleeding Central
Anemia in the elderly. Nattiya Teawtrakul MD., PhD
 Anemia in the elderly Nattiya Teawtrakul MD., PhD Contents Definition of anemia in the elderly The impact of anemia in the elderly Etiology of anemia in the elderly Management of anemia in the elderly
Anemia in the elderly Nattiya Teawtrakul MD., PhD Contents Definition of anemia in the elderly The impact of anemia in the elderly Etiology of anemia in the elderly Management of anemia in the elderly
Martin Besser Consultant Haematologist Papworth Hospital
 Martin Besser Consultant Haematologist Papworth Hospital Important modifiable risk factor for morbidity and mortality in all forms of surgery (Australian PBM guidelines) 140g/l 100g/l 80g/l Patients should
Martin Besser Consultant Haematologist Papworth Hospital Important modifiable risk factor for morbidity and mortality in all forms of surgery (Australian PBM guidelines) 140g/l 100g/l 80g/l Patients should
GP Referral Guidelines. for. South Wales Cancer Network. Document Control Sheet. Specialty/Project Haematological Site Specific Group
 GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Anemia Management: Using Epo and Iron
 Anemia Management: Using Epo and Iron Ky Stoltzfus, MD University of Kansas Medical Center Assistant Professor Department of Internal Medicine January 23, 2013 Regulation of red cell production Treatment
Anemia Management: Using Epo and Iron Ky Stoltzfus, MD University of Kansas Medical Center Assistant Professor Department of Internal Medicine January 23, 2013 Regulation of red cell production Treatment
RAPID REFERRAL ANEMIA CLINICS
 RAPID REFERRAL ANEMIA CLINICS REDUCING INAPPROPRIATE TRANSFUSION AND OPTIMIZING PATIENT CARE ALAN TINMOUTH ORBCON APRIL 11, 2018 www.ohri.ca Affiliated with Affilié à OBJECTIVES 1. Review rationale for
RAPID REFERRAL ANEMIA CLINICS REDUCING INAPPROPRIATE TRANSFUSION AND OPTIMIZING PATIENT CARE ALAN TINMOUTH ORBCON APRIL 11, 2018 www.ohri.ca Affiliated with Affilié à OBJECTIVES 1. Review rationale for
SHARED CARE PRESCRIBING GUIDELINE
 WORKING IN PARTNERSHIP East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG, Surrey Heath CCG, North East Hampshire & Farnham CCG, Crawley CCG, Horsham & Mid-Sussex CCG SHARED
WORKING IN PARTNERSHIP East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG, Surrey Heath CCG, North East Hampshire & Farnham CCG, Crawley CCG, Horsham & Mid-Sussex CCG SHARED
Management of Anaemia reduces Red cell Transfusion in NI. Dr Susan Atkinson NI Transfusion Committee
 Management of Anaemia reduces Red cell Transfusion in NI Dr Susan Atkinson NI Transfusion Committee BBTS September 2014 Patient and Client Council Department of Health Chief Medical Officer Expert Professionals
Management of Anaemia reduces Red cell Transfusion in NI Dr Susan Atkinson NI Transfusion Committee BBTS September 2014 Patient and Client Council Department of Health Chief Medical Officer Expert Professionals
Rory McCulloch. Specialty Trainee Haematology Royal Devon & Exeter Hospital
 Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
My Bloody Talk. Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne
 My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
Cytopaenias in HIV. Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH
 Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
A Patient s guide to. Blood Transfusions and Human Tissue Transplant
 A Patient s guide to Blood Transfusions and Human Tissue Transplant Why might I need a blood transfusion? Blood transfusions are given to replace blood lost in surgery or to treat anaemia (lack of red
A Patient s guide to Blood Transfusions and Human Tissue Transplant Why might I need a blood transfusion? Blood transfusions are given to replace blood lost in surgery or to treat anaemia (lack of red
BONE MARROW PERIPHERAL BLOOD Erythrocyte
 None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
HAEMATOLOGICAL EVALUATION OF ANEMIA. Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore
 HAEMATOLOGICAL EVALUATION OF ANEMIA Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore Learning Objectives Laboratory tests for the evaluation of anemia
HAEMATOLOGICAL EVALUATION OF ANEMIA Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore Learning Objectives Laboratory tests for the evaluation of anemia
DOAC and NOAC are terms for a novel class of directly acting oral anticoagulant drugs including Rivaroxaban, Apixaban, Edoxaban, and Dabigatran.
 Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin
 Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Version: 6 Date: 2 nd March 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Version: 6 Date: 2 nd March 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/
Hematologic changes in systemic diseases. Chittima Sirijerachai
 Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Dr Marina Karakantza Consultant Haematologist, NHSBT
 Dr Marina Karakantza Consultant Haematologist, NHSBT Overview Definition of transfusion thresholds Mechanisms of adaptation to anaemia How RBC transfusion affect adaptation mechanisms to anaemia Triggers
Dr Marina Karakantza Consultant Haematologist, NHSBT Overview Definition of transfusion thresholds Mechanisms of adaptation to anaemia How RBC transfusion affect adaptation mechanisms to anaemia Triggers
Ambulatory Emergency Care Pathways. Painless Obstructive Jaundice
 Ambulatory Emergency Care Pathways Painless Obstructive Jaundice Effective Date: December 2011 Content Summary Ref Title Description 1 Condition Details Identifies pathway details and clinical sign-off
Ambulatory Emergency Care Pathways Painless Obstructive Jaundice Effective Date: December 2011 Content Summary Ref Title Description 1 Condition Details Identifies pathway details and clinical sign-off
2016 Re-Audit of Patient Blood Management in adults undergoing elective, scheduled surgery
 2016 Re-Audit of Patient Blood Management in adults undergoing elective, scheduled surgery 2017 Re-Audit of Red Cell & Platelet Transfusion in Adult Haematology patients South West RTC 2016 Re-Audit of
2016 Re-Audit of Patient Blood Management in adults undergoing elective, scheduled surgery 2017 Re-Audit of Red Cell & Platelet Transfusion in Adult Haematology patients South West RTC 2016 Re-Audit of
NZBS HAEMOCHROMATOSIS & THERAPEUTIC VENESECTION POLICY
 REASON FOR ISSUE: New Document for TV Clinic 1. INTRODUCTION NZBS will provide a venesection service for people in New Zealand who require venesection for conditions that are known to benefit from therapeutic
REASON FOR ISSUE: New Document for TV Clinic 1. INTRODUCTION NZBS will provide a venesection service for people in New Zealand who require venesection for conditions that are known to benefit from therapeutic
Prescribing Framework for Methotrexate for Immunosuppression in ADULTS
 Hull & East Riding Prescribing Committee Prescribing Framework for Methotrexate for Immunosuppression in ADULTS Patient s Name:.. NHS Number: Patient s Address:... (Use addressograph sticker) GP s Name:...
Hull & East Riding Prescribing Committee Prescribing Framework for Methotrexate for Immunosuppression in ADULTS Patient s Name:.. NHS Number: Patient s Address:... (Use addressograph sticker) GP s Name:...
GP refresher course Anaemia. Peter MacCallum Consultant Haematologist Barts Health NHS Trust London January 2018
 GP refresher course Anaemia Peter MacCallum Consultant Haematologist Barts Health NHS Trust London January 2018 None Declarations WHO thresholds Hb (g/l) Children 0.5 5 yrs 110 Children 5 12 yrs 115 Teens
GP refresher course Anaemia Peter MacCallum Consultant Haematologist Barts Health NHS Trust London January 2018 None Declarations WHO thresholds Hb (g/l) Children 0.5 5 yrs 110 Children 5 12 yrs 115 Teens
Haematology Comparability Document
 South Island Quality Assurance Group for Haematology Haematology Comparability Document Version Number: 1_4 Author: John Moodie/Alison Doorey Implementation Date: 21/05/2012 Revision Date: On-going Document
South Island Quality Assurance Group for Haematology Haematology Comparability Document Version Number: 1_4 Author: John Moodie/Alison Doorey Implementation Date: 21/05/2012 Revision Date: On-going Document
Hereditary Haemochromatosis For GPs
 Hereditary Haemochromatosis For GPs What is Hereditary Haemochromatosis? Hereditary Haemochromatosis () is a common autosomal recessive disease resulting in excessive absorption of dietary iron from the
Hereditary Haemochromatosis For GPs What is Hereditary Haemochromatosis? Hereditary Haemochromatosis () is a common autosomal recessive disease resulting in excessive absorption of dietary iron from the
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin
 Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Document Information Version: 2 Date: 28 th December 2013 Authors (incl. job title): Professor David Rees (Consultant
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Document Information Version: 2 Date: 28 th December 2013 Authors (incl. job title): Professor David Rees (Consultant
Introduction. Peripheral arterial disease. Hospital inpatient data - 5,498 FCE (2009/10), & 530 deaths in England alone
, & 530 deaths in England alone") 1 Introduction 2 Introduction Peripheral arterial disease Affects 20% adults in Europe and North America In the UK 500-1000/million PAD, 1-2% require amputation LLA 8-15% in people with diabetes with up
1 Introduction 2 Introduction Peripheral arterial disease Affects 20% adults in Europe and North America In the UK 500-1000/million PAD, 1-2% require amputation LLA 8-15% in people with diabetes with up
A Patient s guide to. Blood Transfusions and Human Tissue Transplant
 A Patient s guide to Blood Transfusions and Human Tissue Transplant Why might I need a blood transfusion? Blood transfusions are given to replace blood lost in surgery or to treat anaemia (lack of red
A Patient s guide to Blood Transfusions and Human Tissue Transplant Why might I need a blood transfusion? Blood transfusions are given to replace blood lost in surgery or to treat anaemia (lack of red
Hydroxyurea (Hydroxycarbamide) - Guidelines for treating children with Sickle Cell Disease
 - Guidelines for treating children with Sickle Cell Disease") Hydroxyurea (Hydroxycarbamide) - Guidelines for treating children with Sickle Cell Disease Document Information Version: 2 Date: July 2014 Authors (incl. job title): Dr Moira Dick Consultant Paediatrician
Hydroxyurea (Hydroxycarbamide) - Guidelines for treating children with Sickle Cell Disease Document Information Version: 2 Date: July 2014 Authors (incl. job title): Dr Moira Dick Consultant Paediatrician
Full Blood Count analysis Is a 3 part-diff good enough? Dr Marion Münster, Sysmex South Africa
 Full Blood Count analysis Is a 3 part-diff good enough? Dr Marion Münster, Sysmex South Africa The Role of the FBC in clinical decision making History Examination Investigations Decision 70% FBC Laboratory
Full Blood Count analysis Is a 3 part-diff good enough? Dr Marion Münster, Sysmex South Africa The Role of the FBC in clinical decision making History Examination Investigations Decision 70% FBC Laboratory
Anaemia is a shortage of red blood cells and haemoglobin. If you have anaemia, doctors say that you are anaemic.
 Freephone helpline 0808 808 5555 information@lymphoma-action.org.uk www.lymphoma-action.org.uk Anaemia Anaemia means that there is too little haemoglobin (the chemical that carries oxygen) and too few
Freephone helpline 0808 808 5555 information@lymphoma-action.org.uk www.lymphoma-action.org.uk Anaemia Anaemia means that there is too little haemoglobin (the chemical that carries oxygen) and too few
Ciclosporin 25mg, 50mg, 100mg capsules Ciclosporin oral solution 100mg/ml
 Shared Care Protocol Ciclosporin for the treatment of rheumatoid arthritis Name of drug, form and strength Background Ciclosporin 25mg, 50mg, 100mg capsules Ciclosporin oral solution 100mg/ml Ciclosporin
Shared Care Protocol Ciclosporin for the treatment of rheumatoid arthritis Name of drug, form and strength Background Ciclosporin 25mg, 50mg, 100mg capsules Ciclosporin oral solution 100mg/ml Ciclosporin
Schedule of Accreditation issued by United Kingdom Accreditation Service 2 Pine Trees, Chertsey Lane, Staines-upon-Thames, TW18 3HR, UK
 2 Pine Trees, Chertsey Lane, Staines-upon-Thames, TW18 3HR, UK Department of Haematology and Blood Transfusion 3 rd Floor Pathology Directorate Darent Valley Hospital Darenth Wood Road Dartford Kent DA2
2 Pine Trees, Chertsey Lane, Staines-upon-Thames, TW18 3HR, UK Department of Haematology and Blood Transfusion 3 rd Floor Pathology Directorate Darent Valley Hospital Darenth Wood Road Dartford Kent DA2
Clinical guideline: manual red cell exchange in patients with sickle cell disease
 Clinical guideline: manual red cell exchange in patients with sickle cell disease HN-504b Introduction Most patients with sickle cell anaemia are relatively asymptomatic despite baseline Hb concentrations
Clinical guideline: manual red cell exchange in patients with sickle cell disease HN-504b Introduction Most patients with sickle cell anaemia are relatively asymptomatic despite baseline Hb concentrations
Morphological classification of anaemia among first-time blood donors in Northwest Nigeria and the implication of empirical haematinics therapy
 International Journal of Biomedical and Health Sciences 0794-4748/2011 $5.00 + 0.00 Vol. 7, No. 2, June 30, 2011 2011 African Studies on Population and Health Printed in Nigeria http://www.asopah.org IJBHS
International Journal of Biomedical and Health Sciences 0794-4748/2011 $5.00 + 0.00 Vol. 7, No. 2, June 30, 2011 2011 African Studies on Population and Health Printed in Nigeria http://www.asopah.org IJBHS
THE KENYA POLYTECHNIC UNIVERSITY COLLEGE
 THE KENYA POLYTECHNIC UNIVERSITY COLLEGE SCHOOL OF HEALTH SCIENCES AND TECHNOLOGY DEPARTMENT OF BIOMEDICAL LABORATORY SCIENCES AND TECHNOLOGY DIPLOMA IN MEDICAL LABORATORY SCIENCE END OF YEAR 1 EXAMINATION
THE KENYA POLYTECHNIC UNIVERSITY COLLEGE SCHOOL OF HEALTH SCIENCES AND TECHNOLOGY DEPARTMENT OF BIOMEDICAL LABORATORY SCIENCES AND TECHNOLOGY DIPLOMA IN MEDICAL LABORATORY SCIENCE END OF YEAR 1 EXAMINATION
Red blood cell transfusion
 Red blood cell transfusion This leaflet explains more about red blood cell transfusion, including the benefits, risks and any alternatives and what you can expect when you come to hospital. If you have
Red blood cell transfusion This leaflet explains more about red blood cell transfusion, including the benefits, risks and any alternatives and what you can expect when you come to hospital. If you have
Nutritional anaemia. Dr J Potgieter Dept of Haematology NHLS - TAD
 Nutritional anaemia Dr J Potgieter Dept of Haematology NHLS - TAD Classification of anaemia Microcytic, hypochromic MCV < 80fl MCH > 27pg Iron deficiency Anaemia of chronic disease Thalassaemia Lead poisoning
Nutritional anaemia Dr J Potgieter Dept of Haematology NHLS - TAD Classification of anaemia Microcytic, hypochromic MCV < 80fl MCH > 27pg Iron deficiency Anaemia of chronic disease Thalassaemia Lead poisoning
INTERELATIONSHIP BETWEEN IDA AND VITAMIN D DEFICIENCY IS NOW ESTABLISHED
 INTERELATIONSHIP BETWEEN IDA AND VITAMIN D DEFICIENCY IS NOW ESTABLISHED Rationale for Combining Iron & Vit-D Vit D deficiency and Iron deficiency Anaemia the two most menacing disorders - are inter-related
INTERELATIONSHIP BETWEEN IDA AND VITAMIN D DEFICIENCY IS NOW ESTABLISHED Rationale for Combining Iron & Vit-D Vit D deficiency and Iron deficiency Anaemia the two most menacing disorders - are inter-related
Approach to the child with anemia. Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital
 Approach to the child with anemia Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital Definition of anemia Hb< 2 SD or P2.5 below the mean for a healthy of the same gender
Approach to the child with anemia Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital Definition of anemia Hb< 2 SD or P2.5 below the mean for a healthy of the same gender
The Full Blood Count. Dave Reynders University of Pretoria Paediatric Oncology and Haematology
 The Full Blood Count Dave Reynders University of Pretoria Paediatric Oncology and Haematology 1 History Empedocles in the 5 th century BC Vasculature contains Blood, Phlegm, Black bile and Yellow Bile.
The Full Blood Count Dave Reynders University of Pretoria Paediatric Oncology and Haematology 1 History Empedocles in the 5 th century BC Vasculature contains Blood, Phlegm, Black bile and Yellow Bile.