Dr. Muhammad Shamim. FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg)
|
|
|
- Paul Woods
- 5 years ago
- Views:
Transcription
, MHPE (Nl & Eg) Assistant Professor, Dept.")

1 Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Salman bin Abdulaziz University Web: surgeonshamim.com 1
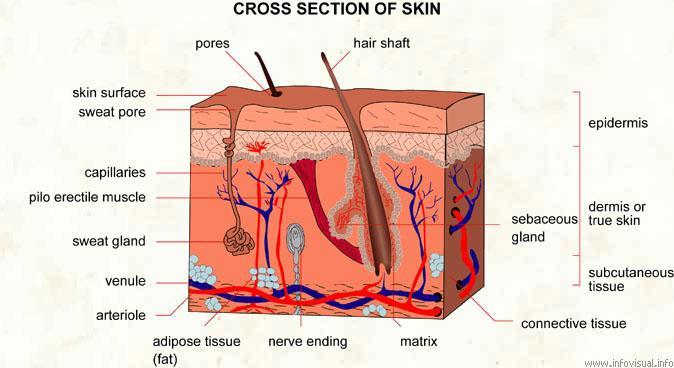
2 A burn is defined as a dissolution in tissue continuity as a result of thermal damage, in which there is coagulative necrosis of tissues. 2
3 Etiology (1) (2) (3) (4) (5) (6) (7) (8) (9) Dry heat Flame Scald Electric contact Thermoelectric Chemical Friction Ionizing radiation Frostbite 3
4 Body s Response to Burns Emergent Phase (Stage 1) Pain response Catecholamine release Tachycardia, Tachypnea, Mild Hypertension, Mild Anxiety Fluid Shift Phase (Stage 2) Length hours Begins after Emergent Phase Reaches peak in 6-8 hours Damaged cells initiate inflammatory response Increased blood flow to cells Shift of fluid from intravascular to extravascular space MASSIVE EDEMA Leaky Capillaries 4
5 Hypermetabolic Phase (Stage 3) Last for days to weeks Large increase in the body s need for nutrients as it repairs itself Resolution Phase (Stage 4) Scar formation General rehabilitation and progression to normal function 5
6 Clinical features Burn shock. Overwhelming sudden intense pain in 2nd degree burn. Burnt wound, depending on the duration, degree & type of thermal injury. 6

7 Immediate Care & Resuscitation 7
8 Prehospital care In burns & scalds Remove the patient from source of heat & extinguish the flame. A standard ABC check followed by a rapid secondary survey. Apply cold, clean water soaks to affected areas & renew these every 3 minutes. In electrical burns Switch off the electrical supply. If victim is unconscious Exclude the presence of cardiac arrest, & if necessary, apply cardio-pulmonary resuscitation. In chemical burns Irrigate affected area with copious amounts of clean water except in phenol burns. In phenol burns Irrigate with polyethylene glycol. Note: Ensure rescuer safety, esp. in house fires & in electrical & chemical injuries. 8
9 Transportation Burn patients must be transported with great care. A secure IV line is required for major cases. Burns should be covered with clean sheets & patient wrapped in warm blankets or foil. Anyone involved in a fire in an enclosed space should receive oxygen, esp. if there is an altered consciousness level. Elevate Sitting a patient up with a burned airway may prove live saving. Elevation of burned limbs will reduce swelling & discomfort. 9
10 Hospital Care Possibility of additional injury must be sought & treated appropriately. Assess major determinants of severity of burn injury; Percentage of total body surface area burnt. Depth of burn. Presence of inhalation injury. 10
11 Priorities in the management of a major burn A. Airway control B. Breathing & ventilation C. Circulation D. Disability (neurological status) E. Exposure with environmental control F. Fluid resuscitation 11

12 Airway In cases of burned airway, secure the airway with an endotracheal tube until the swelling has subsided, which is usually after about 48 hours. Delay can make intubation very difficult due to swelling. Perform an emergency cricothyroidotomy if intubation is delayed. Timeframe from burn to airway occlusion is usually between 4 & 24 hours. 12
13 Breathing Recognition of the potentially burned airway A history of being trapped in the presence of smoke or hot gases. Burns on the palate or nasal mucosa, or loss of all of the nasal hairs. Deep burns around the mouth & neck. Progressive increase in respiratory effort & rate, rising pulse, anxiety & confusion. Decreasing oxygen saturation, & patchy consolidation on chest x-ray. 13
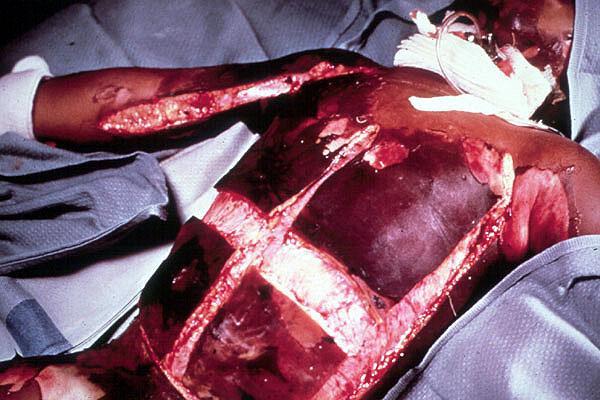
14 Breathing Treatment Physiotherapy, nebulizers & warm humidified oxygen; patient's progress should be monitored using respiratory rate, & blood gas measurements. If condition deteriorates, continous or intermittent positive pressure may be used with a mask or T piece, & in the severest cases, intubation & management in an intensive care unit will be needed. Any mechanical block to breathing from the eschar of a full thickness burn on the chest wall requires escharotomy. 14
15 Assessment Of Burns Injury Extent of total body surface area (TBSA) burnt This is necessary because burn patients require IV resuscitation if their injury exceeds 10% body surface area in children or 15% in adults. Methods of assessment Patient's whole hand is 1% TBSA, & is a useful guide in small burns. Lund & Browder chart is useful in larger burns. Wallace's Rule of Nines is adequate for a first approximation only. 15
 18% (9% x 2). Right lower limb (front & back) 18% (9% x 2). Left lower limb (front & back) 18% (9% x 2).")
16 Wallace's Rule of Nines Head & neck 9%. Anterior aspect of trunk (chest + abdomen) 18% (9% x 2). Posterior aspect of trunk 18% (9% x 2). Upper limbs (right & left) 18% (9% x 2). Right lower limb (front & back) 18% (9% x 2). Left lower limb (front & back) 18% (9% x 2). Perineum 1%. 16
17 Lund & Browder Chart Relative % of area affected by growth Age in years Adult A Head B Thigh C Leg
18 18

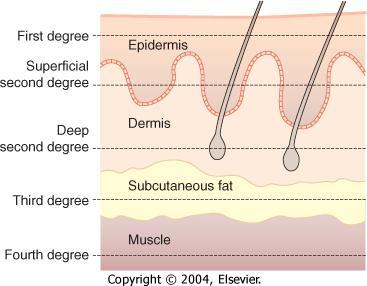
19 Depth of Burn Superficial Burn Partial Thickness Burn Full Thickness Burn 19
20 Depth of burns History is important which includes temperature, time & burning material. Superficial partial thickness burns Injury is upto the papillary dermis, with blistering &/or loss of epidermis. Underlying dermis is pink & moist. Capillary return is clearly visible when blanched, & pinprick sensation is normal. It heal without residual scarring in 2 weeks. Deep partial thickness burns Injury is upto the deeper parts of the reticular dermis, with loss of epidermis. Exposed dermis is not as moist as that in a superficial burn. Color does not blanch with pressure, & the sensation is reduced. It take 3 or more weeks to heal without surgery & usually lead to hypertrophic scarring.. Full-thickness burns These have a dry, charred, waxen, or leathery appearance, & may be white or greyish in color. Thrombosed vessels may be evident. Burn surface is pain free, & is anesthetic to a pinprick or to touch. 20
21 21



22 A superficial partial- thickness scald 24 hours after injury. The dermis is pink and blanches to pressure. At 2 weeks, the wound is healed but lacks pigment. At 3 months, the pigment is returning. 22



23 A deep dermal burn undergoing tangential shaving. The dead dermis is removed layer by layer until healthy bleeding is seen. The burn is pale because it was dressed with silver sulphadiazine cream, but no blanching was visible under this layer. The patient was unable to differentiate between pressure from the sharp and blunt ends of a needle. A thin, split-thickness graft harvested from the thigh. The thin graft is placed in the dermal remnants. 23
24 Criteria for acute admission to burns unit Suspected airway or inhalational injury Any burn likely to require fluid resuscitation Any burn likely to require surgery Significant burns to the hands, face, feet or perineum Patients whose psychiatric or social background makes it inadvisable to send them home Any suspicion of non accidental injury Any burn in a patient at the extremes of age Any burn with potentially serious sequelae including high tension electrical burns & concentrated hydrofluoric acid burns 24
25 Circulatory Support & Fluid Resuscitation Type of fluid 1. Ringer's lactate or Hartman's solution. 2. Human albumin solution or fresh-frozen plasma. 3. Hypertonic saline. Note: If oral fluids are to be used, salt must be added 25
26 Volume of fluid Volume of fluid to be given in first 24 hours is calculated by Parkland formula; Volume in ml = Total percentage body surface area x weight in Kg x 4 Half of this volume is given in the first 8 hours, & the second half is given in the subsequent 16 hours. In children, maintenance fluid (dextrose saline) must also be given, as follows; 100 ml per kg for 24 hours for the first 10 kg 50 ml per kg for the next 10 kg 20 ml per kg for each kg over 20 kg body weight 26
27 Monitoring of resuscitation Examination of patient's general clinical state: Pulse rate Blood pressure Temperature Jugular venous pressure Skin perfusion Color & temperature Urine output should be between 0.5 & 1.0 ml per kg per hour; If the urine output falls, the infusion rate should be increased by 50%. If the urine output is inadequate & patient is showing signs of hypoperfusion then a bolus of 10 ml per kg body weight should be given. Urine output in excess of 2 ml kg body weight per hour should signal a decrease in the rate of infusion. Acid base balance. Hematocrit measurement. 27
28 Burn Wound Care Cold water compresses to relieve pain of partial thickness burns. Remove any adherent clothing, dirt or foreign material by gentle rinsing with warm sterile water. Escharotomy Circumferential full thickness burns to the limbs & chest require emergency incision; whole length of full thickness burn is incised in the mid axial line (avoiding major nerves). Special measures: In hand burns Burnt hands should be enclosed in polythene bags, elevated & actively exercised. In burns of eyelids Skin graft. 28

29 29
30 Burn Wound Care Burns dressing Full thickness & deep dermal burns need antibacterial dressings to delay colonization prior to surgery; 1% silver sulphadiazine cream. 0.5% silver nitrate solution. Matenide acetate cream. Serum nitrate. 30
31 Burns dressing Superficial partial-thickness & mixed depth burns; Superficial partial thickness burns will heal almost irrespective of the dressing. If the wound is heavily contaminated then clean the wound under a general anesthetic. With more chronic contamination, silver sulphadiazine cream dressing for 2 or 3 days is very effective. Simplest method of treating a superficial wound is by exposure. This is often used in hot climates, & for small burns on the face. Burns can be covered with a permeable wound dressing such as Mefix, or with vaseline impregnated gauze with or without an antiseptic eg chlorhexidin, or with a fenestrated silicone sheet. Swabs need to be changed after the first 48 hours as they are often soaked; after that they can be let for longer. Hydrocolloid dressings (eg duoderm) are particularly useful in mixed depth burns, & they need to be changed every 3-5 days. Biological, synthetic (eg biobrane) & natural (eg amniotic membrane) dressings also provide good healing environments & do not need to be changed. 31
32 Analgesics Superficial burns, respond well to simple oral analgesia. Topical cooling is especially soothing. Large burns require continuous analgesia, beginning with infusions & continuing with oral tablets eg slow release morphine. Powerful, short acting analgesia should be given before dressing changes. 32
33 Energy balance & nutrition Burns patients need extra feeding. A nasogastric tube should be used in all patients with burns over 20% TBSA, & feeding should start within 6 hours of the injury to reduce gut mucosal damage. Removing the burn & achieving healing stops the catabolic drive. Monitored by measuring weight & nitrogen balance. 33
34 Other Considerations Control of infection Burns patients are immunocompromized, & are susceptible to infection from many routes. Sterile precautions must be rigorous, & swabs should be taken regularly. A rise in WBC count, thrombocytosis & increased catabolism are warnings of infection. A 5-day course of penicillin or erythromycin is required in patients with deep & full thickness burns. Tetanus toxoid booster should be given in all cases. Prevention of early complications Acute renal failure By early & proper restoration of blood volume & maintenance of fluid balance. Curling's ulcers By prescribing cimetidine or ranitidine. Nursing care Personal hygiene, baths & showers. Physiotherapy Elevation, splintage & exercise reduce swelling & improve the final outcome. Physiotherapy needs to be started on day 1. Psychological support Constant encouragement & positive reassurance. 34
35 Surgery For Acute Burn Wound Any deep partial thickness & full thickness burns, except those which are less than about 4 cm2 need surgery. Deep dermal burns need tangential shaving & split skin grafting. Topical adrenaline reduces bleeding, but the anesthetist needs to be ready for significant blood loss. Full thickness burns require full thickness excision of the skin. Wherever possible, a skin graft should be applied immediately. With very large burns the use of synthetic dermis or homografts provides temporary stable coverage. 35
36 Postoperative management Maintenance of fluid balance & hemoglobin level. Physiotherapy & splints to maintain range of movement & reducing joint contracture. Elevation of appropriate limbs is important. Hand must be splinted in a position of function after grafting. 36
37 Complications of burns Early Acute renal failure Curling's ulcers Late Chronic duodenal ulcer Protein losing enteropathy Chronic renal failure Immune deficiency Marjolin's ulcer 37

38 38
39 Delayed Reconstruction & Scar Management Eyelids must be treated before exposure keratitis arises. Z-plasty is useful in cases of a single band, & a transposition flap is useful in wider bands of scarring. In areas of circumferential or very broad areas of scarring the only treatment is incision & replacement with tissue from either a full thickness graft or vascularized tissue as in a free flap. Burn alopecia is best treated with tissue expansion of unburned hair bearing skin. Hypertrophy is treated with pressure garments; these need to be worn for a period of 6-18 months. Silicone patches will speed scar maturation, as will intralesional injection of steroid. Pharmacological treatment of itch may be required. 39






40 A mixed superficial and deep burn to the face after a petrol explosion. The patient s airway was protected prior to transfer. He has an orogastric tube and feeding has commenced. The face dressed with a hydrocolloid dressing. The endotracheal tube is wired to the teeth. Day 6: the swelling is still present. Six weeks after injury. With the mouth wide open, the lower eyelids are pulled down, demonstrating the intrinsic and extrinsic shortening of the eyelids. Three months after injury. The eyelids have been grafted but note the contracture of the lips. Six months after injury. The patient has had grafts to the upper and lower lips. 40
41 A 13 year old boy, 22 kg, suffers 35% burns involving both upper limbs & anterior aspect of trunk. What is the fluid requirement in first 8 hours? A = 6160 ml B = 4620 ml C = 3080 ml D = 2310 ml E = 1540 ml 22 x 35 x 4 = 3080 / 2 = = 1540/2 = 770 Answer: D 41

42 42
BURNS MODULE. In the paediatric population consider non-accidental injury as a mechanism for burn injuries.
 BURNS MODULE INTRODUCTION Burns are a common cause of trauma. Most burn injuries are a result of flame burns, with scalds also occurring commonly. Electrical and chemical burns are less common. 1 Concurrent
BURNS MODULE INTRODUCTION Burns are a common cause of trauma. Most burn injuries are a result of flame burns, with scalds also occurring commonly. Electrical and chemical burns are less common. 1 Concurrent
Burns. A Comprehensive Review Assessment & Management
 Burns A Comprehensive Review Assessment & Management 1 Objectives Understand types of Burns Understand the pathophysiology of the Burns Understand Rule of Nine Understand Classification of Burns Identify
Burns A Comprehensive Review Assessment & Management 1 Objectives Understand types of Burns Understand the pathophysiology of the Burns Understand Rule of Nine Understand Classification of Burns Identify
Dóra Ujvárosy MD. Medical University of Debrecen Oxyology and Emergency Department
 Dóra Ujvárosy MD. Medical University of Debrecen Oxyology and Emergency Department Functions Definition A burn is a type of injury to the skin caused by heat, electricity, chemicals, light, radiation or
Dóra Ujvárosy MD. Medical University of Debrecen Oxyology and Emergency Department Functions Definition A burn is a type of injury to the skin caused by heat, electricity, chemicals, light, radiation or
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 46 Caring for Clients with Burns Types of Burns Thermal Dry heat flame Moist heat steam or hot liquid
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 46 Caring for Clients with Burns Types of Burns Thermal Dry heat flame Moist heat steam or hot liquid
At the conclusion of this course the learner will be able to
 Objectives At the conclusion of this course the learner will be able to 1. Discuss basic anatomy and pathophysiology of burns 2. Describe burn injuries in terms of size, depth, coloration and characteristics
Objectives At the conclusion of this course the learner will be able to 1. Discuss basic anatomy and pathophysiology of burns 2. Describe burn injuries in terms of size, depth, coloration and characteristics
Burn Injuries & Its Management M JARI.MD
 Burn Injuries & Its Management M JARI.MD 1 BURNS Wounds caused by exposure to: 1. excessive heat 2. Chemicals 3. fire/steam 4. radiation 5. electricity 2 BURNS Results in 10-20 thousand deaths annually
Burn Injuries & Its Management M JARI.MD 1 BURNS Wounds caused by exposure to: 1. excessive heat 2. Chemicals 3. fire/steam 4. radiation 5. electricity 2 BURNS Results in 10-20 thousand deaths annually
Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test
 Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test Purpose: To provide nurses with on overview of burn injuries in pediatric patients. Learning Objectives:
Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test Purpose: To provide nurses with on overview of burn injuries in pediatric patients. Learning Objectives:
IMMEDIATE EMERGENCY BURN CARE » THERMAL BURNS » ELECTRICAL BURNS » CHEMICAL BURNS FIRST AID FOR THE THREE MAJOR CATEGORIES
 IMMEDIATE EMERGENCY BURN CARE 1. Treat according to BLS or ACLS Protocol 2. Use airway and C-Spine precautions. 3. Stop the burning process. FIRST AID FOR THE THREE MAJOR CATEGORIES» THERMAL BURNS + Stop
IMMEDIATE EMERGENCY BURN CARE 1. Treat according to BLS or ACLS Protocol 2. Use airway and C-Spine precautions. 3. Stop the burning process. FIRST AID FOR THE THREE MAJOR CATEGORIES» THERMAL BURNS + Stop
Current Concepts in Burn Rehabilitation
 Current Concepts in Burn Rehabilitation 7 th Congress of the Baltic Association of Rehabilitation Tallinn, Estonia September 2010 R. Scott Ward, PT, PhD Professor and Chair Department of Physical Therapy
Current Concepts in Burn Rehabilitation 7 th Congress of the Baltic Association of Rehabilitation Tallinn, Estonia September 2010 R. Scott Ward, PT, PhD Professor and Chair Department of Physical Therapy
BLS, ILS, ALS OTEP BURNS BURN INTRODUCTION TYPES OF BURNS
 BURNS BLS, ILS, ALS OTEP While we do understand this presentation is an instructional tool for all levels of certification, taking this into consideration everyone taking this class must remember that
BURNS BLS, ILS, ALS OTEP While we do understand this presentation is an instructional tool for all levels of certification, taking this into consideration everyone taking this class must remember that
Advanced Paediatric Nursing. Burn Trauma. 26 April Wong Tze Wing NC (Burns), Burns Centre, Surgery, PWH
, Burns Centre, Surgery, PWH") Advanced Paediatric Nursing Burn Trauma 26 April 2016 Wong Tze Wing NC (Burns), Burns Centre, Surgery, PWH Objective: Understand burn trauma in children Understand Important nursing interventions in burn
Advanced Paediatric Nursing Burn Trauma 26 April 2016 Wong Tze Wing NC (Burns), Burns Centre, Surgery, PWH Objective: Understand burn trauma in children Understand Important nursing interventions in burn
Burn Priorities of Care: Triage/Treatment/Transfer. Via Christi Regional Burn Center Sarah Fischer, MSN, RN
 Burn Priorities of Care: Triage/Treatment/Transfer Via Christi Regional Burn Center Sarah Fischer, MSN, RN Disclosure I have nothing to disclose Objectives Identify American Burn Association referral criteria
Burn Priorities of Care: Triage/Treatment/Transfer Via Christi Regional Burn Center Sarah Fischer, MSN, RN Disclosure I have nothing to disclose Objectives Identify American Burn Association referral criteria
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS. December 19, 2012
 PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
Responsibility This guideline applies to teams of health professions caring for burn patients.
 Page 1 of 9 Guideline: Initial Assessment & Management of Burn Injuries Purpose This document provides a guideline for the initial assessment and management of burn patients. It is not intended as a full
Page 1 of 9 Guideline: Initial Assessment & Management of Burn Injuries Purpose This document provides a guideline for the initial assessment and management of burn patients. It is not intended as a full
Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator
 Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator Lecture Overview Burn statistics and etiologies Pre-hospital evaluation Anatomy of a burn
Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator Lecture Overview Burn statistics and etiologies Pre-hospital evaluation Anatomy of a burn
Objectives. Initial Burn Care and Fluid Resuscitation 6/5/2015 INITIAL MANAGEMENT
 Initial Burn Care and Fluid Resuscitation Sarah Taylor MSN, RN, ACNS-BC Clinical Nurse Specialist Trauma Burn Center University of Michigan Health System Ann Arbor, MI Objectives Discuss the initial assessment
Initial Burn Care and Fluid Resuscitation Sarah Taylor MSN, RN, ACNS-BC Clinical Nurse Specialist Trauma Burn Center University of Michigan Health System Ann Arbor, MI Objectives Discuss the initial assessment
Wisecracks 1. What are the indications for an escharotomy 2. What are the primary considerations in mechanical ventilation of burn patients
 Chapter 63 Thermal Burns Episode Overview Questions 1. List zones of burns 2. List 6 indications for intubation in the burn patient 3. List and describe 2 formulas for fluid resuscitation 4. Describe depth
Chapter 63 Thermal Burns Episode Overview Questions 1. List zones of burns 2. List 6 indications for intubation in the burn patient 3. List and describe 2 formulas for fluid resuscitation 4. Describe depth
The immediate management of burns patients should be similar to management of trauma.
 CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
EmergencyKT: Management of Thermal Injury in Adult Patients
 EmergencyKT: Management of Thermal Injury in Adult Patients Remove patient from source of injury, including burned clothing and jewelry Does patient appear to have minor burns? (See Box A) No Notify Burn
EmergencyKT: Management of Thermal Injury in Adult Patients Remove patient from source of injury, including burned clothing and jewelry Does patient appear to have minor burns? (See Box A) No Notify Burn
BASICS OF BURN MANAGEMENT
 BASICS OF BURN MANAGEMENT Dr S M Keswani Cosmetic Surgeon National Burns Centre, Airoli,Navi-Mumbai Breach Candy Hospital Wockhardt Hospital National Burns Centre, Airoli, Navi-Mumbai. CLASSIFICATION 1.
BASICS OF BURN MANAGEMENT Dr S M Keswani Cosmetic Surgeon National Burns Centre, Airoli,Navi-Mumbai Breach Candy Hospital Wockhardt Hospital National Burns Centre, Airoli, Navi-Mumbai. CLASSIFICATION 1.
Chapter 23 Caring for Clients with Burns
 Chapter 23 Caring for Clients with Burns Burn Injuries 4500 people die from burns each year High risk group ~ children and the elderly The most common cause of burns Smoking material Scalding Lighting
Chapter 23 Caring for Clients with Burns Burn Injuries 4500 people die from burns each year High risk group ~ children and the elderly The most common cause of burns Smoking material Scalding Lighting
Approved By: Airway and Breathing A. Initially give humidified high flow oxygen at 15 L (100%) using a nonrebreather
 using a nonrebreather") Subject: BURN CARE CLINICAL GUIDELINE Originator: Approval Date: 2015 Approved By: Policy: All burn patients presenting to XXXXXX Hospital will have appropriate assessment, stabilization and evaluation
Subject: BURN CARE CLINICAL GUIDELINE Originator: Approval Date: 2015 Approved By: Policy: All burn patients presenting to XXXXXX Hospital will have appropriate assessment, stabilization and evaluation
Mr Zachary Moaveni Plastic Surgeon, Middlemore Hospital. Mr Adam Bialostocki Plastic Surgeon, Tauranga
 Mr Zachary Moaveni Plastic Surgeon, Middlemore Hospital Mr Adam Bialostocki Plastic Surgeon, Tauranga Mr. Adam Bialostocki Plastic Surgeon Minor Burns First Aid Remove the burning agent / wet clothes
Mr Zachary Moaveni Plastic Surgeon, Middlemore Hospital Mr Adam Bialostocki Plastic Surgeon, Tauranga Mr. Adam Bialostocki Plastic Surgeon Minor Burns First Aid Remove the burning agent / wet clothes
LRI Emergency Department. Burn injuries management in adults
 LRI Emergency Department Clinical guideline for: Burn injuries management in adults Authors: Approved by: Martin Wiese Reena Agarwal Claire Porter EF guidelines committee Approval date: 21 Sep 16 Approval
LRI Emergency Department Clinical guideline for: Burn injuries management in adults Authors: Approved by: Martin Wiese Reena Agarwal Claire Porter EF guidelines committee Approval date: 21 Sep 16 Approval
INTRODUCTION OBJECTIVES. When the student has finished this module, he/she will be able to:
 Burn Care and Management WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A., RN.ORG,
Burn Care and Management WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A., RN.ORG,
Burn wounds - Determining the size and type degree
 1 Burn wounds - Determining the size and type degree Determining surface area of burn (Open hand only for small burns) 1 2 Burn depth Most burns are a combination of superficial and deeper burns and the
1 Burn wounds - Determining the size and type degree Determining surface area of burn (Open hand only for small burns) 1 2 Burn depth Most burns are a combination of superficial and deeper burns and the
Management of Acute Burn Injuries: The First 24 Hours
 Speaker Disclosure I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. I will not discuss off label uses of any pharmaceutical products or medical devices. Management of Acute
Speaker Disclosure I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. I will not discuss off label uses of any pharmaceutical products or medical devices. Management of Acute
Chapter 29. Objectives. Objectives 01/09/2013. Burns
 Chapter 29 Burns Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced in
Chapter 29 Burns Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced in
Skin Integrity and Wound Care
 Skin Integrity and Wound Care By Dr. Amer Hasanien & Dr. Ali Saleh Skin Integrity and Wound Care Skin integrity: the presence of normal Skin & Uninterrupted skin layers by wounds. Factors affecting appearance
Skin Integrity and Wound Care By Dr. Amer Hasanien & Dr. Ali Saleh Skin Integrity and Wound Care Skin integrity: the presence of normal Skin & Uninterrupted skin layers by wounds. Factors affecting appearance
QI. Read the following questions and choose the most correct answer (20 Marks):
:") Question One: QI. Read the following questions and choose the most correct answer (20 Marks): 1- Some people are very allergic to some drugs like penicillin. This condition is called: a) Septic shock.
Question One: QI. Read the following questions and choose the most correct answer (20 Marks): 1- Some people are very allergic to some drugs like penicillin. This condition is called: a) Septic shock.
Case Report: Burns Reid Sadoway PGY1 Emergency Medicine, Dalhousie
 Case Report: Burns Reid Sadoway PGY1 Emergency Medicine, Dalhousie History 3 yo boy, presents to pediatric ED with mother Child can be heard crying inside waiting/patient room, has both hands bandaged
Case Report: Burns Reid Sadoway PGY1 Emergency Medicine, Dalhousie History 3 yo boy, presents to pediatric ED with mother Child can be heard crying inside waiting/patient room, has both hands bandaged
Epidemiology. Burn Rehabilitation. Epidemiology. Epidemiology. United States. United States Cause of injury. Incidence has declined
 Burn Rehabilitation Peter Esselman, MD Professor and Chair Department of Rehabilitation Medicine University of Washington Epidemiology United States 450,000 burn injuries/year in USA that receive medical
Burn Rehabilitation Peter Esselman, MD Professor and Chair Department of Rehabilitation Medicine University of Washington Epidemiology United States 450,000 burn injuries/year in USA that receive medical
Burn injury. A : patent airway with smoking inhalation, stridor. D: E4V5M6,pupil 2mm RTLBE
 Burn injury Pinyong Uthaitas Emergency Department Faculty of Medicine, Ramathibodi Hospital A Thai man 52 year old came to the hospital due to flam burn ½ hr ago at his house. He gain conscious but hoarseness
Burn injury Pinyong Uthaitas Emergency Department Faculty of Medicine, Ramathibodi Hospital A Thai man 52 year old came to the hospital due to flam burn ½ hr ago at his house. He gain conscious but hoarseness
WOUNDS. Emergency Procedures in PT
 WOUNDS Emergency Procedures in PT Types of Wounds Abrasions uppermost layer scraped away, minor capillary bleeding occurs, nerve endings exposed Lacerations skin tear with edges jagged and uneven Incisions
WOUNDS Emergency Procedures in PT Types of Wounds Abrasions uppermost layer scraped away, minor capillary bleeding occurs, nerve endings exposed Lacerations skin tear with edges jagged and uneven Incisions
Burns & its Homoeopathic Management - Pawan Satyanarayan Chandak
 Page 1 of 7 Burns & its Homoeopathic Management Pawan Satyanarayan Chandak A burn is a tissue injury from thermal heat or cold application or from the absorption of physical energy or chemical contact.
Page 1 of 7 Burns & its Homoeopathic Management Pawan Satyanarayan Chandak A burn is a tissue injury from thermal heat or cold application or from the absorption of physical energy or chemical contact.
Burns Management in the Emergency Department
 Management in the Emergency Department (Referral Proforma) Time/Date of injury (24hr) Patient demographic data sticker Airway Please remember to protect C-spine until clinically cleared as stable Administer
Management in the Emergency Department (Referral Proforma) Time/Date of injury (24hr) Patient demographic data sticker Airway Please remember to protect C-spine until clinically cleared as stable Administer
Pediatrics Grand Rounds 1 June University of Texas Health Science Center at San Antonio. Management of Burn Wounds. Management of Burn Wounds
 Management of Burn Wounds Management of Burn Wounds History of Burn Care Pathophysiology of Burn Lillian F. Liao, MD, MPH Division of Trauma and Emergency Surgery Department of Surgery UTHSCSA Acute burn
Management of Burn Wounds Management of Burn Wounds History of Burn Care Pathophysiology of Burn Lillian F. Liao, MD, MPH Division of Trauma and Emergency Surgery Department of Surgery UTHSCSA Acute burn
Chapter 24 Soft Tissue Injuries Presentation Notes
 Names: Chapter 24 Soft Tissue Injuries Presentation Notes Anatomy of the Skin - Function of the Skin control Soft-Tissue Injuries injuries Soft-tissue damage the skin injuries Break in the of the skin
Names: Chapter 24 Soft Tissue Injuries Presentation Notes Anatomy of the Skin - Function of the Skin control Soft-Tissue Injuries injuries Soft-tissue damage the skin injuries Break in the of the skin
Skin Anatomy and Physiology
 Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Modern management of paediatric burns
 Modern management of paediatric burns Burn injuries pose a major threat to children in South Africa and remain a devastating injury, because of the resulting severe emotional and physical scarring and
Modern management of paediatric burns Burn injuries pose a major threat to children in South Africa and remain a devastating injury, because of the resulting severe emotional and physical scarring and
INITIAL CARE AND TREATMENT OF BURN INJURIES. November 10,
 INITIAL CARE AND TREATMENT OF BURN INJURIES 2 11/10/2012 November 10, 2012 2 Oregon Burn Center Only burn center in Oregon and SW Washington New unit 16 beds, 20,000 square feet Opened in February 2002
INITIAL CARE AND TREATMENT OF BURN INJURIES 2 11/10/2012 November 10, 2012 2 Oregon Burn Center Only burn center in Oregon and SW Washington New unit 16 beds, 20,000 square feet Opened in February 2002
Speaker Disclosure Emergent Burn Care I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose.
 Speaker Disclosure Emergent Burn Care I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. Debbie Harrell RN, MSN, Shriners Hospitals for Children Cincinnati Cincinnati, Ohio
Speaker Disclosure Emergent Burn Care I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. Debbie Harrell RN, MSN, Shriners Hospitals for Children Cincinnati Cincinnati, Ohio
Burns and electrical injuries. Shelley Westwood, RN, BSN
 Burns and electrical injuries Shelley Westwood, RN, BSN Burns A burn is an injury caused by fire, heat, chemicals, radiation, or electricity. Burns are traumatic in that they can cause extreme pain, permanent
Burns and electrical injuries Shelley Westwood, RN, BSN Burns A burn is an injury caused by fire, heat, chemicals, radiation, or electricity. Burns are traumatic in that they can cause extreme pain, permanent
Erin P. Frazier, OTR/L Occupational Therapist Jessica Maher, PT, MSPT Physical Therapist
 Management of Burns for The Pediatric Patient Erin P. Frazier, OTR/L Occupational Therapist efrazier@mwph.org Jessica Maher, PT, MSPT Physical Therapist jmaher@mwph.org Mt. Washington Pediatric Hospital
Management of Burns for The Pediatric Patient Erin P. Frazier, OTR/L Occupational Therapist efrazier@mwph.org Jessica Maher, PT, MSPT Physical Therapist jmaher@mwph.org Mt. Washington Pediatric Hospital
Review. A. abrasion B. contusion C. hematoma D. avulsion
 Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
Thermal Injuries. Manika Bhandari, Malika Bhola, Rucha Desai, Dhruvika Joshi, Abir Shamim Life Science 4M03
 Thermal Injuries Manika Bhandari, Malika Bhola, Rucha Desai, Dhruvika Joshi, Abir Shamim Life Science 4M03 INTRODUCTION Anatomy of the skin The skin has three anatomical layers Epidermis Dermis Subcutaneous
Thermal Injuries Manika Bhandari, Malika Bhola, Rucha Desai, Dhruvika Joshi, Abir Shamim Life Science 4M03 INTRODUCTION Anatomy of the skin The skin has three anatomical layers Epidermis Dermis Subcutaneous
Patient Details Hospital number NHS number. Surname First name DOB. Permanent address. Post code. Mobile No. Temporary. Mother DOB. Father.
 Burns Unit Page 12 Paediatric Burn Injuries - Assessment & Admission Burns Unit Page 1 Discharge Patient Details Hospital number NHS number Admission date Injury date Hospital Use time time Time: Discharge
Burns Unit Page 12 Paediatric Burn Injuries - Assessment & Admission Burns Unit Page 1 Discharge Patient Details Hospital number NHS number Admission date Injury date Hospital Use time time Time: Discharge
Initial assessment. ATLS/ABLS protocol and assess for other injuries/fractures based on mechanism. Inhalational injury. Vascular compromise:
 Complex Hand Burns Brent Egeland, MD Assistant Professor Dell Medical School Department of Surgery and Perioperative Care Institute of Reconstructive Plastic Surgery Plastic, Hand, and Reconstructive Microsurgery
Complex Hand Burns Brent Egeland, MD Assistant Professor Dell Medical School Department of Surgery and Perioperative Care Institute of Reconstructive Plastic Surgery Plastic, Hand, and Reconstructive Microsurgery
CARE OF PATIENTS WITH BURNS. NUR 240 Donna Ricketts, MSN, RN, OCN
 CARE OF PATIENTS WITH BURNS NUR 240 Donna Ricketts, MSN, RN, OCN INCIDENCE/PREVALENCE OF BURN INJURY 5 th most common unintentional injury deaths 3 rd leading cause of fatal home injuries 4,000 burn deaths
CARE OF PATIENTS WITH BURNS NUR 240 Donna Ricketts, MSN, RN, OCN INCIDENCE/PREVALENCE OF BURN INJURY 5 th most common unintentional injury deaths 3 rd leading cause of fatal home injuries 4,000 burn deaths
MY STRATEGY FOR TREATING BURN INJURIES. Warren Garner MD FACS Keck School of Medicine at USC Los Angeles, CA
 MY STRATEGY FOR TREATING BURN INJURIES Warren Garner MD FACS Keck School of Medicine at USC Los Angeles, CA ASSUMPTIONS: Burns which heal to normal have best outcome. Medical risk, functional recovery,
MY STRATEGY FOR TREATING BURN INJURIES Warren Garner MD FACS Keck School of Medicine at USC Los Angeles, CA ASSUMPTIONS: Burns which heal to normal have best outcome. Medical risk, functional recovery,
Fire Deaths. Dr Julie McAdam Consultant Forensic Pathologist Glasgow University
 Fire Deaths Dr Julie McAdam Consultant Forensic Pathologist Glasgow University Forensic investigation multidisciplinary fire officers, police officers, scientists, photographers, pathologist, procurator
Fire Deaths Dr Julie McAdam Consultant Forensic Pathologist Glasgow University Forensic investigation multidisciplinary fire officers, police officers, scientists, photographers, pathologist, procurator
Burn & Soft Tissue Service Orientation Slides
 Burn & Soft Tissue Service Orientation Slides Damien Wilson Carter, MD Director, Burn/Soft Tissue Service Sue Reeder, BSN, CWOCN Burn Resource Nurse Specialist Scope ALL Burn injuries (> Age 12) Cold injury/
Burn & Soft Tissue Service Orientation Slides Damien Wilson Carter, MD Director, Burn/Soft Tissue Service Sue Reeder, BSN, CWOCN Burn Resource Nurse Specialist Scope ALL Burn injuries (> Age 12) Cold injury/
The Affects of Music Therapy on Management of Pain and Anxiety During Burn Dressing Changes
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2014 The Affects of Music Therapy on Management
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2014 The Affects of Music Therapy on Management
Sidney Miller, MD, FACS Professor of Surgery Director of Research and Development Ohio State University Burn Center
 Management of the Burn Patient Sidney Miller, MD, FACS Professor of Surgery Director of Research and Development Ohio State University Burn Center American Burn Association Transfer Criteria Burn > 10%
Management of the Burn Patient Sidney Miller, MD, FACS Professor of Surgery Director of Research and Development Ohio State University Burn Center American Burn Association Transfer Criteria Burn > 10%
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES
 INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES 180801 1 Tactical Combat Casualty Care for Medical Personnel 1. August 2017 (Based on TCCC-MP Guidelines 180801 In this presentation, we
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES 180801 1 Tactical Combat Casualty Care for Medical Personnel 1. August 2017 (Based on TCCC-MP Guidelines 180801 In this presentation, we
Burn Wound Assessment and Infections
 Burn Wound Assessment and Infections Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Family Health:
Burn Wound Assessment and Infections Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Family Health:
Printed copies of this document may not be up to date, obtain the most recent version from Author Position
 Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle Author Position PICU/BURNS Consultant CATS Consultant Document Owner E. Polke
Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle Author Position PICU/BURNS Consultant CATS Consultant Document Owner E. Polke
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Basic First Aid. Sue Fisher Emergency Management Coordinator CSUF University Police
 Basic First Aid Sue Fisher Emergency Management Coordinator CSUF University Police Information given for this lecture is not meant to replace any official training by the American Red Cross, or any other
Basic First Aid Sue Fisher Emergency Management Coordinator CSUF University Police Information given for this lecture is not meant to replace any official training by the American Red Cross, or any other
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Chapter 28. Wound Care. Copyright 2019 by Elsevier, Inc. All rights reserved.
 Chapter 28 Wound Care Copyright 2019 by Elsevier, Inc. All rights reserved. Lesson 28.1 Define the key terms and key abbreviations in this chapter. Describe skin tears, circulatory ulcers, and diabetic
Chapter 28 Wound Care Copyright 2019 by Elsevier, Inc. All rights reserved. Lesson 28.1 Define the key terms and key abbreviations in this chapter. Describe skin tears, circulatory ulcers, and diabetic
SKIN INTEGRITY & WOUND CARE
 SKIN INTEGRITY & WOUND CARE Chapter 34 1 skin integrity: intact skin refers to the presence of normal skin layer uninterrupted by wound 2 WOUNDS DISRUPTION IN THE INTEGRITY OF BODY TISSUE CLASSIFIED AS:
SKIN INTEGRITY & WOUND CARE Chapter 34 1 skin integrity: intact skin refers to the presence of normal skin layer uninterrupted by wound 2 WOUNDS DISRUPTION IN THE INTEGRITY OF BODY TISSUE CLASSIFIED AS:
Proceedings of the 36th World Small Animal Veterinary Congress WSAVA
 www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
Applicable to. Team Members Performing MD House Staff APRN/PA RN LPN
 Protocol: Adult Burn Fluid Resuscitation Category Clinical Practice Protocol Number Approval Date vember 1, 2016 Due for review vember 1, 2018 Applicable to VUH Children s DOT VMG Off-site locations VMG
Protocol: Adult Burn Fluid Resuscitation Category Clinical Practice Protocol Number Approval Date vember 1, 2016 Due for review vember 1, 2018 Applicable to VUH Children s DOT VMG Off-site locations VMG
NovoSorb BTM. A unique synthetic biodegradable wound scaffold. Regenerating tissue. Changing lives.
 NovoSorb BTM A unique synthetic biodegradable wound scaffold Regenerating tissue. Changing lives. Overview NovoSorb BTM is a unique synthetic biodegradable wound scaffold that delivers good cosmetic and
NovoSorb BTM A unique synthetic biodegradable wound scaffold Regenerating tissue. Changing lives. Overview NovoSorb BTM is a unique synthetic biodegradable wound scaffold that delivers good cosmetic and
Burns and Scalds. Treatment and Management. Accident and Emergency Department. Royal Surrey County Hospital. Patient information leaflet
 Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Burns and Scalds Treatment and Management Accident and Emergency Department A Burn is an injury caused to the skin by thermal
Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Burns and Scalds Treatment and Management Accident and Emergency Department A Burn is an injury caused to the skin by thermal
Burn Management. Praz Patcha, MD 13 March 2014
 Burn Management Praz Patcha, MD 13 March 2014 Epidemiology 500,000 / yr 40,000 to 60,000 requiring admission < 1% total injuries in US but $10.4 billion Risk Factors Age Location Demographics Socioeconomics
Burn Management Praz Patcha, MD 13 March 2014 Epidemiology 500,000 / yr 40,000 to 60,000 requiring admission < 1% total injuries in US but $10.4 billion Risk Factors Age Location Demographics Socioeconomics
Disaster Medical Operations-Part 2
 Disaster Medical Operations-Part 2 Community Emergency Response Team Disaster Medical Operations Part 1 Review The killers Airway obstruction Excessive bleeding Shock All immediate receive airway control,
Disaster Medical Operations-Part 2 Community Emergency Response Team Disaster Medical Operations Part 1 Review The killers Airway obstruction Excessive bleeding Shock All immediate receive airway control,
Current Trends in Burn Care
 Objectives Current Trends in Burn Care Jordan Murphy, BSN, CFRN Clinical Educator-KY/FL PHI Air Medical Describes normal skin anatomy. Differentiates pathophysiology related to etiology of injury. Identify
Objectives Current Trends in Burn Care Jordan Murphy, BSN, CFRN Clinical Educator-KY/FL PHI Air Medical Describes normal skin anatomy. Differentiates pathophysiology related to etiology of injury. Identify
Modern management of paediatric burns
 Modern management of paediatric burns Burn injuries pose a major threat to children in South Africa and remain a devastating injury, because of the resulting severe emotional and physical scarring and
Modern management of paediatric burns Burn injuries pose a major threat to children in South Africa and remain a devastating injury, because of the resulting severe emotional and physical scarring and
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Printed copies of this document may not be up to date, obtain the most recent version from Author Position
 Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle, L Chigaru Author Position PICU/BURNS Consultant CATS Consultants Document
Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle, L Chigaru Author Position PICU/BURNS Consultant CATS Consultants Document
MANAGING THE BURN WOUND
 MANAGING THE BURN WOUND Robert H. Demling, M.D. Leslie DeSanti R.N., Brigham and Women s Hospital Burn Center Harvard Medical School Boston, MA TABLE OF CONTENTS Section I: Section II: Section III: Section
MANAGING THE BURN WOUND Robert H. Demling, M.D. Leslie DeSanti R.N., Brigham and Women s Hospital Burn Center Harvard Medical School Boston, MA TABLE OF CONTENTS Section I: Section II: Section III: Section
Wound Care in the Community. Lisa Sutherland MSc Tissue Viability Senior Lead Ipswich Hospital & Community NHS Trusts
 Wound Care in the Community Lisa Sutherland MSc Tissue Viability Senior Lead Ipswich Hospital & Community NHS Trusts What are the key elements? What is the patient s goal or aim for the wound? What are
Wound Care in the Community Lisa Sutherland MSc Tissue Viability Senior Lead Ipswich Hospital & Community NHS Trusts What are the key elements? What is the patient s goal or aim for the wound? What are
Appendix (i) The ABCDE approach to the sick patient
 The ABCDE approach to the sick patient") Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Bleeding and Shock *** CME Version *** Aaron J. Katz, AEMT-P, CIC
 Bleeding and Shock *** CME Version *** Aaron J. Katz, AEMT-P, CIC www.es26medic.net Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to
Bleeding and Shock *** CME Version *** Aaron J. Katz, AEMT-P, CIC www.es26medic.net Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to
Keloids. Disclaimer. Multimedia Health Education
 Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of must be made in conjunction with your Physician or a licensed healthcare
Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of must be made in conjunction with your Physician or a licensed healthcare
HEAT & COLD. Heat and cold applications applied to skin surface help treat certain conditions
 HEAT AND COLD HEAT & COLD Heat and cold applications applied to skin surface help treat certain conditions Heat and cold applications require a doctor s order when being used on a patient The body can
HEAT AND COLD HEAT & COLD Heat and cold applications applied to skin surface help treat certain conditions Heat and cold applications require a doctor s order when being used on a patient The body can
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
A PROSPECTIVE STUDY ON AURICULAR BURNS
 Int. J. Pharm. Med. & Bio. Sc. 2013 Ramesha K T et al., 2013 Research Paper ISSN 2278 5221 www.ijpmbs.com Vol. 2, No. 4, October 2013 2013 IJPMBS. All Rights Reserved A PROSPECTIVE STUDY ON AURICULAR BURNS
Int. J. Pharm. Med. & Bio. Sc. 2013 Ramesha K T et al., 2013 Research Paper ISSN 2278 5221 www.ijpmbs.com Vol. 2, No. 4, October 2013 2013 IJPMBS. All Rights Reserved A PROSPECTIVE STUDY ON AURICULAR BURNS
Principle Management of Wound and Fracture in Emergency Department
 Principle Management of Wound and Fracture in Emergency Department Presented in Clinical Update Seminar January 15 th 2011 dr. Tedjo Rukmoyo, SpOT (K) Spine Initial Management ATLS Procedure A : airway
Principle Management of Wound and Fracture in Emergency Department Presented in Clinical Update Seminar January 15 th 2011 dr. Tedjo Rukmoyo, SpOT (K) Spine Initial Management ATLS Procedure A : airway
STANDARD OPERATING PROCEDURE #203 LARGE ANIMAL SURGERY
 STANDARD OPERATING PROCEDURE #203 LARGE ANIMAL SURGERY 1. PURPOSE This Standard Operating Procedure (SOP) describes procedures for general surgery of large animal species such as swine, dogs, rabbits,
STANDARD OPERATING PROCEDURE #203 LARGE ANIMAL SURGERY 1. PURPOSE This Standard Operating Procedure (SOP) describes procedures for general surgery of large animal species such as swine, dogs, rabbits,
Introduction (1 of 3)
") Chapter 10 Shock Introduction (1 of 3) Shock (hypoperfusion) means a state of collapse and failure of the cardiovascular system. In the early stages, the body attempts to maintain homeostasis. As shock
Chapter 10 Shock Introduction (1 of 3) Shock (hypoperfusion) means a state of collapse and failure of the cardiovascular system. In the early stages, the body attempts to maintain homeostasis. As shock
Skin Deep. Agenda. Burns Wounds Debridement Evaluation and Management Services. Presented by: Mike Strong, SFM The Work Comp Experts.
 Presented by: Mike Strong, SFM The Work Comp Experts Agenda Wounds Debridement Evaluation and Management Services 2 1 Types of First Degree Second Degree Third Degree Rule of 9 Adults Infants Burn Coding
Presented by: Mike Strong, SFM The Work Comp Experts Agenda Wounds Debridement Evaluation and Management Services 2 1 Types of First Degree Second Degree Third Degree Rule of 9 Adults Infants Burn Coding
Chapter 14 8/23/2016. Surgical Wound Care. Wound Classifications. Wound Healing. Classified According to. Phases
 Chapter 14 Surgical Wound Care All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Wound Classifications Classified According to Cause Incision
Chapter 14 Surgical Wound Care All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Wound Classifications Classified According to Cause Incision
Aviation Rescue Swimmer Course
 Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
Wound Care Program for Nursing Assistants-
 Wound Care Program for Nursing Assistants- Wound Cleansing,Types & Presentation Elizabeth DeFeo, RN, WCC, OMS, CWOCN Wound, Ostomy, & Continence Specialist ldefeo@cornerstonevna.org Outline/Agenda At completion
Wound Care Program for Nursing Assistants- Wound Cleansing,Types & Presentation Elizabeth DeFeo, RN, WCC, OMS, CWOCN Wound, Ostomy, & Continence Specialist ldefeo@cornerstonevna.org Outline/Agenda At completion
Not All That Blisters Is a Burn! Jamie Hoffman-Rosenfeld, MD CHAMP Webinar December 6, 2012
 Not All That Blisters Is a Burn! Jamie Hoffman-Rosenfeld, MD CHAMP Webinar December 6, 2012 Objectives To review the epidemiology of burns in children including burns caused by abuse To review the steps
Not All That Blisters Is a Burn! Jamie Hoffman-Rosenfeld, MD CHAMP Webinar December 6, 2012 Objectives To review the epidemiology of burns in children including burns caused by abuse To review the steps
Surgical Management of wounds, flaps, grafts, and scars
 Disclosures Surgical Management of wounds, flaps, grafts, and scars I have no financial disclosures Cherrie Heinrich, MD, FACS Department of Plastic Surgery Regions Hospital Assistant Professor University
Disclosures Surgical Management of wounds, flaps, grafts, and scars I have no financial disclosures Cherrie Heinrich, MD, FACS Department of Plastic Surgery Regions Hospital Assistant Professor University
Getting Strarted using the Nursing Care Plans Templates
 Getting Strarted using the Nursing Care Plans Templates Using available Nursing Care Plan Templates. These templates are delivered as is and there is nothing which prevents you to use and modify these
Getting Strarted using the Nursing Care Plans Templates Using available Nursing Care Plan Templates. These templates are delivered as is and there is nothing which prevents you to use and modify these
Bleeding and Shock. Circulatory System
 Bleeding and Shock Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to body tissues Delivers
Bleeding and Shock Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to body tissues Delivers
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Purpose To outline the pre-hospital and inter-hospital assessment and management of patients with major burns.
 Major Burns HELI.CLI.08 Purpose To outline the pre-hospital and inter-hospital assessment and management of patients with major burns. Procedure Management of Severe Burns For Review Aug 2015 1. Introduction
Major Burns HELI.CLI.08 Purpose To outline the pre-hospital and inter-hospital assessment and management of patients with major burns. Procedure Management of Severe Burns For Review Aug 2015 1. Introduction
NOTE If it is necessary to perform abdominal thrusts, expose the abdominal area prior to pressing on the abdomen.
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
Gangrene. Introduction Gangrene is the death of tissues in your body. It happens when a part of your body loses its blood supply.
 Gangrene Introduction Gangrene is the death of tissues in your body. It happens when a part of your body loses its blood supply. Gangrene can happen on the surface of the body, such as on the skin. It
Gangrene Introduction Gangrene is the death of tissues in your body. It happens when a part of your body loses its blood supply. Gangrene can happen on the surface of the body, such as on the skin. It
Appendix. Sedatives and Pain Medications. Gabapentin ( mg po q8h) or Pregabalin ( mg po q8h)
 or Pregabalin ( mg po q8h)") Appendix Sedatives and Pain Medications Non-intubated patients Non-opioid analgesics Acetaminophen (500 1,000 mg po q6h) NSAID (Ibuprofen, Naprosyn, Celebrex) Gabapentin (100 300 mg po q8h) or Pregabalin
Appendix Sedatives and Pain Medications Non-intubated patients Non-opioid analgesics Acetaminophen (500 1,000 mg po q6h) NSAID (Ibuprofen, Naprosyn, Celebrex) Gabapentin (100 300 mg po q8h) or Pregabalin
EMERGENCYROOM BURN MANAGEMENT
 EMERGENCYROOM INITIAL ASSESSMENT PRIMARY SURVEY A = Airway and C-spine immobilization B = Breathing and Ventilation C = Circulation D = Disability, Neurologic Deficit E = Expose (remove all clothing and
EMERGENCYROOM INITIAL ASSESSMENT PRIMARY SURVEY A = Airway and C-spine immobilization B = Breathing and Ventilation C = Circulation D = Disability, Neurologic Deficit E = Expose (remove all clothing and
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
1.40 Prevention of Nosocomial Pneumonia
 1.40 Prevention of Nosocomial Pneumonia Purpose Audience Policy Statement: The guideline is designed to reduce the incidence of pneumonia and other acute lower respiratory tract infections. All UTMB healthcare
1.40 Prevention of Nosocomial Pneumonia Purpose Audience Policy Statement: The guideline is designed to reduce the incidence of pneumonia and other acute lower respiratory tract infections. All UTMB healthcare