INITIAL CARE AND TREATMENT OF BURN INJURIES. November 10,
|
|
|
- Beatrix Chapman
- 5 years ago
- Views:
Transcription
1

2 INITIAL CARE AND TREATMENT OF BURN INJURIES 2 11/10/2012 November 10,
3 Oregon Burn Center Only burn center in Oregon and SW Washington New unit 16 beds, 20,000 square feet Opened in February 2002 OBC offers on site therapy, pharmacy and family centered care November 10,



4 4 Oregon Burn Center State Education and Prevention Program Sponsored by: 11/10/2012 November 10,
5 Objectives Evaluate a burn injury Define magnitude and seriousness of injury Identify and establish priorities of treatment Identify airway injuries Discuss optimal fluid resuscitation Determine patients that should be transferred to a burn center 11/10/2012 5
6 Safety at Home 1.5 million people are burned each year Of these 650,000 are cared for by medical professionals Of these 75,000 will be hospitalized The vast majority of these injuries, >80 % will occur in our own home November 10,




7 Hand on stove-18 months Grease from deep fat fryer - 4 years old Partial thickness / second 11/10/2012 7

8 16 year old driving without seatbelt 11/10/2012 8

9 6 year old playing with matches 11/10/2012 9

10 Hot chocolate 11/10/

11 11/10/


12 Tap water 11/10/




13 Priming carburetor with gasoline Gas on trash fire 11/10/

14 Anatomy of the Skin (The Body s Largest Organ) Epidermis Dermis Sub Q Tissue and capillary network 11/10/
15 Functions of the Skin Protects against infection Prevents loss of body fluids Regulates body temperature Excretes body wastes Produces vitamin D Serves as a sensory organ Defines who we are as individuals 11/10/
16 Burn Injury Classification Thermal Electrical Chemical Inhalation 11/10/

17 Burn Types - Flame Burn Cooking caught shirt on fire 11/10/


18 Burn Types - Scald Burn tar Hot water from stove top 11/10/

19 Hot asphalt 11/10/

20 11/10/
21 FIRST AID KIT Mineral Oil or Petroleum Jelly 11/10/

22 Burn Types - Scald Burn Initial scald burn 11/10/

23 Burn Types - Scald Burn Scald, post burn eleven days 11/10/
24 BURN INJURIES ARE DECEIVING BURN INJURIES CAN GET WORSE OVER TIME 11/10/
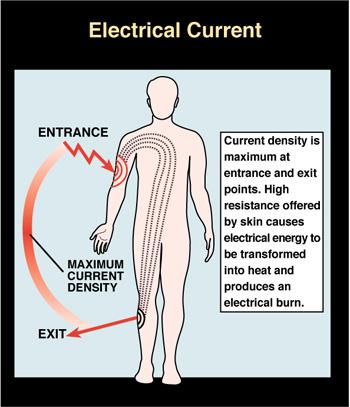
25 Electrical Burn Injuries Electrical injuries are some of the most debilitating burns a body can endure. Actual flame burns. Deep hidden tissue damage. Loss of limb or multiple limbs common. Potential for neurological injury. 11/10/
26 11/10/
27 Arc Injury Current does not pass through the tissue High heat, short duration No contact points No hidden tissue damage Rare cardiac arrythmias Volts- 110, 220,480 (480 most common) 11/10/

28 ARC Clothing on Fire 11/10/

29 Arc Flash Flame Burn 11/10/
30 Current Injury Voltage-> 1000 (usually 7000). Tissue acts as volume conductor. Contact points present. Deep, hidden tissue damage often present. Risk of myoglobinuria/renal failure. Limb loss common-usually multiple limb loss with high voltage. Flame injuries may also be involved. 11/10/

31 First contact or entrance site this arm is eventually amputated just below the shoulder 11/10/
32 WITH ELECTRICAL INJURIES THERE IS ALWAYS A POSSIBILITY OF HIDDEN TISSUE DAMAGE 11/10/

33 Deep Tissue Burn 11/10/

34 Current Injury Low Voltage 11/10/

35 LOW VOLTAGE Point of Grounding 11/10/

36 11/10/2012 Grounding points can vary in size
37 Electrical Injuries Always remember to turn off the electricity then remove the source Cardiac arrythmias are rare- if present they will be seen in the first minutes post injury Can result in cardiac arrest More often respiratory arrest is seen 11/10/
38 You First Do not become a victim Check the scene first Remove source of electricity 11/10/
39 At the Scene Remove the heat/ turn off electricity With electrical injuries there is always the possibility of explosions or a fall from a great height - check for other injuries Victim may often be confused and agitated - will want to move around 11/10/
40 At the Scene Do not need to put anything on the burn (burn gel) If possible obtain an accurate history -What happened -Loss of consciousness? -How many volts in contact with -Did bystanders have to do CPR -Did they fall or was there an explosion 11/10/
41 At the Scene Always consider intubation if necessary or if explosion or injury to face involved Start at least 2 IV sites To start - calculate fluid needs based on burn injuries seen - use parkland formula May need more fluids due to hidden tissue damage 11/10/
42 Get All Electrical Contacts Checked Out By a Physician Potential for hidden damage Possible delayed symptoms 11/10/


43 Hidden Damage 11/10/
44 Electrical Current Injuries Any electrical contact should be immediately considered a candidate for potential neurological injury. Some physical symptoms of neurological damage can be delayed after electrical contact, employees should be monitored for the following abnormal symptoms. 11/10/
45 Tremors Weakness Numbness Delayed Symptoms Ongoing headaches Difficulties with speech Vision impairment or changes (double or triple vision) Problems with balance 11/10/

46 Chemical Burn Caused by Drain Cleaner 11/10/
47 Care and Treatment 11/10/
48 10% RULE 11/10/
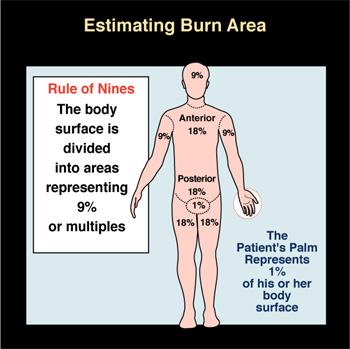
49 Initial Assessment Primary and secondary survey Distinguish between partial and full thickness burns Apply the rule of nines 11/10/
50 Primary Survey A- Airway B- Breathing C- Circulation D- Disability E- Exposure 11/10/
51 Airway Assess and reassess frequently the need for ET intubation 11/10/
52 Airway Management 3 types of inhalation injury 1. Carbon monoxide poisoning 2. Inhalation above the glottis 3. Inhalation below the glottis 11/10/
53 Carbon Monoxide Poisoning Most fatalities are due to CO poisoning Signs and symptoms May have cherry red skin only present in 50% of cases O2 sats are normal Cyanosis and tachypnea not usually present Need to determine CO levels in blood for accurate diagnosis 11/10/
54 BEST TREATMENT FOR CO POISONING IS OXYGEN 11/10/
55 Inhalation Above the Glottis Most heat damage occurs above true vocal cords Results in severe edema that may occlude airway Early intubation preferred 11/10/

56 Flame Face Burn 11/10/

57 5 Hours Later 11/10/
58 Injury Below the Glottis Almost always chemical Chemicals adhere to smoke particles and cause direct damage to epithelium of large airways 11/10/
59 Injury Below the Glottis Severity and extent of damage are unpredictable based on history and physical exam Need to continue to reassess on a regular basis 11/10/
60 Initial Management of Inhalation Injury Give 100% O2 at 15L by nonrebreather mask Intubate if indicated by: Progressive hoarseness and stridor Decreased LOC so that airway protective reflexes are impaired 11/10/
61 Other Physical Findings Carbonaceous sputum Facial burns Singed nasal hairs Agitation due to hypoxia Intercostal retractions Hoarseness, stridor Inability to swallow 11/10/
62 Intubation Have most experienced person intubate Secure tube with umbilical tape Regular tape will not stick to burned skin Emergency Cricothyroidotomy is rare 11/10/
63 IF YOU DO NOT HAVE A DEFINITIVE AIRWAY THERE IS NOT A LOT YOU WILL BE ABLE TO DO. EDEMA WILL CONTINUE FOR UP TO 48 HOURS. 11/10/
64 Inhalation in Pediatrics Upper airways small Obstruction occurs rapidly Use careful tube selection size Position properly Secure well to prevent dislodgement 11/10/

65 11/10/
66 Breathing Listen to breath sounds Apply high flow O2 15 L at 100%- non rebreather mask Monitor chest wall in the presence of deep torso burns 11/10/
67 November 10,
68 Circulation Establish IV access 2 sites if possible, through burned skin is OK Monitor blood pressure Assess and monitor frequently circumferentially burned extremities 11/10/
69 Disability Burn injuries should be alert and oriented IF not consider: Associated injuries CO poisoning Substance abuse Hypoxia Pre-existing medical conditions 11/10/
70 Exposure Remove all clothing and jewelry Maintain body temp, keep patient covered 11/10/
71 ONE OF THE BEST THINGS YOU CAN DO IS KEEP YOUR PATIENT WARM Raise Room Temperature Solar Blankets Clean blanket or sheet 11/10/
72 Secondary Survey Head to Toe to note other injuries Most important is circumstances of injury How did it occur? Inside/outside? Gasoline or other fuel involved? Explosion? Is it a scald, flame, electrical or chemical contact? 11/10/
73 Burn Wound Assessment Superficial Partial thickness Full thickness Fourth degree 11/10/
74 Superficial Burn Characteristics Intact skin Red appearance Painful Burn is through epidermis Usually heals in 5-10 days Example: sunburn 11/10/

75 11/10/
76 ORAL REHYDRATION AND OTC PAIN MEDICINES 11/10/
77 Partial Thickness Burn Burn through epidermis and dermis Skin is not necessarily intact Skin is loose Moist, red appearance Blistered Subcutaneous edema may be present 11/10/

78 11/10/
79 LESS THAN 10% - ORAL REHYDRATION AND OTC PAIN MEDS. ANTIBIOTIC CREAM, KEEP WOUND COVERED. 11/10/
80 Full Thickness Burn Burned through epidermis, dermis, and subcutaneous tissue Dry appearance May be red, white, black, or brown in color Leathery in appearance 11/10/

81 11/10/
82 LESS THAN 10% - ORAL REHYDRATION AND OTC PAIN MEDS. ANTIBIOTIC CREAM, KEEP WOUND COVERED. 11/10/
83 Fourth Degree Burn Burned through epidermis, dermis, subcutaneous tissue, muscle, and bone Charred appearance May appear cracked Immobility of area 11/10/

84 Car fire 11/10/
85 KEEP COVERED AND PROTECTED NEEDS AMPUTATION 11/10/
86 Assessment of Extent of Injury The rule of nines -. >Used for both adults and peds. The rule of palm. >The surface area of the patients hand is = to 1%of their total body surface area. 11/10/
87 11/10/
88 Infant- Modified Rule of Nines 10% 10 16% % Front 16% back 14 % 14% 11/10/
89 Fluid Resuscitation Proper fluid management is critical to survival Objectives are to: -Maintain tissue perfusion and organ function -And to avoid complications of inadequate or excessive fluid therapy 11/10/
90 Excessive Fluid Resuscitation Edema is usually at its max hours post burn Too much fluid will exaggerate edema formation Compromise local blood supply 11/10/
91 Excessive Fluids Patients sensitive to excess fluids are Elderly Children And pre-existing cardiac disease 11/10/
92 Inadequate Resuscitation Results in shock and acute renal failure May have multiple organ dysfunction 11/10/
93 Fluid Resuscitation Establish large bore IV sites 2 if possible Go through burned skin if necessary Interosseous route ok for children 11/10/
94 Fluid Resuscitation Use LR if possible In adults and older children: 2-4 ml x wt in kg x %TBSA In children: 3-4 ml x wt in kg x % TBSA Plus D5LR at a maintenance rate 11/10/
95 Fluid Infuse ½ of estimated volume in first 8 hours and rest over next 16 hours Remember that this is a starting point and must be adjusted to patients needs according to urinary output 11/10/
96 Hourly Urinary Output Adults: cc per hour Children less than 30 kg: 1cc/ kg/ hour 11/10/
97 Changes in Fluids If output is greater or less than recommended increase or decrease fluid by 1/3 11/10/
98 HYDRATION ENEMAS AND OTHER FUN WAYS TO GIVE FLUID! 11/10/
99 Circulation Management Check to see if burn is circumferential in nature -Monitor distal pulses -Escharotomy may be indicated for long transports 11/10/
100 Escharotomy Rarely indicated prior to transfer May be required to permit adequate ventilation in chest burns May be required to maintain tissue perfusion in extremity burns Please consult with burn center before performing escharotomy 11/10/
101 Signs and Symptoms Cyanosis of distal, unburned skin Unrelenting deep tissue pain Progressive numbness Progressive decrease or absence of pulses 11/10/
102 Escharotomy Can reduce chances of escharotomy by elevating area and encouraging ROM 11/10/

103 4 Hours Post Burn 11/10/
104 ESHCAROTOMIES CAN OFTEN WAIT UP TO 8 HOURS - ELEVATE THE AFFECTED AREAS - ENCOURAGE RANGE OF MOTION 11/10/
105 Other Factors to Consider Pre- existing conditions Medications, alcohol, drug use Allergies Tetanus history Last food or drink 11/10/
106 Review of Management Principles Stop the burning process Monitor vital signs frequently Insert Foley* Begin fluid resuscitation Assess extremity perfusion Monitor ventilation frequently Stay on top of pain management Emotional assessment of the patient 11/10/
107 Management of Major Burns Cont: Monitor for Urine Myoglobinuria Monitor Body Temperature Prevent unnecessary contamination of injury Pain Medication as appropriate IV is the only acceptable route 11/10/
108 ABA Transfer Criteria 2 nd degree burns > 10 % Burns to hands, face, feet, genitals, major joints 3 rd degree burns Electrical burns Chemical burns Inhalation injuries Burns with pre-existing medical condition Burns accompanied by trauma where the burn is the greater risk to life Burns to children in hospitals without pediatric services Patients with special social, emotional or rehabilitative needs 11/10/
109 Wound Care 11/10/

110 Prepare Supplies Ahead of Time Set everything up where you can reach it. Open gauze ahead of time. Pull your tape, have scissors ready. Ready a basin of warm soap and water (mild soap, like baby soap)
111 Clean the Wound Do not scrub hard, but try to remove soot, ashes and other dirt as much as possible. Do not worry if you cannot remove all the dirt, it will come off with additional dressing changes. If you are redressing a wound, completely wash away the old silvadene.
112 Keep Patient Warm Increase the room temperature prior to admitting patients or doing dressing changes. Burn patients can become hypothermic quickly when exposed. Dress one limb at a time, keeping the rest of the body covered with warm blankets.
113 If You Have Limited Supplies If you do not have Silvadene Use double antibiotic ointment Goal is to keep the wound moist If you have do not have antibiotic ointment Use petroleum jelly If you have do not have burn pad or gauze Smear on Silvadene or other topical, wrap the patient in a sheet.
114 Wrapping Hands 11/10/

115 Silvadene Smeared on Hand November 10,

116 Hold gauze with the bulk of the roll in the dominant hand, the first layer pulled from under the roll. This makes it easier to unroll and wrap the extremities. November 10,

117 To start: anchor once around wrist November 10,

118 Wrap fingers individually, loop back and forth across dorsum and palm, catching each finger as you go. November 10,

119 Come up across dorsum of hand, then go around and under, across the palm. November 10,
120 Wrapping Heads and Faces 11/10/
121 Make a Vest 11/10/
122 A SUPPLY LIST: Trauma Shears Tylenol Tape Rolls of Gauze Mineral oil Double antibiotic cream Petroleum jelly Blankets Solar blankets Water for washing wounds* Gentle soap Sheets, Pillow Cases Matches Scalpel *Water must be clean 11/10/
123 OTHER ITEMS YOU MAY BE ABLE TO USE: Pillows Tight t- shirts to hold dressings in place Do households around you have any pain medications? Children s dissolvable Tylenol Cotton blankets to assist in moving a patient Garbage bags Burn Gel* 11/10/
124 Summary Burns constitute a major cause of morbidity in traumatized patients. Principles of initial resuscitation include: >Aggressive Airway Management >Breathing >Circulation Management Burn Wound Assessment needs to be done in the secondary survey. 11/10/
125 Thank you!
Burn Priorities of Care: Triage/Treatment/Transfer. Via Christi Regional Burn Center Sarah Fischer, MSN, RN
 Burn Priorities of Care: Triage/Treatment/Transfer Via Christi Regional Burn Center Sarah Fischer, MSN, RN Disclosure I have nothing to disclose Objectives Identify American Burn Association referral criteria
Burn Priorities of Care: Triage/Treatment/Transfer Via Christi Regional Burn Center Sarah Fischer, MSN, RN Disclosure I have nothing to disclose Objectives Identify American Burn Association referral criteria
EmergencyKT: Management of Thermal Injury in Adult Patients
 EmergencyKT: Management of Thermal Injury in Adult Patients Remove patient from source of injury, including burned clothing and jewelry Does patient appear to have minor burns? (See Box A) No Notify Burn
EmergencyKT: Management of Thermal Injury in Adult Patients Remove patient from source of injury, including burned clothing and jewelry Does patient appear to have minor burns? (See Box A) No Notify Burn
Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator
 Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator Lecture Overview Burn statistics and etiologies Pre-hospital evaluation Anatomy of a burn
Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator Lecture Overview Burn statistics and etiologies Pre-hospital evaluation Anatomy of a burn
Burns. A Comprehensive Review Assessment & Management
 Burns A Comprehensive Review Assessment & Management 1 Objectives Understand types of Burns Understand the pathophysiology of the Burns Understand Rule of Nine Understand Classification of Burns Identify
Burns A Comprehensive Review Assessment & Management 1 Objectives Understand types of Burns Understand the pathophysiology of the Burns Understand Rule of Nine Understand Classification of Burns Identify
Objectives. Initial Burn Care and Fluid Resuscitation 6/5/2015 INITIAL MANAGEMENT
 Initial Burn Care and Fluid Resuscitation Sarah Taylor MSN, RN, ACNS-BC Clinical Nurse Specialist Trauma Burn Center University of Michigan Health System Ann Arbor, MI Objectives Discuss the initial assessment
Initial Burn Care and Fluid Resuscitation Sarah Taylor MSN, RN, ACNS-BC Clinical Nurse Specialist Trauma Burn Center University of Michigan Health System Ann Arbor, MI Objectives Discuss the initial assessment
BURNS MODULE. In the paediatric population consider non-accidental injury as a mechanism for burn injuries.
 BURNS MODULE INTRODUCTION Burns are a common cause of trauma. Most burn injuries are a result of flame burns, with scalds also occurring commonly. Electrical and chemical burns are less common. 1 Concurrent
BURNS MODULE INTRODUCTION Burns are a common cause of trauma. Most burn injuries are a result of flame burns, with scalds also occurring commonly. Electrical and chemical burns are less common. 1 Concurrent
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS. December 19, 2012
 PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
IMMEDIATE EMERGENCY BURN CARE » THERMAL BURNS » ELECTRICAL BURNS » CHEMICAL BURNS FIRST AID FOR THE THREE MAJOR CATEGORIES
 IMMEDIATE EMERGENCY BURN CARE 1. Treat according to BLS or ACLS Protocol 2. Use airway and C-Spine precautions. 3. Stop the burning process. FIRST AID FOR THE THREE MAJOR CATEGORIES» THERMAL BURNS + Stop
IMMEDIATE EMERGENCY BURN CARE 1. Treat according to BLS or ACLS Protocol 2. Use airway and C-Spine precautions. 3. Stop the burning process. FIRST AID FOR THE THREE MAJOR CATEGORIES» THERMAL BURNS + Stop
Approved By: Airway and Breathing A. Initially give humidified high flow oxygen at 15 L (100%) using a nonrebreather
 using a nonrebreather") Subject: BURN CARE CLINICAL GUIDELINE Originator: Approval Date: 2015 Approved By: Policy: All burn patients presenting to XXXXXX Hospital will have appropriate assessment, stabilization and evaluation
Subject: BURN CARE CLINICAL GUIDELINE Originator: Approval Date: 2015 Approved By: Policy: All burn patients presenting to XXXXXX Hospital will have appropriate assessment, stabilization and evaluation
BLS, ILS, ALS OTEP BURNS BURN INTRODUCTION TYPES OF BURNS
 BURNS BLS, ILS, ALS OTEP While we do understand this presentation is an instructional tool for all levels of certification, taking this into consideration everyone taking this class must remember that
BURNS BLS, ILS, ALS OTEP While we do understand this presentation is an instructional tool for all levels of certification, taking this into consideration everyone taking this class must remember that
EMERGENCYROOM BURN MANAGEMENT
 EMERGENCYROOM INITIAL ASSESSMENT PRIMARY SURVEY A = Airway and C-spine immobilization B = Breathing and Ventilation C = Circulation D = Disability, Neurologic Deficit E = Expose (remove all clothing and
EMERGENCYROOM INITIAL ASSESSMENT PRIMARY SURVEY A = Airway and C-spine immobilization B = Breathing and Ventilation C = Circulation D = Disability, Neurologic Deficit E = Expose (remove all clothing and
Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test
 Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test Purpose: To provide nurses with on overview of burn injuries in pediatric patients. Learning Objectives:
Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test Purpose: To provide nurses with on overview of burn injuries in pediatric patients. Learning Objectives:
Management of Acute Burn Injuries: The First 24 Hours
 Speaker Disclosure I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. I will not discuss off label uses of any pharmaceutical products or medical devices. Management of Acute
Speaker Disclosure I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. I will not discuss off label uses of any pharmaceutical products or medical devices. Management of Acute
At the conclusion of this course the learner will be able to
 Objectives At the conclusion of this course the learner will be able to 1. Discuss basic anatomy and pathophysiology of burns 2. Describe burn injuries in terms of size, depth, coloration and characteristics
Objectives At the conclusion of this course the learner will be able to 1. Discuss basic anatomy and pathophysiology of burns 2. Describe burn injuries in terms of size, depth, coloration and characteristics
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 46 Caring for Clients with Burns Types of Burns Thermal Dry heat flame Moist heat steam or hot liquid
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 46 Caring for Clients with Burns Types of Burns Thermal Dry heat flame Moist heat steam or hot liquid
The immediate management of burns patients should be similar to management of trauma.
 CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
Chapter 24 Soft Tissue Injuries Presentation Notes
 Names: Chapter 24 Soft Tissue Injuries Presentation Notes Anatomy of the Skin - Function of the Skin control Soft-Tissue Injuries injuries Soft-tissue damage the skin injuries Break in the of the skin
Names: Chapter 24 Soft Tissue Injuries Presentation Notes Anatomy of the Skin - Function of the Skin control Soft-Tissue Injuries injuries Soft-tissue damage the skin injuries Break in the of the skin
Mr Zachary Moaveni Plastic Surgeon, Middlemore Hospital. Mr Adam Bialostocki Plastic Surgeon, Tauranga
 Mr Zachary Moaveni Plastic Surgeon, Middlemore Hospital Mr Adam Bialostocki Plastic Surgeon, Tauranga Mr. Adam Bialostocki Plastic Surgeon Minor Burns First Aid Remove the burning agent / wet clothes
Mr Zachary Moaveni Plastic Surgeon, Middlemore Hospital Mr Adam Bialostocki Plastic Surgeon, Tauranga Mr. Adam Bialostocki Plastic Surgeon Minor Burns First Aid Remove the burning agent / wet clothes
Burns Management in the Emergency Department
 Management in the Emergency Department (Referral Proforma) Time/Date of injury (24hr) Patient demographic data sticker Airway Please remember to protect C-spine until clinically cleared as stable Administer
Management in the Emergency Department (Referral Proforma) Time/Date of injury (24hr) Patient demographic data sticker Airway Please remember to protect C-spine until clinically cleared as stable Administer
ELECTRICAL INJURY 9/21/2015 I HAVE NO DISCLOSURES WE HAVE OBTAINED APPROVAL FOR USE OF IDENTIFIABLE PATIENT PHOTOS
 ELECTRICAL INJURY SAMUEL P. MANDELL, MD, MPH ASSISTANT PROFESSOR OF SURGERY UNIVERSITY OF WASHINGTON SEPTEMBER 28, 2015 I HAVE NO DISCLOSURES WE HAVE OBTAINED APPROVAL FOR USE OF IDENTIFIABLE PATIENT PHOTOS
ELECTRICAL INJURY SAMUEL P. MANDELL, MD, MPH ASSISTANT PROFESSOR OF SURGERY UNIVERSITY OF WASHINGTON SEPTEMBER 28, 2015 I HAVE NO DISCLOSURES WE HAVE OBTAINED APPROVAL FOR USE OF IDENTIFIABLE PATIENT PHOTOS
Dóra Ujvárosy MD. Medical University of Debrecen Oxyology and Emergency Department
 Dóra Ujvárosy MD. Medical University of Debrecen Oxyology and Emergency Department Functions Definition A burn is a type of injury to the skin caused by heat, electricity, chemicals, light, radiation or
Dóra Ujvárosy MD. Medical University of Debrecen Oxyology and Emergency Department Functions Definition A burn is a type of injury to the skin caused by heat, electricity, chemicals, light, radiation or
Chapter 29. Objectives. Objectives 01/09/2013. Burns
 Chapter 29 Burns Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced in
Chapter 29 Burns Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced in
Burns and electrical injuries. Shelley Westwood, RN, BSN
 Burns and electrical injuries Shelley Westwood, RN, BSN Burns A burn is an injury caused by fire, heat, chemicals, radiation, or electricity. Burns are traumatic in that they can cause extreme pain, permanent
Burns and electrical injuries Shelley Westwood, RN, BSN Burns A burn is an injury caused by fire, heat, chemicals, radiation, or electricity. Burns are traumatic in that they can cause extreme pain, permanent
Burn injury. A : patent airway with smoking inhalation, stridor. D: E4V5M6,pupil 2mm RTLBE
 Burn injury Pinyong Uthaitas Emergency Department Faculty of Medicine, Ramathibodi Hospital A Thai man 52 year old came to the hospital due to flam burn ½ hr ago at his house. He gain conscious but hoarseness
Burn injury Pinyong Uthaitas Emergency Department Faculty of Medicine, Ramathibodi Hospital A Thai man 52 year old came to the hospital due to flam burn ½ hr ago at his house. He gain conscious but hoarseness
Disaster Medical Operations-Part 2
 Disaster Medical Operations-Part 2 Community Emergency Response Team Disaster Medical Operations Part 1 Review The killers Airway obstruction Excessive bleeding Shock All immediate receive airway control,
Disaster Medical Operations-Part 2 Community Emergency Response Team Disaster Medical Operations Part 1 Review The killers Airway obstruction Excessive bleeding Shock All immediate receive airway control,
Outpatient Burn Care for Primary Care: Who needs a referral?
 Outpatient Burn Care for Primary Care: Who needs a referral? J. Kevin Bailey, MD Associate Professor Department of Surgery Division of Trauma, Critical Care and Burn The Ohio State University Wexner Medical
Outpatient Burn Care for Primary Care: Who needs a referral? J. Kevin Bailey, MD Associate Professor Department of Surgery Division of Trauma, Critical Care and Burn The Ohio State University Wexner Medical
Acting in an Emergency (Video- Acting in an emergency and preventing disease transmission)
") CHAPTER 2 Acting in an Emergency (Video- Acting in an emergency and preventing disease transmission) Lesson Objectives 1. Explain how bloodborne pathogens may be transmitted from an infected person to
CHAPTER 2 Acting in an Emergency (Video- Acting in an emergency and preventing disease transmission) Lesson Objectives 1. Explain how bloodborne pathogens may be transmitted from an infected person to
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Update on Burn Care and Resuscitation
 Niknam Eshraghi, M.D., F.A.C.S General and Burn Surgery; The Oregon Clinic Director; Oregon Burn Center, Legacy Emanuel Medical Center Affiliate Professor of Surgery, Oregon Health Sciences University
Niknam Eshraghi, M.D., F.A.C.S General and Burn Surgery; The Oregon Clinic Director; Oregon Burn Center, Legacy Emanuel Medical Center Affiliate Professor of Surgery, Oregon Health Sciences University
Burns and Scalds. Treatment and Management. Accident and Emergency Department. Royal Surrey County Hospital. Patient information leaflet
 Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Burns and Scalds Treatment and Management Accident and Emergency Department A Burn is an injury caused to the skin by thermal
Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Burns and Scalds Treatment and Management Accident and Emergency Department A Burn is an injury caused to the skin by thermal
Current Trends in Burn Care
 Objectives Current Trends in Burn Care Jordan Murphy, BSN, CFRN Clinical Educator-KY/FL PHI Air Medical Describes normal skin anatomy. Differentiates pathophysiology related to etiology of injury. Identify
Objectives Current Trends in Burn Care Jordan Murphy, BSN, CFRN Clinical Educator-KY/FL PHI Air Medical Describes normal skin anatomy. Differentiates pathophysiology related to etiology of injury. Identify
Fire Deaths. Dr Julie McAdam Consultant Forensic Pathologist Glasgow University
 Fire Deaths Dr Julie McAdam Consultant Forensic Pathologist Glasgow University Forensic investigation multidisciplinary fire officers, police officers, scientists, photographers, pathologist, procurator
Fire Deaths Dr Julie McAdam Consultant Forensic Pathologist Glasgow University Forensic investigation multidisciplinary fire officers, police officers, scientists, photographers, pathologist, procurator
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Face and Throat Injuries. Chapter 26
 Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Burn Injuries & Its Management M JARI.MD
 Burn Injuries & Its Management M JARI.MD 1 BURNS Wounds caused by exposure to: 1. excessive heat 2. Chemicals 3. fire/steam 4. radiation 5. electricity 2 BURNS Results in 10-20 thousand deaths annually
Burn Injuries & Its Management M JARI.MD 1 BURNS Wounds caused by exposure to: 1. excessive heat 2. Chemicals 3. fire/steam 4. radiation 5. electricity 2 BURNS Results in 10-20 thousand deaths annually
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Airway and Ventilation. Emergency Medical Response
 Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Wisecracks 1. What are the indications for an escharotomy 2. What are the primary considerations in mechanical ventilation of burn patients
 Chapter 63 Thermal Burns Episode Overview Questions 1. List zones of burns 2. List 6 indications for intubation in the burn patient 3. List and describe 2 formulas for fluid resuscitation 4. Describe depth
Chapter 63 Thermal Burns Episode Overview Questions 1. List zones of burns 2. List 6 indications for intubation in the burn patient 3. List and describe 2 formulas for fluid resuscitation 4. Describe depth
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatrics Grand Rounds 1 June University of Texas Health Science Center at San Antonio. Management of Burn Wounds. Management of Burn Wounds
 Management of Burn Wounds Management of Burn Wounds History of Burn Care Pathophysiology of Burn Lillian F. Liao, MD, MPH Division of Trauma and Emergency Surgery Department of Surgery UTHSCSA Acute burn
Management of Burn Wounds Management of Burn Wounds History of Burn Care Pathophysiology of Burn Lillian F. Liao, MD, MPH Division of Trauma and Emergency Surgery Department of Surgery UTHSCSA Acute burn
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions
 83 Questions") Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Responsibility This guideline applies to teams of health professions caring for burn patients.
 Page 1 of 9 Guideline: Initial Assessment & Management of Burn Injuries Purpose This document provides a guideline for the initial assessment and management of burn patients. It is not intended as a full
Page 1 of 9 Guideline: Initial Assessment & Management of Burn Injuries Purpose This document provides a guideline for the initial assessment and management of burn patients. It is not intended as a full
Printed copies of this document may not be up to date, obtain the most recent version from Author Position
 Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle Author Position PICU/BURNS Consultant CATS Consultant Document Owner E. Polke
Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle Author Position PICU/BURNS Consultant CATS Consultant Document Owner E. Polke
Lesson 1: Types of ECG s
 Electrocardiography Lesson 1: Types of ECG s Objectives: Distinguish between a single-channel ECG machine and a multi-channel machine. Distinguish between a manual ECG machine and an automatic ECG machine.
Electrocardiography Lesson 1: Types of ECG s Objectives: Distinguish between a single-channel ECG machine and a multi-channel machine. Distinguish between a manual ECG machine and an automatic ECG machine.
Speaker Disclosure Emergent Burn Care I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose.
 Speaker Disclosure Emergent Burn Care I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. Debbie Harrell RN, MSN, Shriners Hospitals for Children Cincinnati Cincinnati, Ohio
Speaker Disclosure Emergent Burn Care I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. Debbie Harrell RN, MSN, Shriners Hospitals for Children Cincinnati Cincinnati, Ohio
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Advanced Paediatric Nursing. Burn Trauma. 26 April Wong Tze Wing NC (Burns), Burns Centre, Surgery, PWH
, Burns Centre, Surgery, PWH") Advanced Paediatric Nursing Burn Trauma 26 April 2016 Wong Tze Wing NC (Burns), Burns Centre, Surgery, PWH Objective: Understand burn trauma in children Understand Important nursing interventions in burn
Advanced Paediatric Nursing Burn Trauma 26 April 2016 Wong Tze Wing NC (Burns), Burns Centre, Surgery, PWH Objective: Understand burn trauma in children Understand Important nursing interventions in burn
Burn wounds - Determining the size and type degree
 1 Burn wounds - Determining the size and type degree Determining surface area of burn (Open hand only for small burns) 1 2 Burn depth Most burns are a combination of superficial and deeper burns and the
1 Burn wounds - Determining the size and type degree Determining surface area of burn (Open hand only for small burns) 1 2 Burn depth Most burns are a combination of superficial and deeper burns and the
Case Report: Burns Reid Sadoway PGY1 Emergency Medicine, Dalhousie
 Case Report: Burns Reid Sadoway PGY1 Emergency Medicine, Dalhousie History 3 yo boy, presents to pediatric ED with mother Child can be heard crying inside waiting/patient room, has both hands bandaged
Case Report: Burns Reid Sadoway PGY1 Emergency Medicine, Dalhousie History 3 yo boy, presents to pediatric ED with mother Child can be heard crying inside waiting/patient room, has both hands bandaged
Diabetic Emergencies. Chapter 15
 Diabetic Emergencies Chapter 15 Diabetes- is a disorder of glucose metabolism or difficulty metabolizing carbohydrates, fats and proteins Full name is diabetes mellitus which refers to the presence of
Diabetic Emergencies Chapter 15 Diabetes- is a disorder of glucose metabolism or difficulty metabolizing carbohydrates, fats and proteins Full name is diabetes mellitus which refers to the presence of
STS Care of Thermal Burns 20% Total Body Surface Area
 Temp Regulation Transfer Pain Fluids Airway Initial Assessment STS Care of Thermal Burns 20% Total Body Surface Area Remove burned clothing, rings, watches, and jewelry Cervical spine precautions (if history
Temp Regulation Transfer Pain Fluids Airway Initial Assessment STS Care of Thermal Burns 20% Total Body Surface Area Remove burned clothing, rings, watches, and jewelry Cervical spine precautions (if history
WOUNDS. Emergency Procedures in PT
 WOUNDS Emergency Procedures in PT Types of Wounds Abrasions uppermost layer scraped away, minor capillary bleeding occurs, nerve endings exposed Lacerations skin tear with edges jagged and uneven Incisions
WOUNDS Emergency Procedures in PT Types of Wounds Abrasions uppermost layer scraped away, minor capillary bleeding occurs, nerve endings exposed Lacerations skin tear with edges jagged and uneven Incisions
Thermal Burns PFN: SOMEML07. Terminal Learning Objective. References. Hours: 3.0 Instructor: Action: Communicate knowledge of thermal burns
 Thermal Burns PFN: SOMEML07 Hours: 3.0 Instructor: Slide 1 Terminal Learning Objective Action: Communicate knowledge of thermal burns Condition: Given a lecture in a classroom environment Standard: Received
Thermal Burns PFN: SOMEML07 Hours: 3.0 Instructor: Slide 1 Terminal Learning Objective Action: Communicate knowledge of thermal burns Condition: Given a lecture in a classroom environment Standard: Received
Aviation Rescue Swimmer Course
 Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition)
") 2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
UNIT 4: DISASTER MEDICAL OPERATIONS
 UNIT 4: DISASTER MEDICAL OPERATIONS PART 2 Patient Evaluation: How to perform a head-to-toe assessment to identify and treat injuries. Basic Treatment How to: Treat burns Dress and bandage wounds Treat
UNIT 4: DISASTER MEDICAL OPERATIONS PART 2 Patient Evaluation: How to perform a head-to-toe assessment to identify and treat injuries. Basic Treatment How to: Treat burns Dress and bandage wounds Treat
Printed copies of this document may not be up to date, obtain the most recent version from Author Position
 Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle, L Chigaru Author Position PICU/BURNS Consultant CATS Consultants Document
Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle, L Chigaru Author Position PICU/BURNS Consultant CATS Consultants Document
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES
 INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES 180801 1 Tactical Combat Casualty Care for Medical Personnel 1. August 2017 (Based on TCCC-MP Guidelines 180801 In this presentation, we
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES 180801 1 Tactical Combat Casualty Care for Medical Personnel 1. August 2017 (Based on TCCC-MP Guidelines 180801 In this presentation, we
MASSACHUSETTS DEPARTMENT OF PUBLIC HEALTH OFFICE OF EMERGENCY MEDICAL SERVICES Basic EMT Practical Examination Cardiac Arrest Management
 Basic EMT Practical Examination 6.0 - Cardiac Arrest Management Station 1 RESUSCITATION & DEFIBRILLATION No Point WHILE FUNCTIONING AS FIRST RESCUER: Point 1. Verbalizes or takes body substance isolation
Basic EMT Practical Examination 6.0 - Cardiac Arrest Management Station 1 RESUSCITATION & DEFIBRILLATION No Point WHILE FUNCTIONING AS FIRST RESCUER: Point 1. Verbalizes or takes body substance isolation
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Basic First Aid. Sue Fisher Emergency Management Coordinator CSUF University Police
 Basic First Aid Sue Fisher Emergency Management Coordinator CSUF University Police Information given for this lecture is not meant to replace any official training by the American Red Cross, or any other
Basic First Aid Sue Fisher Emergency Management Coordinator CSUF University Police Information given for this lecture is not meant to replace any official training by the American Red Cross, or any other
Skin Anatomy and Physiology
 Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Burns. There is also technically a fourth-degree burn. In this type, the damage of third-degree burns extends beyond the skin into tendons and bones.
 Burns can be caused by a variety of household items, including electrical equipment and chemicals. Very light burns can be treated at home and only cause superficial damage, while more severe burns need
Burns can be caused by a variety of household items, including electrical equipment and chemicals. Very light burns can be treated at home and only cause superficial damage, while more severe burns need
How do scientists design experiments? This activity will introduce you to the concept of variables.
 1.6 (page 1) Science Projects For ALL Students Variables How do scientists design experiments? This activity will introduce you to the concept of variables. Scientists test their ideas by conducting experiments.
1.6 (page 1) Science Projects For ALL Students Variables How do scientists design experiments? This activity will introduce you to the concept of variables. Scientists test their ideas by conducting experiments.
Patient Assessment. Chapter 8
 Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
5/2/2018. Notice. Putting Humpty Dumpty Back Together Again
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Competency Log Professional Responder Courses
 Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Chapter 23 Caring for Clients with Burns
 Chapter 23 Caring for Clients with Burns Burn Injuries 4500 people die from burns each year High risk group ~ children and the elderly The most common cause of burns Smoking material Scalding Lighting
Chapter 23 Caring for Clients with Burns Burn Injuries 4500 people die from burns each year High risk group ~ children and the elderly The most common cause of burns Smoking material Scalding Lighting
OUTLINE SHEET 5.4 PRIMARY SURVEY
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
NOTE If it is necessary to perform abdominal thrusts, expose the abdominal area prior to pressing on the abdomen.
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
Note: This CareKit does not replace expert medical care. Be Prepared
 Note: This CareKit does not replace expert medical care. Be Prepared EMS #: 9-1-1 Poison Control #: 800.222.1222 Take a first aid course. Learn CPR and first aid for choking. Before you give first aid,
Note: This CareKit does not replace expert medical care. Be Prepared EMS #: 9-1-1 Poison Control #: 800.222.1222 Take a first aid course. Learn CPR and first aid for choking. Before you give first aid,
IRECA BLS Challenge 2015 Scenario 1
 Scenario 1 Team Name Team Number Captain Name Judge 1 # Judge 2 # JUDGE S SHEET Overview: This scenario challenges the competitors to use basic triage techniques and then to do the most good for the most
Scenario 1 Team Name Team Number Captain Name Judge 1 # Judge 2 # JUDGE S SHEET Overview: This scenario challenges the competitors to use basic triage techniques and then to do the most good for the most
Smoke inhalation damages the body by simple asphyxiation (lack of oxygen), chemical irritation, chemical asphyxiation, or a combination of these.
, chemical irritation, chemical asphyxiation, or a combination of these.") Print Close 2011 WebMD, LLC. All rights reserved. Smoke Inhalation Recommend 13 Medical Author: Christopher P Holstege, MD Medical Editor: Melissa Conrad Stöppler, MD Smoke Inhalation Overview Smoke Inhalation
Print Close 2011 WebMD, LLC. All rights reserved. Smoke Inhalation Recommend 13 Medical Author: Christopher P Holstege, MD Medical Editor: Melissa Conrad Stöppler, MD Smoke Inhalation Overview Smoke Inhalation
Purpose To outline the pre-hospital and inter-hospital assessment and management of patients with major burns.
 Major Burns HELI.CLI.08 Purpose To outline the pre-hospital and inter-hospital assessment and management of patients with major burns. Procedure Management of Severe Burns For Review Aug 2015 1. Introduction
Major Burns HELI.CLI.08 Purpose To outline the pre-hospital and inter-hospital assessment and management of patients with major burns. Procedure Management of Severe Burns For Review Aug 2015 1. Introduction
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS
 CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
Patient Details Hospital number NHS number. Surname First name DOB. Permanent address. Post code. Mobile No. Temporary. Mother DOB. Father.
 Burns Unit Page 12 Paediatric Burn Injuries - Assessment & Admission Burns Unit Page 1 Discharge Patient Details Hospital number NHS number Admission date Injury date Hospital Use time time Time: Discharge
Burns Unit Page 12 Paediatric Burn Injuries - Assessment & Admission Burns Unit Page 1 Discharge Patient Details Hospital number NHS number Admission date Injury date Hospital Use time time Time: Discharge
Knowledge Objectives (2 of 2) Skills Objectives. Death Scene Considerations. Introduction 12/20/2013
 Skills Objectives. Death Scene Considerations. Introduction 12/20/2013") Fire and Explosion Deaths and Injuries Knowledge Objectives (1 of 2) Identify the effects of fire and explosion on the human body. Discuss the various issues involved in fire or explosion death investigation.
Fire and Explosion Deaths and Injuries Knowledge Objectives (1 of 2) Identify the effects of fire and explosion on the human body. Discuss the various issues involved in fire or explosion death investigation.
Doug Wildermuth Pulse Check Conference September 13, 2014
 www.e5supportservices.com Doug Wildermuth Pulse Check Conference September 13, 2014 How Safe Are We? May 23, 2009 29 Year old male Obviously distraught Appleton Police Department, WI http://www.youtube.com/watch?v=hfeepvo
www.e5supportservices.com Doug Wildermuth Pulse Check Conference September 13, 2014 How Safe Are We? May 23, 2009 29 Year old male Obviously distraught Appleton Police Department, WI http://www.youtube.com/watch?v=hfeepvo
CARE OF PATIENTS WITH BURNS. NUR 240 Donna Ricketts, MSN, RN, OCN
 CARE OF PATIENTS WITH BURNS NUR 240 Donna Ricketts, MSN, RN, OCN INCIDENCE/PREVALENCE OF BURN INJURY 5 th most common unintentional injury deaths 3 rd leading cause of fatal home injuries 4,000 burn deaths
CARE OF PATIENTS WITH BURNS NUR 240 Donna Ricketts, MSN, RN, OCN INCIDENCE/PREVALENCE OF BURN INJURY 5 th most common unintentional injury deaths 3 rd leading cause of fatal home injuries 4,000 burn deaths
Shock Video Shock (3)
") CHAPTER 9 Shock Video Shock (3) Lesson Objectives 1. Explain what happens inside the body with severe blood loss. 2. List common causes of shock. 3. Describe first aid steps for a victim in shock. 4. Describe
CHAPTER 9 Shock Video Shock (3) Lesson Objectives 1. Explain what happens inside the body with severe blood loss. 2. List common causes of shock. 3. Describe first aid steps for a victim in shock. 4. Describe
Chapter 21: Burns Introduction to Burn Injuries (1 of 2) Introduction to Burn Injuries (2 of 2) Reduction in Burn Injuries Pathophysiology of Burns
 Introduction to Burn Injuries (2 of 2) Reduction in Burn Injuries Pathophysiology of Burns") 1 2 3 4 5 6 7 8 Chapter 21: Burns Introduction to Burn Injuries (1 of 2) 1.25-2 million Americans treated for burns annually 50,000 require 3-5% considered life threatening leading cause of death for children
1 2 3 4 5 6 7 8 Chapter 21: Burns Introduction to Burn Injuries (1 of 2) 1.25-2 million Americans treated for burns annually 50,000 require 3-5% considered life threatening leading cause of death for children
STANDARD OPERATING PROCEDURE #203 LARGE ANIMAL SURGERY
 STANDARD OPERATING PROCEDURE #203 LARGE ANIMAL SURGERY 1. PURPOSE This Standard Operating Procedure (SOP) describes procedures for general surgery of large animal species such as swine, dogs, rabbits,
STANDARD OPERATING PROCEDURE #203 LARGE ANIMAL SURGERY 1. PURPOSE This Standard Operating Procedure (SOP) describes procedures for general surgery of large animal species such as swine, dogs, rabbits,
Pressure Ulcers Patient Information Leaflet
 Pressure Ulcers Patient Information Leaflet Shining a light on the future Introduction This leaflet is about pressure ulcers and includes information about what they are what can cause them and how they
Pressure Ulcers Patient Information Leaflet Shining a light on the future Introduction This leaflet is about pressure ulcers and includes information about what they are what can cause them and how they
Pressure Ulcers Patient Information Leaflet
 Further information about the content, reference sources or production of this leaflet can be obtained from the Patient Information Centre. Pressure Ulcers Patient Information Leaflet This information
Further information about the content, reference sources or production of this leaflet can be obtained from the Patient Information Centre. Pressure Ulcers Patient Information Leaflet This information
Going home after an AV Fistula or AV Graft
 Going home after an AV Fistula or AV Graft TGH Information for patients and families During your hospital stay, your surgeon created an: AV Fistula AV Graft Read this booklet to learn: how to care for
Going home after an AV Fistula or AV Graft TGH Information for patients and families During your hospital stay, your surgeon created an: AV Fistula AV Graft Read this booklet to learn: how to care for
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Module Summaries: The emergency plan is a crucial part of the total sports program.
 Module Summaries: Summary - The Emergency Plan The emergency plan is a crucial part of the total sports program. Prior to each season and game, those individuals responsible for the program and athletes
Module Summaries: Summary - The Emergency Plan The emergency plan is a crucial part of the total sports program. Prior to each season and game, those individuals responsible for the program and athletes
LRI Emergency Department. Burn injuries management in adults
 LRI Emergency Department Clinical guideline for: Burn injuries management in adults Authors: Approved by: Martin Wiese Reena Agarwal Claire Porter EF guidelines committee Approval date: 21 Sep 16 Approval
LRI Emergency Department Clinical guideline for: Burn injuries management in adults Authors: Approved by: Martin Wiese Reena Agarwal Claire Porter EF guidelines committee Approval date: 21 Sep 16 Approval
Disaster Medical Operations Part 2. CERT Basic Training Unit 4
 Disaster Medical Operations Part 2 Unit 4 Unit 3 Review 3 Killers Airway obstruction Excessive bleeding Shock 4-1 CERT Sizeup 1. Gather Facts 2. Assess Damage 3. Consider Probabilities 4. Assess Your Situation
Disaster Medical Operations Part 2 Unit 4 Unit 3 Review 3 Killers Airway obstruction Excessive bleeding Shock 4-1 CERT Sizeup 1. Gather Facts 2. Assess Damage 3. Consider Probabilities 4. Assess Your Situation
SEMINOLE COUNTY EMS PROVISIONAL EMT SKILLS VERIFICATION
 The following individual has completed the Seminole County EMS Provisional EMT Skills Verification check in the following areas: Oxygen, Airway and Ventilation Skills ALS Assistance Trauma Management Medical
The following individual has completed the Seminole County EMS Provisional EMT Skills Verification check in the following areas: Oxygen, Airway and Ventilation Skills ALS Assistance Trauma Management Medical
Review. A. abrasion B. contusion C. hematoma D. avulsion
 Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
PEPP Course: PEPP BLS Pretest
 PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
Cellular and Tissue Effects. Pathophysiology of the Burn Wound. Special Topics: Thermal Burns & Smoke Inhalation
 Special Topics: Thermal Burns & Smoke Inhalation MEDICAL RESPONDER AND RECEIVER SEMINAR; EXPLOSION AND BLAST INJURIES Pathophysiology of the Burn Wound The burn wound is the source of virtually all ill
Special Topics: Thermal Burns & Smoke Inhalation MEDICAL RESPONDER AND RECEIVER SEMINAR; EXPLOSION AND BLAST INJURIES Pathophysiology of the Burn Wound The burn wound is the source of virtually all ill
Electrocardiography for Healthcare Professionals
 Electrocardiography for Healthcare Professionals Kathryn A. Booth Thomas O Brien Chapter 4: Performing an ECG Learning Outcomes 4.1 Carry out preparation of the patient, room, and equipment for an ECG.
Electrocardiography for Healthcare Professionals Kathryn A. Booth Thomas O Brien Chapter 4: Performing an ECG Learning Outcomes 4.1 Carry out preparation of the patient, room, and equipment for an ECG.
Table of Contents. Dialysis Port Care Chemotherapy Port Care G-Tube Care Colostomy Bags Wound Dressings
 Table of Contents Dialysis Port Care Chemotherapy Port Care G-Tube Care Colostomy Bags Wound Dressings Dialysis Port Care Know What Type of Vascular Access You Have. Fistula: An artery in your forearm
Table of Contents Dialysis Port Care Chemotherapy Port Care G-Tube Care Colostomy Bags Wound Dressings Dialysis Port Care Know What Type of Vascular Access You Have. Fistula: An artery in your forearm
Chapter 11 - The Primary Assessment
 Introduction to Emergency Medical Care 1 OBJECTIVES 11.1 Define key terms introduced in this chapter. Slides 11 12, 14, 19 21, 28 11.2 Explain the purpose of the primary assessment. Slides 11 13 OBJECTIVES
Introduction to Emergency Medical Care 1 OBJECTIVES 11.1 Define key terms introduced in this chapter. Slides 11 12, 14, 19 21, 28 11.2 Explain the purpose of the primary assessment. Slides 11 13 OBJECTIVES