Sickle Cell Disease Overview/Transfusion Support Wednesday, August 29, :00 p.m. 3:30 p.m. (ET) / 6:00p.m.-7:30 p.m. (GMT)
|
|
|
- Abigayle Tate
- 6 years ago
- Views:
Transcription
 / 6:00p.m.-7:30 p.m. (GMT) When this file is opened, Acrobat Reader will, by default, display the slides including the Acrobat reader controls.")
1 Sickle Cell Disease Overview/Transfusion Support Wednesday, August 29, :00 p.m. 3:30 p.m. (ET) / 6:00p.m.-7:30 p.m. (GMT) When this file is opened, Acrobat Reader will, by default, display the slides including the Acrobat reader controls. To return to full screen mode, hit Ctrl-L on your computer keyboard or use your mouse to click View>Full Screen on the menu bar of the Acrobat Reader program. To take the slides out of full screen mode and display the Acrobat Reader controls, simply hit the Esc key on your computer keyboard. To advance slides during the program, use the Enter, Page Down, down arrow or right arrow on your computer keyboard. To back up slides during the program, use the Page Up, up arrow of left arrow on your computer keyboard. Please remember to logon to the Live Learning Center using your address and session number to complete an evaluation of the program and speakers. At this time, advance to the next slide and wait for the audioconference to begin. A 2012 Audioconference presented to you by AABB

2 Sickle Cell Disease: Overview and Transfusion Support AABB Audioconference August 29, 2012 Jeanne Hendrickson, MD
3 Objectives To define sickle cell disease and determine what population is affected To assess the indications for transfusion of sickle cell patients To review potential adverse outcomes of transfusion in sickle cell patients (eg RBC alloimmunization and delayed hemolytic transfusion reactions)
4 Objectives To define sickle cell disease and determine what population is affected To assess the indications for transfusion of sickle cell patients To review potential adverse outcomes of transfusion in sickle cell patients (eg RBC alloimmunization and delayed hemolytic transfusion reactions)
5 Sickle Cell Disease: 5000 Affected Babies Born Each Year in the U.S. Hb SS: 65% Hb SC: 25% Hb S β+ thalassemia: 8% Hb S β thalassemia: 2%
6 Sickle Cell Trait 8 10% of African Americans in the U.S. have sickle cell trait (Hb AS) 2.5 million people Sickle Dex or sickle prep is positive
7 Hemoglobin S Glutamine to Valine substitution in the 6 th codon of the Beta globin gene cluster on chromosome 11 Leads to polymerization (and sickling) when deoxygenated Membrane changes lead to increased adherence to the vascular endothelium
8
9
10 Newborn Screen **Hemoglobin presented in quantitative order** Hb FA = normal (80% F, 20% A) Hb FS = sickle cell disease Most likely to be Hb SS, but could be Hb S β thalassemia Hb FSA = sickle cell disease Hb S β+ thalassemia Hb FAS = sickle cell trait Hb FSC = SC disease Hb FA with Bart s = alpha thalassemia variant Hb F = beta thalassemia major
11 Sickle Cell Disease: Manifestations Head/ENT Chest Abdomen GU Skeletal Other
12 Objectives To define sickle cell disease and determine what population is affected To assess the indications for transfusion of sickle cell patients To review potential adverse outcomes of transfusion in sickle cell patients (eg RBC alloimmunization and delayed hemolytic transfusion reactions)
13 Risk/Benefit Ratio of RBC Transfusion in Sickle Cell Disease Benefit of increasing oxygen carrying capacity must be balanced by the risk of serious hazards of transfusion
14 in spite of the documented clinical data supporting transfusion therapy, the physiologic and rheologic aspects of this treatment approach are not fully understood Alexy et al, Transfusion 2006
15 Transfusion Options One time vs chronic Simple vs exchange
16 Potential Transfusion Indications To Be Further Discussed: Acute chest syndrome Splenic sequestration Priapism Pre operative transfusion CVA Others

17 Acute Chest Syndrome Defined as a new infiltrate in a patient with sickle cell disease May be accompanied by chest pain, fever, tachypnea, wheezing, or cough A leading cause of death
18 Acute Chest Syndrome Has Many Causes Vichinsky et al, NEJM 2000
19 Transfusion Improves Oxygenation 670 episodes of ACS 68% of patients received simple transfusion pao2 improved from 63 mm Hg to 71 mm Hg with transfusion O2 saturations increased from 91% to 94% with transfusion Similar increases with simple versus exchange transfusion Length of hospital stay decreased with transfusion Vichinsky et al, NEJM 2000
20 Is Simple or Exchange Transfusion Best for ACS? Not known No adequately powered, randomized trials have examined this question
21 Historic Data Suggests Dramatic Response to Exchange 32/35 patients with severe ACS responded dramatically to exchange transfusion Many patients initially received a simple transfusion without improvement Nathan et al, Blood 1993
22 No difference in outcome with simple versus exchange transfusion seen in a recent retrospective study Similar baseline characteristics between patient groups with a few exceptions: Higher admission Hb levels in exchange group Higher post transfusion Hb in exchange group 4 times more blood exposure in exchange group 10.3 versus 2.4 units Turner et al, Transfusion 2009
23 Turner et al, Transfusion 2009
24 Short Term Chronic Transfusion Therapy May Decrease ACS Incidence 27 patients with recurrent or unusually severe ACS were treated with chronic transfusion therapy Incidence of ACS decreased from 1.3 episodes/pt year to 0.1 episodes/pt year No obvious difference in severity of ACS in patients on chronic transfusion therapy Chronic lung damage may be minimized Hankins et al, JPHO 2005

25 Chronic Transfusion Arm of STOP with Less ACS Miller et al, J Pediatr 2001

26 Splenic Sequestration Collection of sickled RBCs in splenic sinusoids Often quite acute; minor episodes also occur Precipitating events unclear Peak age 6 months 2 years Occurs at an earlier age in children with low fetal Hb levels Tends to recur Historically a leading cause of death in infants with Hb SS disease
27 Splenic Sequestration Treatment Transfusion of small aliquots (5 cc/kg) of RBCs slowly is advocated for acute splenic sequestration Beware of autotransfusion Splenectomy is a potential treatment for patients with recurrent sequestration Often done after 2 years of age Chronic transfusion therapy may bridge gap until splenectomy can be done Limited efficacy data
28 Reverse Sequestration in a patient with sickle cell disease Lee et al, Postgrad Med J 1996

29 Priapism Results from vaso occlusion of venous penile drainage
30 Transfusion For Priapism Review of existing case reports (n=42) shows no decrease in time to detumescence with conventional therapy (8 days, n=16) versus transfusion therapy (10.8 days, n=26) Merritt et al, CJEM 2006
31 ASPEN (association of sickle cell disease, priapism, exchange transfusion, and neurologic events) Has been reported in a total of 9 patients May present immediately or within a week following transfusion Etiology unclear Hyperviscosity Release of activated clotting factors, activated platelets, and cytokines from sludge like blood in corpora cavernosa Sickle patients have increased vwf and fibrinogen at baseline, with decreased protein S
32 ASPEN May Occur in Cases with High Post Exchange Hb Levels Rackoff et al, J Peds 1992
33 Pre Operative Transfusion High rates of post operative complications have been reported in patients with sickle cell disease Including VOC, ACS, other Does pre op transfusion decrease this risk? How low does the %S have to be?
34 Pre Operative Transfusion: NIH Guidelines Recommend preoperative simple transfusions to maintain (and not to exceed) a Hgb of 10 g/dl
35 Pre Operative Transfusion Preoperative Transfusion in Sickle Cell Disease Study: 551 patients with Hgb SS disease Randomized to 2 transfusion arms: Aggressive (Hb of 10 g/dl and Hb S <30%) Conservative (Hb of 10 g/dl regardless of percent S)
36 Similar Non transfusion Complication Rates in Each Arm Vichinsky et al, NEJM 1995
37 50% Fewer Transfusion Related Complications in Conservative Arm Vichinsky et al, NEJM 1995
38 Randomized Trial in Cholecystectomy Patients Haberkern et al, Blood 1997
39 May Consider RBC Exchange Prior to High Risk Surgeries: Abdominal procedures Orthopedic procedures Cardiac surgery Retinal surgery

40 CVA At least 10% of patients with HbSS disease will have a clinical stroke by 20 yo A higher percentage will have a silent stroke
41 Most CVAs <20 yo and >30 yo are Ischemic Ohene-Frempong et al, Blood 1998
 DeBaun MR et al, Blood")
42 Silent Cerebral Infarcts Have a High Prevalence (yet are not obviously associated with abnormal TCDs) DeBaun MR et al, Blood 2012
 DeBaun et al, Blood 2012")
43 Wechsler FSIQ Scores are Significantly Lower in Patients with Infarcts (Silent or Overt) DeBaun et al, Blood 2012

44 Treatment of Acute Ischemic Events Case reports of exchange transfusion reversing TIAs Russell et al, JAMA 1979
45 Prevention of Stroke Stroke Prevention Trial in Sickle Cell Anemia (STOP): Randomized at risk children with MCA velocity >200 cm/sec by TCD to standard therapy or chronic transfusion therapy (keeping %S <30) Adams et al, NEJM 1998
46 Chronic Transfusion Therapy Decreased Risk of CVA by 92% Adams et al, NEJM 1998
47 STOP 2: Randomized patients from STOP 1 and others with a history of CVA or abnormal TCD who had been on transfusion therapy for 30 months to discontinue chronic transfusion therapy Adams et al, NEJM 2005

48 Events included abnormal TCDs or CVAs Adams et al, NEJM 2005
49 Chronic Transfusion Therapy How low should we go? Does percent S have to be <30% to be beneficial?
50 SWiTCH Trial Stroke with transfusion changing to hydroxyurea TWiTCH Trial TCD with transfusions changing to hydroxyurea SIT Trial Silent cerebral infarct multicenter transfusion trial
51 SWiTCH: Hydroxyurea Arm (solid line) with 7 CVAs (6 ischemic, 1 hemorrhagic); Transfusion arm (dashed line) with 0 CVAs Ware et al, Blood 2012
52 SWiTCH: Hydroxyurea Arm (solid line) with 9 TIAs; Transfusion Arm (dashed line) with 6 TIAs Ware et al, Blood 2012
53 Progressive Cerebral Infarcts Continue to Occur in a Majority of Patients (18/40) Despite Chronic Transfusion Therapy Hulbert et al, Blood 2011

54 NEJM, 2004
55 Gladwin et al, NEJM 2004
56 Transfusion to Reverse Pulmonary HTN? Trials are ongoing
57 Other Potential (some controversial) Indications for RBC Transfusion Aplastic crises Pregnancy Hepatic sequestration Pain crises Leg ulcers Growth failure
58 Objectives To define sickle cell disease and determine what population is affected To assess the indications for transfusion of sickle cell patients To review potential adverse outcomes of transfusion in sickle cell patients (eg RBC alloimmunization and delayed hemolytic transfusion reactions)
59 Adverse Effects of RBC Transfusion Hyperviscosity RBC Alloimmunization Autoimmunization Iron overload HLA alloimmunization Other serious hazards of transfusion Transfusion reactions Infectious disease transmission
60 RBC Alloimmunization: 1) Increases the risk of immediate as well as delayed hemolytic transfusion reactions #2 cause of transfusion related death reported to the FDA in ) May increase the risk of RBC autoantibody formation 3) May lead to lengthy and costly blood product delays 4) Increases the risk of hemolytic disease of the newborn
61 RBC Alloimmunization Vichinsky et al: NEJM, 1990; 332: % alloimmunization rate in transfused patients with sickle cell disease (5% rate in control, non sickle patients) 17/32 made multiple alloantibodies 66% of alloantibodies were anti C, anti E, or anti K
62 Multiple Studies Show RBC Alloimmunization Rates Are Between 20 40% in Sickle Cell Patients Receiving Non Phenotypically Matched RBCs LaSalle-Williams M et al, Transfusion 2011
63 Average Frequencies of the Most Common Antibodies Made by Patients with Sickle Cell Disease Antibody Average Frequency (%) E 21 K 18 C 14 Le a 8 Fy a 7 Jk b 7 D 7 Le b 7 S 6 Fy b 5 M 4 e 2 c 2 Hillyer et al, Blood Banking and Transfusion Medicine
64 C/E/K Phenotypic Matching Decreases But Does Not Eliminate RBC Alloimmunization Risk LaSalle-Williams M et al, Transfusion 2011
65 C/E/K Phenotypic Matching Decreases But Does Not Eliminate RBC Alloimmunization Risk LaSalle-Williams M et al, Transfusion 2011
66 RBC Phenotypic Matching A 2005 CAP survey found that only 37% of laboratories performed a RBC phenotype on non alloimmunized patients with sickle cell disease Only 75% of these laboratories provided C/E/K phenotypically matched RBCs for such patients Osby M et al, Arch Path Lab Med 2005, and Afenyi-Annan A et al, Immunohematology 2006
67 RBC Genotyping Increasingly being utilized at a number of institutions that care for large numbers of patients with sickle cell disease Longitudinal studies are ongoing to determine feasibility (from a donor and recipient perspective) and to determine the cost/benefit ratio compared to RBC phenotyping alone
68 Scenario 8 yo female with Hgb SS disease, transfused with 2 units crossmatch compatible, leukoreduced, phenotypically similar RBCs during an episode of acute chest syndrome
69 Scenario Returned 12 days later with abdominal pain, blood in urine, and severe anemia (Hgb 3.7) DAT positive Antibody screen remarkable for anti Fy a, anti Jk b, anti S
70 Delayed Hemolytic Transfusion Reaction 3 10 days after transfusion of blood that appears compatible Patients previously immunized Antibody not detected pre transfusion Anamnestic antibody response Intra and/ or extravascular hemolysis Can be severe (ARF, DIC) Rh and Kidd most common offenders
71 Anamnestic Response


72 New Alloantibodies May Not be Found Following DTHRs de Montalembert et al, Haematologica 2011
73 Win et al, Transfusion 2008
74 DHTR in SCD High rate of alloimmunization (18 36%) High rate of DHTR (4 22%) Severe, life threatening anemia Alloantibodies and autoantibodies Bystander hemolysis Hyperhemolysis Suppression of erythropoiesis

75 Scheunemann et al, Am J of Medical Sciences, 2010
76 Scenario 2 years later, patient transfused with 1 unit of crossmatch compatible, leukoreduced, phenotypically similar RBCs during another episode of acute chest syndrome
77 Scenario Re admitted 13 days later with abdominal pain and anemia (Hgb 4.9) DAT positive All panel cells reactive Repeat crossmatch with seg of unit transfused now grossly incompatible
78 Scenario Sample sent to local reference laboratory Antibody thought to be against high incidence antigen Not anti k, Kp b, Js b, Lu b Recommended genotyping and performing MMA
79 Scenario The patient developed joint pains, rashes, and a positive ANA months later Was initially diagnosed with autoimmune disorder, NOS Was later diagnosed with SLE ANA positive 1:2560 Anti DS DNA positive
80 HEA Beadchip Results
81 HEA Beadchip Results
82 Additional (D) Genotyping Results Rh(D) genotyping: R1 allele in trans to an African Black allele (RHCE*ce48C/ RHD*DAU0) This allele could produce a weak anti-rh antibody, potentially of anti-e or anti-f specificity R1R1 cells would be expected to be compatible

83 MMA Positive (33%,9%)

84 Garratty et al, Transfusion 2004

85 Additional Specialized Testing Revealed anti Tca Many thanks to Connie Westoff and the NYBC Immunohematology Reference Laboratory
86 How to prevent adverse transfusion related outcomes? Judicious use of RBCs Obtain accurate transfusion histories Centralize RBC alloimmunization data Provide leukoreduced RBCs Provide phenotypically similar RBCs NIH recommends obtaining a RBC phenotype at 6 months of age and providing antigen matched RBCs C,E,K Fy, Jk, S Consider the role that RBC genotyping may play
87 Summary Transfusion therapy remains critically important for patients with sickle cell disease More patients than ever before are on chronic transfusion therapy, primarily for CNS indications Transfusion alone cannot prevent all complications
88 Thank you
Hydroxyurea and Transfusion Therapy for the Treatment of Sickle Cell Disease
 Hydroxyurea and Transfusion Therapy for the Treatment of Sickle Cell Disease A Pocket Guide for the Clinician Susan E. Creary, MD, MSc 1 John J. Strouse, MD, PhD 2 1 The Ohio State University School of
Hydroxyurea and Transfusion Therapy for the Treatment of Sickle Cell Disease A Pocket Guide for the Clinician Susan E. Creary, MD, MSc 1 John J. Strouse, MD, PhD 2 1 The Ohio State University School of
--Session Current Issues in Blood Banking, Apheresis & Coagulation: A Primer for Speed Dating
 --Session 6001 -- Current Issues in Blood Banking, Apheresis & Coagulation: A Primer for Speed Dating Jeanne E. Hendrickson, MD Delores Mo, MD Kimberly W. Sanford, MD Christopher A. Tormey, MD September
--Session 6001 -- Current Issues in Blood Banking, Apheresis & Coagulation: A Primer for Speed Dating Jeanne E. Hendrickson, MD Delores Mo, MD Kimberly W. Sanford, MD Christopher A. Tormey, MD September
Transfusion Practices and Creation of a Registry for Patients with Sickle Cell Disease within the Atlanta Sickle Cell Consortium
 Transfusion Practices and Creation of a Registry for Patients with Sickle Cell Disease within the Atlanta Sickle Cell Consortium Annie Winkler MD Assistant Professor, Emory University Department of Pathology
Transfusion Practices and Creation of a Registry for Patients with Sickle Cell Disease within the Atlanta Sickle Cell Consortium Annie Winkler MD Assistant Professor, Emory University Department of Pathology
Rationale for RBC Transfusion in SCD
 Rationale for RBC Transfusion in SCD Dilution of HgbS-containing RBCs via the addition of HgbA-containing cells from the blood of normal donors Suppression of erythropoietin release caused by the rise
Rationale for RBC Transfusion in SCD Dilution of HgbS-containing RBCs via the addition of HgbA-containing cells from the blood of normal donors Suppression of erythropoietin release caused by the rise
Sickle Cell Disease. Edward Malters, MD
 Sickle Cell Disease Edward Malters, MD Introduction Vaso-occlusive phenomena and hemolysis are the clinical hallmarks of Sickle Cell Disease (SCD) Inherited disorder due to homozygosity for the abnormal
Sickle Cell Disease Edward Malters, MD Introduction Vaso-occlusive phenomena and hemolysis are the clinical hallmarks of Sickle Cell Disease (SCD) Inherited disorder due to homozygosity for the abnormal
Transfusions in Sickle Cell Disease: How, When and Why
 Transfusions in Sickle Cell Disease: How, When and Why James R. Eckman, MD Professor Emeritus of Hematology and Medical Oncology Emory University School of Medicine This work is supported by the Centers
Transfusions in Sickle Cell Disease: How, When and Why James R. Eckman, MD Professor Emeritus of Hematology and Medical Oncology Emory University School of Medicine This work is supported by the Centers
Anemia s. Troy Lund MSMS PhD MD
 Anemia s Troy Lund MSMS PhD MD lundx072@umn.edu Hemoglobinopathy/Anemia IOM take home points. 1. How do we identify the condtion? Smear, CBC Solubility Test (SCD) 2. How does it present clincally? 3. How
Anemia s Troy Lund MSMS PhD MD lundx072@umn.edu Hemoglobinopathy/Anemia IOM take home points. 1. How do we identify the condtion? Smear, CBC Solubility Test (SCD) 2. How does it present clincally? 3. How
Webinar: Association of Hgb A Clearance & RBC Antibodies
 Webinar: Association of Hgb A Clearance & RBC Antibodies Second Webinar Session A second session of this webinar will be hosted Wednesday, July 12 2:00 PM EST (1800 GMT) Register at the link below: https://attendee.gotowebinar.com/rt/9012031991808089089
Webinar: Association of Hgb A Clearance & RBC Antibodies Second Webinar Session A second session of this webinar will be hosted Wednesday, July 12 2:00 PM EST (1800 GMT) Register at the link below: https://attendee.gotowebinar.com/rt/9012031991808089089
ASFA 2015 Consensus Conference: RBC Exchange in Sickle Cell Disease
 ASFA 2015 Consensus Conference: RBC Exchange in Sickle Cell Disease Session 5B: SELECTION OF RED CELLS Araba Afenyi-Annan, MD, MPH Adjunct Assistant Professor Department of Pathology & Laboratory Medicine,
ASFA 2015 Consensus Conference: RBC Exchange in Sickle Cell Disease Session 5B: SELECTION OF RED CELLS Araba Afenyi-Annan, MD, MPH Adjunct Assistant Professor Department of Pathology & Laboratory Medicine,
Transfusion in Sickle Cell Disease What the guidelines [are likely to] say. Dr Bernard Davis Whittington Hospital, London
![Transfusion in Sickle Cell Disease What the guidelines [are likely to] say. Dr Bernard Davis Whittington Hospital, London](/thumbs/85/91702350.jpg "Transfusion in Sickle Cell Disease What the guidelines [are likely to] say. Dr Bernard Davis Whittington Hospital, London") Transfusion in Sickle Cell Disease What the guidelines [are likely to] say Dr Bernard Davis Whittington Hospital, London Background to BCSH Guideline Rationale Current guidance in disparate publications
Transfusion in Sickle Cell Disease What the guidelines [are likely to] say Dr Bernard Davis Whittington Hospital, London Background to BCSH Guideline Rationale Current guidance in disparate publications
SICKLE CELL DISEASE. Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH. Assistant Professor FACULTY OF MEDICINE -JAZAN
 SICKLE CELL DISEASE Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN Objective: The student should be able: To identify the presentation, diagnosis,
SICKLE CELL DISEASE Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN Objective: The student should be able: To identify the presentation, diagnosis,
Sickle cell disease. Fareed Omar 10 March 2018
 Sickle cell disease Fareed Omar 10 March 2018 Physiology Haemoglobin structure HbA2: 2α and 2δ chains (2-3%) HbF: 2α and 2γ chains (
Sickle cell disease Fareed Omar 10 March 2018 Physiology Haemoglobin structure HbA2: 2α and 2δ chains (2-3%) HbF: 2α and 2γ chains (
Pediatric Red Cell Exchange Indications, Benefits, Barriers. View from California Saturday May 9 th ASFA 2015
 Pediatric Red Cell Exchange Indications, Benefits, Barriers View from California Saturday May 9 th ASFA 2015 Red Cell Exchange: Not SCD Recommendations for Red Cell Exchange Indication Procedure Recommendation
Pediatric Red Cell Exchange Indications, Benefits, Barriers View from California Saturday May 9 th ASFA 2015 Red Cell Exchange: Not SCD Recommendations for Red Cell Exchange Indication Procedure Recommendation
Health Maintenance and Education for Children and Adults
 Health Maintenance and Education for Children and Adults Richard Ward, MSc, MRCP, FRCPath Director, Red Blood Cell Disorders Program, UHN Assistant Professor, Hematology, University of Toronto Chair, Canadian
Health Maintenance and Education for Children and Adults Richard Ward, MSc, MRCP, FRCPath Director, Red Blood Cell Disorders Program, UHN Assistant Professor, Hematology, University of Toronto Chair, Canadian
Hemoglobinopathies NORMAL HEMOGLOBINS
 Hemoglobinopathies Millicent Sutton MD October 28, 2005 NORMAL HEMOGLOBINS Consist of 2 alpha chains and 2 non alpha chains Hb A = α2β2 Hb F= α 2γ2 Hb A2 = α2δ2 1 Hemoglobin Variants Altered the conformational
Hemoglobinopathies Millicent Sutton MD October 28, 2005 NORMAL HEMOGLOBINS Consist of 2 alpha chains and 2 non alpha chains Hb A = α2β2 Hb F= α 2γ2 Hb A2 = α2δ2 1 Hemoglobin Variants Altered the conformational
Chapter 6: Blood Transfusion in the Management of Sickle Cell Disease
 Chapter 6: Blood Transfusion in the Management of Sickle Cell Disease Introduction Donor erythrocyte (red blood cell, RBC) transfusion was the first therapy used in SCD that targets the pathophysiology
Chapter 6: Blood Transfusion in the Management of Sickle Cell Disease Introduction Donor erythrocyte (red blood cell, RBC) transfusion was the first therapy used in SCD that targets the pathophysiology
Optimal RBC products for RBC exchange for patients with sickle cell disease
 Optimal RBC products for RBC exchange for patients with sickle cell disease Stella T. Chou, MD ASFA Annual Meeting Fort Lauderdale, FL May 6, 2016 I have no conflicts of interest to disclose Outline Apheresis
Optimal RBC products for RBC exchange for patients with sickle cell disease Stella T. Chou, MD ASFA Annual Meeting Fort Lauderdale, FL May 6, 2016 I have no conflicts of interest to disclose Outline Apheresis
ASH Draft Recommendations for SCD Related Transfusion Support
 ASH Draft Recommendations for SCD Related Transfusion Support INTRODUCTION American Society of Hematology (ASH) guidelines are based on a systematic review of available evidence. Through a structured process,
ASH Draft Recommendations for SCD Related Transfusion Support INTRODUCTION American Society of Hematology (ASH) guidelines are based on a systematic review of available evidence. Through a structured process,
CHOA and Grady SCD Policies
 29 CHOA and Grady SCD Policies Phenotype all SCD patients for major blood groups C/c, E/e, K, Fya/Fyb, Jka/Jkb, S/s For non-alloimmunized patients, prophylactically match for Rh (D, C/c, E/e) and K For
29 CHOA and Grady SCD Policies Phenotype all SCD patients for major blood groups C/c, E/e, K, Fya/Fyb, Jka/Jkb, S/s For non-alloimmunized patients, prophylactically match for Rh (D, C/c, E/e) and K For
Congenital Haemoglobinopathies
 Congenital Haemoglobinopathies L. DEDEKEN, MD H O P I T A L U N I V E R S I T A I R E D E S E N F A N T S R E I N E F A B I O L A U N I V E R S I T E L I B R E DE B R U X E L L E S Red Blood Cell Disorders
Congenital Haemoglobinopathies L. DEDEKEN, MD H O P I T A L U N I V E R S I T A I R E D E S E N F A N T S R E I N E F A B I O L A U N I V E R S I T E L I B R E DE B R U X E L L E S Red Blood Cell Disorders
PILOT STUDY OF ANTIGEN MATCHING FOR AUTOIMMUNE HEMOLYTIC ANEMIA
 PILOT STUDY OF ANTIGEN MATCHING FOR AUTOIMMUNE HEMOLYTIC ANEMIA Sharon Rice & Fred Plapp Saint Luke s Hospital Kansas City, MO CENTRALIZED TRANSFUSION SERVICE Antibody identification Antibody titer Antigen
PILOT STUDY OF ANTIGEN MATCHING FOR AUTOIMMUNE HEMOLYTIC ANEMIA Sharon Rice & Fred Plapp Saint Luke s Hospital Kansas City, MO CENTRALIZED TRANSFUSION SERVICE Antibody identification Antibody titer Antigen
Dependance on chronic transfusion
 Dependance on chronic transfusion Pr Saliou Diop Hematology Blood transfusion Dakar- Sénégal diop@cnts-dakar.sn Introduction Chronic transfusion: Regular use of blood transfusion in patients with chronic
Dependance on chronic transfusion Pr Saliou Diop Hematology Blood transfusion Dakar- Sénégal diop@cnts-dakar.sn Introduction Chronic transfusion: Regular use of blood transfusion in patients with chronic
How to Write a Life Care Plan for a Child with Hemoglobinopathy
 How to Write a Life Care Plan for a Child with Hemoglobinopathy Tamar Fleischer, BSN, MSN, CNLCP & Mona Yudkoff, RN, MPH, CRRN, CNLCP BalaCare Solutions March 2018 St. Peterburg, Florida What is Hemoglobinopathy?
How to Write a Life Care Plan for a Child with Hemoglobinopathy Tamar Fleischer, BSN, MSN, CNLCP & Mona Yudkoff, RN, MPH, CRRN, CNLCP BalaCare Solutions March 2018 St. Peterburg, Florida What is Hemoglobinopathy?
SICKLE CELL DISEASE TO TREAT OR
 SICKLE CELL DISEASE TO TREAT OR NOT TO TREAT COHEM Barcelona September 8, 2012 Sujit Sheth, M.D. Pediatric Hematology Oncology Disclosures None Outline Morbidity and mortality Definitive therapies Risk
SICKLE CELL DISEASE TO TREAT OR NOT TO TREAT COHEM Barcelona September 8, 2012 Sujit Sheth, M.D. Pediatric Hematology Oncology Disclosures None Outline Morbidity and mortality Definitive therapies Risk
Antibody identification. Antibody specificity
 Red blood cell (RBC) transfusions are frequently used in sickle-cell anaemia (SCA) patients to treat and prevent the complications of their disease. Acute simple transfusions are usually used to treat
Red blood cell (RBC) transfusions are frequently used in sickle-cell anaemia (SCA) patients to treat and prevent the complications of their disease. Acute simple transfusions are usually used to treat
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
A sickle in a pickle! by Julie Kirkegaard, MT(ASCP)SBB Community Blood Center, KC, MO and Elizabeth Jones, MT(ASCP)BB Saint Luke s Hospital, KC, MO
SBB Community Blood Center, KC, MO and Elizabeth Jones, MT(ASCP)BB Saint Luke s Hospital, KC, MO") A sickle in a pickle! by Julie Kirkegaard, MT(ASCP)SBB Community Blood Center, KC, MO and Elizabeth Jones, MT(ASCP)BB Saint Luke s Hospital, KC, MO A couple of definitions! Sickle Cell Disease- an autosomal
A sickle in a pickle! by Julie Kirkegaard, MT(ASCP)SBB Community Blood Center, KC, MO and Elizabeth Jones, MT(ASCP)BB Saint Luke s Hospital, KC, MO A couple of definitions! Sickle Cell Disease- an autosomal
1 Kattamis et al. Growth of Children with Thalassemia: Effect of Different Transfusion Regimens. Archives of
 Objectives Sickle Cell Anemia and Thalassemia: Transplantation Provide overview of hemoglobinopathies: Sickle cell disease and Thalassemia Discuss approaches to therapy Review recent registry collaboration
Objectives Sickle Cell Anemia and Thalassemia: Transplantation Provide overview of hemoglobinopathies: Sickle cell disease and Thalassemia Discuss approaches to therapy Review recent registry collaboration
Clinical decision making: Red blood cell alloantibodies
 Clinical decision making: Red blood cell alloantibodies Beth H. Shaz, MD Chief Medical Officer, VP New York Blood Center; Clinical Associate Professor Emory University School of Medicine 1 5 non-abo fatal
Clinical decision making: Red blood cell alloantibodies Beth H. Shaz, MD Chief Medical Officer, VP New York Blood Center; Clinical Associate Professor Emory University School of Medicine 1 5 non-abo fatal
Transfusion Medicine Potpourri. BUMC - Phoenix Internal Medicine Residents September 29, 2015
 Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Compassionate-use Voxelotor (GBT440) for up to 2 Years in Patients With Severe Sickle Cell Disease and Life-Threatening Comorbidities
 for up to 2 Years in Patients With Severe Sickle Cell Disease and Life-Threatening Comorbidities") Compassionate-use Voxelotor (GBT440) for up to 2 Years in Patients With Severe Sickle Cell Disease and Life-Threatening Comorbidities Gershwin Blyden, MD 1, Kenneth Bridges, MD 2, Lanetta Bronté, MD 1
Compassionate-use Voxelotor (GBT440) for up to 2 Years in Patients With Severe Sickle Cell Disease and Life-Threatening Comorbidities Gershwin Blyden, MD 1, Kenneth Bridges, MD 2, Lanetta Bronté, MD 1
It s a bird, It s a plane, No It s a. Presented by Julie Kirkegaard & Miche Swofford
 It s a bird, It s a plane, No It s a Presented by Julie Kirkegaard & Miche Swofford 55 year old woman admitted 11/23/2015 for colon cancer that metastasized to her liver History of 3 pregnancies Surgery
It s a bird, It s a plane, No It s a Presented by Julie Kirkegaard & Miche Swofford 55 year old woman admitted 11/23/2015 for colon cancer that metastasized to her liver History of 3 pregnancies Surgery
Putting some hematology into Pediatric Hematology/Oncology: a review of Hemophilia and Sickle Cell Disease in the Pediatric Patient
 Putting some hematology into Pediatric Hematology/Oncology: a review of Hemophilia and Sickle Cell Disease in the Pediatric Patient Kristina Haley, DO March 10, 2012 Jovita Reyes Memorial Pediatric Hematology/Oncology
Putting some hematology into Pediatric Hematology/Oncology: a review of Hemophilia and Sickle Cell Disease in the Pediatric Patient Kristina Haley, DO March 10, 2012 Jovita Reyes Memorial Pediatric Hematology/Oncology
Compassionate-use Experience With Voxelotor (GBT440) for Patients With Severe Sickle Cell Disease (SCD) and Life-Threatening Comorbidities
 for Patients With Severe Sickle Cell Disease (SCD) and Life-Threatening Comorbidities") Compassionate-use Experience With Voxelotor (GBT440) for Patients With Severe Sickle Cell Disease (SCD) and Life-Threatening Comorbidities Gershwin Blyden, MD 1, Kenneth R. Bridges, MD 2, Lanetta Bronté,
Compassionate-use Experience With Voxelotor (GBT440) for Patients With Severe Sickle Cell Disease (SCD) and Life-Threatening Comorbidities Gershwin Blyden, MD 1, Kenneth R. Bridges, MD 2, Lanetta Bronté,
Disclosure. Presented analysis part of larger study funded by Terumo BCT
 1 Comparison of Transfusion Adverse Events in Children with Sickle Cell Disease (SCD) Receiving or Automated Red Blood Cell Exchange (arbx) Transfusions for Stroke Prevention Shannon Kelly, M.D. 2 Disclosure
1 Comparison of Transfusion Adverse Events in Children with Sickle Cell Disease (SCD) Receiving or Automated Red Blood Cell Exchange (arbx) Transfusions for Stroke Prevention Shannon Kelly, M.D. 2 Disclosure
8/28/2018. Disclosures. Objectives. None. Automation to PreciseType and Everything in Between
 Automation to PreciseType and Everything in Between Jessie Singer MT(ASCP) Transfusion Medicine Children s Hospital Los Angeles None Disclosures Objectives Describe the application of molecular testing
Automation to PreciseType and Everything in Between Jessie Singer MT(ASCP) Transfusion Medicine Children s Hospital Los Angeles None Disclosures Objectives Describe the application of molecular testing
Automation to PreciseType and Everything in Between. Jessie Singer MT(ASCP) Transfusion Medicine Children s Hospital Los Angeles
 Transfusion Medicine Children s Hospital Los Angeles") Automation to PreciseType and Everything in Between Jessie Singer MT(ASCP) Transfusion Medicine Children s Hospital Los Angeles None Disclosures Objectives Describe the application of molecular testing
Automation to PreciseType and Everything in Between Jessie Singer MT(ASCP) Transfusion Medicine Children s Hospital Los Angeles None Disclosures Objectives Describe the application of molecular testing
Interleukin-1ß and Interleukin-6 Genetic Polymorphisms and Sickle Cell Disease: An Egyptian Study
 Interleukin-1ß and Interleukin-6 Genetic Polymorphisms and Sickle Cell Disease: An Egyptian Study MONA EL-GHAMRAWY, MD, PROFESSOR OF PEDIATRICS & PEDIATRIC HEMATOLOGY, CAIRO UNIVERSITY melghamrawy95@gmail.com
Interleukin-1ß and Interleukin-6 Genetic Polymorphisms and Sickle Cell Disease: An Egyptian Study MONA EL-GHAMRAWY, MD, PROFESSOR OF PEDIATRICS & PEDIATRIC HEMATOLOGY, CAIRO UNIVERSITY melghamrawy95@gmail.com
Sickle Cell Disease and impact on the society
 Sickle Cell Disease and impact on the society Professor Z.A.Jeremiah Ph.D, FRCPath (London) Professor of Haematology and Blood Transfusion Science Niger Delta University, Wilberforce Island Outline What
Sickle Cell Disease and impact on the society Professor Z.A.Jeremiah Ph.D, FRCPath (London) Professor of Haematology and Blood Transfusion Science Niger Delta University, Wilberforce Island Outline What
The Child with a Hematologic Alteration
 47 The Child with a Hematologic Alteration HELPFUL HINT Review the anatomy and physiology of the hematologic system in an anatomy and physiology textbook. MATCHING KEY TERMS Match the term with the correct
47 The Child with a Hematologic Alteration HELPFUL HINT Review the anatomy and physiology of the hematologic system in an anatomy and physiology textbook. MATCHING KEY TERMS Match the term with the correct
Bridging the Gap: Improving Sickle Cell Disease Transition from Pediatric- to Adult-Focused Care ASFA 2017 Annual Meeting
 Bridging the Gap: Improving Sickle Cell Disease Transition from Pediatric- to Adult-Focused Care ASFA 2017 Annual Meeting Kim Smith-Whitley, MD Director Comprehensive Sickle Cell Center The Children s
Bridging the Gap: Improving Sickle Cell Disease Transition from Pediatric- to Adult-Focused Care ASFA 2017 Annual Meeting Kim Smith-Whitley, MD Director Comprehensive Sickle Cell Center The Children s
Provision of Red Cell Transfusion Support for Transfusion Dependent Patients
 1.0 Definition Transfusion dependent patients are those who require frequent and long-term transfusion support to sustain life. Most such patients have been diagnosed with one of the following conditions:
1.0 Definition Transfusion dependent patients are those who require frequent and long-term transfusion support to sustain life. Most such patients have been diagnosed with one of the following conditions:
Hydroxurea: A Novel Approach to Optimizing the Health of Pediatric Patients with Sickle Cell Disease. Maa Ohui Quarmyne September 9 th, 2017
 Hydroxurea: A Novel Approach to Optimizing the Health of Pediatric Patients with Sickle Cell Disease Maa Ohui Quarmyne September 9 th, 2017 Outline Sickle Cell Disease Pathophysiology and Clinical Manifestations
Hydroxurea: A Novel Approach to Optimizing the Health of Pediatric Patients with Sickle Cell Disease Maa Ohui Quarmyne September 9 th, 2017 Outline Sickle Cell Disease Pathophysiology and Clinical Manifestations
It s not just allo-antibodies that a red cell transfusion can stimulate
 It s not just allo-antibodies that a red cell transfusion can stimulate Associate Professor Ralph Green Laboratory Medicine RMIT University Melbourne, Australia Transfusion practice Minimise risk of transmitting
It s not just allo-antibodies that a red cell transfusion can stimulate Associate Professor Ralph Green Laboratory Medicine RMIT University Melbourne, Australia Transfusion practice Minimise risk of transmitting
Blood transfusion as a management strategy for Haemoglobinopathy. Corrina McMahon Our Lady s Children s Hospital, Dublin, Ireland
 Blood transfusion as a management strategy for Haemoglobinopathy Corrina McMahon Our Lady s Children s Hospital, Dublin, Ireland Rationale for BT Sickle cell Disease Reduce the production of Hb Significant
Blood transfusion as a management strategy for Haemoglobinopathy Corrina McMahon Our Lady s Children s Hospital, Dublin, Ireland Rationale for BT Sickle cell Disease Reduce the production of Hb Significant
Medical and Surgical Complications of Sickle Cell Anemia
 Medical and Surgical Complications of Sickle Cell Anemia Ahmed Al-Salem Medical and Surgical Complications of Sickle Cell Anemia Ahmed Al-Salem Department of Surgery Dar A lalafia Medical Company Qatif
Medical and Surgical Complications of Sickle Cell Anemia Ahmed Al-Salem Medical and Surgical Complications of Sickle Cell Anemia Ahmed Al-Salem Department of Surgery Dar A lalafia Medical Company Qatif
World-Wide Distribution of Hemoglobin S. Geographic distribution of hemoglobin S in the world
 Sickle Cell Disease Gerald M. Woods, MD Professor of Pediatrics Division Director, Hematology/Oncology/BMT Director of Sickle Cell Program Children s Mercy Hospitals and Clinics Disclaimer Member of DSMB
Sickle Cell Disease Gerald M. Woods, MD Professor of Pediatrics Division Director, Hematology/Oncology/BMT Director of Sickle Cell Program Children s Mercy Hospitals and Clinics Disclaimer Member of DSMB
Immunohematology (Introduction)
") Modified from Serotonin version Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition Introduction to replace blood
Modified from Serotonin version Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition Introduction to replace blood
Hemolytic anemias (2 of 2)
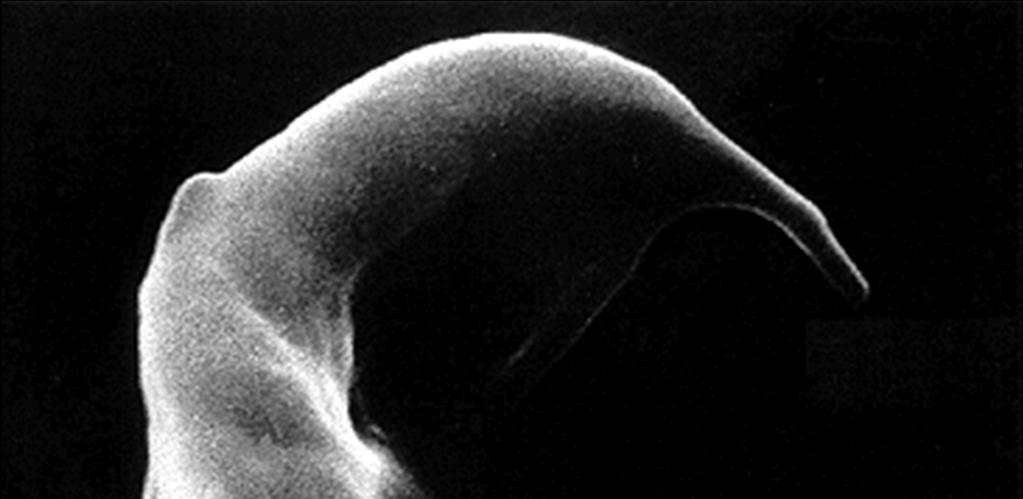
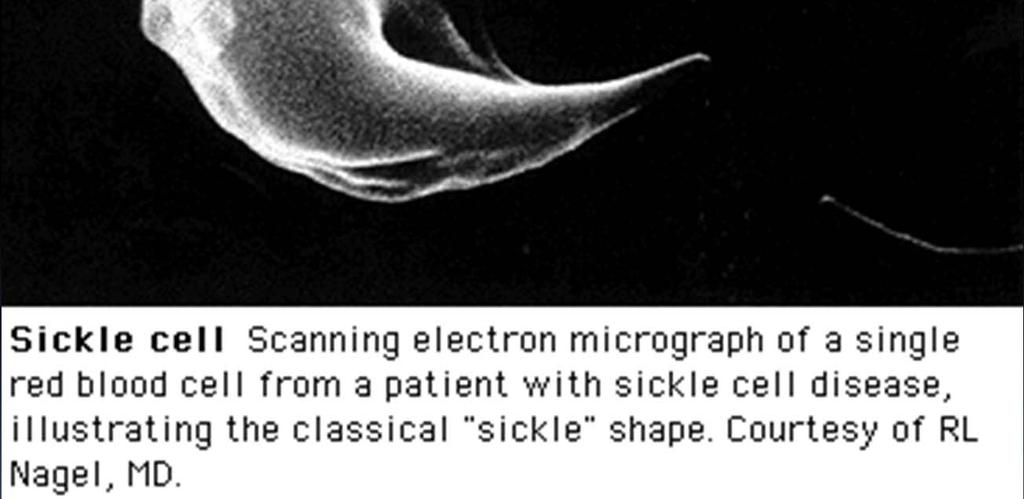
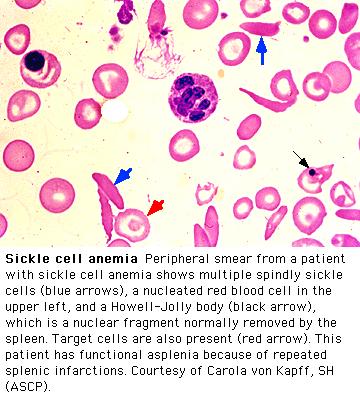
") Hemolytic anemias (2 of 2) Sickle Cell Anemia The most common familial hemolytic anemia in the world Sickle cell anemia is the prototypical (and most prevalent) hemoglobinopathy Mutation in the β-globin
Hemolytic anemias (2 of 2) Sickle Cell Anemia The most common familial hemolytic anemia in the world Sickle cell anemia is the prototypical (and most prevalent) hemoglobinopathy Mutation in the β-globin
Acute Complications of Sickle Cell Disease Case Study 5 year old girl with Hemoglobin SS, weakness and slurred speech
 Acute Complications of Sickle Cell Disease Case Study 5 year old girl with Hemoglobin SS, weakness and slurred speech Beatrice E. Gee, MD Medical Director, Sickle Cell and Hematology Program Children s
Acute Complications of Sickle Cell Disease Case Study 5 year old girl with Hemoglobin SS, weakness and slurred speech Beatrice E. Gee, MD Medical Director, Sickle Cell and Hematology Program Children s
Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition
 References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition") Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition Introduction to replace blood lost by hemorrhage or to correct
Immunohematology (Introduction) References: -Blood Groups and Red Cell Antigens (Laura Dean) -Cellular and molecular immunology, 8 th edition Introduction to replace blood lost by hemorrhage or to correct
Best practices for transfusion for patients with sickle cell disease
 Hematology Reviews 2009; volume 1:e22 Best practices for transfusion for patients with sickle cell disease Ted Wun, 1 Kathryn Hassell 2 1 UC Davis School of Medicine, Sacramento; 2 University of Colorado
Hematology Reviews 2009; volume 1:e22 Best practices for transfusion for patients with sickle cell disease Ted Wun, 1 Kathryn Hassell 2 1 UC Davis School of Medicine, Sacramento; 2 University of Colorado
Dr Banu Kaya Consultant Haematologist Barts Health NHS Trust Royal London Hospital, London, UK SICKLE CELL AND THALASSAEMIA OVERVIEW
 Dr Banu Kaya Consultant Haematologist Barts Health NHS Trust Royal London Hospital, London, UK SICKLE CELL AND THALASSAEMIA OVERVIEW Objectives Gain awareness of haemoglobinopathy inheritance, pathophysiology
Dr Banu Kaya Consultant Haematologist Barts Health NHS Trust Royal London Hospital, London, UK SICKLE CELL AND THALASSAEMIA OVERVIEW Objectives Gain awareness of haemoglobinopathy inheritance, pathophysiology
Hydroxyurea Treatment for Sickle Cell Disease
 Hydroxyurea Treatment for Sickle Cell Disease Before Hydroxyurea After Hydroxyurea Hydroxyurea Treatment for Sickle Cell Disease This document is not intended to take the place of the care and attention
Hydroxyurea Treatment for Sickle Cell Disease Before Hydroxyurea After Hydroxyurea Hydroxyurea Treatment for Sickle Cell Disease This document is not intended to take the place of the care and attention
Transfusion supply of chronically transfusion dependent patients: antigen-, rare blood type and ethnicity-related challenges
 Thierry PEYRARD PharmD, PhD, EurClinChem tpeyrard@ints.fr National Institute of Blood Transfusion - Paris French National Immunohematology Reference Laboratory Transfusion supply of chronically transfusion
Thierry PEYRARD PharmD, PhD, EurClinChem tpeyrard@ints.fr National Institute of Blood Transfusion - Paris French National Immunohematology Reference Laboratory Transfusion supply of chronically transfusion
Blood Transfusions in Children with Haemoglobinopathies
 Blood Transfusions in Children with Haemoglobinopathies Version: 2 Date: 22 nd April 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/ committees involved in
Blood Transfusions in Children with Haemoglobinopathies Version: 2 Date: 22 nd April 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/ committees involved in
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
CURRENT COURSE OFFERINGS
 The American Red Cross offers regular educational opportunities as a convenient way for healthcare providers to receive relevant blood banking and transfusion medicine information. The bi-monthly sessions,
The American Red Cross offers regular educational opportunities as a convenient way for healthcare providers to receive relevant blood banking and transfusion medicine information. The bi-monthly sessions,
TRANSFUSION PRACTICES IN THE MANAGEMENT OF SICKLE CELL DISEASE AMONG FLORIDA PHYSICIANS
 TRANSFUSION PRACTICES IN THE MANAGEMENT OF SICKLE CELL DISEASE AMONG FLORIDA PHYSICIANS By LEVETTE NICOLE DUNBAR A THESIS PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT
TRANSFUSION PRACTICES IN THE MANAGEMENT OF SICKLE CELL DISEASE AMONG FLORIDA PHYSICIANS By LEVETTE NICOLE DUNBAR A THESIS PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT
Immunohematology. Done by : Zaid Al-Ghnaneem
 Immunohematology Done by : Zaid Al-Ghnaneem Hello everyone, in this sheet we will talk mainly about immunohematology which is the reactions between our immune system with Antigens found mainly within blood
Immunohematology Done by : Zaid Al-Ghnaneem Hello everyone, in this sheet we will talk mainly about immunohematology which is the reactions between our immune system with Antigens found mainly within blood
Transfusion Reactions. Directed by M-azad March 2012
 Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
General Characterisctics
 Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
An Approach to the Patient Refractory to Platelets Transfusion. Harold Alvarez, MD
 Harold Alvarez, MD Objectives Explain the etiology of platelet refractoriness Discuss the different types of platelet refractoriness Describe how platelet refractoriness is diagnosed Discuss different
Harold Alvarez, MD Objectives Explain the etiology of platelet refractoriness Discuss the different types of platelet refractoriness Describe how platelet refractoriness is diagnosed Discuss different
Full Case: Questions: What is sickle cell crisis?
 Full Case: 30 y/o with avascular necrosis of her right hip was admitted for a total hip arthroplasty. Her hematocrit was 22%, blood pressure was 130/90 mm Hg, and pulse was 107 beats per minute. She had
Full Case: 30 y/o with avascular necrosis of her right hip was admitted for a total hip arthroplasty. Her hematocrit was 22%, blood pressure was 130/90 mm Hg, and pulse was 107 beats per minute. She had
2. RESPONSIBLE PARTIES:
 Retired Date: Page 1 of 6 1. POLICY: Exchange Transfusion for Sickle Cell 2. RESPONSIBLE PARTIES: Medical Management Administration, Utilization Management, Integrated Care Management, Claims Department,
Retired Date: Page 1 of 6 1. POLICY: Exchange Transfusion for Sickle Cell 2. RESPONSIBLE PARTIES: Medical Management Administration, Utilization Management, Integrated Care Management, Claims Department,
DONE BY : RaSHA RAKAN & Bushra Saleem
 DONE BY : RaSHA RAKAN & Bushra Saleem Hemolytic anemias (2 of 2) Sickle Cell Anemia The most common familial hemolytic anemia in the world Sickle cell anemia is the prototypical (and most prevalent) hemoglobinopathy
DONE BY : RaSHA RAKAN & Bushra Saleem Hemolytic anemias (2 of 2) Sickle Cell Anemia The most common familial hemolytic anemia in the world Sickle cell anemia is the prototypical (and most prevalent) hemoglobinopathy
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Atlantic Provinces Pediatric Hematology Oncology Network Réseau d Oncologie et Hématologie Pédiatrique des Provinces Atlantiques
 Atlantic Provinces Pediatric Hematology Oncology Network Réseau d Oncologie et Hématologie Pédiatrique des Provinces Atlantiques 5850/5980 University Avenue, PO Box 9700 Halifax, NS, B3K 6R8 1.902.470.7429
Atlantic Provinces Pediatric Hematology Oncology Network Réseau d Oncologie et Hématologie Pédiatrique des Provinces Atlantiques 5850/5980 University Avenue, PO Box 9700 Halifax, NS, B3K 6R8 1.902.470.7429
2. Transfusion Support in Thalassemia
 2. Transfusion Support in Thalassemia Principles To promptly identify the indications to start blood transfusion in thalassemia patients To understand the rate and frequency of transfusion in thalassemia
2. Transfusion Support in Thalassemia Principles To promptly identify the indications to start blood transfusion in thalassemia patients To understand the rate and frequency of transfusion in thalassemia
Fetal Anemia 02/13/13. Anjulika Chawla, M.D. Assistant Professor Division of Pediatric Hematology/Oncology
 Fetal Anemia 02/13/13 Anjulika Chawla, M.D. Assistant Professor Division of Pediatric Hematology/Oncology Objectives Definition of anemia Diagnosis of fetal anemia Normal developmental hematopoiesis Etiology
Fetal Anemia 02/13/13 Anjulika Chawla, M.D. Assistant Professor Division of Pediatric Hematology/Oncology Objectives Definition of anemia Diagnosis of fetal anemia Normal developmental hematopoiesis Etiology
Managing Emergencies
 Managing Emergencies Richard Ward, MSc, MRCP, FRCPath Director, Red Blood Cell Disorders Program, UHN Assistant Professor, Hematology, University of Toronto Chair, Canadian Hemoglobinopathy Association
Managing Emergencies Richard Ward, MSc, MRCP, FRCPath Director, Red Blood Cell Disorders Program, UHN Assistant Professor, Hematology, University of Toronto Chair, Canadian Hemoglobinopathy Association
The use of red cell genotyping in the management of sickle cell disease
 The use of red cell genotyping in the management of sickle cell disease Dr Sara Trompeter Consultant Haematologist UCLH and NHSBT Dr Keir Pickard Core Medical Trainee UCLH British Blood Transfusion Society
The use of red cell genotyping in the management of sickle cell disease Dr Sara Trompeter Consultant Haematologist UCLH and NHSBT Dr Keir Pickard Core Medical Trainee UCLH British Blood Transfusion Society
Original Research Article Ssafety and efficacy of prolonged hydroxycarbamide administration in adults with
 1 1 2 3 Original Research Article Ssafety and efficacy of prolonged hydroxycarbamide administration in adults with sickle cell disease in Northwestern Greece 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
1 1 2 3 Original Research Article Ssafety and efficacy of prolonged hydroxycarbamide administration in adults with sickle cell disease in Northwestern Greece 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Hemoglobinopathies Diagnosis and management
 Hemoglobinopathies Diagnosis and management Morgan L. McLemore, M.D. Hematology/Leukemia Department of Hematology and Oncology Winship Cancer Institute at Emory University mlmclem@emory.edu Disclosures
Hemoglobinopathies Diagnosis and management Morgan L. McLemore, M.D. Hematology/Leukemia Department of Hematology and Oncology Winship Cancer Institute at Emory University mlmclem@emory.edu Disclosures
Sickle Cell Disease 101. Objectives. What is SCD? 4/20/2016. Discuss the pathophysiology & genetics of Sickle Cell Disease (SCD).
.") Sickle Cell Disease 101 Jennifer Young, RN, MS, CPNP-AC Sickle Cell & Thalassemia Nurse Practitioner Nationwide Children s Hospital Objectives Discuss the pathophysiology & genetics of Sickle Cell Disease
Sickle Cell Disease 101 Jennifer Young, RN, MS, CPNP-AC Sickle Cell & Thalassemia Nurse Practitioner Nationwide Children s Hospital Objectives Discuss the pathophysiology & genetics of Sickle Cell Disease
Are We There Yet? Gene Therapy and BMT as Curative Therapies in Sickle Cell. Ann Haight, MD 9 Sept 2017
 Are We There Yet? Gene Therapy and BMT as Curative Therapies in Sickle Cell Ann Haight, MD 9 Sept 2017 Spoiler alert Yes (we have a cure) And No Work to do! 2 Sickle Cell Treatment Options Supportive Care
Are We There Yet? Gene Therapy and BMT as Curative Therapies in Sickle Cell Ann Haight, MD 9 Sept 2017 Spoiler alert Yes (we have a cure) And No Work to do! 2 Sickle Cell Treatment Options Supportive Care
Peri-Operative Management: Guidelines for Inpatient Management of Children with Sickle Cell Disease
 Version 02 Approved by Interprofessional Patient Care Committee: September 16, 2016 1.0 Background Children with Sickle Cell are at risk of developing post-operative Acute Chest Syndrome. With improvements
Version 02 Approved by Interprofessional Patient Care Committee: September 16, 2016 1.0 Background Children with Sickle Cell are at risk of developing post-operative Acute Chest Syndrome. With improvements
Making Hope A Reality December 10, Nasdaq : BLUE
 Making Hope A Reality December 10, 2014 Nasdaq : BLUE Forward Looking Statement These slides and the accompanying oral presentation contain forward-looking statements and information. The use of words
Making Hope A Reality December 10, 2014 Nasdaq : BLUE Forward Looking Statement These slides and the accompanying oral presentation contain forward-looking statements and information. The use of words
Red Cell Alloimmunisation in Sickle Cell Disease and Thalassemia. Aleksandar Mijovic Consultant Haematologist King s College Hospital/NHSBT Tooting
 Red Cell Alloimmunisation in Sickle Cell Disease and Thalassemia Aleksandar Mijovic Consultant Haematologist King s College Hospital/NHSBT Tooting BBTS Harrogate, 2014 Alloimmunisation to red cell antigens
Red Cell Alloimmunisation in Sickle Cell Disease and Thalassemia Aleksandar Mijovic Consultant Haematologist King s College Hospital/NHSBT Tooting BBTS Harrogate, 2014 Alloimmunisation to red cell antigens
Transfusion therapy for sickle cell disease: a balancing act
 MANAGEMENT OF SICKLE CELL DISEASE Transfusion therapy for sickle cell disease: a balancing act Stella T. Chou 1 1 Division of Hematology, The Children s Hospital of Philadelphia, Philadelphia, PA Transfusion
MANAGEMENT OF SICKLE CELL DISEASE Transfusion therapy for sickle cell disease: a balancing act Stella T. Chou 1 1 Division of Hematology, The Children s Hospital of Philadelphia, Philadelphia, PA Transfusion
Transfusion Support for Sickle Cell Disease
 Transfusion Support for Sickle Cell Disease Jacob Pendergrast, MD, FRCPC University Health Network Blood Transfusion Service Assistant Professor, University of Toronto DISCLOSURES } Research support from
Transfusion Support for Sickle Cell Disease Jacob Pendergrast, MD, FRCPC University Health Network Blood Transfusion Service Assistant Professor, University of Toronto DISCLOSURES } Research support from
SICKLE CELL AWARENESS. The Sickle Cell Society has produced the following information leaflets available at sicklecellsociety.org
 sickle cell disease in the UK Sickle cell disease (SCD) affects around 15,000 people in the UK People with Sickle Cell Disease have Sickle haemoglobin (HbS) which can make red blood cells rigid and sickle-shaped
sickle cell disease in the UK Sickle cell disease (SCD) affects around 15,000 people in the UK People with Sickle Cell Disease have Sickle haemoglobin (HbS) which can make red blood cells rigid and sickle-shaped
CURRENT RESEARCH STUDIES
 CURRENT RESEARCH STUDIES SCAGO SICKLE CELL RESEARCH DAY MAY 12, 2018 REBECCA LEROUX RN, BSCN, CCRP RED BLOOD CELL DISORDERS PROGRAM, UNIVERSITY HEALTH NETWORK MANUELA MERELLES-PULCINI RN, BSCN, MSN, CCRP
CURRENT RESEARCH STUDIES SCAGO SICKLE CELL RESEARCH DAY MAY 12, 2018 REBECCA LEROUX RN, BSCN, CCRP RED BLOOD CELL DISORDERS PROGRAM, UNIVERSITY HEALTH NETWORK MANUELA MERELLES-PULCINI RN, BSCN, MSN, CCRP
Transfusion Guidelines in AIHA; Indications, Compatibility Testing and Administration.
 Transfusion Guidelines in AIHA; Indications, Compatibility Testing and Administration. Lawrence D. Petz, M.D. Emeritus Professor University of California Los Angeles, California, U.S.A.; Medical Director
Transfusion Guidelines in AIHA; Indications, Compatibility Testing and Administration. Lawrence D. Petz, M.D. Emeritus Professor University of California Los Angeles, California, U.S.A.; Medical Director
QUICK REFERENCE Clinical Practice Guide on Red Blood Cell Transfusion
 QUICK REFERENCE 2012 Clinical Practice Guide on Red Blood Cell Transfusion Presented by the American Society of Hematology, adapted from Red Blood Cell Transfusion: A Clinical Practice Guideline from the
QUICK REFERENCE 2012 Clinical Practice Guide on Red Blood Cell Transfusion Presented by the American Society of Hematology, adapted from Red Blood Cell Transfusion: A Clinical Practice Guideline from the
High Hemoglobin F in a Saudi Child Presenting with Pancytopenia
 Case Report imedpub Journals http://www.imedpub.com Journal of Pediatric Care ISSN 2471-805X DOI: 10.21767/2471-805X.100002 High Hemoglobin F in a Saudi Child Presenting with Pancytopenia Abstract Saudi
Case Report imedpub Journals http://www.imedpub.com Journal of Pediatric Care ISSN 2471-805X DOI: 10.21767/2471-805X.100002 High Hemoglobin F in a Saudi Child Presenting with Pancytopenia Abstract Saudi
Antibody Information
 Antibody Information Rh Blood Group System Anti-D is an IgG antibody directed against the D antigen in the Rh blood group system. Anti-D is Newborn. Patients with Anti-D should receive D- blood (Rh negative).
Antibody Information Rh Blood Group System Anti-D is an IgG antibody directed against the D antigen in the Rh blood group system. Anti-D is Newborn. Patients with Anti-D should receive D- blood (Rh negative).
Blood Component Testing and Labeling
 Blood Component Testing and Labeling Each donor unite must be tested and properly labeled before its release for transfusion. Required Tests: In most blood banks, pretransfusion testing involves determining
Blood Component Testing and Labeling Each donor unite must be tested and properly labeled before its release for transfusion. Required Tests: In most blood banks, pretransfusion testing involves determining
Extra Notes 3. Warm. In the core (center) of the body, where the temperature is 37 C.
 of the body, where the temperature is 37 C.") Extra Notes 3 *The numbers of the slides are according to the last year slides. Slide 33 Autoimmune hemolytic anemia : Abnormal circulating antibodies that target normal antigen on the RBC and cause lysis.
Extra Notes 3 *The numbers of the slides are according to the last year slides. Slide 33 Autoimmune hemolytic anemia : Abnormal circulating antibodies that target normal antigen on the RBC and cause lysis.
HbSC disease is it different and how should we manage it? David Rees Department of Paediatric Haematology, King s College Hospital, London
 HbSC disease is it different and how should we manage it? David Rees Department of Paediatric Haematology, King s College Hospital, London Different types of sickle cell disesease Severe sickle cell disease
HbSC disease is it different and how should we manage it? David Rees Department of Paediatric Haematology, King s College Hospital, London Different types of sickle cell disesease Severe sickle cell disease
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Division of General Internal Medicine and Geriatrics Hospital Medicine 2014
 Division of General Internal Medicine and Geriatrics Hospital Medicine 2014 Objectives Understand workup of acute pain crisis Identify key aspects of management of acute pain crisis in sickle cell patients
Division of General Internal Medicine and Geriatrics Hospital Medicine 2014 Objectives Understand workup of acute pain crisis Identify key aspects of management of acute pain crisis in sickle cell patients
Chest diseases Hospital Laboratory Hematology Practice guidelines
 Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Historic and Current Complications in Children with Sickle Cell Disease
 Historic and Current Complications in Children with Sickle Cell Disease Trish McMahon Peterson RN, MSN, CPNP Thomas C. Hofstra MD Children's Hospital Los Angeles Comprehensive Sickle Cell Program Children's
Historic and Current Complications in Children with Sickle Cell Disease Trish McMahon Peterson RN, MSN, CPNP Thomas C. Hofstra MD Children's Hospital Los Angeles Comprehensive Sickle Cell Program Children's
Genetic Modifiers of Sickle Cell Disease Severity. Kunle Adekile, MD, PhD Professor Department of Pediatrics Kuwait University
 Genetic Modifiers of Sickle Cell Disease Severity Kunle Adekile, MD, PhD Professor Department of Pediatrics Kuwait University Outline Hb Molecule and Genetic control of globin synthesis Pathophysiology
Genetic Modifiers of Sickle Cell Disease Severity Kunle Adekile, MD, PhD Professor Department of Pediatrics Kuwait University Outline Hb Molecule and Genetic control of globin synthesis Pathophysiology
Management of Sickle Cell Disease
 Management of Sickle Cell Disease A.Ferster HUDERF-ULB 29 th BHS meeting Friday 31 January 2014 Introduction > 200.000 affected births each year 2000 births in US 15 births/y in Belgium 80.000 Pts in US
Management of Sickle Cell Disease A.Ferster HUDERF-ULB 29 th BHS meeting Friday 31 January 2014 Introduction > 200.000 affected births each year 2000 births in US 15 births/y in Belgium 80.000 Pts in US
Good afternoon and thank you for joining us today as we discuss hydroxyurea for the treatment of sickle cell disease. Dr. Emily Meier is a pediatric
 Good afternoon and thank you for joining us today as we discuss hydroxyurea for the treatment of sickle cell disease. Dr. Emily Meier is a pediatric hematologist at the Indiana Hemophilia & Thrombosis
Good afternoon and thank you for joining us today as we discuss hydroxyurea for the treatment of sickle cell disease. Dr. Emily Meier is a pediatric hematologist at the Indiana Hemophilia & Thrombosis
Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm
 Overall Algorithm") Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm Decision 1: Triage Decision 2: Analgesic Management Decision 3: Diagnostic
Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm Decision 1: Triage Decision 2: Analgesic Management Decision 3: Diagnostic