Irritable Bowel Syndrome
|
|
|
- Primrose Thompson
- 6 years ago
- Views:
Transcription

1 Irritable Bowel Syndrome
2 Functional gastrointestinal disorders Definition A variable combination of chronic or recurrent gastrointestinal symptoms (attributed to the pharynx, esophagus, stomach, biliary tree, small or large intestine, or anorectum) not explained by structural or biochemical abnormalities. Rome criteria, 1990

3 FGIDs including
4 The Rome III criteria divided Functional Gastrointestinal Disorders (FGIDs) into 8 dignostic classification adult (6 classification) children and adolescents(2 classification)
5 Rome III Functional Gastrointestinal Disorders (adult ) A. Functional esophageal disorders A1. Functional heartburn A2. Functional chest pain of presumed esophageal origin A3. Functional dysphagia A4. Globus B. Functional gastroduodenal disorders B1. Functional dyspepsia B1a. Postprandial distress syndrome B1b. Epigastric pain syndrome B2. Belching disorders B2a. Aerophagia B2b. Unspecified excessive belching B3. Nausea and vomiting disorders B3a. Chronic idiopathic nausea B3b. Functional vomiting B3c. Cyclic vomiting syndrome B4. Rumination syndrome in adults C. Functional bowel disorders C1. Irritable bowel syndrome C2. Functional bloating C3. Functional constipation C4. Functional diarrhea C5. Unspecified functional bowel disorder D. Functional abdominal pain syndrome E. Functional gallbladder and Sphincter of Oddi (SO) disorders E1. Functional gallbladder disorder E2. Functional biliary SO disorder E3. Functional pancreatic SO disorder F. Functional anorectal disorders F1. Functional fecal incontinence F2. Functional anorectal pain F3. Functional defecation disorders

6 Rome III Functional Gastrointestinal Disorders (children and adolescents) G. Functional disorders: neonates and toddlers G1. Infant regurgitation G2. Infant rumination syndrome G3. Cyclic vomiting syndrome G4. Infant colic G5. Functional diarrhea G6. Infant dyschezia G7. Functional constipation H. Functional disorders: children and adolescents H1. Vomiting and aerophagia H1a. Adolescent rumination syndrome H1b. Cyclic vomiting syndrome H1c. Aerophagia H2. Abdominal pain-related functional gastrointestinal disorders H2a. Functional dyspepsia H2b. Irritable bowel syndrome H2c. Abdominal migraine( 偏头痛 ) H2d. Childhood functional abdominal pain H2d1. Childhood functional abdominal pain syndrome H3. Constipation and incontinence


7 Definition Irritable Bowel Syndrome A functional GI disorder characterized - abdominal pain and/or discomfort - associated with altered bowel habits or disturbed defecation - relieve after defecation Not explained by structural or known biochemical abnormalities
8 IBS - Epidemiology 12-22% 15% 19% 14% 8-12% 9% 16% Drossman. DPS 1993;Sandler. GE 1984;Jones. MJ 1992;Thompson. DDS 2002
9 IBS - Epidemiology U.S. Prevalence % >60 age in years male female

10 IBS - Epidemiology Doctor Visits by Gender


11 IBS - Epidemiology Prevalence of Diagnosis Primary Care Practice Gastroenterology Practice

12 IBS - Epidemiology Work or School Absences Days per Year IBS Normal

13 IBS - Epidemiology Among the common diseases impact work because of sickness IBS is just in second only after Upper respiratory tract infection SECOND


14 IBS - Epidemiology Up to 10-20% of population Females > males Younger > older 2/3 do not seek health care 12% primary care practice, 28% GI practice >3x work loss, M.D. visits
15 Pathophysiological mechanisms Abnormal motility Visceral hypersensitivity Brain-gut interactions dysfuction Gut inflammation Psychosocial Factors
16 Pathophysiological mechanisms 1. Altered gut reactivity (motility, secretion) in response to luminal (e.g., meals, gut distention, inflammation, bacterial factors) provocative environmental stimuli, (e.g., psychosocial stress) resulting in symptoms of diarrhea and/or constipation 16

17 IBS - Abnormal motility Sigmoid Motility Index Minutes

18 IBS - Abnormal motility Normal Migrating Motor Complex (MMC) Phase I minutes Quiescence Phase II 60 minutes Irregular contractions Phase III 4-7 minutes Propagated contractions Interdigestive 90 minute cycle

19 IBS - Abnormal motility Prolonged Propagated Contractions (PPCs) More common in IBS Occur in ileum Peristaltic Correlate strongly with pain (IBS patients)

20 IBS - Abnormal motility Discrete Clustered Contractions (DCCs) Phase II of MMC More common in IBS Nonspecific - Obstruction - Pseudo-obstruction Correlates weakly with pain
21 Pathophysiological mechanisms 2. A hypersensitive gut with enhanced visceral perception and pain 21

22 IBS - Visceral hypersensitivity % Reporting Pain Rectosigmoid balloon inflation volume (ml)
23 Pathophysiological mechanisms 3. Dysregulation of the brain-gut axis possibly associated with greater stress-reactivity and altered perception and/or modulation of visceral afferent signals 23

24 IBS brain-gut interaction Brain-Gut Axis Afferent / efferent impulse
25 IBS - brain-gut interaction Enteric Nervous System Independently controls gut function Exhibits simple programmed functions (e.g., MMC, peristalsis) Intrinsic pacemaker controls rhythm Contains multiple neurotransmitters Actions modified by vagal and sympathetic extrinsic nerves
26 IBS - brain-gut interaction Sensitization of visceral afferent fibres Altered spinal modulation Abnormal sensory perception Central Processing Dysregulation of the brain-gut axis Spasm of GI smooth muscle abdominal pain 26
27 Pathophysiological mechanisms 4 Inflammation: gut inflammatory and immune factors persisting following infection or inflammation of the bowel 27
28 Role of psychosocial factors 1) Psychological stress exacerbates GI symptoms. 2) Psychological disturbances modify the experience of illness and illness behaviors such as health care seeking. 3) Psychosocial factors affect health status and clinical outcome. 28


29 Increased motor reactivity Altered visceral sensation CNS - ENS dysregulation inflammation Involves small and large intestine
 abdominal bloating Headaches/backache Poor appetite/weight loss Fatigue and Sleeplessness Anxiety or Depression These symptoms can")
30 Clinical manifestation Symptoms of Irritable Bowel Syndrome can include: abdominal pain/discomfort (often relieved by passing a bowel motion)(essential) Altered defecation (frequency features) Constipation diarrhea (sometimes one alternating with the other) abdominal bloating Headaches/backache Poor appetite/weight loss Fatigue and Sleeplessness Anxiety or Depression These symptoms can occur in any combination or individually

31 Diagnosis approach
32 Diagnosis Diagnostic Criteria* for Irritable Bowel Syndrome (The Rome III) Recurrent abdominal pain or discomfort** at least 3 days per month in the last 3 Months associated with 2 or more of the following: 1. Improvement with defecation 2. Onset associated with a change in frequency of stool 3. Onset associated with a change in form (appearance) of stool *Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis. **
33 IBS - Diagnosis Rome Criteria Symptoms >3 months Abdominal pain/discomfort - Relieved with defecation and/or - With change in stool frequency and/or - With change in stool consistency Two or more at least 1/4 of the time - in stool frequency - in form - Difficult passage - Mucous - Bloating
34 Bristol Stool Form Scale 1-7
35 IBS subtyping The Rome II Irritable bowel syndrome (IBS) diarrhea-predominant pattern constipation-predominant pattern diarrhea- constipation alterative pattern The Rome III Irritable bowel syndrome (IBS) IBS with constipation (IBS-C) IBS with diarrhea (IBS-D ) Mixed IBS (IBS-M) Unsubtyped IBS
36 IBS-Subtypes (Rome III Criteria) (IBS- Constipation) (IBS-Diarrhea) (IBS-Mixed) (IBS-Unsubtyped) unsubtyped Hard and lumpy stools 25%,and watery and loose stools<25% Watery and loose stools 25%,and hard and lumpy stools<25% Hard and lumpy stools 25%,also watery and loose stools 25% Hard and lumpy :Bristol 1~2;watery and loose: Bristol 6~7
37 Two-dimensional display of the 4 possible IBS subtypes according to bowel form at a particular in time (George F. Longstreth et al. Functional Bowel Disorders. Gastroenterology 2006;130: )
38 IBS-C 19%-44% IBS-D 15%-36% IBS-C IBS-D IBS-A/M IBS-A/M 19%-49% 75% patients alternated subtypes Simren et al, Scand J Gastroenterol 2001; 36:545 Tillisch et al, Am J Gastroenterol 2005; 100:896Mearin et al, Eur J Gastroenterol Heoatol 2003; 15:165 Drossman et al, Gastroenterology 2005; 128:580
39 IBS - Diagnosis Additional Specialized Studies Constipation Diarrhea Pain / Bloating Colonic transit Anal manometry and balloon expulsion Rectal sensation and emptying Defecography Stool osmolarity and electrolytes Laxative screen Small bowel / colonic transit Rectal sensation 75 SeHCAT test / Cholestyraminetrial Smal bowel series Antidepressanttrial CHO-H 2 breath test Small bowel manometry
40 IBS - Diagnosis Dietary Factors Lactose Caffeine Alcohol Fat Gas-producing foods Malabsorption Post-gastrectomy Intestinal Pancreatic Infection Giardia lamblia Bacterial Ameba Differential Diagnosis Miscellaneous Endometriosis Endocrine tumors (Carcinoid, VIP, etc.) AIDS Inflammatory Bowel Ulcerative colitis CD Microscopic colitis Mast-cell disease Pschychologic Anxiety/panic Depression Somatization

41 IBS - Diagnosis Historical Weight loss Onset in older patients Nocturnal awakening Family Hx CA / IBD Physical Abnormal exam Fever Positive occult stool Initial Labs Hgb WBC ESR Abnormal chemistry

42 Treatmemt 1.General treatment approach 2. Pharmacological therapies 3.Psychological therapies
43 General treatment approach 1. Establish therapeutic relationship 2. Education and reassurance 3. Dietary and lifestyle modifications
44 IBS general Treatment Approach Physician-Patient Relationship Reassure the patient that they are not unusual Identify why the patient is currently presenting Obtain a history of referral experiences Examine patient fears or agendas Ascertain patient expectations of physician Determine patient willingness to aid in treatment Uncover the symptom most impacting quality of life and the specific treatment designed to improve management of that symptom
45 IBS general Treatment Approach Education and reassurance Education about healthy life style behaviors, Patients should have regular, unhurried meals reassurance that the symptoms are not due to a life-threatening disease
46 IBS general Treatment Approach Dietary Modifications Eliminate offending items - Lactose - Sorbitol gum - Caffeine - Large meals - Fatty foods - Food sensitivity - Alcohol - Gas producing foods Increase fiber (consipation)
47 Pharmacological therapies drug therapy for IBS can be considered in two categories: 1. End organ treatment aimed at relieving abdominal pain (antispasmodic drugs) or disturbed bowel habit (antidiarrhoeal and bulking agents). 2. Central treatment (antidepressants) targeted at patients with associated affective disorder.


48 IBS pharmaceutical Treatment Pharmaceutical Agents Pain Diarrhea Constipation Antispasmodics Anticholinergics selective Ca++ antagonists Trimebutine Antidepressants (low dose initially) Loperamide Diphenoxylate Cholestyramine Fiber Osmotic laxatives Cisapride Misoprostil PEG solution
49 Antispasmodics Pharmacological therapies Anticholingergic drugs may provide temporary relief for symptoms such as painful cramps related to intestinal spasm Selective Ca++ antagonists (Pinaverium Bromide, Otilonium Bromide ) Smooth muscle relaxant papaverine peripherally acting opiate-based agonist (Trimebutine)
50 Antidiarrheal Pharmacological therapies Peripherally acting opiate-based agents Loperamide 2-4mg erery 4-6hours up to maximum of 12g/d, Diphenoxylate Cholestyramine bile acid binder
51 Pharmacological therapies Anti-constiption High fiber diets and bulking agents Water-holding action of fibers contribute to increase stool bulk, speed up colonic transit. improve in constipation. psyllium produced greater improvement in stool pattern and abdominal pain than bran, it tends to produce less bloating and distention Osmotic laxatives(e.g. lactulose)
52 Pharmacological therapies Serotonin Receptor Agonist and Antagonists Serotonin 3 receptor agonist for IBS-D alosetron reduces perception of painful visceral stimulation in IBS, also induce rectal relaxation, increases rectal compliance, and delay colonic transit, especially efficacious in women Serotonin 4 receptor antagonist for IBS-C Misoprostil Cisapride Tegaserod exhibit prokinetic activity by stimulating peristalsis, acceleate intestinal and ascending colonic transit in IBS-C
53 Psychological therapies Cognitive-behavioral treatment Antidepressants are recommended for moderate to severe symptoms - tricyclic antidepressant in IBS-D -selective serotonin reuptake inhibitor(ssri)- IBS-C Psychological treatments are initiated when symptoms are severe enough to impair health-related quality of life. -standard psychotherapy -hypnotherapy
54 Irritable bowel syndrome Definition:abdominal pain or discomfort and altered bowel habits without demonstrable organic disease. Pathophysiological mechanisms Clinical Features: 1. Diarrhea-predominant; 2. Constipation-predominant; 3. Mixed Diagnosis: Rome III Criteria Treatment: 1.General treatment approach; 2. Pharmacological therapies 3.Psychological therapies
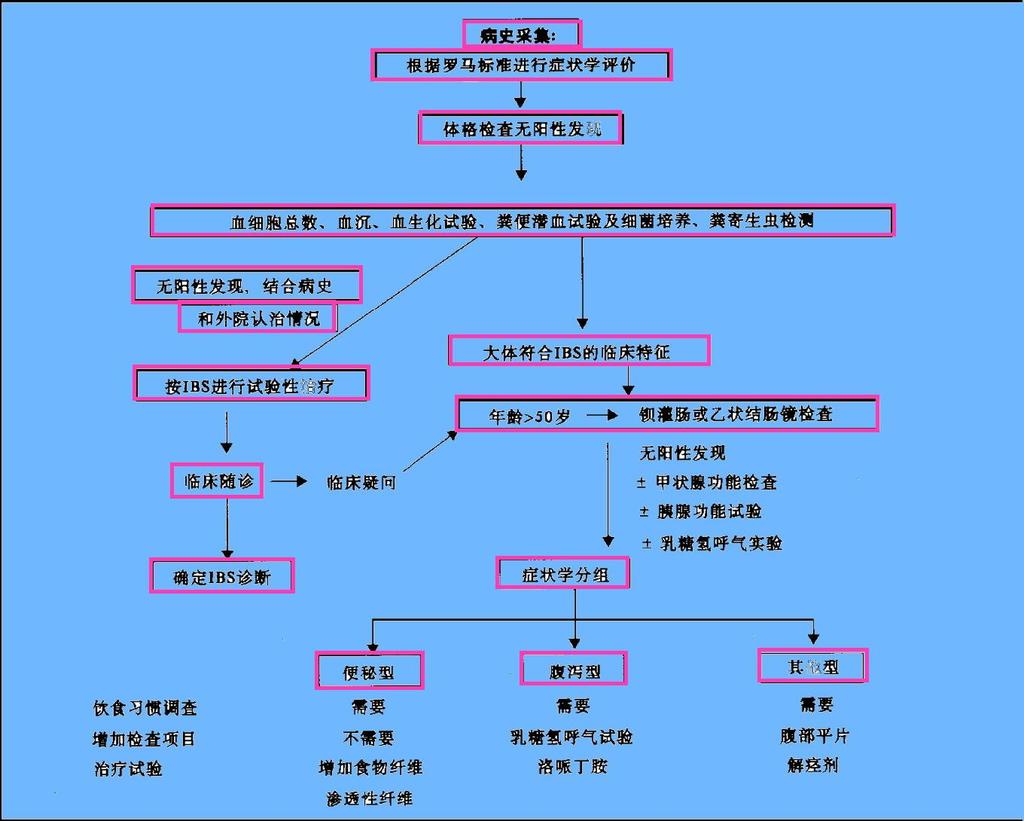

55 IBS 诊治流程
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University
 Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University") CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
IBS - Definition. Chronic functional disorder of GI generally characterized by:
 IBS - Definition Chronic functional disorder of GI generally characterized by: 3500 3000 No. of Publications 2500 2000 1500 1000 Irritable Bowel syndrome Irritable Bowel Syndrome 500 0 1968-1977 1978-1987
IBS - Definition Chronic functional disorder of GI generally characterized by: 3500 3000 No. of Publications 2500 2000 1500 1000 Irritable Bowel syndrome Irritable Bowel Syndrome 500 0 1968-1977 1978-1987
SUPPLEMENTARY INFORMATION Associated with
 Table1: Rome III and Rome IV diagnostic criteria for IBS, functional constipation and functional dyspepsia. Rome III diagnostic criteria 1,2 Rome IV diagnostic criteria 3,4 Diagnostic criteria for IBS
Table1: Rome III and Rome IV diagnostic criteria for IBS, functional constipation and functional dyspepsia. Rome III diagnostic criteria 1,2 Rome IV diagnostic criteria 3,4 Diagnostic criteria for IBS
Irritable Bowel Syndrome Now. George M. Logan, MD Friday, May 5, :35 4:05 PM
 Irritable Bowel Syndrome Now George M. Logan, MD Friday, May 5, 2017 3:35 4:05 PM Dr. Logan indicated no potential conflict of interest to this presentation. He does not intend to discuss any unapproved/investigative
Irritable Bowel Syndrome Now George M. Logan, MD Friday, May 5, 2017 3:35 4:05 PM Dr. Logan indicated no potential conflict of interest to this presentation. He does not intend to discuss any unapproved/investigative
Why does my stomach hurt? Exploring irritable bowel syndrome
 Why does my stomach hurt? Exploring irritable bowel syndrome By Flavio M. Habal, MD, PhD, FRCPC Case In this article: 1. What is IBS? A 45-year-old female is referred to your office with recurrent 2. How
Why does my stomach hurt? Exploring irritable bowel syndrome By Flavio M. Habal, MD, PhD, FRCPC Case In this article: 1. What is IBS? A 45-year-old female is referred to your office with recurrent 2. How
... SELECTED ABSTRACTS...
 ... SELECTED ABSTRACTS... The following abstracts, from medical journals containing literature on irritable bowel syndrome, were selected for their relevance to this supplement. A Technical Review for
... SELECTED ABSTRACTS... The following abstracts, from medical journals containing literature on irritable bowel syndrome, were selected for their relevance to this supplement. A Technical Review for
Is one of the most common chronic disorders. causing patients to seek medical treatment.
 ILOs After this lecture you should be able to : Define IBS Identify causes and risk factors of IBS Determine the appropriate therapeutic options for IBS Is one of the most common chronic disorders causing
ILOs After this lecture you should be able to : Define IBS Identify causes and risk factors of IBS Determine the appropriate therapeutic options for IBS Is one of the most common chronic disorders causing
190 Index Case studies, abdominal pain, 2 Crohn s disease, 2 3, cyclic vomiting syndrome (CVS), 2 fecal incontinence (FI), 2 medical c
, 2 fecal incontinence (FI), 2 medical c") Index Abdominal pain, case study, 2 Achalasia, 75 Acupuncture 108 American Academy of Pediatrics, 49 Anxiety, 8 9, 98 Autism, GI disorders and, 25 27 BASC. See Behavior Assessment System for Children (BASC)
Index Abdominal pain, case study, 2 Achalasia, 75 Acupuncture 108 American Academy of Pediatrics, 49 Anxiety, 8 9, 98 Autism, GI disorders and, 25 27 BASC. See Behavior Assessment System for Children (BASC)
The Role of Food in the Functional Gastrointestinal Disorders
 The Role of Food in the Functional Gastrointestinal Disorders H. Vahedi, MD. Gastroentrologist Associate professor of medicine DDRI 92.4.27 vahedi@ams.ac.ir Disorder Sub-category A. Oesophageal disorders
The Role of Food in the Functional Gastrointestinal Disorders H. Vahedi, MD. Gastroentrologist Associate professor of medicine DDRI 92.4.27 vahedi@ams.ac.ir Disorder Sub-category A. Oesophageal disorders
FUNCTIONAL DISORDERS ROME IV CRITERIA AND DIAGNOSTIC QUESTIONNAIRE DDW 2016,REVIEW. Presented by; Marjan Mokhtare Gastroenterologist, IUMS
 FUNCTIONAL DISORDERS ROME IV CRITERIA AND DIAGNOSTIC QUESTIONNAIRE DDW 2016,REVIEW Presented by; Marjan Mokhtare Gastroenterologist, IUMS Functional gastrointestinal disorders (FGIDs), the most common
FUNCTIONAL DISORDERS ROME IV CRITERIA AND DIAGNOSTIC QUESTIONNAIRE DDW 2016,REVIEW Presented by; Marjan Mokhtare Gastroenterologist, IUMS Functional gastrointestinal disorders (FGIDs), the most common
Bloating, Flatulence, and
 A 45-Year-Old Man With Recurrent Abdominal Pain, Bloating, Flatulence, and Intermittent Loose Stools Anthony J. Lembo, MD Associate Professor of Medicine Harvard Medical School Director, GI Motility Laboratory
A 45-Year-Old Man With Recurrent Abdominal Pain, Bloating, Flatulence, and Intermittent Loose Stools Anthony J. Lembo, MD Associate Professor of Medicine Harvard Medical School Director, GI Motility Laboratory
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
Rome III: an ongoing journey for better diagnosis and treatment of functional gastrointestinal disorders
 Mædica - a Journal of Clinical Medicine EDITORIALS Rome III: an ongoing journey for better diagnosis and treatment of functional gastrointestinal disorders Mircea DICULESCU, MD, Tudor ARBANAS, MD Gastroenterology
Mædica - a Journal of Clinical Medicine EDITORIALS Rome III: an ongoing journey for better diagnosis and treatment of functional gastrointestinal disorders Mircea DICULESCU, MD, Tudor ARBANAS, MD Gastroenterology
IBS Irritable Bowel syndrome Therapeutics II PHCL 430
 Salman Bin AbdulAziz University College Of Pharmacy IBS Irritable Bowel syndrome Therapeutics II PHCL 430 Email:- ahmedadel.pharmd@gmail.com Ahmed A AlAmer PharmD R.S is 32-year-old woman experiences intermittent
Salman Bin AbdulAziz University College Of Pharmacy IBS Irritable Bowel syndrome Therapeutics II PHCL 430 Email:- ahmedadel.pharmd@gmail.com Ahmed A AlAmer PharmD R.S is 32-year-old woman experiences intermittent
Irritable Bowel Syndrome. Paul Sheykhzadeh, DO, FACG Digestive Health Associates Reno, NV NAPNA Symposium March 5, 2016
 Irritable Bowel Syndrome Paul Sheykhzadeh, DO, FACG Digestive Health Associates Reno, NV NAPNA Symposium March 5, 2016 Definition of Irritable Bowel Syndrome (IBS) Rome III Criteria Recurrent abdominal
Irritable Bowel Syndrome Paul Sheykhzadeh, DO, FACG Digestive Health Associates Reno, NV NAPNA Symposium March 5, 2016 Definition of Irritable Bowel Syndrome (IBS) Rome III Criteria Recurrent abdominal
A Guide to Gastrointestinal Motility Disorders
 A Guide to Gastrointestinal Motility Disorders Albert J. Bredenoord André Smout Jan Tack A Guide to Gastrointestinal Motility Disorders Albert J. Bredenoord Gastroenterology and Hepatology Academic Medical
A Guide to Gastrointestinal Motility Disorders Albert J. Bredenoord André Smout Jan Tack A Guide to Gastrointestinal Motility Disorders Albert J. Bredenoord Gastroenterology and Hepatology Academic Medical
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
Xifaxan, Lotronex and Viberzi Prior Authorization and Quantity Limit Program Summary
 Xifaxan, Lotronex and Viberzi Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1,2 Lotronex (alosetron) a Indication For women with severe diarrheapredominant irritable
Xifaxan, Lotronex and Viberzi Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1,2 Lotronex (alosetron) a Indication For women with severe diarrheapredominant irritable
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders What are functional GI disorders?
 The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD and Kellie Bunn, PA-C What are functional GI
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD and Kellie Bunn, PA-C What are functional GI
David Leff, DO. April 13, Disclosure. I have the following financial relationships to disclosure:
 David Leff, DO AOMA 94 th Annual Convention April 13, 2016 Disclosure I have the following financial relationships to disclosure: Speaker s Bureau: Allergan Labs, Takeda Pharmaceutical, Valeant Pharmaceutical
David Leff, DO AOMA 94 th Annual Convention April 13, 2016 Disclosure I have the following financial relationships to disclosure: Speaker s Bureau: Allergan Labs, Takeda Pharmaceutical, Valeant Pharmaceutical
Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider
 For the Primary Care Provider") Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider Elizabeth Coss, MD General Gastroenterologist Audie Murphy Veterans Hospital UT Health This presentation does not
Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider Elizabeth Coss, MD General Gastroenterologist Audie Murphy Veterans Hospital UT Health This presentation does not
Primary Management of Irritable Bowel Syndrome
 Primary Management of Irritable Bowel Syndrome Jasmine Zia, MD Acting Instructor, Division of Gastroenterology Current Concepts in Drug Therapy CME Course April 23, 2015 Irritable Bowel Syndrome (IBS)
Primary Management of Irritable Bowel Syndrome Jasmine Zia, MD Acting Instructor, Division of Gastroenterology Current Concepts in Drug Therapy CME Course April 23, 2015 Irritable Bowel Syndrome (IBS)
Common Gastrointestinal Problems in the Elderly
 Common Gastrointestinal Problems in the Elderly Brian Viviano, D.O. Objectives Understand the pathophysiology, clinical manifestations, diagnosis and management of GI diseases of the elderly. Differentiate
Common Gastrointestinal Problems in the Elderly Brian Viviano, D.O. Objectives Understand the pathophysiology, clinical manifestations, diagnosis and management of GI diseases of the elderly. Differentiate
Evolving Therapy in Irritable Bowel Syndrome (IBS)
") Evolving Therapy in Irritable Bowel Syndrome (IBS) Dr. Syed Mohammad Arif MBBS, FCPS (Medicine), MD (Gastro) Associate Professor Department of Medicine Dhaka Medical College A good set of bowels is worth
Evolving Therapy in Irritable Bowel Syndrome (IBS) Dr. Syed Mohammad Arif MBBS, FCPS (Medicine), MD (Gastro) Associate Professor Department of Medicine Dhaka Medical College A good set of bowels is worth
4) Irritable Bowel Syndrome - Dr. Shaikhani. Epidemiology. Pathophysiology. Burden. Diagnosis
 Irritable Bowel Syndrome - Dr. Shaikhani. Epidemiology. Pathophysiology. Burden. Diagnosis") 4) Irritable Bowel Syndrome - Dr. Shaikhani Epidemiology A common disorder, with a 7% prevalence. Women are 1.5 times more likely to be affected than men, most commonly between ages 20-40 years. Onset
4) Irritable Bowel Syndrome - Dr. Shaikhani Epidemiology A common disorder, with a 7% prevalence. Women are 1.5 times more likely to be affected than men, most commonly between ages 20-40 years. Onset
IBS current status Peter Laszlo Lakatos
 IBS current status Peter Laszlo Lakatos Semmelweis University 1st Department of Medicine Functional gastrointestinal disorders Chronic or fluctuating functional gastrointestinal symptoms that can not be
IBS current status Peter Laszlo Lakatos Semmelweis University 1st Department of Medicine Functional gastrointestinal disorders Chronic or fluctuating functional gastrointestinal symptoms that can not be
Outline. Definition (s) Epidemiology Pathophysiology Management With an emphasis on recent developments
 Epidemiology Pathophysiology Management With an emphasis on recent developments") Chronic Dyspepsia Eamonn M M Quigley MD FRCP FACP MACG FRCPI Lynda K and David M Underwood Center for Digestive Disorders Houston Methodist Hospital Houston, Texas Outline Definition (s) Epidemiology Pathophysiology
Chronic Dyspepsia Eamonn M M Quigley MD FRCP FACP MACG FRCPI Lynda K and David M Underwood Center for Digestive Disorders Houston Methodist Hospital Houston, Texas Outline Definition (s) Epidemiology Pathophysiology
Chronic Abdominal Pain. Dr. Robert B. Smith Tupelo Digestive Health Specialists August 26, 2016
 Chronic Abdominal Pain Dr. Robert B. Smith Tupelo Digestive Health Specialists August 26, 2016 Disclosures Speaker Bureau for Allergan Pharmaceuticals Abdominal Pain - Definitions Acute occurring for several
Chronic Abdominal Pain Dr. Robert B. Smith Tupelo Digestive Health Specialists August 26, 2016 Disclosures Speaker Bureau for Allergan Pharmaceuticals Abdominal Pain - Definitions Acute occurring for several
Constipation An Overview. Definition Physiology of GI tract Etiology Assessment Treatment
 CONSTIPATION Constipation An Overview Definition Physiology of GI tract Etiology Assessment Treatment Definition Constipation = the infrequent passage of hard feces Definition of Infrequent The meaning
CONSTIPATION Constipation An Overview Definition Physiology of GI tract Etiology Assessment Treatment Definition Constipation = the infrequent passage of hard feces Definition of Infrequent The meaning
Zelmac Learning System: Module 2
 Learning Objectives Zelmac Learning System: Module 2 Overview of Gastrointestinal Disorders 2-1 Learning Objectives Recognize that a variety of GI conditions can cause symptoms similar to those present
Learning Objectives Zelmac Learning System: Module 2 Overview of Gastrointestinal Disorders 2-1 Learning Objectives Recognize that a variety of GI conditions can cause symptoms similar to those present
Irritable bowel syndrome (IBS) is a ... PRESENTATION... Defining and Diagnosing Irritable Bowel Syndrome
 is a ... PRESENTATION... Defining and Diagnosing Irritable Bowel Syndrome") ... PRESENTATION... Defining and Diagnosing Irritable Bowel Syndrome Based on a presentation by Marvin M. Schuster, MD Presentation Summary Approximately 20% of the general population has irritable bowel
... PRESENTATION... Defining and Diagnosing Irritable Bowel Syndrome Based on a presentation by Marvin M. Schuster, MD Presentation Summary Approximately 20% of the general population has irritable bowel
What is Irritable Bowel Syndrome (IBS)?
?") What is Irritable Bowel Syndrome (IBS)? Irritable bowel syndrome (IBS) is a health issue found in your intestines (gut). IBS can cause symptoms such as: Belly pain. Cramping. Gas. Bloating (or swelling)
What is Irritable Bowel Syndrome (IBS)? Irritable bowel syndrome (IBS) is a health issue found in your intestines (gut). IBS can cause symptoms such as: Belly pain. Cramping. Gas. Bloating (or swelling)
Clinically proven to quickly relieve symptoms of common gastrointestinal disorders. TERRAGASTRO - Good health starts in the gut
 Clinically proven to quickly relieve symptoms of common gastrointestinal disorders GASTROINTESTINAL DISEASE Referred to as gastrointestinal diseases, they are common disorders which affect the esophagus,
Clinically proven to quickly relieve symptoms of common gastrointestinal disorders GASTROINTESTINAL DISEASE Referred to as gastrointestinal diseases, they are common disorders which affect the esophagus,
At the outset, we want to clear up some terminology issues. IBS is COPYRIGHTED MATERIAL. What Is IBS?
 1 What Is IBS? At the outset, we want to clear up some terminology issues. IBS is the abbreviation that doctors use for irritable bowel syndrome, often when they are talking about people with IBS. We will
1 What Is IBS? At the outset, we want to clear up some terminology issues. IBS is the abbreviation that doctors use for irritable bowel syndrome, often when they are talking about people with IBS. We will
Functional Dyspepsia. Norbert Welkovics Heine van der Walt
 Norbert Welkovics Heine van der Walt Characteristics: Central abdomen Pain or discomfort Not associated with bowel movements No structural or biochemical abnormalty Definition Part of Gastroduodenal disorders
Norbert Welkovics Heine van der Walt Characteristics: Central abdomen Pain or discomfort Not associated with bowel movements No structural or biochemical abnormalty Definition Part of Gastroduodenal disorders
Advancing gastroenterology, improving patient care
 American College of Gastroenterology Advancing gastroenterology, improving patient care Note to Visitors: A fully updated ACG Systematic Review on the Management of Chronic Idiopathic Constipation and
American College of Gastroenterology Advancing gastroenterology, improving patient care Note to Visitors: A fully updated ACG Systematic Review on the Management of Chronic Idiopathic Constipation and
Irritable Bowel Syndrome. Mustafa Giaffer March 2017
 Irritable Bowel Syndrome Mustafa Giaffer March 2017 Introduction First described in 1771. 50% of patients present
Irritable Bowel Syndrome Mustafa Giaffer March 2017 Introduction First described in 1771. 50% of patients present
Objectives. Identify age-related changes in the gastrointestinal tract
 The Primary Care Physician s Approach to Gastrointestinal Complaints in the Elderly Brian Viviano, D.O. Medical Associates of Erie Objectives Identify age-related changes in the gastrointestinal tract
The Primary Care Physician s Approach to Gastrointestinal Complaints in the Elderly Brian Viviano, D.O. Medical Associates of Erie Objectives Identify age-related changes in the gastrointestinal tract
Presenter. Irritable Bowel Syndrome. Objectives. Introduction. Rome Criteria. Irritable Bowel Syndrome 2/28/2018
 Presenter Irritable Bowel Syndrome Current evidence for diagnosis & management Julie Daniels DNP, CNM Assistant Professor Course Coordinator of Primary Care of Women Faculty at Frontier Nursing University
Presenter Irritable Bowel Syndrome Current evidence for diagnosis & management Julie Daniels DNP, CNM Assistant Professor Course Coordinator of Primary Care of Women Faculty at Frontier Nursing University
Section Coordinator: Jerome W. Breslin, PhD, Assistant Professor of Physiology, MEB 7208, ,
 IDP Biological Systems Gastrointestinal System Section Coordinator: Jerome W. Breslin, PhD, Assistant Professor of Physiology, MEB 7208, 504-568-2669, jbresl@lsuhsc.edu Overall Learning Objectives 1. Characterize
IDP Biological Systems Gastrointestinal System Section Coordinator: Jerome W. Breslin, PhD, Assistant Professor of Physiology, MEB 7208, 504-568-2669, jbresl@lsuhsc.edu Overall Learning Objectives 1. Characterize
Protectives and Adsorbents. Inorganic chemistry Course 1 Third year Assist. Lecturer Ahlam A. Shafeeq MSc. Pharmaceutical chemistry
 Protectives and Adsorbents Inorganic chemistry Course 1 Third year 2016-2017 Assist. Lecturer Ahlam A. Shafeeq MSc. Pharmaceutical chemistry Protectives and Adsorbents This group of gastrointestinal agents
Protectives and Adsorbents Inorganic chemistry Course 1 Third year 2016-2017 Assist. Lecturer Ahlam A. Shafeeq MSc. Pharmaceutical chemistry Protectives and Adsorbents This group of gastrointestinal agents
Lower Gastrointestinal Tract KNH 406
 Lower Gastrointestinal Tract KNH 406 Lower GI Tract A&P Small Intestine Anatomy Duodenum, jejunum, ileum Maximum surface area for digestion and absorption Specialized enterocytes from stem cells of crypts
Lower Gastrointestinal Tract KNH 406 Lower GI Tract A&P Small Intestine Anatomy Duodenum, jejunum, ileum Maximum surface area for digestion and absorption Specialized enterocytes from stem cells of crypts
Functional Heartburn and Dyspepsia
 Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
 Disorders in which symptoms cannot be explained by the presence of structural or tissue abnormalities Irritable bowel syndrome Functional heartburn Functional dyspepsia Functional constipation Functional
Disorders in which symptoms cannot be explained by the presence of structural or tissue abnormalities Irritable bowel syndrome Functional heartburn Functional dyspepsia Functional constipation Functional
UNDERSTANDING IBS AND CC Implications for diagnosis and management
 UNDERSTANDING IBS AND CC Implications for diagnosis and management J. TACK, M.D., Ph.D. Department of Gastroenterology University Hospitals, K.U. Leuven Leuven, Belgium TYPES OF GASTROINTESTINAL DISORDERS
UNDERSTANDING IBS AND CC Implications for diagnosis and management J. TACK, M.D., Ph.D. Department of Gastroenterology University Hospitals, K.U. Leuven Leuven, Belgium TYPES OF GASTROINTESTINAL DISORDERS
Elderly Man With Chronic Constipation
 Elderly Man With Chronic Constipation Linda Nguyen, MD Director, Neurogastroenterology and Motility Clinical Assistant Professor Stanford University Overview Normal bowel function Defining Constipation:
Elderly Man With Chronic Constipation Linda Nguyen, MD Director, Neurogastroenterology and Motility Clinical Assistant Professor Stanford University Overview Normal bowel function Defining Constipation:
IBS: overview and assessment of pain outcomes and implications for inclusion criteria
 IBS: overview and assessment of pain outcomes and implications for inclusion criteria William D. Chey, MD Professor of Medicine University of Michigan What is the Irritable Bowel Syndrome Symptom based
IBS: overview and assessment of pain outcomes and implications for inclusion criteria William D. Chey, MD Professor of Medicine University of Michigan What is the Irritable Bowel Syndrome Symptom based
GI Pharmacology -4 Irritable Bowel Syndrome and Antiemetics. Dr. Alia Shatanawi
 GI Pharmacology -4 Irritable Bowel Syndrome and Antiemetics Dr. Alia Shatanawi 11-04-2018 Drugs used in Irritable Bowel Syndrome Idiopathic, chronic, relapsing disorder characterized by abdominal discomfort
GI Pharmacology -4 Irritable Bowel Syndrome and Antiemetics Dr. Alia Shatanawi 11-04-2018 Drugs used in Irritable Bowel Syndrome Idiopathic, chronic, relapsing disorder characterized by abdominal discomfort
Management of Functional Bowel Disorders
 Management of Functional Bowel Disorders Amy Foxx-Orenstein, DO, FACG, FACP Professor of Medicine Mayo Clinic Tucson Osteopathic Medical Foundation May 1, 2016 Objectives Review epidemiology and pathophysiology
Management of Functional Bowel Disorders Amy Foxx-Orenstein, DO, FACG, FACP Professor of Medicine Mayo Clinic Tucson Osteopathic Medical Foundation May 1, 2016 Objectives Review epidemiology and pathophysiology
Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514
 Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514 Normal Gastrointestinal Motility and Function "Motility" is an unfamiliar word to many people; it is used primarily
Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514 Normal Gastrointestinal Motility and Function "Motility" is an unfamiliar word to many people; it is used primarily
IBS. Patient INFO. A Guide to Irritable Bowel Syndrome
 Patient INFO IBS A Guide to Irritable Bowel Syndrome The information provided by the AGA Institute is not medical advice and should not be considered a replacement for seeing a medical professional. About
Patient INFO IBS A Guide to Irritable Bowel Syndrome The information provided by the AGA Institute is not medical advice and should not be considered a replacement for seeing a medical professional. About
6/25/ % 20% 50% 19% Functional Dyspepsia Peptic Ulcer GERD Cancer Other
 Peptic Ulcer Disease and Dyspepsia John M. Inadomi, MD Professor of Medicine UCSF Chief, Clinical Gastroenterology San Francisco General Hospital Case History 49 y/o woman complains of several months of
Peptic Ulcer Disease and Dyspepsia John M. Inadomi, MD Professor of Medicine UCSF Chief, Clinical Gastroenterology San Francisco General Hospital Case History 49 y/o woman complains of several months of
Human Anatomy rectum
 rectum The colon is also called the large intestine. The ileum (last part of the small intestine) connects to the cecum (first part of the colon) in the lower right abdomen. The rest of the colon is divided
rectum The colon is also called the large intestine. The ileum (last part of the small intestine) connects to the cecum (first part of the colon) in the lower right abdomen. The rest of the colon is divided
Diarrhea may be: Acute (short-term, usually lasting several days), which is usually related to bacterial or viral infections.
, which is usually related to bacterial or viral infections.") Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
Constipation. What is constipation? What is the criteria for having constipation? What are the different types of constipation?
 What is constipation? is defined as having a bowel movement less than 3 times per week. It is usually associated with hard stools or difficulty passing stools. You may have pain while passing stools or
What is constipation? is defined as having a bowel movement less than 3 times per week. It is usually associated with hard stools or difficulty passing stools. You may have pain while passing stools or
IRRITABLE BOWEL SYNDROME Dr E Lalor, MB ChB, FRCPC 2016 (but written before Rome IV see Gastroenterology, May 2016).
.") IRRITABLE BOWEL SYNDROME Dr E Lalor, MB ChB, FRCPC 2016 (but written before Rome IV see Gastroenterology, May 2016). Irritable bowel syndrome (IBS) is one of the functional GI (gastro-intestinal) disorders,
IRRITABLE BOWEL SYNDROME Dr E Lalor, MB ChB, FRCPC 2016 (but written before Rome IV see Gastroenterology, May 2016). Irritable bowel syndrome (IBS) is one of the functional GI (gastro-intestinal) disorders,
Irritable Bowel Syndrome and Chronic Constipation. Treatment of IBS. Susan Lucak, M.D. Columbia University Medical Center
 Ti tl e s l i d e - p a rt 1 Irritable Bowel Syndrome and Chronic Constipation Susan Lucak, M.D. Columbia University Medical Center Treatment of IBS Abdominal pain / discomfort Antispasmodics Antidepressants
Ti tl e s l i d e - p a rt 1 Irritable Bowel Syndrome and Chronic Constipation Susan Lucak, M.D. Columbia University Medical Center Treatment of IBS Abdominal pain / discomfort Antispasmodics Antidepressants
Irritable Bowel Syndrome (IBS)
") Irritable Bowel Syndrome (IBS) Dr Rex J Polson 17 th January 2018 Overview Description of the condition Discussion of symptoms and investigations that may be required Discussion of management and treatment
Irritable Bowel Syndrome (IBS) Dr Rex J Polson 17 th January 2018 Overview Description of the condition Discussion of symptoms and investigations that may be required Discussion of management and treatment
Disclosures. Objectives. Pre-Test Question 1. Pre-Test Question 2. Pre-Test Question 3 9/23/2016
 Disclosures Beating the Bowel Blues: An Update on the Treatment of Irritable Bowel Syndrome Matthew Nelson, PharmDBCPS, Roosevelt University College of Pharmacy Matthew Nelson declares no conflicts of
Disclosures Beating the Bowel Blues: An Update on the Treatment of Irritable Bowel Syndrome Matthew Nelson, PharmDBCPS, Roosevelt University College of Pharmacy Matthew Nelson declares no conflicts of
Chapter 41. Media Directory. Lower Digestive Tract. Constipation (continued) Constipation
 Constipation") Chapter 41 Drugs for Bowel Disorders and Other Gastrointestinal Conditions Slide 43 Media Directory Tegaserod Animation Upper Saddle River, New Jersey 07458 All rights reserved. Lower Digestive Tract Figure
Chapter 41 Drugs for Bowel Disorders and Other Gastrointestinal Conditions Slide 43 Media Directory Tegaserod Animation Upper Saddle River, New Jersey 07458 All rights reserved. Lower Digestive Tract Figure
What you really need to know about Gastroparesis?
 What you really need to know about Gastroparesis? John M. Wo, MD Division of Gastroenterology/Hepatology Director of GI Motility and Neurogastroenterology 8/3/2016 1/4/2017 1 What you really need to know
What you really need to know about Gastroparesis? John M. Wo, MD Division of Gastroenterology/Hepatology Director of GI Motility and Neurogastroenterology 8/3/2016 1/4/2017 1 What you really need to know
10/10/16. Disclosures. Educational Objectives
 Nimish Vakil, MD, FACP, FACG, AGAF, FASGE Clinical Adjunct Professor University of Wisconsin Madison, Wisconsin Disclosures All faculty, course directors, planning committee, content reviewers and others
Nimish Vakil, MD, FACP, FACG, AGAF, FASGE Clinical Adjunct Professor University of Wisconsin Madison, Wisconsin Disclosures All faculty, course directors, planning committee, content reviewers and others
Gastrointestinal Motility 2: Intestinal and Colonic Motility Jack Grider, Ph.D.
 Gastrointestinal Motility 2: Intestinal and Colonic Motility Jack Grider, Ph.D. OBJECTIVES: 1. Contrast the types of motility in the small intestine. 2. Describe the neural circuits that mediate peristalsis.
Gastrointestinal Motility 2: Intestinal and Colonic Motility Jack Grider, Ph.D. OBJECTIVES: 1. Contrast the types of motility in the small intestine. 2. Describe the neural circuits that mediate peristalsis.
Identify electrolytes that should be monitored whenever prolonged or severe diarrhea is present
 Chapter 35 Drugs Used to Treat Constipation and Diarrhea Learning Objectives State the underlying causes of constipation Explain the meaning of normal bowel habits Cite nine causes of diarrhea Describe
Chapter 35 Drugs Used to Treat Constipation and Diarrhea Learning Objectives State the underlying causes of constipation Explain the meaning of normal bowel habits Cite nine causes of diarrhea Describe
Irritable Bowel Syndrome: Update on Pathogenesis and Management
 Review Med Principles Pract 2002;11:2 17 Received: December 16, 2000 Revised: July 24, 2001 Irritable Bowel Syndrome: Update on Pathogenesis and Management Osama Alaradi Jamie S. Barkin Division of Gastroenterology,
Review Med Principles Pract 2002;11:2 17 Received: December 16, 2000 Revised: July 24, 2001 Irritable Bowel Syndrome: Update on Pathogenesis and Management Osama Alaradi Jamie S. Barkin Division of Gastroenterology,
Emerging Treatments for IBS-C and Clinical Trial Endpoints
 Emerging Treatments for IBS-C and Clinical Trial Endpoints Lin Chang, M.D. Oppenheimer Family Center for Neurobiology of Stress David Geffen School of Medicine at UCLA Learning Objectives Describe current
Emerging Treatments for IBS-C and Clinical Trial Endpoints Lin Chang, M.D. Oppenheimer Family Center for Neurobiology of Stress David Geffen School of Medicine at UCLA Learning Objectives Describe current
Throughout recorded history, and alongside structural
 GASTROENTEROLOGY 2006;130:1377 1390 INTRODUCTION The Functional Gastrointestinal Disorders and the Rome III Process DOUGLAS A. DROSSMAN, Guest Editor Division of Gastroenterology and Hepatology, UNC Center
GASTROENTEROLOGY 2006;130:1377 1390 INTRODUCTION The Functional Gastrointestinal Disorders and the Rome III Process DOUGLAS A. DROSSMAN, Guest Editor Division of Gastroenterology and Hepatology, UNC Center
J Neurogastroenterol Motil, Vol. 17 No. 3 July, 2011 DOI: /jnm Journal of Neurogastroenterology and Motility
 ㅋ JNM J Neurogastroenterol Motil, Vol. 17 No. 3 July, 2011 DOI: 10.5056/jnm.2011.17.3.279 Journal of Neurogastroenterology and Motility Original Article Functional Gastrointestinal Disorders Diagnosed
ㅋ JNM J Neurogastroenterol Motil, Vol. 17 No. 3 July, 2011 DOI: 10.5056/jnm.2011.17.3.279 Journal of Neurogastroenterology and Motility Original Article Functional Gastrointestinal Disorders Diagnosed
Constipation and bowel obstruction
 Constipation and bowel obstruction Constipation Infrequent or difficult defecation with reduced number of bowel movements, which may or may not be abnormally hard with increased difficulty or discomfort
Constipation and bowel obstruction Constipation Infrequent or difficult defecation with reduced number of bowel movements, which may or may not be abnormally hard with increased difficulty or discomfort
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514
 Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514 History of Functional Disorders Douglas A. Drossman, MD Melissa Swantkowski THE PAST HISTORICAL PRECEDENTS Historians
Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514 History of Functional Disorders Douglas A. Drossman, MD Melissa Swantkowski THE PAST HISTORICAL PRECEDENTS Historians
UKLIN1693a, date of preparation: March 2013.
 1 This table shows the ICE model. Defining the patient s ideas, concerns, and expectations is an important part of the consultation that can lead to better outcomes. 2 Patients with IBS may have visceral
1 This table shows the ICE model. Defining the patient s ideas, concerns, and expectations is an important part of the consultation that can lead to better outcomes. 2 Patients with IBS may have visceral
Drugs Affecting the Gastrointestinal System. Antidiarrheal and Laxatives
 Drugs Affecting the Gastrointestinal System Antidiarrheal and Laxatives Diarrhea Abnormal frequent passage of loose stools or Abnormal passage of stools with increased frequency, fluidity, and weight,
Drugs Affecting the Gastrointestinal System Antidiarrheal and Laxatives Diarrhea Abnormal frequent passage of loose stools or Abnormal passage of stools with increased frequency, fluidity, and weight,
IBS. Dan Carter, M.D. Institute of Gastroenterology Sheba medical center
 IBS Dan Carter, M.D. Institute of Gastroenterology Sheba medical center Epidemiology Irritable bowel syndrome is a common functional gastrointestinal disorder that manifests as abdominal pain or discomfort
IBS Dan Carter, M.D. Institute of Gastroenterology Sheba medical center Epidemiology Irritable bowel syndrome is a common functional gastrointestinal disorder that manifests as abdominal pain or discomfort
Biofeedback for Pelvic Floor Disorders and Incontinence
 The UNC Center for Functional GI & Motility Disorders www.med.unc.edu/ibs Biofeedback for Pelvic Floor Disorders and Incontinence Olafur S. Palsson, Psy.D. Associate Professor of Medicine UNC Center for
The UNC Center for Functional GI & Motility Disorders www.med.unc.edu/ibs Biofeedback for Pelvic Floor Disorders and Incontinence Olafur S. Palsson, Psy.D. Associate Professor of Medicine UNC Center for
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
Clinical problems related to GI involvement in SSc
 Clinical problems related to GI involvement in SSc Incontinence Abdominal pain/distension Gastro-oesophageal Diarrhoea Weight loss/al Issues Constipation Management of incontinence Establish diagnosis
Clinical problems related to GI involvement in SSc Incontinence Abdominal pain/distension Gastro-oesophageal Diarrhoea Weight loss/al Issues Constipation Management of incontinence Establish diagnosis
Functional Dyspepsia
 Functional Dyspepsia American College of Gastroenterology Boston Massachusetts, June 2015 Brian E. Lacy, PhD, MD, FACG Professor of Medicine Geisel School of Medicine at Dartmouth Chief, Section of Gastroenterology
Functional Dyspepsia American College of Gastroenterology Boston Massachusetts, June 2015 Brian E. Lacy, PhD, MD, FACG Professor of Medicine Geisel School of Medicine at Dartmouth Chief, Section of Gastroenterology
Functional bowel disorders and functional abdominal pain
 Gut 1999;45(Suppl II):II43 II47 II43 Chair, Committee on Functional Bowel Disorders and Functional Abdominal Pain, Multinational Working Teams to Develop Diagnostic Criteria for Functional Gastrointestinal
Gut 1999;45(Suppl II):II43 II47 II43 Chair, Committee on Functional Bowel Disorders and Functional Abdominal Pain, Multinational Working Teams to Develop Diagnostic Criteria for Functional Gastrointestinal
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
IRRITABLE BOWEL SYNDROME
 c IRRITABLE BOWEL SYNDROME Success is no accident. It is hard work, perseverance, learning, studying, sacrifice and most of all, love of what you are doing or learning to do. Color code Important doctor
c IRRITABLE BOWEL SYNDROME Success is no accident. It is hard work, perseverance, learning, studying, sacrifice and most of all, love of what you are doing or learning to do. Color code Important doctor
Chapter 34. Nursing Care of Patients with Lower Gastrointestinal Disorders
 Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Gastrointestinal. Issues in ElderCare. TCHP Education. Consortium. Part of the ElderCare: Healthcare for the Aging Series
 TCHP Education Consortium Gastrointestinal Issues in ElderCare Part of the ElderCare: Healthcare for the Aging Series TCHP Education Consortium, 2004, 2007 This educational activity expires December 31,
TCHP Education Consortium Gastrointestinal Issues in ElderCare Part of the ElderCare: Healthcare for the Aging Series TCHP Education Consortium, 2004, 2007 This educational activity expires December 31,
Propulsion and mixing of food in the alimentary tract Chapter 63
 Propulsion and mixing of food in the alimentary tract Chapter 63 Types of GI movements: Propulsive movement-peristalsis Propulsion: controlled movement of ingested foods, liquids, GI secretions, and sloughed
Propulsion and mixing of food in the alimentary tract Chapter 63 Types of GI movements: Propulsive movement-peristalsis Propulsion: controlled movement of ingested foods, liquids, GI secretions, and sloughed
Efficacy and Safety of Lubiprostone. Laura Wozniak February 23, 2010 K30 Monthly Journal Club
 Efficacy and Safety of Lubiprostone Laura Wozniak February 23, 2010 K30 Monthly Journal Club Objectives Brief overview of constipation Review of article Discussion Constipation in Children 3-5% of all
Efficacy and Safety of Lubiprostone Laura Wozniak February 23, 2010 K30 Monthly Journal Club Objectives Brief overview of constipation Review of article Discussion Constipation in Children 3-5% of all
Understanding & Alleviating Constipation. Living (Well!) with Gastroparesis Program Warm-Up Class
 with Gastroparesis Program Warm-Up Class") Understanding & Alleviating Constipation Living (Well!) with Gastroparesis Program Warm-Up Class Please Remember The information presented is for educational purposes only and is in no way intended as
Understanding & Alleviating Constipation Living (Well!) with Gastroparesis Program Warm-Up Class Please Remember The information presented is for educational purposes only and is in no way intended as
Diet and Gastrointestinal Problems
 Chapter 20 Diet and Gastrointestinal Problems Objectives Explain uses of diet therapy in gastrointestinal disturbances Identify foods allowed and disallowed in therapeutic diets discussed Adapt normal
Chapter 20 Diet and Gastrointestinal Problems Objectives Explain uses of diet therapy in gastrointestinal disturbances Identify foods allowed and disallowed in therapeutic diets discussed Adapt normal
Weekly Prevalence of Symptoms USA vs. Colombia
 THE OVERLAP BETWEEN INFLAMMATORY BOWEL DISEASE AND FUNCTIONAL GASTROINTESTINAL DISORDERS: CHALLENGES AND TREATMENT IMPLICATIONS Miguel Saps, MD Professor of Pediatrics, Ohio State University Director of
THE OVERLAP BETWEEN INFLAMMATORY BOWEL DISEASE AND FUNCTIONAL GASTROINTESTINAL DISORDERS: CHALLENGES AND TREATMENT IMPLICATIONS Miguel Saps, MD Professor of Pediatrics, Ohio State University Director of
New Tests and Treatments for Dyspepsia and Irritable Bowel Syndrome
 New Tests and Treatments for Dyspepsia and Irritable Bowel Syndrome Soojong Hong Chae, MD Clinical Assistant Professor Digestive Diseases and Nutrition University of South Florida ROME III Functional dyspepsia
New Tests and Treatments for Dyspepsia and Irritable Bowel Syndrome Soojong Hong Chae, MD Clinical Assistant Professor Digestive Diseases and Nutrition University of South Florida ROME III Functional dyspepsia
Amyloidosis & the GI Tract
 Amyloidosis & the GI Tract John O. Clarke, M.D. Director, Esophageal Program Clinical Associate Professor of Medicine Stanford University john.clarke@stanford.edu 2017 Topics to cover 1) Patterns of GI
Amyloidosis & the GI Tract John O. Clarke, M.D. Director, Esophageal Program Clinical Associate Professor of Medicine Stanford University john.clarke@stanford.edu 2017 Topics to cover 1) Patterns of GI
IBS-D: The Role of Pathophysiology in Assessment and Treatment ReachMD Page 1 of 7
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
with DIARRHEA (IBS-D)
") Understanding IRRITABLE BOWEL SYNDROME with DIARRHEA (IBS-D) What is Irritable Bowel Syndrome with Diarrhea (IBS-D)? Irritable Bowel Syndrome (IBS) is a common chronic gastrointestinal disorder that involves
Understanding IRRITABLE BOWEL SYNDROME with DIARRHEA (IBS-D) What is Irritable Bowel Syndrome with Diarrhea (IBS-D)? Irritable Bowel Syndrome (IBS) is a common chronic gastrointestinal disorder that involves
Managing constipation in residential care
 Managing constipation in residential care Amanda Lee Lecturer, Hull University ; PhD Candidate, Gastroesophageal cancers Key Points Constipation is a major problem in residential care Early detection and
Managing constipation in residential care Amanda Lee Lecturer, Hull University ; PhD Candidate, Gastroesophageal cancers Key Points Constipation is a major problem in residential care Early detection and
ABDOMINAL PAIN, CHRONIC
 Introduction Incidence Aetiology Clinical Assessment Formulation Investigations Management Prognosis Conclusion References Introduction The generally accepted definition of this condition is three or more
Introduction Incidence Aetiology Clinical Assessment Formulation Investigations Management Prognosis Conclusion References Introduction The generally accepted definition of this condition is three or more
Diagnosis and Treatment of Irritable Bowel Syndrome
 Special Issue Diagnosis and Treatment of Irritable Bowel Syndrome Myung Gyu Choi, M.D. Department of Internal Medicine The Catholic University of Korea, College of Medicine Kangnam St. Mary's Hospital
Special Issue Diagnosis and Treatment of Irritable Bowel Syndrome Myung Gyu Choi, M.D. Department of Internal Medicine The Catholic University of Korea, College of Medicine Kangnam St. Mary's Hospital
Irritable Bowel Syndrome
 68 TH ANNUAL MCGILL REFRESHER COURSE FOR FAMILY PHYSICIANS 2017 Irritable Bowel Syndrome Gad Friedman, MDCM, FRCPC Jewish General Hospital DISCLOSURES I have no disclosures LEARNING OBJECTIVES 1. Review
68 TH ANNUAL MCGILL REFRESHER COURSE FOR FAMILY PHYSICIANS 2017 Irritable Bowel Syndrome Gad Friedman, MDCM, FRCPC Jewish General Hospital DISCLOSURES I have no disclosures LEARNING OBJECTIVES 1. Review
Chapter 31 Bowel Elimination
 Chapter 31 Bowel Elimination Defecation Defecation: the act of expelling feces from the body Peristalsis: rhythmic contractions of intestinal smooth muscle to facilitate defecation Gastrocolic reflex:
Chapter 31 Bowel Elimination Defecation Defecation: the act of expelling feces from the body Peristalsis: rhythmic contractions of intestinal smooth muscle to facilitate defecation Gastrocolic reflex:
IBS-D: What to Do When Typical Treatment Methods Fail
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including