Contemporary Management of Spinal Cord Injury
|
|
|
- Jesse Lee
- 6 years ago
- Views:
Transcription




1 Contemporary Management of Spinal Cord Injury Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery
2 Disclosures I have nothing to disclose
3 Spinal Cord Injury Spinal Cord Injury Basics What works What may work What doesn't work
4 Spinal Cord Injury 12,000 new cases in US/year 238,00 332,000 in US live with SCI 80% are male
5 Spinal Cord Injury Two peaks Age Age > years avg age at time of injury in geriatric population with SCI
6 Spinal Cord Injury Incomplete quadriplegia 41% Incomplete paraplegia 19% Complete paraplegia 18% Complete quadriplegia 12%
7 Spinal Cord Injury Estimated lifetime costs $1.1 million $4.6 million
8 Mechanism of Injury MVC is most common cause Falls second (common in elderly) GSW Sport related injuries
9 Mechanism of Injury Spinal injuries include: Fractures Ligamentous disruptions Combined Direct compression and injury to spinal cord
10 Pathophysiology
11 Pathophysiology
12 Pathophysiology
13 Pathophysiology

14 Secondary Injury
15 Pathophysiology
16 Treatment - overview No single pathway has been a successful target of pharmacologic intervention
17 Treatment - overview No single pathway has been a successful target of pharmacologic intervention Mainstay of treatment Attenuate Mitigate Prevent
18 Spinal Cord Injury Spinal Cord Injury Basics What works What may work What doesn't work
19 Spinal Cord Injury Spinal Cord Injury Basics What works What may work What doesn't work
20 What Works
21 Initial Management
22
23 Initial Management Airway for high SCI Above C5 Up to 65% with cervical SCI have resp dysfunction Avoid hypoxia Avoid hypotension
24 Initial Management Airway for high SCI Above C5 Up to 65% with cervical SCI have resp dysfunction Avoid hypoxia Avoid hypotension Neurogenic shock
25
26 Sympathectomy and loss of supraspinal control of sympathetic nervous system
27 Sympathectomy and loss of supraspinal control of sympathetic nervous system Unopposed parasympathetic activity and stimulation of vagus nerve

28 Sympathectomy and loss of supraspinal control of sympathetic nervous system Unopposed parasympathetic activity and stimulation of vagus nerve Hypotention and profound bradycardia and atrioventricular nodal block
29 Neurogenic Shock Lasts 1-3 weeks Fluid resuscitation to maintain euvolemia Pressors, inotropes, or combination No established recommendations
30 Neurogenic Shock Agent Alpha Activity Beta Activity Comments Norepinephrine Probably preferred Phenylephrine ++ None May worsen bradycardia Dopamine Low dose (3-10) + ++ May lead to diuresis High Dose (10-20) Epinephrine Rarely needed Dobutamine None +++ May cause hypotension
31 Neurogenic Shock Agent Alpha Activity Beta Activity Comments Norepinephrine Probably preferred Phenylephrine ++ None May worsen bradycardia Dopamine Low dose (3-10) + ++ May lead to diuresis High Dose (10-20) Epinephrine Rarely needed Dobutamine None +++ May cause hypotension
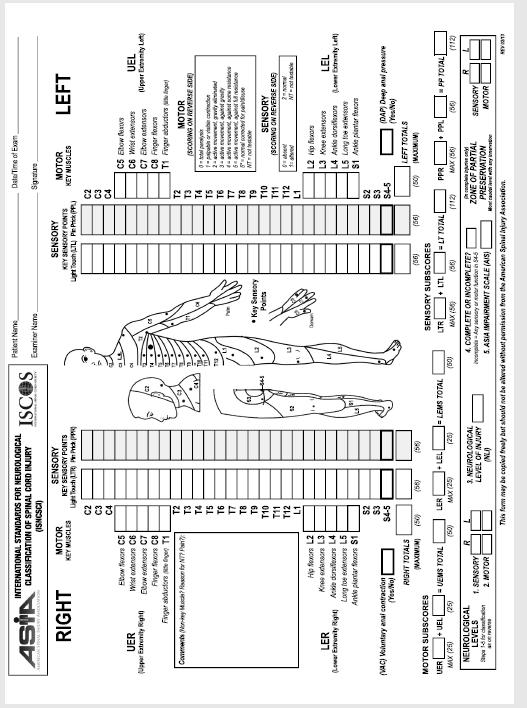
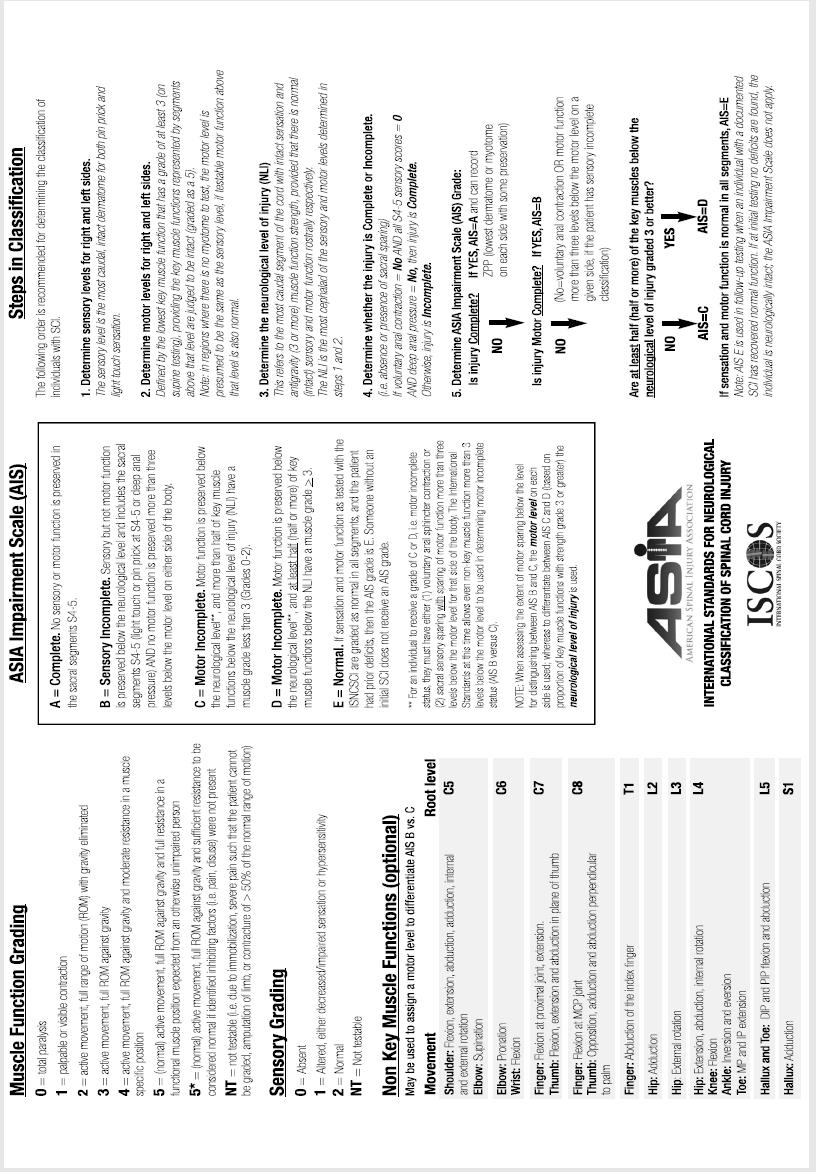
32 Initial Management Detailed neurological examination American Spinal Injury Association (ASIA)
33
34
35 What else Works
36 Surgical Management Goals Stabilize the spine Decompress the spinal canal Prevent further injury
37 Timing??

38 Timing of Stabilization Controversial Experimental evidence < 1 Hour
39 Timing of Stabilization How early is early? 8, 24, 72 hours? 5 Days? What is the endpoint? Improved neurological recovery? Improved morbidity?
40 Non-Neurological Benefits Strong evidence that early (< 72 hours) stabilization: pneumonia DVT LOS Medical Costs
41 What about Neurologic Recovery??
42 2012
43 2012 Cervical SCI Early decompression (<24 hours) 182 patients Late decompression ( 24 hours) 131 patients 1 Outcome change in ASIA grade at 6 months
44 2012 Early decompression (<24 hours) 19.8% showed 2 grade improvement 24.2% complications Late decompression ( 24 hours) 8.8% showed 2 grade improvement 30.5% complications
45 2012 Early decompression (<24 hours) 19.8% showed 2 grade improvement 24.2% complications Late decompression ( 24 hours) 8.8% showed 2 grade improvement 30.5% complications Early surgery OR 2.83 (1.10, 7.28)

46 2012 Decompression within 24 hours is safe and associated with improved neurologic outcomes
47
48 Existing evidence supports improved neurological recovery among cervical SCI patients undergoing early surgery
49 What Always Works
50 DVT Prophylaxis
51 DVT Prophylaxis Incidence of VTE 12% - 64% Accounts for 10% of deaths in first year
52 DVT Prophylaxis Mechanical compression should be implemented asap
53 DVT Prophylaxis Mechanical compression should be implemented asap Level I Recommendations: LMWH, rotating beds, or a combination Low dose heparin in combination with pneumatic compression stockings or electrical stimulation
54 DVT Prophylaxis Level II Recommendations: Early administration within 72 hours 3-month duration of prophylactic treatment Level II Recommendations: Vena cava filters not recommended for prophylaxis
55 What else Works Aggressive screening and treatment of infections Treatment of hyperglycemia Early nutrition Protection against pressure ulceration Transfer to SCI center
56 Spinal Cord Injury Spinal Cord Injury Basics What works What may work What doesn't work
57 What May Work
58 Cardiopulmonary Management Maintain MAP mm Hg For first 7 days Level III recommendations Based on case series and small studies No consensus on choice of agent
59 Cardiopulmonary Management Agent Alpha Activity Beta Activity Comments Norepinephrine Probably preferred Phenylephrine ++ None May worsen bradycardia Dopamine Low dose (3-10) + ++ May lead to diuresis High Dose (10-20) Epinephrine Rarely needed Dobutamine None +++ May cause hypotension
60 Hypothermia??
61 Mechanism Decreased metabolic rate -1C = -6 to 10% demand Secondary effects Apoptosis pathways Dampened neuro-excitatory pathways Regulated free-radical production Anti-inflammatory

62


63 Hypothermia and SCI C3 C4 fracture with SCI Cooled to 33.3 C immediately and for 48 hrs Steroids Immediate decompression

64 Walking again
65 2009

66 2009 Modest hypothermia : 32-34C Robust experimental studies demonstrate benefit Some clinical evidence demonstrates usefulness

67 August patient Nontraumatic SCI Cooled to 32 C for 24 hours Return of neurological function

68 1 patient Complete SCI Cooled Other interventions utilized Conclusions?
69 Hypothermia and SCI Animal studies Case reports Further studies needed

70 Spinal Cord Injury Spinal Cord Injury Basics What works What may work What doesn't work
71 What Doesn t Work Pharmacologic Therapy
72 What Doesn t Work Pharmacologic Therapy Steroids GM1 ganglioside Thyrotropin releasing hormone Nimodipine Gacyclidine (GK-11)
73 Steroids and Spinal Cord Injury NASCIS I Published in 1984 Prospective randomized Methylprednisolone Low dose vs. higher dose
74 Steroids and Spinal Cord Injury 1990 (follow-up 1992) NASCIS II Prospective randomized Methylprednisolone, naloxone, placebo for 24 hours
75 Steroids and Spinal Cord Injury Post hoc analysis NASCIS II Included 38% of study patients Improvement in motor and sensory score if given within 8 hours
76 Steroids and Spinal Cord Injury 1997 NASCIS III Prospective randomized 24 hour steroids vs. 48 hour steroids vs. 48 hour tirilazad
77 Steroids and Spinal Cord Injury Post hoc analysis NASCIS III Included 30% of study patients Improvement in motor score if given between 3 and 8 hours for 48 hours
78 Steroid Summary No difference in initial study outcomes Post hoc analysis Not clinically significant Side effects There is no convincing evidence to support the use of methylprednisolone in acute SCI
79 Guidelines for the Management of Acute SCI MP is not recommended No Class I or Class II evidence supporting its use Class I, II, and III evidence demonstrates harmful side effects of high dose MP
80 On the horizon? Stem Cells New Technologies Modern wheelchairs Computer adaptations Electronic aids to daily living Electrical stimulation devices Robotic gait training





81
82 Spinal Cord Injury What works ATLS, early surgery, DVT proph, supp care What may work Hypertension, hypothermia What doesn t work Pharmacologic therapy (steroids)
83 Spinal Cord Injury What works ATLS, early surgery, DVT proph, supp care What may work Hypertension, hypothermia What doesn t work Pharmacologic therapy (steroids)

84
ว ทยาการความก าวหน าในการร กษาผ ป วยบาดเจ บ กระด กส นหล งและไขส นหล ง. Piyawat Bintachitt, MD.
 ว ทยาการความก าวหน าในการร กษาผ ป วยบาดเจ บ กระด กส นหล งและไขส นหล ง Piyawat Bintachitt, MD. Thank you Outline Pathophysiology Neurological classification Imaging Airway management Cardiovascular management
ว ทยาการความก าวหน าในการร กษาผ ป วยบาดเจ บ กระด กส นหล งและไขส นหล ง Piyawat Bintachitt, MD. Thank you Outline Pathophysiology Neurological classification Imaging Airway management Cardiovascular management
Traumatic Spinal Cord Injury. 39 th CANP Annual Educational Conference March 18 th, :00pm-6:15pm Carl Wherry, ACNP-bc Amanda Severson, ACNP-bc
 Traumatic Spinal Cord Injury 39 th CANP Annual Educational Conference March 18 th, 2016 5:00pm-6:15pm Carl Wherry, ACNP-bc Amanda Severson, ACNP-bc Disclosures No conflicts of interest to disclose. Introduction
Traumatic Spinal Cord Injury 39 th CANP Annual Educational Conference March 18 th, 2016 5:00pm-6:15pm Carl Wherry, ACNP-bc Amanda Severson, ACNP-bc Disclosures No conflicts of interest to disclose. Introduction
Acute Care of Spinal Cord Injury. Meghan Smith, RN, PA-C
 Acute Care of Spinal Cord Injury Meghan Smith, RN, PA-C Physician Assistant, Neuro Surgical, Trauma Services, Intermountain Medical Center, Intermountain Healthcare; Salt Lake City, Utah Objectives: Discuss
Acute Care of Spinal Cord Injury Meghan Smith, RN, PA-C Physician Assistant, Neuro Surgical, Trauma Services, Intermountain Medical Center, Intermountain Healthcare; Salt Lake City, Utah Objectives: Discuss
Neuroprotection. Key Points. What is neuroprotection? Secondary injury. Neuroprotection
 Authors: SCIRE Community Team Reviewed by: Chris S. Bailey MD, FRCSC, MSc Last updated: Jan 22, 2018 describes a wide range of treatments that aim to protect the spinal cord from further damage in the
Authors: SCIRE Community Team Reviewed by: Chris S. Bailey MD, FRCSC, MSc Last updated: Jan 22, 2018 describes a wide range of treatments that aim to protect the spinal cord from further damage in the
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
Management of Spinal Cord Injury (in Cri5cal Care by an Anaesthe5st)
") Management of Spinal Cord Injury (in Cri5cal Care by an Anaesthe5st) Dr Ma& Wiles Consultant in Neuroanaesthesia & Neurocri5cal Care Sheffield Teaching Hospitals NHS Founda5on Trust @STHJournalClub h&p://sthjournalclub.wordpress.com/
Management of Spinal Cord Injury (in Cri5cal Care by an Anaesthe5st) Dr Ma& Wiles Consultant in Neuroanaesthesia & Neurocri5cal Care Sheffield Teaching Hospitals NHS Founda5on Trust @STHJournalClub h&p://sthjournalclub.wordpress.com/
Spinal injury. Structure of the spine
 Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
SPINAL CORD INJURIES DR. F. DE V. THERON MUELMED/PAH HOSPITAL SPINAL UNIT 2012
 SPINAL CORD INJURIES DR. F. DE V. THERON MUELMED/PAH HOSPITAL SPINAL UNIT 2012 INTRODUCTION Mortal condition recognised since antiquity First described in the Edwin Smith papyrus 2500BC An ailment not
SPINAL CORD INJURIES DR. F. DE V. THERON MUELMED/PAH HOSPITAL SPINAL UNIT 2012 INTRODUCTION Mortal condition recognised since antiquity First described in the Edwin Smith papyrus 2500BC An ailment not
Declaring Brain Death. Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery
 Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
American Board of Physical Medicine & Rehabilitation. Part I Curriculum & Weights
 American Board of Physical Medicine & Rehabilitation Part I Curriculum & Weights Neurologic Disorders 30% Stroke Spinal Cord Injury Traumatic Brain Injury Neuropathies a) Mononeuropathies b) Polyneuropathies
American Board of Physical Medicine & Rehabilitation Part I Curriculum & Weights Neurologic Disorders 30% Stroke Spinal Cord Injury Traumatic Brain Injury Neuropathies a) Mononeuropathies b) Polyneuropathies
INTRAOPERATIVE MANAGEMENT OF FREE FLAPS SURVEY
 INTRAOPERATIVE MANAGEMENT OF FREE FLAPS SURVEY Dear Esteemed Colleague, You are being contacted at the e mail address identified in your professional organization directory to participate in this important
INTRAOPERATIVE MANAGEMENT OF FREE FLAPS SURVEY Dear Esteemed Colleague, You are being contacted at the e mail address identified in your professional organization directory to participate in this important
Update on early management of acute spinal cord injuries. Mr Jonathon L Richards Orthopaedic & Spinal surgeon
 Update on early management of acute spinal cord injuries Mr Jonathon L Richards Orthopaedic & Spinal surgeon Overview: Aetiology/Cost Pathophysiology Early surgical intervention Emerging therapies Steroids
Update on early management of acute spinal cord injuries Mr Jonathon L Richards Orthopaedic & Spinal surgeon Overview: Aetiology/Cost Pathophysiology Early surgical intervention Emerging therapies Steroids
Review of clinical trials of neuroprotection in acute spinal cord injury
 Neurosurg Focus 6 (1):Article 8, 1999 Review of clinical trials of neuroprotection in acute spinal cord injury Charles H. Tator, M.D., Ph.D., and Michael G. Fehlings, M.D., Ph.D. Division of Neurosurgery,
Neurosurg Focus 6 (1):Article 8, 1999 Review of clinical trials of neuroprotection in acute spinal cord injury Charles H. Tator, M.D., Ph.D., and Michael G. Fehlings, M.D., Ph.D. Division of Neurosurgery,
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
EMT. Chapter 10 Review
 EMT Chapter 10 Review 1. The term shock is MOST accurately defined as: A. a decreased supply of oxygen to the brain. B. cardiovascular collapse leading to inadequate perfusion. C. decreased circulation
EMT Chapter 10 Review 1. The term shock is MOST accurately defined as: A. a decreased supply of oxygen to the brain. B. cardiovascular collapse leading to inadequate perfusion. C. decreased circulation
Paraplegia: Exercise and Health Considerations. By: Juli and Trina
 Paraplegia: Exercise and Health Considerations By: Juli and Trina What is paraplegia? Paraplegia is impairment of motor and/or sensory function to the lower extremities, and sometimes the lower trunk Complete
Paraplegia: Exercise and Health Considerations By: Juli and Trina What is paraplegia? Paraplegia is impairment of motor and/or sensory function to the lower extremities, and sometimes the lower trunk Complete
Pulmonary Rehabilitation in Acute Spinal Cord Injury. Jatuporn Jatutawanit Physical therapist, Physical therapy unit, Prince of songkla university
 Pulmonary Rehabilitation in Acute Spinal Cord Injury Jatuporn Jatutawanit Physical therapist, Physical therapy unit, Prince of songkla university Causes of spinal cord injury Traumatic injury Motor vehicle
Pulmonary Rehabilitation in Acute Spinal Cord Injury Jatuporn Jatutawanit Physical therapist, Physical therapy unit, Prince of songkla university Causes of spinal cord injury Traumatic injury Motor vehicle
RESPIRATORY COMPLICATIONS AFTER SCI
 SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question.
 EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Acute to Rehab Spinal Cord Injuries Anna Brown CNC, Certificate SCI Nursing, Grad Dip Rehabilitation Studies, La Trobe
 Acute to Rehab Spinal Cord Injuries Anna Brown CNC, Certificate SCI Nursing, Grad Dip Rehabilitation Studies, La Trobe Victorian Spinal Cord Service Austin Health SCI Acute to Rehab Let the rollercoaster
Acute to Rehab Spinal Cord Injuries Anna Brown CNC, Certificate SCI Nursing, Grad Dip Rehabilitation Studies, La Trobe Victorian Spinal Cord Service Austin Health SCI Acute to Rehab Let the rollercoaster
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Intra-operative neurologic injuries: Avoidance and prompt response
 Intra-operative neurologic injuries: Avoidance and prompt response James S. Harrop MD, FACS Professor Neurological and Orthopedic Surgery Director, Division of Spine and Peripheral Nerve Surgery Nsurg
Intra-operative neurologic injuries: Avoidance and prompt response James S. Harrop MD, FACS Professor Neurological and Orthopedic Surgery Director, Division of Spine and Peripheral Nerve Surgery Nsurg
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Chapter 39 Trauma in the Elderly
 Chapter 39 Trauma in the Elderly Episode Overview 1) 5 Risk Factors for falls in the elderly? 2) What anatomic and physiologic changes in the elderly patient are important for the management of trauma
Chapter 39 Trauma in the Elderly Episode Overview 1) 5 Risk Factors for falls in the elderly? 2) What anatomic and physiologic changes in the elderly patient are important for the management of trauma
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Autonomic Division of NS
 Autonomic Division of NS Compare and contrast the structures of the sympathetic and the parasympathetic divisions, including functions and neurotransmitters. Show the levels of integration in the ANS,
Autonomic Division of NS Compare and contrast the structures of the sympathetic and the parasympathetic divisions, including functions and neurotransmitters. Show the levels of integration in the ANS,
Chapter 32. Injuries to the Spine by Pearson Education, Inc. Upper Saddle River, New Jersey
 Chapter Injuries to the Spine Topics Anatomy and physiology of the spine Spinal injuries Guidelines for immobilization Special considerations Enrichment Introduction Injuries to the spine are among the
Chapter Injuries to the Spine Topics Anatomy and physiology of the spine Spinal injuries Guidelines for immobilization Special considerations Enrichment Introduction Injuries to the spine are among the
John E. O Toole, Marjorie C. Wang, and Michael G. Kaiser
 Hypothermia and Human Spinal Cord Injury: Updated Position Statement and Evidence Based Recommendations from the AANS/CNS Joint Section on Disorders of the Spine Peripheral Nerves John E. O Toole, Marjorie
Hypothermia and Human Spinal Cord Injury: Updated Position Statement and Evidence Based Recommendations from the AANS/CNS Joint Section on Disorders of the Spine Peripheral Nerves John E. O Toole, Marjorie
Acute spinal cord injury
 Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
What is a spinal cord injury?
 Spinal Cord Injury What is a spinal cord injury? A spinal cord injury (SCI) is when the spinal cord is damaged Such damage causes 2 things: - loss or change of movement (paralysis) - loss or change of
Spinal Cord Injury What is a spinal cord injury? A spinal cord injury (SCI) is when the spinal cord is damaged Such damage causes 2 things: - loss or change of movement (paralysis) - loss or change of
11. Spinal cord injury
 11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine
11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine
Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc. Copyright 2014, 2011, 2006 by Saunders, an imprint of Elsevier, Inc.
 Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc 1 Spinal Cord Injury Results from fracture and/or dislocation of vertebrae // Compresses, stretches, or tears spinal cord Cervical
Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc 1 Spinal Cord Injury Results from fracture and/or dislocation of vertebrae // Compresses, stretches, or tears spinal cord Cervical
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
Shepherd Center: A Catastrophic Care Hospital. The Jane Woodruff Pavilion
 Shepherd Center: A Catastrophic Care Hospital The Jane Woodruff Pavilion Acute Management of SCI & Prevention of Secondary Complications Joycelyn Craig, BSN, RN, CRRN SCI Nurse Education Manager FACTS
Shepherd Center: A Catastrophic Care Hospital The Jane Woodruff Pavilion Acute Management of SCI & Prevention of Secondary Complications Joycelyn Craig, BSN, RN, CRRN SCI Nurse Education Manager FACTS
Wounds and Injuries of the Spinal Column and Cord
 Wounds and Injuries of the Spinal Column and Cord Chapter 20 Wounds and Injuries of the Spinal Column and Cord Introduction Combat injuries of the spinal column, with or without associated spinal cord
Wounds and Injuries of the Spinal Column and Cord Chapter 20 Wounds and Injuries of the Spinal Column and Cord Introduction Combat injuries of the spinal column, with or without associated spinal cord
Misunderstandings of Venous thromboembolism prophylaxis
 Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Dr Brigitta Brandner UCLH
 Dr Brigitta Brandner UCLH 2.5% paraplegia/paraparesis (EUROSTAR) Some studies up to 8% Immediate, recurrent and delayed 37% deficits are delayed: present 13 hours 91 days post op >50% will resolve with
Dr Brigitta Brandner UCLH 2.5% paraplegia/paraparesis (EUROSTAR) Some studies up to 8% Immediate, recurrent and delayed 37% deficits are delayed: present 13 hours 91 days post op >50% will resolve with
Predicting Venous Thromboembolic Complications following Neurosurgical Procedures
 1 Predicting Venous Thromboembolic Complications following Neurosurgical Procedures David Dornbos III, Varun Shah, Blake Priddy, Victoria Schunemann, Ciarán Powers Venous Thromboembolic (VTE) Complications
1 Predicting Venous Thromboembolic Complications following Neurosurgical Procedures David Dornbos III, Varun Shah, Blake Priddy, Victoria Schunemann, Ciarán Powers Venous Thromboembolic (VTE) Complications
Trauma Echo PVA. Improving Spinal Cord Injury Acute Management
 Improving Spinal Cord Injury Acute Management William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies Trauma Echo PVA 86 yo PVA
Improving Spinal Cord Injury Acute Management William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies Trauma Echo PVA 86 yo PVA
Medical Patients: A Population at Risk
 Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Integrated Cardiopulmonary Pharmacology Third Edition
 Integrated Cardiopulmonary Pharmacology Third Edition Chapter 3 Pharmacology of the Autonomic Nervous System Multimedia Directory Slide 19 Slide 37 Slide 38 Slide 39 Slide 40 Slide 41 Slide 42 Slide 43
Integrated Cardiopulmonary Pharmacology Third Edition Chapter 3 Pharmacology of the Autonomic Nervous System Multimedia Directory Slide 19 Slide 37 Slide 38 Slide 39 Slide 40 Slide 41 Slide 42 Slide 43
Spinal Trauma. General Rehabilitation of Patient with Spinal Trauma. Common Spinal Injuries. Important Anatomical Structures at each Vertebral Level
 Asian Association for Dynamic Osteosynthesis Workshop on Management of Spinal Trauma 22 April 2007 (Sunday) Orthopaedic Learning Centre, PWH, Shatin, Hong Kong General Rehabilitation of Patient with Spinal
Asian Association for Dynamic Osteosynthesis Workshop on Management of Spinal Trauma 22 April 2007 (Sunday) Orthopaedic Learning Centre, PWH, Shatin, Hong Kong General Rehabilitation of Patient with Spinal
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
Spinal Cord Injury. 1Demographics. 1.1 Incidence. 1.2 Causes. 2Neurological Level and Severity. 2.1 Level of Injury
 Spinal Cord Injury 1Demographics 1.1 Incidence Varies from 29-50 per million population per year in USA to 9 per million population per year in Denmark. Mortality is decreasing improvement in EMS care
Spinal Cord Injury 1Demographics 1.1 Incidence Varies from 29-50 per million population per year in USA to 9 per million population per year in Denmark. Mortality is decreasing improvement in EMS care
Sir William Asher ANATOMY
 SPINAL CORD INJURY BASICS RELATED TO LIFE CARE PLANNING Lesson 1 Sir William Asher Picture the pathetic patient lying long abed, the urine leaking from his distended bladder, the lime draining from his
SPINAL CORD INJURY BASICS RELATED TO LIFE CARE PLANNING Lesson 1 Sir William Asher Picture the pathetic patient lying long abed, the urine leaking from his distended bladder, the lime draining from his
THROMBOPROPHYLAXIS: NON-ORTHOPEDIC SURGERY
 THROMBOPROPHYLAXIS: NON-ORTHOPEDIC SURGERY OBJECTIVE: To outline a practical approach for the prevention of venous thromboembolism (VTE) in patients undergoing non-orthopedic surgery. BACKGROUND: VTE is
THROMBOPROPHYLAXIS: NON-ORTHOPEDIC SURGERY OBJECTIVE: To outline a practical approach for the prevention of venous thromboembolism (VTE) in patients undergoing non-orthopedic surgery. BACKGROUND: VTE is
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Role of methyleprednisolone succinate in the management of acute spinal cord injury
 Original Article Role of methyleprednisolone succinate in the management of acute spinal cord injury NK Karn, BP Shrestha, GP Khanal, R Rijal, P Chaudhary, IP Mahato, N Das B.P. Koirala Institute of Health
Original Article Role of methyleprednisolone succinate in the management of acute spinal cord injury NK Karn, BP Shrestha, GP Khanal, R Rijal, P Chaudhary, IP Mahato, N Das B.P. Koirala Institute of Health
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
SPINE EVALUATION AND CLEARANCE Basic Principles
 SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
Competencies and Objectives
 Competencies and Objectives Chapter 1 EMS Systems Preparatory Emergency Medical Services (EMS) Systems Research Public Health Chapter 2 Workforce Safety and Wellness Medicine Infectious Diseases Preparatory
Competencies and Objectives Chapter 1 EMS Systems Preparatory Emergency Medical Services (EMS) Systems Research Public Health Chapter 2 Workforce Safety and Wellness Medicine Infectious Diseases Preparatory
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Bolus (Push Dose) Pressors: Good Idea or a bit Much?
 Pressors: Good Idea or a bit Much?") Bolus (Push Dose) Pressors: Good Idea or a bit Much? Robert Katzer MD MBA FACEP FAEMS Associate Professor, Emergency Medicine University of California, Irvine Pressors: Which Ones Are Out There, What Do
Bolus (Push Dose) Pressors: Good Idea or a bit Much? Robert Katzer MD MBA FACEP FAEMS Associate Professor, Emergency Medicine University of California, Irvine Pressors: Which Ones Are Out There, What Do
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Ten Second Step Test" as a New Quantifiable Parameter of Cervical Myelopathy. Spine January 1, 2009; Volume 34; Issue 1; pp 82-86
 Ten Second Step Test" as a New Quantifiable Parameter of Cervical Myelopathy 1 Spine January 1, 2009; Volume 34; Issue 1; pp 82-86 Yukawa, Yasutsugu; Kato, Fumihiko; Ito, Keigo; Horie, Yumiko; Nakashima,
Ten Second Step Test" as a New Quantifiable Parameter of Cervical Myelopathy 1 Spine January 1, 2009; Volume 34; Issue 1; pp 82-86 Yukawa, Yasutsugu; Kato, Fumihiko; Ito, Keigo; Horie, Yumiko; Nakashima,
DENOMINATOR: All surgical patients aged 18 years and older undergoing procedures for which VTE prophylaxis is indicated in all patients
 Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES:
Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES:
NICE Guidance: Venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital 1
 in patients admitted to hospital 1") The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS
 EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS Samuel Z. Goldhaber, MD Director, VTE Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS Samuel Z. Goldhaber, MD Director, VTE Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Pharmacological Management of Acute Spinal Cord Injury
 SUPPLEMENT TO JAPI may 2012 VOL. 60 13 Pharmacological Management of Acute Spinal Cord Injury Alok Sharma * Introduction Medical care for acute spinal cord injury has advanced greatly in the last 50 years.
SUPPLEMENT TO JAPI may 2012 VOL. 60 13 Pharmacological Management of Acute Spinal Cord Injury Alok Sharma * Introduction Medical care for acute spinal cord injury has advanced greatly in the last 50 years.
CPT only copyright 2014 American Medical Association. All rights reserved. 12/23/2014 Page 66 of 593
 Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2015 PQRS OPTIONS FOR INDIVIDUAL MEASURES:
Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2015 PQRS OPTIONS FOR INDIVIDUAL MEASURES:
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
QUIZ 2. Tuesday, April 6, 2004
 Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Dr Richard Pugh Consultant Anaesthetics/ Intensive Care Medicine May 2010
 Dr Richard Pugh Consultant Anaesthetics/ Intensive Care Medicine May 2010 The brainstem: Midbrain, pons, medulla Consciousness Cardiovascular and respiratory regulation Sleep- wake cycle Integration of
Dr Richard Pugh Consultant Anaesthetics/ Intensive Care Medicine May 2010 The brainstem: Midbrain, pons, medulla Consciousness Cardiovascular and respiratory regulation Sleep- wake cycle Integration of
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES:
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Northwest Community EMS System Continuing Education Class Credit Questions for October 2014 Spine Motion Restriction (Didactic)
") Northwest Community EMS System Continuing Education Class Credit Questions for October 2014 Spine Motion Restriction (Didactic) Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete
Northwest Community EMS System Continuing Education Class Credit Questions for October 2014 Spine Motion Restriction (Didactic) Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
Audit of perioperative management of patients with fracture neck of femur
 Audit of perioperative management of patients with fracture neck of femur *M Dissanayake 1, N Wijesuriya 2 Registrar in Anaesthesia 1, Consultant Anaesthetist 2, North Colombo Teaching Hospital, Ragama,
Audit of perioperative management of patients with fracture neck of femur *M Dissanayake 1, N Wijesuriya 2 Registrar in Anaesthesia 1, Consultant Anaesthetist 2, North Colombo Teaching Hospital, Ragama,
Top Ten Reasons For Failure To Prevent Postoperative Thrombosis
 Top Ten Reasons For Failure To Prevent Postoperative Thrombosis Joseph A. Caprini, MD, MS, FACS, RVT, FACCWS Louis W. Biegler Chair of Surgery NorthShore University HealthSystem, Evanston, IL Clinical
Top Ten Reasons For Failure To Prevent Postoperative Thrombosis Joseph A. Caprini, MD, MS, FACS, RVT, FACCWS Louis W. Biegler Chair of Surgery NorthShore University HealthSystem, Evanston, IL Clinical
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Anticoagulation for prevention of venous thromboembolism
 Anticoagulation for prevention of venous thromboembolism Original article by: Michael Tam Note: updated in June 2009 with the eighth edition (from the seventh) evidence-based clinical practice guidelines
Anticoagulation for prevention of venous thromboembolism Original article by: Michael Tam Note: updated in June 2009 with the eighth edition (from the seventh) evidence-based clinical practice guidelines
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Intravenous Infusions
 Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Looking for sepsis. Sepsis: Update. Prevalence of High Profile Dzs. Screening and risk stratification. Mortality of High Profile Diseases
 Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Index. Note: Page numbers of article titles are in bold face type.
 Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Spinal Cord Injury Robert Morgan, MD
 Spinal Cord Injury Robert Morgan, MD Original Author: Mitch Harris, MD; March 2004 New Author: Michael J. Vives, MD; Revised January 2006 Updated Author: Robert Morgan, MD; Revised November 2010 Overview
Spinal Cord Injury Robert Morgan, MD Original Author: Mitch Harris, MD; March 2004 New Author: Michael J. Vives, MD; Revised January 2006 Updated Author: Robert Morgan, MD; Revised November 2010 Overview
droxidopa (Northera )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not