APPROACH TO HEME/ONC EMERGENCIES. By Kashif Khan (PGY-3)
|
|
|
- Erik Butler
- 5 years ago
- Views:
Transcription


1 APPROACH TO HEME/ONC EMERGENCIES By Kashif Khan (PGY-3)
2 LEARNING OBJECTIVE Identify commonly encountered Hematological and Oncological emergencies Order appropriate labs/radiological tests Initiate timely treatment Early sub-specialty consultations
3 WHAT IS AN ONCOLOGICAL EMERGENCY A clinical condition resulting from a metabolic, neurologic, cardiovascular, hematologic, and/or infectious change caused by cancer or its treatment that requires immediate intervention to prevent loss of life or quality of life.

4
5 CASE - 1
6 A 60 yo M with PMH of HTN, GERD, depression, who presents with 1 month history of progressively worsening generalized fatigue, weakness, and feeling unwell. ROS: Positive for dry cough, night sweats, 20 lb unintentional wt loss in last 3 months Vitals: HR 110/m, otherwise stable Being an excellent new intern, you perform a full physical and find bilateral cervical and supraclavicular lymphadenopathy and palpable hepatosplenomegaly. Remainder of the exam was unremarkable. Labs: CBC/diff: WBC 15k H/h 7.9/25 Plt 75k Diff: 85%L 10%N 5%M RFP: Na138, K 5.6, Cl 105, Bicarb 22, BUN 35, Cr 1.9(baseline Cr 0.8) LDH 1205, uric acid 12.6, calcium 7.0, phosphorus 6.5, albumin 3.2
7 TUMOR LYSIS SYNDROME

8 TUMOR LYSIS SYNDROME (TLS) TLS is the result of a massive and abrupt release of cellular contents into the bloodstream after rapid lysis of malignant cells K + Ca 2+ K + Uric Acid PO 4 CaPO 4 Ca 2+
9 TUMOR LYSIS SYNDROME (TLS) Seen in high grade liquid tumors like leukemia with leukocytosis, high grade lymphomas, and some solid tumors like small cell lung ca Clinical Features: weakness, arrhythmias, paralysis, acute renal failure, tetany, altered mental status, seizures Diagnosis: Laboratory o 2 laboratory abnormalities OR o 25% change in 2 values from baseline value HyperKalemia HyperUricemia HyperPhosphatemia HypoCalcemia Clinical o Laboratory diagnosis + end organ damage
10 TUMOR LYSIS SYNDROME (TLS) Treatment: Aggressive IV Fluids &/or diuresis (Most important) Manage electrolyte abnormalities Rasburicase (Check G-6PD before!) Allopurinol (Does not decrease uric acid) HD Prevention: Fluids, Allopurinol, Rasburicase
11 CASE - 2
12 A middle aged F with HTN, DM, metastatic breast ca, presents with worsening back pain x 2 weeks. Developed after lifting boxes while moving. More recently has been feeling some RLE numbness and worsening pain. ROS: Denies fevers/chills, weakness, loss of sensation, bowel/bladder incontinence Oncologic history: diagnosed with metastatic breast ca 3 yrs ago, last PET-CT 2 months ago showed stable/shrinking osseous mets in L scapula, multiple ribs, thoracic spine (T8), and R femur. O/E: severe pain on palpation of mid-thoracic spine, strength and sensation intact throughout, normal reflexes, no saddle anesthesia, normal rectal tone Labs: Unremarkable
13 MALIGNANT SPINAL CORD COMPRESSION

14 SPINAL CORD COMPRESSION

15 SPINAL CORD COMPRESSION Majority from: Breast Lung Prostate Lymphoma Myeloma About 6-10% of patients with cancer Thoracic spine (up to 70%)
16 SPINAL CORD COMPRESSION Presentation Pain may not always be present or may be underwhelming Weakness Sensory deficits: numbness, paresthesias Cauda equina syndrome: saddle anesthesia, bowel/ bladder dysfunction, hyporeflexia
17 SPINAL CORD COMPRESSION Obtain a good history and neurologic exam MRI (CT Myelography) Steroids: dexamethasone 10mg IV STAT then 4mg q6 Time is money! ortho/ neurosurgery, radiation oncology Pain control Primary determinant of the efficacy of therapy is the patient's neurologic status at time treatment
18 CASE - 3
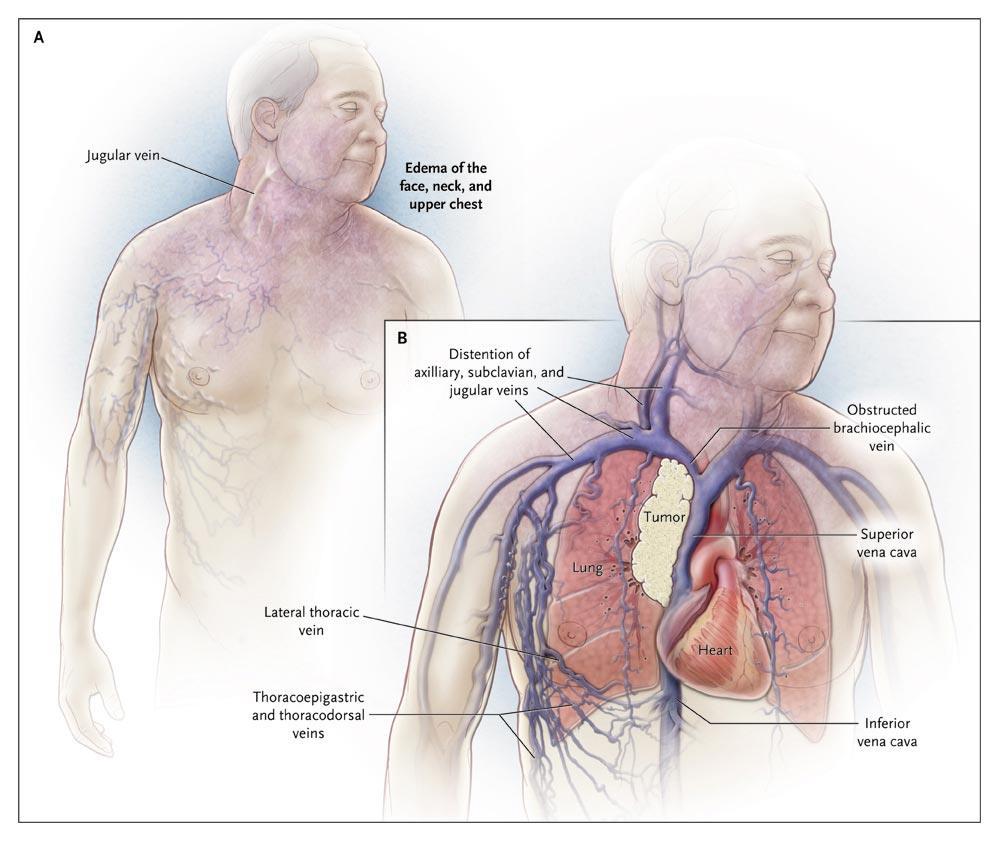
19 75 yo M, heavy smoker, presents with 4 weeks of SOB, worsening non-productive cough, and 20 lb weight loss. Developed neck swelling last week, which worsens on bending forwards. ROS - negative Vitals: Stable O/E: R mid-lung crackles, no wheezing/stridor, swelling of neck and right upper extremity, distension of superficial anterior chest and neck veins, no focal neuro deficits Labs: unremarkable


20

21
22 SUPERIOR VENA CAVA SYNDROME
23
24 SUPERIOR VENA CAVA SYNDROME (SVC) Most cases are not a true emergency Majority of cases are due to Lung Ca or NHL (intrathoracic malignancies) Dyspnea (most common). Facial edema, arm edema, distended veins, facial plethora, cough, airway etc. Diagnosis: o CT/ MRI o Histological Dx
25 SUPERIOR VENA CAVA SYNDROME (SVC) Treat underlying cancer! Endovascular stents/ Radiotherapy Supportive care: Head elevation, Diuretics Avoid high volume fluid infusion through upper extremities Anticoagulation Steroids o Severe Airway Obstruction o Lymphoma
26 CASE - 4
27 55Y F with AML presents with profound fatigue and 1 week of SOB. Accompanying family members report report she initially complained of a headache and dizziness, and since then has started acting confused and been more somnolent. Vitals: T:100.6, PR: 115/m, BP: 110/76, RR: 26/m, 80%RA Pertinent exam: A&Ox1 (wrong date and location), confused, strength and sensation intact, ataxic gait, bilateral lung crackles Labs: CBC: WBC 88K with 78% blasts, H/h 10/30 Plt 3k RFP:

28
29 LEUKOSTASIS Increased blood viscosity impedes blood flow, and local hypoxemia is worsened by high metabolic activity of cells and cytokine release Symptoms: (CNS/Eyes/Lungs) Pulmonary: hypoxia, interstitial/alveolar infiltrates Neurological: headache, dizziness, ataxia, confusion, somnolence, blurry vision Management: Rapid cytoreduction with chemotherapy Consider hydroxyurea or leukapheresis if unable to give chemo

30 LEUKOSTASIS WBC counts (X 10 9 /L) as indication for leukapheresis inhyperleukocytosis Piccirillo N, Laurenti L, Chiusolo P, et al. Reliability of leukostasis grading score to identify patients with high-risk hyperleukocytosis. Am J Hematol.2009;84(6):
31 CASE - 5
32 A 70 yo M with metastatic colon ca (finished cycle #3 FOLFOX ten days ago), who presents with fevers for 2 days at home. He states he checked his temperature at home and it has ranged from 99 to 102 F. ROS: Unremarkable Vitals: T: 38.7 o C, PR: 105/m, BP: 115/75, RR: 16/m,SP02 97%RA Exam: Mild oral mucositis, Mediport c/d/i, lungs clear, abdominal exam benign, otherwise no focal findings Labs: CBC/diff: WBC 2.0k H/h 8.5/28 Plt 85k Diff: 68%L 20%N 9%M 3%E RFP: WNL

33 FEBRILE NEUTROPENIA
34 FEBRILE NEUTROPENIA Infection in a neutropenic patient is an emergency Pathogenesis: Breeches in host defenses (breakdown of mucosal barriers) Immune system suppression Majority of cases of neutropenic fever thought to be caused by bloodstream seeding from GI tract flora Infectious source: 30%.
35 FEBRILE NEUTROPENIA Diagnosis: ANC<500 or ANC<1000 with expected nadir <500 over next 48 hours + T: 38 o C for >1 hour or T>38.3 o C once Next Steps: Is patient HDS? Stable for floor? Examine patient: any localizing symptoms? Any role for imaging? Cultures STAT (2 sets bld cx peripheral, culture from lines or ports, sputum or stool cx/c Diff or wound cx as indicated), UA, UCx, CXR Antibiotics (30-60min)
36 FEBRILE NEUTROPENIA Clinical Scenario Medication

37 FEBRILE NEUTROPENIA LOW RISK PATIENTS Certain low-risk patients can be treated at home with PO antibiotics (typically Ciprofloxacin + Augmentin) after initial IV dose and brief observation IDSA: anticipated neutropenia 7d, clinically stable, ANC > 100, and no medical comorbidities ASCO: MASCC score 21
38 MALIGNANT PERICARDIAL EFFUSION

39
40

41
42 MALIGNANT PERICARDIAL EFFUSION Can be related to cancer OR chemo/rt/infection/autoimmune Clinical manifestations Dyspnea, cough, Chest pain, orthopnea, palpitations. Exam findings: Beck s triad (JVD, hypotension, decreased heart sounds), narrow pulse pressure, pulsus paradoxus Treatment: Small/moderate effusions are usually asymptomatic and do not require urgent treatment Acute management: drainage with pericardiocentesis Prevention of re-accumulation: drainage catheter, pericardial window Treat underlying cancer
43 ACUTE CHEST SYNDROME
44 ACUTE CHEST SYNDROME Vaso-occlusive crises of pulmonary vasculature in patients with sickle cell anemia. Leading cause of death in SCD. New radio-density on CXR AND any one (T >38.5 O C, >2% drop in SpO 2, CP, cough, wheezing, rales, tachypnea) Maintain high suspicion, as some may develop ACS within 48-72hours after initial pain episode!
45 ACUTE CHEST SYNDROME Don t Forget other D/D Treatment: T&S, adequate pain control, IV access, fluids, oxygen, incentive spirometry, antibiotics, VTE prophylaxis, hematology consult. Consider simple Vs exchange transfusion & MICU transfer Can use simple transfusion to bridge to exchange transfusion while waiting for MICU bed (does not remove HgbS)
46 OTHER TIPS
47 Primary Oncologist? Date of last chemo? (Check on EMR IV chemo) What was their last chemo? (know your acronyms) Did they get any medications with chemo? (G-CSF) What is their previous oncologic course? Access for Chemo? (mediport, PICC?) Sickle cell crises: check care path in portal and OARRS Inform primary oncologist of patient s admission
48 REFERENCES Wilson FP et al. Onco-nephrology: tumor lysis syndrome. Clin J Am Soc Nephrol Oct;7(10): [PMID: ] McCurdy MT et al. Oncologic emergencies. Crit Care Med Jul;40(7): [PMID: ] Freifeld AG et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 Update by the Infectious Diseases Society of America. Clin Infect Dis Feb 15;52(4): [PMID: ] Chen KN, Xu SF, Gu ZD, et al. Surgical treatment of complex malignant anterior mediastinal tumors invading the superior vena cava. World J Surg 2006; 30:162 Wilson LD, Detterbeck FC, Yahalom J. Clinical practice. Superior vena cava syndrome with malignant causes. N Engl J Med 2007; 356:1862 Symposium on neoplastic hematology and medical oncology - Emergencies in Hematology and Oncology. Mayo Clinic 2017 Savage P, Sharkey R, Kua T, et al. Clinical characteristics and outcomes for patients with an initial emergency presentation of malignancy: a 15 month audit of patient level data. Cancer Epidemiol. 2015;39(1):86-90
49 THANK YOU
It s Not A Tumor! Oncologic Emergencies
 It s Not A Tumor! Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator Department of Emergency Medicine Harbor-UCLA Medical Center Increasing
It s Not A Tumor! Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator Department of Emergency Medicine Harbor-UCLA Medical Center Increasing
Educational Session: Oncology Emergencies
 Educational Session: Oncology Emergencies Diane M. Birnbaumer, MD, FACEP 3/24/2010 10:00 AM - 11:00 AM Oncologic Emergencies Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California,
Educational Session: Oncology Emergencies Diane M. Birnbaumer, MD, FACEP 3/24/2010 10:00 AM - 11:00 AM Oncologic Emergencies Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California,
It s Not A Tumor! Oncologic Emergencies
 It s Not A Tumor! Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator Department of Emergency Medicine Harbor-UCLA Medical Center Increasing
It s Not A Tumor! Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator Department of Emergency Medicine Harbor-UCLA Medical Center Increasing
Hematologic Emergencies. Udomsak Bunworasate Chulalongkorn University
 Hematologic Emergencies Udomsak Bunworasate Chulalongkorn University Hematologic Emergencies Hyperleukocytosis Tumor lysis syndrome SVC syndrome Spinal cord compression Hypercalcemia 1. Hyperleukocytosis
Hematologic Emergencies Udomsak Bunworasate Chulalongkorn University Hematologic Emergencies Hyperleukocytosis Tumor lysis syndrome SVC syndrome Spinal cord compression Hypercalcemia 1. Hyperleukocytosis
Oncologic Emergencies
 Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Managing patients with bulky cancers
 SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p2pjfjp8nha
SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p2pjfjp8nha
Oncologic Emergencies
 Oncologic Emergencies Objectives Identify the major oncologic emergencies Describe the assessment for each emergency Outline the standard of care of patients experiencing oncologic emergencies Structural
Oncologic Emergencies Objectives Identify the major oncologic emergencies Describe the assessment for each emergency Outline the standard of care of patients experiencing oncologic emergencies Structural
Malignant related superior vena cava (SVC) syndrome
 syndrome") Malignant related superior vena cava (SVC) syndrome Manit Sae-teaw B.Pharm, BCP, BCOP Grad dip in Pharmacotherapy Faculty of pharmaceutical sciences Ubon Ratchathani University 1 Outline Introduction Etiology
Malignant related superior vena cava (SVC) syndrome Manit Sae-teaw B.Pharm, BCP, BCOP Grad dip in Pharmacotherapy Faculty of pharmaceutical sciences Ubon Ratchathani University 1 Outline Introduction Etiology
Professor Dr. Saiyeedur Rahman Professor and Head Department of Medicine SBMCH, Barisal
 Professor Dr. Saiyeedur Rahman Professor and Head Department of Medicine SBMCH, Barisal What is Oncologic Emergency? An oncologic emergency is an acute, potentially life-threatening event resulting from
Professor Dr. Saiyeedur Rahman Professor and Head Department of Medicine SBMCH, Barisal What is Oncologic Emergency? An oncologic emergency is an acute, potentially life-threatening event resulting from
Easy Trick to Spot Leukemia for Pediatricians
 Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
HEMATOLOGIC & ONCOLOGIC EMERGENCIES MEG KELLEY MS, FNP- BC, OCN
 HEMATOLOGIC & ONCOLOGIC EMERGENCIES MEG KELLEY MS, FNP- BC, OCN COURSE OBJECTIVES At the conclusion of this presentation, participants should be able to: 1. Define hematological and oncologic (heme-onc)
HEMATOLOGIC & ONCOLOGIC EMERGENCIES MEG KELLEY MS, FNP- BC, OCN COURSE OBJECTIVES At the conclusion of this presentation, participants should be able to: 1. Define hematological and oncologic (heme-onc)
GOOD MORNING! July 3, 2014
 GOOD MORNING! July 3, 2014 OUR PATIENT 4yo Female with: 2 days of fever, sore throat, swollen nodes in neck and abdominal pain PMH: Tonsillectomy age 2 Immunizations: UTD NKDA DIFFERENTIAL: OUR PATIENT
GOOD MORNING! July 3, 2014 OUR PATIENT 4yo Female with: 2 days of fever, sore throat, swollen nodes in neck and abdominal pain PMH: Tonsillectomy age 2 Immunizations: UTD NKDA DIFFERENTIAL: OUR PATIENT
Oncologic Emergencies
 Oncologic Emergencies Oncologic Emergencies KELLY YOUNG, CNP DNP MN ONCOLOGY Neutropenic Fevers Disseminated Intravascular Coagulation (DIC) Tumor Lysis Syndrome (TLS) Infusion related reaction Spinal
Oncologic Emergencies Oncologic Emergencies KELLY YOUNG, CNP DNP MN ONCOLOGY Neutropenic Fevers Disseminated Intravascular Coagulation (DIC) Tumor Lysis Syndrome (TLS) Infusion related reaction Spinal
Palpable Pulsus Paradoxus in the Setting of Malignant Pericardial Effusion and Tamponade Akshay Pendyal, MD
 Palpable Pulsus Paradoxus in the Setting of Malignant Pericardial Effusion and Tamponade Akshay Pendyal, MD University of Colorado Department of Internal Medicine None Conflicts of Interest Objectives
Palpable Pulsus Paradoxus in the Setting of Malignant Pericardial Effusion and Tamponade Akshay Pendyal, MD University of Colorado Department of Internal Medicine None Conflicts of Interest Objectives
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
Palliative Care Emergencies
 Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Hematologic Emergency. Le Wang, MD, PhD Hematology & Oncology
 Hematologic Emergency Le Wang, MD, PhD Hematology & Oncology Severe Thrombocytopenia (ITP) Clinical: bleeding risk 0 no bleeding; 1 minimal bleeding after trauma; 2 spontaneous but selflimited bleeding;
Hematologic Emergency Le Wang, MD, PhD Hematology & Oncology Severe Thrombocytopenia (ITP) Clinical: bleeding risk 0 no bleeding; 1 minimal bleeding after trauma; 2 spontaneous but selflimited bleeding;
Oncologic Care for Old-Aged Patients
 Oncologic Care for Old-Aged Patients Elderly & Cancer People 65 years or older are at the higher risk for cancer. For all cancers combined, those over 65 years have an incidence rate 10 times greater than
Oncologic Care for Old-Aged Patients Elderly & Cancer People 65 years or older are at the higher risk for cancer. For all cancers combined, those over 65 years have an incidence rate 10 times greater than
42 y/o woman with unwitnessed episode of loss of consciousness and urinary incontinence
 Top Five Neurological Emergencies: When To Refer February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation 1 CASE 1 42 y/o woman with unwitnessed episode
Top Five Neurological Emergencies: When To Refer February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation 1 CASE 1 42 y/o woman with unwitnessed episode
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
BACK AND NECK PAIN QUESTIONNAIRE
 Neurological Surgery and Spine Surgery, S.C. 1 Westbrook Corporate Center, Suite 800 Westchester, Illinois 60154 BACK AND NECK PAIN QUESTIONNAIRE Please PRINT all information CLEARLY and answer all questions
Neurological Surgery and Spine Surgery, S.C. 1 Westbrook Corporate Center, Suite 800 Westchester, Illinois 60154 BACK AND NECK PAIN QUESTIONNAIRE Please PRINT all information CLEARLY and answer all questions
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy
 Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
First Take Home point
 Common Presentations of Childhood Cancer First Take Home point Childhood Cancer is a rare disease New Cases of Cancer in the U.S. in 2003 Number 140000 120000 100000 80000 60000 40000 20000 0 130,000 105,000000
Common Presentations of Childhood Cancer First Take Home point Childhood Cancer is a rare disease New Cases of Cancer in the U.S. in 2003 Number 140000 120000 100000 80000 60000 40000 20000 0 130,000 105,000000
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
Index. Note: Page numbers of article numbers are in boldface type.
 Index Note: Page numbers of article numbers are in boldface type. A Abdomen, acute, as cancer emergency, 381 399 in cancer patients, etiologies unique to, 390 392 in perforation, 388 surgery of, portal
Index Note: Page numbers of article numbers are in boldface type. A Abdomen, acute, as cancer emergency, 381 399 in cancer patients, etiologies unique to, 390 392 in perforation, 388 surgery of, portal
Palliative Care Emergencies. Additional module if needed
 Palliative Care Emergencies Additional module if needed Learning objectives Understand emergency /urgent / important Describe common emergencies in PC Explore principles of essential management Outline
Palliative Care Emergencies Additional module if needed Learning objectives Understand emergency /urgent / important Describe common emergencies in PC Explore principles of essential management Outline
Tumor Lysis Syndrome Nephrology Grand Rounds Tuesday, July 27 th, 2010 Aditya Mattoo
 Tumor Lysis Syndrome Nephrology Grand Rounds Tuesday, July 27 th, 2010 Aditya Mattoo Outline Background/Definition Epidemiology/Risk Stratification Pathophysiology Treatment Renal Replacement Therapy Background/Definition
Tumor Lysis Syndrome Nephrology Grand Rounds Tuesday, July 27 th, 2010 Aditya Mattoo Outline Background/Definition Epidemiology/Risk Stratification Pathophysiology Treatment Renal Replacement Therapy Background/Definition
INTRODUCTION TO WEISMAN/ RATNOFF NELROY G. JONES
 INTRODUCTION TO WEISMAN/ RATNOFF NELROY G. JONES OUTLINE GENERAL INFO COMMON ADMISSIONS TIPS AND TRICKS COMMUNICATION--- NURSES, SW, CARE CO-ORDINATOR GOC WEISMAN/ RATNOFF WEISMAN- SEIDMAN 4 RATNOFF- SEIDMAN
INTRODUCTION TO WEISMAN/ RATNOFF NELROY G. JONES OUTLINE GENERAL INFO COMMON ADMISSIONS TIPS AND TRICKS COMMUNICATION--- NURSES, SW, CARE CO-ORDINATOR GOC WEISMAN/ RATNOFF WEISMAN- SEIDMAN 4 RATNOFF- SEIDMAN
Radiation 2012 econference
 Copyright 2012 Oncology Nursing Society. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, without
Copyright 2012 Oncology Nursing Society. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, without
Cancer Care Kenya Notes for General Practioners:
 Cancer Care Kenya Notes for General Practioners: Site specific symptoms for detecting cancers at an early stage is given below. Please refer patients for detailed work up. 1. Brain /CNS tumors: Sub acute
Cancer Care Kenya Notes for General Practioners: Site specific symptoms for detecting cancers at an early stage is given below. Please refer patients for detailed work up. 1. Brain /CNS tumors: Sub acute
MSCC CARE PATHWAYS & CASE STUDIES. By Michael Balloch Spine CNS
 MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Therapeutic Leukocyte Reduction (TLR) For Myeloid Leukaemia's : A Four Year Experience From An Oncology Centre In India
 For Myeloid Leukaemia's : A Four Year Experience From An Oncology Centre In India") Therapeutic Leukocyte Reduction (TLR) For Myeloid Leukaemia's : A Four Year Experience From An Oncology Centre In India Anita Tendulkar, Jain P, Gupta A, Sharma N, Navkudkar A, Patle V Dr Anita Tendulkar
Therapeutic Leukocyte Reduction (TLR) For Myeloid Leukaemia's : A Four Year Experience From An Oncology Centre In India Anita Tendulkar, Jain P, Gupta A, Sharma N, Navkudkar A, Patle V Dr Anita Tendulkar
Emergencies in Palliative Medicine
 Emergencies in Palliative Medicine Objectives Recognise palliative care emergencies Be aware of their existence Recognise signs and symptoms of common emergencies Anticipate occurrence of emergencies Manage
Emergencies in Palliative Medicine Objectives Recognise palliative care emergencies Be aware of their existence Recognise signs and symptoms of common emergencies Anticipate occurrence of emergencies Manage
Faculty/Presenter Disclosure
 CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure Speaker: Dr. Kimberly Hagel Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria: None Consulting Fees:
CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure Speaker: Dr. Kimberly Hagel Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria: None Consulting Fees:
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION
 BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
Disclosures/COI. Cases in Hematopathology. Outline. Heme Path Findings Not to Miss. Normal Peripheral Smear 6/30/2016
 Disclosures/COI Cases in Hematopathology Vamsi Kota Assistant Professor Department of Hematology & Medical Oncology Leukemia/BMT I have no disclosures or conflicts of interest regarding this presentation.
Disclosures/COI Cases in Hematopathology Vamsi Kota Assistant Professor Department of Hematology & Medical Oncology Leukemia/BMT I have no disclosures or conflicts of interest regarding this presentation.
Choosing Wisely (Outpatient Edition)
") Choosing Wisely (Outpatient Edition) Michael Johansen, MD, MS Assistant Professor - Clinical Department of Family Medicine The Ohio State University Wexner Medical Center Prostate Cancer Screening (and
Choosing Wisely (Outpatient Edition) Michael Johansen, MD, MS Assistant Professor - Clinical Department of Family Medicine The Ohio State University Wexner Medical Center Prostate Cancer Screening (and
Choosing Wisely (Outpatient Edition)
") Choosing Wisely (Outpatient Edition) Michael Johansen, MD, MS Assistant Professor - Clinical Department of Family Medicine The Ohio State University Wexner Medical Center Prostate Cancer Screening (and
Choosing Wisely (Outpatient Edition) Michael Johansen, MD, MS Assistant Professor - Clinical Department of Family Medicine The Ohio State University Wexner Medical Center Prostate Cancer Screening (and
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Oncologic Emergencies
 Oncologic Emergencies Luca Delatore, MD James Emergency Department Medical Director Associate Professor Clinical Department of Emergency Medicine The Ohio State University Wexner Medical Center Prevalence
Oncologic Emergencies Luca Delatore, MD James Emergency Department Medical Director Associate Professor Clinical Department of Emergency Medicine The Ohio State University Wexner Medical Center Prevalence
Oncologic Emergencies
 Oncologic Emergencies Luca Delatore, MD James Emergency Department Medical Director Associate Professor Clinical Department of Emergency Medicine The Ohio State University Wexner Medical Center Prevalence
Oncologic Emergencies Luca Delatore, MD James Emergency Department Medical Director Associate Professor Clinical Department of Emergency Medicine The Ohio State University Wexner Medical Center Prevalence
INVESTIGATION OF ADVERSE TRANSFUSION REACTIONS TABLE OF RECOMMENDED TESTS. Type of Reaction Presentation Recommended Tests Follow-up Tests
 Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Hospital, Chengdu , China. Hospital, Chengdu , China
 Hyperuricemia and acute renal failure secondary to spontaneous tumor lysis syndrome in low risk myelodysplastic syndrome. Yunlin Feng, M.D. 1,, Tao Jiang 2 Correspondence: Yunlin Feng fengyunlin@tsinghua.org.cn
Hyperuricemia and acute renal failure secondary to spontaneous tumor lysis syndrome in low risk myelodysplastic syndrome. Yunlin Feng, M.D. 1,, Tao Jiang 2 Correspondence: Yunlin Feng fengyunlin@tsinghua.org.cn
I-Ming Chen, MD. Endovascular Stenting for Palliative Treatment of Superior Vena Cava Syndrome in End-Stage Lung Cancer
 Endovascular Stenting for Palliative Treatment of Superior Vena Cava Syndrome in End-Stage Lung Cancer I-Ming Chen, MD Division of CardioVascular Surgery Taipei Veterans General Hospital, Taiwan (Live
Endovascular Stenting for Palliative Treatment of Superior Vena Cava Syndrome in End-Stage Lung Cancer I-Ming Chen, MD Division of CardioVascular Surgery Taipei Veterans General Hospital, Taiwan (Live
Objectives. Emergency Department: Rapid Fire Diagnosis 10/4/16. Why emergency medicine is unique. Approach to the emergent patient
 Emergency Department: Rapid Fire Diagnosis Julie Beard DO St. Luke s Hospital Emergency Department October 4 th, 2016 Objectives Why emergency medicine is unique Approach to the emergent patient Discuss
Emergency Department: Rapid Fire Diagnosis Julie Beard DO St. Luke s Hospital Emergency Department October 4 th, 2016 Objectives Why emergency medicine is unique Approach to the emergent patient Discuss
Case Presentation: Diagnosing Spinal Epidural Abscess
 Case Presentation: Diagnosing Spinal Epidural Abscess Introduction Failure to diagnose is the most common medical error in the practice of emergency, urgent care and primary care medicine. Spinal epidural
Case Presentation: Diagnosing Spinal Epidural Abscess Introduction Failure to diagnose is the most common medical error in the practice of emergency, urgent care and primary care medicine. Spinal epidural
Contents. Contributors. Reviewers. Acknowledgements I CARDIOVASCULAR COMPLICATIONS
 Contributors Reviewers Acknowledgements Preface xii xvi xvii xviii I CARDIOVASCULAR COMPLICATIONS 1 Cardiac Complications of Cancer and Anticancer Treatment 3 Introduction 3 Malignant Pericardial Effusion
Contributors Reviewers Acknowledgements Preface xii xvi xvii xviii I CARDIOVASCULAR COMPLICATIONS 1 Cardiac Complications of Cancer and Anticancer Treatment 3 Introduction 3 Malignant Pericardial Effusion
Malignant Spinal cord Compression. Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania
 Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
Disclosures. Learning Objectives 4/21/2015. Incorporating Nutrition-Focused Physician Assessment into Malnutrition Diagnosis. None
 Incorporating Nutrition-Focused Physician Assessment into Malnutrition Diagnosis Robert DeChicco MS, RD, LD, CNSC Manager, Nutrition Support Team Center for Human Nutrition Cleveland Clinic Health System,
Incorporating Nutrition-Focused Physician Assessment into Malnutrition Diagnosis Robert DeChicco MS, RD, LD, CNSC Manager, Nutrition Support Team Center for Human Nutrition Cleveland Clinic Health System,
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
ULYRICE. Protocol Code. Lymphoma. Tumour Group. Dr. Laurie Sehn. Contact Physician
 BCCA Protocol Summary for the Treatment of Relapsed or Refractory Advanced Stage Aggressive B-Cell Non-Hodgkin s Lymphoma with Ifosfamide, CARBOplatin, Etoposide and rituximab Protocol Code Tumour Group
BCCA Protocol Summary for the Treatment of Relapsed or Refractory Advanced Stage Aggressive B-Cell Non-Hodgkin s Lymphoma with Ifosfamide, CARBOplatin, Etoposide and rituximab Protocol Code Tumour Group
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology
 REVIEWED DATE / INITIALS Safety: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: If YES, please list medication allergies: Do you have
REVIEWED DATE / INITIALS Safety: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: If YES, please list medication allergies: Do you have
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression. Tuesday 17 th September 2013
 Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology
 REVIEWED DATE / INITIALS Safety: Yes No Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: Yes No If YES, please list medication allergies:
REVIEWED DATE / INITIALS Safety: Yes No Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: Yes No If YES, please list medication allergies:
CAR-T. Subrena Powell RN, MSN, BMTCN
 CAR-T Subrena Powell RN, MSN, BMTCN Objectives Discuss the treatment timeline of a patient receiving CAR-T therapy Describe the side effects and management of symptoms of CAR-T therapy Treatment Schema
CAR-T Subrena Powell RN, MSN, BMTCN Objectives Discuss the treatment timeline of a patient receiving CAR-T therapy Describe the side effects and management of symptoms of CAR-T therapy Treatment Schema
2:39 2: Dizziness and nausea Cerebral. 2:57 1: Vomiting Gastro-intestinal
 Supplemental: Table B: Detailed description of adverse events by time, treatment group and procedure T-spinal to incident T-spinal to PACU discharge Group THA/TKA Adverse event description Adverse event
Supplemental: Table B: Detailed description of adverse events by time, treatment group and procedure T-spinal to incident T-spinal to PACU discharge Group THA/TKA Adverse event description Adverse event
The Role of Observation Care in the Evaluation and Management of Cancer Emergencies
 The Role of Observation Care in the Evaluation and Management of Cancer Emergencies Adam Klotz, MD Associate Attending Physician Memorial Sloan Kettering Cancer Center FACULTY DISCLOSURE Nothing to disclose
The Role of Observation Care in the Evaluation and Management of Cancer Emergencies Adam Klotz, MD Associate Attending Physician Memorial Sloan Kettering Cancer Center FACULTY DISCLOSURE Nothing to disclose
Recognition & Treatment of Malignant Spinal Cord Compression
 Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
Symptoms and Signs in Hematology/ 2013
 Symptoms and Signs in Hematology/ 2013 Abdallah Abbadi.MD.FRCP Professor of Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Diseases of Blood & Blood forming organs A- Benign
Symptoms and Signs in Hematology/ 2013 Abdallah Abbadi.MD.FRCP Professor of Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Diseases of Blood & Blood forming organs A- Benign
Case conference. Welcome Dr. Lawrence Tierney
 Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Spontaneous Tumor Lysis Syndrome in Small Cell Lung Cancer
 Open Access Case Report DOI: 10.7759/cureus.1017 Spontaneous Tumor Lysis Syndrome in Small Cell Lung Cancer Venkatkiran Kanchustambham 1, Swetha Saladi 2, Setu Patolia 2, David Stoeckel 2 1. Pulmonary
Open Access Case Report DOI: 10.7759/cureus.1017 Spontaneous Tumor Lysis Syndrome in Small Cell Lung Cancer Venkatkiran Kanchustambham 1, Swetha Saladi 2, Setu Patolia 2, David Stoeckel 2 1. Pulmonary
Exam 1 Review. Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies
 Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
EMERGENCIES IN HEMATOLOGY AND ONCOLOGY. South Dakota ACP Meeting September 14, 2018 Keely Hack, MD
 EMERGENCIES IN HEMATOLOGY AND ONCOLOGY South Dakota ACP Meeting September 14, 2018 Keely Hack, MD Objectives Discuss common emergencies in the care of patients with oncologic and hematologic diseases including:
EMERGENCIES IN HEMATOLOGY AND ONCOLOGY South Dakota ACP Meeting September 14, 2018 Keely Hack, MD Objectives Discuss common emergencies in the care of patients with oncologic and hematologic diseases including:
Dyspnea in the Cancer Patient 33 rd Annual PSONS Nursing Symposium April 1, 2011
 Dyspnea in the Cancer Patient 33 rd Annual PSONS Nursing Symposium April 1, 2011 Kathy Witmer, MN, ARNP Swedish Cancer Institute Thoracic Surgery - Oncology Dyspnea The word denotes disordered breathing
Dyspnea in the Cancer Patient 33 rd Annual PSONS Nursing Symposium April 1, 2011 Kathy Witmer, MN, ARNP Swedish Cancer Institute Thoracic Surgery - Oncology Dyspnea The word denotes disordered breathing
Palliative RT. Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University
 Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Bone Metastases. Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital
 Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Palliative Emergencies. Ken Stakiw
 Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
2.1 mmol/l or 25% increase from baseline mmol/l or 25% decrease from baseline
 22.1 Hyperleukocytosis and tumour lysis syndrome The guideline is addressed for ALL patients with hyperleukocytosis (WBC 100 x109/l) only and should not be used without modifications in case of other diseases
22.1 Hyperleukocytosis and tumour lysis syndrome The guideline is addressed for ALL patients with hyperleukocytosis (WBC 100 x109/l) only and should not be used without modifications in case of other diseases
JC Hofmann, MD 1,2 ; KM Grant, MD 3 ; DD Kiprov, MD 1,2. Apheresis Care Group, 2. Division of Immunotherapy, 3
 Greater Than Ninety Percent of Patients with Acute Leukemia and Hyperleukocytosis Who Receive Leukocytapheresis Treatment Successfully Undergo Induction Chemotherapy: Follow-up Analysis of Data from 2006-2013
Greater Than Ninety Percent of Patients with Acute Leukemia and Hyperleukocytosis Who Receive Leukocytapheresis Treatment Successfully Undergo Induction Chemotherapy: Follow-up Analysis of Data from 2006-2013
A Journey Down The Canal
 A Journey Down The Canal Radiological Assessment of Spinal Cord Masses John Berry-Candelario HMS III Gillian Lieberman, MD BIDMC Objectives Patient review Anatomy of the spine Imaging techniques Classification
A Journey Down The Canal Radiological Assessment of Spinal Cord Masses John Berry-Candelario HMS III Gillian Lieberman, MD BIDMC Objectives Patient review Anatomy of the spine Imaging techniques Classification
2 Diagnosis and Staging of Cancer 2.1 Pathophysiology of cancer 2.2 Classification and staging 2.3 Diagnostic measures for specific cancer types
 Oncology Nursing Sub-Specialty Module Reference: Gobel B. M., Triest-Robertson S. & Vogel W.H. (Eds). (205). Advanced Oncology Nursing Certificate Review and Resources Manual. Pittsburgh: Oncology Nursing
Oncology Nursing Sub-Specialty Module Reference: Gobel B. M., Triest-Robertson S. & Vogel W.H. (Eds). (205). Advanced Oncology Nursing Certificate Review and Resources Manual. Pittsburgh: Oncology Nursing
Oncological emergencies. Harmesh Naik, MD. Medical Oncology Hope Cancer Clinic
 Oncological emergencies Harmesh Naik, MD. Medical Oncology Hope Cancer Clinic Presentation to Internal Medicine GME resident physicians: October 24, 2013 Presentation goals Briefly review clinical presentation,
Oncological emergencies Harmesh Naik, MD. Medical Oncology Hope Cancer Clinic Presentation to Internal Medicine GME resident physicians: October 24, 2013 Presentation goals Briefly review clinical presentation,
Case Presentation: Mr. S
 Case Presentation: Mr. S History Seen as inpatient in May, but has significant prior history and is a poor historian 53 y.o. Male no PMH, has been out of contact with medicine for years aside from hernia
Case Presentation: Mr. S History Seen as inpatient in May, but has significant prior history and is a poor historian 53 y.o. Male no PMH, has been out of contact with medicine for years aside from hernia
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Acute Respiratory Distress
 Acute Respiratory Distress Respiratory Distress: Amos Charles, MD Clinical Associate Professor of Medicine Warren Alpert School of Medicine of the Brown University Providence Rhode Island. Waleed Ibrahim-Ali
Acute Respiratory Distress Respiratory Distress: Amos Charles, MD Clinical Associate Professor of Medicine Warren Alpert School of Medicine of the Brown University Providence Rhode Island. Waleed Ibrahim-Ali
Shannon Carty, PGY-2 ICCR IRB Project Proposal April 9, 2008
 Shannon Carty, PGY-2 ICCR IRB Project Proposal April 9, 2008 Study Title: Observational Study to Determine the Effect of an Emergency Department Adult Oncology Stat Antibiotic Protocol on Clinical Outcomes
Shannon Carty, PGY-2 ICCR IRB Project Proposal April 9, 2008 Study Title: Observational Study to Determine the Effect of an Emergency Department Adult Oncology Stat Antibiotic Protocol on Clinical Outcomes
Suspecting Tumors, or Could it be cancer?
 Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
CLINICAL GUIDELINES. Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision
 CLINICAL GUIDELINES Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision TRIAGE At the initial visit, a focused history and physical examination is performed to assign
CLINICAL GUIDELINES Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision TRIAGE At the initial visit, a focused history and physical examination is performed to assign
Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm
 Overall Algorithm") Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm Decision 1: Triage Decision 2: Analgesic Management Decision 3: Diagnostic
Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm Decision 1: Triage Decision 2: Analgesic Management Decision 3: Diagnostic
By Your Sis: Ghada Odeh :)
") By Your Sis: Ghada Odeh :) Hx: Chest pain ACS. Hx.: Cough Bronchiectasis. Hx: Epigastric pain Peptic ulcer disease. Hx: Joints Pain SLE. Hx: Hematurea post-strep Glomerulonephritis. Hx: Jaundice Chronic
By Your Sis: Ghada Odeh :) Hx: Chest pain ACS. Hx.: Cough Bronchiectasis. Hx: Epigastric pain Peptic ulcer disease. Hx: Joints Pain SLE. Hx: Hematurea post-strep Glomerulonephritis. Hx: Jaundice Chronic
OMT for the ACOFP Boards: A Review of Clinical and Basic Information
 OMT for the ACOFP Boards: A Review of Clinical and Basic Information Kevin D. Treffer, D.O., FACOFP Associate Professor, Department of OMM and Primary Care Interim Chair, Department of OMM Kansas City
OMT for the ACOFP Boards: A Review of Clinical and Basic Information Kevin D. Treffer, D.O., FACOFP Associate Professor, Department of OMM and Primary Care Interim Chair, Department of OMM Kansas City
PUFF THE MAGIC DRAGON
 PUFF THE MAGIC DRAGON AN UNUSUAL CASE OF A PUFFY FACE MA ACP Annual Scientific Meeting Gurbir Gill, M.D., PGY-3 (Associate) George M. Abraham, MD, MPH, FACP Department of Medicine, Saint Vincent Hospital,
PUFF THE MAGIC DRAGON AN UNUSUAL CASE OF A PUFFY FACE MA ACP Annual Scientific Meeting Gurbir Gill, M.D., PGY-3 (Associate) George M. Abraham, MD, MPH, FACP Department of Medicine, Saint Vincent Hospital,
Clinical Summary Note. Digital photographs. Echo Cardiogram. Mammogram. Angiogram. BMD scan Pet scan. Xray US
 Ankle brachial inde Radiation Records (H) Eternal econsult Guidelines Updated 12/9/2016 Allergy Allergy Audiology Otorhinolaryngology Breast Clinic BRCA Mutation Family History Ca Breast Genetic Susceptibility
Ankle brachial inde Radiation Records (H) Eternal econsult Guidelines Updated 12/9/2016 Allergy Allergy Audiology Otorhinolaryngology Breast Clinic BRCA Mutation Family History Ca Breast Genetic Susceptibility
Objectives. Identify and differentiate appropriate surgical cases. Good Surgical Outcomes
 ECHO February 5 th, 2015 Surgical Selection for Low Back Pain Objectives Identify and differentiate appropriate surgical cases Disclosures Medical director for UHN Rehabilitations Solution Back and Neck
ECHO February 5 th, 2015 Surgical Selection for Low Back Pain Objectives Identify and differentiate appropriate surgical cases Disclosures Medical director for UHN Rehabilitations Solution Back and Neck
A walk through a STEMI
 A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
M Y ELO I D D I FFER ENTIATI O N OPENS UP THE POSSIBILITIES
 IDHIFA (enasidenib) is indicated for the treatment of adult patients with relapsed or refractory (R/R) acute myeloid leukemia (AML) with an isocitrate dehydrogenase-2 (IDH2) mutation as detected by an
IDHIFA (enasidenib) is indicated for the treatment of adult patients with relapsed or refractory (R/R) acute myeloid leukemia (AML) with an isocitrate dehydrogenase-2 (IDH2) mutation as detected by an
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
An Uncommon Presentation of Large B-cell Lymphoma of the kidney A Case Report and Literature Review
 An Uncommon Presentation of Large B-cell Lymphoma of the kidney A Case Report and Literature Review CHRISTOPHER ADILETTA M.D., AJAZ SHAWL M.D. ST. JOSEPH S HEALTH, SYRACUSE, NY Our Patient Case We present
An Uncommon Presentation of Large B-cell Lymphoma of the kidney A Case Report and Literature Review CHRISTOPHER ADILETTA M.D., AJAZ SHAWL M.D. ST. JOSEPH S HEALTH, SYRACUSE, NY Our Patient Case We present
Emergency Neurological Life Support Spinal Cord Compression
 Emergency Neurological Life Support Spinal Cord Compression Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Spinal Cord Compression Table of Contents Emergency Neurological Life Support...
Emergency Neurological Life Support Spinal Cord Compression Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Spinal Cord Compression Table of Contents Emergency Neurological Life Support...
Metastatic Spinal Disease
 Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of