Recognition & Treatment of Malignant Spinal Cord Compression Study Day
|
|
|
- Tabitha Weaver
- 5 years ago
- Views:
Transcription


1 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital
 Incidence Symptoms & signs Investigations Treatments Outcomes NICE")
2 Outline of Talk Clinical case The anatomy of the spinal cord Definition of malignant spinal cord compression (MSCC) Incidence Symptoms & signs Investigations Treatments Outcomes NICE guidance
3 Clinical Case 56 year old man with history of HTN & OA Presents to GP with 1 month history of back pain unresponsive to paracetamol Pain beginning to wake him at night More pain with lying down Shooting pains down right leg
4 Examination Observations - normal range CVS, Resp, GI, GU exams - normal Back exam Inspection: normal Palpation: some pain in L1 region ROM: normal Some pain in right leg with straight leg raising

5 Lumbar Spine x-ray Age related degeneration Working diagnosis Sciatica V Back strain Treatment recommended NSAIDS Few days of bed rest
6 4 weeks later Pain does not resolve Various forms of pain control tried & fail Wakes up, difficulty supporting his weight subjective leg muscle weakness Wife calls 999 Taken to local A&E
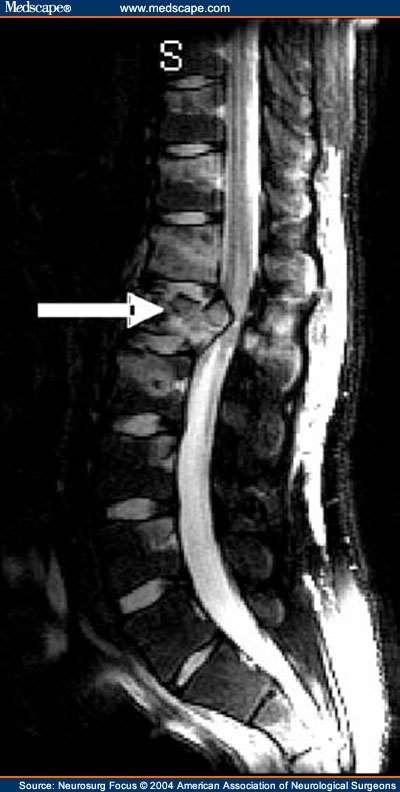
7 In A&E Objective leg weakness on physical exam A very keen medical student does a rectal exam and discovers a large nodular prostate PSA: 45.0 MRI Spine..

8

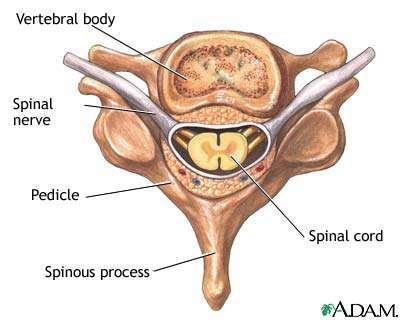
9 Anatomy of the spine

10 Different spinal cord levels supply nerves for different regions of the body
 on the spinal cord & nerves")
11 What is malignant spinal cord Occurs when cancer cells grow in/near to spine and press on the spinal cord & nerves Results in swelling & reduction in the blood supply to the spinal cord & nerve roots The symptoms are caused by the increasing pressure (compression) on the spinal cord & nerves compression?
 4% Intramedullary spread 1%(Low) Direct spread to epidural")
12 Method of spread 85%From vertebral body or pedicle 10% Through intervertebral foramina (from paravertebral nodes or mass) 4% Intramedullary spread 1%(Low) Direct spread to epidural space


13
14 Location Thoracic spine 60% Lumbosacral spine 30% Cervical spine 10%
15 What types of cancer cause it? Most commonly seen in Breast Lung Prostate Lymphoma Myeloma 3-5% of patients with cancer overall Approx 200 cases per annum in North Trent
16 What are the signs & symptoms of MSCC?
17 First Symptoms Pain 95% Weakness 5% Ataxia 1% Sensory loss 1% RED FLAGS..
18 First Red Flag: Pain Usually first symptom 80-90% of the time Usually precedes other neurologic symptoms by 7 weeks Increases in intensity Severe local back pain Aggravated by lying down Distension of venous plexus Bach, F, Larsen, BH, Rohde, K, et al. Metastatic spinal cord compression. Occurrence, symptoms, clinical presentations and prognosis in 398 patients with spinal cord compression. Acta Neurochir (Wien) 1990; 107:37.
19 Back pain may be mild to begin with lasts for more than 1-2 weeks Pain may feel like a 'band' around the chest or abdomen (radicular) Can radiate over the lower back, into the buttocks or legs
20 Second Red Flag: Motor Weakness: 60-85% Tends to be symmetrical Severity greatest with thoracic mets At or above conus medularis Extensors of the upper extremities Above the thoracic spine Weakness from corticospinal dysfunction Affects flexors in the lower extremities Patients may be hyper reflexic below the lesion and have extensor plantars Greenberg, HS, Kim, JH, Posner, JB. Epidural spinal cord compression from metastatic tumor: Results with a new treatment protocol. Ann Neurol 1980; 8:361.
21 Third Red Flag: Sensory Less common than motor findings Still present in majority of cases Ascending numbness and parathesias Numbness or 'pins and needles' in toes & fingers or over the buttocks Sensory level Saddle anaesthesia Feeling unsteady on feet, having difficulty with walking, or legs giving way
22 Fourth Red Flag: Bladder & Loss is late finding Bowel Function Problems passing urine may include difficulty controlling bladder function passing very little urine or passing none at all Constipation or problems controlling bowels Autonomic neuropathy presents usually as urinary retention Rarely sole finding
23 Duration of symptoms before diagnosis 2-5 months median
24 It is an oncological emergency Requires very prompt diagnosis & treatment to try and prevent catastrophic consequences of paralysis & incontinence

25 Investigations & information needed prior to Rx 1. MRI scan of the whole spine Can get compression at multiple levels 2. Knowledge of cancer type & stage 3. Knowledge of patient fitness 4. Current neurological function Have they lost power in their legs? Can they walk? Do they need a catheter? 5. Do they have pain?

26 MRI of spinal cord compression in a women with past history of breast cancer
27 Differential diagnosis Metastatic cancer Herniated disc Benign bony lesion Abscess Alcoholic neuropathy Primary tumour Osteoporosis Low potassium Case report 3/11 cases confirmed MSCC
28 Treatment Until spinal stability is confirmed patients should be managed on bed rest BUT Wherever possible keep the patient moving
29 Treatment Objectives Pain control Avoidance of complications Preserve or improve neurological function
30 Treatment options include: 1. Steroids & gastric protection 2. Analgesia 3. Surgery decompression & stabilisation of the spine 4. Radiotherapy 5. Chemotherapy e.g. lymphoma 6. Hormonal manipulation e.g. prostate Ca
31 WPH Reducing regimen for Spinal Cord Compression Day Dexamethasone daily dose Administration mg 16mg OM or 8mg BD (8am & 12noon) 4-6 8mg 8mg OM 7-9 4mg 4mg OM mg 2mg OM 13 Discontinue While the patient is on steroids commence PPI (e.g. Lansoprazole) for gastric protection. A slower reducing regimen may be required for patients who have received previous courses of steroids.
32 Anticoagulation Cancer is a hypercoaguable state High burden of tumour in metastatic disease Possible value in prophylaxis against venous thromboembolism If patient not mobile subcutaneous low molecular weight heparin +/- compression devices
33 Factors Constipation Autonomic dysfunction Limited mobility Opiate analgesic Risk of perforation Masked by corticosteroids Bowel regimen needed
34 Surgery RCT comparing surgery followed by RT vs. RT alone Improvement in surgery + RT Days remained ambulatory (126 vs. 35) Percent that regained ambulation after therapy (56% vs. 19%) Days remained continent (142 vs. 12) Less steroid dose, less narcotics Trend to increase survival Patchell, R, Tibbs, PA, Regine, WF, et al. A randomized trial of direct decompressive surgical resection in the treatment of spinal cord compression caused by metastasis (abstract). proc Am Soc Clin Oncol 2003; 22:1.
35 Direct decompressive surgery Relieves compression Removes tumour Stabilises spine But many patients not suitable Unfit Tumour factors
36 Indications for Surgery Unknown primary tumour Relapse post RT Progression while on RT Intractable pain Instability of spine Patients with a single level of cord compression who have not been totally paraplegic for longer than 48 hours Prognosis >4 months
37 Radiotherapy Urgent access 24/7 Dose & schedule Depending on neurological deficit, PS, previous treatment and cancer features Single V fractionated treatment SCORAD trial

38 Radiotherapy
39 Radiotherapy Pre operatively no Post operatively routinely Definitive all pts unsuitable for surgery Unless Total paraplegia (>24hrs) Very poor prognosis
40 Chemotherapy Can be successful in chemosensitive tumours Hodgkin s lymphoma Non-Hodgkin s lymphoma Neuroblastoma Germ cell Breast cancer (hormonal manipulation) Prostate cancer (hormonal manipulation)
41 Other considerations 1. Bed rest V mobilisation Rehabilitation Braces & collars 2. Psychological issues 3. Urinary catheter 4. Bowel function 5. Nutrition 6. Discharge issues
42 Prognosis Median survival with MSCC is 6 months Ambulatory patients with radiosensitive tumours have the best prognosis Likely to remain mobile Sorensen, PS, Borgesen, SE, Rohde, K, et al. Metastatic epidural spinal cord compression. Results of treatment and survival. Cancer 1990; 65:1502. MSCC is a poor prognostic indicator in cancer patients Need better detection rates
43 Number of days survival following admission with spinal cord compression Data from WPH audit Number of days from admission with spinal cord compression to death Range = 2 days to 319 days Mean = 58.6 days

44 Metastatic spinal cord compression Implementing NICE guidance 2008 NICE clinical guideline 75
45 Key priorities for implementation The areas identified as key priorities for implementation are: Service configuration & urgency of treatment Early detection Imaging Treatment of spinal metastases & MSCC Supportive care & rehabilitation
46 Early detection Inform patients with cancer who are at risk of MSCC information about the symptoms of MSCC what to do & who to contact if symptoms develop Discuss with the MSCC coordinator immediately patients with cancer who have symptoms of spinal metastases & neurological symptoms or signs suggestive of MSCC view as an emergency. Discuss with the MSCC coordinator within 24 hours patients with cancer who have symptoms suggestive of spinal metastases
47
48
49

50
Recognition & Treatment of Malignant Spinal Cord Compression
 Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Metastatic Spinal Cord Compression
 Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK Introduction 2-5% of cancer patients have an episode of MSCC Initial
Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK Introduction 2-5% of cancer patients have an episode of MSCC Initial
MSCC CARE PATHWAYS & CASE STUDIES. By Michael Balloch Spine CNS
 MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
Management of Acute Oncological emergencies
 Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Malignant Spinal cord Compression. Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania
 Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
Metastatic Spinal Disease
 Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Spinal Cord Compression Diagnosis and Management. Information for Shared Care Centres and Community Staff
 Reference: CG1412 Written by: Dr Daniel Yeomanson Peer reviewer Dr Jeanette Payne Approved: August 2016 Approved by D&TC: 10 th June 2016 Review Due: August 2019 Intended Audience This document contains
Reference: CG1412 Written by: Dr Daniel Yeomanson Peer reviewer Dr Jeanette Payne Approved: August 2016 Approved by D&TC: 10 th June 2016 Review Due: August 2019 Intended Audience This document contains
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway
 Clinical guidelines and pathway") Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION
 CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
Update on Management of Malignant Spinal Cord Compression. Heino Hugel Consultant in Palliative Medicine University Hospital Aintree
 Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Radiotherapy symptoms control in bone mets. Francesco Cellini GemelliART. Ernesto Maranzano,MD. Session 5: Symptoms management
 Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator
 Clinical Advisor Coordinator") Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator Induction Training 2016 Version Control This is a controlled document please destroy all previous versions on receipt of a new version.
Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator Induction Training 2016 Version Control This is a controlled document please destroy all previous versions on receipt of a new version.
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. Version:
 GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
Spinal cord compression as a first presentation of cancer: A case report
 J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽
 외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽 Index Introduction Etiology & Type Assessment History taking & Physical examination Red flag sign Imaging Common disorder Management Reference Introduction Pain
외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽 Index Introduction Etiology & Type Assessment History taking & Physical examination Red flag sign Imaging Common disorder Management Reference Introduction Pain
Metastatic spinal cord compression (MSCC) What happens? MSCC. MSCC is a palliative care emergency. Signs/symptoms
 What happens? MSCC. MSCC is a palliative care emergency. Signs/symptoms") A patient with suspected metastatic spinal cord compression and the dilemma of non-resident status Sandra Notley CNS-Palliative Care 1 Metastatic spinal cord compression (MSCC) Is indentation, displacement
A patient with suspected metastatic spinal cord compression and the dilemma of non-resident status Sandra Notley CNS-Palliative Care 1 Metastatic spinal cord compression (MSCC) Is indentation, displacement
Palliative Care Emergencies
 Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Surgery. Conus medullaris and Cauda Equina Syndromes. Anatomy. See online here
 Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE
 THE CHRISTIE, GREATER MANCHESTER & CHESHIRE") PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
Guidelines for the Management. Malignant Spinal Cord Compression. Final Guideline
 Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Paul Allan Regional Clinical Lead - South. Lumbar Spine. Assessment & Differential Diagnosis
 Paul Allan Regional Clinical Lead - South Lumbar Spine Assessment & Differential Diagnosis Aims Refresh lumbar spine anatomy Red flags Discuss common pathologies seen in general practice Subjective and
Paul Allan Regional Clinical Lead - South Lumbar Spine Assessment & Differential Diagnosis Aims Refresh lumbar spine anatomy Red flags Discuss common pathologies seen in general practice Subjective and
Suspecting Tumors, or Could it be cancer?
 Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Emergency Neurological Life Support Spinal Cord Compression
 Emergency Neurological Life Support Spinal Cord Compression Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Spinal Cord Compression Table of Contents Emergency Neurological Life Support...
Emergency Neurological Life Support Spinal Cord Compression Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Spinal Cord Compression Table of Contents Emergency Neurological Life Support...
Spinal cord compression
 Spinal cord compression Urology Department Patient Information Leaflet Introduction If you have been diagnosed with cancer, you need to know about spinal cord compression and the warning signs. This leaflet
Spinal cord compression Urology Department Patient Information Leaflet Introduction If you have been diagnosed with cancer, you need to know about spinal cord compression and the warning signs. This leaflet
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression. Tuesday 17 th September 2013
 Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
Palliative treatments for lung cancer: What can the oncologist do?
 Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Developing spinal cord compression care guidelines at WPH
 Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Dr Bernie Foran, Suzanne Hodson, Liz Kirkham, Rebecca Mills, Jan Siddall, Rebecca Walsh,
Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Dr Bernie Foran, Suzanne Hodson, Liz Kirkham, Rebecca Mills, Jan Siddall, Rebecca Walsh,
Lumbar Spinal Stenosis
 Lumbar Spinal Stenosis by David Borenstein, MD In a previous article on low back pain, I reviewed the anatomy of the spine and discussed three causes of low back pain: muscle strain, herniated intervertebral
Lumbar Spinal Stenosis by David Borenstein, MD In a previous article on low back pain, I reviewed the anatomy of the spine and discussed three causes of low back pain: muscle strain, herniated intervertebral
Suspected spinal cord compression form
 Suspected spinal cord compression form Enter this form into the notes at the appropriate date in the Progress / Evaluation sheets. Please copy this form to Lisa Lewis, Medical PA (ext 4551), for audit
Suspected spinal cord compression form Enter this form into the notes at the appropriate date in the Progress / Evaluation sheets. Please copy this form to Lisa Lewis, Medical PA (ext 4551), for audit
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
CP80 Version: V01. Acute Oncology Management Service Date approved: 8 th May 2015 Date ratified: 1 st June 2015 Review date: 1 st June 2017
 STANDARD OPERATING PROCEDURE (SOP) AND PATHWAY FOR THE MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION (MSCC) WITHIN THE CHRISTIE (Refer to the Manchester Cancer Network MSCC Pathway flowchart)
STANDARD OPERATING PROCEDURE (SOP) AND PATHWAY FOR THE MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION (MSCC) WITHIN THE CHRISTIE (Refer to the Manchester Cancer Network MSCC Pathway flowchart)
Developing spinal cord compression care guidelines at WPH
 Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Bernie Foran, Suzanne Hodson, Jane Mason, Rebecca Mills, Jan Siddall, Rebecca Walsh, Clare
Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Bernie Foran, Suzanne Hodson, Jane Mason, Rebecca Mills, Jan Siddall, Rebecca Walsh, Clare
The surgical treatment of metastatic disease of the spine
 The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
NICE National Institute for Health and Clinical Excellence Metastic Spinal Cord Compression
 NICE - Metastic Spinal Cord Compression 26/11/2008 (Livello 2) NICE National Institute for Health and Clinical Excellence Metastic Spinal Cord Compression Documento Documento Documento Documento file:///c
NICE - Metastic Spinal Cord Compression 26/11/2008 (Livello 2) NICE National Institute for Health and Clinical Excellence Metastic Spinal Cord Compression Documento Documento Documento Documento file:///c
Analysis of Malignant Spinal Cord Compression Patients Treated In a Radiotherapy Centre
 Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2013; 1(6):906-910 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2013; 1(6):906-910 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
Emergencies in Palliative Medicine
 Emergencies in Palliative Medicine Objectives Recognise palliative care emergencies Be aware of their existence Recognise signs and symptoms of common emergencies Anticipate occurrence of emergencies Manage
Emergencies in Palliative Medicine Objectives Recognise palliative care emergencies Be aware of their existence Recognise signs and symptoms of common emergencies Anticipate occurrence of emergencies Manage
BRIEFING PAPER THE USE OF RED FLAGS TO IDENTIFY SERIOUS SPINAL PATHOLOGY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. Version:
 BRIEFING PAPER THE USE OF RED FLAGS TO IDENTIFY SERIOUS SPINAL PATHOLOGY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Jackie Turnpenney Version: Accountable Committee:
BRIEFING PAPER THE USE OF RED FLAGS TO IDENTIFY SERIOUS SPINAL PATHOLOGY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Jackie Turnpenney Version: Accountable Committee:
Epidemiology of Low back pain
 Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Wendy Field Advanced Physiotherapy Practitioner June 2018
 Wendy Field Advanced Physiotherapy Practitioner June 2018 Radiculopathy???? Lumbar radicular pain is where the clinician suspects the pain is coming from a lumbar nerve root. Essentially we are looking
Wendy Field Advanced Physiotherapy Practitioner June 2018 Radiculopathy???? Lumbar radicular pain is where the clinician suspects the pain is coming from a lumbar nerve root. Essentially we are looking
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center
 Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Bone Metastases. Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital
 Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Radiotherapy for lymphoma
 Radiotherapy for lymphoma The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer by using high energy
Radiotherapy for lymphoma The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer by using high energy
The Role of Radiotherapy in Metastatic Breast Cancer. Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health
 The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
Red Flags, and Clinical Presentation Mapping. Sue Greenhalgh Consultant Physiotherapist NHS Bolton
 , and Clinical Presentation Mapping Sue Greenhalgh Consultant Physiotherapist NHS Bolton Be Aware! Clinical Reasoning Recognition of serious pathology early depends on awareness, vigilance and suspicion
, and Clinical Presentation Mapping Sue Greenhalgh Consultant Physiotherapist NHS Bolton Be Aware! Clinical Reasoning Recognition of serious pathology early depends on awareness, vigilance and suspicion
 www.fisiokinesiterapia.biz NOTE : THIS PRESENTATION DOES NOT REPLACE ATTENDANCE OR INFORMATION GIVEN IN THE LECTURE.IT IS INTENDED AS A HIGHLIGHT FOR THE TOPIC INTRODUCTION 60-80% of people will have LBP
www.fisiokinesiterapia.biz NOTE : THIS PRESENTATION DOES NOT REPLACE ATTENDANCE OR INFORMATION GIVEN IN THE LECTURE.IT IS INTENDED AS A HIGHLIGHT FOR THE TOPIC INTRODUCTION 60-80% of people will have LBP
Metastatic disease of the Spine
 Metastatic disease of the Spine Jwalant S. Mehta MS (Orth); MCh (Orth); D Orth; FRCS (Tr & Orth) Consultant Spine Surgeon The Royal Orthopaedic Hospital Birmingham Children s Hospital MSCC Metastatic Spinal
Metastatic disease of the Spine Jwalant S. Mehta MS (Orth); MCh (Orth); D Orth; FRCS (Tr & Orth) Consultant Spine Surgeon The Royal Orthopaedic Hospital Birmingham Children s Hospital MSCC Metastatic Spinal
Common Thoraco- Lumbar Problems in the Mature Athlete
 Common Thoraco- Lumbar Problems in the Mature Athlete Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Review the pathophysiology of the
Common Thoraco- Lumbar Problems in the Mature Athlete Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Review the pathophysiology of the
Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology
 Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Spinal cord compression: what it means and how it can be treated
 Spinal cord compression: what it means and how it can be treated Patient Information Oncology Department Author ID: Acute Oncology Nurse Specialist Leaflet Number: CC 036 Version: 2.1 Name of Leaflet:
Spinal cord compression: what it means and how it can be treated Patient Information Oncology Department Author ID: Acute Oncology Nurse Specialist Leaflet Number: CC 036 Version: 2.1 Name of Leaflet:
Palliative RT. Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University
 Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Case Studies, Impairment of the Spine in Washington State
 Case Studies, Impairment of the Spine in Washington State NAOEM at Skamania, 2015 25 Sep, 2015 Tim Gilmore, MD Several Slides from this Presentation Borrowed with permission from the Washington State Department
Case Studies, Impairment of the Spine in Washington State NAOEM at Skamania, 2015 25 Sep, 2015 Tim Gilmore, MD Several Slides from this Presentation Borrowed with permission from the Washington State Department
Back pain and bladder problems
 Back pain and bladder problems Search Learn the causes and symptoms of chronic back pain, as well as safe techniques that provide back pain relief better than prescriptions drugs. If back pain is reducing
Back pain and bladder problems Search Learn the causes and symptoms of chronic back pain, as well as safe techniques that provide back pain relief better than prescriptions drugs. If back pain is reducing
42 y/o woman with unwitnessed episode of loss of consciousness and urinary incontinence
 Top Five Neurological Emergencies: When To Refer February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation 1 CASE 1 42 y/o woman with unwitnessed episode
Top Five Neurological Emergencies: When To Refer February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation 1 CASE 1 42 y/o woman with unwitnessed episode
Disclosure. Thoracolumbar Tumors. Intraspinal Tumor Removal Options 6/4/2011. Minimally Invasive Approaches for Spinal Tumors
 Minimally Invasive Approaches for Spinal Tumors Praveen V. Mummaneni, M.D. Disclosure Medtronic (Consultant, Grants) DePuy (Consultant, Other Financial Support) Associate Professor Dept. of Neurosurgery
Minimally Invasive Approaches for Spinal Tumors Praveen V. Mummaneni, M.D. Disclosure Medtronic (Consultant, Grants) DePuy (Consultant, Other Financial Support) Associate Professor Dept. of Neurosurgery
EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS
 CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
Regional Back Pain and Radicular Pain Pathway Frequently asked Questions and Answers
 In Partnership with Regional Back Pain and Radicular Pain Pathway Frequently asked Questions and Answers Moving BACK to health Don t let your back pain get the better of you! The Regional Back Pain and
In Partnership with Regional Back Pain and Radicular Pain Pathway Frequently asked Questions and Answers Moving BACK to health Don t let your back pain get the better of you! The Regional Back Pain and
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Common Treatment Related Sideeffects. Radical Prostatectomy Urinary Effects. Survivorship what is the unmet need?
 Side Effects of Prostate Cancer Treatment Christian Smith Clinician Nurse, Velindre Cancer Centre Common Treatment Related Sideeffects Urinary RP, EBRT, Brachy Bowel EBRT & Brachy Sexual All treatment
Side Effects of Prostate Cancer Treatment Christian Smith Clinician Nurse, Velindre Cancer Centre Common Treatment Related Sideeffects Urinary RP, EBRT, Brachy Bowel EBRT & Brachy Sexual All treatment
Corporate Medical Policy
 Corporate Medical Policy Epidural Steroid Injections for Back Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: epidural_steroid_injections_for_back_pain 2/2016 4/2017 4/2018
Corporate Medical Policy Epidural Steroid Injections for Back Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: epidural_steroid_injections_for_back_pain 2/2016 4/2017 4/2018
A Syndrome (Pattern) Approach to Low Back Pain. History
 Approach to Low Back Pain. History") A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
agreed MSCC pathways and guidelines).
.") Referral of Patients with Spinal Metastatic Disease and Suspected Metastatic Spinal Cord Compression (to be used in association with locally West Midlands Clinical Networks and Clinical Senate Coversheet
Referral of Patients with Spinal Metastatic Disease and Suspected Metastatic Spinal Cord Compression (to be used in association with locally West Midlands Clinical Networks and Clinical Senate Coversheet
Radiotherapy in oncological emergencies. Is it still a mainstay?
 Radiotherapy in oncological emergencies. Is it still a mainstay? Paweł Potocki, MD Jagiellonian University Medical College Kraków University Hospital Departament of Clinical Oncology ppotocki@su.krakow.pl
Radiotherapy in oncological emergencies. Is it still a mainstay? Paweł Potocki, MD Jagiellonian University Medical College Kraków University Hospital Departament of Clinical Oncology ppotocki@su.krakow.pl
Disclosures. Disclosures 27/01/2019. Modern approach and pitfalls in metastatic spine surgery. None.. Jeremy Reynolds
 Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
Radiotherapy for Patients with Symptomatic Intramedullary Spinal Cord Metastasis
 J. Radiat. Res., 52, 641 645 (2011) Regular Paper Radiotherapy for Patients with Symptomatic Intramedullary Spinal Cord Metastasis Haruko HASHII 1,4 *, Masashi MIZUMOTO 1,4 *, Ayae KANEMOTO 1,4, Hideyuki
J. Radiat. Res., 52, 641 645 (2011) Regular Paper Radiotherapy for Patients with Symptomatic Intramedullary Spinal Cord Metastasis Haruko HASHII 1,4 *, Masashi MIZUMOTO 1,4 *, Ayae KANEMOTO 1,4, Hideyuki
Brain and Spine Tumors
 Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Title Protocol for the management of suspected cauda equine syndrome & decompensating spinal stenosis at NDDH
 Document Control Title Protocol for the management of suspected cauda equine syndrome & decompensating spinal stenosis at NDDH Author Author s job title Consultant T&O Directorate Scheduled Care Department
Document Control Title Protocol for the management of suspected cauda equine syndrome & decompensating spinal stenosis at NDDH Author Author s job title Consultant T&O Directorate Scheduled Care Department
Oncologic Emergencies
 Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Diagnosis. Lumpers vs splitters. Non specific Low back pain Biopsychosocial model good GPs already incorporate this into daily practice
 Spinal Pain COL Tony Delaney RFD MB BS FACSP Sports Physician Narrabeen Sports Medicine Centre Sydney Academy of Sport Chair ADF Musculoskeletal, Sports, Rehabilitation Consultative Group 1999-2012 Background
Spinal Pain COL Tony Delaney RFD MB BS FACSP Sports Physician Narrabeen Sports Medicine Centre Sydney Academy of Sport Chair ADF Musculoskeletal, Sports, Rehabilitation Consultative Group 1999-2012 Background
Back Pain. John W. Engstrom, MD December 16, Disclosures. A Clinical Approach to the Evaluation of Back Pain and Lumbar Radiculopathy
 Disclosures Nothing to declare --- or --- Significant ownership interests Speaker bureaus, honorarium, grants A Clinical Approach to the Evaluation of and Lumbar Radiculopathy John Engstrom, MD Acute Low
Disclosures Nothing to declare --- or --- Significant ownership interests Speaker bureaus, honorarium, grants A Clinical Approach to the Evaluation of and Lumbar Radiculopathy John Engstrom, MD Acute Low
Palliative Care Emergencies
 Palliative Care Emergencies Dr. T. Thirukkumaran Palliative Care Services Northwest Tasmania What are the emergencies in Palliative Medicine? Palliative Emergencies (a) Disease related or Symptom related
Palliative Care Emergencies Dr. T. Thirukkumaran Palliative Care Services Northwest Tasmania What are the emergencies in Palliative Medicine? Palliative Emergencies (a) Disease related or Symptom related
Speaker: Dr Gautam (Vini) Khurana MBBS (Syd, Hons), BScMed (Syd, Medal), PhD (Mayo Clinic), FRACS
 Khurana MBBS (Syd, Hons), BScMed (Syd, Medal), PhD (Mayo Clinic), FRACS") A Pain in the Back GPCE Workshop Sydney Olympic Park May 22-24, 2015 Speaker: Dr Gautam (Vini) Khurana MBBS (Syd, Hons), BScMed (Syd, Medal), PhD (Mayo Clinic), FRACS www.cnsneurosurgery.com.au VMO Neurosurgeon
A Pain in the Back GPCE Workshop Sydney Olympic Park May 22-24, 2015 Speaker: Dr Gautam (Vini) Khurana MBBS (Syd, Hons), BScMed (Syd, Medal), PhD (Mayo Clinic), FRACS www.cnsneurosurgery.com.au VMO Neurosurgeon
Lumbar disc prolapse. Done by : Areej Al-Hadidi
 Lumbar disc prolapse Done by : Areej Al-Hadidi Anatomy of IVD IVD is composed of two components: 1. anulus fibrosus : it is the outer fibrous layer (fibrocartilage ) **It is comressible &tough 2. nucleus
Lumbar disc prolapse Done by : Areej Al-Hadidi Anatomy of IVD IVD is composed of two components: 1. anulus fibrosus : it is the outer fibrous layer (fibrocartilage ) **It is comressible &tough 2. nucleus
CLINICAL GUIDELINES. Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision
 CLINICAL GUIDELINES Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision TRIAGE At the initial visit, a focused history and physical examination is performed to assign
CLINICAL GUIDELINES Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision TRIAGE At the initial visit, a focused history and physical examination is performed to assign
A Patient s Guide to Spinal Tumors
 A Patient s Guide to Spinal Tumors 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Spinal Tumors 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
Chiropractic Health Plan - Diagnosis of Low Back Pain
 Chiropractic Health Plan - Diagnosis of Low Back Pain 1 Adult Patient with ot for major Trauma Low back pain 2 Intake Evaluation (Inset 1) Recommendation 1 3 Potentially Serious Condition Strongly Suspected
Chiropractic Health Plan - Diagnosis of Low Back Pain 1 Adult Patient with ot for major Trauma Low back pain 2 Intake Evaluation (Inset 1) Recommendation 1 3 Potentially Serious Condition Strongly Suspected
Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures
 Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures All Referrals (see notes): Spinal Surgeons Locally or Trauma SpR at UHW Oncology SpR at Velindre / Singleton
Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures All Referrals (see notes): Spinal Surgeons Locally or Trauma SpR at UHW Oncology SpR at Velindre / Singleton
Red Flags for serious spinal pathology: A collaborative approach
 Red Flags for serious spinal pathology: A collaborative approach Professor James Selfe DSc, PhD, MA, GD Phys (Distinction), FCSP Serious Spinal Pathology Background Collaboration Communication Solutions
Red Flags for serious spinal pathology: A collaborative approach Professor James Selfe DSc, PhD, MA, GD Phys (Distinction), FCSP Serious Spinal Pathology Background Collaboration Communication Solutions
Back Pain Policies Summary
 Back Pain Policies Summary These policies are part of the wider project, Reviewing local health policies, which is reviewing and updating more than 100 policies, of which back pain are part of. This review
Back Pain Policies Summary These policies are part of the wider project, Reviewing local health policies, which is reviewing and updating more than 100 policies, of which back pain are part of. This review
Primary care referral criteria for musculoskeletal MRI scans
 Appendix 1 Primary care referral criteria for musculoskeletal MRI scans Accepted Criteria for Direct Access MRI Body Part Symptoms Imaging indicated Lumbar Spine Low Back Pain with adverse symptoms or
Appendix 1 Primary care referral criteria for musculoskeletal MRI scans Accepted Criteria for Direct Access MRI Body Part Symptoms Imaging indicated Lumbar Spine Low Back Pain with adverse symptoms or
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
Lumbar Spinal Stenosis
 Lumbar Spinal Stenosis This article is also available in Spanish: Estenosis de la columna lumbar (topic.cfm?topic=a00701). A common cause of low back and leg pain is lumbar spinal stenosis. As we age,
Lumbar Spinal Stenosis This article is also available in Spanish: Estenosis de la columna lumbar (topic.cfm?topic=a00701). A common cause of low back and leg pain is lumbar spinal stenosis. As we age,
Spinal Trauma. General Rehabilitation of Patient with Spinal Trauma. Common Spinal Injuries. Important Anatomical Structures at each Vertebral Level
 Asian Association for Dynamic Osteosynthesis Workshop on Management of Spinal Trauma 22 April 2007 (Sunday) Orthopaedic Learning Centre, PWH, Shatin, Hong Kong General Rehabilitation of Patient with Spinal
Asian Association for Dynamic Osteosynthesis Workshop on Management of Spinal Trauma 22 April 2007 (Sunday) Orthopaedic Learning Centre, PWH, Shatin, Hong Kong General Rehabilitation of Patient with Spinal
The in-hospital management of COPD-exacerbation includes three core processes:
 Appendix 1A. Process flow for in-hospital management of COPDexacerbation The in-hospital management of COPD-exacerbation includes three core processes: 1. Diagnostic assessment 2. Pharmacological management
Appendix 1A. Process flow for in-hospital management of COPDexacerbation The in-hospital management of COPD-exacerbation includes three core processes: 1. Diagnostic assessment 2. Pharmacological management
Metastatic epidural spinal cord compression (MESCC)
") SPINE Volume 39, Number 9, pp E587 - E592 2014, Lippincott Williams & Wilkins LITERATURE REVIEW Direct Decompressive Surgery Followed by Radiotherapy Versus Radiotherapy Alone for Metastatic Epidural Spinal
SPINE Volume 39, Number 9, pp E587 - E592 2014, Lippincott Williams & Wilkins LITERATURE REVIEW Direct Decompressive Surgery Followed by Radiotherapy Versus Radiotherapy Alone for Metastatic Epidural Spinal
Benefits of Radiation Therapy in the Palliative Cancer Patient
 Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
Are you getting the best treatment for your low back pain?
 Are you getting the best treatment for your low back pain? Dr.Rahimian Orthopedic surgon Spine fellowship resident Why are we here? To update you on the best evidence for the treatments available To give
Are you getting the best treatment for your low back pain? Dr.Rahimian Orthopedic surgon Spine fellowship resident Why are we here? To update you on the best evidence for the treatments available To give
APPROPRIATE USE GUIDELINES
 APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Neck Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Updated June, 2017 Contents
APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Neck Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Updated June, 2017 Contents
Spinal Cord Compression in Metastatic Prostate Cancer
 European Urology European Urology 44 (2003) 527 532 Spinal Cord Compression in Metastatic Prostate Cancer H. Tazi, A. Manunta *, A. Rodriguez, J.J. Patard, B. Lobel, F. Guillé Service d Urologie, Centre
European Urology European Urology 44 (2003) 527 532 Spinal Cord Compression in Metastatic Prostate Cancer H. Tazi, A. Manunta *, A. Rodriguez, J.J. Patard, B. Lobel, F. Guillé Service d Urologie, Centre
A new score predicting the survival of patients with spinal cord compression from myeloma
 Douglas et al. BMC Cancer 2012, 12:425 RESEARCH ARTICLE Open Access A new score predicting the survival of patients with spinal cord compression from myeloma Sarah Douglas 1, Steven E Schild 2 and Dirk
Douglas et al. BMC Cancer 2012, 12:425 RESEARCH ARTICLE Open Access A new score predicting the survival of patients with spinal cord compression from myeloma Sarah Douglas 1, Steven E Schild 2 and Dirk
Chapter 35 Back Pain. Episode overview: Wisecracks: Crack Cast Show Notes Back Pain July 2016
 Chapter 35 Back Pain Episode overview: 1) List 10 historical red flags for back pain 2) List 6 Emergent Diagnosis for back pain Wisecracks: 1) Describe the most common sites of disc protrusion with their
Chapter 35 Back Pain Episode overview: 1) List 10 historical red flags for back pain 2) List 6 Emergent Diagnosis for back pain Wisecracks: 1) Describe the most common sites of disc protrusion with their
All About? What is Sciatica. Disclaimer. Integrated web marketing. Multimedia Health Education
 What is Sciatica All About? Disclaimer This movie is an educational resource only and should not be used to manage sciatica. All decisions about the management of sciatica must be made in conjunction with
What is Sciatica All About? Disclaimer This movie is an educational resource only and should not be used to manage sciatica. All decisions about the management of sciatica must be made in conjunction with
The ABC s of LUMBAR SPINE DISEASE
 The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery URMC Neurosurgery APP s Objectives Identify the most common pathology that leads to spine
The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery URMC Neurosurgery APP s Objectives Identify the most common pathology that leads to spine
Minimally Invasive Discectomy/ Decompression
 Minimally Invasive Discectomy/ Decompression What Is A Minimally Invasive Lumbar Discectomy? A lumbar discectomy is a surgical procedure that involves relieving the pressure placed on nerve roots and/or
Minimally Invasive Discectomy/ Decompression What Is A Minimally Invasive Lumbar Discectomy? A lumbar discectomy is a surgical procedure that involves relieving the pressure placed on nerve roots and/or