CRPS is a multiple system output, activated by the pain neuromatrix (brain map) in response to perceived threat. CRPS OPTA June 2016
|
|
|
- Christian Gaines
- 5 years ago
- Views:
Transcription


 in response to")


1 Kory Zimney, PT, DPT, CSMT Many VERY smart people have contributed to this I am dumbing it down because that is the only way I understand it Will all neuroscientists, neurobiologists and immunologists please leave A LOT remains unknown about CRPS CRPS is a multiple system output, activated by the pain neuromatrix (brain map) in response to perceived threat Adapted from Moseley GL. A pain neuromatrix approach to patients with chronic pain. Man Ther. Aug 2003;8(3): Pain in combination with sensory, autonomic, trophic and motor abnormalities. CRPS-1: Nerve lesion cannot be identified CRPS-2: Nerve lesion can be identified 5 6


 and swollen (Veldman 1993).")

2 Criticism of CRPS 1 and CRPS 2 Fracture or surgery - damage peripheral nerve, but usually Dx as CRPS 1 Nerve degeneration causes CRPS-1? Other causes of neuropathic pain are frequently associated with a loss of C-fiber peripheral terminals, the specificity of these findings with respect to CRPS is questionable (Devigili). Our understanding of CRPS has increased substantially in the past decade. Three major pathophysiological pathways: 1. Aberrant inflammatory mechanisms 2. Vasomotor dysfunction 3. Maladaptive neuroplasticity. Between-individual variability 7 8 After minor or moderate tissue injury (i.e., a wrist fracture). In the acute phase, the injured limb is usually extremely painful, red, warm (although sometimes it quickly becomes cold) and swollen (Veldman 1993) Allodynia (non-painful stimuli evoke pain) Hyperalgesia (painful stimuli evoke more intense pain than usual) Changes in sweating Changes in hair and nail growth Muscle weakness Mechanical and thermal hyperalgesia are frequently present Pain often spreads Voluntary motor control is reduced Hyperpathia Negative sensory signs Hypoesthesia (reduced sense of touch) Hypoalgesia (decreased sensitivity to painful stimuli) Hypothermesthesia (abnormally decreased sensitivity to heat) 11 12
 and can even")
 Diagnosis according to the Budapest criteria - grouping of")


3 Mixture of noxious sensations and sensory loss Over months: Warm limb becomes cold Dystonia Tremor Myoclonus Activity of the limb: exacerbates signs and symptoms Over time, clinical features spread proximally (but not distally) and can even emerge on the opposite or ipsilateral limb Diagnosis of CRPS: Orlando criteria International Association for the Study of Pain Modified version called the Budapest criteria (panel) Diagnosis according to the Budapest criteria - grouping of signs and symptoms into four distinct categories Unclear 5 cases per person-years in the USA 26 per person-years in the Netherlands. Might expect that new cases of CRPS would be identified per year in the USA. Incidence increases with age until 70 years of age, and 3 4 times more women than men are affected. The arm is affected in about 60% of cases and the leg in about 40%. Resolution rate: Ranging from 74% in the first year to 36% within 6 years
.")




4 Fractures (about 45%), sprain (about 18%), and elective surgery (about 12%) are the most frequently reported triggering events. Spontaneous-onset CRPS - uncommon (<10% of cases). Associated with substantial disability, loss of quality of life, and personal and societal economic burden Lots of people have fractures, injuries and surgery and DO NOT develop CRPS Some individuals are more susceptible than others. 1. Psychological factors 2. Immobilization of injured limb 3. Epidemiological factors 4. Genetic factors Compelling evidence that patients with CRPS are more anxious and depressed than healthy control individuals. Whether patients with CRPS are more anxious and depressed than patients with other chronic pain syndromes is unclear No evidence of psychological risk factors for CRPS onset A large population-based case control study reported no difference in psychological variables between those who developed CRPS after trauma Recent prospective multi center cohort study consecutive patients with a fracture reported that none of the psychological factors predicted the development of CRPS-1. The popular presumption that anxiety and depression predispose to CRPS is incorrect
: Mechano sensitivity Thermo sensitivity, Perceptual disturbances reported in people whose limb was subsequently immobilized for 24")


5 Immobilization - risk factor for CRPS. Topical application of capsaicin (induces neurogenic inflammation): Mechano sensitivity Thermo sensitivity, Perceptual disturbances reported in people whose limb was subsequently immobilized for 24 h, but not in people whose limb was not immobilized (Moseley GL, unpublished). The signs rapidly resolved once the limb was moved again. Angiotensin-converting-enzyme inhibitors at the time of trauma and a history of migraine or asthma - associated with increased risk of developing CRPS. Migraine - risk factor for CRPS Both of these risk factors implicate inflammation: angiotensin-converting-enzyme inhibitors increase the availability of substance P and bradykinin, which are important mediators of inflammation, and migraine and asthma share an underlying mechanism of neurogenic inflammation with CRPS Fracture - more favorable course than soft tissue injury Gender does not seem to affect prognosis Women > men: risk for more severe form of CRPS Cold CRPS: Worse prognosis than warm CRPS Longitudinal study 1549 nearly consecutive patients who presented with wrist fracture and who were managed non-surgically were assessed within 1 week of their fracture and then followed up 4 months later (Moseley GL, unpublished). Mean pain intensity over the past 2 days (> 5/10): Red flag for CRPS CRPS sometimes occurs in several family members and siblings of young-onset cases have an increased risk of developing the syndrome Suggest potential genetic predisposition to CRPS Need more research 1. Anxiety/depression no 2. Immobilization after fracture yes 3. Neurogenic inflammation yes 4. High level ofacute pain yes 5. Genetics likely 6. Gender, fracture, etc. not compelling 29 30



6 A neuroscience explanation of these risk factors is needed to start the understanding the vast neurobiological and neurophysiological processes that underpin the development and maintenance of CRPS Electrical Activity 31 Action Potential Voltage Various kinds of channels Every 48 hours







7 Genetic Coding DNA mrna Proteins DNA mrna Proteins Distribution of ion channels Removing myelin Mechanical Immune Chemical Sensitization Louw A, Butler DS. Chronic Pain. In: S.B. B, Manske R, eds. Clinical Orthopaedic Rehabilitation. 3rd Edition ed. Philadelphia, PA: Elsevier; Genetics/family ion channel expression Stress/Anxiety High level of initial pain adrenaline ion channels Fracture, surgery, sprain adrenaline ion channels Temperature sensitization ion channels Female/male -? Hormonal/ion channels Extreme sensitization nerve up-regulation Spreading pain connected nervous system Immobilization movement channels More to come 42






8 Three major pathophysiological pathways: 1. Aberrant inflammatory mechanisms 2. Vasomotor dysfunction 3. Maladaptive neuroplasticity Minor tissue trauma increase cytokine signaling in the injured tissue Cytokines and nerve growth factor (NGF) wake up nociceptors and increase nerve sensitivity Tissues Bradykinin Prostaglandin Serotonin Nerves Nerve Growth Factor Neurokines Noradrenalin Immune Cells Macrophages Cytokines 48
.")


9 Activation of cutaneous nociceptors can induce retrograde depolarization of small-diameter primary afferents (axon reflex), causing the release of neuropeptides such as substance P and calcitonin-gene-related peptide (CGRP). Neuropeptides - vasodilation extravasation in the tissue: and protein Neurogenic inflammation Redness, warm and swelling Substance P Serum concentrations of CGRP and substance P higher in patients with CRPS than in healthy control individuals. Elevated CGRP release is probably responsible for the augmented flare response in patients with CRPS Substance P CGRP CGRP leads to autonomic changes locally primarily, hyperhidrosis. Substance P also involved in increasing osteoclastic activity locally. Substance P CGRP Mechanism for neurogenic inflammation Substance P produces greater extravasation in both the affected and the unaffected limbs of patients with CRPS than in control individuals. Facilitated cutaneous neuropeptide signaling contributes directly to the enhanced extravasation, limb edema, and increased cytokine expression that are present in CRPS
10 Concentrations of TNFα and interleukin-6 (IL- 6) in blister fluid are greater in the CRPSaffected limb than the unaffected one. TNFα and IL-6 concentrations are also higher in skin biopsies from patients with CRPS than in patients with fracture who do not have CRPS. Cytokine changes are associated with the extent of mechanical hyperalgesia Mechanical hyperalgesia Hallmark of central sensitization Excitability of neurons in the spinal cord is increased Inflammatory cytokines: Acts locally in the limb Sensitization of secondary nociceptive neurons in the spinal cord or by glial neuronal interaction Substance P release Capillaries open Swelling Warmth 59 60




.")
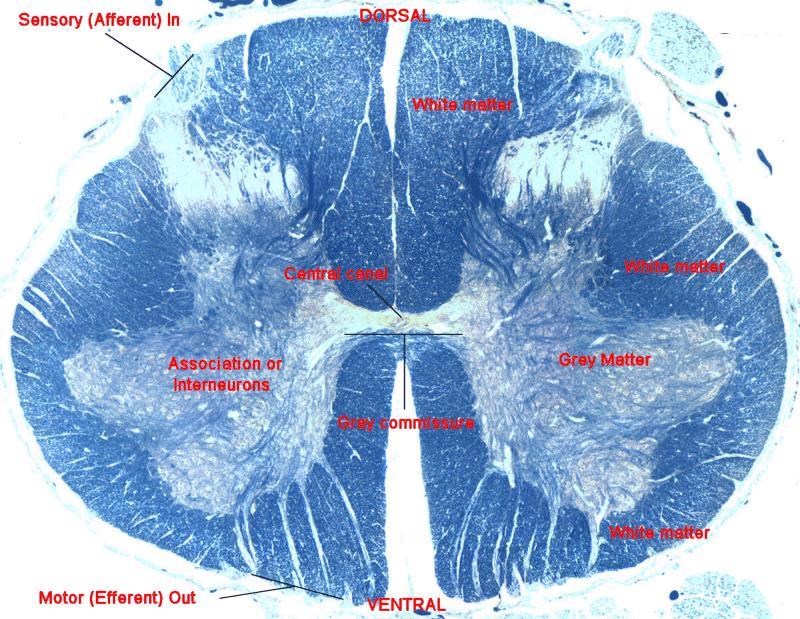
11 Substance P Mast cells degranulation Histamine Increased Enzyme activity Dorsal root ganglion non-myelinated Action potential develop due to adrenaline Nerve fires.both ways Image from Elsevier Medical 63 Common in CRPS Affected limb: Usually warmer than the healthy limb early on Colder than the healthy limb later Temperature shift - activity in vasoconstrictor neurons Three distinct patterns of temperature change: 1. Warm type 2. Intermediate type 3. Cold type Warm type Affected limb warmer and skin perfusion values were higher than the contralateral limb (CPRS for a mean of 4 months). Norepinephrine concentrations from the venous effluent above the painful area is lower in the affected limb than in the contralateral one
. Norepinephrine concentrations lower on the affected side.")
12 Intermediate type Temperature and perfusion either warmer or colder, depending on the amount of sympathetic activity (mean disease duration of 15 months). Cold type Temperature and perfusion in the affected limb consistently lower than those in the contralateral limb (mean of 28 months). Norepinephrine concentrations lower on the affected side. Inhibition of cutaneous sympathetic vasoconstrictor neurons Thermoregulatory impairment probably caused by functional changes in the spinal cord, brainstem, or brain that are triggered by the initial trauma There are suggestions that cutaneous sympathetic vasoconstrictor activity returns to normal as CRPS persists, even though the limb becomes cold and bluish. Central disturbances acute Neurovascular transmission chronic About 20% of patients with CRPS have the cold type from the start. These patients not only differ in skin temperature but also in sensory symptoms and history The sympathetic nervous system, in addition to its effect on peripheral circulation in CRPS, might also contribute to pain. Nociceptors develop catecholamine sensitivity, probably as a result of decreased activity of cutaneous sympathetic vasoconstrictor neurons. Norepinephrine released by the sympathetic nerve fibers activate or sensitize the altered afferent neurons. Changes in the endothelium play a part in impaired peripheral circulation in chronic CRPS. Endothelial dysfunction is associated with a decreased ability to release endothelial nitric oxide, which leads to sustained vasoconstriction. Decreased concentrations of nitric oxide have been noted in CRPS




13 Maybe you can start seeing why it is COMPLEX regional pain syndrome International Journal of Genius




14 What is 1 + 1? C fibers A-Beta fibers 79 Second Order Nociceptive Specific Second Order Wide Dynamic Ranging Neuron Second Order Nociceptive Specific Other Side Sympathetic Second Order Wide Dynamic Ranging Neuron A-Beta fibers A-Beta fibers Other Levels Interneuron Interneuron C fibers C fibers VS. Distortion or suppress non-noxious sensations Loss of an inhibitory influence of normal cutaneous sensations 84

15 The CNS undergoes functional and structural changes in people with persistent pain Central Sensitization Sensitized spinal nociceptive neurons become: More responsive to peripheral input Might even fire in the absence of such input Central sensitization can cause chronic pain, hyperalgesia, and allodynia, as well as the spreading Hyperalgesic priming In some patients a transient insult can lead to chronic pain A transient insult triggers long lasting changes in primary afferent nociceptors that prime them to become hyper-responsive to future mild insults that would normally not evoke pain in the unprimed state. Impaired motor function Common after most injuries but generally resolves In CRPS susceptible patients develop marked movement disorders. Dystonia - most prevalent movement disorder in CRPS Characterized in the arm by persistent flexion postures of the fingers and wrist The risk of dystonia spreading to additional limbs in patients with CRPS increases with the number of limbs that are already dystonic. This accelerated disease course is a typical characteristic of maladaptive neuronal plasticity. CRPS is a brain disorder We have only really covered the periphery to this point We have not even covered the brain yet This is where the MAJOR changes occur 89 90

. 2003. Glasgow, Scotland. 2. Flor, H., The functional organization of the brain in chronic pain, in Progress in Brain Research, Vol 129, J.")
: p. 1-5. 5. Moseley, G.L.")
16 Input to the brain A-Beta fibers Interneuron Second Order Nociceptive Specific Second Order Wide Dynamic Ranging Neuron Initial response: DANGER - Basic protection - Motor - Autonomic C fibers Followed by higher centers, including feelings/processing Initial response: DANGER - Basic protection - Motor - Autonomic Development of a neural signature The Brain s Processing Grandma GRANNY The Brain s processing of LBP Common areas are frequently ignited Via connections, backfiring neurons, and neurotransmitters, pain is perceived the pain neural signature 1. Flor, H. The image of pain. in Annual scientific meeting of The Pain Society (Britain) Glasgow, Scotland. 2. Flor, H., The functional organization of the brain in chronic pain, in Progress in Brain Research, Vol 129, J. Sandkühler, B. Bromm, and G.F. Gebhart, Editors. 2000, Elsevier: Amsterdam. 3. Casey, K.L. and M.C. Bushnell, Pain imaging. Pain: Clinical Updates, : p Petrovic, P. and M. Ingvar, Imaging cognitive modulation of pain processing. Pain, (1-2): p Moseley, G.L., Widespread brain activity during an abdominal task markedly reduced after pain physiology education: fmri evaluation of a single patient with chronic low back pain. Aust J Physiother, (1): p


17 Louw A, Butler DS, Diener I, Puentedura E and Peoples, R; 2013 Preoperative Neuroscience Education for Lumbar Radiculopathy: A Single Case fmri Study A TYPICAL PAIN NEUROTAG 1. PREMOTOR/ MOTOR CORTEX organize and prepare movements 2. CINGULATE CORTEX concentration, focusing PREFRONTAL CORTEX problem solving, memory AMYGDALA fear, fear conditioning, addiction 7 5. SENSORY CORTEX sensory discrimination 9 6. HYPOTHALAMUS/ THALAMUS stress responses, autonomic regulation, motivation 7. CEREBELLUM movement and cognition 8. HIPPOCAMPUS memory, spacial recognition, fear conditioning 9. SPINAL CORD gating from the periphery Butler & Moseley 2003 But Denotes synaptic modulation There s more complexity Denotes synaptic modulation Denotes synaptic modulation Beliefs Beliefs Knowledge, logic

18 Denotes synaptic modulation Denotes synaptic modulation Beliefs Knowledge, logic Social context Beliefs Knowledge, logic Social context Anticipated consequences Denotes synaptic modulation Denotes synaptic modulation Beliefs Knowledge, logic Social context Anticipated consequences Other sensory cues Beliefs Knowledge, logic Social context Anticipated consequences Other sensory cues Physical therapy Nerves that fire together wire together Living your pain Nerves that fire together, wire together
19 Living your pain Long Term Potentiation Definition of Pain Pain is an unpleasant sensory and emotional experience which follows actual or potential tissue damage or is described in terms of such damage Definition of Pain: Update Pain is produced by the brain after a person s neural signature has been activated and concluded the body is in danger and action is required (Moseley 2003; Moseley 2007). How Dangerous is this? This is dangerous More information Facilitation Neuronal adaption How Dangerous is this? This is not dangerous Inhibition Endogenous




20 So What? Pain is based on PERCEPTION of threat Any clinical examples of THREAT for CRPS? Write 5 down






21 How about this Internet image? The CNS undergoes functional and structural changes in people with persistent pain. Lead to central sensitization Similar changes occur in structures involved in the emotional aspects of pain Amygdala Anterior cingulate Prefrontal cortex 12 2 Enter the homunculus Activation and up-regulation of glutamate receptors, which enhance signal transmission in the nociceptive circuitry from the spinal cord to the cerebral cortex Glutamate excitatory neurotransmitter 70% of all brain synapses are glutamate synapses People with longstanding CRPS tend to perceive their affected limb to be larger than it really is. CRPS patient believes the hand feels 107% bigger Hurts more when it looks bigger Does not move different More swelling when it looks bigger Unaffected side Affected side




22 Smudging 12 7 Image from Butler Image from Butler Distortions of the mental image of their limb Missing components or alterations in shape, posture, and temperature of the whole limb or of discrete parts of the limb. Feelings of hostility or disgust towards the affected limb Feel as though it is a separate entity Foreign body that they would like to have amputated

23 Swelling and pain evoked by movement of the CRPSaffected limb is more severe if patients view a magnified image of the limb; if it looked bigger, it hurt more and became more swollen The perceptual disturbances in CRPS similar to disturbances associated with unilateral neglect after stroke. Patients can perceive touch on the affected limb if they watch the mirror image of the unaffected limb being touched. Acerra & Moseley 2005 Neurology 65; Patients perform poorly on tasks in which they are required to judge the laterality of a pictured limb


 contralateral to the affected limb in patients with CRPS.")
24 17 4 Recent work has suggested that cold-type CRPS is associated with a cold side of space i.e., crossing the arms so that the healthy hand is on the affected side of the midline reduces the temperature of the healthy hand Gallace A, Torta DM, Moseley GL, Iannetti GD. The analgesic effect of crossing the arms. Pain. Jun 2011;152(6): Aware of their altered feelings towards the limb Although they believe that the limb is theirs, they feel as though it is not. Neglect-like disturbances reported in CRPS are a result of: Avoid provocation of pain Altered representation of aspects of the limb Substantial reorganization of the somatotopic map within the primary somatosensory cortex (S1) contralateral to the affected limb in patients with CRPS. Cortical reorganization might explain: The spatial distribution of sensory disturbances in a glove-like or stocking-like pattern, the occurrence of tactile induced referred sensations The perception that the limb is bigger than it really is, and the presence of hemi-sensory deficits


25 Cortical changes also affect the primary motor cortex in patients with CRPS. Decreased inhibitory mechanisms and increased excitability in the contralateral primary motor cortex in patients with CRPS. Widespread impairment of central motor processing in CRPS. Of the 3 major pathophysiological pathways it seems neuroplasticity may be a BIG PART: 1. Aberrant inflammatory mechanisms 2. Vasomotor dysfunction 3. Maladaptive neuroplasticity High levels of acute pain, immobilization and increased inflammation seems to predict CRPS development 2. With the above factors, there is likely an immediate upregulation of the peripheral and central nervous system thus nerves become extra sensitive 3. Nerves fire both ways 4. Nerves firing down to the extremity produce increased inflammatory and immune cells, which causes swelling, heat and sensitivity. These changes likely influence the sensory and motor maps in the brain sees the hand altered and not using the hand. 5. The nervous system fire into the CNS, causing longlasting neuroplastic events culminating in central sensitization. This additionally confuses the brain, leading to changes in the maps related to the specific body part 6. There is an immune response in the blood-spinal cord barrier which alters the brain s view of the hand/foot 7. Thoughts are nerve impulses and the impulses drive both antidromic (retrograde) depolarization leading to persistent inflammation and central nervous system plasticity changes The whole brain processes all the danger and thus busy with pain, leading to changes in various output systems, including motor control, immune and endocrine system 9. Maps of the body parts are altered in the brain (CNS, visual, peripheral and immune system altering the bloodbrain barrier), resulting in the extremity looking different usually larger and problem discerning left and right 10. With increased confusion, the brain bring in its most potent defender: PAIN

26 Are these complex biological processes going on in your patient? 1. Perform an in-depth subjective examination, especially the deeper pain questions to establish 2. Use outcome measures that have been validated and able to provide reliable, objective measures, specifically to function 3. Realize that traditional movement-based examinations such as ROM and strength may be too difficult for patients to perform due to the severe pain and sensitivity



27 Fear Definition: A distressing negative sensation induced by a perceived threat. FABQ Clinical Fear Avoidance Model Pull back Do less Increased fear Could also be emotional overload Choice made Importance of early education? Testing a Sensitive Nervous System? Nijs J, Van Houdenhove B, Oostendorp RA. Recognition of central sensitization in patients with musculoskeletal pain: Application of pain neurophysiology in manual therapy practice. Manual therapy. Apr 2010;15(2): Irrational thoughts Knowledge Limited knowledge Threatening and provocative words; Medical tests; Various opinions; Internet information; Experiences Why do physical tests? CONFIRM diagnosis VERY careful with CRPS patient Physical Tests in CRPS Likely induces ++ fear and anxiety
 ROM in adjacent joints Swelling/tape measure By not doing a physical exam (expected and feared by the CRPS patient)")

28 If you HAVE to: Nerve Palpation (?) ROM in adjacent joints Swelling/tape measure By not doing a physical exam (expected and feared by the CRPS patient) it may actually help with pain Limited sensitivity, specificity and reliability in these patients anyway Away from the hot spot Left/Right Discrimination As long as the brain does not understand the pain and does not even know what left and right is, there is no incentive to reduce it s most potent protector: PAIN



29 As long as pain and sensitivity is so high, the extremity does not want to be touched, moved or used Narrative synthesis of the results, based on effect size, found there was good to very good quality level II evidence that graded motor imagery is effective in reducing pain in adults with CRPS-1, irrespective of the outcome measure used Therapeutic Neuroscience Education Graded Motor Imagery Sensory Discrimination Regular Therapy Sensory integration ROM Function Etc. So the brain understands Restoring the extremity/body part back in the brain Function/ROM Review of the sequence: 1. Therapeutic Neuroscience Education 2. Left/Right Discrimination 3. Motor Imagery 4. Sensory Discrimination and Graphesthesia 5. Mirror Therapy Education Why educate patients in PAIN about anatomy and biomechanics? Why not just teach them more about.pain? Image: Clinical Journal of Genius






30 Biomedical Education Does not explain pain Induces fear Does not include the nervous system, brain or pain processing Origins of Neuroscience Education Patients want to know more about: PAIN The origins of neuroscience education Moseley L. Combined physiotherapy and education is efficacious for chronic low back pain. Aust J Physiother. 2002;48(4): Therapeutic Neuroscience Education Therapeutic Neuroscience Education Emerging research shows that explaining to patients their pain experience from a biological and physiological perspective of how the nervous system/ brain s processes pain allow patients to move better, exercise better, think different about pain, push further into pain, etc. Louw A, Puentedura EJ. Therapeutic Neuroscience Education. Vol 1. Minneapolis, MN: OPTP; Louw A, Diener I, Butler DS, Puentedura EJ. The effect of neuroscience education on pain, disability, anxiety, and stress in chronic musculoskeletal pain. Archives of physical medicine and rehabilitation. Dec 2011;92(12):




:2041-2056.")



31 Efficacy Neuroscience Education Louw A, Diener I, Butler DS, Puentedura EJ. The effect of neuroscience education on pain, disability, anxiety, and stress in chronic musculoskeletal pain. Archives of physical medicine and rehabilitation. Dec 2011;92(12): Louw, Puentedura, et. al 2014 submitted for publication Metaphors and examples Pictures One-on-one Therapist CRPS Essentials: Sensitivity Left/Right issues Brain plasticity What pain means How/why this started




32 Pain is normal, but. Also Why so much pain? Left or Right? Use it or lose it Athletes, musicians Amputees All body parts represented in the brain Normal: Sharp, know where it is CRPS: Fuzzy; Not sure Images from ISPI All body parts represented in the brain Normal: Sharp, know where it is Pain: Fuzzy; Not sure Pain: Left and Right Thinking, worrying, not sure, questions, anger, frustration







33 The good news: Left/Right Your hand Normal hand Restoring the map Want to see something really cool? 1. Develop, recite the MANTRA 2. Explain the SSH to someone Alarm System 2. Alarm System






34 2. Alarm System 2. Waking up the alarm system 2. Waking up the alarm system 2. Alarm System YOUR turn: Draw normal electrical activity Action potential Why Do I Hurt?; Louw 2013 OPTP Extra sensitive nerves 2. Waking up the alarm system 2. Waking up the alarm system House Alarm System Car Alarm Louw, A; Your Nerves Are Having Back Surgery How do you know this? 2. Why did they stay up there? 3. How do we calm it down?









35 2. Waking up the alarm system 2. Waking up the alarm system 1. How do you know this? 2. Why did my nerves stay so sensitive? 2. Waking up the alarm system 3. What do we do about it? 2. Waking up the alarm system 3A: Education A: Education B: Exercise C: Medicine 2. Waking up the alarm system 3B: Exercise - Blood and Oxygen 2. Waking up the alarm system 3C: Medication







36 2. Waking up the alarm system 2. Waking up the alarm system 3C: Medication Recovery 3. Nerve Sensors 3. Nerve Sensors 3. Nerve Sensors 3. Nerve Sensors Examples



37 3. Nerve Sensors 3. Nerve Sensors What can be done? EDUCATION: Example Phase 2: Laterality Left/right discrimination is the accuracy and speed of identifying whether a picture or body part is a right or left Magazines Make flash cards Internet images Take photos Make a PowerPoint noigroup.com Flashcards Online Smartphone publications


 Hands versus")





38 Cards Internet Images GOAL: Under 3 seconds > 80% accurate (? 90) Hands versus feet Dyslexia 10-20% no shift; move on Emotions L/R should be continued Injury, pain and immobilization Why do you yawn, when you see someone else yawning? Easiest way to start urinating? 26 2
 Static")






39 The story of the monkeys Imagine extremity (see it visually) Static Dynamic Doing tasks Giving the brain map exercise without moving the extra sensitive extremity Been used for years in Sport Very important potential role in acute/severe pain Ask patient for top 10 tasks needed to be performed with painful extremity Find 10 such activities/images on the Internet Draw card; imagine static hand in that position Imagine moving hand to similar position Imagine performing the task Repeat; repeat; repeat




40 Why discrimination and not integration? If you know your neighbors, you can find your house Patient Example CRPS Face






41 Patient Example Hypersensitive feet s/p MVC Beans Introduce (visual) the sensation of beans Deliberate Close eyes form a memory Add other objects Teach what they should feel like Into the beans go hunt!


 and post hand surgery pain (Rosen and Lundborg 2005).")

42 If it was only this simple Using mirrors to trick the brain Have to restore L and R first If not confusion = more pain Slowly expose the patient to image There is good evidence for the use of mirror therapy alone for acute CRPS (McCabe, Haigh et al. 2003; McCabe, Haigh et al. 2004) There are case reports of successful mirror therapy management of CRPS (Karmarker and Lieberman 2006) and post hand surgery pain (Rosen and Lundborg 2005). Benefits of mirror box therapy with cognitive behavioural therapy demonstrated in three patients with CRPS1. (Vladimir Tichelar, Geertzen et al. 2007) Prepare the patient TNE Emotional Sit evenly No jewelry? Cover tatoos Outside (normal) hand works If bilateral: Least affected = normal side







43 CRPS 29 5







44 Therapeutic Neuroscience Education Graded Motor Imagery Sensory Discrimination Regular Therapy Sensory integration ROM Function Etc. Acute




45 30 5 Kory.zimney@usd.edu Tina, Tyler, Ella, and Lanie Zimney Dr. Adriaan Louw Dr. Louie Puentedura ISPI/EIM staff and faculty University of South Dakota Nova Southeastern University
Use of Therapeutic Neuroscience Education to address Psychosocial Factors Associated with Acute Low Back Pain: A Case Report
 Use of Therapeutic Neuroscience Education to address Psychosocial Factors Associated with Acute Low Back Pain: A Case Report Physiotherapy Theory and Practice (in press) Kory Zimney, PT, DPT, CSMT YOUR
Use of Therapeutic Neuroscience Education to address Psychosocial Factors Associated with Acute Low Back Pain: A Case Report Physiotherapy Theory and Practice (in press) Kory Zimney, PT, DPT, CSMT YOUR
PAIN MANAGEMENT in the CANINE PATIENT
 PAIN MANAGEMENT in the CANINE PATIENT Laurie Edge-Hughes, BScPT, MAnimSt (Animal Physio), CAFCI, CCRT Part 1: Laurie Edge-Hughes, BScPT, MAnimSt (Animal Physio), CAFCI, CCRT 1 Pain is the most common reason
PAIN MANAGEMENT in the CANINE PATIENT Laurie Edge-Hughes, BScPT, MAnimSt (Animal Physio), CAFCI, CCRT Part 1: Laurie Edge-Hughes, BScPT, MAnimSt (Animal Physio), CAFCI, CCRT 1 Pain is the most common reason
Receptors and Neurotransmitters: It Sounds Greek to Me. Agenda. What We Know About Pain 9/7/2012
 Receptors and Neurotransmitters: It Sounds Greek to Me Cathy Carlson, PhD, RN Northern Illinois University Agenda We will be going through this lecture on basic pain physiology using analogies, mnemonics,
Receptors and Neurotransmitters: It Sounds Greek to Me Cathy Carlson, PhD, RN Northern Illinois University Agenda We will be going through this lecture on basic pain physiology using analogies, mnemonics,
211MDS Pain theories
 211MDS Pain theories Definition In 1986, the International Association for the Study of Pain (IASP) defined pain as a sensory and emotional experience associated with real or potential injuries, or described
211MDS Pain theories Definition In 1986, the International Association for the Study of Pain (IASP) defined pain as a sensory and emotional experience associated with real or potential injuries, or described
Somatic Sensation (MCB160 Lecture by Mu-ming Poo, Friday March 9, 2007)
") Somatic Sensation (MCB160 Lecture by Mu-ming Poo, Friday March 9, 2007) Introduction Adrian s work on sensory coding Spinal cord and dorsal root ganglia Four somatic sense modalities Touch Mechanoreceptors
Somatic Sensation (MCB160 Lecture by Mu-ming Poo, Friday March 9, 2007) Introduction Adrian s work on sensory coding Spinal cord and dorsal root ganglia Four somatic sense modalities Touch Mechanoreceptors
Pathophysiology of Pain. Ramon Go MD Assistant Professor Anesthesiology and Pain medicine NYP-CUMC
 Pathophysiology of Pain Ramon Go MD Assistant Professor Anesthesiology and Pain medicine NYP-CUMC Learning Objectives Anatomic pathway of nociception Discuss the multiple target sites of pharmacological
Pathophysiology of Pain Ramon Go MD Assistant Professor Anesthesiology and Pain medicine NYP-CUMC Learning Objectives Anatomic pathway of nociception Discuss the multiple target sites of pharmacological
Pathophysiology of Pain
 Pathophysiology of Pain Wound Inflammatory response Chemical mediators Activity in Pain Path PAIN http://neuroscience.uth.tmc.edu/s2/chapter08.html Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University
Pathophysiology of Pain Wound Inflammatory response Chemical mediators Activity in Pain Path PAIN http://neuroscience.uth.tmc.edu/s2/chapter08.html Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University
Pain Pathways. Dr Sameer Gupta Consultant in Anaesthesia and Pain Management, NGH
 Pain Pathways Dr Sameer Gupta Consultant in Anaesthesia and Pain Management, NGH Objective To give you a simplistic and basic concepts of pain pathways to help understand the complex issue of pain Pain
Pain Pathways Dr Sameer Gupta Consultant in Anaesthesia and Pain Management, NGH Objective To give you a simplistic and basic concepts of pain pathways to help understand the complex issue of pain Pain
Neuropathic pain, pain matrix dysfunction, and pain syndromes
 Neuropathic pain, pain matrix dysfunction, and pain syndromes MSTN121 - Neurophysiology Session 3 Department of Myotherapy Session objectives Describe the mechanism of nociceptive chronic pain. Define
Neuropathic pain, pain matrix dysfunction, and pain syndromes MSTN121 - Neurophysiology Session 3 Department of Myotherapy Session objectives Describe the mechanism of nociceptive chronic pain. Define
Stanmore Therapy Service Approach to Management of Phantom Pain in the Post-operative Phase
 Stanmore Therapy Service Approach to Management of Phantom Pain in the Post-operative Phase Jennifer Fulton Physiotherapy Clinical Specialist in Amputee Rehabilitation PHANTOM LIMB PHENOMENON Truly it
Stanmore Therapy Service Approach to Management of Phantom Pain in the Post-operative Phase Jennifer Fulton Physiotherapy Clinical Specialist in Amputee Rehabilitation PHANTOM LIMB PHENOMENON Truly it
Therapeutic Neuroscience Eduction Know Pain; Know Gain
 Therapeutic Neuroscience Eduction Know Pain; Know Gain Kory Zimney, PT, DPT, CSMT, CAFS without permission 1 10 Visits 64 year old lady with 3 years of CLBP Numerous treatments Numerous clinicians Pain
Therapeutic Neuroscience Eduction Know Pain; Know Gain Kory Zimney, PT, DPT, CSMT, CAFS without permission 1 10 Visits 64 year old lady with 3 years of CLBP Numerous treatments Numerous clinicians Pain
Maria Polaczuk Occupational Therapist Wellington Regional Pain Management Service Graded Motor Imagery
 Maria Polaczuk Occupational Therapist Wellington Regional Pain Management Service 2014 Graded Motor Imagery Introduction Whenever we get a referral for a patient with a unilateral or neuropathic pain condition,
Maria Polaczuk Occupational Therapist Wellington Regional Pain Management Service 2014 Graded Motor Imagery Introduction Whenever we get a referral for a patient with a unilateral or neuropathic pain condition,
ANAT2010. Concepts of Neuroanatomy (II) S2 2018
 S2 2018") ANAT2010 Concepts of Neuroanatomy (II) S2 2018 Table of Contents Lecture 13: Pain and perception... 3 Lecture 14: Sensory systems and visual pathways... 11 Lecture 15: Techniques in Neuroanatomy I in vivo
ANAT2010 Concepts of Neuroanatomy (II) S2 2018 Table of Contents Lecture 13: Pain and perception... 3 Lecture 14: Sensory systems and visual pathways... 11 Lecture 15: Techniques in Neuroanatomy I in vivo
Lesson 14. The Nervous System. Introduction to Life Processes - SCI 102 1
 Lesson 14 The Nervous System Introduction to Life Processes - SCI 102 1 Structures and Functions of Nerve Cells The nervous system has two principal cell types: Neurons (nerve cells) Glia The functions
Lesson 14 The Nervous System Introduction to Life Processes - SCI 102 1 Structures and Functions of Nerve Cells The nervous system has two principal cell types: Neurons (nerve cells) Glia The functions
Pain. Pain. Pain: One definition. Pain: One definition. Pain: One definition. Pain: One definition. Psyc 2906: Sensation--Introduction 9/27/2006
 Pain Pain Pain: One Definition Classic Paths A new Theory Pain and Drugs According to the international Association for the Study (Merskey & Bogduk, 1994), Pain is an unpleasant sensory and emotional experience
Pain Pain Pain: One Definition Classic Paths A new Theory Pain and Drugs According to the international Association for the Study (Merskey & Bogduk, 1994), Pain is an unpleasant sensory and emotional experience
ANAT2010. Concepts of Neuroanatomy (II) S2 2018
 S2 2018") ANAT2010 Concepts of Neuroanatomy (II) S2 2018 Table of Contents Lecture 13: Pain and perception... 3 Lecture 14: Sensory systems and visual pathways... 11 Lecture 15: Techniques in Neuroanatomy I in vivo
ANAT2010 Concepts of Neuroanatomy (II) S2 2018 Table of Contents Lecture 13: Pain and perception... 3 Lecture 14: Sensory systems and visual pathways... 11 Lecture 15: Techniques in Neuroanatomy I in vivo
PSYC& 100: Biological Psychology (Lilienfeld Chap 3) 1
 1") PSYC& 100: Biological Psychology (Lilienfeld Chap 3) 1 1 What is a neuron? 2 Name and describe the functions of the three main parts of the neuron. 3 What do glial cells do? 4 Describe the three basic
PSYC& 100: Biological Psychology (Lilienfeld Chap 3) 1 1 What is a neuron? 2 Name and describe the functions of the three main parts of the neuron. 3 What do glial cells do? 4 Describe the three basic
Pain and Temperature Objectives
 Pain and Temperature Objectives 1. Describe the types of sensory receptors that transmit pain and temperature. 2. Understand how axon diameter relates to transmission of pain and temp information. 3. Describe
Pain and Temperature Objectives 1. Describe the types of sensory receptors that transmit pain and temperature. 2. Understand how axon diameter relates to transmission of pain and temp information. 3. Describe
The Nervous System and the Endocrine System
 The Nervous System and the Endocrine System Neurons: The Building Blocks of the Nervous System Nervous System The electrochemical communication system of the body Sends messages from the brain to the
The Nervous System and the Endocrine System Neurons: The Building Blocks of the Nervous System Nervous System The electrochemical communication system of the body Sends messages from the brain to the
Human Nervous System. The nervous system has three functions
 Chapter 37 Human Nervous System The nervous system has three functions 1) Receive sensory input from both external and internal stimuli 2) Perform integration. (Coordinating all of the various inputs of
Chapter 37 Human Nervous System The nervous system has three functions 1) Receive sensory input from both external and internal stimuli 2) Perform integration. (Coordinating all of the various inputs of
The Nervous System IN DEPTH
 The Nervous System IN DEPTH The right half of the brain controls the left half of the body. This means that only left handed people are in their right mind. Note taking tips Make sure that you have written
The Nervous System IN DEPTH The right half of the brain controls the left half of the body. This means that only left handed people are in their right mind. Note taking tips Make sure that you have written
biological psychology, p. 40 The study of the nervous system, especially the brain. neuroscience, p. 40
 biological psychology, p. 40 The specialized branch of psychology that studies the relationship between behavior and bodily processes and system; also called biopsychology or psychobiology. neuroscience,
biological psychology, p. 40 The specialized branch of psychology that studies the relationship between behavior and bodily processes and system; also called biopsychology or psychobiology. neuroscience,
A Patient s Guide to Pain Management: Complex Regional Pain Syndrome
 A Patient s Guide to Pain Management: Complex Regional Pain Syndrome Suite 11-13/14/15 Mount Elizabeth Medical Center 3 Mount Elizabeth Singapore, 228510 Phone: (65) 6738 2628 Fax: (65) 6738 2629 DISCLAIMER:
A Patient s Guide to Pain Management: Complex Regional Pain Syndrome Suite 11-13/14/15 Mount Elizabeth Medical Center 3 Mount Elizabeth Singapore, 228510 Phone: (65) 6738 2628 Fax: (65) 6738 2629 DISCLAIMER:
Sensory coding and somatosensory system
 Sensory coding and somatosensory system Sensation and perception Perception is the internal construction of sensation. Perception depends on the individual experience. Three common steps in all senses
Sensory coding and somatosensory system Sensation and perception Perception is the internal construction of sensation. Perception depends on the individual experience. Three common steps in all senses
Basic Neuroscience. Sally Curtis
 The Physiology of Pain Basic Neuroscience Sally Curtis sac3@soton.ac.uk The behaviour of humans is a result of the actions of nerves. Nerves form the basis of Thoughts, sensations and actions both reflex
The Physiology of Pain Basic Neuroscience Sally Curtis sac3@soton.ac.uk The behaviour of humans is a result of the actions of nerves. Nerves form the basis of Thoughts, sensations and actions both reflex
A Patient s Guide to Pain Management: Complex Regional Pain Syndrome
 A Patient s Guide to Pain Management: Complex Regional Pain Syndrome 950 Breckinridge Lane Suite 220 Louisville, KY 40223 Phone: 502.708.2940 DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Pain Management: Complex Regional Pain Syndrome 950 Breckinridge Lane Suite 220 Louisville, KY 40223 Phone: 502.708.2940 DISCLAIMER: The information in this booklet is compiled from
Unit 3: The Biological Bases of Behaviour
 Unit 3: The Biological Bases of Behaviour Section 1: Communication in the Nervous System Section 2: Organization in the Nervous System Section 3: Researching the Brain Section 4: The Brain Section 5: Cerebral
Unit 3: The Biological Bases of Behaviour Section 1: Communication in the Nervous System Section 2: Organization in the Nervous System Section 3: Researching the Brain Section 4: The Brain Section 5: Cerebral
Chapter 14: The Cutaneous Senses
 Chapter 14: The Cutaneous Senses Somatosensory System There are three parts Cutaneous senses - perception of touch and pain from stimulation of the skin Proprioception - ability to sense position of the
Chapter 14: The Cutaneous Senses Somatosensory System There are three parts Cutaneous senses - perception of touch and pain from stimulation of the skin Proprioception - ability to sense position of the
Seizure: the clinical manifestation of an abnormal and excessive excitation and synchronization of a population of cortical
 Are There Sharing Mechanisms of Epilepsy, Migraine and Neuropathic Pain? Chin-Wei Huang, MD, PhD Department of Neurology, NCKUH Basic mechanisms underlying seizures and epilepsy Seizure: the clinical manifestation
Are There Sharing Mechanisms of Epilepsy, Migraine and Neuropathic Pain? Chin-Wei Huang, MD, PhD Department of Neurology, NCKUH Basic mechanisms underlying seizures and epilepsy Seizure: the clinical manifestation
Overview of Questions
 Overview of Questions What are the sensors in the skin, what do they respond to and how is this transmitted to the brain? How does the brain represent touch information? What is the system for sensing
Overview of Questions What are the sensors in the skin, what do they respond to and how is this transmitted to the brain? How does the brain represent touch information? What is the system for sensing
synapse neurotransmitters Extension of a neuron, ending in branching terminal fibers, through which messages pass to other neurons, muscles, or glands
 neuron synapse The junction between the axon tip of a sending neuron and the dendrite of a receiving neuron Building block of the nervous system; nerve cell Chemical messengers that cross the synaptic
neuron synapse The junction between the axon tip of a sending neuron and the dendrite of a receiving neuron Building block of the nervous system; nerve cell Chemical messengers that cross the synaptic
By the end of this lecture the students will be able to:
 UNIT VII: PAIN Objectives: By the end of this lecture the students will be able to: Review the concept of somatosensory pathway. Describe the function of Nociceptors in response to pain information. Describe
UNIT VII: PAIN Objectives: By the end of this lecture the students will be able to: Review the concept of somatosensory pathway. Describe the function of Nociceptors in response to pain information. Describe
CHAPTER 10 THE SOMATOSENSORY SYSTEM
 CHAPTER 10 THE SOMATOSENSORY SYSTEM 10.1. SOMATOSENSORY MODALITIES "Somatosensory" is really a catch-all term to designate senses other than vision, hearing, balance, taste and smell. Receptors that could
CHAPTER 10 THE SOMATOSENSORY SYSTEM 10.1. SOMATOSENSORY MODALITIES "Somatosensory" is really a catch-all term to designate senses other than vision, hearing, balance, taste and smell. Receptors that could
Applied Neuroscience. Conclusion of Science Honors Program Spring 2017
 Applied Neuroscience Conclusion of Science Honors Program Spring 2017 Review Circle whichever is greater, A or B. If A = B, circle both: I. A. permeability of a neuronal membrane to Na + during the rise
Applied Neuroscience Conclusion of Science Honors Program Spring 2017 Review Circle whichever is greater, A or B. If A = B, circle both: I. A. permeability of a neuronal membrane to Na + during the rise
Our senses provide us with wonderful capabilities. If you had to lose one, which would it be?
 Our senses provide us with wonderful capabilities. If you had to lose one, which would it be? Neurological disorders take away sensation without a choice! http://neuroscience.uth.tmc.edu/s2/chapter04.html
Our senses provide us with wonderful capabilities. If you had to lose one, which would it be? Neurological disorders take away sensation without a choice! http://neuroscience.uth.tmc.edu/s2/chapter04.html
Somatosensation. Recording somatosensory responses. Receptive field response to pressure
 Somatosensation Mechanoreceptors that respond to touch/pressure on the surface of the body. Sensory nerve responds propotional to pressure 4 types of mechanoreceptors: Meissner corpuscles & Merkel discs
Somatosensation Mechanoreceptors that respond to touch/pressure on the surface of the body. Sensory nerve responds propotional to pressure 4 types of mechanoreceptors: Meissner corpuscles & Merkel discs
Name: Period: Test Review: Chapter 2
 Name: Period: Test Review: Chapter 2 1. The function of dendrites is to A) receive incoming signals from other neurons. B) release neurotransmitters into the spatial junctions between neurons. C) coordinate
Name: Period: Test Review: Chapter 2 1. The function of dendrites is to A) receive incoming signals from other neurons. B) release neurotransmitters into the spatial junctions between neurons. C) coordinate
(Based on work of Adriaan Louw, PT, PhD, CSMT and others at ISPI, and at NOI group)
") Therapeutic Neuroscience Education Highlights (Based on work of Adriaan Louw, PT, PhD, CSMT and others at ISPI, and at NOI group) Importance of understanding pain better Pain that is understood is not
Therapeutic Neuroscience Education Highlights (Based on work of Adriaan Louw, PT, PhD, CSMT and others at ISPI, and at NOI group) Importance of understanding pain better Pain that is understood is not
BodyinMind.org. CRPS symposium June 2011
 BodyinMind.org CRPS symposium June 2011 Acute injury rehabilitation Chronic pain management Acute injury CRPS Chronic pain Injury 6 weeks 3 months Convention Acute injury rehabilitation Chronic pain management
BodyinMind.org CRPS symposium June 2011 Acute injury rehabilitation Chronic pain management Acute injury CRPS Chronic pain Injury 6 weeks 3 months Convention Acute injury rehabilitation Chronic pain management
Therapeutic Neuroscience Education Highlights
 Therapeutic Neuroscience Education Highlights (adapted from TNE course taught by Adriaan Louw, PT, PhD, CSMT, co-founder of ISPI, (ispinstitute.com) with permission, by Laura Pizer Gueron, PT) lgueron@gillettechildrens.com
Therapeutic Neuroscience Education Highlights (adapted from TNE course taught by Adriaan Louw, PT, PhD, CSMT, co-founder of ISPI, (ispinstitute.com) with permission, by Laura Pizer Gueron, PT) lgueron@gillettechildrens.com
Somatosensory Physiology (Pain And Temperature) Richard M. Costanzo, Ph.D.
 Richard M. Costanzo, Ph.D.") Somatosensory Physiology (Pain And Temperature) Richard M. Costanzo, Ph.D. OBJECTIVES After studying the material of this lecture the student should be familiar with: 1. The relationship between nociception
Somatosensory Physiology (Pain And Temperature) Richard M. Costanzo, Ph.D. OBJECTIVES After studying the material of this lecture the student should be familiar with: 1. The relationship between nociception
Pain teaching. Muhammad Laklouk
 Pain teaching Muhammad Laklouk Definition Pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage. Sensory (discriminatiory)
Pain teaching Muhammad Laklouk Definition Pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage. Sensory (discriminatiory)
Western Montana Pain Symposium Treating Persistent Pain Does Not Need to Be Painful Improving Outcomes through Pain Education
 Western Montana Pain Symposium Treating Persistent Pain Does Not Need to Be Painful Improving Outcomes through Pain Education Nora Stern, PT, MS PT Providence Persistent Pain Project Program Manager Portland,
Western Montana Pain Symposium Treating Persistent Pain Does Not Need to Be Painful Improving Outcomes through Pain Education Nora Stern, PT, MS PT Providence Persistent Pain Project Program Manager Portland,
The Nervous System. Anatomy of a Neuron
 The Nervous System Chapter 38.1-38.5 Anatomy of a Neuron I. Dendrites II. Cell Body III. Axon Synaptic terminal 1 Neuron Connections dendrites cell body terminal cell body cell body terminals dendrites
The Nervous System Chapter 38.1-38.5 Anatomy of a Neuron I. Dendrites II. Cell Body III. Axon Synaptic terminal 1 Neuron Connections dendrites cell body terminal cell body cell body terminals dendrites
Chapter 17. Nervous System Nervous systems receive sensory input, interpret it, and send out appropriate commands. !
 Chapter 17 Sensory receptor Sensory input Integration Nervous System Motor output Brain and spinal cord Effector cells Peripheral nervous system (PNS) Central nervous system (CNS) 28.1 Nervous systems
Chapter 17 Sensory receptor Sensory input Integration Nervous System Motor output Brain and spinal cord Effector cells Peripheral nervous system (PNS) Central nervous system (CNS) 28.1 Nervous systems
Nervous System C H A P T E R 2
 Nervous System C H A P T E R 2 Input Output Neuron 3 Nerve cell Allows information to travel throughout the body to various destinations Receptive Segment Cell Body Dendrites: receive message Myelin sheath
Nervous System C H A P T E R 2 Input Output Neuron 3 Nerve cell Allows information to travel throughout the body to various destinations Receptive Segment Cell Body Dendrites: receive message Myelin sheath
What is Pain? An unpleasant sensory and emotional experience associated with actual or potential tissue damage. Pain is always subjective
 Pain & Acupuncture What is Pain? An unpleasant sensory and emotional experience associated with actual or potential tissue damage. NOCICEPTION( the neural processes of encoding and processing noxious stimuli.)
Pain & Acupuncture What is Pain? An unpleasant sensory and emotional experience associated with actual or potential tissue damage. NOCICEPTION( the neural processes of encoding and processing noxious stimuli.)
The biochemical origin of pain: The origin of all pain is inflammation and the inflammatory response: Inflammatory profile of pain syndromes
 The biochemical origin of pain: The origin of all pain is inflammation and the inflammatory response: Inflammatory profile of pain syndromes 1 Medical Hypothesis 2007, Vol. 69, pp. 1169 1178 Sota Omoigui
The biochemical origin of pain: The origin of all pain is inflammation and the inflammatory response: Inflammatory profile of pain syndromes 1 Medical Hypothesis 2007, Vol. 69, pp. 1169 1178 Sota Omoigui
Chapter 8. The Nervous System
 Chapter 8 The Nervous System The Nervous System Consists of the Central and Peripheral Nervous Systems Principle Parts of Nervous System Central Nervous System (CNS) Components: brain and spinal cord
Chapter 8 The Nervous System The Nervous System Consists of the Central and Peripheral Nervous Systems Principle Parts of Nervous System Central Nervous System (CNS) Components: brain and spinal cord
Guided Reading Activities
 Name Period Chapter 28: Nervous Systems Guided Reading Activities Big idea: Nervous system structure and function Answer the following questions as you read modules 28.1 28.2: 1. Your taste receptors for
Name Period Chapter 28: Nervous Systems Guided Reading Activities Big idea: Nervous system structure and function Answer the following questions as you read modules 28.1 28.2: 1. Your taste receptors for
Prof Wayne Derman MBChB,BSc (Med)(Hons) PhD, FFIMS. Pain Management in the Elite Athlete: The 2017 IOC Consensus Statement
(Hons) PhD, FFIMS. Pain Management in the Elite Athlete: The 2017 IOC Consensus Statement") Prof Wayne Derman MBChB,BSc (Med)(Hons) PhD, FFIMS Pain Management in the Elite Athlete: The 2017 IOC Consensus Statement 2 as 20 Experts published and leaders in their respective field 12 month lead in
Prof Wayne Derman MBChB,BSc (Med)(Hons) PhD, FFIMS Pain Management in the Elite Athlete: The 2017 IOC Consensus Statement 2 as 20 Experts published and leaders in their respective field 12 month lead in
Name: Period: Chapter 2 Reading Guide The Biology of Mind
 Name: Period: Chapter 2 Reading Guide The Biology of Mind The Nervous System (pp. 55-58) 1. What are nerves? 2. Complete the diagram below with definitions of each part of the nervous system. Nervous System
Name: Period: Chapter 2 Reading Guide The Biology of Mind The Nervous System (pp. 55-58) 1. What are nerves? 2. Complete the diagram below with definitions of each part of the nervous system. Nervous System
Visualizing Psychology
 Visualizing Psychology by Siri Carpenter & Karen Huffman PowerPoint Lecture Notes Presentation Chapter 2: Neuroscience and Biological Foundations Siri Carpenter, Yale University Karen Huffman, Palomar
Visualizing Psychology by Siri Carpenter & Karen Huffman PowerPoint Lecture Notes Presentation Chapter 2: Neuroscience and Biological Foundations Siri Carpenter, Yale University Karen Huffman, Palomar
Cephalization. Nervous Systems Chapter 49 11/10/2013. Nervous systems consist of circuits of neurons and supporting cells
 Nervous Systems Chapter 49 Cephalization Nervous systems consist of circuits of neurons and supporting cells Nervous system organization usually correlates with lifestyle Organization of the vertebrate
Nervous Systems Chapter 49 Cephalization Nervous systems consist of circuits of neurons and supporting cells Nervous system organization usually correlates with lifestyle Organization of the vertebrate
Pharmacology of Pain Transmission and Modulation
 Pharmacology of Pain Transmission and Modulation 2 Jürg Schliessbach and Konrad Maurer Nociceptive Nerve Fibers Pain is transmitted to the central nervous system via thinly myelinated Aδ and unmyelinated
Pharmacology of Pain Transmission and Modulation 2 Jürg Schliessbach and Konrad Maurer Nociceptive Nerve Fibers Pain is transmitted to the central nervous system via thinly myelinated Aδ and unmyelinated
MYOFASCIAL PAIN. Dr. Janet Travell ( ) credited with bringing MTrPs to the attention of healthcare providers.
 credited with bringing MTrPs to the attention of healthcare providers.") Myofascial Trigger Points background info Laurie Edge-Hughes BScPT, MAnimSt (Animal Physio), CAFCI, CCRT History lesson Dr. Janet Travell (1901 1997) credited with bringing MTrPs to the attention of healthcare
Myofascial Trigger Points background info Laurie Edge-Hughes BScPT, MAnimSt (Animal Physio), CAFCI, CCRT History lesson Dr. Janet Travell (1901 1997) credited with bringing MTrPs to the attention of healthcare
The Physiology of the Senses Chapter 8 - Muscle Sense
 The Physiology of the Senses Chapter 8 - Muscle Sense www.tutis.ca/senses/ Contents Objectives... 1 Introduction... 2 Muscle Spindles and Golgi Tendon Organs... 3 Gamma Drive... 5 Three Spinal Reflexes...
The Physiology of the Senses Chapter 8 - Muscle Sense www.tutis.ca/senses/ Contents Objectives... 1 Introduction... 2 Muscle Spindles and Golgi Tendon Organs... 3 Gamma Drive... 5 Three Spinal Reflexes...
UNDERSTANDING AND DEALING WITH PAIN. Lorimer Moseley Talk. Disclosure. Patient C.C. Patient C.C. Goals 06/12/2017
 UNDERSTANDING AND DEALING WITH PAIN DAVID V. SMITH MD CHKD SPORTS MEDICINE Lorimer Moseley Talk https://www.youtube.com/watch?v=gwdwldihjs&feature=youtu.be ALEXANDRA LARAMEE, LCSW CHKD BEHAVIORAL HEALTH
UNDERSTANDING AND DEALING WITH PAIN DAVID V. SMITH MD CHKD SPORTS MEDICINE Lorimer Moseley Talk https://www.youtube.com/watch?v=gwdwldihjs&feature=youtu.be ALEXANDRA LARAMEE, LCSW CHKD BEHAVIORAL HEALTH
1. Processes nutrients and provides energy for the neuron to function; contains the cell's nucleus; also called the soma.
 1. Base of brainstem; controls heartbeat and breathing 2. tissue destruction; a brain lesion is a naturally or experimentally caused destruction of brain tissue 3. A thick band of axons that connects the
1. Base of brainstem; controls heartbeat and breathing 2. tissue destruction; a brain lesion is a naturally or experimentally caused destruction of brain tissue 3. A thick band of axons that connects the
Medical Neuroscience Tutorial
 Pain Pathways Medical Neuroscience Tutorial Pain Pathways MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. NCC3. Genetically determined circuits are the foundation
Pain Pathways Medical Neuroscience Tutorial Pain Pathways MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. NCC3. Genetically determined circuits are the foundation
PAIN IS A SUBJECTIVE EXPERIENCE: It is not a stimulus. MAJOR FEATURES OF THE PAIN EXPERIENCE: Sensory discriminative Affective (emotional) Cognitive
 Cognitive") PAIN PAIN IS A SUBJECTIVE EXPERIENCE: It is not a stimulus MAJOR FEATURES OF THE PAIN EXPERIENCE: Sensory discriminative Affective (emotional) Cognitive MEASUREMENT OF PAIN: A BIG PROBLEM Worst pain ever
PAIN PAIN IS A SUBJECTIVE EXPERIENCE: It is not a stimulus MAJOR FEATURES OF THE PAIN EXPERIENCE: Sensory discriminative Affective (emotional) Cognitive MEASUREMENT OF PAIN: A BIG PROBLEM Worst pain ever
Primary Functions. Monitor changes. Integrate input. Initiate a response. External / internal. Process, interpret, make decisions, store information
 NERVOUS SYSTEM Monitor changes External / internal Integrate input Primary Functions Process, interpret, make decisions, store information Initiate a response E.g., movement, hormone release, stimulate/inhibit
NERVOUS SYSTEM Monitor changes External / internal Integrate input Primary Functions Process, interpret, make decisions, store information Initiate a response E.g., movement, hormone release, stimulate/inhibit
Warm-Up. Label the parts of the neuron below.
 Warm-Up Label the parts of the neuron below. A B C D E F G Warm-Up 1. One neuron transmits a nerve impulse at 40 m/s. Another conducts at the rate of 1 m/s. Which neuron has a myelinated axon? 2. List
Warm-Up Label the parts of the neuron below. A B C D E F G Warm-Up 1. One neuron transmits a nerve impulse at 40 m/s. Another conducts at the rate of 1 m/s. Which neuron has a myelinated axon? 2. List
Mechanism of Pain Production
 Mechanism of Pain Production Pain conducting nerve fibers are small myelinated (A-delta) or unmyelinated nerve fibers (C-fibers). Cell bodies are in the dorsal root ganglia (DRG) or sensory ganglia of
Mechanism of Pain Production Pain conducting nerve fibers are small myelinated (A-delta) or unmyelinated nerve fibers (C-fibers). Cell bodies are in the dorsal root ganglia (DRG) or sensory ganglia of
Biomechanics of Pain: Dynamics of the Neuromatrix
 Biomechanics of Pain: Dynamics of the Neuromatrix Partap S. Khalsa, D.C., Ph.D. Department of Biomedical Engineering The Neuromatrix From: Melzack R (1999) Pain Suppl 6:S121-6. NIOSH STAR Symposium May
Biomechanics of Pain: Dynamics of the Neuromatrix Partap S. Khalsa, D.C., Ph.D. Department of Biomedical Engineering The Neuromatrix From: Melzack R (1999) Pain Suppl 6:S121-6. NIOSH STAR Symposium May
Outline. Animals: Nervous system. Neuron and connection of neurons. Key Concepts:
 Animals: Nervous system Neuron and connection of neurons Outline 1. Key concepts 2. An Overview and Evolution 3. Human Nervous System 4. The Neurons 5. The Electrical Signals 6. Communication between Neurons
Animals: Nervous system Neuron and connection of neurons Outline 1. Key concepts 2. An Overview and Evolution 3. Human Nervous System 4. The Neurons 5. The Electrical Signals 6. Communication between Neurons
Biological Process 9/7/10. (a) Anatomy: Neurons have three basic parts. 1. The Nervous System: The communication system of your body and brain
 Anatomy: Neurons have three basic parts. 1. The Nervous System: The communication system of your body and brain") Biological Process Overview 1. The Nervous System: s (a) Anatomy, (b) Communication, (c) Networks 2. CNS/PNS 3. The Brain (a) Anatomy, (b) Localization of function 4. Methods to study the brain (Dr. Heidenreich)
Biological Process Overview 1. The Nervous System: s (a) Anatomy, (b) Communication, (c) Networks 2. CNS/PNS 3. The Brain (a) Anatomy, (b) Localization of function 4. Methods to study the brain (Dr. Heidenreich)
Foreword...xi. Overview of the Pain Mechanism Classification System and Mechanical Diagnosis and Therapy...17
 Table of Contents Foreword...xi CHAPTER 1 Musculoskeletal Pain: The Big Picture... 1 Complex and Chronic Nature of Musculoskeletal Pain...2 Factors Correlated with Musculoskeletal Pain...2 Socioeconomic
Table of Contents Foreword...xi CHAPTER 1 Musculoskeletal Pain: The Big Picture... 1 Complex and Chronic Nature of Musculoskeletal Pain...2 Factors Correlated with Musculoskeletal Pain...2 Socioeconomic
The Somatosensory System
 The Somatosensory System Reading: BCP Chapter 12 cerebrovortex.com Divisions of the Somatosensory System Somatosensory System Exteroceptive External stimuli Proprioceptive Body position Interoceptive Body
The Somatosensory System Reading: BCP Chapter 12 cerebrovortex.com Divisions of the Somatosensory System Somatosensory System Exteroceptive External stimuli Proprioceptive Body position Interoceptive Body
Somatic Sensory System I. Background
 Somatic Sensory System I. Background A. Differences between somatic senses and other senses 1. Receptors are distributed throughout the body as opposed to being concentrated at small, specialized locations
Somatic Sensory System I. Background A. Differences between somatic senses and other senses 1. Receptors are distributed throughout the body as opposed to being concentrated at small, specialized locations
MANAGING CHRONIC PAIN
 George Hardas MANAGING CHRONIC PAIN The guide to understanding chronic pain and how to manage it. George Hardas MMed (UNSW) MScMed (Syd) MChiro (Macq) BSc (Syd) Grad Cert Pain Management (Syd) Cognitive
George Hardas MANAGING CHRONIC PAIN The guide to understanding chronic pain and how to manage it. George Hardas MMed (UNSW) MScMed (Syd) MChiro (Macq) BSc (Syd) Grad Cert Pain Management (Syd) Cognitive
Biology 3201 Quiz on Nervous System. Total 33 points
 Biology 3201 Quiz on Nervous System Total 33 points Name: Circle the best response to the following: (33 points) 1. What do we call the long fibre that carries impulses away from the nerve cell body? A.
Biology 3201 Quiz on Nervous System Total 33 points Name: Circle the best response to the following: (33 points) 1. What do we call the long fibre that carries impulses away from the nerve cell body? A.
Pain and impulse conduction
 1 Pain and impulse conduction L.H.D.J. Booij According to the World Health Organisation pain is defined as an unpleasant sensation that occurs from imminent tissue damage. From a physiological perspective,
1 Pain and impulse conduction L.H.D.J. Booij According to the World Health Organisation pain is defined as an unpleasant sensation that occurs from imminent tissue damage. From a physiological perspective,
NEURONS ARE ORGANIZED INTO NERVOUS SYSTEMS 34.5
 NEURONS ARE ORGANIZED INTO NERVOUS SYSTEMS 34.5 INTRODUCTION The cnidarians have nerve nets, the most simple type of nervous system. The sea anemone has a nerve net that serves simple behaviours such as
NEURONS ARE ORGANIZED INTO NERVOUS SYSTEMS 34.5 INTRODUCTION The cnidarians have nerve nets, the most simple type of nervous system. The sea anemone has a nerve net that serves simple behaviours such as
Spinal Cord Injury Pain. Michael Massey, DO CentraCare Health St Cloud, MN 11/07/2018
 Spinal Cord Injury Pain Michael Massey, DO CentraCare Health St Cloud, MN 11/07/2018 Objectives At the conclusion of this session, participants should be able to: 1. Understand the difference between nociceptive
Spinal Cord Injury Pain Michael Massey, DO CentraCare Health St Cloud, MN 11/07/2018 Objectives At the conclusion of this session, participants should be able to: 1. Understand the difference between nociceptive
Pain. Types of Pain. Types of Pain 8/21/2013
 Pain 1 Types of Pain Acute Pain Complex combination of sensory, perceptual, & emotional experiences as a result of a noxious stimulus Mediated by rapidly conducting nerve pathways & associated with increased
Pain 1 Types of Pain Acute Pain Complex combination of sensory, perceptual, & emotional experiences as a result of a noxious stimulus Mediated by rapidly conducting nerve pathways & associated with increased
PART IV: NEUROPATHIC PAIN SYNDROMES JILL SINDT FEBRUARY 7, 2019
 PART IV: NEUROPATHIC PAIN SYNDROMES JILL SINDT FEBRUARY 7, 2019 NEUROPATHIC PAIN PAIN ARISING AS DIRECT CONSEQUENCE OF A LESION OR DISEASE AFFECTING THE SOMATOSENSORY SYSTEM AFFECTS 3-8% OF POPULATION
PART IV: NEUROPATHIC PAIN SYNDROMES JILL SINDT FEBRUARY 7, 2019 NEUROPATHIC PAIN PAIN ARISING AS DIRECT CONSEQUENCE OF A LESION OR DISEASE AFFECTING THE SOMATOSENSORY SYSTEM AFFECTS 3-8% OF POPULATION
San Francisco Chronicle, June 2001
 PAIN San Francisco Chronicle, June 2001 CONGENITAL INSENSITIVITY TO PAIN PAIN IS A SUBJECTIVE EXPERIENCE: It is not a stimulus MAJOR FEATURES OF THE PAIN EXPERIENCE: Sensory discriminative Affective (emotional)
PAIN San Francisco Chronicle, June 2001 CONGENITAL INSENSITIVITY TO PAIN PAIN IS A SUBJECTIVE EXPERIENCE: It is not a stimulus MAJOR FEATURES OF THE PAIN EXPERIENCE: Sensory discriminative Affective (emotional)
Movement management of low back pain Dr Neil Langridge DClinP MSc MMACP MCSP
 Movement management of low back pain Dr Neil Langridge DClinP MSc MMACP MCSP What underlies LBP? MRI Disc degeneration = 91% Loss of disc height = 51% Disc bulges = 64% Disc protrusion = 32% Annular tear
Movement management of low back pain Dr Neil Langridge DClinP MSc MMACP MCSP What underlies LBP? MRI Disc degeneration = 91% Loss of disc height = 51% Disc bulges = 64% Disc protrusion = 32% Annular tear
Biology 12 Human Biology - The Nervous System Name. Main reference: Biology Concepts and Connects Sixth edition Chapter 28
 Biology 12 Human Biology - The Nervous System Name Main reference: Biology Concepts and Connects Sixth edition Chapter 28 Vocabulary acetylcholine (ACh), acetylcholinesterase (AChE), action potential,
Biology 12 Human Biology - The Nervous System Name Main reference: Biology Concepts and Connects Sixth edition Chapter 28 Vocabulary acetylcholine (ACh), acetylcholinesterase (AChE), action potential,
Physiology of Tactile Sensation
 Physiology of Tactile Sensation Objectives: 1. Describe the general structural features of tactile sensory receptors how are first order nerve fibers specialized to receive tactile stimuli? 2. Understand
Physiology of Tactile Sensation Objectives: 1. Describe the general structural features of tactile sensory receptors how are first order nerve fibers specialized to receive tactile stimuli? 2. Understand
Psychology in Your Life
 Sarah Grison Todd Heatherton Michael Gazzaniga Psychology in Your Life SECOND EDITION Chapter 2 The Role of Biology in Psychology 1 2016 W. W. Norton & Company, Inc. 2.1 How Do Our Nervous Systems Affect
Sarah Grison Todd Heatherton Michael Gazzaniga Psychology in Your Life SECOND EDITION Chapter 2 The Role of Biology in Psychology 1 2016 W. W. Norton & Company, Inc. 2.1 How Do Our Nervous Systems Affect
The Nervous System. Nervous System Functions 1. gather sensory input 2. integration- process and interpret sensory input 3. cause motor output
 The Nervous System Nervous System Functions 1. gather sensory input 2. integration- process and interpret sensory input 3. cause motor output The Nervous System 2 Parts of the Nervous System 1. central
The Nervous System Nervous System Functions 1. gather sensory input 2. integration- process and interpret sensory input 3. cause motor output The Nervous System 2 Parts of the Nervous System 1. central
Brain and behaviour (Wk 6 + 7)
") Brain and behaviour (Wk 6 + 7) What is a neuron? What is the cell body? What is the axon? The basic building block of the nervous system, the individual nerve cell that receives, processes and transmits
Brain and behaviour (Wk 6 + 7) What is a neuron? What is the cell body? What is the axon? The basic building block of the nervous system, the individual nerve cell that receives, processes and transmits
Function of the Nervous System
 Nervous System Function of the Nervous System Receive sensory information, interpret it, and send out appropriate commands to form a response Composed of neurons (functional unit of the nervous system)
Nervous System Function of the Nervous System Receive sensory information, interpret it, and send out appropriate commands to form a response Composed of neurons (functional unit of the nervous system)
Neurons, Synapses and Signaling. Chapter 48
 Neurons, Synapses and Signaling Chapter 48 Warm Up Exercise What types of cells can receive a nerve signal? Nervous Organization Neurons- nerve cells. Brain- organized into clusters of neurons, called
Neurons, Synapses and Signaling Chapter 48 Warm Up Exercise What types of cells can receive a nerve signal? Nervous Organization Neurons- nerve cells. Brain- organized into clusters of neurons, called
Basic Nervous System anatomy. Neurobiology of Happiness
 Basic Nervous System anatomy Neurobiology of Happiness The components Central Nervous System (CNS) Brain Spinal Cord Peripheral" Nervous System (PNS) Somatic Nervous System Autonomic Nervous System (ANS)
Basic Nervous System anatomy Neurobiology of Happiness The components Central Nervous System (CNS) Brain Spinal Cord Peripheral" Nervous System (PNS) Somatic Nervous System Autonomic Nervous System (ANS)
Anatomical Substrates of Somatic Sensation
 Anatomical Substrates of Somatic Sensation John H. Martin, Ph.D. Center for Neurobiology & Behavior Columbia University CPS The 2 principal somatic sensory systems: 1) Dorsal column-medial lemniscal system
Anatomical Substrates of Somatic Sensation John H. Martin, Ph.D. Center for Neurobiology & Behavior Columbia University CPS The 2 principal somatic sensory systems: 1) Dorsal column-medial lemniscal system
Duplex Theory of Texture Perception
 Duplex Theory of Texture Perception Katz (1925) proposed that perception of texture depends on two cues: Spatial cues are determined by the size, shape, and distribution of surface elements Temporal cues
Duplex Theory of Texture Perception Katz (1925) proposed that perception of texture depends on two cues: Spatial cues are determined by the size, shape, and distribution of surface elements Temporal cues
NERVOUS SYSTEM C H A P T E R 2 8
 NERVOUS SYSTEM C H A P T E R 2 8 CAN AN INJURED SPINAL CORD BE FIXED? Injuries to the spinal cord disrupt communication between the central nervous system (brain and spinal cord) and the rest of the body
NERVOUS SYSTEM C H A P T E R 2 8 CAN AN INJURED SPINAL CORD BE FIXED? Injuries to the spinal cord disrupt communication between the central nervous system (brain and spinal cord) and the rest of the body
ANATOMY AND PHYSIOLOGY OF NEURONS. AP Biology Chapter 48
 ANATOMY AND PHYSIOLOGY OF NEURONS AP Biology Chapter 48 Objectives Describe the different types of neurons Describe the structure and function of dendrites, axons, a synapse, types of ion channels, and
ANATOMY AND PHYSIOLOGY OF NEURONS AP Biology Chapter 48 Objectives Describe the different types of neurons Describe the structure and function of dendrites, axons, a synapse, types of ion channels, and
Neural Integration I: Sensory Pathways and the Somatic Nervous System
 15 Neural Integration I: Sensory Pathways and the Somatic Nervous System PowerPoint Lecture Presentations prepared by Jason LaPres Lone Star College North Harris An Introduction to Sensory Pathways and
15 Neural Integration I: Sensory Pathways and the Somatic Nervous System PowerPoint Lecture Presentations prepared by Jason LaPres Lone Star College North Harris An Introduction to Sensory Pathways and
The anatomy and physiology of pain
 The anatomy and physiology of pain Charlotte E Steeds Abstract Pain is an unpleasant experience that results from both physical and psychological responses to injury. A complex set of pathways transmits
The anatomy and physiology of pain Charlotte E Steeds Abstract Pain is an unpleasant experience that results from both physical and psychological responses to injury. A complex set of pathways transmits
Chapter 11 Introduction to the Nervous System and Nervous Tissue Chapter Outline
 Chapter 11 Introduction to the Nervous System and Nervous Tissue Chapter Outline Module 11.1 Overview of the Nervous System (Figures 11.1-11.3) A. The nervous system controls our perception and experience
Chapter 11 Introduction to the Nervous System and Nervous Tissue Chapter Outline Module 11.1 Overview of the Nervous System (Figures 11.1-11.3) A. The nervous system controls our perception and experience
Nervous System (cont)
") Nervous System (cont) Dopamine Deals with motor movement and alertness. Lack of dopamine has been linked to Parkinson s disease. Too much has been linked to schizophrenia. Endorphins Involved in pain control.
Nervous System (cont) Dopamine Deals with motor movement and alertness. Lack of dopamine has been linked to Parkinson s disease. Too much has been linked to schizophrenia. Endorphins Involved in pain control.
Cortical Control of Movement
 Strick Lecture 2 March 24, 2006 Page 1 Cortical Control of Movement Four parts of this lecture: I) Anatomical Framework, II) Physiological Framework, III) Primary Motor Cortex Function and IV) Premotor
Strick Lecture 2 March 24, 2006 Page 1 Cortical Control of Movement Four parts of this lecture: I) Anatomical Framework, II) Physiological Framework, III) Primary Motor Cortex Function and IV) Premotor
Phantom limb pain. Advice for amputee patients
 Phantom limb pain Advice for amputee patients The purpose of this information leaflet is to increase your understanding of phantom pain. All pain sufferers benefit from knowing more and understanding the
Phantom limb pain Advice for amputee patients The purpose of this information leaflet is to increase your understanding of phantom pain. All pain sufferers benefit from knowing more and understanding the
Chapter 6 Section 1. The Nervous System: The Basic Structure
 Chapter 6 Section 1 The Nervous System: The Basic Structure Essential Question: How does studying the biology of the brain give us an understanding of our behavior? Draw or type 2 things you already know
Chapter 6 Section 1 The Nervous System: The Basic Structure Essential Question: How does studying the biology of the brain give us an understanding of our behavior? Draw or type 2 things you already know