Update on IBD. Dr Richard POLLOK Consultant Gastroenterologist and Honorary Senior Lecturer. Queen Mary s Hospital. St George s Hospital
|
|
|
- Jack Glenn
- 5 years ago
- Views:
Transcription
1 Update on IBD Dr Richard POLLOK Consultant Gastroenterologist and Honorary Senior Lecturer Queen Mary s Hospital St George s Hospital Parkside Hospital
2 Miss LF, aged 24 Recent diagnosis of distal colitis at FS and confirmed histologically Patient treated elsewhere with prednisolone Presented with BO x5/d with blood and hip pain Cause of hip pain?

3 Avascular necrosis of L femoral head
4 BSG guideline bone protection in IBD All >65: consider bisphosphonate at start of steroid treatment <65 at high risk and steroids >3/12: DEXA and bisphosphonates if T score < 1.5 Give Vit D and Calcium whilst on steroid DEXA scan for those at high risk of osteoporosis: (1) > 10kg wt loss (2) BMI <20 or (3) Age >70

5 UC disease extent Extensive or Pancolitis 37% Left sided ulcerative colitis 37% Distal UC 36% Proctitis




6
7 Topical 5-ASA treatment Proctitis: 5-ASA supps Distal colitis: 5-ASA foam enema L sided colitis: 5-ASA liquid enema Extensive/pancolitis: topical Rx PLUS oral Rx
8

9 Miss LF has an immediate relapsewhat are the options? Further courses of steroids Further courses of topical treatment Add in a thiopurine (azathioprine or 6- mercaptopurine infliximab
10 Azathioprine pathway

11 TPMT activity

12 azathioprine induced neutropaenia Colombel et al 2007
13 Drug monitoring for azathioprine 6MMP zero low high High/norm 6TG zero low Low/normal high Action Poor Compliance OR increase dose Noncompliant Coprescribe alopurinol Reduce dose
14
15 Case Miss JE 22yo female student Pan UC Refractory 2/52 oral pred HR 88, T 37.2 C BO x 12/d bloody Day 1 Hydrocortisone 100 qds Mesalazine 1.2g bd LMW Heparin Hb 13.4 WC 8.9 ESR 45 Alb 40 CRP 39 Stool MC&S NEG AXR mucosal oedema
16 Day 3 Poor clinical response CRP 33 BO x 6/d Options?
17 Day 3 Increase dose of steroids start ciclosporin 2 mg/kg Start infliximab 5mg/kg colectomy

18 Day 6 Symptoms unchanged CRP 102 Needs colectomy? Yes No Clostridium difficile toxin +VE

19 Clostridium difficile annual rates

20 Jen et al 2011

21 Fidaxomicin versus vancomycin Louie 2011
22 Faecal transplant-rct Vanc 500mg qds 5/7 followed by gut lavage then donor faeces duodenal infusion, n=16 Vanc 500mg qds 14/7, n=13 Vanc 500mg qds 14/7 followed by gut lavage, n=13 Van Nood 2013

23
24 C difficile and IBD majority community acquired Higher rates of carriage in IBD ~8-10% Usually not associated with antibiotic use Associated with steroids and colonic disease Always test on admission Pseudo-membranes uncommon Co-infection associated with poorer outcomes
25 Case history aged 16 school boy, diagnosed with ileocaecal CD given several # CS over 3 years Strictureplasty, aged 19 Azathioprine initiated post-op Well 6 years, MRE inflammation and mild stenosis noted
26 Case history cont. 1 year later obstructive symptoms and admitted c anorexia and rapid weight loss CT Abdo: ileal stricture and possible entero-enteric fistula Treatment c CS and IFX initiated-good initial response 6/12 later recurrent sub-acute obstuctive symptoms requiring resective

27 Questions What is optimal time to introduce thiopurines-would earlier introduction have avoided surgery? Should anti-tnfs have be introduced before clinical deterioration-would they avoid need for further surgery?

28 Can medical treatment alter disease progression Early treatment Altered progression
29 Kaplan-Meier curve showing time from diagnosis to start of thiopurine therapy in the three gr within 5 years of diagnosis. Group A versus B (p ), Group A versus C (p < ), G Time versus from C (p < diagnosis ) to start of thiopurines Group C ( ) Group B ( ) Group A ( ) Months from diagnosis 5 year cumulative probability increased from 12% (Group A) to 25% (Group C) Number at risk Group A ( ) Group B ( ) Group C ( ) Pollok et al 2012
30 Time from diagnosis to first intestinal surgery 5 year cumulative probability reduced from 14% (Group A) to 9% (Group C) Pollok et al 2012
31 Thiopurines and risk of intestinal surgery in Crohn s diseases Pollok et al 2013 in press

32 Biologics
33 Harvey-Bradshaw score 8 infliximab or adulimimab indicated
34 What Role biologics in altering longterm surgical outcomes? DoH UK 2011
35 Cumulative risk of surgery for IFX patients according to response Combe 2011
36 A midwife with watery diarrhoea 58 yo midwife presented with intermittent watery diarrhoea for 6 months She opens her bowels 3-6/d has had diarrhoea at night. she has lost 3kg. No abnormality was seen at a recent colonoscopy performed elsewhere Options? Colonoscopy with colonic biopsies

37 Collagenous Colitis
38 Microscopic colitis Collagenous colitis Lymphocytic colitis

39
40 Mrs SC Aged 72 History of ulcerative colitis > 20 years BO>6/d c nocturnal symptoms Intolerant to AZA, 6MP and methotrexate Maintained on prednisolone long term >18mo by prior Gastroenterologist No recent investigation Options?
41 Colonoscopy #1 Pan colitis with features of chronic inflammation including inflammatory polyps and a villiform appearance to the mucosa Biopsies confirm above, and x1 biopsy:..indeterminate for dysplasia Treated with IFX x 3 induction infusions and repeat colonoscopy
42 Repeat Colonoscopy Repeat biopsies from flat mucosa reveal changes consistent with high grade dysplasia Options?
43 dysplasia in UC High grade dysplasia Colectomy recommended, up to 40% may have occult CRC Low grade dysplasia Controversial need 2 specialist pathologists 10-30% may develop CRC within 1 year Consider colectomy or 3-6 monthly colonoscopy

44

45 Miss EW, aged 34 Crohn s disease 5 years in stable remission for 3 years on azathioprine Plans to visit S America Attends IBD clinic prior to departure, mentions incidentally she d had yellow fever vaccination that morning at her GP practice Options?
46 Vaccinations in IBD ECCO guidelines 2010
47 Miss JE 26 yo IT specialist with a history of distal colitis Repeated flare-ups with abdo pain, loose stool and occasional fresh blood on paper Receives several course of prednisolone with short-lived benefit FS is normal, Proctoscopy-haemorrhoids Q. what is your diagnosis and how do you approach the problem
48 Prevalence of IBS-like symptoms in IBD Simrén et al. (2002) 57% (23/40) of CD had IBS-like symptoms 33% (14/43) of UC in remission This is 2-3 times higher than in the general population (IBS prevalence = ~15-20%). Assoc. with depression and visits to GP & Gastroenterologist.
49 low FODMAP diet Fermentable Oligosaccharides Disaccharides Monosaccharides And Polyols
50 Excess Fructose Lactose Fructans & Galactans Polyols Apple Pear Peach Watermelon Mango Sugar snap peas Honey High fructose corn syrup Milk (cow, goat & sheep) Yoghurt Cheeses Bread Pasta Couscous Biscuits Cereals Chickpeas Lentils Kidney beans Baked beans Apricot Cherries Plums Prunes Pears Cauliflower Mushrooms Avocado Large serves of: Dried fruit Fruit juice Brocolli Cabbage Brussel sprouts Onion / garlic Sweeteners e.g. Xylitol Sorbitol

51 The FODMAP Hypothesis Loose stools Bloating Small intestine Colon Pain Flatulence
52 Summary A low FODMAP diet is useful in patients with functional symptoms It is supported by high quality studies that show efficacy and mechanisms Better quality trials are needed in patients with IBD
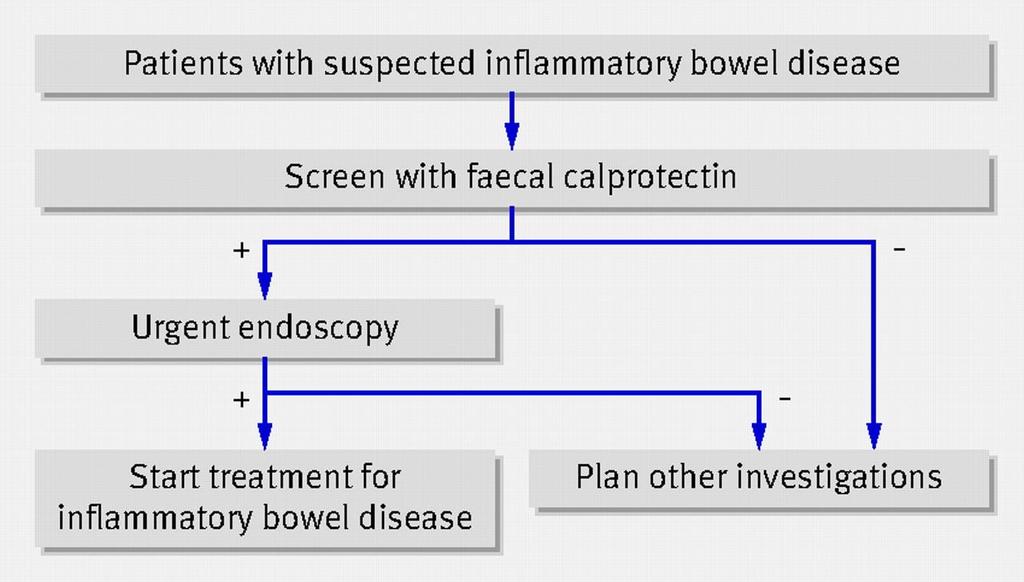
53 Faecal calprotectin To help distinguish between IBD and IBS To assess laboratory disease activity in IBD To assess responses to treatment To assess disease prognosis Research uses
54 Tibble et al 2002
55 In a population with suspected IBD, n=100 (an overall prevalence of IBD 32%) Adults Children true positive true negative false positive 3 9 false negative 2 5 Meta analysis BMJ, 2010
56

57 Dr Richard POLLOK Consultant Gastroenterologist Parkside Hospital SW19 St George s Hospital Queen Mary s Roehampton
58 Calprotectin as a predictor of relapse in IBD U.C < 250 mg/l C.D < 250 mg/l R E M I S S I O N p < C.D > 250 mg/l U.C >250 mg/l Month Gastroenterology 2000;119:15-22

59 Traditional Dietary Recommendations Fibre Manipulation Avoid triggers Fatty Foods Dairy Caffeine Fructose Alcohol Spicy Foods Sweeteners
60 Results 74% (46 patients) reported positive improvements in all abdominal symptoms. However; Retrospective Uncontrolled Regression to the mean? Changes to medication


61 Double-blind, Randomised, Placebo-Controlled Evidence Patients with FM and improved symptoms on LFD (n=25) Runin Wash -out Wash -out Wash -out 14d 14d 14d Fructan Fructose Mix Glucose
62 In summary High level evidence that FODMAPs trigger symptoms in IBS with FM. Symptom severity is dose dependent. 75% of patients improved on the LFD. Improvements are due to restriction of FODMAPs and not placebo alone.
63 Does it work in clinical practice? 62 patients with IBS Educated on a LFD. Telephone interview (2-40 months later). Shepherd & Gibson, 2006
64 Primary Outcome Were your symptoms adequately controlled in this phase? Proportion (%) answering Yes
Irritable Bowel Syndrome
 Irritable Bowel Syndrome Irritable bowel syndrome (IBS) has a variety of symptoms, most commonly cramping, abdominal pain, bloating, constipation, and diarrhea. Symptoms can vary from person to person,
Irritable Bowel Syndrome Irritable bowel syndrome (IBS) has a variety of symptoms, most commonly cramping, abdominal pain, bloating, constipation, and diarrhea. Symptoms can vary from person to person,
What Is the Low-FODMAP Diet?
 LOW-FODMAP DIET What Is the Low-FODMAP Diet? FODMAP refers to a group of five sugars found in certain foods. These sugars are lactose, fructose (in excess), fructans, galactans and polyols. Specifically,
LOW-FODMAP DIET What Is the Low-FODMAP Diet? FODMAP refers to a group of five sugars found in certain foods. These sugars are lactose, fructose (in excess), fructans, galactans and polyols. Specifically,
Diarrhoea for the Acute Physician
 Diarrhoea for the Acute Physician STEPHEN INNS GASTROENTEROLOGIST AND PHYSICIAN HUTT VALLEY DHB August 2013 Outline Case History 1 Initial assessment of acute diarrhoea Management of fulminant UC Management
Diarrhoea for the Acute Physician STEPHEN INNS GASTROENTEROLOGIST AND PHYSICIAN HUTT VALLEY DHB August 2013 Outline Case History 1 Initial assessment of acute diarrhoea Management of fulminant UC Management
It is believed that a meal plan that includes low FODMAPs also may help ease symptoms from other health conditions, such as:
 If you have digestive issues, this could be why. You don't have to have IBS (Irritable Bowel Syndrome) or Colitis (a chronically inflammed colon), to experience some of these symptoms. FODMAP The acronym
If you have digestive issues, this could be why. You don't have to have IBS (Irritable Bowel Syndrome) or Colitis (a chronically inflammed colon), to experience some of these symptoms. FODMAP The acronym
I. Identification Presenters: Date: Name of Organization: Goal Statement: Title of Presentation: Audience Description: Physical Set-up: -
 I. Identification Presenters: Written by Jen Barnes, training will be presented by Cooking Matters managers Date: TBD Name of Organization: Cooking Matters Spring 2013 Contact: Jessica Caouette jcaouette@strength.org
I. Identification Presenters: Written by Jen Barnes, training will be presented by Cooking Matters managers Date: TBD Name of Organization: Cooking Matters Spring 2013 Contact: Jessica Caouette jcaouette@strength.org
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture,
 To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
-2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency
 rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency") SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
Primary & Secondary Care Inflammatory Bowel Disease Pathway February 2018
 South East London Area Prescribing Committee: Primary & Secondary Care Inflammatory Bowel Disease Pathway February 2018 Developed by: South East London IBD Pathway Development Group Approved: February
South East London Area Prescribing Committee: Primary & Secondary Care Inflammatory Bowel Disease Pathway February 2018 Developed by: South East London IBD Pathway Development Group Approved: February
IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital
 IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital Aims To understand the aetiology of IBD To understand the impact that
IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital Aims To understand the aetiology of IBD To understand the impact that
GETTING REAL WITH GUT HEALTH
 THE IMPORTANCE OF YOUR HEALTH STORY Reflections Do you regularly experience any of the following: Indigestion or food repeats on you after you eat Excessive burping or belching following meals Bloating
THE IMPORTANCE OF YOUR HEALTH STORY Reflections Do you regularly experience any of the following: Indigestion or food repeats on you after you eat Excessive burping or belching following meals Bloating
New treatment options in UC. Rob Bryant IBD Consultant Royal Adelaide Hospital
 New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
Implementation of disease and safety predictors during disease management in UC
 Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Irritable Bowel Syndrome
 Irritable Bowel Syndrome A Simple Tool for Identification and Dietary Management Dr Adrian Gilliland, GP and Clinical Advisor Primary Care, Capital and Coast DHB. Dr Rees Cameron, Gastroenterologist, Capital
Irritable Bowel Syndrome A Simple Tool for Identification and Dietary Management Dr Adrian Gilliland, GP and Clinical Advisor Primary Care, Capital and Coast DHB. Dr Rees Cameron, Gastroenterologist, Capital
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
INFLAMMATORY BOWEL DISEASE
 1. Medical Condition INFLAMMATORY BOWEL DISEASE (IBD) specifically includes Crohn s disease (CD) and ulcerative colitis (UC) but also includes IBD unclassified (IBDu), seen in about 10% of cases. These
1. Medical Condition INFLAMMATORY BOWEL DISEASE (IBD) specifically includes Crohn s disease (CD) and ulcerative colitis (UC) but also includes IBD unclassified (IBDu), seen in about 10% of cases. These
WHOLE HEALTH: INFORMATION FOR VETERANS. Eating to Reduce Irritable Bowel Symptoms: The FODMaP Diet
 WHOLE HEALTH: INFORMATION FOR VETERANS Eating to Reduce Irritable Bowel Symptoms: The FODMaP Diet Whole Health is an approach to health care that empowers and enables YOU to take charge of your health
WHOLE HEALTH: INFORMATION FOR VETERANS Eating to Reduce Irritable Bowel Symptoms: The FODMaP Diet Whole Health is an approach to health care that empowers and enables YOU to take charge of your health
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
What s new in IBD? Dr AB Hawthorne Consultant Gastroenterologist University Hospital of Wales Cardiff
 What s new in IBD? Dr AB Hawthorne Consultant Gastroenterologist University Hospital of Wales Cardiff Case: Kelly age 19 Admitted via medical intake to local hospital with D&V for 10 days. Ate take-away
What s new in IBD? Dr AB Hawthorne Consultant Gastroenterologist University Hospital of Wales Cardiff Case: Kelly age 19 Admitted via medical intake to local hospital with D&V for 10 days. Ate take-away
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Doncaster & Bassetlaw Medicines Formulary
 Doncaster & Bassetlaw Medicines Formulary Section 1.5 Chronic Bowel Disorders (including IBD) Aminosalicylates: Mesalazine 400mg and 800mg MR Tablets (Octasa) Mesalazine 1.2g MR Tablets (Mezavant XL) Mesalazine
Doncaster & Bassetlaw Medicines Formulary Section 1.5 Chronic Bowel Disorders (including IBD) Aminosalicylates: Mesalazine 400mg and 800mg MR Tablets (Octasa) Mesalazine 1.2g MR Tablets (Mezavant XL) Mesalazine
Trust Guideline. for Ciclosporin Treatment & Monitoring for Adult* Patients with Acute, Severe Ulcerative Colitis. (*ie aged 16 years and over)
") Trust Guideline for Ciclosporin Treatment & Monitoring for Adult* Patients with Acute, Severe Ulcerative Colitis (*ie aged 16 years and over) abc A guideline recommended for use In: Gastroenterology/Medical
Trust Guideline for Ciclosporin Treatment & Monitoring for Adult* Patients with Acute, Severe Ulcerative Colitis (*ie aged 16 years and over) abc A guideline recommended for use In: Gastroenterology/Medical
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
FODMAPS: Presenta(on Overview
 FODMAPS: Prac%cal Applica%on in Paediatrics Stephanie Brown, NZRD Paediatric Gastroenterology DieFFan Christchurch Public Hospital Presenta(on Overview What are FODMAPs? FODMAP diet and IBS? Foods high
FODMAPS: Prac%cal Applica%on in Paediatrics Stephanie Brown, NZRD Paediatric Gastroenterology DieFFan Christchurch Public Hospital Presenta(on Overview What are FODMAPs? FODMAP diet and IBS? Foods high
IBD Case Studies. David Rowbotham. Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital
 IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
Inflammatory or Irritable? (the bowel, not the speaker)
") South GP CME Edgar Centre, Dunedin August 2014 Inflammatory or Irritable? (the bowel, not the speaker) Dr Jason Hill MBChB FRACP FRCP Edin Department of Gastroenterology, Southern DHB Dunedin School Of
South GP CME Edgar Centre, Dunedin August 2014 Inflammatory or Irritable? (the bowel, not the speaker) Dr Jason Hill MBChB FRACP FRCP Edin Department of Gastroenterology, Southern DHB Dunedin School Of
Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152
 Crohn's disease: management Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Crohn's disease: management Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Dietary advice for people with Inflammatory Bowel Disease
 Dietary advice for people with Inflammatory Bowel Disease Crohn s disease and Ulcerative colitis Information for patients Name Your Dietitian Dietitian contact number: 0118 322 7116 What is Inflammatory
Dietary advice for people with Inflammatory Bowel Disease Crohn s disease and Ulcerative colitis Information for patients Name Your Dietitian Dietitian contact number: 0118 322 7116 What is Inflammatory
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
Achieving Success in Ulcerative Colitis: the Role of Infliximab
 Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Management of the Hospitalized IBD Patient. Drew DuPont MD
 Management of the Hospitalized IBD Patient Drew DuPont MD Ulcerative Colitis: Indications for Admission Severe ulcerative colitis Frequent loose bloody stools ( 6 per day) Severe cramps Systemic toxicity:
Management of the Hospitalized IBD Patient Drew DuPont MD Ulcerative Colitis: Indications for Admission Severe ulcerative colitis Frequent loose bloody stools ( 6 per day) Severe cramps Systemic toxicity:
Dr. Ann Haiden. Your Best Health, Vitality, Life! with bonus FODMAPs food list. The Do s. Get Rid of Sugar, Starches & FODMAPs
 Dr. Ann Haiden Your Best Health, Vitality, Life! 6 IBS Do s Don ts and with bonus FODMAPs food list Try these six tips to break free from IBS! The Do s 1 Get Rid of Sugar, Starches & FODMAPs Remove these
Dr. Ann Haiden Your Best Health, Vitality, Life! 6 IBS Do s Don ts and with bonus FODMAPs food list Try these six tips to break free from IBS! The Do s 1 Get Rid of Sugar, Starches & FODMAPs Remove these
Melbourne GI & Endoscopy
 1 Melbourne GI & Endoscopy Multi-disciplinary care for your patients Gastroenterology Hepatobiliary & upper gastrointestinal surgery Colorectal surgery Oncology Perioperative care One contact & one address
1 Melbourne GI & Endoscopy Multi-disciplinary care for your patients Gastroenterology Hepatobiliary & upper gastrointestinal surgery Colorectal surgery Oncology Perioperative care One contact & one address
ENZYMES: Clinical Considerations in IBS, SIBO, Dysbiosis, and the Leaky Gut
 ENZYMES: Clinical Considerations in IBS, SIBO, Dysbiosis, and the Leaky Gut Michael T. Murray, N.D. AllHealth BeginsintheGut Hippocrates Key Objectives To provide an overview of the key role digestive
ENZYMES: Clinical Considerations in IBS, SIBO, Dysbiosis, and the Leaky Gut Michael T. Murray, N.D. AllHealth BeginsintheGut Hippocrates Key Objectives To provide an overview of the key role digestive
Dietary Interventions for IBS, IBD & Coeliac Disease. Debbie Blissitt Registered Dietitian
 Dietary Interventions for IBS, IBD & Coeliac Disease Debbie Blissitt Registered Dietitian This session will cover 1. Coeliac 2. IBS First Line 3. IBS FODMAP 4. IBD 5. Dietetic Services 6. Questions Coeliac
Dietary Interventions for IBS, IBD & Coeliac Disease Debbie Blissitt Registered Dietitian This session will cover 1. Coeliac 2. IBS First Line 3. IBS FODMAP 4. IBD 5. Dietetic Services 6. Questions Coeliac
Common Questions in Crohn s Disease Therapy. Case
 Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Low FODMAP Diet. OK, but what are FODMAPs and who should avoid them?
 Low FODMAP Diet FODMAP? What does that stand for? Fermentable Oligosaccharides (oligo few, saccharide sugar ) Disaccharides ( two sugars ) Monosaccharides ( one sugar ) And Polyols (these are sugar alcohols)
Low FODMAP Diet FODMAP? What does that stand for? Fermentable Oligosaccharides (oligo few, saccharide sugar ) Disaccharides ( two sugars ) Monosaccharides ( one sugar ) And Polyols (these are sugar alcohols)
Nutrition and IBD. IBD Talk. Presented by. Hannah Price, paediatric dietitian at RHH. Lauren Farquhar, adult dietitian at RHH
 Nutrition and IBD IBD Talk Presented by Hannah Price, paediatric dietitian at RHH Hannah.price@ths.tas.gov.au Lauren Farquhar, adult dietitian at RHH Lauren.farquhar@ths.tas.gov.au Microbiota and IBD The
Nutrition and IBD IBD Talk Presented by Hannah Price, paediatric dietitian at RHH Hannah.price@ths.tas.gov.au Lauren Farquhar, adult dietitian at RHH Lauren.farquhar@ths.tas.gov.au Microbiota and IBD The
Whole Health in Your Practice - Applying CIH March Whole Health in Your Practice 14. APPLYING CIH. Lucky Sarah VETERANS HEALTH ADMINISTRATION
 Whole Health in Your Practice 14. APPLYING CIH Lucky Sarah 1 Not-so-lucky Joe Joe - GI 31 yo Diarrhea predominant IBS after being treated for a GI infection during a tour in Iraq Symptoms: Bloating and
Whole Health in Your Practice 14. APPLYING CIH Lucky Sarah 1 Not-so-lucky Joe Joe - GI 31 yo Diarrhea predominant IBS after being treated for a GI infection during a tour in Iraq Symptoms: Bloating and
Biologics in IBD. Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College
 Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
Nutrition as primary therapy in IBD. Dr Clare Donnellan Leeds General Infirmary
 Nutrition as primary therapy in IBD Dr Clare Donnellan Leeds General Infirmary Case GB 34 year old female Diagnosed with Crohn s in 2002? Extent Offered steroids or surgery Declined both GB Represented
Nutrition as primary therapy in IBD Dr Clare Donnellan Leeds General Infirmary Case GB 34 year old female Diagnosed with Crohn s in 2002? Extent Offered steroids or surgery Declined both GB Represented
Endpoints for Stopping Treatment in UC
 Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Dietary Advice for Inflammatory Bowel Disease in Adults
 Dietary Advice for Inflammatory Bowel Disease in Adults There are two main types of Inflammatory Bowel Disease (IBD): Ulcerative Colitis Crohn s Disease. When you eat and drink, food travels through your
Dietary Advice for Inflammatory Bowel Disease in Adults There are two main types of Inflammatory Bowel Disease (IBD): Ulcerative Colitis Crohn s Disease. When you eat and drink, food travels through your
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Protocol for the management of acute severe ulcerative colitis in children
 Protocol for the management of acute severe ulcerative colitis in children Introduction: Paediatric UC is severe and more extensive than adult onset UC with 6-8% presenting as pancolitis (1,2) Within five
Protocol for the management of acute severe ulcerative colitis in children Introduction: Paediatric UC is severe and more extensive than adult onset UC with 6-8% presenting as pancolitis (1,2) Within five
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Dr David Rowbotham. The Leeds Teaching Hospitals NHS Trust NHS
 Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Useful Titbits from the World of Gastroenterology David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Useful Titbits from the World of Gastroenterology David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
The Best of IBD at UEGW (Crohn s)
") The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
William D. Chey, MD, FACG. Page 1 of ACG Midwest Regional Postgraduate Course Copyright 2016 American College of Gastroenterology
 Dietary and Other Non-pharmacological Management of IBS William D. Chey, MD, FACG Nostrant Professor of Medicine Director GI Nutrition Program University of Michigan Peter Loftus, May 2, 2016 Page 1 of
Dietary and Other Non-pharmacological Management of IBS William D. Chey, MD, FACG Nostrant Professor of Medicine Director GI Nutrition Program University of Michigan Peter Loftus, May 2, 2016 Page 1 of
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 3 October 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
Dietary Options for Inflammatory Bowel Disease
 Dietary Options for Inflammatory Bowel Disease Michael J. Rosen, MD, MSCI Schubert-Martin Inflammatory Bowel Disease Center Learning objectives Worldwide rise in the incidence of IBD The relationship between
Dietary Options for Inflammatory Bowel Disease Michael J. Rosen, MD, MSCI Schubert-Martin Inflammatory Bowel Disease Center Learning objectives Worldwide rise in the incidence of IBD The relationship between
Management and Lifestyle Advice for Adults with Irritable Bowel Syndrome Information for Patients
 Management and Lifestyle Advice for Adults with Irritable Bowel Syndrome Information for Patients 1 This patient information is written to provide patients with information and advice on how to manage
Management and Lifestyle Advice for Adults with Irritable Bowel Syndrome Information for Patients 1 This patient information is written to provide patients with information and advice on how to manage
Dietary advice for people with colostomies
 Dietary advice for people with colostomies Introduction During your surgery, you have had a colostomy formed. Colostomies are formed due to problems in the colon (large bowel). This leaflet is designed
Dietary advice for people with colostomies Introduction During your surgery, you have had a colostomy formed. Colostomies are formed due to problems in the colon (large bowel). This leaflet is designed
IRRITABLE BOWEL SYNDROME
 IRRITABLE BOWEL SYNDROME CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Here are some questions to ask your doctor. WHAT IS IRRITABLE BOWEL SYNDROME? 4
IRRITABLE BOWEL SYNDROME CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Here are some questions to ask your doctor. WHAT IS IRRITABLE BOWEL SYNDROME? 4
Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Case Discussion. Nutrition in IBD. Rémy Meier MD. Ulcerative colitis. Crohn s disease
 26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
Gastroenterologist & Hepatologist Auckland City Hospital Auckland
 Dr David Rowbotham Gastroenterologist & Hepatologist Auckland City Hospital Auckland 14:00-14:55 WS #138: IBD in Primary Care - Practical Management Tips 15:05-16:00 WS #150: IBD in Primary Care - Practical
Dr David Rowbotham Gastroenterologist & Hepatologist Auckland City Hospital Auckland 14:00-14:55 WS #138: IBD in Primary Care - Practical Management Tips 15:05-16:00 WS #150: IBD in Primary Care - Practical
What s New in IBS with Diarrhea. Dr. Geoffrey K. Turnbull, MD April 6, 2018.
 What s New in IBS with Diarrhea Dr. Geoffrey K. Turnbull, MD April 6, 2018. Objectives To learn how to diagnose IBS with particular emphasis on patients who have diarrhea predominantly. Review management
What s New in IBS with Diarrhea Dr. Geoffrey K. Turnbull, MD April 6, 2018. Objectives To learn how to diagnose IBS with particular emphasis on patients who have diarrhea predominantly. Review management
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
What I will cover today
 What I will cover today Cost of IBS and the background to the CCG business case Allergy in FODMAP non-responders Frequently asked questions on the FODMAP diet Case study The reality IBS patients incur
What I will cover today Cost of IBS and the background to the CCG business case Allergy in FODMAP non-responders Frequently asked questions on the FODMAP diet Case study The reality IBS patients incur
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL
 NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
An Evidence-based Approach to Dietary Treatment of Irritable Bowel Syndrome
 An Evidence-based Approach to Dietary Treatment of Irritable Bowel Syndrome American College of Gastroenterology August 2014, Indianapolis Brian E. Lacy, Ph.D., M.D. Professor of Medicine, Geisel School
An Evidence-based Approach to Dietary Treatment of Irritable Bowel Syndrome American College of Gastroenterology August 2014, Indianapolis Brian E. Lacy, Ph.D., M.D. Professor of Medicine, Geisel School
Irritable Bowel Disease. Dr. Alexandra Ilnyckyj MD
 Irritable Bowel Disease Dr. Alexandra Ilnyckyj MD Exactly what is IBS? Common condition affecting mostly women Symptoms are variable but they reflect altered gut movement (motility) and sensation Commonly
Irritable Bowel Disease Dr. Alexandra Ilnyckyj MD Exactly what is IBS? Common condition affecting mostly women Symptoms are variable but they reflect altered gut movement (motility) and sensation Commonly
The long-term impact of the low-fodmap diet for management of irritable bowel syndrome. Dr Miranda Lomer RD.
 The long-term impact of the low-fodmap diet for management of irritable bowel syndrome Dr Miranda Lomer RD Email: miranda.lomer@kcl.ac.uk What is IBS - ROME IV Criteria A functional bowel disorder in which
The long-term impact of the low-fodmap diet for management of irritable bowel syndrome Dr Miranda Lomer RD Email: miranda.lomer@kcl.ac.uk What is IBS - ROME IV Criteria A functional bowel disorder in which
Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider
 For the Primary Care Provider") Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider Elizabeth Coss, MD General Gastroenterologist Audie Murphy Veterans Hospital UT Health This presentation does not
Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider Elizabeth Coss, MD General Gastroenterologist Audie Murphy Veterans Hospital UT Health This presentation does not
Current management options and recent advances in IBD
 n DRUG REVIEW Current management options and recent advances in IBD Ben Warner BSc, MRCP and Peter Irving MA, MD, FRCP SPL The advent of biological therapies has revolutionised the management of inflammatory
n DRUG REVIEW Current management options and recent advances in IBD Ben Warner BSc, MRCP and Peter Irving MA, MD, FRCP SPL The advent of biological therapies has revolutionised the management of inflammatory
Anti-TNF and cyclosporine are identical choices for severe ulcerative colitis refractory to steroid therapy CON Peter Laszlo LAKATOS Semmelweis
 Anti-TNF and cyclosporine are identical choices for severe ulcerative colitis refractory to steroid therapy CON Peter Laszlo LAKATOS Semmelweis University, 1st Department of Medicine Budapest June 13-15,
Anti-TNF and cyclosporine are identical choices for severe ulcerative colitis refractory to steroid therapy CON Peter Laszlo LAKATOS Semmelweis University, 1st Department of Medicine Budapest June 13-15,
IBD Updates. Themes in IBD IBD management journey. New tools for therapeutic monitoring. First-line treatment in IBD
 IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
Clinical Study Clinical Study of the Relation between Mucosal Healing and Long-Term Outcomes in Ulcerative Colitis
 Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2013, Article ID 192794, 6 pages http://dx.doi.org/10.1155/2013/192794 Clinical Study Clinical Study of the Relation between
Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2013, Article ID 192794, 6 pages http://dx.doi.org/10.1155/2013/192794 Clinical Study Clinical Study of the Relation between
Irritable Bowel Syndrome, Inflammatory Bowel Disease and Gastroesophageal Reflux Disease Study Guide
 Irritable Bowel Syndrome, Inflammatory Bowel Disease and Gastroesophageal Reflux Disease Study Guide Class Preparation: Before class, students will be expected to review the online lecture, study guide
Irritable Bowel Syndrome, Inflammatory Bowel Disease and Gastroesophageal Reflux Disease Study Guide Class Preparation: Before class, students will be expected to review the online lecture, study guide
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Dr David Epstein Vincent Pallotti Hospital and University of Cape Town
 Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 20 October 2010
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 20 October 2010 MEZAVANT LP 1200 mg, prolonged-release gastro-resistant tablets B/60 (CIP code: 378 689-2) Applicant
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 20 October 2010 MEZAVANT LP 1200 mg, prolonged-release gastro-resistant tablets B/60 (CIP code: 378 689-2) Applicant
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Ulcerative colitis: the management of ulcerative colitis Quality standard title: Ulcerative
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Ulcerative colitis: the management of ulcerative colitis Quality standard title: Ulcerative
DENOMINATOR: All patients aged 18 and older with a diagnosis of inflammatory bowel disease
 Measure #270: Inflammatory Bowel Disease (IBD): Preventive Care: Corticosteroid Sparing Therapy National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Measure #270: Inflammatory Bowel Disease (IBD): Preventive Care: Corticosteroid Sparing Therapy National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Positioning Biologics in Ulcerative Colitis
 Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
The Spectrum of IBD. Inflammatory Bowel Disease. Symptoms. Epidemiology. Tests for IBD. CD or UC? Inflamatory Bowel Disease. Fernando Vega, M.D.
 The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
5/2/2018 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD
 5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
A FODMAP Diet Update: Craze or Credible?
 A FODMAP Diet Update: Craze or Credible? Carol Rees Parrish, M.S., R.D., Series Editor J. Reggie Thomas Rakesh Nanda Lin H Shu FODMAP is an acronym for Fermentable Oligosaccharides, Disaccharides, Monosaccharides,
A FODMAP Diet Update: Craze or Credible? Carol Rees Parrish, M.S., R.D., Series Editor J. Reggie Thomas Rakesh Nanda Lin H Shu FODMAP is an acronym for Fermentable Oligosaccharides, Disaccharides, Monosaccharides,
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND. Fabrizio Parente
 NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
September 12, 2015 Millie D. Long MD, MPH, FACG
 Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Algorithm for managing severe ulcerative colitis
 Tropical Gastroenterology 2014;Suppl:S40 44 Algorithm for managing severe ulcerative colitis Vineet Ahuja 1, Ajay Kumar 2, Rakesh Kochhar 3 ABSTRACT Dept of Gastroenterology, 1 All India Institute of Medical
Tropical Gastroenterology 2014;Suppl:S40 44 Algorithm for managing severe ulcerative colitis Vineet Ahuja 1, Ajay Kumar 2, Rakesh Kochhar 3 ABSTRACT Dept of Gastroenterology, 1 All India Institute of Medical
NW SMS icons. MFLN Intro
 NW SMS icons The low FODMAP diet for irritable bowel syndrome: from evidence to practice Get handouts etc. by following the link below: learn.extension.org/events/3300 This material is based upon work
NW SMS icons The low FODMAP diet for irritable bowel syndrome: from evidence to practice Get handouts etc. by following the link below: learn.extension.org/events/3300 This material is based upon work
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών. Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων
 Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων Conflict of interest By means of this, the speaker confirms that
Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων Conflict of interest By means of this, the speaker confirms that
The Road to Remission
 The Road to Remission Understanding, Treating and Living with Inflammatory Bowel Disease IBDCenterOrlando.com As many as 1.5 million Americans currently suffer from inflammatory bowel disease (IBD), and
The Road to Remission Understanding, Treating and Living with Inflammatory Bowel Disease IBDCenterOrlando.com As many as 1.5 million Americans currently suffer from inflammatory bowel disease (IBD), and
Rome III Criteria for IBS. Irritable Bowel Syndrome: What s the Latest? IBS: What s the Latest? Distinguishing IBS-C from CC
 Rome III Criteria for IBS Irritable Bowel Syndrome: What s the Latest? Tim Burke, DO Pacific Digestive Associates Clackamas, OR Recurrent abdominal pain or discomfort at least 3 days/month in the last
Rome III Criteria for IBS Irritable Bowel Syndrome: What s the Latest? Tim Burke, DO Pacific Digestive Associates Clackamas, OR Recurrent abdominal pain or discomfort at least 3 days/month in the last
I B D. etter than this. isease UNDERSTANDING INFLAMMATORY BOWEL DISEASES
 I B D m etter than this isease UNDERSTANDING INFLAMMATORY BOWEL DISEASES What types of people have learned how to manage their IBD? Athletes Musicians Firefighters DOCTORS HEROES Artists Presidents Actors
I B D m etter than this isease UNDERSTANDING INFLAMMATORY BOWEL DISEASES What types of people have learned how to manage their IBD? Athletes Musicians Firefighters DOCTORS HEROES Artists Presidents Actors
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Geographical and Cultural Food-related Symptoms, Food Avoidance and Elimination
 Geographical and Cultural Food-related Symptoms, Food Avoidance and Elimination Sheila E. Crowe, MD, FRCPC, FACP, FACG, AGAF Digestive Health Center of Excellence University of Virginia Adverse Reactions
Geographical and Cultural Food-related Symptoms, Food Avoidance and Elimination Sheila E. Crowe, MD, FRCPC, FACP, FACG, AGAF Digestive Health Center of Excellence University of Virginia Adverse Reactions
Patho Basic Chronic Inflammatory Bowel Diseases. Jürg Vosbeck Pathology
 Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease