Image Diagnostic Technology Ltd 53 Windermere Road, London W5 4TJ Tel: +44 (0)
|
|
|
- Earl Parrish
- 5 years ago
- Views:
Transcription
20 8819 9158 www.idtscans.com email: info@idtscans.")
1 Image Diagnostic Technology Ltd 53 Windermere Road, London W5 4TJ Tel: +44 (0)
2 Dental Radiography and Quality Assurance Anthony Reynolds BA MSc PhD Registered Clinical Scientist CS03469 Image Diagnostic Technology Ltd.

3 Who or what is IDT? Image Diagnostic Technology Ltd aka IDT Scans Specialises in: arranging dental CT/CBCT scans 3D processing radiology reports implant simulation 3D models surgical drill guides 32,000 scans processed since 1991
4 What can IDT do with my images Prepare datasets for planning implants Radiology Reports Treatment Plans 3D Models Surgical Drill Guides

5
6
7
8 Outline of Lectures Introduction / Disclosures Diagnostic Imaging in Dentistry Conventional Radiography CT / CBCT Scans Quality Assurance Radiation Dose and Risk Compliance with the Legislation
9 What do we use dental imaging for? Review patient anatomy and pathology diagnostic quality images at a low radiation dose Answer specific clinical questions is caries present how many teeth are present quality and quantity of bone radio-lucencies or radio-opacities
10 Imaging for specific dental applications Planning dental implants Orthodontics Endodontics Surgical Planning
11 What Imaging Modalities are available? Intra-oral radiography Periapicals, bitewings, occlusal views Extra-oral radiography AP and Lateral cephs Dental Panoramic Tomography (DPT or OPG) Cone Beam computed tomography (CBCT)
 + Fast, convenient, low dose")
 bone quality Distance")
12 Intra-oral Imaging + Very high resolution (20 lp/mm) + Fast, convenient, low dose Magnification / Distortion No (quantitative) bone quality Distance measurements not reliable
13 Distortion in intra-orals X-RAYS FILM TOOTH Solutions: bisecting angle paralleling technique


14 Extra-oral: Lateral Cephs + Good overview + Useful for orthodontics Magnification / Distortion Distance measurements not reliable
15 Conventional Tomography (tomography by blurring) TUBE T 1 T 2 Q R P FILM Q 2 P 2 R 2 R 1 P 1 Q 1
")
16 Dental Panoramic Tomography (DPT)

17 Dental Panoramic Tomography (DPT, OPG, OPT) + Very good overview + Mandibular fractures, unerupted teeth + Sufficient detail for caries diagnosis Variable Magnification / Distortion Patient positioning is crucial

 Computed Tomography (CT")
18 Cross-Sectional Imaging Linear Tomography Complex Motion Tomography (CMT) Ultrasound Magnetic Resonance Imaging (MRI) Computed Tomography (CT or CBCT)


19 Dental (CB)CT Scans The dentoalveolar region has high natural contrast So we can get away with - high resolution images - low radiation dose We can reduce the dose and get away with images that would not be acceptable for a medical CT scan.
20 CBCT is useful for: planning dental implants maxillofacial surgery cleft palate assessment TMJ and airway analysis impacted, supernumerary and abnormal teeth root canals, root fractures etc periapical disease CBCT is not good for: dental caries soft tissue tumours

21 Systematic Review of Indications for CBCT
22 Cone Beam CT (CBCT) Scanner GXCB-500 is a trademark of Gendex Dental Systems of Lake Zurich, USA
23 Cone Beam CT (CBCT) Scanner GXCB-500 is a trademark of Gendex Dental Systems of Lake Zurich, USA
24 (Review Paper)
25
26 DentoMaxilloFacial Radiology CBCT Special Issue



27 how CT works Godfrey Hounsfield Allan Cormack Nobel prize in Medicine, 1979 Animation courtesy of Demetrios J. Halazonetis
28 detectors x-ray source
29 reconstruction Animation courtesy of Demetrios J. Halazonetis
30 volume dataset Animation courtesy of Demetrios J. Halazonetis
31 Animation courtesy of Demetrios J. Halazonetis



32 Animation courtesy of Demetrios J. Halazonetis
33 Animation courtesy of Demetrios J. Halazonetis
34 Voxels (Volume elements) Animation courtesy of Demetrios J. Halazonetis
 Animation courtesy of Demetrios J.")
35 Voxels (Volume elements) density: x 512 x 400 slices 100 million voxels (200 Mb) Animation courtesy of Demetrios J. Halazonetis

36 cone-beam CT (CBCT) Animation courtesy of Demetrios J. Halazonetis

37 cone-beam CT (CBCT) Animation courtesy of Demetrios J. Halazonetis
38 cone-beam CT (CBCT) Animation courtesy of Demetrios J. Halazonetis
39 cone-beam CT (CBCT) X-ray Tube Detector

40 CB-500 CBCT Scanner fast scan times 4.8s to 23s pulsed x-ray tube low dose typical Mx 35µSv typical Mn 60µSv adjustable collimator 4 to 8.6 cm height 8.6 or 15.6 cm width large detector 8cm x 8cm adjustable chair Around 90K Gendex is a trademark of Gendex Dental Systems of Lake Zurich, USA

41 DP-700 CBCT Scanner variable ma fixed scan times 11s for SFOV 45s for MFOV medium dose typical Mx 60µSv typical Mn 100µSv fixed collimator 4cm x 6cm SFOV 8cm x 6cm MFOV Around 45K small detector no chair Gendex is a trademark of Gendex Dental Systems of Lake Zurich, USA

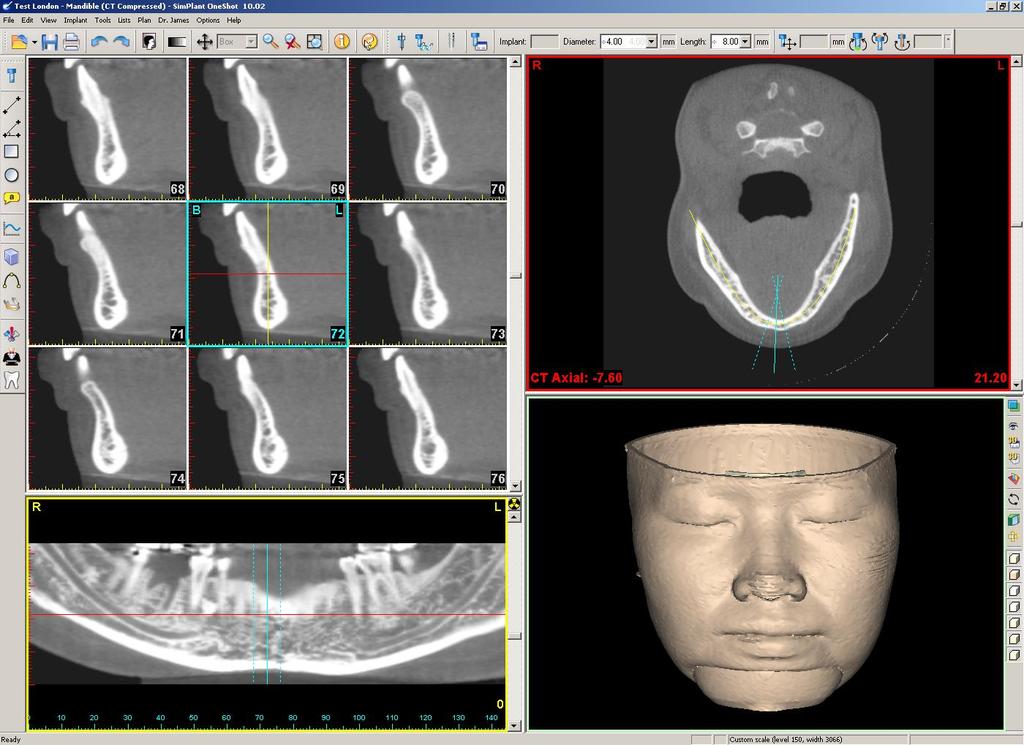
42 Basic CBCT images Panoramic Transaxial Cross-sectional





43 Basic CBCT images Axials Panoramics Cross Sections Sagittal Coronal


44
45

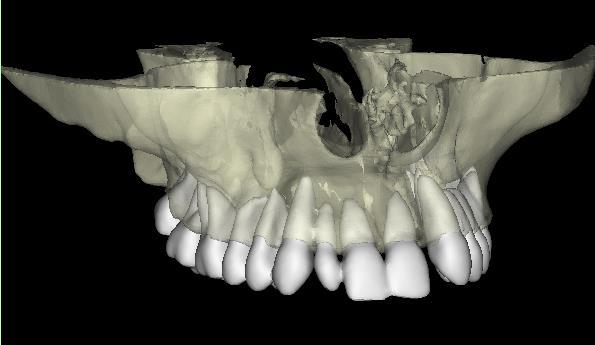

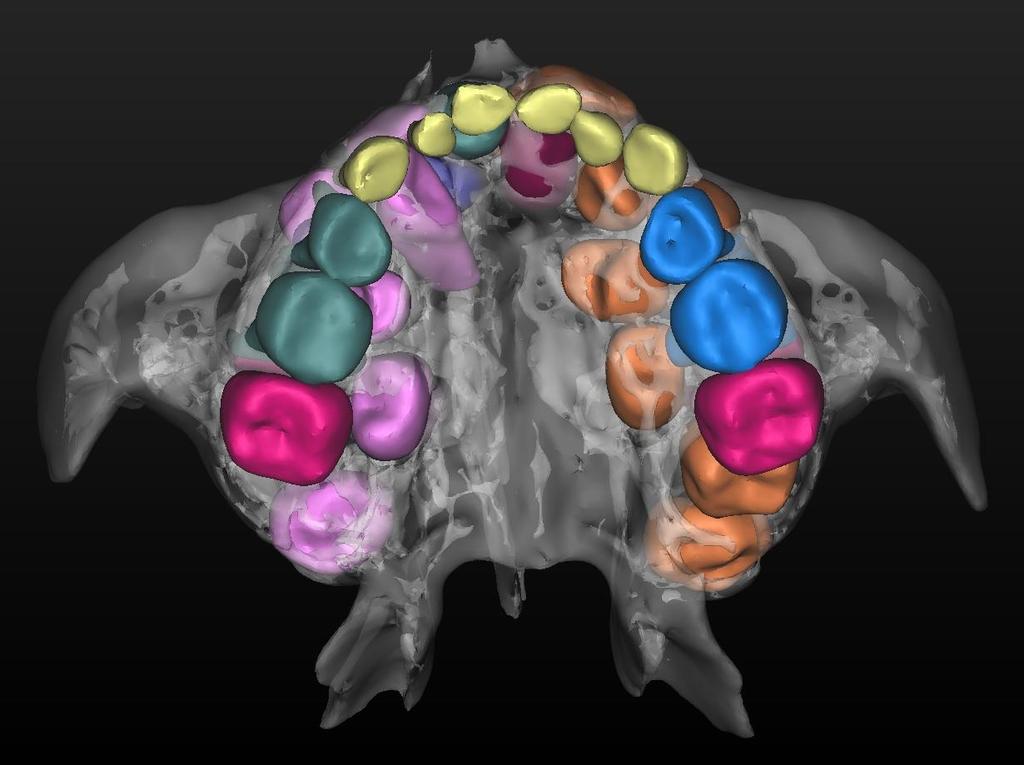
46 Segmentation
47

48



49 Hyperdontia Courtesy of Nicolette Schroeder
50


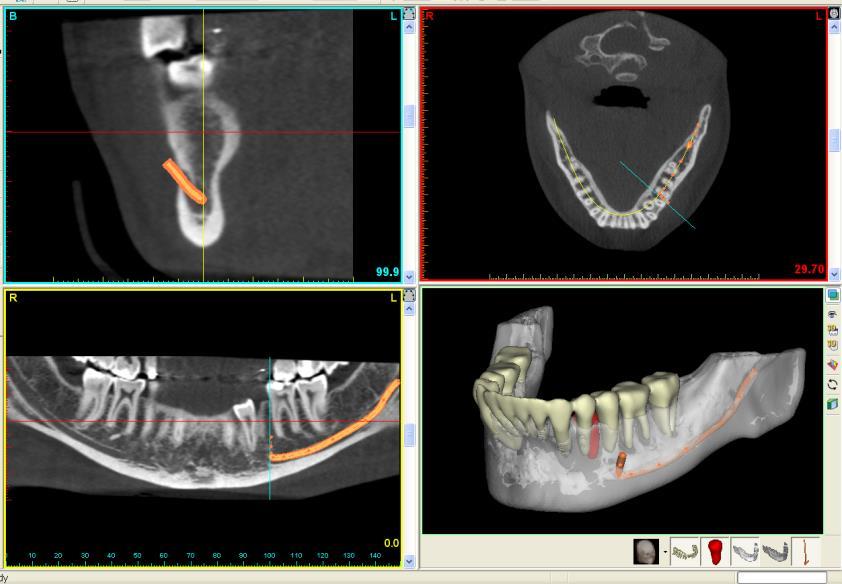
51 Third Molars Courtesy of Barry Dace



52 Implants: Make Your Own Surgical Drill Guide Bone Mucosa Teeth Bone Supported Guides: - Bone crest must be clearly visible in the CBCT images and 3cm long Mucosa Supported Guides: - Patient must be scanned with a radio-opaque scanning stent in place Tooth Supported Guides: - Tips of teeth must be clearly visible in the CBCT images - A recent and accurate plaster cast will be required Need to think about the Guide before you request the CBCT Scan!
53 Tooth Supported Guides Drill Guide will be supported on patient s existing teeth Need a recent and accurate impression or plaster cast Optical (laser) scan of plaster cast Import optical scan into the implant planning software Guide will be designed to fit the plaster cast.


54 Optical Scan of Plaster Cast

55 BLUE SKY PLAN

56 BLUE SKY PLAN

57 Design the Guide

58 Print it on a 3D Printer
59 Outline of Lectures Introduction / Disclosures Diagnostic Imaging in Dentistry Conventional Radiography CT / CBCT Scans Quality Assurance Radiation Dose and Risk Compliance with the Legislation
60 What is Quality Assurance? An on-going audit of the entire imaging process from start to finish, to make sure we are getting the best possible image quality at the lowest practical radiation dose.
61 Why Quality Assurance? Ensure images are produced under the most favourable conditions Cost and time savings from fewer repeats Regulatory compliance QA is a requirement under IR(ME)R 2017 (used to be a requirement under IRR 99)
62 Quality Assurance (QA) versus Quality Control (QC) Quality Assurance is process oriented makes sure you are doing the right things, in the right way Quality Control is equipment oriented makes sure the equipment is performing as you expected.
63 Quality Control Regular testing of equipment detect malfunctions assess image quality and radiation dose Ensure it produces consistent images acceptable image quality low radiation dose as good as new! (within acceptable limits)
64 Quality Control Program QC tests should be written down Make them the responsibility of a named individual Simple tests can be done by the person who takes the x-rays More complicated tests require a physicist or engineer.
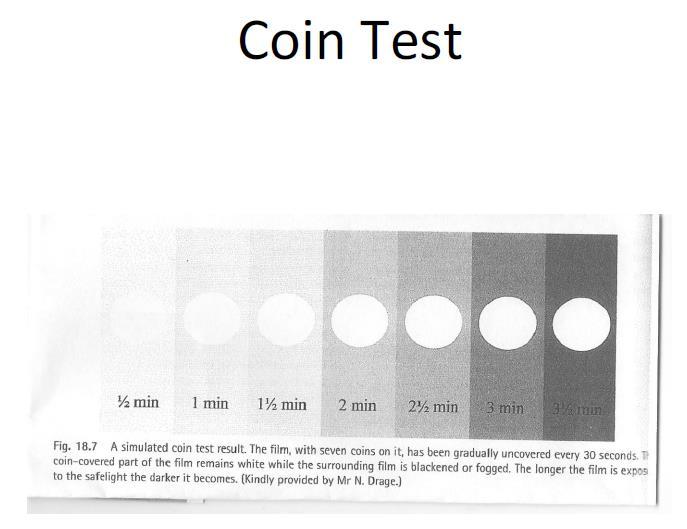
65 If you have a Darkroom (applies also to Daylight Loaders) Need to look at: Film storage Safe light levels Film processing Chemicals Temperature Cleaning
66
67 When should QC tests be performed? Before first clinical use At regular intervals (every few months) After a major repair.
68 Critical Examination Must be performed before first use or after a major repair Evaluation of safety features Responsibility of the installer/repairer Performed by engineer or physicist Evaluation of shielding and radiation protection Evaluation of warning signals Evaluation of exposure controls Acceptable functioning of cut-out switches etc Report should be kept with equipment records.
69 Acceptance Testing Ensures equipment meets its specifications Responsibility of the purchaser Performed by Radiation Protection Advisor (RPA) or Medical Physics Expert (MPE) Provides a baseline for Quality Control tests.
70 Routine QC Tests Monthly tests can be performed by the Operator Annual tests should be performed by RPA or MPE Follow manufacturer s instructions for QC tests See also Medical and Dental Guidance Notes (2002) 20 from Institute of Physics and Engineering in Medicine (IPEM) JournalsPublications/Medicaland DentalGuidanceNotes.aspx

71 Monthly Tests example: i-cat CBCT Scanner Scan the supplied QC phantom using the recommended settings Follow the manufacturer s instructions to measure density of inserts and number of line pairs visible Measure the distance to check geometrical accuracy


72
73 Recommended Annual Tests Usually performed by RPA or MPE Is radiation output within specs? Is tube voltage (kvp) within specs? Tube Current (ma) accuracy Timer (s) accuracy Half value layer Tube leakage Focal spot size Collimation accuracy Tube stability & mechanical safety
74 Quality Assurance Program Takes a holistic approach choosing equipment installing and testing equipment training staff acquiring images viewing images storing images reject analysis
75 Choosing Dental X-ray Equipment Should be designed to meet European standards (CE Marking) Must meet requirements of Medicines and Healthcare Products Regulatory Agency in the UK (Health Products Regulatory Authority in Ireland) Manufacturers must provide adequate information on use, testing and maintenance.

76
77 Before taking radiographs Is the radiograph necessary? Is adequate clinical information available? Do we understand the referrer s objectives?
78 Before taking radiographs Do we have the correct patient? Name Address Date of Birth Pregnancy status Exposing the wrong patient is automatically notifiable to Care Quality Commission (CQC) Check the problem area with the patient before the exposure.

79 Google for MGTI Guidance
80 Radiographic Technique Record who received what training when Intra-oral technique Use of film holders and beam aiming devices DPT technique Correct patient positioning Patient immobilisation Use of light beams

81 Bisecting Angle Technique Not the technique of choice Only use when paralleling technique cannot be used e.g. small mouthed patient patient cannot tolerate film holder Images can be elongated or distorted

82 Paralleling Technique Beam aiming device must be used Film holder must be far enough into mouth to ensure film is parallel to the tooth Magnification but no distortion (provided it is performed correctly)

83
84 Dental Panoramic Tomogram (DPT) aka Orthopantogram (OPG or OPT) Patient Positioning head and neck straight shoulder clearance bite block between central incisors follow infection control protocol. Light beams mid sagittal frankfort plane AP (canine line) position.

85 Correct Orientation of Cassette Tube side facing the patient Arrow aligned with arrow on the machine Label with L and R markers
86 Cassette Care Clean cassettes once a month Check for scratches or marks Check for light leaks (e.g. hinges) Check film/screen contact as poor contact may cause blurring.
87 no Acquiring the Image Use appropriate settings refer to chart for Adult / Child Observe patient during exposure no patient movement not in distress
88 Digital Radiography Two types: CMOS or CCD detector Photostimulable Phosphor Plate (PSPP)

89

90
91 Digital QA CCD/CMOS sensors should be inspected monthly for damage PSPP sensors should be cleaned and inspected monthly for dirt, scratches or bends Test objects can be x-rayed to check for geometrical accuracy.
92 Viewing Conditions Radiographs should be viewed on a viewing box Digital images should be viewed on a calibrated monitor Room lights should be dimmed.

93 SMPTE Test Pattern (Society of Motion Picture and Television Engineers)
94 Reject Analysis Studies have shown that up to 50% of dental x-rays are of poor standard. Assign (subjective) image quality ratings to rejected images Analyse the results.
95 Triage based on Image Quality 1. Excellent No errors of positioning, exposure or processing Should be 70% or more in this category 2. Acceptable Some errors but still diagnostic Not more than 20% in this category 3. Unacceptable Unusable, must be repeated Not more than 10% in this category
96 Rejected radiographs Grade 3 (unacceptable) radiographs should be examined to look for trends: Operator Date taken Nature of deficiency Cause of deficiency Number of repeat radiographs.
97 Any questions? Thank you!
98 Outline of Lectures Introduction / Disclosures Diagnostic Imaging in Dentistry Conventional Radiography CT / CBCT Scans Quality Assurance Radiation Dose and Risk Compliance with the Legislation
99 Radiation Dose and Risk Anthony Reynolds BA MSc PhD Registered Clinical Scientist CS03469 Image Diagnostic Technology Ltd.
100 Topics What is radiation? Sources of radiation Is radiation harmful? How can I estimate the risk?
101 What is Radiation? Energy travelling through space Sunshine is a familiar example A small amount is beneficial Too much can be harmful

102 The Electro-Magnetic Spectrum High Frequency Low Frequency from Energy depends on the frequency E = hν
103 Gamma Rays and X-Rays Referred to as Ionising Radiation Can disrupt atoms and turn them into positive and negative ions This can cause damage at molecular level.
104 Sources of Ionising Radiation 1. Environmental (e.g. Radon) 2. Cosmic Rays 3. Radioactive Isotopes inside or outside the body natural or man-made 4. Medical and Dental x-rays The first 3 make up Background Radiation The first 4 make up Per-Capita Dose.

105 Per-Capita Dose in the UK Background Radiation Medical and Dental Average Per-Capita Dose 2.2mSv 0.5mSv 2.7mSv per person per year

106 Vacuum Tube X-Ray Tubes High Voltage (60 to 120 kvp) Low Current (1 to 100 ma) 12 KiloWatts of Power!! Mostly appears as heat but about 1% appears as x-rays.
107 Advantage of X-Ray Tubes Produce an intense stream of x-ray photons from a small focal spot When the tube is switched off, there is no more radiation A Controlled Area only exists while the power is on. X-ray tubes cannot induce radioactivity in other objects (or people).
108 X-Ray Spectrum Dental x-ray tubes operate in the range 60 to 120 kvp Bremsstrahlung produces x-ray photons with a range of energies Characteristic Radiation produces discrete lines indicative of the target material Filtration removes the least energetic x-ray photons. X-ray Energy
109 Absorption/Attenuation of X-Rays At diagnostic energies (60 to 120 kev) x-rays lose their energy by interacting with electrons. For energies up to about 70 kev the photoelectric effect is the most important Coherent scattering also occurs at energies up to about 70 kev For energies greater than about 70 kev Compton scattering is the most important.
110 Coherent (aka Rayleigh or Elastic) Scattering Coherent scattering low-energy electrons are unable to eject an electron. Instead they bounce off the electron and continue in a different direction, without any loss in energy.
111 Photoelectric and Compton effects Photoelectric x-ray loses all of its energy by ejecting a K-shell electron. X-ray is halted but an outer shell electron may drop into the K-shell with the emission of Characteristic Radiation. Compton x-ray loses some of its energy by ejecting an outer shell electron. X-ray continues at a lower energy and in a different direction.
112 Energy and Tissue Dependence Differences in x-ray absorption are perceived as contrast between Bone and Muscle in the images. Lower energies produce more contrast at the expense of more patient dose. Optimum is around 90 kvp for CBCT.
113 Energy and Tissue Dependence Differences in x-ray absorption are perceived as contrast between Bone and Muscle in the images. Lower energies produce more contrast at the expense of more patient dose. Optimum is around 90 kvp for CBCT.
114 What happens to the energy? The energy lost by the x-rays is imparted to the tissue!

115 Absorbed Dose

116 Equivalent Dose Also known as Organ Dose or Local Dose

117 Effective Dose From ICRP 103 Often referred to simply as The Dose
118
119 Topics What is radiation? Sources of radiation Is radiation harmful? How can I estimate the risk?

120

121 26 April 1986

122 14 June 2017

123
124 Dose Rate at Chernobyl (2017) 200m from the reactor 1.35 microsievert per hour Background Dose Rate in the UK (Average) 0.25 microsievert per hour Flight from the UK to Chernobyl 3 hours x 2.5 μsv/hr = 7.5 μsv Dental x-ray (intraoral) 1 microsievert CBCT scan (both jaws) 100 microsievert

125 Biological Effects of Radiation

126 DNA Damage - Simple Most likely damage is single strand break Occur spontaneously all the time ~100% successfully repairable Occurs ~1000x more frequently from cellular processes than from background radiation.

127 DNA Damage - Complex With radiation there is a greater frequency of more complex breaks Double strand breaks may not be repaired successfully Successful repair more difficult at higher dose rates.
128 Deterministic and Stochastic effects Deterministic Effects are reproducible severity of the effect increases with the dose not observed below a threshold dose of about 500mSv Stochastic Effects are random the risk (not the severity) increases with the dose known to occur above 20mSv or so below about 20mSv we don t know if they occur or not Hereditary Effects are random (stochastic) but the incidence in humans is very low.
129 Deterministic Effects For a high dose of radiation received over a short period of time, it is just about certain that the following effects will occur: radiation sickness: 1-2Gy (whole body dose) skin erythema: 2-5Gy (local dose) sterility: 2-3Gy (local dose) hair loss: 2-5Gy (local dose) death: 3-5Gy (whole body dose) We should never see any of these effects in a dental practice!

130 Deterministic Effects in Radiation Workers

131
132 Stochastic Effects For a high dose of radiation received over a short period of time, it is very likely (but not certain) that cancer will be induced. For a low dose of radiation, we think that cancer may be induced (maybe many years after exposure) but we don t know for sure.
 An additional 4000 may have died from stochastic effects we don t know for sure. http://www.who.")
133 Effects of Chernobyl Disaster 28 workers known to have died from Radiation Sickness (deterministic effect) 15 children known to have died from thyroid cancer (stochastic effect) An additional 4000 may have died from stochastic effects we don t know for sure. chernobyl/backgrounder/en/
134 Should not see in dental practice!

135
136 Estimated excess relative risk (±1 SE) of mortality ( ) from solid cancers among groups of survivors in the LSS cohort of atomic bomb survivors, who were exposed to low doses (<500 msv) of radiation (2). Brenner D J et al. PNAS 2003;100: by National Academy of Sciences
137 Schematic representation of different possible extrapolations of measured radiation risks down to very low doses, all of which could, in principle, be consistent with higher-dose epidemiological data. Brenner D J et al. PNAS 2003;100: msv 2003 by National Academy of Sciences
138 The Linear No-Threshold (LNT) Model Assumes that the risk of producing cancer is proportional to the dose (no safety threshold) Assumes that cellular damage does not accumulate from one x-ray exposure to the next Assumes that the risk for a given exposure depends only on the dose for that x-ray exposure and not on the patient s previous dose history Assumes that x-ray exposures are independent events.
139 Criticism of the LNT Model Doesn t take dose rate into account Implies that cells do not have a repair mechanism (if they did, the curve would be less than linear and maybe have a threshold) Implies that cellular damage does not accumulate from one x-ray exposure to the next (if it did, the curve would be greater than linear) There is no proof that the LNT model is correct but it is prudent to use it for Radiation Protection.
140 The concept of Effective Dose We know the risks from high doses of radiation e.g. Atom Bomb survivors Atom Bomb survivors received whole body doses Dental patients receive doses to a very small region How can we relate the risks? Effective Dose is a way of describing the dose to a limited region in terms of the whole body dose that would result in the same risk to the patient Effective Dose is a measure of risk!
141 Effective Dose (Recap) Absorbed Dose Energy absorbed by tissue (Gray, Gy) 1 Gray (Gy) = 1 Joule per Kilogram (J/Kg) Equivalent Dose H T (Sievert, Sv) Multiply the Absorbed Dose by the Radiation Weighting factor W R (= 1 for x-rays) to get H T Local Dose Effective Dose E (Sievert, Sv) Multiply the Equivalent Dose H T by the Tissue Weighting factor (W T ) for each organ, and add them up to get the Effective Dose E Whole Body Dose
142 More about Effective Dose The Effective Dose calculation takes the size of the region and the body parts irradiated into account It s tempting to say My CBCT scanner might deliver a high Effective Dose, but it s only to a very small region but this argument is not valid.

143 To obtain the Effective Dose in practice: Method 1: Measure it! 1. Measure Absorbed Dose to each organ of interest 2. Apply Radiation Weighting factor to obtain Equivalent Dose for each organ of interest 3. Take the weighted sum of all the Equivalent Doses.

144 Method 2: Use published data. SEDENTEXT paper Eur J Radiol 81,2, (February 2012)

145 DentoMaxilloFacial Radiology CBCT Special Issue
146 SEDENTEXCT measured Effective Doses for common CBCT scanners and found they were in the range 20 microsieverts to 370 microsieverts
147 Prof. Ria Bogaerts, Katholieke Universiteit Leuven, March 2011
148 Prof. Ria Bogaerts, Katholieke Universiteit Leuven, March 2011
149 Prof. Ria Bogaerts, Katholieke Universiteit Leuven, March 2011

150
151 Method 3: Use the DAP (with caution!) Sara Lofthag-Hansen
152 Dose versus DAP Effective Dose (µsv) = 0.1 x DAP (mgy.cm2) for Maxilla Effective Dose (µsv) = 0.15 x DAP (mgy.cm2) for Mandible Effective Dose (µsv) = x DAP (mgy.cm2) for Mn & Mx VERY ROUGH USE WITH CAUTION!
153

154 Use the DAP with caution! Same DAP Different Dose
155 How accurate do we need to be? A factor of 2 change in risk is unlikely to bring about a change in the patient s management. A factor of 10 would be in line with estimates of risk in other areas.
156 Calman Risk Table

157 Dental x-rays are in the range Negligible to Minimal
158 ICRP 103: Effective dose is not recommended for epidemiological evaluations, nor should it be used for detailed specific retrospective investigations of individual exposure and risk. - But we use it anyway!
159 What is the Risk from an Intraoral x-ray? Assume adult patient, F speed, rectangular collimation Effective Dose might be 2 microsieverts (worst case) Risk that patient might develop fatal cancer in 20 years time = 5% (1 in 20) per Sievert (from ICRP103) = 1 in 20 million for 1 microsievert = 2 in 20 million for 2 microsieverts = 1 in 10 million for 2 microsieverts Health & Safety people would call this a Negligible Risk
160
161 What is the Risk from a CBCT scan? Assume adult patient, dento-alveolar scan, both jaws Effective Dose might be 100 microsieverts (worst case) Risk that patient might develop fatal cancer in 20 years time = 5% (1 in 20) per Sievert (from ICRP103) = 1 in 20 million for 1 microsv = 100 in 20 million for 100 microsv = 1 in 200,000 (roughly) for CBCT scan Health & Safety people would call this a Minimal Risk * If your patient is a child the risk is 3x more

162 Risk varies with Age 5% per Sievert at age 30
163 What is the Dose from a Dental CT or CBCT Scan? Medical CT Scanner (using dental protocol): About 300 µsv per jaw (20 x OPG) Cone Beam CT: About 50 µsv per jaw (3 x OPG) Equivalent to about 8 days of Background Radiation (per jaw) Carries a theoretical risk of about 1 in 200,000 of inducing a fatal cancer (1 in 400,000 per jaw) On top of 1 in 3 risk we all have already Much safer than smoking, driving or playing soccer!

164 The Risk of Not Having a CBCT Scan

165
166 Typical Doses from Dental X-Rays Effective Dose (µsv) Intraoral (F speed, rect coll) 2 Risk Intraoral (E speed, round coll) 6 Lateral Ceph 10 Panoramic 3 to 24 Cone Beam CT 19 to 1073 Medical CT (using dental protocol) 280 to 1410
167 Typical Doses from Dental X-Rays Effective Dose (µsv) Risk Intraoral (F speed, rect coll) 2 1 in 10 million Negligible Intraoral (E speed, round coll) 6 1 in 3.3 million Negligible Lateral Ceph 10 1 in 2 million Negligible Panoramic 3 to 24 1 in 6.7 million to 833 thousand Negligible to Minimal Cone Beam CT 19 to in 1.05 million to 1 in 19 thousand Mimimal to Very Low Medical CT (using dental protocol) 280 to in 71 thousand to 1 in 14 thousand Very Low
168 Risks from Dental x-rays Negligible to Very Low risk of radiation induced cancers Negligible risk of serious hereditary disease in an individual s descendants
169 Radiation dose from x-ray exams Examination Effective dose (msv) Dental intraoral hours Dental CBCT scan weeks Lumbar spine x-ray months Low-dose CT lung months Equivalent period of background radiation (UK)* CT brain months Barium enema years CT chest CT abdomen or pelvis years 4.6 years *UK annual background dose 2.2 msv approx.
 Compared to 155,000 cancer deaths from other")
170 If everyone in the UK had a dental CBCT scan every year... There might be 160 extra cancer deaths per year (if LNT is correct) Compared to 155,000 cancer deaths from other causes
171 Quiz - True or False? 1. Medical CT scanners should never be used for dental CT scans. 2. Radiation damage is cumulative. 3. The risk of cancer increases with the number of scans. NEVER SAY NEVER NOT FOR DIAGNOSTIC X-RAYS TRUE AS FAR AS WE KNOW 4. The CBCT scan was non-diagnostic but I shouldn t repeat it because of the dose. 5. My patient has had several CBCT scans already - she shouldn t have any more. FALSE FALSE
172 Outline of Lectures Introduction / Disclosures Diagnostic Imaging in Dentistry Conventional Radiography CT / CBCT Scans Quality Assurance Radiation Dose and Risk Compliance with the Legislation
173 Compliance with the Legislation Anthony Reynolds BA MSc PhD Registered Clinical Scientist CS03469 Image Diagnostic Technology Ltd.
174
175 European Directives for Radiation Safety Basic Safety Standards Directive 96/29/Euratom of 13 May 1996 Medical Exposure Directive 97/43/Euratom of 30 June 1997 Basic Safety Standards Directive (revised) 2013/59/Euratom of 5 December 2013
176 Transposition into UK Law Ionisation Radiations Regulations 1999 IRR99 Exposure of members of the public (e.g. staff and visitors) Enforced by Heath and Safety Executive (HSE) Ionising Radiation (Medical Exposure) Regulations 2000 (amended in 2006 and 2011) IR(ME)R 2000 Medical exposures (e.g. patients) Enforced by Care Quality Commission Both IRR99 and IR(ME)R 2000 were revised in 2017.
177 Framework for Radiation Protection Based on International Commission for Radiation Protection (ICRP) an advisory body with no formal powers Legal & Administrative Requirements IRR 2017 IR(ME)R 2017 SI 478 of 2002 in Ireland (hasn t yet been revised to meet BSSD) Local Rules / Written Procedures at each hospital or dental practice Each professional has an individual responsibility
178 Ionising Radiation Regulations 2017 (IRR 2017) Regulates all use of radiation in the workplace (industry as well as medicine and dentistry) Not directly concerned with patient exposures (unless accidental) Regulated by Health and Safety Executive (HSE) not Department of Health or Care Quality Commission.
179 Terminology The Employer is the legal person responsible for compliance with IRR The Employer could be: An NHS Trust The owner of a dental practive The owner of an x-ray repair and servicing company etc.
180 IRR New System of Authorisation Under IRR99 employers had to notify HSE 28 days in advance of commencing work with ionising radiation. Under IRR 2017 you just have to register in advance (doesn t specify how much in advance). Graded system under IRR2017: Notification: work with radionuclides only Registration: work with radiation generators including x-ray tubes. Costs 25 to register (for all sites under one Employer). Consent: administering radiopharmaceuticals to patients (costs 25 per Employer) Must re-register (and pay a new fee) after a material change (such as change of Employer s name or address)
181 IRR New System of Authorisation Employers (e.g. dental practice owners) had to register and pay 25 fee by 5 February Associates (working at someone else s practice and following the owner s rules and regulations) do not have to register. If you should have registered but haven t already done so you can register online here:
182 Employer s Duties Risk Assessment identify main radiological risks Contingency plans for reasonably foreseeable radiation accidents Keep employees and other persons exposure ALARP (As Low As Reasonably Practical) Comply with Dose Limits Measure and/or estimate maximum annual Effective Doses Measure and/or estimate maximum annual Equivalent Doses to lens of the eye, extremities, single organ or tissue Provide adequate training for employees Appoint Radiation Protection Advisor (RPA) and consult him/her on the observance of IRR 2017 Draw up Local Rules and appoint Radiation Supervisor Designate and demarcate Controlled and Supervised Areas Ensure built-in features, safety features and engineering controls are designed to keep exposure to radiation ALARP.
183 Risk Assessment A Risk Assessment is required before commencing new activities involving ionising radiation. 1. Look for the hazards 2. Decide who may be harmed and how 3. Decide if existing control measures are adequate or if more are needed 4. Record the findings of the Risk Assessment 5. Review the Assessment periodically (e.g. once per year) and revise if necessary.
184 Hierarchy of Control Measures Control Measures should be considered in this order: 1. Engineering Controls Beam collimation, shielding, warning devices 2. Systems of Work Controlled Areas Local Rules 3. Personal Protective Equipment (should be a last resort) Lead aprons
185 Staff Protection Based on 3 principles: Distance the further you are from the source the less radiation you receive follows Inverse Square Law (1/d 2 ) Shielding fixed (built into the walls) or a mobile shield something you wear (e.g. lead apron for staff) Time shorter exposure to radiation results in less dose. Staff are present 8 hours a day so it is vital to protect them.
186 Patient Protection Addressed in more detail under IR(ME)R lead aprons for patients not usually necessary in dental radiography you can give the patient a lead apron if it makes them feel more comfortable. thyroid shields for patients can be useful for CBCT scans.
187 Members of the Public Adequate shielding needs to be built into the walls, ceilings, floors, doors, windows of rooms containing x-ray equipment if you have windows in the doors make sure they contain lead Think carefully about the best locations for waiting rooms, toilets etc Think how to prevent members of the public from walking into a Controlled Area warning signs radiographer stands at the door good building design ensuring the public have no reason to walk past a Controlled Area.
188 Sources of Radiation Primary Beam only the patient should be exposed to the primary beam. Tube Leakage must be less than 1mGy/hour at 1 meter tests are performed to ensure this. Scattered Radiation radiation scattered from the patient staff can protect themselves through Distance, Shielding, Time.
189 Pregnant and Breastfeeding Employees Breastfeeding not relevant (unless administering radiopharmaceuticals) Female employees should be advised of the importance of informing employer of pregnancy Risk Assessment should be carried out Dose to foetus must be less than 1mSv (2mSv to surface of abdomen) for the remainder of pregnancy Changes to work practices are not usually required (except for increased monitoring).
190 Personal Monitors Staff in dental practices usually receive a negligible radiation dose (less than 1mSv per year). Personal Monitors (film badges) are not usually necessary. However, they can be reassuring if an incident occurs. They can also be useful to prove that dose limits have not been exceeded.
191 Dose Limits Dose Limits are set so that risks to staff are comparable with other industries e.g. manufacturing, trade, service, government. Risk of death in safe industries is approximately 1 in 10,000 per year Risk to most radiation workers would be much lower than this.

192 Dose Limits for Employees IRR 2017: Dose Limit to Lens of Eye is now 20mSv per year
193 Classified Persons Employees must be classified if they are likely to receive: An Effective Dose of more than 6mSv per year, or An Equivalent Dose to lens of eye of more than 15mSv per year, or An Equivalent Dose to extremities of more than 150mSv per year (skin, hands, forearms, feet or ankles) If they are Classified they must have An appointed doctor A passbook if they work in another Employer s controlled environment. You don t want this to happen in your dental practice!
194 Controlled Areas An area is Controlled if special procedures designed to restrict significant exposure are necessary. Workloads up to 100 intra-orals or 50 DPTs: Within the primary x-ray beam until sufficiently attenuated Within 1.5m of the x-ray tube and patient in any other direction. Dental CBCT: Usually the entire room is a Controlled Area.

195 Controlled Areas Radiation Protection Advisor (RPA) will advise on: Room Shielding Controlled / Supervised Areas Warning Signs Local Rules For dental radiography, a Controlled Area only exists while the power is on.

196 Local Rules Work in a Controlled Area must be carried out according to Local Rules Local Rules should be on display in each room where x-ray equipment is used Employees must read Local Rules and sign an undertaking that they have been read. Some dental practices put the Local Rules on their website.
197 Minimum Content Local Rules should contain at least the following: Description of the Controlled Area Arrangements to restrict access Conditions under which members of the public may enter (e.g. comforters and carers) Instructions for safe working Dose investigation levels Contingency arrangements for foreseeable radiation accidents The names of the Radiation Protection Supervisor and the Radiation Protection Adviser.
198 Radiation Protection Advisor Dental Practices must appoint a suitable RPA Must consult RPA to ensure observance of IRR 2017 RPA should review radiation safety for each new x-ray installation and at least every 3 years for existing installations e.g. adequate shielding designation of controlled areas training of operators local rules / written procedures
199 Radiation Protection Advisor RPA is generally a physicist with certification from HSE-approved Assessing Body Usually an outside consultant Should be available for consultation (otherwise, get a different one) A list of RPAs is available at
200 Radiation Protection Supervisor (RPS) Where work is subject to Local Rules, employer must appoint a Radiation Protection Supervisor (RPS) Usually a member of staff who can command authority (e.g. a dentist) Should be trained to have knowledge of the Regulations and understand the precautions to be taken Legal responsibility remains with the employer.
201 IRR 2017 Differences from IRR99 An Outside Worker is someone who carries out work in the Controlled Area of an Employer other than their own Includes both Classified and Non-Classified workers Service engineers, contractors etc You are responsible for their safety However, you can hand over responsibility temporarily through a Handover Procedure.
202 Handover Procedure Applies to x-ray equipment undergoing testing, service or repair by an external physicist or engineer Equipment is handed over to physicist or engineer who accepts responsibility for radiation safety during the repair Equipment is handed back after repair is complete Forms signed by Employer (equipment owner) and external Physicist / Engineer.

203
204 IRR Employee Co-operation Employees have a duty to co-operate with the Employer under IRR Must wear and take reasonable care of Personal Protective Equipment (PPE) including dosemeters if they have been provided by the Employer. Employee may be commiting an offence under section 7 of the Health & Safety at Work Act if they fail to co-operate with their Employer.
205 Ionising Radiation (Medical Exposure) Regulations 2017 Ionising Radiation (Medical Exposure) Regulations 2000 (amended in 2006 and 2011) IR(ME)R 2000 Medical exposures (e.g. patients) Enforced by Care Quality Commission IR(ME)R 2000 was replaced by IR(ME)R 2017.
206 Principles of Patient Protection Justification (benefits must outweigh the risks) Optimisation (keep doses As Low As Reasonably Practicable) (consistent with the intended diagnostic purpose) Dose Constraints (20 msv per year for Classified Persons) (1 msv per year for members of the public) (no dose limits for medical exposures) (must set limits for research programs) (must set limits for carers and comforters)
207 Duty Holders under IR(ME)R 2000 The Employer provides a framework of policies and procedures The Referrer ( Prescriber in most EU countries) must supply sufficient clinical information to allow the exposure to be justified The Practitioner is responsible for justifying the exposure in terms of benefits versus risks The Operator is responsible for carrying it out safely.
208 Employer Employers (e.g. practice owners, or Trusts) must set up written policies and procedures They must also identify those individuals who can refer patients. As a minimum, this would be a list of dentists they agree to accept referrals from. Best Practice would be to have a written Service Level Agreement (SLA) between the referring dentist and the practice owner / Trust.
209 Employer s Procedures Correctly identify patient to be exposed Establish whether the patient may be pregnant (not a contra-indication for dental x-rays in most cases) Identify individuals entitled to act as referrer, practitioner, operator Record an evaluation for each exposure including factors relevant to patient dose Ensure accidental or unintended exposures are kept ALARP Set Dose Constraints for Carers and Comforters Set Dose Constraints for Research Programs.
210 Employer s Procedures Ensure referrer, practitioner and patient are informed of any significant accidental or unintended exposure Document procedures to be observed for non-medical exposures (medico-legal, insurance, sports medicine ) Dose Constraints and guidance for exposure of carers and comforters Wherever practical and prior to an exposure, provide the patient with information relating to benefits and risks Ensure that QA programmes (written procedures, written protocols) are followed CT/CBCT equipment installed after 5 Feb 2018 must have the capacity to transfer all dose related parameters to the patient s exposure record.
211 Informed Consent We must convey information on the benefits and risks to those likely to be affected by it. We must not tell them: What is not understood What cannot be remembered What is not believable What is not relevant (Prof Jim Malone) For dental radiography, informative leaflets in the waiting room would usually be sufficient.
212 Accidental or Unintended Exposures Significant events (not defined) must be analysed, recorded and reported (including near misses) Includes equipment or procedural failures Duty of candour to disclose clinically significant (not defined) events to patient, referrer, practitioner professionals involved with the care of the patient If not in patient s best interests to inform patient then representatives must be informed instead.
213 Dose Reference Levels (DRLs) Local DRLs should be set for each type of x-ray procedure Local DRLs should not normally exceed National DRLs For intra-orals the National DRL is 1.7 mgy (entrance dose) For DPTs the National DRL is 67 mgy.cm for children and 93 mgy.cm 2 for adults (Dose Area Product, DAP)
214 Estimates of Population Doses Employers must collect dose estimates and provide these (when requested) in a form that allows generation of National DRLs
215 Practitioner Practitioner must decide if the exposure is justified (i.e. the benefits must outweigh the risks) Must take into account the objectives of the exposure and the characteristics of the patient Is there another way to obtain the required information? What do the Referral Guidelines say? Urgency of the procedure (e.g. pregnant women may prefer to postpone it).
216 Justifying the Exposure There must be procedures to ensure that a clinical evaluation of the outcome of the exposure is carried out and recorded If it is known, prior to the exposure, that no clinical evaluation will occur then the procedure cannot be justified and the exposure must not take place If exposure will not change the patient s management it cannot be justified and must not take place.
217 Referrer Referrers may prescribe (request) x-ray examinations. They must be registered health care professionals. They must provide sufficient clinical information to substantiate the need for an x-ray examination. A history and clinical examination of the patient is essential prior to any request for an exposure. Previous x-ray examinations should also be investigated Routine x-rays are not allowed.
218 Operator Operators are responsible for carrying out the exposure safely. They should ensure the dose from the exposure is as low as reasonably practicable and consistent with the intended diagnostic purpose dose should not be so low as to give nondiagnostic images There should be written protocols in place for each type of examination If the dose is above the Diagnostic Reference Levels (DRL) the reason should be recorded.
219 Medical Physics Expert (MPE) Under IRR 2017 dental practices have to appoint an RPA Under IR(ME)R 2017 they have to appoint an MPE (who will often be the same person): MPE to be available for consultation on Optimisation Give advice on radiological equipment Setting of local DRLs Establish and maintain QA programme A list of RPAs and MPEs is available at
220 Optimisation Want to Optimise Benefit to Patient* Risk to Patient * not to the dentist!

221 CBCT Scans Risk Exposure to ionising radiation Might induce a cancer Might induce a hereditary defect Benefit Accurately pre-plan the treatment Less risk of damaging a critical structure Reduce operating time Improved aesthetic results Clinical Decision
 Reduces the risk without loss of benefit in most cases.")
222 Dose Practical ways to Reduce the Risk CBCT Scans: 1. Reduce the Height (vertical collimation) Reduces the risk without loss of benefit in most cases. Absorbed Dose outside primary beam is effectively zero
223 CBCT Scans 2. Reduce the mas (tube current, scan time) - Reducing the mas may have a negative impact on image quality - On some scanners, the voxel size is linked to the mas
 There may be some loss of")
224 3. Reduce the Width (horizontal collimation) X-ray Tube Detector Absorbed Dose outside primary beam is not zero (about 50% from SEDENTEXCT measurements) There may be some loss of benefit

225 Sorry mate no can do!
226 Summary of Changes in IR(ME)R 2017 Evolution of IR(ME)R 2000, not revolution Now covers non-medical imaging using medical radiological equipment (replaces medico-legal exposures ) Doses to comforters and carers must be justified and optimised and are subject to constraints Clarification of Medical Physics Expert (MPE) role Equipment QA is now addressed in IR(ME)R instead of IRR.
227 Training Requirements IRR 2017 and IR(ME)R 2017 Employers must maintain an up-to-date record of training, available for inspection, with date and nature of training recorded.
228 Practitioner Training Practitioners must have received adequate training both in radiation safety and clinical aspects (e.g. selection criteria) - for dentists this would normally be a degree course - must keep up to date with CPD
229 Operator Training Operators must have received adequate training specific to the tasks that they undertake - dental nurses, hygienists, therapists etc required to take x-rays would normally require the Certificate in Dental Radiography or equivalent - must receive training on practical aspects of operating the equipment - must keep up to date with CPD
230 Referrer Training There are no specific requirements in IR(ME)R 2017 for Referrer training, however, many people believe that training of Referrers would be beneficial, especially for Dental CBCT.

231
232


233
234 Radiology Reports IR(ME)R 2017 requires a clinical evaluation of the outcome of each exposure (other than for carers and comforters) and that this must be recorded. There is no legal requirement to send the images to a Radiologist for reporting If you have received sufficient training, it is good practice to report on the images yourself If you haven t received sufficient training, or if you suspect pathology may be present, it is good practice to send the images to a Specialist in Dental and Maxillofacial Radiology for a Report.
235 Due Diligence In any proceedings against any person for an offence consisting of the contravention of these Regulations it is a defence for that person to show that the person took all reasonable steps and exercised all due diligence to avoid committing the offence Document everything!
R Companion Guide to be published. IR(ME)R 2017 legislation is available here: www.legislation.gov.")
236 Guidance Documents New Approved Code of Practice L121 (costs 27) Revised Medical and Dental Guidance Notes to be published. Guidance Notes for Dental Practitioners on the Safe Use of X-Ray Equipment no updates planned. IR(ME)R Companion Guide to be published. IR(ME)R 2017 legislation is available here:
R 2000, equipment To be revised for IRR 2017 and IR(ME)R 2017 IPEM 2002 Costs")
237 Medical and Dental Guidance Notes Provide general guidance on good practice Not an attempt to interpret legal requirements Following the guidance is not compulsory but should be sufficient to comply with the law Covers IR99, IR(ME)R 2000, equipment To be revised for IRR 2017 and IR(ME)R 2017 IPEM 2002 Costs 20


238
Image Diagnostic Technology Ltd 53 Windermere Road, London W5 4TJ Tel: +44 (0)
") Image Diagnostic Technology Ltd 53 Windermere Road, London W5 4TJ Tel: +44 (0)20 8819 9158 www.idtscans.com email: info@idtscans.com Diagnostic Imaging and Radiation Safety Anthony Reynolds BA MSc PhD
Image Diagnostic Technology Ltd 53 Windermere Road, London W5 4TJ Tel: +44 (0)20 8819 9158 www.idtscans.com email: info@idtscans.com Diagnostic Imaging and Radiation Safety Anthony Reynolds BA MSc PhD
SUMMARY AND EXTRACTS FROM THE 2010 GUIDANCE ON THE SAFE USE OF DENTAL CONE BEAM CT (COMPUTED TOMOGRAPHY) EQUIPMENT
 EQUIPMENT") SUMMARY AND EXTRACTS FROM THE 2010 GUIDANCE ON THE SAFE USE OF DENTAL CONE BEAM CT (COMPUTED TOMOGRAPHY) EQUIPMENT The use of dental CBCT equipment must comply with all the regulations (IRR99 and IR(ME)R2000)
SUMMARY AND EXTRACTS FROM THE 2010 GUIDANCE ON THE SAFE USE OF DENTAL CONE BEAM CT (COMPUTED TOMOGRAPHY) EQUIPMENT The use of dental CBCT equipment must comply with all the regulations (IRR99 and IR(ME)R2000)
IONISING RADIATION REGULATIONS 99
 IONISING RADIATION REGULATIONS 99 & IRMER IONISING RADIATION MEDICAL EXPOSURE REGULATIONS BARBARA LAMB Specialist Radiographer Dental and maxillofacial radiography BarbaraHLamb@googlemail.com 07775994424
IONISING RADIATION REGULATIONS 99 & IRMER IONISING RADIATION MEDICAL EXPOSURE REGULATIONS BARBARA LAMB Specialist Radiographer Dental and maxillofacial radiography BarbaraHLamb@googlemail.com 07775994424
The checklist for the use of Ionising Radiation in Primary Dental Care. Not fully compliant
 The checklist for the use of Ionising Radiation in Primary Dental Care Health and Safety Executive (HSE) 1 The practice has registered with the HSE that radiographic equipment is being used on the premise
The checklist for the use of Ionising Radiation in Primary Dental Care Health and Safety Executive (HSE) 1 The practice has registered with the HSE that radiographic equipment is being used on the premise
Information and Guidance
 Health and Safety Executive (HSE) 1 The practice has registered with the HSE that radiographic equipment is being used on the premise and confirmed compliance with IRR17 by 5/2/2018. 2 HSE have confirmed
Health and Safety Executive (HSE) 1 The practice has registered with the HSE that radiographic equipment is being used on the premise and confirmed compliance with IRR17 by 5/2/2018. 2 HSE have confirmed
IRMER Ionising Radiation Medical Exposure Regulations
 IRMER Ionising Radiation Medical Exposure Regulations Download for information at www.scottishdental.org IONISING RADIATION (MEDICAL EXPOSURE ) REGULATION 2000 (as Amended) (IR(ME)R AN EXPLANATION GUIDE
IRMER Ionising Radiation Medical Exposure Regulations Download for information at www.scottishdental.org IONISING RADIATION (MEDICAL EXPOSURE ) REGULATION 2000 (as Amended) (IR(ME)R AN EXPLANATION GUIDE
Higher National Unit specification: general information
 Higher National Unit specification: general information Unit code: H0AH 36 Superclass: PF Publication date: February 2015 Source: Scottish Qualifications Authority Version: 05 Unit purpose This Unit is
Higher National Unit specification: general information Unit code: H0AH 36 Superclass: PF Publication date: February 2015 Source: Scottish Qualifications Authority Version: 05 Unit purpose This Unit is
BRITISH SOCIETY OF DENTAL AND MAXILLOFACIAL RADIOLOGY CORE CURRICULA IN DENTAL RADIOGRAPHY AND RADIOLOGY FOR THE DENTAL TEAM
 BRITISH SOCIETY OF DENTAL AND MAXILLOFACIAL RADIOLOGY CORE CURRICULA IN DENTAL RADIOGRAPHY AND RADIOLOGY FOR THE DENTAL TEAM 2015 0 INTRODUCTION The original core curriculum in Dental Radiography and Radiology
BRITISH SOCIETY OF DENTAL AND MAXILLOFACIAL RADIOLOGY CORE CURRICULA IN DENTAL RADIOGRAPHY AND RADIOLOGY FOR THE DENTAL TEAM 2015 0 INTRODUCTION The original core curriculum in Dental Radiography and Radiology
Image Diagnostic Technology Ltd IDT Ireland, 15 Market Street, Kinsale, Co. Cork, Ireland P17 XN65 Tel: Mob: IRL:
 Image Diagnostic Technology Ltd IDT Ireland, 15 Market Street, Kinsale, Co. Cork, Ireland P17 XN65 Tel: +44 20 8819 9158 Mob: +44 7767 366596 IRL: +353 21 470 9501 Web: www.simplantscans.com Email: info@ctscan.co.uk
Image Diagnostic Technology Ltd IDT Ireland, 15 Market Street, Kinsale, Co. Cork, Ireland P17 XN65 Tel: +44 20 8819 9158 Mob: +44 7767 366596 IRL: +353 21 470 9501 Web: www.simplantscans.com Email: info@ctscan.co.uk
Table of Contents. Introduction 3. Background 4
 Training manual Table of Contents Introduction 3 Background 4 What are X-rays? 4 How are X-rays Generated? 5 Primary and Scatter Radiation 6 Interactions with Matter 6 Biological Effects of Radiation 7
Training manual Table of Contents Introduction 3 Background 4 What are X-rays? 4 How are X-rays Generated? 5 Primary and Scatter Radiation 6 Interactions with Matter 6 Biological Effects of Radiation 7
Health and Safety Policy Arrangements: Radiation Protection Guidelines
 Health and Safety Policy Arrangements: Radiation Protection Guidelines Author: Dr N. Sarrami Date of Approval: 12//2010 Due Review Date: 12//2012 1 Radiation Protection Guidelines CONTENTS Section Section
Health and Safety Policy Arrangements: Radiation Protection Guidelines Author: Dr N. Sarrami Date of Approval: 12//2010 Due Review Date: 12//2012 1 Radiation Protection Guidelines CONTENTS Section Section
Appendix I. List of stakeholders consulted with on the Patient Radiation Protection Manual and members of the Medical Exposure Radiation Unit
 References References The accuracy, quality and relevance of these works are not guaranteed or uniform and more recent information may have superseded these works. This list is not exhaustive. It does
References References The accuracy, quality and relevance of these works are not guaranteed or uniform and more recent information may have superseded these works. This list is not exhaustive. It does
Code of Practice for Radiation Protection in Dentistry. Code of Practice For Radiation Protection in Dentistry
 Code of Practice for Radiation Protection in Dentistry Code of Practice For Radiation Protection in Dentistry 10 OCTOBER 2017 CONTENTS 1. INTRODUCTION... 3 1.0 CITATION... 3 1.1 BACKGROUND... 3 1.2 PURPOSE
Code of Practice for Radiation Protection in Dentistry Code of Practice For Radiation Protection in Dentistry 10 OCTOBER 2017 CONTENTS 1. INTRODUCTION... 3 1.0 CITATION... 3 1.1 BACKGROUND... 3 1.2 PURPOSE
On successful completion of the Unit the learner will be able to:
 Higher National Unit specification General information Unit code: H9R8 34 Superclass: PF Publication date: September 2015 Source: Scottish Qualifications Authority Version: 03 Unit purpose This Unit is
Higher National Unit specification General information Unit code: H9R8 34 Superclass: PF Publication date: September 2015 Source: Scottish Qualifications Authority Version: 03 Unit purpose This Unit is
created by high-voltage devices Examples include medical and dental x-rays, light, microwaves and nuclear energy
 What is radiation? Radiation is energy emitted from a source, that travels through space and can penetrate matter. Listed below are two types that we are exposed to and contribute to our overall radiation
What is radiation? Radiation is energy emitted from a source, that travels through space and can penetrate matter. Listed below are two types that we are exposed to and contribute to our overall radiation
Trust Policy 218 Ionising Radiation Safety Policy
 Trust Policy 218 Ionising Radiation Safety Policy Purpose Date Version August 2016 7 To ensure that Plymouth Hospitals NHS Trust complies with all relevant legislation with regard to the use of ionising
Trust Policy 218 Ionising Radiation Safety Policy Purpose Date Version August 2016 7 To ensure that Plymouth Hospitals NHS Trust complies with all relevant legislation with regard to the use of ionising
Ionising Radiation Policy
 Ionising Radiation Policy CONTENTS 1. University Policy. 2. Procedures / Guidance. 2.1 Responsibilities of the Deans of Schools and/or Heads of Departments 2.2 Radiation Protection Advisor / Radiation
Ionising Radiation Policy CONTENTS 1. University Policy. 2. Procedures / Guidance. 2.1 Responsibilities of the Deans of Schools and/or Heads of Departments 2.2 Radiation Protection Advisor / Radiation
Kodak Dental Radiography Series. Radiation Safety in Dental Radiography. Dental
 Kodak Dental Radiography Series Radiation Safety in Dental Radiography Dental Radiation Safety in Dental Radiography The goal of dental radiography is to obtain diagnostic information while keeping the
Kodak Dental Radiography Series Radiation Safety in Dental Radiography Dental Radiation Safety in Dental Radiography The goal of dental radiography is to obtain diagnostic information while keeping the
RADIATION SAFETY POLICY. Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead: Approved By:
 RADIATION SAFETY POLICY CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead: Approved By: Policy Health
RADIATION SAFETY POLICY CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead: Approved By: Policy Health
 Page 1 of 5 Patient Safety: Radiation Dose in X-Ray and CT Exams What are x-rays and what do they do? X-rays are forms of radiant energy, like light or radio waves. Unlike light, x-rays can penetrate the
Page 1 of 5 Patient Safety: Radiation Dose in X-Ray and CT Exams What are x-rays and what do they do? X-rays are forms of radiant energy, like light or radio waves. Unlike light, x-rays can penetrate the
The College of Dental Surgeons of Saskatchewan Radiation and Imaging Standard
 The College of Dental Surgeons of Saskatchewan Radiation and Imaging Standard Legislation Radiation safety has long been a priority in Saskatchewan. This province, the first in Canada to have radiation
The College of Dental Surgeons of Saskatchewan Radiation and Imaging Standard Legislation Radiation safety has long been a priority in Saskatchewan. This province, the first in Canada to have radiation
COMMON COURSE OUTLINE: Course discipline/number/title: DS 1300: Dental Radiology
 COMMON COURSE OUTLINE: Course discipline/number/title: DS 1300: Dental Radiology A. CATALOG DESCRIPTION 1. Credits: 3 2. Hours/Week: 2 hour lecture, 2 hour lab 3. Prerequisites (Course discipline/number):
COMMON COURSE OUTLINE: Course discipline/number/title: DS 1300: Dental Radiology A. CATALOG DESCRIPTION 1. Credits: 3 2. Hours/Week: 2 hour lecture, 2 hour lab 3. Prerequisites (Course discipline/number):
Managing Cone Beam CT Dose in Paediatric Dental Imaging
 Ask EuroSafe Imaging Tips & Tricks Paediatric Imaging Working Group Managing Cone Beam CT Dose in Paediatric Dental Imaging Raija Seuri (HUS Medical Imaging Center, FI) Cristina Almeida (Centro Hospitalar
Ask EuroSafe Imaging Tips & Tricks Paediatric Imaging Working Group Managing Cone Beam CT Dose in Paediatric Dental Imaging Raija Seuri (HUS Medical Imaging Center, FI) Cristina Almeida (Centro Hospitalar
Ionising Radiations Regulations 2017
 Health and Safety Executive Ionising Radiations Regulations 2017 New Provisions etc. James Taylor Principal Specialist Inspector (Radiation) Tel: 07879 661820 email: james.taylor@hse.gov.uk Graded Approach
Health and Safety Executive Ionising Radiations Regulations 2017 New Provisions etc. James Taylor Principal Specialist Inspector (Radiation) Tel: 07879 661820 email: james.taylor@hse.gov.uk Graded Approach
Radiation Safety - Things You Need to Know
 Radiation Safety - Things You Need to Know Michael Casey Ph.D. Phlebotomy Autumn Seminar 13 th October 2012 Radiation is a form of energy transport What is Radiation? It is caused by electrical disturbances
Radiation Safety - Things You Need to Know Michael Casey Ph.D. Phlebotomy Autumn Seminar 13 th October 2012 Radiation is a form of energy transport What is Radiation? It is caused by electrical disturbances
Ionising Radiation Safety Type: Policy Register No: Status: Public. For compliance with the Ionising Radiations Regulations 1999
 Ionising Radiation Safety Type: Policy Register : 14022 Status: Public Developed in response to: Contributes to CCQ Core Outcome 4 For compliance with the Ionising Radiations Regulations 1999 Consulted
Ionising Radiation Safety Type: Policy Register : 14022 Status: Public Developed in response to: Contributes to CCQ Core Outcome 4 For compliance with the Ionising Radiations Regulations 1999 Consulted
CAMOSUN COLLEGE School of Health & Human Services Dental Programs. DHYG 131 Dental Radiology. Winter, 2013 COURSE OUTLINE
 CAMOSUN COLLEGE School of Health & Human Services Dental Programs DHYG 131 Dental Radiology Winter, 2013 COURSE OUTLINE The Approved Course Description is available on the web @ http://camosun.ca/learn/calendar/current/web/dhyg.html
CAMOSUN COLLEGE School of Health & Human Services Dental Programs DHYG 131 Dental Radiology Winter, 2013 COURSE OUTLINE The Approved Course Description is available on the web @ http://camosun.ca/learn/calendar/current/web/dhyg.html
X-rays How safe are they?
 X-rays How safe are they? Patient information Thirty years ago, X-rays were the only way to see what was going on inside your body. Now other methods of medical imaging are available, some using different
X-rays How safe are they? Patient information Thirty years ago, X-rays were the only way to see what was going on inside your body. Now other methods of medical imaging are available, some using different
Dental Radiography Core Subject. Digital Radiography
 Dental Radiography Core Subject Digital Radiography Aims: To develop an understanding of the history of digital radiography, the different types of digital x-rays and the advantages and disadvantages of
Dental Radiography Core Subject Digital Radiography Aims: To develop an understanding of the history of digital radiography, the different types of digital x-rays and the advantages and disadvantages of
Questions for ionising radiation applications
 Questions for ionising radiation applications Note from HSE November 2017 This document represents a near-final draft of the questions that HSE will be asking those who apply via the graded approach online
Questions for ionising radiation applications Note from HSE November 2017 This document represents a near-final draft of the questions that HSE will be asking those who apply via the graded approach online
RADIOGRAPHY & RADIATION PROTECTION
 RADIOGRAPHY & RADIATION PROTECTION F`` A Guide for the Dental Team CPD Module 020 Page 2 Fig.1 RADIOGRAPHY AND RADIATION PROTECTION CPD Module 020 Suitability Dentists Dental Care Professionals Receptionists
RADIOGRAPHY & RADIATION PROTECTION F`` A Guide for the Dental Team CPD Module 020 Page 2 Fig.1 RADIOGRAPHY AND RADIATION PROTECTION CPD Module 020 Suitability Dentists Dental Care Professionals Receptionists
UQ X-ray Safety Training Module
 UQ X-ray Safety Training Module 23 January 2018, v2 1 UQ X-ray Safety Training Module Course Overview: This training module has been developed for workers at the University of Queensland, and forms part
UQ X-ray Safety Training Module 23 January 2018, v2 1 UQ X-ray Safety Training Module Course Overview: This training module has been developed for workers at the University of Queensland, and forms part
Doses to Patients arising from Dental X-ray Examinations in the UK, A Review of Dental X-ray Protection Service Data
 HPA-RPD-22 Doses to Patients arising from Dental X-ray Examinations in the UK, 22 24 A Review of Dental X-ray Protection Service Data A D Gulson, T A Knapp and P G Ramsden ABSTRACT The Dental X-ray Protection
HPA-RPD-22 Doses to Patients arising from Dental X-ray Examinations in the UK, 22 24 A Review of Dental X-ray Protection Service Data A D Gulson, T A Knapp and P G Ramsden ABSTRACT The Dental X-ray Protection
User Guide for Dental and Maxillofacial Cone Beam Computed Tomography (CBCT)
") User Guide for Dental and Maxillofacial Cone Beam Computed Tomography (CBCT) Poster No.: C-0756 Congress: ECR 2014 Type: Educational Exhibit Authors: J. Ukkonen, J. Asp; Helsinki/FI Keywords: Education
User Guide for Dental and Maxillofacial Cone Beam Computed Tomography (CBCT) Poster No.: C-0756 Congress: ECR 2014 Type: Educational Exhibit Authors: J. Ukkonen, J. Asp; Helsinki/FI Keywords: Education
STANDARD OF PRACTICE. Dental CT Scanners CONTENTS. April 2011
 April 2011 STANDARD OF PRACTICE Approved by Council April 18, 2011 Dental CT Scanners This document is the standard of practice in relation to the use of dental computed tomography (CT) scanners with respect
April 2011 STANDARD OF PRACTICE Approved by Council April 18, 2011 Dental CT Scanners This document is the standard of practice in relation to the use of dental computed tomography (CT) scanners with respect
Radiation Safety Manual
 King Abdulaziz University Faculty of Dentistry Radiation Safety Manual FOR X-RAY EQUIPMENT OPERATORS October 2009 Radioactivity and Radiation All matter in our environment is made of atoms. Most atoms
King Abdulaziz University Faculty of Dentistry Radiation Safety Manual FOR X-RAY EQUIPMENT OPERATORS October 2009 Radioactivity and Radiation All matter in our environment is made of atoms. Most atoms
Managing the imaging dose during Image-guided Radiotherapy. Martin J Murphy PhD Department of Radiation Oncology Virginia Commonwealth University
 Managing the imaging dose during Image-guided Radiotherapy Martin J Murphy PhD Department of Radiation Oncology Virginia Commonwealth University Radiographic image guidance has emerged as the new paradigm
Managing the imaging dose during Image-guided Radiotherapy Martin J Murphy PhD Department of Radiation Oncology Virginia Commonwealth University Radiographic image guidance has emerged as the new paradigm
Radiation Safety for New Medical Physics Graduate Students
 Radiation Safety for New Medical Physics Graduate Students John Vetter, PhD Medical Physics Department UW School of Medicine & Public Health Background and Purpose of This Training This is intended as
Radiation Safety for New Medical Physics Graduate Students John Vetter, PhD Medical Physics Department UW School of Medicine & Public Health Background and Purpose of This Training This is intended as
making a referral for breast imaging Standard Operating Procedure
 Document Control Title Reporting Radiographer Author Directorate Surgery Date Version Issued 0.1 May 2016 Status Draft Author s job title Reporting Radiographer Department Breast Imaging Comment / Changes
Document Control Title Reporting Radiographer Author Directorate Surgery Date Version Issued 0.1 May 2016 Status Draft Author s job title Reporting Radiographer Department Breast Imaging Comment / Changes
A Guide to IR(ME)R for Referrers
R for Referrers") A Guide to IR(ME)R for Referrers Ionising Radiation (Medical Exposure) Regulations 2017 IR(ME)R Radiology Department Information for Staff 1 The Ionising Radiation (Medical Exposures) Regulations 2017
A Guide to IR(ME)R for Referrers Ionising Radiation (Medical Exposure) Regulations 2017 IR(ME)R Radiology Department Information for Staff 1 The Ionising Radiation (Medical Exposures) Regulations 2017
CT Scanning Protocol For V2R Guided Surgery Solutions
 CT Scanning Protocol For V2R Guided Surgery Solutions 2 V2R CT Scanning Protocol \\ Contents Contents General requirements... 3 V2R Dual Scan Protocol... 5 V2R Single Scan Protocol... 8 Overview... 10
CT Scanning Protocol For V2R Guided Surgery Solutions 2 V2R CT Scanning Protocol \\ Contents Contents General requirements... 3 V2R Dual Scan Protocol... 5 V2R Single Scan Protocol... 8 Overview... 10
Proposed Radiation Safety Regulations: Submission form
 Proposed Radiation Safety Regulations: Submission form Making a submission This form is designed to assist submitters responding to the discussion points in Proposed Radiation Safety Regulations: A consultation
Proposed Radiation Safety Regulations: Submission form Making a submission This form is designed to assist submitters responding to the discussion points in Proposed Radiation Safety Regulations: A consultation
Dental Radiography STANDARDS & GUIDELINES TABLE OF CONTENTS. College of Dental Surgeons of BC
 STANDARDS & GUIDELINES Dental Radiography TABLE OF CONTENTS Standards and guidelines inform practitioners and the public of CDSBC s expectations for registrants. This document primarily contains guidelines
STANDARDS & GUIDELINES Dental Radiography TABLE OF CONTENTS Standards and guidelines inform practitioners and the public of CDSBC s expectations for registrants. This document primarily contains guidelines
NEW JERSEY RADIOLOGIC TECHNOLOGY BOARD OF EXAMINERS (BOARD) DENTAL RADIOGRAPHY CURRICULUM REQUIREMENTS GENERAL REQUIREMENTS
 DENTAL RADIOGRAPHY CURRICULUM REQUIREMENTS GENERAL REQUIREMENTS") CHRIS CHRISTIE DEPARTMENT OF ENVIRONMENTAL PROTECTION BOB MARTIN Governor Division of Environmental Safety and Health Commissioner Bureau of X-Ray Compliance, Technologist Certification Section KIM GUADAGNO
CHRIS CHRISTIE DEPARTMENT OF ENVIRONMENTAL PROTECTION BOB MARTIN Governor Division of Environmental Safety and Health Commissioner Bureau of X-Ray Compliance, Technologist Certification Section KIM GUADAGNO
RADIATION SAFETY. Junior Radiology Course
 RADIATION SAFETY Junior Radiology Course Expectations for the Junior Radiology Course Medical School wants students to learn basic principles, factual knowledge, safety info, etc. Medical Students want
RADIATION SAFETY Junior Radiology Course Expectations for the Junior Radiology Course Medical School wants students to learn basic principles, factual knowledge, safety info, etc. Medical Students want
Dental Hygiene Spring 2018 Summer 2014 Fall COURSE OUTLINE DHT 1032 Dental Radiography 2 Credit Hours
 COURSE OUTLINE DHT 1032 Dental Radiography 2 Credit Hours Course Description This course prepares the dental hygiene student to expose, process and critique intra and extraoral radiographs for clinical
COURSE OUTLINE DHT 1032 Dental Radiography 2 Credit Hours Course Description This course prepares the dental hygiene student to expose, process and critique intra and extraoral radiographs for clinical
Basic radiation protection & radiobiology
 Basic radiation protection & radiobiology By Dr. Mohsen Dashti Patient care & management 202 Wednesday, October 13, 2010 Ionizing radiation. Discussion issues Protecting the patient. Protecting the radiographer.
Basic radiation protection & radiobiology By Dr. Mohsen Dashti Patient care & management 202 Wednesday, October 13, 2010 Ionizing radiation. Discussion issues Protecting the patient. Protecting the radiographer.
Radiation Safety For Anesthesiologists. R2 Pinyada Pisutchareonpong R2 Nawaporn Sateantantikul Supervised by Aj Chaowanan Khamtuicrua
 Radiation Safety For Anesthesiologists R2 Pinyada Pisutchareonpong R2 Nawaporn Sateantantikul Supervised by Aj Chaowanan Khamtuicrua Modern World Non Ionizing VS Ionizing Non Ionizing Harmless Ex. visible
Radiation Safety For Anesthesiologists R2 Pinyada Pisutchareonpong R2 Nawaporn Sateantantikul Supervised by Aj Chaowanan Khamtuicrua Modern World Non Ionizing VS Ionizing Non Ionizing Harmless Ex. visible
Radiation Safety & Determining Need for Radiographs
 Radiation Safety & Determining Need for Radiographs Guidelines for Radiographic Examination All radiation is harmful! These guidelines have been established to protect the patient and operator from unnecessary
Radiation Safety & Determining Need for Radiographs Guidelines for Radiographic Examination All radiation is harmful! These guidelines have been established to protect the patient and operator from unnecessary
Head to new heights with your imaging SCANORA 3D
 SCANORA 3D Head to new heights with your imaging Benefits at a glance The solution for dentomaxillofacial and ENT imaging Easy Patient seated for added stability during exposure. Clear, self-explinatory
SCANORA 3D Head to new heights with your imaging Benefits at a glance The solution for dentomaxillofacial and ENT imaging Easy Patient seated for added stability during exposure. Clear, self-explinatory
Patient Management Image Selection Radiation Biology, Dosimetry & Protection
 Patient Management Image Selection Radiation Biology, Dosimetry & Protection Objectives: Following this course, the participants will have the information necessary to: 1. Identify the techniques used
Patient Management Image Selection Radiation Biology, Dosimetry & Protection Objectives: Following this course, the participants will have the information necessary to: 1. Identify the techniques used
Radiation Safety in the Catheterization Lab
 SCAI FALL FELLOWS COURSE - 2015 Radiation Safety in the Catheterization Lab V. Vivian Dimas, MD, FSCAI Associate Professor Pediatrics, Cardiology UT Southwestern Medical Center Dallas TX None Disclosures
SCAI FALL FELLOWS COURSE - 2015 Radiation Safety in the Catheterization Lab V. Vivian Dimas, MD, FSCAI Associate Professor Pediatrics, Cardiology UT Southwestern Medical Center Dallas TX None Disclosures
X-RAY REGULATORY GUIDE
 Minnesota Department of Health Radiation Control, X-ray Unit Protecting, maintaining and improving the health of all Minnesotans by promoting radiation safety through guidance and collaboration with the
Minnesota Department of Health Radiation Control, X-ray Unit Protecting, maintaining and improving the health of all Minnesotans by promoting radiation safety through guidance and collaboration with the
Implementation of the 2012 ACR CT QC Manual in a Community Hospital Setting BRUCE E. HASSELQUIST, PH.D., DABR, DABSNM ASPIRUS WAUSAU HOSPITAL
 Implementation of the 2012 ACR CT QC Manual in a Community Hospital Setting BRUCE E. HASSELQUIST, PH.D., DABR, DABSNM ASPIRUS WAUSAU HOSPITAL Conflict of Interest Disclaimer Employee of Aspirus Wausau
Implementation of the 2012 ACR CT QC Manual in a Community Hospital Setting BRUCE E. HASSELQUIST, PH.D., DABR, DABSNM ASPIRUS WAUSAU HOSPITAL Conflict of Interest Disclaimer Employee of Aspirus Wausau
The wonderful world of dental radiology
 The wonderful world of dental radiology Dr Christine Hawke BSc(Vet)(Hons) BVSc(Hons) PhD MACVSc (Veterinary Dentistry) PO Box 3001 Willoughby North 2068 Phone: 0408 782 611 Email: christine@sydneypetdentistry.com.au
The wonderful world of dental radiology Dr Christine Hawke BSc(Vet)(Hons) BVSc(Hons) PhD MACVSc (Veterinary Dentistry) PO Box 3001 Willoughby North 2068 Phone: 0408 782 611 Email: christine@sydneypetdentistry.com.au
Dental Intraoral X-ray Systems
 Dental Intraoral X-ray Systems PROPOSED REVISIONS TO 4732.XXXX, 2.0 4732.#### DENTAL INTRAORAL X-RAY SYSTEMS; STATIONARY AND MOBILE. Commented [JC(1]: Based on part 4732.0880. Subpart 1. Applicability.
Dental Intraoral X-ray Systems PROPOSED REVISIONS TO 4732.XXXX, 2.0 4732.#### DENTAL INTRAORAL X-RAY SYSTEMS; STATIONARY AND MOBILE. Commented [JC(1]: Based on part 4732.0880. Subpart 1. Applicability.
ICRP Recommendations Evolution or Revolution? John R Cooper Main Commission
 ICRP Recommendations Evolution or Revolution? John R Cooper Main Commission 3 September 2009 ICRP Recommendations 1. Reasons for new Recommendations 2. Summary of health risks 3. Summary of changes to
ICRP Recommendations Evolution or Revolution? John R Cooper Main Commission 3 September 2009 ICRP Recommendations 1. Reasons for new Recommendations 2. Summary of health risks 3. Summary of changes to
Agenda: Dental Cone Beam Imaging
 Cone Beam Imaging Agenda: Dental Cone Beam Imaging *Definition and Functionality *Usage and diagnostics benefits *Comparative radiation information *Federal regulatory responsibilities: manufacturing *State
Cone Beam Imaging Agenda: Dental Cone Beam Imaging *Definition and Functionality *Usage and diagnostics benefits *Comparative radiation information *Federal regulatory responsibilities: manufacturing *State
X-ray (Radiography) - Chest
 - Chest") Scan for mobile link. X-ray (Radiography) - Chest Chest x-ray uses a very small dose of ionizing radiation to produce pictures of the inside of the chest. It is used to evaluate the lungs, heart and chest
Scan for mobile link. X-ray (Radiography) - Chest Chest x-ray uses a very small dose of ionizing radiation to produce pictures of the inside of the chest. It is used to evaluate the lungs, heart and chest
NEW JERSEY RADIOLOGIC TECHNOLOGY BOARD OF EXAMINERS (BOARD) DENTAL RADIOGRAPHY CURRICULUM REQUIREMENTS
 DENTAL RADIOGRAPHY CURRICULUM REQUIREMENTS") CHRIS CHRISTIE DEPARTMENT OF ENVIRONMENTAL PROTECTION BOB MARTIN Governor Division of Environmental Safety and Health Commissioner Bureau of X-Ray Compliance, Technologist Certification Section KIM GUADAGNO
CHRIS CHRISTIE DEPARTMENT OF ENVIRONMENTAL PROTECTION BOB MARTIN Governor Division of Environmental Safety and Health Commissioner Bureau of X-Ray Compliance, Technologist Certification Section KIM GUADAGNO
CERTIFICATION OF PERSONNEL IN RADIATION SAFETY AND PROTECTION
 Certification Services Division Newton Building, St Georges Avenue Northampton NN2 6JB United Kingdom Tel: +44(0) 1604-893811 Fax: +44(0) 1604-893868 E-mail: pcn@bindt.org PCN/GEN APPENDIX E3 ISSUE 8 Further
Certification Services Division Newton Building, St Georges Avenue Northampton NN2 6JB United Kingdom Tel: +44(0) 1604-893811 Fax: +44(0) 1604-893868 E-mail: pcn@bindt.org PCN/GEN APPENDIX E3 ISSUE 8 Further
The use of lateral oblique radiographs in dental treatment planning for patients with special needs
 The use of lateral oblique radiographs in dental treatment planning for patients with special needs A Pradhan 1 and M Gryst 2 1. Senior Lecturer, Oral Health Centre, The University of Queensland, 2. Senior
The use of lateral oblique radiographs in dental treatment planning for patients with special needs A Pradhan 1 and M Gryst 2 1. Senior Lecturer, Oral Health Centre, The University of Queensland, 2. Senior
TEST GDP DCP. Dental Hygienists and Therapists. Radiography and Radiation Protection. Radiography and Radiation Protection IR(ME)R 2000
R 2000") Radiography and Radiation Protection IR(ME)R 2000 J Makdissi DDS IQE MMedSc FDSRCS(Eng.) DDRRCR Clinical Senior Lecturer and Honorary Consultant Dental and Maxillofacial Radiology GDP a) Radiation physics
Radiography and Radiation Protection IR(ME)R 2000 J Makdissi DDS IQE MMedSc FDSRCS(Eng.) DDRRCR Clinical Senior Lecturer and Honorary Consultant Dental and Maxillofacial Radiology GDP a) Radiation physics
Ionising radiation is EM radiation that causes ionisation of atoms. The minimum energy needed to ionise any atom is 12 ev.
 Radiation Dosimetry, Protection and Legislation Radiation is present in the environment naturally and we are all exposed to some extent. The effect this radiation has on humans depends on the type, source
Radiation Dosimetry, Protection and Legislation Radiation is present in the environment naturally and we are all exposed to some extent. The effect this radiation has on humans depends on the type, source
REGULATION: QUALITY ASSURANCE PROGRAMS FOR MEDICAL DIAGNOSTIC X-RAY INSTALLATIONS N.J.A.C. 7:28-22
 REGULATION: QUALITY ASSURANCE PROGRAMS FOR MEDICAL DIAGNOSTIC X-RAY INSTALLATIONS N.J.A.C. 7:28-22 New Jersey Department of Environmental Protection Bureau of X-ray Compliance PO Box 420, Mail Code 25-01
REGULATION: QUALITY ASSURANCE PROGRAMS FOR MEDICAL DIAGNOSTIC X-RAY INSTALLATIONS N.J.A.C. 7:28-22 New Jersey Department of Environmental Protection Bureau of X-ray Compliance PO Box 420, Mail Code 25-01
Radiation Safety Guide. Analytical X-Ray Equipment
 Radiation Safety Guide Analytical X-Ray Equipment Table of Content Page 1. Radiation 2 A. Radiation Quantities 2 B. Background Radiation 2 C. Biological Effect of Radiation 3 D. Radiation Injury To The
Radiation Safety Guide Analytical X-Ray Equipment Table of Content Page 1. Radiation 2 A. Radiation Quantities 2 B. Background Radiation 2 C. Biological Effect of Radiation 3 D. Radiation Injury To The
Utilize radiation safety principles to reduce the amount of radiation used to achieve desired clinical result.
 Minimizing Dose Understand the importance and methods of pre-procedure patient assessment including a review of previous radiologic exams, disease processes and anatomical considerations that may increase
Minimizing Dose Understand the importance and methods of pre-procedure patient assessment including a review of previous radiologic exams, disease processes and anatomical considerations that may increase
GUIDELINES ON IONISING RADIATION DOSE LIMITS AND ANNUAL LIMITS ON INTAKE OF RADIOACTIVE MATERIAL
 RADIATION PROTECTION AUTHORITY OF ZIMBABWE (RPAZ) RADIATION PROTECTION ACT [CHAPTER 15:15] GUIDELINES ON IONISING RADIATION DOSE LIMITS AND ANNUAL LIMITS ON INTAKE OF RADIOACTIVE MATERIAL Compiled by Radiation
RADIATION PROTECTION AUTHORITY OF ZIMBABWE (RPAZ) RADIATION PROTECTION ACT [CHAPTER 15:15] GUIDELINES ON IONISING RADIATION DOSE LIMITS AND ANNUAL LIMITS ON INTAKE OF RADIOACTIVE MATERIAL Compiled by Radiation
X-ray (Radiography) - Bone
 - Bone") Scan for mobile link. X-ray (Radiography) - Bone Bone x-ray uses a very small dose of ionizing radiation to produce pictures of any bone in the body. It is commonly used to diagnose fractured bones or
Scan for mobile link. X-ray (Radiography) - Bone Bone x-ray uses a very small dose of ionizing radiation to produce pictures of any bone in the body. It is commonly used to diagnose fractured bones or
Radiation Safety for Dental Auxiliaries. Susan W. Grammer, RDH, M.Ed. Course Content. A. Radiation History and the Use of Radiographs
 Radiation Safety for Dental Auxiliaries Susan W. Grammer, RDH, M.Ed. Course Content A. Radiation History and the Use of Radiographs B. Introduction to Physics C. X-ray Machine and Production of X-Rays
Radiation Safety for Dental Auxiliaries Susan W. Grammer, RDH, M.Ed. Course Content A. Radiation History and the Use of Radiographs B. Introduction to Physics C. X-ray Machine and Production of X-Rays
ACADEMY FOR DENTAL ASSISTANTS
 ACADEMY FOR DENTAL ASSISTANTS 12 Week Dental Assisting Program Section 2 Quiz Chapter 38 1. Exposure to radiation: a. no matter how small, has the potential to cause harmful biologic changes. b. has a
ACADEMY FOR DENTAL ASSISTANTS 12 Week Dental Assisting Program Section 2 Quiz Chapter 38 1. Exposure to radiation: a. no matter how small, has the potential to cause harmful biologic changes. b. has a
New York Radiation Health and Safety (NYR)
") New York Radiation Health and Safety (NYR) Exam Outline and Suggested References State Regulations Each state s dental board implements regulations and establishes rules for delegating legally allowable
New York Radiation Health and Safety (NYR) Exam Outline and Suggested References State Regulations Each state s dental board implements regulations and establishes rules for delegating legally allowable
Patti Edwards, Senior Radiographer, West Herts Hospitals, UK. February Radiation Safety
 Patti Edwards, Senior Radiographer, West Herts Hospitals, UK. February 2008. Radiation Safety Sub -headings Background Radiation Effects of Radiation Safe Levels Effective Doses ALARA Principle Radiation
Patti Edwards, Senior Radiographer, West Herts Hospitals, UK. February 2008. Radiation Safety Sub -headings Background Radiation Effects of Radiation Safe Levels Effective Doses ALARA Principle Radiation
The wonderful world of dental radiology
 The wonderful world of dental radiology Dr Christine Hawke BSc(Vet)(Hons) BVSc(Hons) PhD MACVSc (Veterinary Dentistry) PO Box 3001 Willoughby North 2068 Phone: 0408 782 611 Email: christine@sydneypetdentistry.com.au
The wonderful world of dental radiology Dr Christine Hawke BSc(Vet)(Hons) BVSc(Hons) PhD MACVSc (Veterinary Dentistry) PO Box 3001 Willoughby North 2068 Phone: 0408 782 611 Email: christine@sydneypetdentistry.com.au
IONISING RADIATION POLICY (for the Safe Use of)
") IONISING RADIATION POLICY (for the Safe Use of) Document Author Written By: Radiation Medical Expert Authorised Authorised By: Chief Executive Date: 1 April 2015 Date: 5 October 2015 Lead Director: Consultant
IONISING RADIATION POLICY (for the Safe Use of) Document Author Written By: Radiation Medical Expert Authorised Authorised By: Chief Executive Date: 1 April 2015 Date: 5 October 2015 Lead Director: Consultant
People Exposed to More Radiation from Medical Exams
 People Exposed to More Radiation from Medical Exams With its release of a new report, titled Ionizing Radiation Exposure of the Population of the United States (Report No. 160, 2009), the National Council
People Exposed to More Radiation from Medical Exams With its release of a new report, titled Ionizing Radiation Exposure of the Population of the United States (Report No. 160, 2009), the National Council
Debra Pennington, MD Director of Imaging Dell Children s Medical Center
 Debra Pennington, MD Director of Imaging Dell Children s Medical Center 1 Gray (Gy) is 1 J of radiation energy/ 1 kg matter (physical quantity absorbed dose) Diagnostic imaging doses in mgy (.001 Gy)
Debra Pennington, MD Director of Imaging Dell Children s Medical Center 1 Gray (Gy) is 1 J of radiation energy/ 1 kg matter (physical quantity absorbed dose) Diagnostic imaging doses in mgy (.001 Gy)
I AM SAFER. Reliable X-ray technology that reduces radiation exposure
 I AM SAFER Reliable X-ray technology that reduces radiation exposure EN 40 cm / 80 cm / 110 cm (16 / 31 / 43 ) 70 cm (27 ) 9 cm (3,5 ) 36 cm (14 ) 79 cm / 119 cm / 149 cm (31 / 46 / 59 ) 87 cm (34 ) 81
I AM SAFER Reliable X-ray technology that reduces radiation exposure EN 40 cm / 80 cm / 110 cm (16 / 31 / 43 ) 70 cm (27 ) 9 cm (3,5 ) 36 cm (14 ) 79 cm / 119 cm / 149 cm (31 / 46 / 59 ) 87 cm (34 ) 81
Managing Patient Dose in Computed Tomography (CT)
") Managing Patient Dose in Computed Tomography (CT) International Commission on Radiological Protection Information abstracted from ICRP Publication 87 Available at www.icrp.org Task Group: M.M. Rehani,
Managing Patient Dose in Computed Tomography (CT) International Commission on Radiological Protection Information abstracted from ICRP Publication 87 Available at www.icrp.org Task Group: M.M. Rehani,
RECTANGULAR COLLIMATION
 A SPECIAL REPORT RECTANGULAR COLLIMATION No longer a matter of choice! Robert Langlais DDS MS FACD University of Texas San Antonio, Texas This Special Report is made available by Interactive Diagnostic
A SPECIAL REPORT RECTANGULAR COLLIMATION No longer a matter of choice! Robert Langlais DDS MS FACD University of Texas San Antonio, Texas This Special Report is made available by Interactive Diagnostic
Dental Extraoral X-ray Systems
 Dental Extraoral X-ray Systems PROPOSED REVISIONS TO 4732.XXXX, 1.0 4732.#### DENTAL EXTRAORAL X-RAY SYSTEMS; STATIONARY AND MOBILE. Subpart 1. Applicability. A registrant s x-ray system used for dental
Dental Extraoral X-ray Systems PROPOSED REVISIONS TO 4732.XXXX, 1.0 4732.#### DENTAL EXTRAORAL X-RAY SYSTEMS; STATIONARY AND MOBILE. Subpart 1. Applicability. A registrant s x-ray system used for dental
Ionising Radiation Policy
 Document Author Written By: Radiation Protection Adviser Authorised Authorised By: Chief Executive Date: 24/08/2018 Date: 22 nd vember 2018 Lead Director: Consultant Radiologist Effective Date: 22 nd vember
Document Author Written By: Radiation Protection Adviser Authorised Authorised By: Chief Executive Date: 24/08/2018 Date: 22 nd vember 2018 Lead Director: Consultant Radiologist Effective Date: 22 nd vember
The Radiation Health and Safety Act, 1985
 1 The Radiation Health and Safety Act, 1985 Repealed by Chapter S-15.1 of the Statutes of Saskatchewan, 2013 (effective April 29, 2014) Formerly Chapter R-1.1 of the Statutes of Saskatchewan, 1984-85-86
1 The Radiation Health and Safety Act, 1985 Repealed by Chapter S-15.1 of the Statutes of Saskatchewan, 2013 (effective April 29, 2014) Formerly Chapter R-1.1 of the Statutes of Saskatchewan, 1984-85-86
DIRECT ACCESS - Guidance to BSDHT Members
 DIRECT CCESS - Guidance to BSDHT Members Direct ccess came into effect from 1 May 2013. But what does it mean for dental hygienists and dental therapists? The GDC have published guidance notes on the subject
DIRECT CCESS - Guidance to BSDHT Members Direct ccess came into effect from 1 May 2013. But what does it mean for dental hygienists and dental therapists? The GDC have published guidance notes on the subject
Managing Patient Dose in Computed Tomography (CT) INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION
 INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION") Managing Patient Dose in Computed Tomography (CT) International Commission on Radiological Protection Information abstracted from ICRP Publication 87 Available at www.icrp.org Task Group: M.M. Rehani,
Managing Patient Dose in Computed Tomography (CT) International Commission on Radiological Protection Information abstracted from ICRP Publication 87 Available at www.icrp.org Task Group: M.M. Rehani,
Facing the challenges: IAEA activities to protect the patients
 Facing the challenges: IAEA activities to protect the patients Debbie Gilley Radiation Protection of Patients Radiation Safety and Monitoring Section Division of Radiation, Transport and Waste Safety 18
Facing the challenges: IAEA activities to protect the patients Debbie Gilley Radiation Protection of Patients Radiation Safety and Monitoring Section Division of Radiation, Transport and Waste Safety 18
CERTIFICATE IN ORTHODONTIC NURSING
 NATIONAL EXAMINING BOARD FOR DENTAL NURSES CERTIFICATE IN ORTHODONTIC NURSING PROSPECTUS 108-110 LONDON STREET FLEETWOOD LANCASHIRE FY7 6EU TEL: 01253 778417 FAX: 01253 777268 NEBDN is a limited company
NATIONAL EXAMINING BOARD FOR DENTAL NURSES CERTIFICATE IN ORTHODONTIC NURSING PROSPECTUS 108-110 LONDON STREET FLEETWOOD LANCASHIRE FY7 6EU TEL: 01253 778417 FAX: 01253 777268 NEBDN is a limited company
RADIATION SAFETY DIRECTORATE
 RADIATION SAFETY DIRECTORATE Pursuant to Article 26-e, paragraph 1, item 7 of the Law on Ionising Radiation Protection and Radiation Safety (Official Gazette of the Republic of Macedonia No. 48/02 and
RADIATION SAFETY DIRECTORATE Pursuant to Article 26-e, paragraph 1, item 7 of the Law on Ionising Radiation Protection and Radiation Safety (Official Gazette of the Republic of Macedonia No. 48/02 and
DETERMINATION OF ENTRANCE SKIN DOSE FROM DIAGNOSTIC X-RAY OF HUMAN CHEST AT FEDERAL MEDICAL CENTRE KEFFI, NIGERIA
 DETERMINATION OF ENTRANCE SKIN DOSE FROM DIAGNOSTIC X-RAY OF HUMAN CHEST AT FEDERAL MEDICAL CENTRE KEFFI, NIGERIA Full Length Research Article 1 Ibrahim, U, 3 Daniel, I.H., 3 Ayaninola, O., 4 Ibrahim,
DETERMINATION OF ENTRANCE SKIN DOSE FROM DIAGNOSTIC X-RAY OF HUMAN CHEST AT FEDERAL MEDICAL CENTRE KEFFI, NIGERIA Full Length Research Article 1 Ibrahim, U, 3 Daniel, I.H., 3 Ayaninola, O., 4 Ibrahim,
Radiation Protection in Dental Intraoral Radiography Edition
 Radiation Protection In Intraoral Dental Radiography is one of a series of training CDs designed for staff that use or are exposed to radiation in their daily work. It would be useful to take the Basic
Radiation Protection In Intraoral Dental Radiography is one of a series of training CDs designed for staff that use or are exposed to radiation in their daily work. It would be useful to take the Basic
Dental Cone Beam CT. What is Dental Cone Beam CT?
 Scan for mobile link. Dental Cone Beam CT Dental cone beam computed tomography (CT) is a special type of x-ray equipment used when regular dental or facial x-rays are not sufficient. Your doctor may use
Scan for mobile link. Dental Cone Beam CT Dental cone beam computed tomography (CT) is a special type of x-ray equipment used when regular dental or facial x-rays are not sufficient. Your doctor may use
Scientific Affairs. Scientific Affairs
 The use of cone-beam computed tomography in dentistry : An advisory statement from the American Dental Association Council on Scientific Affairs The American Dental Association Council on Scientific Affairs
The use of cone-beam computed tomography in dentistry : An advisory statement from the American Dental Association Council on Scientific Affairs The American Dental Association Council on Scientific Affairs
Test Bank CHAPTER 1. Multiple Choice. 1. Who was awarded the first Nobel Prize for physics in 1901, for his experimental work with. radiation?
 Test Bank CHAPTER 1 Multiple Choice 1. Who was awarded the first Nobel Prize for physics in 1901, for his experimental work with radiation? a. W. J. Morton b. O. Walkhoff c. W. D. Coolidge d. W. C. Roentgen
Test Bank CHAPTER 1 Multiple Choice 1. Who was awarded the first Nobel Prize for physics in 1901, for his experimental work with radiation? a. W. J. Morton b. O. Walkhoff c. W. D. Coolidge d. W. C. Roentgen
Dosimetric Consideration in Diagnostic Radiology
 Dosimetric Consideration in Diagnostic Radiology Prof. Ng Kwan-Hoong Department of Biomedical Imaging University of Malaya ngkh@um.edu.my Radiation Dosimetry Workshop, 28-29 March 2014 2 Why do we measure
Dosimetric Consideration in Diagnostic Radiology Prof. Ng Kwan-Hoong Department of Biomedical Imaging University of Malaya ngkh@um.edu.my Radiation Dosimetry Workshop, 28-29 March 2014 2 Why do we measure
icat Precise Policy and Procedure Manual
 ORAL SURGERY GROUP P.A. PRACTICE LIMITED TO ORAL AND MAXILLOFACIAL SURGERY DENTAL IMPLANTS, WISDOM TEETH, ORAL PATHOLOGY, AND ORAL MEDICINE Dr. David M. Rauch Dr. Philip S. Engel Dr. Richard K. Stern Dr.
ORAL SURGERY GROUP P.A. PRACTICE LIMITED TO ORAL AND MAXILLOFACIAL SURGERY DENTAL IMPLANTS, WISDOM TEETH, ORAL PATHOLOGY, AND ORAL MEDICINE Dr. David M. Rauch Dr. Philip S. Engel Dr. Richard K. Stern Dr.
Periapical Radiography
 Periapical Radiography BARBARA E. DIXON B.D.S., M.Sc., D.P.D.S. Main Indications Detection of Apical infection/inflammation Assessment of the periodontal status After trauma Assessment of Unerupted teeth
Periapical Radiography BARBARA E. DIXON B.D.S., M.Sc., D.P.D.S. Main Indications Detection of Apical infection/inflammation Assessment of the periodontal status After trauma Assessment of Unerupted teeth
Dental ConeBeam Computed Tomography (CBCT) X-ray Systems
 X-ray Systems") Dental ConeBeam Computed Tomography (CBCT) X-ray Systems PROPOSED REVISIONS TO 4732.XXXX, 1.0 4732.#### DENTAL CONEBEAM COMPUTED TOMOGRAPHY (CBCT) X-RAY SYSTEMS; STATIONARY AND MOBILE. Subpart 1. Applicability.
Dental ConeBeam Computed Tomography (CBCT) X-ray Systems PROPOSED REVISIONS TO 4732.XXXX, 1.0 4732.#### DENTAL CONEBEAM COMPUTED TOMOGRAPHY (CBCT) X-RAY SYSTEMS; STATIONARY AND MOBILE. Subpart 1. Applicability.
Document Control Report
 Document Control Report Title Recording Clinical Evaluation and Dose - IR(ME)R 2000 Standard Operating Procedure Author Gill Kite Author s job title Senior Radiographer Directorate Sub-directorate Department
Document Control Report Title Recording Clinical Evaluation and Dose - IR(ME)R 2000 Standard Operating Procedure Author Gill Kite Author s job title Senior Radiographer Directorate Sub-directorate Department
Establishment of local diagnostic reference levels for quality control in intraoral radiography
 Oral Radiol (27) 33:38 44 DOI.7/s282-6-24-9 ORIGINAL ARTICLE Establishment of local diagnostic reference levels for quality control in intraoral radiography Maki Izawa Yasuo Harata Noriyoshi Shiba Nobuhide
Oral Radiol (27) 33:38 44 DOI.7/s282-6-24-9 ORIGINAL ARTICLE Establishment of local diagnostic reference levels for quality control in intraoral radiography Maki Izawa Yasuo Harata Noriyoshi Shiba Nobuhide
Radiation Dose in X-Ray and CT Exams
 Scan for mobile link. Patient Safety: Radiation Dose in X-Ray and CT Exams What are x-rays and what do they do? X-rays are forms of radiant energy, like light or radio waves. Unlike light, x-rays can penetrate
Scan for mobile link. Patient Safety: Radiation Dose in X-Ray and CT Exams What are x-rays and what do they do? X-rays are forms of radiant energy, like light or radio waves. Unlike light, x-rays can penetrate