Assessment of bone healing after Le Fort I osteotomy with 3-dimensional computed tomography
|
|
|
- Moris Stone
- 5 years ago
- Views:
Transcription
1 Assessment of bone healing after Le Fort I osteotomy with 3-dimensional computed tomography Koichiro UEKI, DDS PhD 1, Mao MIYAZAKI, DDS 1, Katsuhiko OKABE, DDS 1, Aya MUKOZAWA, DDS 1, Kohei MARUKAWA, DDS PhD 1, Akinori MOROI, DDS 1, Kiyomasa NAKAGAWA, DDS PhD 1, Etsuhide YAMAMOTO, DDS PhD 1 1 Department of Oral and Maxillofacial Surgery (Head: Prof. Dr. E. Yamamoto), Graduate School of Medicine, Kanazawa University, 13-1 Takaramachi, Kanazawa , Japan. Address correspondence and request for offprints to: Koichiro Ueki, DDS, PhD. Department of Oral and Maxillofacial Surgery, Graduate School of Medicine, Kanazawa University, 13-1 Takaramachi, Kanazawa , Japan. Tel: ; Fax: kueki@med.kanazawa-u.ac.jp Key words: Bone healing, Pterygoid plate, Le Fort I osteotomy, ultrasonic bone curette, 3-demensional computed tomography (3DCT)
2 Abstract Purpose. The purpose of this study was to examine bone healing after Le Fort I osteotomy in Class III patients. Patients and Methods. The study group consisted of 18 Japanese patients with mandibular prognathism with and without asymmetry, maxillary retrognathism or open bite. A total of 36 sides were examined. Le Fort I osteotomy was performed without a pterygoid osteotome, with an ultrasonic curette used to remove interference at the pterygomaxillary region. Titanium plates (Universal Mid-face fixation module, Stryker, Freiburg, German) were used for four patients, absorbable plates (poly-l-lactic acid (PLLA): NEOFIX, Gunze, kyoto, Japan) were used for four patients and other absorbable plates (uncalcined and unsintered hydroxyapatite and poly-l-lactic acid (uha/plla): super FIXSORB MX, Takiron Co. Ltd, Osaka, Japan) were used for ten patients, in the same manner. Postoperative computed tomography (CT) was analyzed for all patients pre-operatively and 1 year post-operative. The anterior and lateral areas between the maxillary segments were measured with 3-dimensional (3D) CT. Bone healing at the pterygomaxillary region was also assessed. Results. There were no significant differences in the area of bone defect healing among the plate types. The areas of bone defect after 1 year were significantly smaller than that immediately after surgery on the right side (p=0.0145) and left side (p=0.0010) in the frontal view and right side in the lateral view (p=0.0118). Bone healing at the pterygo-maxillary junction was found in all cases without artificial pterygoid plate fracture. 14 of 22 sides with artificial pterygoid plate fracture by an ultrasonic curette showed bone continuity between the pterygoid plate and posterior part of maxilla. Conclusion. This study suggested that bony healing could occur in spaces between the segments of maxilla and pterygomaxillary regions as well as the region of the anterior and lateral walls in the maxilla, but it is not always complete within 1 year after Le Fort I osteotomy.
3 Introduction Le Fort I osteotomy is one of the standard procedures for the management of dentofacial deformities (Bell et al., 1980; Bell et al., 1988). Factors that have been implicated for instability after Le Fort I osteotomies include presurgical orthodontics, inadequate mobilization, inappropriate or lack of grafting, increased masticatory forces, inadequate methods of fixation, type and amount of movement, soft tissue tension, and presence of cleft. Various fixation techniques have been used for maxillary stabilization including trans-osseous and suspension wires, intraoral skeletal fixation appliances, and bone plating (Ueki et al., 2007; Marşan et al., 2009; Mavili et al., 2009; Kretschmer et al.,2010). Post-operatively, the maxilla appears to be healed and in a stable position on clinical assessment. With regard to animal studies, Bell et al. have reported primate studies that provide biologic insight into the bone healing and revascularization processes that accompany maxillary osteotomies (Bell, 1969; Bell & Levy, 1971; Bell et al., 1975). These studies have indicated that osseous union of osteotomized sites occurs as early as six weeks postoperative. However, there have been few histologic studies on human tissue to verify the type of repair that is initiated. A previous study by Compton et al. (1984) indicated that the area between the segments healed with mature compact bone, from the evaluation of punch biopsy at the osteotomy site of five patients after Le Fort I osteotomy. However, the period of biopsy was not constant, ranged from 17 to 30 months, and there was no detailed description of the site that was taken for biopsy. It was unclear whether all sites on the osteotomy line could induce new bone. Although the evaluation of bone healing after Le Fort I osteotomy is needed to determine the site and method of the fixation plate, there is no report on bone healing using 3-dimensional computed tomography (3DCT) after Le Fort I osteotomy. The purpose of this study was to examine bone healing of the anterior and lateral walls of the maxilla and pterygomaxillary junction regions, after Le Fort I osteotomy in Class III patients, using 3DCT.
4 Patients and Methods Patients The 18 Japanese adults (men:5, women: 13) in this study presented with jaw deformities and diagnosed as mandibular prognathism with/without bi-maxillary asymmetry, maxillary retrognathism or open bite. At the time of the orthognathic surgery, the patients ranged in age from 16 to 42 years, with a mean age of 24.1 years (standard deviation, 7.3 years). Informed consent was obtained from the patients and the study was approved by Kanazawa University Hospital. Fourteen patients underwent Le Fort I osteotomy with bilateral sagittal split ramus osteotomy (SSRO), three patients underwent Le Fort I osteotomy with intraoral vertical ramus osteotomy (IVRO) and one patient underwent Le Fort I osteotomy with SSRO for right side and IVRO for left side (Table 1.). Surgical procedure All patients underwent a standard Le Fort I osteotomy following a periodontal incision at the anterior teeth and a vestibular incision at the posterior teeth to prevent any postoperative scar at the labial gingival tissue, with inter-maxillary fixation screws (Stryker LEIBINGER, Freiburg, Germany or Jeil Medical, Seoul, Korea) implanted in the bimaxillary anterior alveolar bone. The lateral wall of the maxillary sinus was cut using a reciprocating saw, and the nasal septum and lateral nasal walls were sectioned with a chisel. Pterygomaxillary separation was performed without an osteotome. A bone separator was fixed in a thick bony area of the lateral wall of the maxillary sinus, attached with screws implanted in the maxilla, and wired to fracture and pull down the maxillary segment. This method could facilitate the down fracture rather than the conventional method. Furthermore, pulling down the wires made it easier to see and operate in the pterygomaxillary region. The posterior wall of the maxillary sinus, the maxillary tuberosity, and the pterygoid process were then exposed. The maxillary segment was pulled down and forward and small
5 bone pieces were removed along with surplus sinus membranes, allowing the descending palatine artery to be seen from the pterygopalatine fossa to the nasal wall. The Sonopet UST-2001 ultrasonic bone curette (Miwatec Co., Ltd., Kawasaki, Kanagawa, Japan) was used to remove interference between the pterygoid process and the posterior part of the maxilla without damaging the descending palatine artery or other vessels and nerves. Artificial fracture of pterygoid plate could facilitate movement of the maxilla (Ueki et al., 2004; Ueki et al., 2009). The maxillary segment was then repositioned with an intermediate occlusal splint and fixed with mini-plates and mono-cortical screws. Two L-type titanium plates at the site of the piriform rim, two straight titanium plates at the site of the zygomatic buttress and screws (Universal Mid-face fixation module, Stryker, Freiburg, German) were used for four patients, Two L-type absorbable plates at the site of the piriform rim, two straight titanium plates at the site of zygomatic buttress and screws (poly-l-lactic acid (PLLA): NEOFIX, Gunze, kyoto, Japan) were used for four patients and other absorbable plates and screws (uncalcined and unsintered hydroxyapatite and poly-l-lactic acid (uha/plla): super FIXSORB MX, Takiron Co. Ltd, Osaka, Japan) were used for ten patients, in the same manner (Table.1). Post-operative inter-maxillary fixation was not performed, but traction by elastic was performed in all cases. CT assessment The patients were placed in the gantry with the tragacanthal line perpendicular to the ground for CT scanning. They were instructed to breathe normally and to avoid swallowing during the scanning process. CT scans were obtained in the radiology department by skilled radiology technicians using a high-speed, advantage-type CT generator (Light Speed Plus; GE Healthcare, Milwaukee, WI, USA) with each sequence taken 1.25 mm apart for the 3D reconstruction (120 kv, average 150 ma, 0.7 sec/rotation, helical pitch 0.75). The 3-D image was reconstructed by 3D visualization and measurement software Med View version 5.5 (LEXI Co, Tokyo, Japan). The threshold of the CT value (Hounsfield units: HU) of the measurable maxillary bone was standardized as over 1200 for
6 both of pre- and postoperative images of all patients. 1 year follow up CT scan was taken for all patients who underwent orthognathic surgery and informed consent was obtained. Measurements using CT The frontal and lateral ( right and left) views perpendicular to the FH (Frankfurt) plane were reconstructed to measure the bone defect area between the superior and inferior segments of the maxilla after Le Fort I osteotomy on the right and left sides. A total of 36 sides (18 right and 18 left sides) were measured. The defective area was measured in the frontal and lateral views (as 2 dimensional images) made from the 3DCT images using the image software(scion image, Scion corporation ML, USA)and Med View version 5.5 (LEXI Co, Tokyo, Japan). The same horizontal plane images parallel to the FH plane at immediately and 1 year post-surgery including the region where the pterygoid plate was fractured or the anterior aspect of pterygoid plate removed were used to evaluate bone healing at the pterygomaxillary junction region. Evaluation of bone formation between the posterior part of the maxilla and pterygoid plate was set at window width of 2000 and window level of 200. Completion of bone healing at the pterygomaxillary region was judged as bone continuity between the pterygoid plate and the posterior part of the maxillary segments. All CT images were measured by an author. Fifteen patients were selected randomly and CT images were measured again 10 days later (paired t-test; p>.05). All CT images were measured by an author (K.U.). Fifteen patients were selected for calculations using the Dahlberg s formula (Dahlberg, 1940): ME= d 2 /2n where d is the difference between 2 registrations of a pair, and n is the number of double registrations. The random errors did not exceed 0.21 mm for the linear measurements, and 2.0 mm 2 for the square measurements. Statistical analysis
7 Data were compared between the right and left by paired t-test using the Stat View version 4.5 software program (Abacus Concepts, Inc., Berkeley, CA, USA). Differences were considered significant at p<0.05. Results No fracture was noted in the upper third of the pterygoid plates, and there was no fracture of the cranial base. Eleven patients (22 sides) underwent an artificial pterygoid fracture or bone removal in the pterygomaxillary region. Intended maxillary movement by simulation surgery could be achieved in all cases by using fore-mentioned ultrasonic bone curette. Therefore, there was no difference between intended maxillary movement and actual post-operative maxillary movement. Blood loss was small and no patient required transfusion. The titanium plate and uha/plla plate were visible, but the PLLA plate was invisible on the 3DCT image. At 1 year postoperative, the shape of the uha/plla plate did not change in all cases. Therefore, the overlapped area between the bone defect and the plate was not included in the measurement of the area in the cases where the titanium plate and uha/plla plate (Fig.1) were used. The subjects were divided into three groups (titanium, PLLA, and uha/plla), although the sample number was small. The difference in the area of the defects between immediately after surgery and 1 year after surgery was calculated, and multiple comparisons were performed statistically. However, there were no significant differences in the area of bone defect healing among the plate types. The results of the statistic analysis without group division showed that the areas of bone defect after 1 year were significantly smaller than that immediately after surgery on the right side (p=0.0145) and left side in the frontal view (p=0.0010) and right side in the lateral view (p=0.0118) (Fig. 2). After 1 year, complete bone continuity between segments could be recognized in 3/18 sides on the right and 5/18 sides on the left in the frontal view, and 4/18 sides on the right and 2 /18 sides on the left in the lateral view (Fig. 3). However,
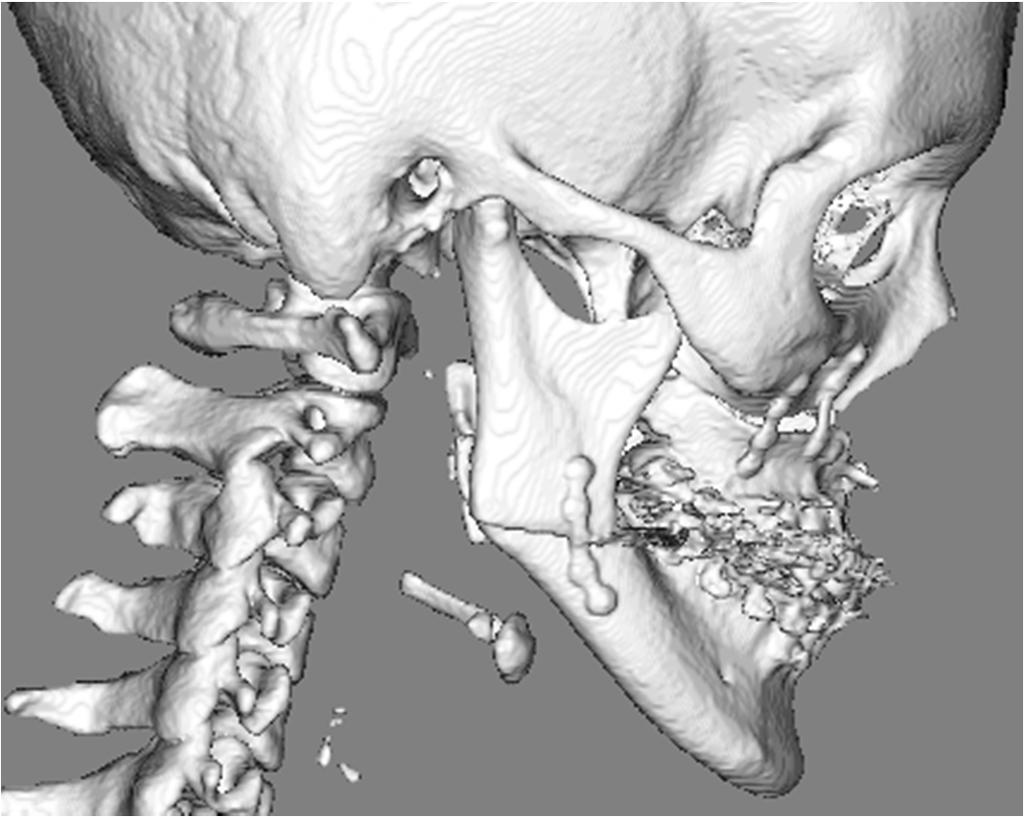
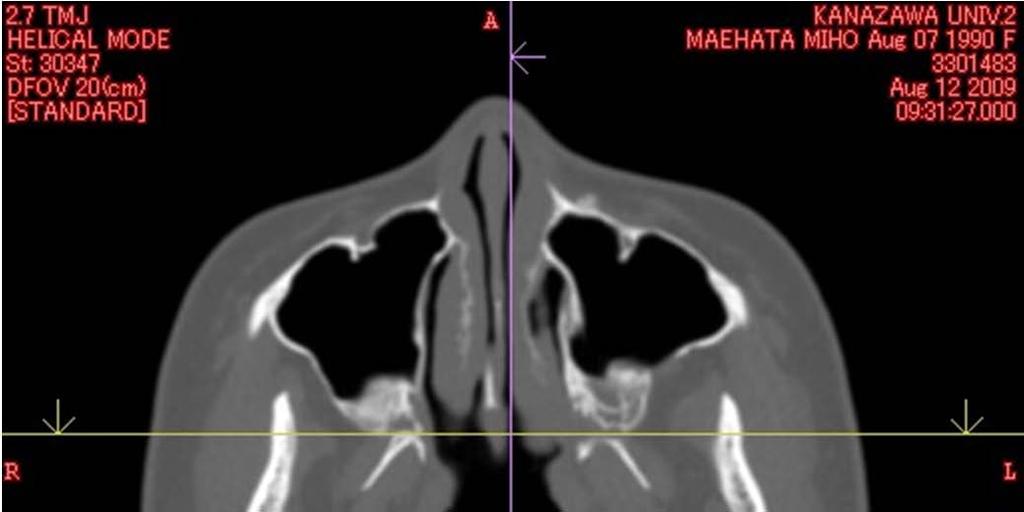
8 the area of bone defect after 1 year increased in 6 /18 sides on the right and 3/18 sides on the left in the frontal view, and 2/18 sides on the right and 6 /18 sides on the left in the lateral view (Fig. 4). Bone healing at the pterygo-maxillary junction was found in all cases without artificial pterygoid plate fracture. In 14 of 22 sides (63.6%) with artificial pterygoid plate fracture, there was bone healing between the pterygoid plate and posterior part of the maxilla (Fig. 5). However, 8 of 22 sides (35.4%) with artificial pterygoid plate fracture did not show bone continuity between the pterygoid plate and posterior part of the maxilla (Fig.6). Discussion In Le Fort I osteotomy, incomplete ossification of osteosynthesis is one of the major problems (Proffit et al., 2003). If the size of the defect between the advanced inferior maxillary segment and the superior segment exceeded 3mm at the levels of the piriform rim and zygomaticomaxillary junction following Le Fort I osteotomy, use of a bone graft can become necessary for stabilization. Furthermore, bone recovery would be inadequate if there is a defect of more than 3 mm between the segments along the line of osteosynthesis. The line of osteosynthesis would involve a fibrous tissue rather than osseous tissue. In this instance, resistance to relapse would be via this fibrous tissue and the initial plate and screw rather than a robust osseous tissue (Holmes et al., 1988; Proffit et al., 2003). However, there has been no well-controlled study in which the maxilla is advanced to a large distance with and without bone grafting. In orthognathic surgery, bone fragments are usually fixed with the use of metallic plates and screws. Recently, the use of resorbable materials to stabilize the maxillofacial skeleton has been reported (Ueki et al., 2005, Ueki et al., 2006). In this study, there was no significant difference between the titanium plate, PLLA plate and uha/plla plate. It has been proven that the uha/plla plate produced osteoconductivity in vitro (Shikinami et al., 2005). However, in this study, the finding was that new bone formation surrounding
9 the uha/plla plate was not found in the 3DCT image at1 year postsurgery. Currently, several studies have reported the interpretation of the 3DCT and multiplanar reconstructed images by CT as supplying more information than axial (2D) images, providing more reliable diagnosis, effective therapeutics, evaluation of treatment, and consequently reducing the manifestation of sequelae (Albrecht & Blomley, 1998; Cavalcanti et al., 1999; Chacon et al., 2003, Ueki et al., 2009b). When the 3DCT reconstruction was performed and evaluated, the threshold of the CT value was very important to judge whether it was matured bone or soft tissue. Lettry et al. (2003) reported that the CT values of mandibular cortical bones in 10 cadavers ranged from 976 HU to 1478 HU, with a mean of HU (SD 112.1). However, there is no report regarding the anterior and lateral walls of the maxillary bone that will allow CT values be determined as over 1200 HU. Although immature bone tissue might not be detected in this study, this determination of CT value was considered acceptable, because the detection of just hard bone tissue to keep the skeletal strength and stability was necessary for this study. The areas of bone defect after 1 year were significantly smaller than that immediately after surgery in the right and left anterior wall and right lateral wall of the maxilla. However, the area of bone defect increases in some cases. The patient who underwent 5 mm maxillary advancement had the largest bone gap between the segments in this study, but complete bone healing at the anterior and lateral walls could occur after 1 year. On the other hand, although bone contact between segments could be established in the maxillary impaction cases intra-operatively, there were cases where complete bone healing could not be achieved after 1 year. This suggested that thin bone at the edge along the osteotomy line could be resorbed after 1 year postsurgery. In our previous report, there was no difference in the stability following Le Fort I osteotomy without bone graft between a titanium plate group and an absorbable plate group in most frontal and lateral cephalometric measurements. However, a significant difference in the A point in the lateral cephalometric measurements was found between the two groups (Ueki et al., 2006). This suggested that the difference between titanium and the absorbable plate could affect the stability following Le Fort I osteotomy. On the other hand, in the
10 animal study of Calhoun et al., the healing findings provided only a qualitative evaluation of differences in the stages of healing (Calhoum et al., 1989). The finding of better healing with semi-rigid fixation than with rigid fixation suggested that a small amount of movement between bone segments might stimulate healing. Actually, the absorbable plate is weaker than the titanium plate. However, it was proved that PLLA and uha/plla plates were stronger rather than the surrounding cortical bone (Shikinami et al., 2005; Marumo et al., 2006). Furthermore, this study showed that there were no significant differences in the area of bone defect among the plate types. It was considered that various factors such as preoperative bone thickness, occlusion, inter-maxillary traction, moving direction and amount, age and gender etc. were associated with the healing at the anterior and lateral wall of maxilla. The change in the stress distribution at the region of the space between segments might also affect the change in the bone area. At least, use of bone graft or an alternative material may not be decided on the basis of only the amount of bony gap by movement of the maxillary segment. In the previous study with CT after Le Fort I osteotomy, exact separation of the pterygomaxillary junction at the posterior nasal spine level was found in only 18 of 74 sides (24%). In 29 of 74 sides (39.2%), separation occurred anteriorly to the descending palatine artery. In 29 of 74 sides (39.2%), complete separation between the maxillary tuberosity and the lateral and/or medial pterygoid plate did not occur at the pterygomaxillary junction at the posterior nasal spine level. However, exact separation occurred more frequently at the lower level, with no complications (Ueki et al., 2009a). It remains unclear whether bone healing could occur at the region of the pterygo-maxillary junction after artificial pterygoid fracture of the anterior part of the pterygoid plate. Bone healing at the pterygo-maxillary junction was found in all cases without artificial pterygoid plate fracture. This result might be due to the fact that the amount of the maxillary advancement or impaction was comparatively small in this study. Furthermore, in 14 of 22 sides (63.6%) with artificial pterygoid plate fracture, there was bone healing between the pterygoid plate and posterior part of maxilla. However, 8 of 22 sides (35.4%) with artificial pterygoid plate fracture did not show bone continuity. We did
11 not use an osteotome to separate the pterygomaxillary junction, suggesting a green stick fracture occurred in most cases when the maxillary segment was fractured down in the previous study. Pterygomaxillary dysjunction was found in only 24% of cases, so the pterygomaxillary junction might not always be adequate to separate the segments at the posterior nasal spine level. Thus, the separation pattern at the pterygomaxillary junction varied greatly indicating that the pattern of bone healing could vary. Removal volume of the pterygoid plate or posterior part of the maxilla and the distance between the pterygoid plate and maxillary segment might be related to healing at this region after 1year. If the mechanical stress stimulation at the pterygomaxillary region increases according to recovery of the occlusal force after more than 1 year, bone healing volume may increase there. Conclusion This study suggested that bony healing could occur in the space between the segments of the maxilla and pterygomaxillary regions as well as at the region of anterior and lateral wall in maxilla, but it is not always complete within 1 year after Le Fort I osteotomy. However, further examination using a large sample number will be necessary.
12 References Albrecht T, Blomley MJK: Spiral computed tomography: principles and clinical use. Hosp Med 59: 121-5, Bell WH: Revascularization and bone healing after posterior maxillary osteotomy. J Oral Surg 27:249-55, Bell WH, Levy BM: Revascularization and bone healing after posterior maxillary osteotomy. J Oral Surg 29: , Bell WH, Fonseca RJ, Kennedy JW, Levy BM: Bone healing and revascularization after total maxillary osteotomy. J Oral Surg 33: , Bell W, Proffit W, White R: Surgical Correction of Dentofacial Deformities, vols 1 and 2. Philadelphia, Saunders, Bell WH, Mannai C, Luhr HG: Art and science of the Le Fort I downfracture. Int J Adult Orthod Orthognath Surg 3: 23-52, Calhoum NR, Tsaknis PJ, Hughes D, Ajagbe O: Osseous repair with Le Fort I osteotomy. Oral Surg Oral Med Oral Pathol 67: , Cavalcanti MGP, Haller JW, Vannier MW: Three-dimensional computed tomography landmark measurement in craniofacial surgery planning: experimental validation in vitro. J Oral Maxillofac Surg 57: 690-4, Chacon G, Dawson KH, Myall RWT, Beirne RO: A comparative study of 2 imaging techniques for the diagnosis of condylar fractures in children. J Oral Maxillofac Surg 61: , Compton JE, Jacobs JD, Dunsworth AR: Healing of the bone incision following Le Fort I osteotomy. J Oral Maxillofac Surg 42: , Dahlberg G: Statistical methods for medical and biological students. George Allen and Unwin, London, pp Holmes RE, Wardrop RW, Wolford LM: Hydroxyapatite as a bone graft substitute in orthognathic surgery: histologic and histometric findings. J Oral Maxillofac Surg 46: , 1988.
13 Kretschmer WB, Baciut G, Baciut M, Zoder W, Wangerin K: Stability of Le Fort I osteotomy in bimaxillary osteotomies: single-piece versus 3-piece maxilla. J Oral Maxillofac Surg 68: , Lettry S, Seedhom BB, Berry E, Cuppone M: Quality assessment of the cortical bone of the human mandible. Bone 32: 35-44, Luyk NH, Ward-Booth RP: The stability of Le Fort I advancement osteotomies using bone plates without bone grafts. J Maxillofac Surg 13: 250-3, Marumo K, Sato Y, Suzuki H, Kurosawa D: MRI study of bioabsorbable poly-l-lactic acid devices used for fixation of fracture and osteotomies. J Orthop Sci. 11: , Marşan G, Cura N, Emekli U: Soft and hard tissue changes after bimaxillary surgery in Turkish female Class III patients. J Craniomaxillofac Surg 37: 8-17, Mavili ME, Canter HI, Saglam-Aydinatay B: Semirigid fixation of mandible and maxilla in orthognathic surgery: stability and advantages. Ann Plast Surg 63: , Proffit WR, White RP, Sarver DM: Contemporary treatment of dentofacial deformity. 1 st ed. St Louis: Mosby; 298-9, Shikinami Y, Matsusue Nakamura T: The complete process of bioresorption and bone replacement using devices made of forged composite of raw hydroxyapatite particles/poly L-lactide (F-u-HA/PLLA). Biomaterials 26: , Ueki K, Nakagawa K, Marukawa K, Yamamoto E. Le Fort I osteotomy using an ultrasonic bone curette to fracture the pterygoid plates. J Craniomaxillofac Surg 32: 381-6, Ueki K, Nakagawa K, Marukawa K, Takazakura D, Shimada M, Takatsuka S, Yamamoto E: Changes in condylar long axis and skeletal stability after bilateral sagittal split ramus osteotomy with poly-l-lactic acid or titanium plate fixation. Int J Oral Maxillofac Surg. 34: , Ueki K, Marukawa K, Shimada M, Nakagawa K, Aalm S, Yamamoto E: Maxillary stability following Le Fort I osteotomy in combination with sagittal split ramus osteotomy and intraoral vertical ramus osteotomy: a comparative study between titanium miniplate and poly-l-lactic acid plate. J Oral Maxillofac Surg. 64: 74-80, 2006.
14 Ueki K, Hashiba Y, Marukawa K, Yoshida K, Shimizu C, Nakagawa K, Yamamoto E: Comparison of maxillary stability after Le Fort I osteotomy for occlusal cant correction surgery and maxillary advanced surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 104: 38-43, Ueki K, Hashiba Y, Marukawa K, Okabe K, Alam S, Nakagawa K, Yamamoto E: Assessment of pterygomaxillary separation in Le Fort I osteotomy in Class III patients. J Oral Maxilofac Surg 67: 833-9, 2009a. Ueki K, Hashiba Y, Marukawa K, Nakagawa K, Okabe K, Yamamoto E: Determining the anatomy of the descending palatine artery and pterygoid plates with computed tomography in Class III patients. J CranioMaxillofac Surg 37: , 2009b.
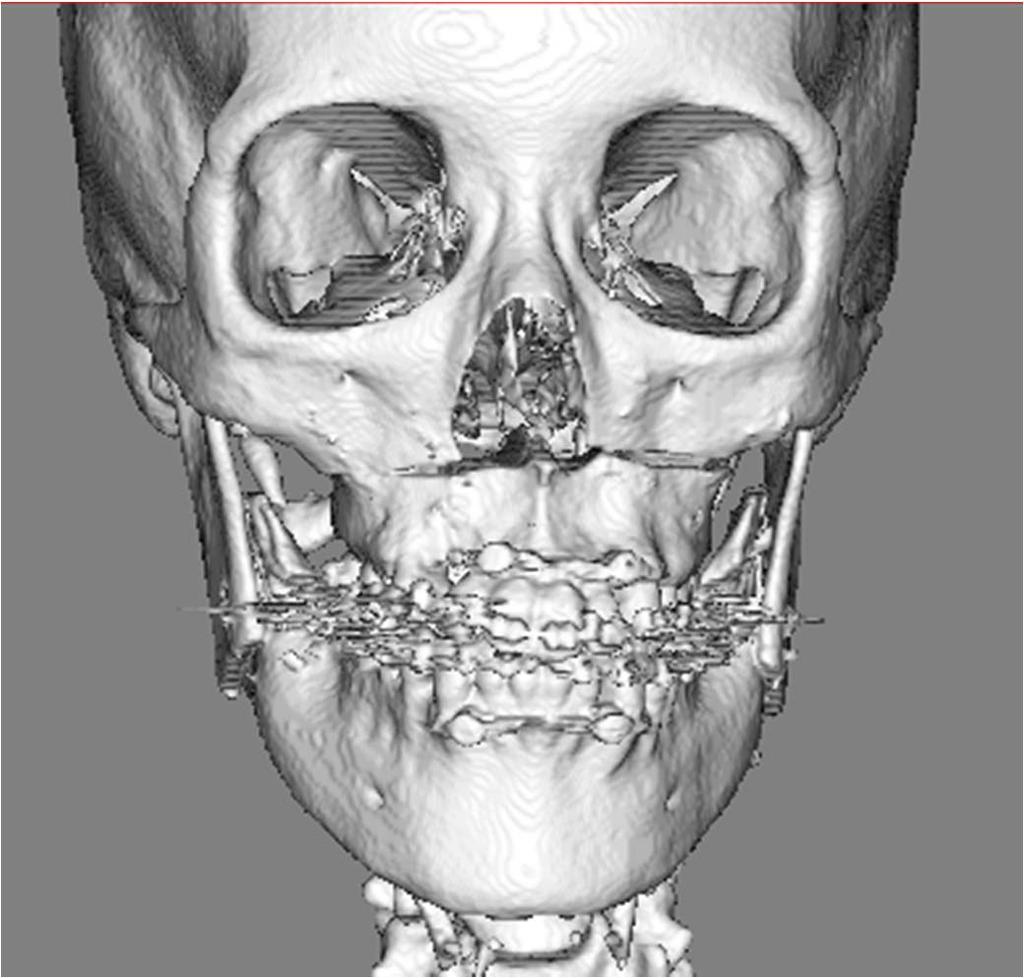
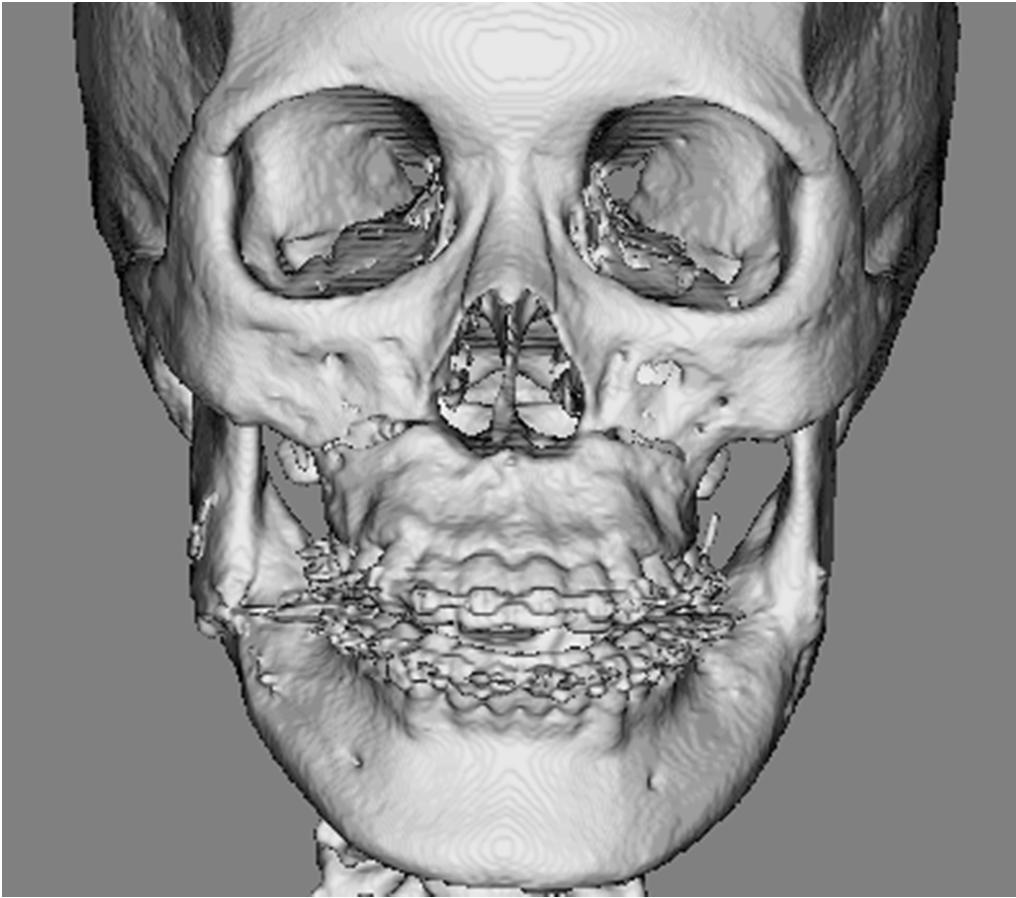
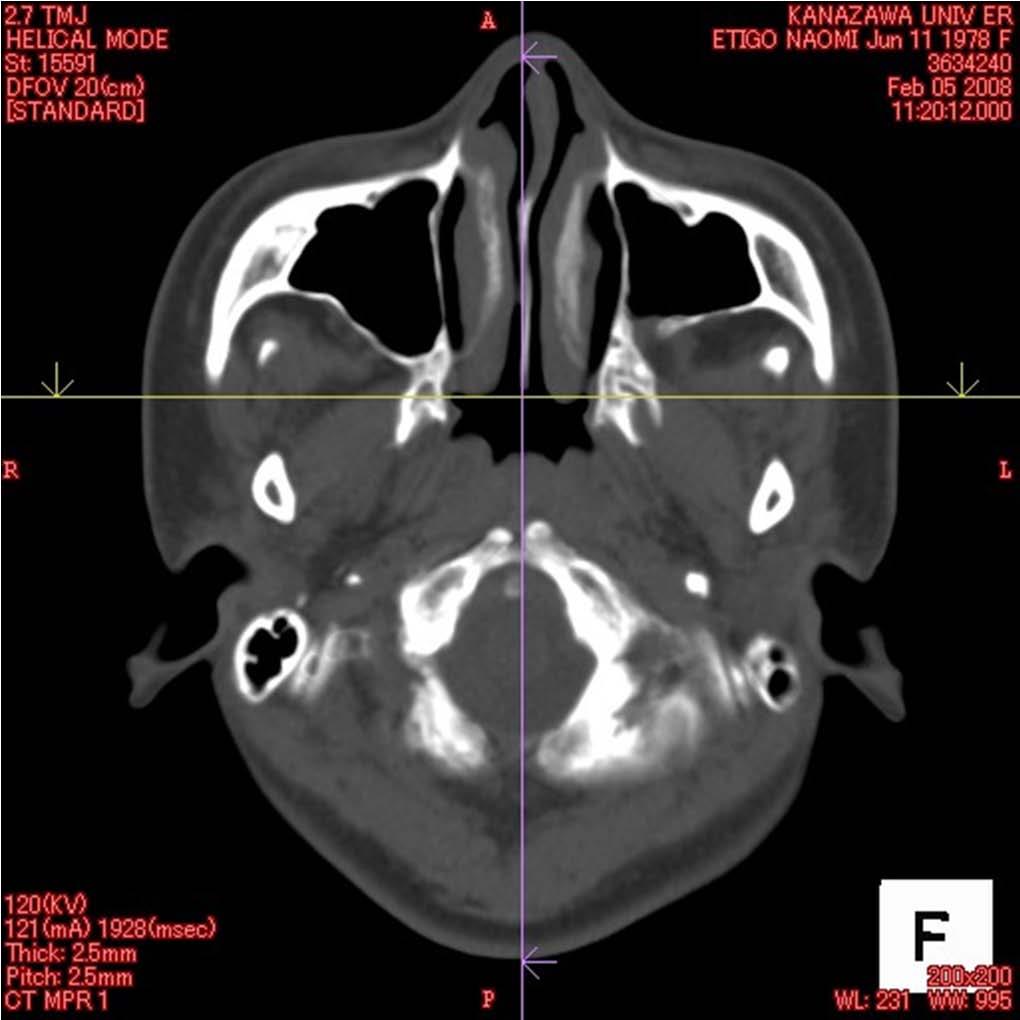
15 Legends Fig.1 Measurements of the area of bone defects on 3DCT image. A: frontal view, B: lateral view. Red area shows bone defect. A uha/plla plate was used in this case, so that the plate was visible. Fig. 2 The area of defects between segments. Error bars show the standard deviation. * indicates a significant difference at P<0.05. Fig. 3 Frontal view of the case where a PLLA plate was used. A: immediately after surgery. The bone defect was recognized. B: 1 year after surgery. The bone healing completed. The PLLA plate was not visible on the 3DCT. Fig. 4 Frontal view of the case where a PLLA plate was used. A: immediately after surgery. The bone defect was recognized. B: 1 year after surgery. Although bone continuity between segments at the lateral wall region was found, the bone defect increased at the frontal wall of the maxilla. The PLLA plate was not visible on the 3DCT. Fig. 5 Horizontal plane of CT at the pterygomaxillary junction. A: immediately after surgery. The anterior part of pterygoid plate was removed and pterygoid fracture was performed. Red arrows show the space between the maxillary segments and pterygoid plate. B: 1 year after surgery. Bone healing with continuity between the maxillary segments and pterygoid plate completed. Fig. 6 Horizontal plane of CT at the pterygomaxillary junction. A: immediately after surgery. The anterior part of the pterygoid plate was removed and pterygoid fracture was performed. Fracture of the posterior wall of the maxilla could be observed. Red arrows showed the space between the maxillary segments and pterygoid plate. B: 1 year after
16 surgery. The area of bone healing increased and fracture of the posterior wall of the maxilla healed, but bone continuity between the maxillary segments and pterygoid plate did complete. Table. 1. Table I. Patient data. SSRO: sagittal split ramus osteotomy, IVRO: intraoral vertical ramus osteotomy, L1:Le Fort I osteotomy, PLLA: poly-l-lactic acid (absorbable) plate. uha/plla: uncalcined and unsintered hydroxyapatite and poly-l-lactic acid (absorbable) plate
17 Case number Diagnosis Age Sex Procedures Setback right Setback left Plate Osteotomy in Maxillary movement (yrs) (mm) (mm) pterygoid process 1 bi-maxillary asymmetry, mandibular prognathia 20 F L1,IVRO 3 0 titanium bilateral 2 mm side shift to the right, right 4 mm up 2 mandibular prognathia, open bite 28 F L1,SSRO 8 8 PLLA bilateral whole 8 mm up 3 mandibular prognathia 21 M L1,SSRO PLLA bilateral 4 mm up at the postrior teeth 4 mandibular prognathia, maxillary retrognathism 18 F L1,SSRO 8 9 titanium n 5 mm advance 5 bi-maxillary asymmetry, mandibular prognathia 34 F L1,SSRO 9 2 titanium bilateral right 3 mm up and left 3 mm down 6 bi-maxillary asymmetry, mandibular prognathia 42 F L1,SSRO 6 5 uha/plla n right 3 mm down and left 3 mm up 7 bi-maxillary asymmetry, mandibular prognathia 17 F L1,SSRO 6 5 uha/plla bilateral 2 mm advance, right 3 mm down and left 3 mm up 8 mandibular prognathia, maxillary retrognathism 16 F L1,SSRO 8 8 uha/plla n 4 mm advance 9 bi-maxillary asymmetry, mandibular prognathia 24 M L1,SSRO,IVRO 4 3 titanium bilateral right 8 mm up and left 5 mm up 10 mandibular prognathia, maxillary retrognathism 16 F L1,SSRO 6 6 uha/plla n 4 mm advance, right 3 mm up and left 4 mm up 11 mandibular prognathia, open bite 23 F L1,SSRO 4 2 uha/plla bilateral whole 8 mm up 12 bi-maxillary asymmetry, mandibular prognathia,open bite 21 M L1,SSRO 3 3 uha/plla bilateral 2 mm advanve, right 3 mm up and left 5 mm up at the posterior teeth 13 mandibular prognathia, maxillary retrognathism 20 M L1,SSRO 8 6 uha/plla n 2 mm advance and 4 pieces segmental osteotomy 14 bi-maxillary asymmetry, mandibular prognathia 28 F L1,SSRO 8 7 uha/plla n right 8 mm up and left 3 mm up 15 bi-maxillary asymmetry, mandibular prognathia 37 F L1,IVRO 1 1 PLLA n whole 4 mm up 16 bi-maxillary asymmetry, mandibular prognathia 26 M L1,IVRO 4 1 uha/plla bilateral right 4 mm up 17 bi-maxillary asymmetry, mandibular prognathia 24 F L1,SSRO 1 1 uha/plla bilateral 3 mm down at the anterior teeth and 8 mm up at the posterior teeth 18 mandibular prognathia 19 F L1,SSRO 5 5 PLLA bilateral left 4 mm up average sd Table. 1

18 A B Fig. 1
19 (mm 2 ) 60 * * * Right frontal Right frontal Left frotal Left frotal Right lateral Right lateral Left lateral Left lateral 1week 1 year 1week 1 year 1week 1 year 1week 1 year (Site) (Period) Fig. 2

20 A B Fig. 3

21 A B Fig. 4

22 A B Fig. 5

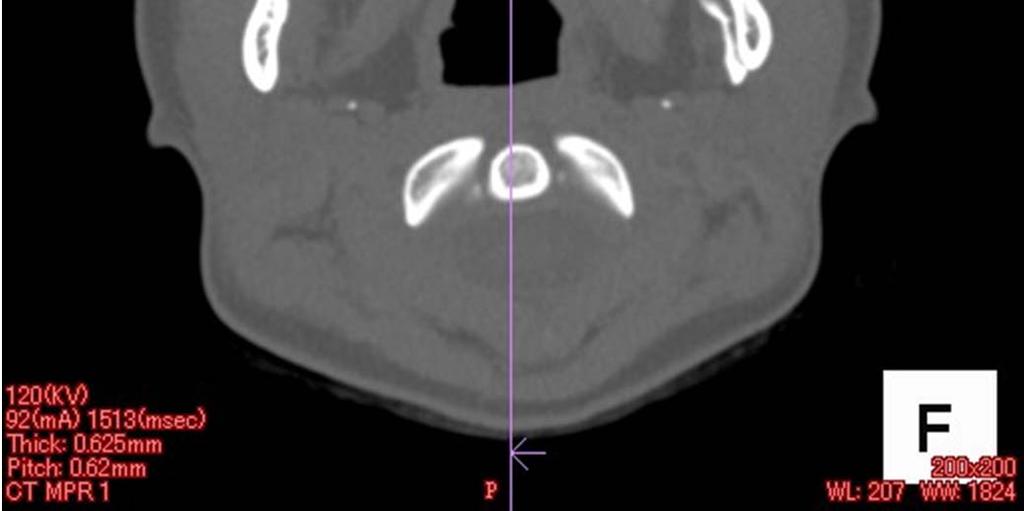
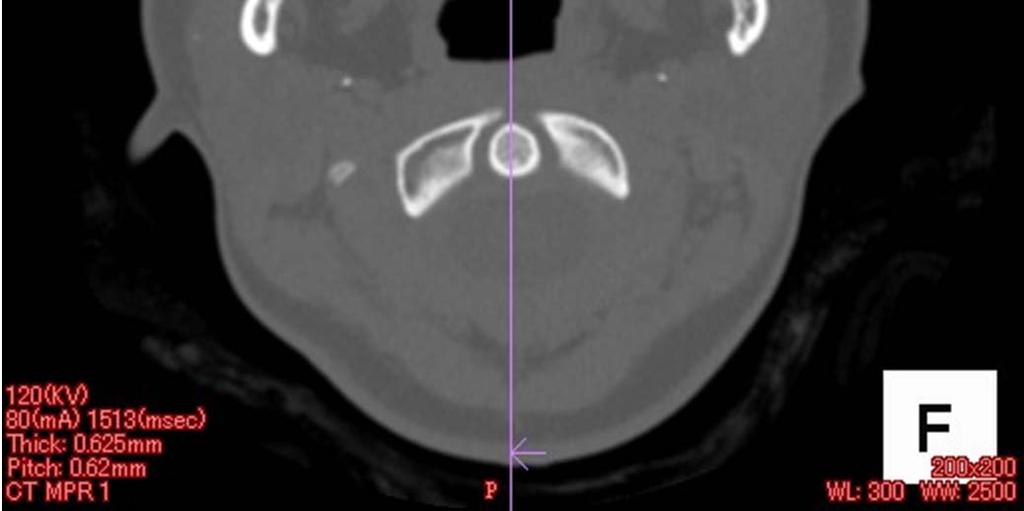
23 A B Fig. 6
Post-operative stability of the maxilla treated with Le Fort I and horseshoe osteotomies in bimaxillary surgery
 European Journal of Orthodontics 24 (2002) 471 476 2002 European Orthodontic Society Post-operative stability of the maxilla treated with Le Fort I and horseshoe osteotomies in bimaxillary surgery Kiyoshi
European Journal of Orthodontics 24 (2002) 471 476 2002 European Orthodontic Society Post-operative stability of the maxilla treated with Le Fort I and horseshoe osteotomies in bimaxillary surgery Kiyoshi
Unilateral intraoral vertical ramus osteotomy based on preoperative three-dimensional simulation surgery in a patient with facial asymmetry
 CASE REPORT http://dx.doi.org/10.5125/jkaoms.2014.40.1.32 pissn 2234-7550 eissn 2234-5930 Unilateral intraoral vertical ramus osteotomy based on preoperative three-dimensional simulation surgery in a patient
CASE REPORT http://dx.doi.org/10.5125/jkaoms.2014.40.1.32 pissn 2234-7550 eissn 2234-5930 Unilateral intraoral vertical ramus osteotomy based on preoperative three-dimensional simulation surgery in a patient
Assessment of Relapse Following Intraoral Vertical Ramus Osteotomy Mandibular Setback and Short-term Immobilization
 Assessment of Relapse Following Intraoral Vertical Ramus Osteotomy Mandibular Setback and Short-term Immobilization Koroush Taheri Talesh, DDS, a Mohammad Hosein Kalantar Motamedi, DDS, b Mahdi Sazavar,
Assessment of Relapse Following Intraoral Vertical Ramus Osteotomy Mandibular Setback and Short-term Immobilization Koroush Taheri Talesh, DDS, a Mohammad Hosein Kalantar Motamedi, DDS, b Mahdi Sazavar,
The Skeletal Stability of Maxillary Advancement in Combination with Bilateral Sagittal Split Ramus Osteotomy. Mohamed Diaa Z.
 The Skeletal Stability of Maxillary Advancement in Combination with Bilateral Sagittal Split Ramus Osteotomy Mohamed Diaa Z. Ismail Associate Professor of Oral and Maxillofacial Surgery, Faculty of Dentistry,
The Skeletal Stability of Maxillary Advancement in Combination with Bilateral Sagittal Split Ramus Osteotomy Mohamed Diaa Z. Ismail Associate Professor of Oral and Maxillofacial Surgery, Faculty of Dentistry,
Author(s) Fujimura, Kazuma; Bessho, Kazuhisa.
 Fujimura, Kazuma; Bessho, Kazuhisa.") Title Rigid fixation of intraoral mandibular prognathism. vertico Author(s) Fujimura, Kazuma; Bessho, Kazuhisa Citation Journal of oral and maxillofacial s 1173 Issue Date 2012-05 URL http://hdl.handle.net/2433/155855
Title Rigid fixation of intraoral mandibular prognathism. vertico Author(s) Fujimura, Kazuma; Bessho, Kazuhisa Citation Journal of oral and maxillofacial s 1173 Issue Date 2012-05 URL http://hdl.handle.net/2433/155855
Case Report. Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System and MatrixORTHOGNATHIC Plating System.
 Case Report Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System and MatrixORTHOGNATHIC Plating System. Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System
Case Report Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System and MatrixORTHOGNATHIC Plating System. Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System
Postoperative Evaluation on SSRO performed by Short Lingual Osteotomy and IVRO
 140 J Meikai Dent Med 43 2, 140 147, 2014 Short Lingual Osteotomy SSRO IVRO 1 1 1 1 1 1 2 2 1 2 1 1 2 SSRO SSRO IVRO SSRO short lingual osteotomy SL SL IVRO SL 4 6 IVRO SL IVRO SL 1 IVRO SL short lingual
140 J Meikai Dent Med 43 2, 140 147, 2014 Short Lingual Osteotomy SSRO IVRO 1 1 1 1 1 1 2 2 1 2 1 1 2 SSRO SSRO IVRO SSRO short lingual osteotomy SL SL IVRO SL 4 6 IVRO SL IVRO SL 1 IVRO SL short lingual
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
Evaluation of Maximum Mouth Opening after Bilateral Sagittal Split Osteotomy in Patients with Mandibular Prognathism
 43 1 / 35 / 1390 / **** *** ** #* * * ** *** **** 89/9/22 : 89/3/12 : Evaluation of Maximum Mouth Opening after Bilateral Sagittal Split Osteotomy in Patients with Mandibular Prognathism Baratoallah Shaban*,
43 1 / 35 / 1390 / **** *** ** #* * * ** *** **** 89/9/22 : 89/3/12 : Evaluation of Maximum Mouth Opening after Bilateral Sagittal Split Osteotomy in Patients with Mandibular Prognathism Baratoallah Shaban*,
The Application of Cone Beam CT Image Analysis for the Mandibular Ramus Bone Harvesting
 44 The Application of Cone Beam CT Image Analysis for the Mandibular Ramus Bone Harvesting LivingWell Institute of Dental Research Lee, Jang-yeol, Youn, Pil-sang, Kim, Hyoun-chull, Lee Sang-chull Ⅰ. Introduction
44 The Application of Cone Beam CT Image Analysis for the Mandibular Ramus Bone Harvesting LivingWell Institute of Dental Research Lee, Jang-yeol, Youn, Pil-sang, Kim, Hyoun-chull, Lee Sang-chull Ⅰ. Introduction
Correction of Dentofacial Deformities (Orthognathic Surgery)
") Correction of Dentofacial Deformities (Orthognathic Surgery) BDS, MSc, German board of Oral and Maxillofacial Surgery ( Berlin-Germany), Doctoral degree by LBMS Definition Orthognathic surgery is a combination
Correction of Dentofacial Deformities (Orthognathic Surgery) BDS, MSc, German board of Oral and Maxillofacial Surgery ( Berlin-Germany), Doctoral degree by LBMS Definition Orthognathic surgery is a combination
Stability of maxillary advancement using rigid fixation and porous-block hydroxyapatite grafting: Cleft palate versus non-cleft patients
 Pushkar Mehra, BDS, DMD Formerly,Fellow Oral and Maxillofacial Currently, Assistant Professor Oral and Maxillofacial Boston University School of Dental Medicine Director Boston Medical Center Boston, Massachusetts
Pushkar Mehra, BDS, DMD Formerly,Fellow Oral and Maxillofacial Currently, Assistant Professor Oral and Maxillofacial Boston University School of Dental Medicine Director Boston Medical Center Boston, Massachusetts
Orthognathic surgery for a patient with trichorhinophalangeal syndrome type I: A case report
 Orthognathic surgery for a patient with trichorhinophalangeal syndrome type I: A case report Kentaro Kunimori, DDS, a Kiyoshi Harada, DDS, PhD, b Yutaka Maruoka, DDS, PhD, c and Ken Omura, DDS, PhD, d
Orthognathic surgery for a patient with trichorhinophalangeal syndrome type I: A case report Kentaro Kunimori, DDS, a Kiyoshi Harada, DDS, PhD, b Yutaka Maruoka, DDS, PhD, c and Ken Omura, DDS, PhD, d
The America Association of Oral and Maxillofacial Surgeons classify occlusion/malocclusion in to the following three categories:
 Subject: Orthognathic Surgery Policy Effective Date: 04/2016 Revision Date: 07/2018 DESCRIPTION Orthognathic surgery is an open surgical procedure that corrects anomalies or malformations of the lower
Subject: Orthognathic Surgery Policy Effective Date: 04/2016 Revision Date: 07/2018 DESCRIPTION Orthognathic surgery is an open surgical procedure that corrects anomalies or malformations of the lower
Mixed-reality simulation for orthognathic surgery
 Fushima and Kobayashi Maxillofacial Plastic and Reconstructive Surgery (2016) 38:13 DOI 10.1186/s40902-016-0059-z METHODOLOGY Mixed-reality simulation for orthognathic surgery Kenji Fushima 1* and Masaru
Fushima and Kobayashi Maxillofacial Plastic and Reconstructive Surgery (2016) 38:13 DOI 10.1186/s40902-016-0059-z METHODOLOGY Mixed-reality simulation for orthognathic surgery Kenji Fushima 1* and Masaru
Three-dimensional analysis of pharyngeal airway change of skeletal class III patients in cone beam computed tomography after bimaxillary surgery
 ORIGINAL ARTICLE http://dx.doi.org/10.5125/jkaoms.2012.38.1.9 Three-dimensional analysis of pharyngeal airway change of skeletal class III patients in cone beam computed tomography after bimaxillary surgery
ORIGINAL ARTICLE http://dx.doi.org/10.5125/jkaoms.2012.38.1.9 Three-dimensional analysis of pharyngeal airway change of skeletal class III patients in cone beam computed tomography after bimaxillary surgery
Research report for MSc Dent. University of Witwatersrand. Faculty of health science. Dr J Beukes. Student number: h
 Research report for MSc Dent University of Witwatersrand Faculty of health science Dr J Beukes Student number: 9507510h Supervisor: Prof JP Reyneke October 2011 1 1. Title 2. Aim 3. Introduction 4. Objectives
Research report for MSc Dent University of Witwatersrand Faculty of health science Dr J Beukes Student number: 9507510h Supervisor: Prof JP Reyneke October 2011 1 1. Title 2. Aim 3. Introduction 4. Objectives
Patients with cleft lip and palate (CLP) usually
 usually") Comparison of Treatment Outcome and Stability Between Distraction Osteogenesis and LeFort I Osteotomy in Cleft Patients With Maxillary Hypoplasia Seung-Hak Baek, DDS, MSD, PhD,* Jin-Kyung Lee, DDS, 1 Jong-Ho
Comparison of Treatment Outcome and Stability Between Distraction Osteogenesis and LeFort I Osteotomy in Cleft Patients With Maxillary Hypoplasia Seung-Hak Baek, DDS, MSD, PhD,* Jin-Kyung Lee, DDS, 1 Jong-Ho
Title. Class III Patients. Author(s) Issue Date Journal Article. Text version author.
 Issue Date Journal Article. Text version author.") Title Author(s) Citation Assessment of Pterygomaxillary Sepa Class III Patients Ueki, Koichiro; Hashiba, Yukari; Ma Alam, Shamiul; Nakagawa, Kiyomasa; Journal of Oral and Maxillofacial S Issue Date 2009-04
Title Author(s) Citation Assessment of Pterygomaxillary Sepa Class III Patients Ueki, Koichiro; Hashiba, Yukari; Ma Alam, Shamiul; Nakagawa, Kiyomasa; Journal of Oral and Maxillofacial S Issue Date 2009-04
Soft and Hard Tissue Changes after Bimaxillary Surgery in Chinese Class III Patients
 Original Article Soft and Hard Tissue Changes after Bimaxillary Surgery in Chinese Class III Patients Ming Tak Chew a Abstract: Cephalometric studies have shown that the Chinese race tends to have a greater
Original Article Soft and Hard Tissue Changes after Bimaxillary Surgery in Chinese Class III Patients Ming Tak Chew a Abstract: Cephalometric studies have shown that the Chinese race tends to have a greater
Correlation between Gonial Angle and Different Variables after Bilateral Sagittal Split Ramus Osteotomy
 Original Article Correlation between Gonial Angle and Different Variables after Bilateral Sagittal Split Ramus Osteotomy M. Bayat 1,2, M. Ja'farian 3, O. Ghassemi Habashi 4 1 Assistant Professor, Department
Original Article Correlation between Gonial Angle and Different Variables after Bilateral Sagittal Split Ramus Osteotomy M. Bayat 1,2, M. Ja'farian 3, O. Ghassemi Habashi 4 1 Assistant Professor, Department
Virtual model surgery and wafer fabrication for orthognathic surgery
 Int. J. Oral Maxillofac. Surg. 2009; 38: 1306 1323 available online at http://www.sciencedirect.com Technical Note Orthognathic Surgery Virtual model surgery and wafer fabrication for orthognathic surgery
Int. J. Oral Maxillofac. Surg. 2009; 38: 1306 1323 available online at http://www.sciencedirect.com Technical Note Orthognathic Surgery Virtual model surgery and wafer fabrication for orthognathic surgery
Surgically assisted rapid palatal expansion (SARPE) prior to combined Le Fort I and sagittal osteotomies: A case report
 prior to combined Le Fort I and sagittal osteotomies: A case report") 200 Carlos Alberto E. Tavares, DDS, MS, DOrth Professor Department of Orthodontics Associação Brasileira de Odontologia - RS Porto Alegre, Brazil Miguel Scheffer, DDS, MS Chairman Department of Oral and
200 Carlos Alberto E. Tavares, DDS, MS, DOrth Professor Department of Orthodontics Associação Brasileira de Odontologia - RS Porto Alegre, Brazil Miguel Scheffer, DDS, MS Chairman Department of Oral and
Maxillofacial Plastic and Reconstructive Surgery. Sung-Ho Shin, Yei-Jin Kang and Seong-Gon Kim *
 Shin et al. Maxillofacial Plastic and Reconstructive Surgery (2018) 40:36 https://doi.org/10.1186/s40902-018-0174-0 Maxillofacial Plastic and Reconstructive Surgery RESEARCH Open Access The effect of botulinum
Shin et al. Maxillofacial Plastic and Reconstructive Surgery (2018) 40:36 https://doi.org/10.1186/s40902-018-0174-0 Maxillofacial Plastic and Reconstructive Surgery RESEARCH Open Access The effect of botulinum
PREDICTING LOWER LIP AND CHIN RESPONSE TO MANDIBULAR ADVANCEMENT WITH GENIOPLASTY A CEPHALOMETRIC STUDY
 PREDICTING LOWER LIP AND CHIN RESPONSE TO MANDIBULAR ADVANCEMENT WITH GENIOPLASTY A CEPHALOMETRIC STUDY Dr. Deepthi T. Amanna Authors : Dr. Deepthi T. Amanna Assistant Professor Dr. E.T. Roy Professor
PREDICTING LOWER LIP AND CHIN RESPONSE TO MANDIBULAR ADVANCEMENT WITH GENIOPLASTY A CEPHALOMETRIC STUDY Dr. Deepthi T. Amanna Authors : Dr. Deepthi T. Amanna Assistant Professor Dr. E.T. Roy Professor
MAHP Orthognathic Surgery Guidelines. Medical Policy Statement. Criteria
 Introduction The word orthognathic comes from the Greek words for straighten and jaw. Orthognathic surgery is the surgical correction of abnormalities of the mandible and/or maxilla. 1 It involves the
Introduction The word orthognathic comes from the Greek words for straighten and jaw. Orthognathic surgery is the surgical correction of abnormalities of the mandible and/or maxilla. 1 It involves the
Post-graduate Student, Department of Oral and Maxillofacial Radiology, School of Dentistry, Isfahan University of Medical Sciences, Isfahan, Iran
 Journal section: Oral Surgery Publication Types: Research doi:10.4317/jced.53824 http://dx.doi.org/10.4317/jced.53824 Evaluation of orthognathic surgery on articular disc position and temporomandibular
Journal section: Oral Surgery Publication Types: Research doi:10.4317/jced.53824 http://dx.doi.org/10.4317/jced.53824 Evaluation of orthognathic surgery on articular disc position and temporomandibular
UNCORRECTED PROOF. G.R. Hoffman a,1, P.A. Brennan b,c, * Introduction. Patients and methods 40
 British Journal of Oral and Maxillofacial Surgery (2004) xxx, xxx xxx The skeletal stability of one-piece Le Fort 1 osteotomy to advance the maxilla Part 2. The influence of uncontrollable clinical variables
British Journal of Oral and Maxillofacial Surgery (2004) xxx, xxx xxx The skeletal stability of one-piece Le Fort 1 osteotomy to advance the maxilla Part 2. The influence of uncontrollable clinical variables
Postoperative mandibular stability after orthognathic surgery in patients with mandibular protrusion and mandibular deviation
 Wenli Lai, DDS, PhD Lecturer Department of Orthodontics West China College of Stomatology Sichuan University Chengdu, China Kazuhiro Yamada, DDS, PhD Lecturer Division of Orthodontics Department of Oral
Wenli Lai, DDS, PhD Lecturer Department of Orthodontics West China College of Stomatology Sichuan University Chengdu, China Kazuhiro Yamada, DDS, PhD Lecturer Division of Orthodontics Department of Oral
THE USE OF TEMPORARY ANCHORAGE DEVICES FOR MOLAR INTRUSION & TREATMENT OF ANTERIOR OPEN BITE By Eduardo Nicolaievsky D.D.S.
 THE USE OF TEMPORARY ANCHORAGE DEVICES FOR MOLAR INTRUSION & TREATMENT OF ANTERIOR OPEN BITE By Eduardo Nicolaievsky D.D.S. Skeletal anchorage, the concept of using the facial skeleton to control tooth
THE USE OF TEMPORARY ANCHORAGE DEVICES FOR MOLAR INTRUSION & TREATMENT OF ANTERIOR OPEN BITE By Eduardo Nicolaievsky D.D.S. Skeletal anchorage, the concept of using the facial skeleton to control tooth
DOWNLOAD OR READ : RIGID FIXATION FOR MAXILLOFACIAL SURGERY PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : RIGID FIXATION FOR MAXILLOFACIAL SURGERY PDF EBOOK EPUB MOBI Page 1 Page 2 rigid fixation for maxillofacial surgery rigid fixation for maxillofacial pdf rigid fixation for maxillofacial
DOWNLOAD OR READ : RIGID FIXATION FOR MAXILLOFACIAL SURGERY PDF EBOOK EPUB MOBI Page 1 Page 2 rigid fixation for maxillofacial surgery rigid fixation for maxillofacial pdf rigid fixation for maxillofacial
ORTHOGNATHIC SURGERY
 ORTHOGNATHIC SURGERY MEDICAL POLICY Effective Date: February 1, 2017 Review Dates: 1/93, 7/95, 10/97, 4/99, 10/00, 8/01, 12/01, 4/02, 2/03, 1/04, 1/05, 12/05, 12/06, 12/07, 12/08, 12/09, 12/10, 12/11,
ORTHOGNATHIC SURGERY MEDICAL POLICY Effective Date: February 1, 2017 Review Dates: 1/93, 7/95, 10/97, 4/99, 10/00, 8/01, 12/01, 4/02, 2/03, 1/04, 1/05, 12/05, 12/06, 12/07, 12/08, 12/09, 12/10, 12/11,
Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report
 Case Report Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report 1 Vinni Arora, 2 Rekha Sharma, 3 Sachin Parashar 1 Senior Resident, 2 Professor and Head of Department, 3 Former Resident
Case Report Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report 1 Vinni Arora, 2 Rekha Sharma, 3 Sachin Parashar 1 Senior Resident, 2 Professor and Head of Department, 3 Former Resident
NIH Public Access Author Manuscript Int J Oral Maxillofac Surg. Author manuscript; available in PMC 2014 June 01.
 NIH Public Access Author Manuscript Published in final edited form as: Int J Oral Maxillofac Surg. 2013 June ; 42(6): 780 789. doi:10.1016/j.ijom.2013.01.002. One-year assessment of surgical outcomes in
NIH Public Access Author Manuscript Published in final edited form as: Int J Oral Maxillofac Surg. 2013 June ; 42(6): 780 789. doi:10.1016/j.ijom.2013.01.002. One-year assessment of surgical outcomes in
Stability and Relapse in Orthognathic Surgery
 Stability and Relapse in Orthognathic Surgery Neeraj Panchal, DDS, MD, MA Christine Ellis, DDS, MSD Paul Tiwana, DDS, MD, MS, FACS INTRODUCTION The long-term success of orthognathic reconstructive surgery
Stability and Relapse in Orthognathic Surgery Neeraj Panchal, DDS, MD, MA Christine Ellis, DDS, MSD Paul Tiwana, DDS, MD, MS, FACS INTRODUCTION The long-term success of orthognathic reconstructive surgery
SURGICAL MODEL ACCURACY DEVICE. 25 years - manufacturing and distribution - around the globe research - design - manufacturing - distribution
 SURGICAL MODEL ACCURACY DEVICE 25 years - manufacturing and distribution - around the globe research - design - manufacturing - distribution 2 SMAD - SURGICAL MODEL ACCURACY DEVICE SMAD has be designed
SURGICAL MODEL ACCURACY DEVICE 25 years - manufacturing and distribution - around the globe research - design - manufacturing - distribution 2 SMAD - SURGICAL MODEL ACCURACY DEVICE SMAD has be designed
Topic: Orthognathic Surgery Date of Origin: October 5, Section: Surgery Last Reviewed Date: December 2013
 Medical Policy Manual Topic: Orthognathic Surgery Date of Origin: October 5, 2004 Section: Surgery Last Reviewed Date: December 2013 Policy No: 137 Effective Date: March 1, 2014 IMPORTANT REMINDER Medical
Medical Policy Manual Topic: Orthognathic Surgery Date of Origin: October 5, 2004 Section: Surgery Last Reviewed Date: December 2013 Policy No: 137 Effective Date: March 1, 2014 IMPORTANT REMINDER Medical
Variations in the anatomical dimensions of the mandibular ramus and the presence of third molars: its effect on the sagittal split ramus osteotomy
 1 Variations in the anatomical dimensions of the mandibular ramus and the presence of third molars: its effect on the sagittal split ramus osteotomy J. Beukes 1,, J. P. Reyneke 1,2,3,4, P. J. Becker 5,6
1 Variations in the anatomical dimensions of the mandibular ramus and the presence of third molars: its effect on the sagittal split ramus osteotomy J. Beukes 1,, J. P. Reyneke 1,2,3,4, P. J. Becker 5,6
Condylar positioning changes following unilateral sagittal split ramus osteotomy in patients with mandibular prognathism
 Kim et al. Maxillofacial Plastic and Reconstructive Surgery (2015) 37:36 DOI 10.1186/s40902-015-0036-y CASE REPORT Open Access Condylar positioning changes following unilateral sagittal split ramus osteotomy
Kim et al. Maxillofacial Plastic and Reconstructive Surgery (2015) 37:36 DOI 10.1186/s40902-015-0036-y CASE REPORT Open Access Condylar positioning changes following unilateral sagittal split ramus osteotomy
Surgically assisted rapid maxillary expansion is efficient for
 Rev Bras Otorrinolaringol 2006;72(4):457-61. ORIGINAL ARTICLE Surgically assisted rapid maxillary expasion: a preliminar study Belmiro Cavalcanti do Egito Vasconcelos 1, Antonio Figueiredo Caubi 2, Emanuel
Rev Bras Otorrinolaringol 2006;72(4):457-61. ORIGINAL ARTICLE Surgically assisted rapid maxillary expasion: a preliminar study Belmiro Cavalcanti do Egito Vasconcelos 1, Antonio Figueiredo Caubi 2, Emanuel
Long-Term Results of. Vertical Height Augmentation Genioplasty using Autogenous Iliac Bone Graft
 Long-Term Results of Vertical Height Augmentation Genioplasty using Autogenous Iliac Bone Graft Gi Jung Kim Department of Dentistry The Graduate School Yonsei University Long-Term Results of Vertical Height
Long-Term Results of Vertical Height Augmentation Genioplasty using Autogenous Iliac Bone Graft Gi Jung Kim Department of Dentistry The Graduate School Yonsei University Long-Term Results of Vertical Height
Three Dimensional Titanium Mini Plates in Management of Mandibular Fractures
 Biomedical & Pharmacology Journal Vol. 7(1), 241-246 (2014) Three Dimensional Titanium Mini Plates in Management of Mandibular Fractures R. BALAKRISHNAN, VIJAY EBENEZER and ABU DAKIR Department of Oral
Biomedical & Pharmacology Journal Vol. 7(1), 241-246 (2014) Three Dimensional Titanium Mini Plates in Management of Mandibular Fractures R. BALAKRISHNAN, VIJAY EBENEZER and ABU DAKIR Department of Oral
Clinical evaluation of temporomandibular joint disorder after orthognathic surgery in skeletal class II malocclusion patients
 ORIGINAL ARTICLE http://dx.doi.org/10.5125/jkaoms.2012.38.3.139 pissn 22347550 eissn 22345930 Clinical evaluation of temporomandibular joint disorder after orthognathic surgery in skeletal class II malocclusion
ORIGINAL ARTICLE http://dx.doi.org/10.5125/jkaoms.2012.38.3.139 pissn 22347550 eissn 22345930 Clinical evaluation of temporomandibular joint disorder after orthognathic surgery in skeletal class II malocclusion
Genioglossus Advancement Accompanied by Mandibular Setback and Maxillary Advancement Surgery in Severely Obese Patient
 Shimane J. Med. Sci., Vol.33 pp.93-98, 2017 Genioglossus Advancement Accompanied by Mandibular Setback and Maxillary Advancement Surgery in Severely Obese Patient Taichi IDE, Takahiro KANNO, Masaaki KARINO,
Shimane J. Med. Sci., Vol.33 pp.93-98, 2017 Genioglossus Advancement Accompanied by Mandibular Setback and Maxillary Advancement Surgery in Severely Obese Patient Taichi IDE, Takahiro KANNO, Masaaki KARINO,
CT of Maxillofacial Injuries
 CT of Maxillofacial Injuries Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Viking 1 1976 MGS 2001 Technology changes the diagnosis Technologic Evolution
CT of Maxillofacial Injuries Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Viking 1 1976 MGS 2001 Technology changes the diagnosis Technologic Evolution
Effects of different surgical procedures on the pharyngeal space with mandibular prognathism
 J Osaka Dent Univ 2015 (October) ; 49 (2) : 143 148. Effects of different surgical procedures on the pharyngeal space with mandibular prognathism Yutaka Yamada and Naoyuki Matsumoto Department of Orthodontics,
J Osaka Dent Univ 2015 (October) ; 49 (2) : 143 148. Effects of different surgical procedures on the pharyngeal space with mandibular prognathism Yutaka Yamada and Naoyuki Matsumoto Department of Orthodontics,
ORTHOGNATHIC SURGERY
 Status Active Medical and Behavioral Health Policy Section: Surgery Policy Number: IV-16 Effective Date: 10/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Status Active Medical and Behavioral Health Policy Section: Surgery Policy Number: IV-16 Effective Date: 10/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Orthodontic and Orthognathic Surgical Correction of a Skeletal Class III Malocclusion
 Dental Medicine Research 30 2) 161 166, 2010 161 Case Report Orthodontic and Orthognathic Surgical Correction of a Skeletal Class III Malocclusion Tetsutaro Yamaguchi, Yoko Tomoyasu, Tatsuo Shirota*, Masashi
Dental Medicine Research 30 2) 161 166, 2010 161 Case Report Orthodontic and Orthognathic Surgical Correction of a Skeletal Class III Malocclusion Tetsutaro Yamaguchi, Yoko Tomoyasu, Tatsuo Shirota*, Masashi
King's College Hospital Dental School, London, S.E. 5.
 OSTECTOMY AT THE MANDIBULAR SYMPHYSIS J. H. SOWRAY, B.D.S., F.D.S.R.C.S. (Eng.), L.R.C.P., M.R.C.S. and R. HASKELL, M.B., B.S., F.D.S.R.C.S. (Eng.). King's College Hospital Dental School, London, S.E.
OSTECTOMY AT THE MANDIBULAR SYMPHYSIS J. H. SOWRAY, B.D.S., F.D.S.R.C.S. (Eng.), L.R.C.P., M.R.C.S. and R. HASKELL, M.B., B.S., F.D.S.R.C.S. (Eng.). King's College Hospital Dental School, London, S.E.
Technique Guide. IMF Screw Set. For intermaxillary fixation.
 Technique Guide IMF Screw Set. For intermaxillary fixation. Table of Contents Introduction IMF Screw Set 2 Indications and Contraindications 3 Surgical Technique Preparation 4 Insert IMF Screw 6 Insert
Technique Guide IMF Screw Set. For intermaxillary fixation. Table of Contents Introduction IMF Screw Set 2 Indications and Contraindications 3 Surgical Technique Preparation 4 Insert IMF Screw 6 Insert
Intraoral mandibular distraction osteogenesis in facial asymmetry patients with unilateral temporomandibular joint bony ankylosis
 Int. J. Oral Maxillofac. Surg. 2002; 31: 544 548 doi:10.1054/ijom.2002.0297, available online at http://www.idealibrary.com on Intraoral mandibular distraction osteogenesis in facial asymmetry patients
Int. J. Oral Maxillofac. Surg. 2002; 31: 544 548 doi:10.1054/ijom.2002.0297, available online at http://www.idealibrary.com on Intraoral mandibular distraction osteogenesis in facial asymmetry patients
Professor, Department of Craniofacial Orthodontics, Chang Gung Memorial Hospital,
 Dr. Ellen Wen-Ching Ko, DDS, MS Professor, Department of Craniofacial Orthodontics, Chang Gung Memorial Hospital, Taipei, Taiwan Professor, Graduate Institute of Craniofacial and Dental Science, Chang
Dr. Ellen Wen-Ching Ko, DDS, MS Professor, Department of Craniofacial Orthodontics, Chang Gung Memorial Hospital, Taipei, Taiwan Professor, Graduate Institute of Craniofacial and Dental Science, Chang
Arnett FAB Orthognathic System
 Craniomaxillofacial Surgery Arnett FAB Orthognathic System face, airway, bite Designed in cooperation with Dr. William Arnett, Santa Barbara, CA The goals of Orthognathic Surgery are facial, airway, and
Craniomaxillofacial Surgery Arnett FAB Orthognathic System face, airway, bite Designed in cooperation with Dr. William Arnett, Santa Barbara, CA The goals of Orthognathic Surgery are facial, airway, and
An Adult Case of Skeletal Open Bite with a Severely Narrowed Maxillary Dental Arch
 Case Report An Adult Case of Skeletal Open Bite with a Severely Narrowed Maxillary Dental Arch Michiru Takeuchi, DDS a ; Eiji Tanaka, DDS, PhD b ; Daisuke Nonoyama, DDS c ; Junko Aoyama, DDS d ; Kazuo
Case Report An Adult Case of Skeletal Open Bite with a Severely Narrowed Maxillary Dental Arch Michiru Takeuchi, DDS a ; Eiji Tanaka, DDS, PhD b ; Daisuke Nonoyama, DDS c ; Junko Aoyama, DDS d ; Kazuo
DISTRACTION PRODUCT OVERVIEW. For a wide variety of facial applications
 DISTRACTION PRODUCT OVERVIEW For a wide variety of facial applications DISTRACTION PRODUCT OVERVIEW. STRONG, MODULAR, VERSATILE CRANIOFACIAL DISTRACTION External Midface Distractor Distraction of the maxilla,
DISTRACTION PRODUCT OVERVIEW For a wide variety of facial applications DISTRACTION PRODUCT OVERVIEW. STRONG, MODULAR, VERSATILE CRANIOFACIAL DISTRACTION External Midface Distractor Distraction of the maxilla,
CT of Maxillofacial Fracture Patterns. CT of Maxillofacial Fracture Patterns
 CT of Maxillofacial Fracture Patterns CT of Maxillofacial Fracture Patterns Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Viking 1 1976 MGS 2001 Technology
CT of Maxillofacial Fracture Patterns CT of Maxillofacial Fracture Patterns Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Viking 1 1976 MGS 2001 Technology
Midline Mandibular Osteotomy in an Asymmetric Patient
 Case Report Midline Mandibular Osteotomy in an Asymmetric Patient M. L. Anghinoni a ; A. S. Magri b ; A. Di Blasio c ; L. Toma d ; E. Sesenna e ABSTRACT This case report shows the possibility of the application
Case Report Midline Mandibular Osteotomy in an Asymmetric Patient M. L. Anghinoni a ; A. S. Magri b ; A. Di Blasio c ; L. Toma d ; E. Sesenna e ABSTRACT This case report shows the possibility of the application
Interesting Case Series. Virtual Surgical Planning in Orthognathic Surgery
 Interesting Case Series Virtual Surgical Planning in Orthognathic Surgery Suraj Jaisinghani, MS, a Nicholas S. Adams, MD, b,c Robert J. Mann, MD, b,c,d John W. Polley, MD, b,c,d, and John A. Girotto, MD,
Interesting Case Series Virtual Surgical Planning in Orthognathic Surgery Suraj Jaisinghani, MS, a Nicholas S. Adams, MD, b,c Robert J. Mann, MD, b,c,d John W. Polley, MD, b,c,d, and John A. Girotto, MD,
Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient
 Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
intraoral vertical ramus osteotomy
 Title Author(s) Citation The effects of changing position an intraoral vertical ramus osteotomy Ueki, Koichiro; Hashiba, Yukari; Ma Kiyomasa; Alam, Shamiul; Okabe, Kat International Journal of Oral and
Title Author(s) Citation The effects of changing position an intraoral vertical ramus osteotomy Ueki, Koichiro; Hashiba, Yukari; Ma Kiyomasa; Alam, Shamiul; Okabe, Kat International Journal of Oral and
Treatment of severe unilateral open bite and crossbite in cleft lip and palate patients
 European Journal of Orthodontics 6 (1984) 294-3(12 1984 European Orthodontic Society Treatment of severe unilateral open bite and crossbite in cleft lip and palate patients Hans Enemark Aarhus, Denmark
European Journal of Orthodontics 6 (1984) 294-3(12 1984 European Orthodontic Society Treatment of severe unilateral open bite and crossbite in cleft lip and palate patients Hans Enemark Aarhus, Denmark
CHAPTER. 1. Uncontrolled systemic disease 2. Retrognathic jaw relationship
 CHAPTER 7 Immediate Implant Supported Restoration of the Edentulous Arch Stephen G. Alfano and Robert M. Laughlin Department of Oral and Maxillofacial Surgery, Naval Medical Center San Diego, San Diego,
CHAPTER 7 Immediate Implant Supported Restoration of the Edentulous Arch Stephen G. Alfano and Robert M. Laughlin Department of Oral and Maxillofacial Surgery, Naval Medical Center San Diego, San Diego,
Skeletal Relapse after Correction of Mandibular Prognathism by Bilateral Sagittal Split Ramus Osteotomy
 Original Article Skeletal Relapse after Correction of Mandibular Prognathism by Bilateral Sagittal Split Ramus Osteotomy H. Mohajerani 1, M. Mehdizadeh 2, A. Khalighi Sigaroodi 3 1 Assistant Professor,
Original Article Skeletal Relapse after Correction of Mandibular Prognathism by Bilateral Sagittal Split Ramus Osteotomy H. Mohajerani 1, M. Mehdizadeh 2, A. Khalighi Sigaroodi 3 1 Assistant Professor,
3. The Jaw and Related Structures
 Overview and objectives of this dissection 3. The Jaw and Related Structures The goal of this dissection is to observe the muscles of jaw raising. You will also have the opportunity to observe several
Overview and objectives of this dissection 3. The Jaw and Related Structures The goal of this dissection is to observe the muscles of jaw raising. You will also have the opportunity to observe several
Orthodontics-surgical combination therapy for Class III skeletal malocclusion
 [Downloaded free from http://www.contempclindent.org on Tuesday, July 16, 2013, IP: 164.100.31.82] Click here to download free Android application for this jou Orthodontics-surgical combination therapy
[Downloaded free from http://www.contempclindent.org on Tuesday, July 16, 2013, IP: 164.100.31.82] Click here to download free Android application for this jou Orthodontics-surgical combination therapy
Displacement Patterns of the Maxilla During Parallel and Rotational Setback Movements: A Finite Element Analysis
 e-issn 1643-3750 DOI: 10.12659/MSM.900749 Received: 2016.07.25 Accepted: 2016.08.17 Published: 2017.04.02 Displacement Patterns of the Maxilla During Parallel and Rotational Setback Movements: A Finite
e-issn 1643-3750 DOI: 10.12659/MSM.900749 Received: 2016.07.25 Accepted: 2016.08.17 Published: 2017.04.02 Displacement Patterns of the Maxilla During Parallel and Rotational Setback Movements: A Finite
Objective: The antilingular prominence (AP) is a well-known landmark used during planning
 is a well-known landmark used during planning") *Revised Manuscript without title page Abstract Objective: The antilingular prominence (AP) is a well-known landmark used during planning of intraoral vertical ramus osteotomy (IVRO) in order to prevent
*Revised Manuscript without title page Abstract Objective: The antilingular prominence (AP) is a well-known landmark used during planning of intraoral vertical ramus osteotomy (IVRO) in order to prevent
Non-osseointegrated. What type of mini-implants? 3/27/2008. Require a tight fit to be effective Stability depends on the quality and.
 Non-osseointegrated What type of mini-implants? Require a tight fit to be effective Stability depends on the quality and quantity of cortical and trabecular bone. Osseointegrated Non-osseointegrated AbsoAnchor
Non-osseointegrated What type of mini-implants? Require a tight fit to be effective Stability depends on the quality and quantity of cortical and trabecular bone. Osseointegrated Non-osseointegrated AbsoAnchor
Mesial Step Class I or Class III Dependent upon extent of step seen clinically and patient s growth pattern Refer for early evaluation (by 8 years)
") Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Case Study. Micrognathia Secondary to Pierre Robin Sequence. Treated with distraction osteogenesis using an internal mandible distractor.
 Case Study Micrognathia Secondary to Pierre Robin Sequence. Treated with distraction osteogenesis using an internal mandible distractor. Micrognathia Secondary to Pierre Robin Sequence Patient profile
Case Study Micrognathia Secondary to Pierre Robin Sequence. Treated with distraction osteogenesis using an internal mandible distractor. Micrognathia Secondary to Pierre Robin Sequence Patient profile
Imaging Orbit/Periorbital Injury
 Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
Two- and Three-dimensional Orthodontic Imaging Using Limited Cone Beam Computed Tomography
 Original Article Two- and Three-dimensional Orthodontic Imaging Using Limited Cone Beam Computed Tomography Akira Nakajima a ; Glenn T. Sameshima b ; Yoshinori Arai c ; Yoshito Homme d ; Noriyoshi Shimizu
Original Article Two- and Three-dimensional Orthodontic Imaging Using Limited Cone Beam Computed Tomography Akira Nakajima a ; Glenn T. Sameshima b ; Yoshinori Arai c ; Yoshito Homme d ; Noriyoshi Shimizu
Craniomaxillofacial Surgery. Arnett FAB. Orthognathic System. face, airway, bite. Designed in cooperation with Dr. William Arnett, Santa Barbara, CA
 Craniomaxillofacial Surgery Arnett FAB Orthognathic System face, airway, bite ed in cooperation with Dr. William Arnett, Santa Barbara, CA Surgeons and orthodontists both correct the occlusion with varying
Craniomaxillofacial Surgery Arnett FAB Orthognathic System face, airway, bite ed in cooperation with Dr. William Arnett, Santa Barbara, CA Surgeons and orthodontists both correct the occlusion with varying
Educational Training Document
 Educational Training Document Table of Contents Part 1: Resource Document Disclaimer Page: 2 Part 2: Line Item Grade Sheets Page: 3 Release: 11/2016 Page 1 of 6 Part 1: Resource Document Disclaimer The
Educational Training Document Table of Contents Part 1: Resource Document Disclaimer Page: 2 Part 2: Line Item Grade Sheets Page: 3 Release: 11/2016 Page 1 of 6 Part 1: Resource Document Disclaimer The
Case Report Decompression of the inferior alveolar nerve to treat the pain of the mandible caused by fibrous dysplasia-case report
 Int J Clin Exp Med 2015;8(10):19535-19539 www.ijcem.com /ISSN:1940-5901/IJCEM0014642 Case Report Decompression of the inferior alveolar nerve to treat the pain of the mandible caused by fibrous dysplasia-case
Int J Clin Exp Med 2015;8(10):19535-19539 www.ijcem.com /ISSN:1940-5901/IJCEM0014642 Case Report Decompression of the inferior alveolar nerve to treat the pain of the mandible caused by fibrous dysplasia-case
LOGIC SURGICAL TECHNIQUE GUIDE. In d i c at i o n s. Co n t r a i n d i c at i o n s. Mandibular Distraction System
 TM SURGICAL TECHNIQUE GUIDE In d i c at i o n s The OSTEOMED Mandibular Distractor system is indicated for use as a mandibular bone lengthener for patients diagnosed with conditions where treatment includes
TM SURGICAL TECHNIQUE GUIDE In d i c at i o n s The OSTEOMED Mandibular Distractor system is indicated for use as a mandibular bone lengthener for patients diagnosed with conditions where treatment includes
Intramembranous autogenous bone graft is the gold
 CASE LETTER CBCT Morphologic Analysis of Edentulous Posterior Mandible for Mandibular Body Bone Graft Jae-Min Song, DDS, MSD, PhD 1 Jae-Yeol Lee, DDS, MSD, PhD 1,2 Yong-Deok Kim, DDS, MSD, PhD 2,3 * INTRODUCTION
CASE LETTER CBCT Morphologic Analysis of Edentulous Posterior Mandible for Mandibular Body Bone Graft Jae-Min Song, DDS, MSD, PhD 1 Jae-Yeol Lee, DDS, MSD, PhD 1,2 Yong-Deok Kim, DDS, MSD, PhD 2,3 * INTRODUCTION
Do Patients Treated With Bimaxillary Surgery Have More Stable Condylar Positions Than Those Who Have Undergone Single-Jaw Surgery?
 CRANIOMAXILLOFACIAL DEFORMITIES/COSMETIC SURGERY Do Patients Treated With Bimaxillary Surgery Have More Stable Condylar Positions Than Those Who Have Undergone Single-Jaw Surgery? Yoon-Ji Kim, DDS, MSD,*
CRANIOMAXILLOFACIAL DEFORMITIES/COSMETIC SURGERY Do Patients Treated With Bimaxillary Surgery Have More Stable Condylar Positions Than Those Who Have Undergone Single-Jaw Surgery? Yoon-Ji Kim, DDS, MSD,*
Q2Q3 Reza Movahed, DMD a, *, Larry Wolford, DMD b,c. oralmaxsurgery.theclinics.com KEYWORDS KEY POINTS
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 Protocol for Concomitant Temporomandibular
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 Protocol for Concomitant Temporomandibular
The use of a LeFort I osteotomy to correct
 ORIGINAL ARTICLE LeFort I maxillary advancement: 3-year stability and risk factors for relapse Paul A. Dowling, a Lisen Espeland, b Leiv Sandvik, c Karim A. Mobarak, d and Hans Erik Hogevold e Dublin,
ORIGINAL ARTICLE LeFort I maxillary advancement: 3-year stability and risk factors for relapse Paul A. Dowling, a Lisen Espeland, b Leiv Sandvik, c Karim A. Mobarak, d and Hans Erik Hogevold e Dublin,
A lingual orthodontic case with 3M Incognito Appliance System combined with orthognathic surgery.
 SM 3M Health Care Academy A lingual orthodontic case with 3M Incognito Appliance System combined with orthognathic surgery. Dr. B. Iglesias-Sánchez Dr. F. Hernandez-Alfaro Dr. J.C. Pérez-Varela DDS, MS.
SM 3M Health Care Academy A lingual orthodontic case with 3M Incognito Appliance System combined with orthognathic surgery. Dr. B. Iglesias-Sánchez Dr. F. Hernandez-Alfaro Dr. J.C. Pérez-Varela DDS, MS.
Patient information booklet Orthognathic Surgery
 Patient information booklet Orthognathic Surgery 2 Table of contents This patient information booklet contains all the answers to your questions regarding orthognathic surgery. + + + + + + What is Orthognathic
Patient information booklet Orthognathic Surgery 2 Table of contents This patient information booklet contains all the answers to your questions regarding orthognathic surgery. + + + + + + What is Orthognathic
Research Article Length and Geometric Patterns of the Greater Palatine Canal Observed in Cone Beam Computed Tomography
 International Dentistry Volume 2010, Article ID 292753, 6 pages doi:10.1155/2010/292753 Research Article Length and Geometric Patterns of the Greater Palatine Canal Observed in Cone Beam Computed Tomography
International Dentistry Volume 2010, Article ID 292753, 6 pages doi:10.1155/2010/292753 Research Article Length and Geometric Patterns of the Greater Palatine Canal Observed in Cone Beam Computed Tomography
06/12/18. [Note: When orthognathic surgery is not a covered benefit, it is non-covered for any diagnosis, including sleep apnea.]
![06/12/18. [Note: When orthognathic surgery is not a covered benefit, it is non-covered for any diagnosis, including sleep apnea.]](/thumbs/84/91182117.jpg "06/12/18. [Note: When orthognathic surgery is not a covered benefit, it is non-covered for any diagnosis, including sleep apnea.]") Reference #: MC/B002 Page: 1 of 5 PRODUCT APPLICATION: PreferredOne Community Health Plan (PCHP) PreferredOne Administrative Services, Inc. (PAS) ERISA PreferredOne Administrative Services, Inc. (PAS)
Reference #: MC/B002 Page: 1 of 5 PRODUCT APPLICATION: PreferredOne Community Health Plan (PCHP) PreferredOne Administrative Services, Inc. (PAS) ERISA PreferredOne Administrative Services, Inc. (PAS)
Mechanical Effects of Down Fracture in Le Fort osteotomy on the Skull Base
 J Meikai Dent Med 46 1, 55 63, 2017 55 Le Fort Victor Jose KITANO FLORES Le Fort Le Fort Le Fort Le Fort 2 7 Le Fort Le Fort Mechanical Effects of Down Fracture in Le Fort osteotomy on the Skull Base Takuya
J Meikai Dent Med 46 1, 55 63, 2017 55 Le Fort Victor Jose KITANO FLORES Le Fort Le Fort Le Fort Le Fort 2 7 Le Fort Le Fort Mechanical Effects of Down Fracture in Le Fort osteotomy on the Skull Base Takuya
Osteochondroma of the mandibular condyle cured by conservative resection
 Journal of Dental Sciences (2014) 9, 91e95 Available online at www.sciencedirect.com journal homepage: www.e-jds.com CASE REPORT Osteochondroma of the mandibular condyle cured by conservative resection
Journal of Dental Sciences (2014) 9, 91e95 Available online at www.sciencedirect.com journal homepage: www.e-jds.com CASE REPORT Osteochondroma of the mandibular condyle cured by conservative resection
Relationship of the Mandibular Canal and Fixation Placement to Sensory Alteration following Orthognathic Surgery.
 Relationship of the Mandibular Canal and Fixation Placement to Sensory Alteration following Orthognathic Surgery. Gary R Tucker Jr., DDS A thesis submitted to the faculty of the University of North Carolina
Relationship of the Mandibular Canal and Fixation Placement to Sensory Alteration following Orthognathic Surgery. Gary R Tucker Jr., DDS A thesis submitted to the faculty of the University of North Carolina
RapidSorb Resorbable Tacks. Resorbable Fixation System.
 RapidSorb Resorbable Tacks. Resorbable Fixation System. Fast Safe Resorbable Drill Press Fixed Table of Contents Introduction Overview 2 Indications and Contraindications 4 RapidSorb 5 Surgical Technique
RapidSorb Resorbable Tacks. Resorbable Fixation System. Fast Safe Resorbable Drill Press Fixed Table of Contents Introduction Overview 2 Indications and Contraindications 4 RapidSorb 5 Surgical Technique
Arrangement of the artificial teeth:
 Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Intraoperative measurement of maxillary repositioning in a series of 30 patients with maxillomandibular vertical asymmetries
 Giancarlo Renzi, MD Andrea Carboni, MD Maurizio Perugini, MD Fellow Maxilllofacial Surgery Department University La Sapienza Rome, Italy Roberto Becelli, PhD, MDS Professor Maxillofacial Surgery Teaching
Giancarlo Renzi, MD Andrea Carboni, MD Maurizio Perugini, MD Fellow Maxilllofacial Surgery Department University La Sapienza Rome, Italy Roberto Becelli, PhD, MDS Professor Maxillofacial Surgery Teaching
sagittal split ramus osteotomy
 Title Author(s) Citation Position of mandibular canal and ra sagittal split ramus osteotomy Ueki, Koichiro; Okabe, Katsuhiko; M Marukawa, Kohei; Nakagawa, Kiyomasa Journal of Oral and Maxillofacial S Issue
Title Author(s) Citation Position of mandibular canal and ra sagittal split ramus osteotomy Ueki, Koichiro; Okabe, Katsuhiko; M Marukawa, Kohei; Nakagawa, Kiyomasa Journal of Oral and Maxillofacial S Issue
IJCMR 553. ORIGINAL RESEARCH Different Population- Different Analysis A Cephalometric Study. Sachin Singh 1, Jayesh Rahalkar 2 ABSTRACT INTRODUCTION
 IJCMR 553 ORIGINAL RESEARCH Different Population- Different Analysis A Cephalometric Study Sachin Singh 1, Jayesh Rahalkar 2 ABSTRACT Introduction: Cephalometric norms derived for Caucasian population
IJCMR 553 ORIGINAL RESEARCH Different Population- Different Analysis A Cephalometric Study Sachin Singh 1, Jayesh Rahalkar 2 ABSTRACT Introduction: Cephalometric norms derived for Caucasian population
Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery FACIAL FRACTURES
 Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery A. General Considerations FACIAL FRACTURES Look for other fractures like skull and/or cervical spine fractures Test function
Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery A. General Considerations FACIAL FRACTURES Look for other fractures like skull and/or cervical spine fractures Test function
Severe Malocclusion: Appropriately Timed Treatment. This article discusses challenging issues clinicians face when treating
 Severe Malocclusion: The Importance of Appropriately Timed Treatment A Synchronized and Simultaneous Interdisciplinary Plan Using Cosmetic Dentistry Principles David M. Sarver, DMD, MS Abstract This article
Severe Malocclusion: The Importance of Appropriately Timed Treatment A Synchronized and Simultaneous Interdisciplinary Plan Using Cosmetic Dentistry Principles David M. Sarver, DMD, MS Abstract This article
Different Non Surgical Treatment Modalities for Class III Malocclusion
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 9, Issue 6 (Sep.- Oct. 2013), PP 48-52 Different Non Surgical Treatment Modalities for Class III Malocclusion
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 9, Issue 6 (Sep.- Oct. 2013), PP 48-52 Different Non Surgical Treatment Modalities for Class III Malocclusion
Upper arch. 1Prosthodontics. Dr.Bassam Ali Al-Turaihi. Basic anatomy & & landmark of denture & mouth
 1Prosthodontics Lecture 2 Dr.Bassam Ali Al-Turaihi Basic anatomy & & landmark of denture & mouth Upper arch Palatine process of maxilla: it form the anterior three quarter of the hard palate. Horizontal
1Prosthodontics Lecture 2 Dr.Bassam Ali Al-Turaihi Basic anatomy & & landmark of denture & mouth Upper arch Palatine process of maxilla: it form the anterior three quarter of the hard palate. Horizontal
Surgical Orthodontic Correction of Acromegaly with Mandibular Prognathism
 Case Report Surgical Orthodontic Correction of Acromegaly with Mandibular Prognathism Takakaza Yagi, DDS, PhD a ; Masayoshi Kawakami, DDS, PhD b ; Kenji Takada, PhD, DDS c Abstract: A male (30 years five
Case Report Surgical Orthodontic Correction of Acromegaly with Mandibular Prognathism Takakaza Yagi, DDS, PhD a ; Masayoshi Kawakami, DDS, PhD b ; Kenji Takada, PhD, DDS c Abstract: A male (30 years five
Maxillary Growth Control with High Pull Headgear- A Case Report
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 01 Ver. X January. (2018), PP 09-13 www.iosrjournals.org Maxillary Growth Control with High
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 01 Ver. X January. (2018), PP 09-13 www.iosrjournals.org Maxillary Growth Control with High
Case Study. Case # 1 Author: Dr. Suheil Boutros (USA) 2013 Zimmer Dental, Inc. All rights reserved. 6557, Rev. 03/13.
 2013 Zimmer Dental, Inc. All rights reserved. 6557, Rev. 03/13.") Placement of a Zimmer Trabecular Metal Dental Implant with Simultaneous Ridge Augmentation and Immediate Non-Functional Loading Following Tooth Extraction and Orthodontic Treatment for Implant Site Development
Placement of a Zimmer Trabecular Metal Dental Implant with Simultaneous Ridge Augmentation and Immediate Non-Functional Loading Following Tooth Extraction and Orthodontic Treatment for Implant Site Development
Original Article Factors affecting the outcomes of non-surgical treatment for intracapsular condylar fractures
 Int J Clin Exp Med 2016;9(6):10847-10855 www.ijcem.com /ISSN:1940-5901/IJCEM0021362 Original Article Factors affecting the outcomes of non-surgical treatment for intracapsular condylar fractures Bao-Li
Int J Clin Exp Med 2016;9(6):10847-10855 www.ijcem.com /ISSN:1940-5901/IJCEM0021362 Original Article Factors affecting the outcomes of non-surgical treatment for intracapsular condylar fractures Bao-Li