Skin Cut Up D R R O K I A H A L I C O N S U L T A N T D E R M A T O P A T H O L O G I S T S T H
|
|
|
- Rosamond Walker
- 6 years ago
- Views:
Transcription
1 Skin Cut Up D R R O K I A H A L I C O N S U L T A N T D E R M A T O P A T H O L O G I S T S T H
2 General Instructions The type of biopsy is documented Orientated or not (suture indicating what margin according to hours on the face of a clock). If more than one suture, indicate which margins these represent The no. of fragments (if more than one, either mention exact no. e.g. two or if multiple e.g. for greater than 10, then mention multiple) is documented.
3 General Instructions Small biopsies (less than 5 mm) are submitted intact and three automatic levels requested If biopsy size is between 5 mm & 10 mm, decision to slice or not depends on individual case. If uncertain, this is to be discussed with the supervising consultant.
4 General Instructions All small biopsies are submitted in mesh bags to prevent loss of tissue Measurements are in three dimensions; length(l), width(w) and depth(d) Type of lesion should be described (e.g. nodule, macule) etc. For dysplastic naevus size of lesion, pigmentation (uniform or variable), type of lesion (macule, nodule or nodule in macule), borders(regular/irregular). For blistering disease presence or absence of blister.
5 General Instructions Lesion should be described as centrally located or peripheral towards any one edge. Measurement of the lesion is made. The nearest resection margins whether involved or clear should be recorded macroscopically Best practice suggests inking the surgical margins of specimens. This is more relevant to all neoplastic skins in general and particularly when there is clinical query of atypia or malignancy. Inking of margins also helps orientation during embedding and when sections are cut, helps in obtaining full-face sections.
6 General Instructions *If no obvious lesion, describe skin surface If specimen is orientated with one suture, indicate what margin the suture indicates. The suture usually is indicated or taken to represent the 12 o clock margin unless stated otherwise (to represent some other margin).
7 General Instructions The o clock resection margin is inked (inclusive of the deep margin on this half of specimen) & the o clock margin is either left un-inked or a different colour is used. The specimen is then sliced serially from 12 to 6 o clock position & tissue submitted maintaining the sequence/order of slices.
8 General Instructions If two sutures are present. Comment indicating the margins these represent. Process as explained above and additionally mention in which cassette the section corresponding to the second suture margin is submitted, to enable accurate assessment and specific comment of this margin (which often the clinician is concerned about).
9 General Instructions The no. of fragments placed in each cassette should be documented. This should be double checked when reporting to ensure that all fragments submitted are examined. This can sometimes also be helpful in detecting mislabelling or when cases get mixed up If order of slices obtained are to be maintained, either this is submitted one section per cassette or up to a maximum of two slices in sequential order (agar can be used for denoting the sequence of order).
10 General Instructions If polar margins are included for microscopy, it is advisable that the section does not include lesional tissue, so that it does not necessitate request for levels through the block to accurately assess the margins. This will sometimes render fairly small pieces of polar margins (especially if lesion is close to this margin) but this should not be too small that there is a risk of loss of tissue. Both polar margins can be submitted in one cassette if the specimen is not orientated.
11 General Instructions If dealing with orientated specimens, they can be submitted with the next section in sequential order or separately in sequence. It is useful at this point to remember that the more the number of tissues in a cassette, the more difficult it is to ensure that all the fragments are well orientated at embedding. Also mixtures of small and larger pieces makes it more difficult to obtain full-face sections of all pieces without cutting in too deep and hence risking cutting out of smaller fragments.
12 General Instructions It should be documented if all tissue has been taken (all taken AT, only representative sections sampled RST, all lesional tissue sampled but tissue remaining ALTS) Documentation if tissue stored or no tissue stored/empty (TS or E) If there is any doubt in dealing with the specimen, it is best to seek help from the supervising consultant or if no consultants are available (e.g. at a departmental meeting), the specimen should be left aside to be dealt with later when help is available.
13 General Instructions Remember that once a tissue is cut-up suboptimally it is very difficult to salvage the specimen & usually this causes difficulties at reporting (either diagnostically or in providing prognostic parameters e.g. clearance margins).
14 General Instructions Microscopy should always include comments on margins irrespective of type of biopsy (margins expected to be involved or not!). Stating completeness or incompleteness of excision implies intent and may not be relevant to all sample types. It may be preferable to simply state if the margin is involved or clear, whereby this represents a factual finding.
15 General Instructions This information is often useful, more so, if lesion recurs at surgical site e.g. in context of a recurrent naevus. Sometimes the type of biopsy may not reflect the clinician s expectation e.g. punch excision for small lesions.

16 Punch Biopsy
17 Punch Biopsy These are usually done for diagnostic purposes of neoplasia and inflammatory skin diseases. Occasionally these serve therapeutic removal of a small lesion (punch excision) The punch biopsies vary in diameter usually ranging between 3 and 5 mm. The specimen is measured in two dimensions: diameter and depth. All punch biopsies should be submitted in mesh bags to prevent loss of tissue. These are submitted intact.
18 Punch Biopsy Punch biopsies ideally should not be bisected unless the biopsy is greater than 5 mm diameter and the lesion is central, in which case care must be taken so that the specimen is bisected into two equal halves (which may be difficult to obtain!) and each submitted separately in two different cassettes. This may help to cut straight into the lesion without the necessity of trimming in deep, to get to the lesion (however the risk of poor tissue sections due to difficulty in bisecting the biopsy should be carefully considered first!).
19 Punch Biopsy Routinely most centres perform three automatic levels (saving spares for any special stains or immunocytochemistry later on if needed) for all punch biopsies The punch biopsies should be orientated on edge at the time of embedding to ensure that the plane of section is across all tissue layers (epidermis, dermis & subcutis) For neoplastic disease, margins should be commented although in most cases this is expected to be involved However, sometimes the punch is meant as a therapeutic tool with the aim of complete clearance of a small lesion.
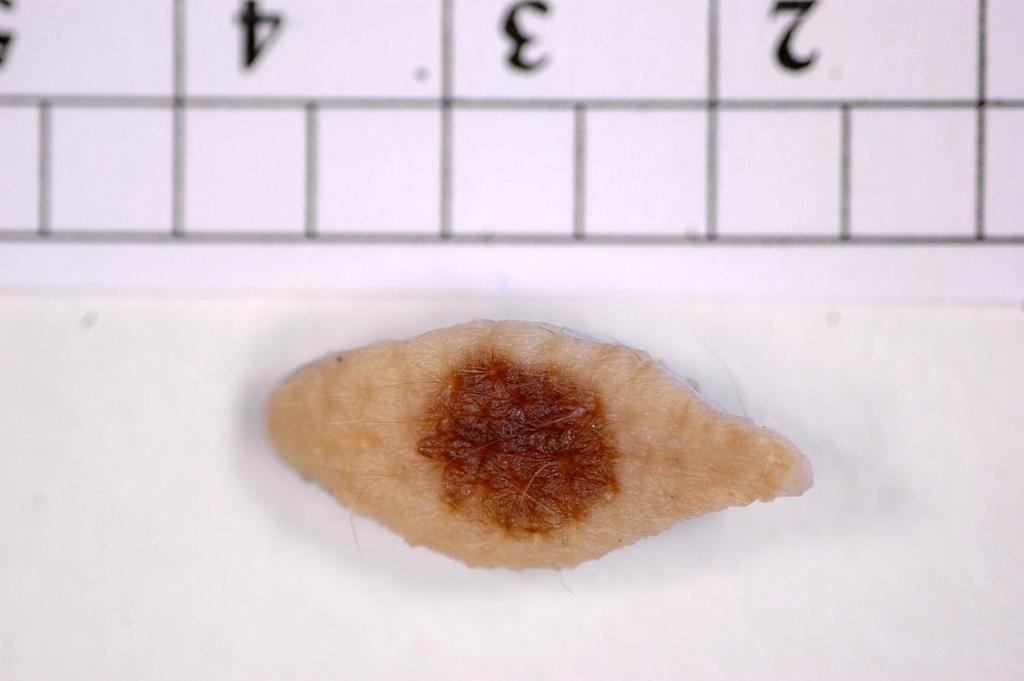
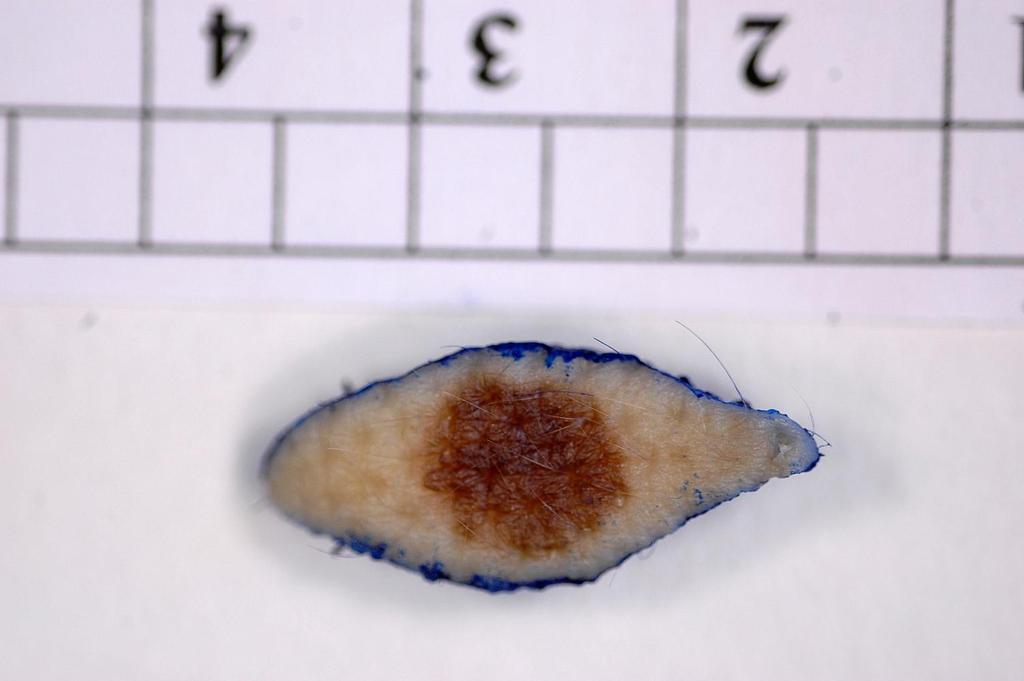
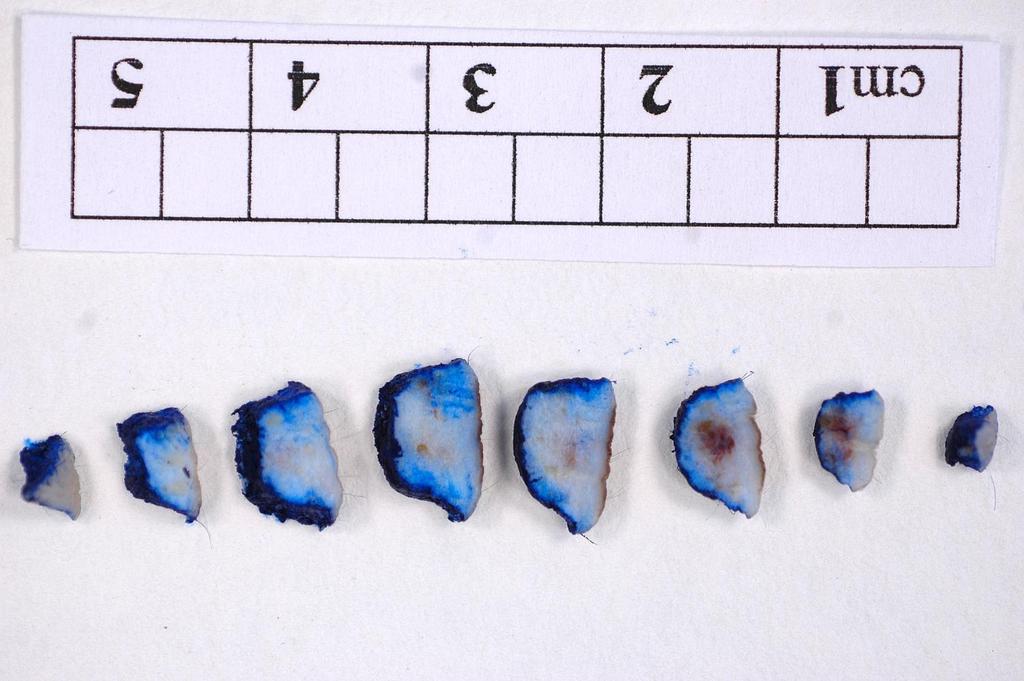
20 Shave Biopsy These are usually done either for confirmation/removal of a benign lesion or as a diagnostic biopsy for a suspected atypical or malignant lesion. The number (one, exact no. of fragments or multiple) and size of the biopsy (at least two dimensions and if possible in three dimensions) is noted. It is recommended to place the fragment/fragments in a mesh bag to prevent any loss of tissue. The shave biopsies are usually submitted intact.
21 Shave Biopsy Transversely slicing into one or more sections is recommended if the size of specimen is relatively big (length or width more than 10 mm) and of sufficient depth. If the specimens are thin, it is better to leave the specimen intact to enable better handling at time of embedding. At time of embedding, the specimens should be orientated on edge, so that the plane of section is through all tissue layers. Although the margins are usually involved, this should be documented in the microscopy.
22 Curettage The indications are similar as for shave biopsies This is done alone or in combination with cryo or cautery. This usually results in multiple fragments The number of fragments and size is documented Usually slicing is not possible and not necessary unless the specimen is relatively large (more than 10 mm).
23 Curettage It may be useful to select diagnostically relevant pieces of tissue if there are too many fragments In some cases, it may be helpful to separate the fragments more likely to be diagnostic and to submit the rest in another cassette (e.g. keratin) The fragments are all submitted intact in a mesh bag Although the margins are usually involved, this should be documented in the microscopy.
24 Incision Biopsy These are usually done for inflammatory skin diseases or as a diagnostic biopsy for neoplastic conditions These are usually ellipses of skin and therefore gross examination does not help in alerting the individual cutting-up that this is an incision biopsy, and therefore the importance of reading the request form carefully. * Inking is optional but usually useful
25 Incision Biopsy It is usually a single fragment that includes both the abnormal area and the adjacent normal skin. The specimen is measured and processed intact unless the specimen is too wide. In that case, the specimen can be sliced longitudinally to maintain the relationship of the normal skin to abnormal skin. If specimens are bisected longitudinally, it is preferable to place only one half in a cassette.
26 Incision Biopsy It is absolutely vital that incisional specimens especially in cases of inflammatory skins are not sliced transversely One peripheral margin is usually involved and this should be documented.
27 Excision Biopsy These are usually done for neoplastic skins including benign lesions (naevi, seborrhoeic keratosis), dysplastic conditions e.g. squamous actinic keratosis, dysplastic naevi and for malignancies (basal cell carcinomas, squamous cell carcinomas and malignant melanomas).
28 Excision Biopsy The specimen should be measured in three dimensions as recommended The presence or absence of a grossly discernible lesion should be documented. If lesion is present, this is described (size, colour, nature of lesion nodule, macule, vesicle etc.) If lesion is centrally located, this is very useful information to be included as this reflects the fact that the nearest margins are likely to be the circumferential peripheral margins and that the polar peripheral margins are probably uninvolved. *Perfectly reasonable to sample lesion only If lesion is not central i.e. peripherally located towards one edge of the biopsy, this should also be mentioned.
29 Not Orientated

30 Not Orientated
31 Not Orientated
32 Not Orientated
33 Excision Biopsy If possible the nearest margins as appreciated grossly should be measured and documented If no lesion can be visualized, the appearance of the skin surface should be described e.g. nodular, keratotic or irregular If the whole skin appears normal, this should be mentioned. In these cases, it is important to examine the whole specimen by inking the margins and bread slicing the specimen from one end to the other and processing in entirety If the biopsy is too small and slicing is awkward or difficult, please submit intact after inking margins.
34 Excision Biopsy If specimen is orientated with one suture, indicate what margin the suture indicates. The suture usually indicates the 12 o clock margin unless otherwise stated to represent some other margin. The o clock resection margin is inked (inclusive of the deep margin on this half of specimen) & the o clock margin is either left un-inked or a different colour is used. The specimen is then sliced from 12 to 6 o clock position & tissue submitted maintaining the sequence/order of slices. * Vertical vs. horizontal ellipse and disc of skin

35 One Suture

36 One Suture

37 One Suture

38 One Suture

39 One Suture
40 Excision Biopsy If two sutures are present. Comment indicating the margins these represent. Process as explained above and additionally mention in which cassette the second suture margin is submitted to enable accurate assessment and specific comment of this margin during microscopy (which often the clinician is concerned about!) The alignment is maintained preferably by submitting each piece in one cassette in sequential order or if using agar to indicate sequence, up to no more than two sections in one cassette.
41 Excision Biopsy If the specimen is large (dinner-plate type), it is advisable to do a thorough gross examination so as to enable selective sampling. Two different inks can be used as recommended previously. However, in centres dealing with a large number of plastic surgery excisions, 4 different inks are commonly used to indicate the 4 quadrants for easy reference and orientation. * Jumbo blocks
42 Excision Biopsy Sampling can be limited to examination of the tumour and the nearest margins. For the former, representative sections of the tumour (often large) is sampled. For the latter, cruciate blocks including tumour and the nearest margins are recommended (often this can be fairly well appreciated grossly). Documentation of sampled sections and margins are very important to assist microscopic examination and reporting.
43 Excision Biopsy Correct orientation at embedding is relatively easy as this is embedded with the cut surface down margins. Microscopy should include clearance
44 Wide excision/re-excision This is usually done either to ensure complete clearance of a tumour which involved the surgical margins or in cases where the surgical margins were clear in the primary excision, this is done to ensure the amount of clearance is in-line with the British Association of Dermatologists guidelines advocated or as per management decision made at the skin cancer MDT.
45 Wide Excision/Re-excision Measure specimen, ink margins Comment on scar if present and measure this Comment if any other lesion or residual lesion present These are usually dealt with as for an excision specimen by bread-slicing and submitting all tissue, maintaining the sections in sequence.
46 Wide Excision/Re-excision In case of melanoma re-excisions, if the original report indicates involvement of margins, the specimen should all be processed as described above. In cases where the primary biopsy records clear margins but the wide-excision is advocated for adherence to recommended margin of clearance, one section from the middle, incorporating the scar may suffice but more blocks may be taken according to individual preferences. In this case, knowledge of the previous histology report and the clearance margins would be relevant. (*Audit)

47 Dog-Ear Specimen

48 Dog-Ear Specimen
49 Dog-Ear Specimens The British Society of Dermatological Surgery guidelines definition states: Dog ears are redundant tissue at the end of an excision line. The redundant tissue is tented with a skin hook and either divided along the roof into two triangles which are then excised, or pulled to one side and the base divided on one side then the other (giving one piece of tissue). These represent the untidy excess of skin which is excised to enable cosmetically acceptable apposition of margins after excision of lesions They are common in the following situations: Sides of excision are unequal lengths Broad ellipse or circular defect
50 Dog-Ear Specimens Altered skin elasticity Convex surface e.g. forearm Often these are not of any clinical concern but sometimes there is a genuine concern in these specimens especially if lesional tissue is thought to be present. Sometimes this incidentally displays presence of tumour or other significant pathological changes. These therefore have to be processed for examination Simple general rules of dealing with specimen include -
51 Dog-Ear Specimens Measuring the specimen and processing all tissue If tissue is small, submit intact However, usually the specimen needs bisecting/trisecting for proper orientation at embedding Sometimes the margin of concern is expressed and this may be sent inked. In that case, handling of this specimen is dependant of the margin of concern and assessed on an individual basis.
52 Direct Immunofluorescence Usually two specimens are sent; one for histology and the other DIF The one for histology will be sent in formalin as usual and dealt with as explained above If this is for a blistering disorder, submit intact The other specimen for DIF will be sent in saline soaked gauze/saline/mitchel s medium This is sent to lab to be kept frozen and handled as per the DIF specimen standard operating procedure (SOP).
53 Electron Microscopy Usually two specimens are sent, one for histology and the other for EM The one for histology is sent in formalin and handled appropriately The one for EM should be sent in Glutaraldehyde but this is often not available in minor surgery units and Gluteraldehyde can also cause severe allergic contact dermatitis in susceptible individuals. Therefore these specimens are often sent in formalin or soaked in saline.
54 Electron Microscopy Formalin as media of transport does not alter the cytological/nuclear details too much to hinder in the EM interpretation but this should be limited to only a short period. Formalin is preferred over saline soaked gauze as the latter can dry out tissue if left unattended. As soon as received in the lab, these specimens need to be transferred in Glutaraldehyde and sent to EM unit for processing.
55 MOHs MOHs surgical excision technique has been developed to excise neoplastic lesions (particularly basal cell carcinomas) with as little surrounding normal tissue as possible. In theory, MMS should enable the physician to successfully excise all cutaneous tumours that are contiguous. The limitation of the procedure revolves around the ability of the surgeon to accurately identify neoplastic cells by frozen section and the difficulty of the MOHs technician to consistently prepare sections that are histologically complete without distracting artefact. The lesion is often curetted first and then a series of shave excisions is undertaken, with frozen sections being assessed to determine clearance at each stage.
56 MOHs The frozen sections are routinely interpreted by the MOHs surgeon who is usually a Dermatologist trained to perform the procedure and to interpret the histopathology. The MOHs surgeon usually prefers toluidine blue stain to haematoloxylin and eosin for their histology interpretation. Uncommonly, if there is difficulty with interpretation the MOHs surgeon may seek help directly or via the BMS for help in the histological interpretation.
57 MOHs When interpretation is complete, the frozen specimens are then transferred to formalin for fixation and subsequently processed in the normal way. The paraffin sections are then used to confirm the frozen section findings. Thus, the main laboratory usually receives a series of formalin processed, (previously frozen) sections, the residual tissue from each of the shave excisions and residual curetted tissue.
58 MOHs Each shave excision biopsy should be measured (preferably in three dimensions) and then placed intact into the tissue cassette with its cut surface (marked with blue ink) face downwards. Sandwiching the tissue between pieces of foam helps to ensure that the cut face is as flat as possible for embedding.
59 MOHs Minimal curettings are usually received. The tissue should be described with an indication of the size/amount of tissue present (see 6.4). The entire specimen should be submitted for processing in a mesh bag.
60 Thank you for listening I would like to express my gratitude to: Ms. Susan Cossins Ms. Louisa Millward Ms. Cathryn Leng
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
TISSUE PATHWAYS FOR INFLAMMATORY AND NON-NEOPLASTIC DERMATOSES AND NON-NEOPLASTIC LESIONS
 The Royal College of Pathologists Pathology: the science behind the cure TISSUE PATHWAYS FOR INFLAMMATORY AND NON-NEOPLASTIC DERMATOSES AND NON-NEOPLASTIC LESIONS September 2008 Unique document number
The Royal College of Pathologists Pathology: the science behind the cure TISSUE PATHWAYS FOR INFLAMMATORY AND NON-NEOPLASTIC DERMATOSES AND NON-NEOPLASTIC LESIONS September 2008 Unique document number
What is melanoma? Melanoma dealing with the diagnosis. What is melanoma?
 Melanoma is a form of cancer which develops from that part of the skin which produces its colour. It grows from the cell which produces the brown pigment in our skin: the melanocyte. Often the melanoma
Melanoma is a form of cancer which develops from that part of the skin which produces its colour. It grows from the cell which produces the brown pigment in our skin: the melanocyte. Often the melanoma
ANATOMICAL PATHOLOGY TARIFF
 ANATOMICAL PATHOLOGY TARIFF A GUIDE TO UTILISATION. The following guidelines have been agreed by consensus of Anatomical Pathologists who are members of the Anatomical Pathologist s Group, or the National
ANATOMICAL PATHOLOGY TARIFF A GUIDE TO UTILISATION. The following guidelines have been agreed by consensus of Anatomical Pathologists who are members of the Anatomical Pathologist s Group, or the National
Benign vs. Cancer. Oculofacial Biopsy. Evolution of skin cancer. Richard E. Castillo, OD, DO
 Oculofacial Biopsy Richard E. Castillo, OD, DO Benign vs. Cancer Evolution of skin cancer Metaplasia Dysplasia Carcinoma-in-situ Invasive carcinoma Intravasation Overview Preoperative Planning Choosing
Oculofacial Biopsy Richard E. Castillo, OD, DO Benign vs. Cancer Evolution of skin cancer Metaplasia Dysplasia Carcinoma-in-situ Invasive carcinoma Intravasation Overview Preoperative Planning Choosing
Periocular skin cancer
 Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
Glenn D. Goldman, MD. Fletcher Allen Health Care. University of Vermont College of Medicine
 Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Basics of Skin Biopsy Techniques
 Basics of Skin Biopsy Techniques Kelly Quinn, D.O. Lehigh Valley Health Network/PCOM Department of Dermatology Osteopathic Medical Conference and Exposition October 7, 2017 None to disclose Conflicts of
Basics of Skin Biopsy Techniques Kelly Quinn, D.O. Lehigh Valley Health Network/PCOM Department of Dermatology Osteopathic Medical Conference and Exposition October 7, 2017 None to disclose Conflicts of
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW
 MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
Skin biopsy. Sophia Otto SA Pathology
 Skin biopsy Sophia Otto SA Pathology RCPA (Royal College of Pathologists of Australasia) The RCPA is the leading organisation representing pathologists in Australasia. Its mission is to train and support
Skin biopsy Sophia Otto SA Pathology RCPA (Royal College of Pathologists of Australasia) The RCPA is the leading organisation representing pathologists in Australasia. Its mission is to train and support
MOHS MICROGRAPHIC SURGERY
 MOHS MICROGRAPHIC SURGERY What are the aims of this leaflet? This leaflet has been written to help you understand more about Mohs micrographic surgery. It tells you what it is, what is involved and what
MOHS MICROGRAPHIC SURGERY What are the aims of this leaflet? This leaflet has been written to help you understand more about Mohs micrographic surgery. It tells you what it is, what is involved and what
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
CUT-UP PROTOCOL Foreskin SCC, Glansectomy, and Penectomy BASIC ANATOMY
 BASIC ANATOMY Orientating the specimen is essential. The urethra runs within the corpus spongiosum which expands to form the glans. The frenulum of the foreskin is on the ventral aspect. DORSAL Proximal
BASIC ANATOMY Orientating the specimen is essential. The urethra runs within the corpus spongiosum which expands to form the glans. The frenulum of the foreskin is on the ventral aspect. DORSAL Proximal
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Audit of plastic surgeons understanding of pathology reports of skin neoplasia
 The British Association of Plastic Surgeons (2004) 57, 134 138 Audit of plastic surgeons understanding of pathology reports of skin neoplasia Y.S. Lau a, S.K. Suvarna b, *, L. Kangesu a, A. Mosahebi a
The British Association of Plastic Surgeons (2004) 57, 134 138 Audit of plastic surgeons understanding of pathology reports of skin neoplasia Y.S. Lau a, S.K. Suvarna b, *, L. Kangesu a, A. Mosahebi a
Mohs. Micrographic Surgery. For Treating Skin Cancer
 Mohs Micrographic Surgery For Treating Skin Cancer Skin Cancer Basics Skin cancer is common. Over the past three decades, more people have had skin cancer than all other cancers combined. Each year in
Mohs Micrographic Surgery For Treating Skin Cancer Skin Cancer Basics Skin cancer is common. Over the past three decades, more people have had skin cancer than all other cancers combined. Each year in
Handout for Dr Allison s Lectures on Grossing Breast Specimens:
 Handout for Dr Allison s Lectures on Grossing Breast Specimens: Dr. Kimberly H. Allison Director of Breast Pathology and Breast Pathology Fellowship Director of Residency Training in Pathology Stanford
Handout for Dr Allison s Lectures on Grossing Breast Specimens: Dr. Kimberly H. Allison Director of Breast Pathology and Breast Pathology Fellowship Director of Residency Training in Pathology Stanford
Frequently Asked Questions
 Ida Orengo, M.D. Mohsin Mir, M.D. Department of Dermatology 1977 Butler Boulevard, Suite E6.200 Houston, TX 77030 (713) 798-6925 / (713) 798-6624 telephone (713) 798-5535 fax Frequently Asked Questions
Ida Orengo, M.D. Mohsin Mir, M.D. Department of Dermatology 1977 Butler Boulevard, Suite E6.200 Houston, TX 77030 (713) 798-6925 / (713) 798-6624 telephone (713) 798-5535 fax Frequently Asked Questions
MELANOMA. Some people are more likely to get a m Melanoma than others:
 MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
Frozen section control of excision of eyelid basal cell carcinomas: 81/2 years' experience
 British Journal of Ophthalmology, 1989, 73, 328-332 Frozen section control of excision of eyelid basal cell carcinomas: 81/2 years' experience HELENA J FRANK From the Royal Victoria Hospital, Bournemouth
British Journal of Ophthalmology, 1989, 73, 328-332 Frozen section control of excision of eyelid basal cell carcinomas: 81/2 years' experience HELENA J FRANK From the Royal Victoria Hospital, Bournemouth
Technicians & Nurses Program
 ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
SURGICAL PATHOLOGY - HISTOLOGY
 SURGICAL PATHOLOGY - HISTOLOGY Request Forms The following information is required on the Anatomic Pathology Request form in General Information in all instances: Patient s full name Room number Medical
SURGICAL PATHOLOGY - HISTOLOGY Request Forms The following information is required on the Anatomic Pathology Request form in General Information in all instances: Patient s full name Room number Medical
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
You Were Audited for What? Tales From the Trenches
 You Were Audited for What? Tales From the Trenches Howard W. Rogers M.D., Ph.D. Advanced Dermatology Norwich, CT rogershoward@sbcglobal.net Conflict of Interest Statement I have no relevant financial conflicts
You Were Audited for What? Tales From the Trenches Howard W. Rogers M.D., Ph.D. Advanced Dermatology Norwich, CT rogershoward@sbcglobal.net Conflict of Interest Statement I have no relevant financial conflicts
MOHS MICROGRAPHIC SURGERY
 MOHS MICROGRAPHIC SURGERY The Treatment of Skin Cancer What is Mohs Micrographic Surgery? Mohs Micrographic surgery is a specialized, highly effective technique used to treat skin cancer. The goal of Mohs
MOHS MICROGRAPHIC SURGERY The Treatment of Skin Cancer What is Mohs Micrographic Surgery? Mohs Micrographic surgery is a specialized, highly effective technique used to treat skin cancer. The goal of Mohs
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
SKIN SERVICES REVIEW Changes to Medicare Benefits Schedule for 1 November 2016
 Attachment A SKIN SERVICES REVIEW Changes to Medicare Benefits Schedule for 1 November 2016 Deleted items 31200-31215, 31230-31240 31255-31335 Colour Coding for new / updated items: MUCOSAL BIOPSY AND
Attachment A SKIN SERVICES REVIEW Changes to Medicare Benefits Schedule for 1 November 2016 Deleted items 31200-31215, 31230-31240 31255-31335 Colour Coding for new / updated items: MUCOSAL BIOPSY AND
Skin lesions suspicious for melanoma: New Zealand excision margin guidelines in practice
 Skin lesions suspicious for melanoma: excision margin guidelines in practice Tess Brian MBBS; 1 Michael B. Jameson MBChB, FRACP, FRCP, PhD 2,3 1 Department of Plastic and Reconstructive Surgery, Waikato
Skin lesions suspicious for melanoma: excision margin guidelines in practice Tess Brian MBBS; 1 Michael B. Jameson MBChB, FRACP, FRCP, PhD 2,3 1 Department of Plastic and Reconstructive Surgery, Waikato
MING H. JIH, MD,PHD, PAUL M. FRIEDMAN, MD,LEONARD H. GOLDBERG, MD,AND ARASH KIMYAI-ASADI, MD. Methods Phase I: Retrospective (Group 1)
") Curettage prior to Mohs Micrographic Surgery for Previously Biopsied Nonmelanoma Skin Cancers: What Are We Curetting? Retrospective, Prospective, and Comparative Study MING H. JIH, MD,PHD, PAUL M. FRIEDMAN,
Curettage prior to Mohs Micrographic Surgery for Previously Biopsied Nonmelanoma Skin Cancers: What Are We Curetting? Retrospective, Prospective, and Comparative Study MING H. JIH, MD,PHD, PAUL M. FRIEDMAN,
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Contributions to Anatomic Pathology, over the years
 Contributions to Anatomic Pathology, over the years Anatomic Pathology, part 1 G.B. Morgagni Xavier Bichat Rudolf Wirchow Anatomic Pathology, part 1 Anatomic pathology materials: morphological samples
Contributions to Anatomic Pathology, over the years Anatomic Pathology, part 1 G.B. Morgagni Xavier Bichat Rudolf Wirchow Anatomic Pathology, part 1 Anatomic pathology materials: morphological samples
LYMPH NODE: BIOPSY Guideline & Procedure: Lymph Node Biopsy
 LYMPH NODE: BIOPSY Guideline & Procedure: Lymph Node Biopsy (Discuss with hematopathology attending for lymphoma work up case prior to proceed to gross at LBJ) 1. Measure the specimen (three dimensions).
LYMPH NODE: BIOPSY Guideline & Procedure: Lymph Node Biopsy (Discuss with hematopathology attending for lymphoma work up case prior to proceed to gross at LBJ) 1. Measure the specimen (three dimensions).
Skin lesions The Good and the Bad. Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry
 Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
Malignant Melanoma Care Pathway
 Malignant Melanoma Care Pathway Level 1-4 Community Skin Cancer Service Sussex Community Dermatology Service Version 3.0 Scope of Community Services for Malignant Melanoma All suspected cases of malignant
Malignant Melanoma Care Pathway Level 1-4 Community Skin Cancer Service Sussex Community Dermatology Service Version 3.0 Scope of Community Services for Malignant Melanoma All suspected cases of malignant
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Alcohol should be avoided for 3 days prior to surgery and 2 days after the procedure.
 Mohs Surgery Information Packet Be sure to bring the following to your appointment: Insurance Card Insurance Referral ( If required by your insurance) Name and address of your primary care provider as
Mohs Surgery Information Packet Be sure to bring the following to your appointment: Insurance Card Insurance Referral ( If required by your insurance) Name and address of your primary care provider as
Policy #: 127 Latest Review Date: June 2011
 Name of Policy: Mohs Micrographic Surgery Policy #: 127 Latest Review Date: June 2011 Category: Surgery Policy Grade: Active Policy but no longer scheduled for regular literature reviews and updates. Background/Definitions:
Name of Policy: Mohs Micrographic Surgery Policy #: 127 Latest Review Date: June 2011 Category: Surgery Policy Grade: Active Policy but no longer scheduled for regular literature reviews and updates. Background/Definitions:
Proposal for a 2-stage RCT in high risk primary SCC: COMMISSAR Catherine Harwood Barts Health NHS Trust / QMUL
 Proposal for a 2-stage RCT in high risk primary SCC: COMMISSAR Catherine Harwood Barts Health NHS Trust / QMUL on behalf of Dr Louise Lansbury, Prof Fiona Bath-Hextall Nottingham Centre for Evidence Based
Proposal for a 2-stage RCT in high risk primary SCC: COMMISSAR Catherine Harwood Barts Health NHS Trust / QMUL on behalf of Dr Louise Lansbury, Prof Fiona Bath-Hextall Nottingham Centre for Evidence Based
Dermatology Procedure Coding
 Dermatology Procedure Coding Anatomy Two layers that make up human skin Epidermis most superficial layer Composed of four to five layers called stratum Anyone remember the mnemonic? Thickness varies based
Dermatology Procedure Coding Anatomy Two layers that make up human skin Epidermis most superficial layer Composed of four to five layers called stratum Anyone remember the mnemonic? Thickness varies based
Mohs surgery. Information for patients Dermatology
 Mohs surgery Information for patients Dermatology Why have I been given this leaflet? You have been given this leaflet because you are going to have a procedure known as Mohs surgery. This leaflet explains
Mohs surgery Information for patients Dermatology Why have I been given this leaflet? You have been given this leaflet because you are going to have a procedure known as Mohs surgery. This leaflet explains
SQUAMOUS CELL CARCINOMA
 SQUAMOUS CELL CARCINOMA What are the aims of this leaflet? This leaflet has been written to help you understand more about squamous cell carcinomas of the skin. It tells you what they are, what causes
SQUAMOUS CELL CARCINOMA What are the aims of this leaflet? This leaflet has been written to help you understand more about squamous cell carcinomas of the skin. It tells you what they are, what causes
MELANOMA. 4 Fitzroy Square, London W1T 5HQ Tel: Fax: Registered Charity No.
 MELANOMA This leaflet had been written to help you understand more about melanoma. It tells you what it is, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet had been written to help you understand more about melanoma. It tells you what it is, what causes it, what can be done about it, how it can be prevented, and where you can find out
UWMC Roosevelt Clinic Rotation Goals 2011 Procedural Dermatology Fellowship Program 1
 Procedural Dermatology Fellowship Objectives University of Washington Medical Center-Roosevelt Rotation The primary goal of the University of Washington rotation of the Procedural Dermatology fellowship
Procedural Dermatology Fellowship Objectives University of Washington Medical Center-Roosevelt Rotation The primary goal of the University of Washington rotation of the Procedural Dermatology fellowship
For additional information on meeting the criteria for Mohs, see Appendix 2.
 Position Statement on Appropriate Uses of Paraffin Sections in Association (Approved by the Board of Directors: August 1, 2011; Revised November 5, 2011; Revised August 9, 2014) According to AMA/CPT, Mohs
Position Statement on Appropriate Uses of Paraffin Sections in Association (Approved by the Board of Directors: August 1, 2011; Revised November 5, 2011; Revised August 9, 2014) According to AMA/CPT, Mohs
Small diagnostic biopsies Handling and reporting issues. Dr Varsha Shah Consultant Histopathologist Royal Gwent Hospital Newport
 Small diagnostic biopsies Handling and reporting issues Dr Varsha Shah Consultant Histopathologist Royal Gwent Hospital Newport RCPath 2017 Biopsy vs. resection specimens Smaller Tissues: Larger Issues
Small diagnostic biopsies Handling and reporting issues Dr Varsha Shah Consultant Histopathologist Royal Gwent Hospital Newport RCPath 2017 Biopsy vs. resection specimens Smaller Tissues: Larger Issues
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT
 Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Moh's Surgery Information Packet
 Moh's Surgery Information Packet BE SURE TO BRING THE FOLLOWING TO YOUR APPOINTMENT Insurance card Insurance referral (if required by your insurance) Name and address of your primary care provider as well
Moh's Surgery Information Packet BE SURE TO BRING THE FOLLOWING TO YOUR APPOINTMENT Insurance card Insurance referral (if required by your insurance) Name and address of your primary care provider as well
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Evaluation of Breast Specimens Removed by Needle Localization Technique
 Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
How to decipher a pathology report for alopecia
 How to decipher a pathology report for alopecia DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Lynne J. Goldberg, MD S063-Hair Disorders Made Easier DISCLOSURES I do not have any relationships with industry
How to decipher a pathology report for alopecia DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Lynne J. Goldberg, MD S063-Hair Disorders Made Easier DISCLOSURES I do not have any relationships with industry
Chapter 11 Worksheet Code It
 Class: Date: Chapter 11 Worksheet 3 2 1 Code It True/False Indicate whether the statement is true or false. 1. Surgical destruction is considered part of the surgical procedure description. 2. Prepping
Class: Date: Chapter 11 Worksheet 3 2 1 Code It True/False Indicate whether the statement is true or false. 1. Surgical destruction is considered part of the surgical procedure description. 2. Prepping
Skin Cancer and Mohs Micrographic Surgery Patient Education
 Patient Care Services 300 Pasteur Drive Stanford, CA 94305 Skin Cancer and Mohs Micrographic Surgery Patient Education Skin Cancer How Common is Skin Cancer? Skin cancer is the most common form of cancer
Patient Care Services 300 Pasteur Drive Stanford, CA 94305 Skin Cancer and Mohs Micrographic Surgery Patient Education Skin Cancer How Common is Skin Cancer? Skin cancer is the most common form of cancer
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Destruction or Excision: What's Happening in Your Dermatology Office?
 Questions Destruction or Excision: What's Happening in Your Dermatology Office? Answers Webinar Subscription Access Expires December 31. Doc excises a "pendunculated gluteal mass" with a fullthickness
Questions Destruction or Excision: What's Happening in Your Dermatology Office? Answers Webinar Subscription Access Expires December 31. Doc excises a "pendunculated gluteal mass" with a fullthickness
Skin Cancer A Personal Approach. Dr Matthew Strack Dunedin New Zealand
 Skin Cancer A Personal Approach Dr Matthew Strack Dunedin New Zealand Outline Dermoscopy Instruments and setup Photochemosurgery Clinical Aim: Leave with 2-3 ideas JLE Benign Junctional Nevus Management
Skin Cancer A Personal Approach Dr Matthew Strack Dunedin New Zealand Outline Dermoscopy Instruments and setup Photochemosurgery Clinical Aim: Leave with 2-3 ideas JLE Benign Junctional Nevus Management
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: mohs_micrographic_surgery 07/2004 11/2017 11/2018 11/2017 Description of Procedure or Service Mohs Micrographic
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: mohs_micrographic_surgery 07/2004 11/2017 11/2018 11/2017 Description of Procedure or Service Mohs Micrographic
Mohs Micrographic Surgery
 Mohs Micrographic Surgery Mohs Clinics Dordrecht Spuiboulevard 226 3311 GR Dordrecht T: +31 (0)78 632 10 80 F: +31 (0)78 632 10 81 E: contact@mohsklinieken.nl Mohs Clinics Amsterdam Zwaansvliet 5 1080
Mohs Micrographic Surgery Mohs Clinics Dordrecht Spuiboulevard 226 3311 GR Dordrecht T: +31 (0)78 632 10 80 F: +31 (0)78 632 10 81 E: contact@mohsklinieken.nl Mohs Clinics Amsterdam Zwaansvliet 5 1080
(SCARD) At any time to clarify any issues you can contact us by on
 At any time to clarify any issues you can contact us by on") The SCCANZ Skin Cancer Audit and Research Database (SCARD) TO USE THE PROGRAM At any time to clarify any issues you can contact us by email on support@skincanceraudit.com The Notice Board on the home-page
The SCCANZ Skin Cancer Audit and Research Database (SCARD) TO USE THE PROGRAM At any time to clarify any issues you can contact us by email on support@skincanceraudit.com The Notice Board on the home-page
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
PATIENT INFORMATION. Mohs Micrographic Surgery. In the Treatment of Skin Cancer
 PATIENT INFORMATION Mohs Micrographic Surgery In the Treatment of Skin Cancer What is Mohs Micrographic Surgery? Mohs micrographic surgery is a specialized, highly effective technique for the removal
PATIENT INFORMATION Mohs Micrographic Surgery In the Treatment of Skin Cancer What is Mohs Micrographic Surgery? Mohs micrographic surgery is a specialized, highly effective technique for the removal
The Role of Mohs Micrographic Surgery in Skin Cancer Treatment
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/the-role-of-mohs-micrographic-surgery-in-skincancer-treatment/3643/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/the-role-of-mohs-micrographic-surgery-in-skincancer-treatment/3643/
Melanoma. Consultation on draft guideline - stakeholder comments. Comments to be submitted before 5pm on Friday 13 March 2015
 Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Mohs Micrographic Surgery
 Mohs Micrographic Surgery Patient Information Dermatology Department The aim of this leaflet is to give you information about Mohs Micrographic Surgery. What is Mohs Surgery? Mohs surgery is a specialised,
Mohs Micrographic Surgery Patient Information Dermatology Department The aim of this leaflet is to give you information about Mohs Micrographic Surgery. What is Mohs Surgery? Mohs surgery is a specialised,
Eyelid basal cell carcinoma Patient information
 Eyelid basal cell carcinoma Patient information Your procedure relates to the face, eyelids, orbit or tear drainage system that together are treated by specialist surgeons in the field of oculoplastic
Eyelid basal cell carcinoma Patient information Your procedure relates to the face, eyelids, orbit or tear drainage system that together are treated by specialist surgeons in the field of oculoplastic
Skin SSG (Anglia East & Anglia West)
") Skin SSG (Anglia East & Anglia West) Author: Dr Jennifer Garioch, Consultant Dermatologist Dr Pamela Todd, Consultant Dermatologist Approved by: Anglia Cancer Network Skin NSSG Approved on: Reviewed and
Skin SSG (Anglia East & Anglia West) Author: Dr Jennifer Garioch, Consultant Dermatologist Dr Pamela Todd, Consultant Dermatologist Approved by: Anglia Cancer Network Skin NSSG Approved on: Reviewed and
CONSULTATION DURING SURGERY / NOT A FINAL DIAGNOSIS. FROZEN SECTION DIAGNOSIS: - A. High grade sarcoma. Wait for paraffin sections results.
 Pathology Report Date: 3/5/02 A, B. Biopsy right distal femur- high grade spindle cell sarcoma Immunohistochemistry studies are pending to further classify the nature of the tumor. CONSULTATION DURING
Pathology Report Date: 3/5/02 A, B. Biopsy right distal femur- high grade spindle cell sarcoma Immunohistochemistry studies are pending to further classify the nature of the tumor. CONSULTATION DURING
Diagnostics guidance Published: 11 November 2015 nice.org.uk/guidance/dg19
 VivaScope 1500 and 3000 imaging systems for detecting skin cancer lesions Diagnostics guidance Published: 11 November 2015 nice.org.uk/guidance/dg19 NICE 2018. All rights reserved. Subject to Notice of
VivaScope 1500 and 3000 imaging systems for detecting skin cancer lesions Diagnostics guidance Published: 11 November 2015 nice.org.uk/guidance/dg19 NICE 2018. All rights reserved. Subject to Notice of
Common Benign Lesions and Skin Cancers. 22nd May 2015 Dr Mark Foley
 Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Image guided core biopsies:
 Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
BREAST PATHOLOGY GROSSING GUIDELINES
 THINGS TO CONSIDER: A. Please review ALL imaging and previous biopsies PRIOR to grossing any breast case. a. It may be helpful to draw out your own guide to assist when grossing B. Faxitron your breast
THINGS TO CONSIDER: A. Please review ALL imaging and previous biopsies PRIOR to grossing any breast case. a. It may be helpful to draw out your own guide to assist when grossing B. Faxitron your breast
Patient information factsheet
 Patient information factsheet Surgery for eyelid cancers What are the aims of surgery? The priority is to completely remove the cancer. Most skin cancers have roots that spread beyond the visible limit
Patient information factsheet Surgery for eyelid cancers What are the aims of surgery? The priority is to completely remove the cancer. Most skin cancers have roots that spread beyond the visible limit
Histopathological and SIAscopic Correlation of Pigmented Skin Lesions
 Histopathological and SIAscopic Correlation of Pigmented Skin Lesions Professor Sujatha Fernando MBBS(Hon), MSc(London, Distinction), FRSTM&H, FRCPA, FIAC, FACTM Senior Consultant in Anatomical Pathology,
Histopathological and SIAscopic Correlation of Pigmented Skin Lesions Professor Sujatha Fernando MBBS(Hon), MSc(London, Distinction), FRSTM&H, FRCPA, FIAC, FACTM Senior Consultant in Anatomical Pathology,
Minor Surgery. Using the Limbs & Things skin pads and jig. Skin Pad Jig Mk 3. Skin Pad Jig Strap. 44 Minor Surgery
 Using the Limbs & Things skin pads and jig The Skin Pad Jig can be used initially on a work surface for ease of learning, and can then be attached to the body of a fellow trainee to practise these skills,
Using the Limbs & Things skin pads and jig The Skin Pad Jig can be used initially on a work surface for ease of learning, and can then be attached to the body of a fellow trainee to practise these skills,
PanMidlands Ocular Cancer Pathway March 2008 Approved by The Midland Oculoplastic Surgery Society
 PanMidlands Ocular Cancer Pathway March 2008 Approved by The Midland Oculoplastic Surgery Society Periocular Skin Pathway Referrals to Oculoplastics Strong Indication: Lesion within orbital rim Medial
PanMidlands Ocular Cancer Pathway March 2008 Approved by The Midland Oculoplastic Surgery Society Periocular Skin Pathway Referrals to Oculoplastics Strong Indication: Lesion within orbital rim Medial
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Using the Mohs Technique for Thin Melanomas
 Dermatology Associates Mohs Micrographic Surgery 2300 W Stone Drive Kingsport TN 37660 Telephone 423-246-4961 1-800-445-7274 (VA Toll Free) Fax 423-245-1200 Using the Mohs Technique for Thin Melanomas
Dermatology Associates Mohs Micrographic Surgery 2300 W Stone Drive Kingsport TN 37660 Telephone 423-246-4961 1-800-445-7274 (VA Toll Free) Fax 423-245-1200 Using the Mohs Technique for Thin Melanomas
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee
 I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
What in the world is Histotechnology? Karen Stiffler, MA, HTL Program Director for Histotechnology
 What in the world is Histotechnology? Karen Stiffler, MA, HTL Program Director for Histotechnology The Basics of Histology Histology: the study of body tissues "histo" is from the Greek "histos" meaning
What in the world is Histotechnology? Karen Stiffler, MA, HTL Program Director for Histotechnology The Basics of Histology Histology: the study of body tissues "histo" is from the Greek "histos" meaning
A PATIENT S GUIDE to MOHS MICROGRAPHIC SURGERY
 A PATIENT S GUIDE to MOHS MICROGRAPHIC SURGERY Microscopically Controlled Surgery for Skin Cancer ALBUQUERQUE DERMATOLOGY ASSOCIATES, P.A. Sky B. Connolly, M.D. F.A.A.D A Checklist Before Surgery Please
A PATIENT S GUIDE to MOHS MICROGRAPHIC SURGERY Microscopically Controlled Surgery for Skin Cancer ALBUQUERQUE DERMATOLOGY ASSOCIATES, P.A. Sky B. Connolly, M.D. F.A.A.D A Checklist Before Surgery Please
29/06/1439 بسم ا هلل ا لرحمن ا لر حيم
 بسم ا هلل ا لرحمن ا لر حيم 1 LID RECONSTRUCTION by Ali M ISMAIL professor of ophthalmology @SOHAG U H Occuloplastic fellow @NNUH Occuloplastic fellow @Cambridge UH Honor fellow @ Mooorfield eye Hospital
بسم ا هلل ا لرحمن ا لر حيم 1 LID RECONSTRUCTION by Ali M ISMAIL professor of ophthalmology @SOHAG U H Occuloplastic fellow @NNUH Occuloplastic fellow @Cambridge UH Honor fellow @ Mooorfield eye Hospital
Histotechnological problems in dermatopathology and their possible consequences
 Histotechnological problems in dermatopathology and their possible consequences Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology University of Washington, Seattle,
Histotechnological problems in dermatopathology and their possible consequences Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology University of Washington, Seattle,
Skin Cancer. Dr Elizabeth Ogden Associate Specialist in Dermatology East and North Herts Dr Elizabeth Ogden
 Skin Cancer Dr Elizabeth Ogden Associate Specialist in Dermatology East and North Herts 13.10.16 Skin Cancer Melanoma mole cancer - is a true cancer which can metastasize and kill Non Melanoma skin cancer
Skin Cancer Dr Elizabeth Ogden Associate Specialist in Dermatology East and North Herts 13.10.16 Skin Cancer Melanoma mole cancer - is a true cancer which can metastasize and kill Non Melanoma skin cancer
University College Hospital. Mohs micrographic surgery. Dermatology Services
 University College Hospital Mohs micrographic surgery Dermatology Services 2 If you would like this document in another language or format, or require the services of an interpreter, please contact us
University College Hospital Mohs micrographic surgery Dermatology Services 2 If you would like this document in another language or format, or require the services of an interpreter, please contact us
Coding Wars: The Coding and Documentation Weapons to Win the Battle
 Coding Wars: The Coding and Documentation Weapons to Win the Battle Howard W. Rogers M.D., Ph.D. Advanced Dermatology Norwich, CT rogershoward@sbcglobal.net Conflict of Interest Statement I have no relevant
Coding Wars: The Coding and Documentation Weapons to Win the Battle Howard W. Rogers M.D., Ph.D. Advanced Dermatology Norwich, CT rogershoward@sbcglobal.net Conflict of Interest Statement I have no relevant
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
PREPARING FOR YOUR MOHS SURGERY
 Patient Education provided by Leslie Storey, MD Board Certified, Mohs Fellowship Trained, Dermatologist PREPARING FOR YOUR MOHS SURGERY 1 Your surgery date is: _ 2 Welcome...5 What is Mohs Surgery?...6
Patient Education provided by Leslie Storey, MD Board Certified, Mohs Fellowship Trained, Dermatologist PREPARING FOR YOUR MOHS SURGERY 1 Your surgery date is: _ 2 Welcome...5 What is Mohs Surgery?...6
PREPARING FOR YOUR MOHS SURGERY
 Patient Education provided by Leslie Storey, MD Board Certified, Mohs Fellowship Trained, Dermatologist PREPARING FOR YOUR MOHS SURGERY Welcome...5 Your surgery date is: What is Mohs Surgery?...6 When
Patient Education provided by Leslie Storey, MD Board Certified, Mohs Fellowship Trained, Dermatologist PREPARING FOR YOUR MOHS SURGERY Welcome...5 Your surgery date is: What is Mohs Surgery?...6 When
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Guideline for the Handling of Pathology Lung Tissue Specimens
 Guideline for the Handling of Pathology Lung Tissue Specimens Version Date Summary of Change/Process 0.1 29.06.11 Produced by Simon Trotter and circulated to Lung Network Site Specific Group for reviewing
Guideline for the Handling of Pathology Lung Tissue Specimens Version Date Summary of Change/Process 0.1 29.06.11 Produced by Simon Trotter and circulated to Lung Network Site Specific Group for reviewing
BASAL CELL CARCINOMA WITH ECCRINE DIFFERENTIATION: A RARE ENTITY Divvya B 1, Rehana Tippoo 2, P. Viswanathan 3, B. Krishnaswamy 4, A.
 BASAL CELL CARCINOMA WITH ECCRINE DIFFERENTIATION: A RARE ENTITY Divvya B 1, Rehana Tippoo 2, P. Viswanathan 3, B. Krishnaswamy 4, A. Anvar Ali 5 HOW TO CITE THIS ARTICLE: Divvya B, Rehana Tippoo, P. Viswanathan,
BASAL CELL CARCINOMA WITH ECCRINE DIFFERENTIATION: A RARE ENTITY Divvya B 1, Rehana Tippoo 2, P. Viswanathan 3, B. Krishnaswamy 4, A. Anvar Ali 5 HOW TO CITE THIS ARTICLE: Divvya B, Rehana Tippoo, P. Viswanathan,
July 2012 SKIN SURGERY SERVICE BRIEFING NOTES
 SKIN SURGERY SERVICE BRIEFING NOTES Introduction The WBoP PHO has an agreement with the BoP District Health Board to deliver the Skin Surgery Service. The current period will expire on 30 June 2012 and
SKIN SURGERY SERVICE BRIEFING NOTES Introduction The WBoP PHO has an agreement with the BoP District Health Board to deliver the Skin Surgery Service. The current period will expire on 30 June 2012 and
Use of Histopathology and Microbiology in Veterinary Dermatology
 Use of Histopathology and Microbiology in Veterinary Dermatology Dr R D Last BVSc; M.Med.Vet (Pathology) Specialist Veterinary Pathologist Introduction The skin is the largest of the organ systems and
Use of Histopathology and Microbiology in Veterinary Dermatology Dr R D Last BVSc; M.Med.Vet (Pathology) Specialist Veterinary Pathologist Introduction The skin is the largest of the organ systems and