Corneal specimens that influence clinical decisions
|
|
|
- Ralph Cross
- 6 years ago
- Views:
Transcription
1 Corneal specimens that influence clinical decisions Refractive surgery Corneal dystrophies Microbial infections J. Douglas Cameron, MD Chief, Ophthalmic Pathology Division Neuropathology Department Armed Forces Institute of Pathology Washington, DC, /5/2010
2 45 year-old man with progressive corneal opacification and extreme pain 3/5/2010
3 Critical Anatomy Tear film Oxygen delivery system Passive resistance to infection Mucous Lysozymes Glycocalyx Active resistance to infection Non-nodal lymphocytes Langerhans cells 3/5/2010
4 Stratified squamous epithelium Conserved radius of curvature Homogeneous cell population Lipid barrier to drug delivery Sensory nerve plexus Able to secrete proteolytic enzymes 3/5/2010
5 The Limbus; junction of cornea and sclera Arteriovenous arcades Lymphatic channels Stem cells; source of corneal epithelial cells 3/5/2010
6 Bowman s membrane Acellular No mechanism for repair 3/5/2010
7 Corneal stroma (matrix) Type I collagen and proteoglycans (nonrenewable_ Resting keratocyte (fibroblast) population Collagenase Gelatinase High tensile strength Limited repair capacity 3/5/2010
8 Descemet s membrane Resistant to proteolysis Not attached to collagen matrix Not attached to endothelium 3/5/2010
9 Corneal endothelium Not vascular endothelium A type of mesothelium Not renewable Can undergo fibrous metaplasia 3/5/2010
10 Refractive Surgery Surgical methods for changing the optic characteristics of the eye Usually performed on the cornea Does not completely eliminate the need for glasses. 3/5/2010
11 Radial Keratotomy Obsolete procedure Free-hand incisions of the cornea 4 to 40 incisions Compromised architectural integrity Unstable radius of curvature-changing vision through the day Wound rupture with minimal trauma 3/5/2010
12 LASIK (Laser assisted in situ keratomileusis) [?LAISK] Thinning a cornea with an excimer [excited dimer] laser Short wave length superficial penetration Surface pain and scarring Superficial flap Apply laser energy directly to corneal matrix 3/5/2010
13 LASIK Short circuits host defenses; alters repair mechanisms Microbial infection Epithelial ingrowth Altered biochemical environment Sands of Sahara syndrome Epithelial ingrowth 3/5/2010
14 Corneal Dystrophy Visible, heritable, biochemical abnormality of the cornea Classification changing with new genetic mapping Bilateral Progressive, variable clinical expression 3/5/2010
15 Keratoconus Progressive weakening of the architectural strength of the cornea (? Proteolysis, matrix metalloproteinases) Progressive change of corneal curvature Risk of rupture of Descemet's membrane [corneal hydrops] Risk of rupture of the fullthickness cornea [corneal perforation] 3/5/2010
16 Keratoconus Risk of perforating Descemet s membrane; corneal hydrops Sudden onset Partially reversible Risk of perforating fullthickness cornea A surgical emergency Risk of bacterial endophthalmitis 3/5/2010
17 Recurrence of Corneal Dystrophies Granular dystrophy Abnormal protein produced by epithelium Graft epithelium is replaced by host epithelium Lattice corneal dystrophy Amyloid (? keratocytes) Primary localized amyloidosis Graft keratocytes replaced by host keratocytes. 3/5/2010
18 Fuchs endothelial dystrophy Progressive dysfunction of the corneal endothelium since birth Clinical expression at age 60 to 80 years Progressive corneal edema (endothelial pump failure ) Treatment Penetrating keratoplasty Deep lamellar endothelial keratoplasty (DLEK) 3/5/2010
19 Endothelial Failure (PKP) Epithelium Subepithelial bullae Intraepithelial basement membrane formation Descemet s membrane Generalized thickening Localized thickening (guttata) Loss of endothelial cell density 3/5/2010
20 Endothelial Failure (DLEK) Anterior cornea remains intact Deep lamellar keratoplasty Posterior corneal stroma replaced Descemet s membrane replaced Descemet s membrane Excrescences of Descemet s membrane En face sections of guttata Few if any endothelial cells identified. 3/5/2010
21 Microbial Infection of the Cornea Host defenses Passive Tear film Mucous Glycocalyx Lipid epithelial barrier Vulnerable posterior to corneal epithelium Limited density and activity of keratocytes Langerhans cells Non-nodal lymphocytes 3/5/2010
22 Pseudomonas Keratitis Contact lens overwear Oxygen deprivation Loss of passive proteins Adhesion of pseudomonas organisms Production of collagenase By the organism By PMN Progressive corneal proteolysis ( melting ) 3/5/2010
23 Crystalline Keratopathy Prolonged treatment with topical steroids Corneal surgery allergic keratitis Creation of localized immune deficiency Proliferation of bacteria in colonies Separated by stromal lamellae, appearance of crystals S. epidermidis 3/5/2010
24 Herpes Simplex Keratitis (HSV-1) Primary cutaneous infection Residual organism in ganglia (dormant) Reactivation and migration to cornea epithelium via sensory axons 3/5/2010
25 Epithelial Herpes Simplex Keratitis (Dendritic keratitis) Intraepithelial proliferation Loss of desmosomes (vesicles) Cell death; linear ulceration dendritic figures Spontaneous resolution Mechanical removal Antivirals 3/5/2010
26 Stromal Herpes Simplex Keratitis (Discoid keratitis, Herpes metaherpetica) Recurrence at unpredictable rate and interval Change in antigen status of stromal matrix Giant cell reaction to membranes Proteolysis of matrix Corneal perforation Tissue adhesives Penetrating keratoplasty 3/5/2010
27 Acanthamoeba Keratitis Acanthamoeba Protozoan commonly found in water Forms Trophozoite Encysted Organism neurotrophic Presents with extreme pain Progressive ring opacity followed by ulceration 3/5/2010
28 Acanthamoeba Corneal Risk Factors Contact lens overwear Oxygen deprivation Microrupture of corneal epithelium Large areas of epithelial cell loss (corneal abrasion) Exposure to high organism concentration in hot tubs Exposure to stagnant water (Mississippi River Flood 1993) 3/5/2010
29 Acanthamoeba Infection Crosses lipid barrier Stimulation of corneal nerves Production of proteases and migration through the corneal matrix Able to penetrate to and through Descemet s membrane Not associated with endophthalmitis Both cornea and conjunctiva are infected 3/5/2010
30 Acanthamoeba Organism Clinical confocal microscopy Trophozoites not visible Double wall of encysted organism Light microscopy Trophozoites not visible Any stain Thick walled cysts Usually no inflammatory infiltrate Treatment: unsatisfactory 3/5/2010
31 Cornea: Review of Important Points (1): The corneal epithelium is the principle dynamic element in corneal pathology Protects the structurally essential nature of the collagen matrix from infection Able to contribute to structural damage by producing proteases Biochemical abnormalities of the epithelium may lead to progressive corneal opacity (granular dystrophy) 3/5/2010
32 Cornea: Review of Important Points (2): Refractive surgery potentially compromises the function of the cornea Loss of architectural strength (radial keratotomy [RK]) Corneal scarring (photorefractive keratectomy [PRK]} Circumvent corneal defenses (laser-assisted in situ keratomileusis [LASIK]) 3/5/2010
33 Cornea: Review of Important Points (3): Corneal dystrophies recur following penetrating keratoplasty The biochemical defect is in the cells of the host The donor cells of corneal transplantation are replaced by host cells 3/5/2010
34 Cornea: Review of Important Points (4): Corneal infections are often associated with proteolysis leading to corneal ulceration and possible corneal perforation Pseudomonas keratitis Herpes simplex keratitis Acanthamoeba keratitis 3/5/2010
35 Corneal specimens that influence clinical decisions Refractive surgery Corneal dystrophies Microbial infections J. Douglas Cameron, MD Chief, Ophthalmic Pathology Division Neuropathology Department Armed Forces Institute of Pathology Washington, DC, /5/2010
36 USCAP 2010: AAOP Society Companion Meeting 20MAR10 1) Corneal specimens that influence clinical decisions: refractive surgery, corneal dystrophy, microbial infections. 2) Case presentation: 45 year-old man with progressive corneal opacity and extreme pain a) Commonly used clinical terms i) Corneal infiltrate = corneal opacity (1) Most likely due to edema of the cornea and loss of transparency (2) Not associated with a cellular inflammatory infiltrate ii) Corneal melting = loss of corneal tissue (1) Most likely due to proteolysis (2) Not due to a change in temperature (3) Change in temperature would cause shrinking and opacification due to denaturation of collagen 3) Critical anatomy a) Tear film: Components produced by the conjunctiva and eyelid i) Oxygen delivery system ii) Passive resistance to microbial infection (1) Mucous (2) Lysozymes (3) Glycocalyx iii) Active resistance to microbial infection (1) Non-nodal lymphocytes (2) Langerhans cells b) Stratified squamous epithelium i) Conserved radius of curvature ii) Homogeneous cell population (no goblet cells) iii) Lipid barrier to drug delivery iv) Sensory nerve plexus v) Able to secrete proteolytic enzymes c) Limbus i) Arteriovenous arcades ii) Lymphatic channels iii) Stem cells, source of epithelial cells d) Bowman s membrane i) Acellular collagen ii) No mechanism of repair e) Stroma i) Type I collagen and proteoglycans (non-renewable) ii) Resting keratocyte (fibroblast) population iii) Keratocytes able to produce collagenase and gelatinase iv) High tensile strength v) Limited repair capacity 1 P a g e
37 USCAP 2010: AAOP Society Companion Meeting 20MAR10 f) Descemet s membrane i) Resistant to proteolysis ii) Not attached to collagen matrix iii) Not attached to endothelium g) Endothelium i) Not vascular endothelium ii) A type of mesothelium iii) Not renewable iv) Can undergo fibrous metaplasia 4) Refractive surgery a) Surgical methods for changing the optical characteristics of the eye i) Usually performed on the cornea ii) Does not completely eliminate need for glasses b) Refractive keratotomy- compromise of architectural strength i) Obsolete surgical procedure (1) Free-hand incisions of the cornea (2) 4 to 40 wounds (3) Compromised architectural integrity of the cornea ii) Unstable radius of curvature- variable refractive error through the day iii) Wound rupture- with minimal trauma c) LASIK (Laser-assisted in situ keratomileusis)[mileusis: Greek carving] i) Currently used surgical procedure (1) Thinning of the cornea with a excimer (excited dimer) laser (a) Short wavelength (193 nm) (b) Superficial penetration (2) Surface application; post-operative pain and corneal scarring (3) Superficial stromal application; access via a surgically created flap ii) Short circuits host defenses, alters repair mechanisms (1) Microbial infection- destroys host tissue, no repair mechanism (2) Epithelial ingrowth - creates correctable opacity iii) Altered biochemical environment- favors inflammation, protein deposits (1) Sands of Sahara syndrome (2) Acceleration of opacification in granular dystrophy 5) Corneal dystrophy a) A visible, heritable, biochemical abnormality of the cornea i) Classification changing with new genetic mapping (5q31) ii) Bilateral, may be symmetrical iii) Progressive, but with variable clinical expression b) Keratoconus- most common, generally non-heritable i) Weakening of corneal architecture-?proteolysis [matrix metalloproteinase] ii) Progressive change of corneal curvature-non-homogeneous 2 P a g e
38 USCAP 2010: AAOP Society Companion Meeting 20MAR10 iii) Risk of perforation of Descemet s membrane-corneal hydrops (1) Sudden onset (2) Partially reversible iv) Risk of perforation of full-thickness cornea (1) A surgical emergency (2) Risk of bacterial endophthalmitis c) Recurrence of stromal dystrophies i) Granular corneal dystrophy- (1) deposition of abnormal protein produced by host epithelium (2) donor epithelium replaced by host epithelium ii) Lattice corneal dystrophy- deposition of amyloid (primary localized amyloidosis) d) Fuchs endothelial dystrophy i) Progressive dysfunction of corneal endothelium since birth (1) Clinical expression at age 60 to 80 years (2) Progressive corneal edema (endothelial pump failure ) ii) Treatment of Fuchs dystrophy (1) Penetrating keratoplasty (PKP) (a) Epithelium (i) Subepithelial bullae (ii) Intraepithelial basement membrane (b) Descemet s membrane (i) Generalized and localized thickening (guttata) (ii) Loss of endothelial cell density (2) Deep lamellar endothelial keratoplasty (DLEK) (a) Excrescences of Descemet s membrane (b) Few if any endothelial cells 6) Microbial infection a) Host defenses i) Passive (1) Tear film (2) Mucous (3) Glycocalyx ii) Lipid epithelial barrier (1) Vulnerable posterior to the epithelium (2) Limited density and reactivity of keratocytes b) Pseudomonas keratitis i) Contact lens overwear; oxygen deprivation ii) Adhesion of pseudomonas organisms iii) Production of collagenase (1) Organism itself (2) Polymorphonuclear leukocytes (PMN) 3 P a g e
39 USCAP 2010: AAOP Society Companion Meeting 20MAR10 iv) Progressive corneal matrix proteolysis c) Crystalline keratopathy i) Prolonged treatment with topical steroid (1) Usually following corneal surgery (2) Resistant corneal allergy ii) Creation of local immune deficiency iii) Proliferation of bacterial organism between collagen lamellae ( crystalline serrated edges) iv) Intrastromal colonies of bacteria (Staphlococcus epidermidis) d) Herpes simplex keratitis (Herpes simplex type I) i) Primary cutaneous infection ii) Residual organisms in ganglia, dormant iii) Reactivation and migration to corneal epithelium, sensory axons iv) Intraepithelial proliferation (1) Loss of desmosomes: vesicles (2) Cell death: linear ulceration, dendritic figures v) Spontaneous resolution vi) Recurrence at unpredictable rate and interval vii) Change in antigen status of stromal matrix; stimulates inflammation viii) Proteolytic destruction of stroma ix) Corneal perforation x) Treatment (1) Tissue adhesives (2) Penetrating keratoplasty e) Acanthamoeba keratitis i) Protozoan commonly present in water supplies ii) Forms (1) Trophozoite; mobile (not seen by light microscopy) (2) Encysted; unfavorable environment iii) Presents with extreme pain (1) Organism neurotrophic (2) Progressive ring opacity/ulceration of cornea iv) Infection (1) Cornea compromised by (a) Contact lens overwear (i) Oxygen deprivation (ii) Microrupture of epithelium (iii) Large areas of epithelial cell loss (abrasion) (b) Exposure to high organism content in hot tubs (c) Exposure to stagnant water; e.g. Mississippi River flood 1993 (2) Neural trophism; associated with extreme pain (3) Lipid barrier lost 4 P a g e
40 USCAP 2010: AAOP Society Companion Meeting 20MAR10 (a) Trophozoite produces protease (b) Migrates through full thickness of cornea (c) Does not cause endophthalmitis v) Identification of organism (1) Confocal microscopy; method of clinical identification (2) Light microscopy (a) Stains with all routine stains (b) May not be accompanied by an inflammatory reaction. 7) Summary of Important Points a) The corneal epithelium is the principle dynamic element in corneal pathology i) Protects the structurally essential nature of the collagen matrix from infection ii) Able to contribute to structural damage by producing proteases iii) Biochemical abnormalities of the epithelium may lead to progressive corneal opacity (granular dystrophy) b) Refractive surgery potentially compromises the function of the cornea i) Loss of architectural strength (radial keratotomy [RK]) ii) Corneal scarring (photorefractive keratectomy [PRK]} iii) Circumvent corneal defenses (laser-assisted in situ keratomileusis [LASIK]) c) Corneal dystrophies recur following penetrating keratoplasty i) The biochemical defect is in the cells of the host ii) The donor cells of corneal transplantation are replaced by host cells d) Corneal infections are often associated with proteolysis leading to corneal ulceration and possible corneal perforation i) Pseudomonas keratitis ii) Herpes simplex keratitis iii) Acanthamoeba keratitis 5 P a g e
41 Advances in Melanocytic Lesions of Conjunctiva Codrin E. Iacob, New York Eye and Ear Infirmary, New York, NY American Association of Ophthalmic Pathologists USCAP Companion Society Meeting Washington, DC, Saturday, March 20 th, 2010 Handout Particularities of conjunctiva as compared to the skin Conjunctival lamina propria is a thin layer of loosely collagenous tissue rich in vascular supply and in immediate contact to Tenon s capsule, sclera, ocular adnexae, and to anterior orbit. As a protective barrier conjunctival lamina propria is less efficient than dermis. Constant mechanical abrasion due to blinking favors development of flattened conjunctival lesions. On the other hand translucency and large mobility of conjunctiva over the underlying tissues permits early detection of lesions and easier assessment of depth of location and attachment to deep structures. But palpebral and forniceal conjunctival location of melanocytic lesions are often time related to delayed diagnosis. Lesions of the conjunctiva not derived from melanocytes that may simulate pigmented lesions Pigemented squamous lesions (papillomas or conjunctival intraepithelial neoplasia with various degrees of dysplasia up to squamous cell carcinoma, including spindle cell carcinoma) Pharmaceutical agents (epinephrine plaques, argyrosis, minocyclin deposits) Metallic (foreign bodies, iron, heavy metals) or industrial products) quinones, aniline dyes) deposition Mascara deposits Lymphoid lesions ( salmon patch lesions) Mesenchymal proliferative conditions (fibroma, fibrous histiocytoma, elastofibroma, myxoma, nodular fasciitis) Juvenile xanthogranuloma Neurofibroma Pinguecula and pterigium Pyogenic granuloma Hemangiopericytoma
42 Inflammatory conditions (sarcoidosis, other granulomatous or allergic processes) Pseudopigmentations (blue sclera, staphyloma, scleromalacia perforans) Endogeneus pigmentations (hemosiderin, bilirubin depositions, Addison disease, Peutz- Jegher syndrome) Metabolic disorders (ochronosis, Gaucher s disease) Ephelis (freckle) Increased local pigmentation in basal epithelial cells without melanocytic hyperplasia Complexion-Associated conjunctival pigmentation (racial melanosis) Increased bilateral and symmetrical pigmentation in basal epithelial cells without melanocytic hyperplasia is seen. The pigment tends to be most intense at the limbus, fanning out toward the fornices. Lentigo simplex Increased local pigmentation in basal epithelial cells with basal melanocytic hyperplasia Nevi Congenital or acquired hamartomatous, well circumscribed, melanocytic lesions on epibulbar conjunctiva, plica, caruncle, or eyelid margins: rarely seen on palpebral conjunctiva. Specific to conjunctiva are Henle epithelial crypts entrapped in subepithelial nevi forming cystic spaces. Generally follow the description of their skin counterparts: - junctional nevi - subepithelial nevi (analogous to intradermal nevi) - compound nevi - blue nevi - dysplastic nevi (proliferation of cytologically atypical melanocytes attached to a nevus) - Spitz nevi - Congenital melanosis oculi and congenital oculodermal melanosis (nevus of Ota): defect of melanocyte migration with formation of diffuse blue nevus in skin, periocular soft tissues, episclera, and sclera in the distribution of the opthalmic branch of trigeminal nerve; associated with melanocytic proliferation in uveal tract, meninges of optic nerve and orbital periosteum.
43 Primary acquired melanosis Specific terminology is used by ophthalmologists and ophthalmic pathologists although the lesions match their skin counterparts. In an effort to reconcile different terms used in the past, the World Health Organizations proposed the currently used term of Primary Acquired Melanosis (PAM) which better characterizes conjunctival melanocytic lesions where application of cutaneous criteria of asymmetry, superficial spreading, and depth of invasion are problematic. Clinically it presents as an acquired unilateral golden-brown flat pigmentation of the bulbar, forniceal, or palpebral conjunctiva in middle aged persons. It displays irregular borders, variable degrees of pigmentation, relentless growth, or waxing and waning evolution. Palpebral lesions are sometime continuous with lentigo maligna (Hutchinson freckle) of the eyelid skin. Characteristically PAM is freely movable over sclera. PAM without atypia (31% of cases) Some show basal conjunctival epithelial hyperpigmentation without melanocytic hyperplasia (reactive acquired melanosis). Histomorphologic overlap with freckle, but clinically more widely spread. Some show conjunctival epithelial hyperpigmentation with melanocytic hyperplasia which is uniform and confined to basal layer. Histomorphologic overlap with lentigo simplex but clinically more widely spread. Both have extremely low potential to evolve to melanoma. PAM with atypia (68% of cases) Conjunctival melanocytes harbor enlarged nuclei, palisading of enlarged melanocytes along the basal layer, local pagetoid invasion of melanocytes into the conjunctival epithelium, and nesting of melanocytes. Lesional melanocytes are characterized by cytologic and architectural features which are used to classify PAM with atypia into low and high risk categories for invasive melanoma. The skin counterparts of these two entities could be considered lentigo maligna and lentigo maligna melanoma, respectively. Low risk cytologic atypia includes small polyhedral, spindle, and large melanocytes with pigmented arborizing dendrites. High risk cytologic atypia includes epithelioid melanocytes (75% risk of evolution to malignant melanoma). Low risk architectural growth patterns are basilar hyperplasia, basilar nesting, and occasional suprabasilar intraepithelial nesting (all 22% risk of evolution to malignant melanoma). High risk architectural patterns are pagetoid involvement (multiple buckshot type melanocytic clusters of various sizes) and nearly complete epithelial replacement (both 90% risk of evolution to malignant melanoma). Malignant melanoma Invasion of conjunctival lamina propria and neighboring structures by atypical melanocytes is the harbinger of conjunctival malignant melanoma. In 35-40% of cases malignant melanomas arise from junctional (rare) or compound nevi; in 25-30% of cases they come from primary acquired melanosis; and in of cases they arise de novo or
44 indeterminately. The ones arising from preexisting nevi have a slightly better prognosis than the ones arising in preexisting PAM with atypia or arising de novo. Melanomas in this location can be primary or secondary (from intraocular of distant skin melanomas). Prognostically important factors are: - unfavorable locations: palpebral conjunctiva, fornices, plica, caruncle, and lid margins - favorable location: bulbar conjunctiva - depth of invasion (measured from the epithelial surface): less than 1.5 mm the prognosis for life is excellent - some studies consider this threshold at 0.8 mm and consider lesions of 1-4 mm to have a two times higher death rate while those of greater than 4 mm thickness a four times higher death rate. - more than 5 mitoses/10 high power fields is associated with poor prognosis - lack of lymphocytic host response is associated with poor prognosis - lymphatic, vascular, or perineural invasion are also associated with poor prognosis Bibliography 1. Shields JA, Shields CL, Mashayekhi A, Marr BP, Benavides R, Thangappan A, Eagle RC. Primary acquired melanosis of the conjunctiva: experience with 311 eyes. Trans American Ophthalmology Society.2007; 105: Shields CL, Shields JA. Tumors of the conjunctiva and cornea. Surv Opthalmology 2004; 49: Ackerman AB, Sood R, Koenig M. Primary acquired melanosis of the conjunctiva is melanoma in situ. Mod Pathology 1991; 4: Jakobiec FA, Folberg R, Iwamoto T. Clinicopathologic characteristics of premalignant and malignant melanocytic lesions of the conjunctiva. Opthalmology 1989; 96: Patel BC, Egan CA, Lucius RW, et al. Cutaneous malignant melanoma and oculodermal melanocytosis (nevus of Ota): report of a case and review of the literature. Journal of American Academy of Dermatology 1998; 2: Shields CL. Conjunctival melanoma: risk factors for recurrence, exenteration, metyastatsis, and death in 150 consecutive patients. Trans American Ophthalmological Society 2000; 98: Suguira M, Colby KA, Mihm MC Jr., et al. Low-risk and high-risk histologic features in conjunctival primary acquired melanosis with atypia:clinicopathologic analysis of 29 cases. American Journal of Surgical Pathology2007; 31: Leon Barnes. Surgical pathology of the Head and Neck. Third edition, Font LR, Croxatto JO, Rao NA. Tumors of the Eye and Ocular Adnexa. AFIP Atlas of Tumor Pathology. Fourth series, Yanoff M, sassani J. Ocular pathology. Sixth edition, 2008.
45 AAOP Companion Society Meeting USCAP 2010 Melanocytic Lesions of Conjunctiva: WT1 and BCl2 As Useful Markers? Emiko Furusato, MD From the Division of Ophthalmic Pathology, Armed Forces Institute of Pathology, Washington, DC.
46 Background Melanocytic lesions of the conjunctiva encompass a spectrum that ranges from benign or atypical nevi to malignant melanoma categories. Occasionally, definitive diagnosis of malignancy based on morphologic features alone can be extremely difficult. The aggressive clinical behavior of malignant melanoma and the increasing practice of multimodality therapy demand additional biological end points to augment conventional histopathologic stratification of patients.
47 Background (cont.) Recent studies indicate that WT1 and Bcl2 protein are detected in melanocytic lesions of the skin. Expression of the Wilms tumor gene (WT1) has been documented in several cancer cell types, including cutaneous melanomas. Burwell et al. Oncogene. 2007;26(23): Hohenstein et al. Hum Mol Genet. 2006;15(Spec No. 2):R196-R201. Rodeck et al. Int J Cancer. 1994;59(1): Wagner et al. Cell Growth Differ. 2002; 13(7): Nakatsuka et al. Mod Pathol. 2006;19(6): Wilsher et al. Histopathology. 2007; 51(5): Wagner et al. Pflugers Arch. 2008;455(5):
48 Background (cont.) Bcl2 protein is detected in benign and malignant melanocytic neoplasms of the skin in addition to follicular lymphomas. van den Oord et al. Am J Pathol Aug;145(2): Saenz-Santamaria et al. J Cutan Pathol Oct;21(5): Cerroni et al. Am J Dermatopathol Feb; 17(1):7-11. Ramsay et al. Mod Pathol Feb; 8(2):150-4.
49 Background (cont.) Bcl2 is an integral outer mitochondrial membrane protein that blocks the apoptotic death of some cells such as lymphocytes. Constitutive expression of Bcl2, such as in the case of translocation of Bcl2 to Ig heavy chain locus, is thought to be the cause of follicular lymphoma. Currently, there are no published reports of Bcl2 studies in melanocytic lesions of the conjunctiva.
50 Objective Evaluation of WT1 and Bcl2 expression in conjunctival melanocytic lesions and comparison the results with other immunohistochemical markers.
51 Materials and Methods Cases (conjunctival melanocytic lesions) (n=123) Benign nevi (n=72) Atypical nevi (n=21) Primary Acquired Melanosis (PAM) (n=11) Malignant Melanomas (MM) (n=20) Ages ranged from 2 to 84 years
52 Materials and Methods (cont.) Immunohistochemistry Monoclonal antibodies WT1 (Cell Marque Corp, 1:10 dilution) Bcl2 (Dako, 1 : 50 dilution) HMB45 (Dako, 1 : 50 dilution) Melan A (Ventana, prediluted) Polyclonal antibody S-100 (Dako, 1: 600 dilution) Red chromogen was used as the counter stain in heavily pigmented cases
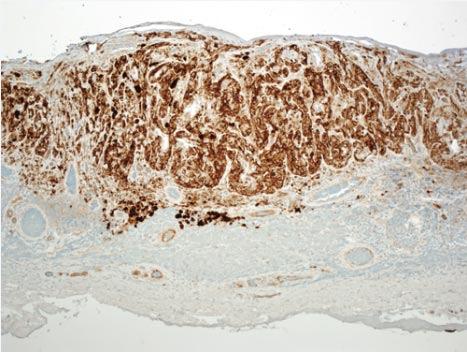
53 Amelanotic nevus of the nasal conjunctiva. Furusato, E. et al. Arch Ophthalmol 2009;127:




54 HE Bcl2 HMB45 WT1 HE


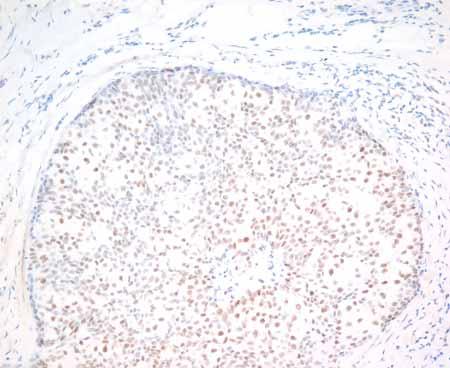
55 Malignant melanoma of the conjunctiva and cornea Furusato, E. et al. Arch Ophthalmol 2009;127:



56 HE Bcl2 HMB45 WT1
57 Immunoreactivity and Staining Patterns for Bcl2, HMB45, S100, and Melan A in Conjunctival Melanocytic Lesions Furusato, E. et al. Arch Ophthalmol 2009;127:
58 Immunoreactivity and Staining Patterns for WT1 Conjunctival Melanocytic Lesions Furusato, E. et al. Arch Ophthalmol 2009;127:
59 Degree of Positivity for Bcl2, HMB45, S100, and Melan A in Conjunctival Melanocytic Lesions Furusato, E. et al. Arch Ophthalmol 2009;127:
60 WT1 and HMB45 intensity distributions of nevi and malignant melanomas WT1 HMB45 Furusato, E. et al. Arch Ophthalmol 2009;127:
61 Summary Bcl-2 expression was positive in all benign and malignant melanocytic lesions (100%) with strong and diffuse reactivity in most cases. The expression was more consistent, stronger, and more diffuse than for S100, HMB45, Melan A and WT1. HMB 45 and WT1 showed significant differences in staining between benign nevi and malignant melanomas.
62 Summary (cont.) HMB45 and WT1 showed weak or moderate expression in benign nevi, but was strong and diffuse in malignant melanomas. Bcl-2, S100 and Melan A did not show meaningful differences compared to HMB45 and WT1.
63 Conclusions Bcl2 is a highly sensitive immunohitochmical marker for melanocytic tumors of the conjunctiva HMB45 and WT1 staining can assist in distinguishing benign from malignant lesions
64 Thank you Nevus Melanoma Bcl2 HMB45 WT1
65 Questions
66 69 yo female presented with the conjunctival lesion seen above. Which marker is least helpful in confirming the diagnosis? A. S100 B. HMB45 C. CD45 D. MART1 E. SMA
67 Answer is E This lesion could be either a lymhocytic or amelanotic lesion; therefore, SMA (smooth muscle actin) is not helpful in this setting.
68 Which markers are helpful in distinguishing between benign from malignant melanocytic lesions of the conjunctiva? (Select two) A. MelanA B. S100 C. HMB45 D. WT1 E. Bcl2
69 Answer is C and D. HMB45 and WT1 WT1 and HMB45 frequently show diffuse and strong staining in atypical nevi, primary acquired melanosis with atypia, and malignant melanomas compared with benign lesions. Reference: Furusato et al. Arch Ophthalmol 2009;127: Jakobiec et al. Arch Ophthalmol 2010;128:
70 Squamous and Sebaceous Lesions of Conjunctiva: Advances in Immunohistochemical and Molecular Markers Charles Eberhart, M.D., Ph.D. AAOP/USCAP 2010 Washington DC
71 Overview Conjunctival Intraepithelial Neoplasia (CIN) and Squamous Cell Carcinoma Conjunctival Spindle Cell Carcinoma Sebaceous Carcinoma


72 Conjunctival Intraepithelial Neoplasia (CIN) Older individuals, M>F Associated with sun exposure, HIV, HPV Generally involve perilimbal conjunctiva Sharply demarcated Can recur and progress to SCC Shields and Shields




73



74




75 Conjunctival Squamous Cell Carcinoma
76 Conjunctival Intraepithelial Neoplasia (CIN) Proposed prognostic markers: p53, Ki67, AgNOR Other roles of special stains: Rule out melanocytic lesions (Melan A, MITF, etc.) Rule out sebaceous carcinoma on frozen material (Oil Red O) Look for HPV (in situ)
77 HPV in Conjunctival CIN and Squamous Cell Carcinoma Several studies suggested that high risk HPV is often present Other studies failed to detect HPV It has recently been suggested that the cutaneous HPV types 5 and 8 are involved
 in situ and invasive conjunctival SCC, but also in 32% of normal conjunctival")
78 HPV 16 or HPV 18 DNA and mrna detected in 10/10 CIN and no controls HPV 16 or HPV 18 DNA detected in 25 of 45 (56%) in situ and invasive conjunctival SCC, but also in 32% of normal conjunctival specimens.




79 HPV 16 HPV 18 HPV 6/11
80 HPV in Conjunctival CIN and Squamous Cell Carcinoma Several studies suggested that high risk HPV is often present Other studies failed to detect HPV It has recently been suggested that the cutaneous HPV types 5 and 8 are involved


81 No HPV DNA detected in 30 cases of CIN and SCC 24 consecutive cases of CIN and SCC from a single institution examined using IHC and PCR. 15 HPV subtypes analyzed none detected.
82 HPV in Conjunctival CIN and Squamous Cell Carcinoma Several studies suggested that high risk HPV is often present Other studies failed to detect HPV It has recently been suggested that the cutaneous HPV types 5 and 8 are involved
83 Study in Uganda involving 94 conjunctival SCC, 39 CIN, and 285 controls PCR tests for 75 HPV types used Mucosal HPV rare or absent Cutaneous HPV (especially types 5 and 8) identified in 45% of SCC and 41% of CIN Cutaneous HPV infection and squamous conjunctival lesions seldom seen in the absence of HIV

84 Conjunctival Spindle Cell Carcinoma

85 CAM5.2

86 AE1/AE3
 Elderly")

87 Sebaceous Carcinoma Rare (1% to 3% of all malignant eyelid tumors) Elderly individuals (F>M) Often multicentric Prominent intraepithelial spread Shields and Shields

88

89



90 Intraepithelial Sebaceous Carcinoma

91 EMA and p16 Immunostains in Sebaceous Carcinoma EMA p16


92 EMA p16


93 p16 Highlights Intraepithelial Spread EMA p16

94 p16




95 p16


96



97 Adipophilin can distinguish sebaceous tumors from basal cell carcinoma and squamous lesions
98 Mismatch Repair in Sebaceous Carcinoma Sebaceous gland tumors and visceral malignancies (most frequently colorectal carcinoma) occur together in Muir-Torre syndrome (MTS) Sebaceous adenoma more common than carcinoma Mutations in MLH1, MSH2 and other genes associated with DNA mismatch repair


99 61 year old female with MTS



100 MLH1 PMS2 MSH2 MSH6
101 Our experience with MMR gene IHC and MSI in sporadic sebaceous carcinoma 9 sporadic cases stained with antibodies specific for MSH2, MSH6, MLH1 and PMS2 No loss of staining in any sporadic tumor Also no signs of microsatellite instability (MSI) in any sporadic sebaceous carcinoma case tested by PCR analysis of multiple markers




102 MSH6 MLH1 MSH2 PMS2

103


104 FHIT may be involved in Muir-Torre cases lacking MSH/MLH changes

105
106 Conclusions The role of HPV in the pathogenesis of CIN and conjuntival squamous cell carcinoma is not clear p16 immunostains can be useful in tracking intraepithelial spread of sebaceous carcinoma Immunohistochemical stains suggest an intact mismatch repair system in sporadic periocular sebaceous carcinoma
107 AAOP companion society meeting, USCAP 2010 Non-neoplastic conjunctival desease Milman T 1 AAOP Companion Society Meeting, USCAP 2010 Saturday March 20, Marriott Wardman Park, Washington, DC Advances in Non-neoplastic Conjunctival Disease - Inflammation, Degenerations and Deposits Tatyana Milman, MD Assistant Professor of Ophthalmology Associate Attending Pathologist Department of Pathology and Laboratory Medicine New York Eye and Ear Infirmary OUTLINE I. INTRODUCTION II. IMMUNOLOGIC DISORDERS OF THE CONJUNCTIVA III. MEMBRANOUS AND PSEUDOMEMBRANOUS CONJUNCTIVITIS IV. CONJUNCTIVAL DEGENERATIONS V. CONJUNCTIVAL DEPOSITS VI. REFERENCES I. INTRODUCTION Significant advances have been made in the understanding of the genetic, molecular and immunologic aspects of various conjunctival disorders. The following conjunctival conditions have been selected because these advances translate into the ophthalmic pathology practice. II. IMMUNOLOGIC DISORDERS OF THE CONJUNCTIVA Numerous immunologic disorders can affect conjunctiva, including Stevens-Johnson syndrome and toxic epidermal necrolysis, ocular cicatricial pemphigoid, drug-induced pemphigoid, linear IgA bullous dermatosis, graft-vs-host disease, dermatitis herpetiformis, epidermolysis bullosa, lichen planus, paraneoplastic pemphigus, pemphigus vulgaris, pemphigus foliaceous, discoid lupus erythematosus, and phlyctenular conjunctivitis. A. Mucous membrane pemphigoid (ocular cicatricial pemphigoid) Definition. Mucous membrane pemphigoid (MMP) and its subset, ocular cicatricial pemphigoid (OCP), is a type II immune-mediated hypersensitivity disorder, characterized by deposition of autoantibodies or complement to the components of basement membrane zone (BMZ) at the epithelial-subepithelial junction of mucous membranes and
108 AAOP companion society meeting, USCAP 2010 Non-neoplastic conjunctival desease Milman T 2 occasionally at the dermo-epidermal junction of the skin. MMP is associated most frequently with autoantibodies against against bullous pemphigoid (BP) antigen 180 (BP180) and less often with autoantibodies against BP230, laminin 5/epiligrin, laminin 6, uncein, type VII collagen and integrin subunits ß4 and α6. OCP is associated mainly with autoantibodies against laminin 5 or ß4 integrin. General features. Binding of the antibodies to the target antigens at BMZ leads to complement activation, deposition, and inflammatory cell infiltration, manifesting clinically by sub-epithelial bullae formation and eventual cicatrization. Approximately 10 30% of patients with OCP demonstrate circulating IgG and IgA autoantibodies and display serologic activity against classical bullous pemphigoid antigens. Environmental triggers, such as topical medications, have been occasionally implicated in pathogenesis of OCP in genetically predisposed individuals (pseudopemphigoid). Rarely, cicatricial pemphigoid with its representative pathologic findings is observed as a sequela of SJS. Recent research has focused on elucidating the reasons why despite similar immunopathology of BP and MMP, the MMP is associated with disabling scarring while BP is not. Some studies have found high levels of TGF-β in OCP conjunctiva and implicated this cytokine in fibrogenesis. Other studies have suggested that high levels of expression of vascular cellular adhesion molecule (VCAM) and intercellular adhesion molecule (ICAM-1) on endothelial cells in MMP leads to IL-4 mediated stimulation of perivascular fibroblasts to lay down scar tissue. Clinical features. The disease most commonly begins in the sixth or seventh decade of life and has a slight female predominance. The mucous membrane affected are most frequently oral (85%) and conjunctival (60 80%), followed by nasal, nasopharyngeal, anogenital, skin (20%), larynx and esophagus. Patients with extraocular MMP have approximately 4% per year risk of developing ocular involvement. The conjunctival lesions begin in one eye, but bilateral involvement eventually occurs. The clinical course of OCP is characterized by slow relapsing-remitting progression from chronic conjunctivitis to sub-epithelial fibrosis, fornix foreshortening, symblepharon and ankyloblepharon formation, corneal ulceration and opacification, and ocular surface keratinization. Microscopic findings. Histopathology of the conjunctiva in acute stage of OCP shows subepithelial bullae with predominantly subepithelial inflammatory infiltrate, composed mostly of T-lymphocytes, and to a lesser extent of macrophages, dendritic cells, and neutrophils. Later in the course of disease, squamous metaplasia and loss of goblet cells are observed within the epithelium. Activation of fibroblasts leads to abnormal deposition of extracellular matrix and collagen in the substantia propria in the cicatrizing stages of OCP. Immunohistologic findings. Direct immunofluorescence, immunoperoxidase technique, and immunoelectron microscopy demonstrate deposition of IgA, IgG, IgM, and C3 along the BMZ, but negative conjunctival biopsy does not exclude the diagnosis of OCP. Positive predictive value of conjunctival biopsy with direct immunofluorescence is 60 80%. Repeat biopsy from extraocular site increases the chance of confirming a diagnosis of MMP.
109 AAOP companion society meeting, USCAP 2010 Non-neoplastic conjunctival desease Milman T 3 An antilaminin 5 ELISA with high specificity and sensitivity has been developed for circulating antilaminin 5 autoangibodies. Its role in pure OCP has yet to be determined. Differential diagnosis. 1. Other causes of cicatrizing conjunctivitis: infectious (adenovirus, streptococcus, chlamydia, diphtheria, gonococcus), inflammatory (rosacea blepharoconjunctivitis) atopic keratoconjunctivitis, immune (Stevens-Johnson, toxic epidermal necrolysis, lichen planus, graft-versus-host disease), trauma (chemical, radiation), drug-induced pseudopemphigoid (topical ocular medications, systemic practolol), post-surgical changes, sarcoidosis, lupus erythematosus. 2. Other bullous disorders: subepithelial (linear IgA disease, epidermolysis bullosa) and intraepithelial (paraneoplastic pemphigus, pemphigus vulgaris). 3. Occular surface neoplasia. Treatment and prognosis. Systemic immunosuppressive therapy is a mainstay of treatment and includes methotrexate, cyclophosphamide, dapsone, azathioprine, mycophenolate, and possibly IVIg. Topical corticosteroids may suppress the inflammatory response during acute exacerbations. Topical Vitamin A has been shown to reverse, to some extent, keratinization. Surgical therapies include correction of eyelid deformities, mucosal grafting for fornix reconstruction, cultivated corneal/limbal epithelial cell transplantation with amniotic membrane grafting, and keratoprosthesis. B. Linear IgA bullous disease Definition and general/clinical features. Linear IgA bullous disease (LABD) is an autoimmune sub-epithelial and sub-epidermal blistering disorder, which typically affects middle age adults, but has also been reported in children. Purely ocular form can occur, which is difficult do distinguish clinically and pathologically from OCP. Microscopic/immunohistologic findings. Histopathology is similar to OCP. Immunofluorescence demonstrates linear deposition of IgA along BMZ. Deposits of IgG/C3 may also be present. Circulating IgA antibodies to BMZ, epidermal (epithelial), and dermal (stromal) sites can occur in some patients and are helpful in establishing the diagnosis of LABD. Treatment. Treatment is similar to OCP. III. MEMBRANOUS AND PSEUDOMEMBRANOUS CONJUNCTIVIITIS Membranous and pseudomembranous conjunctivitis occurs when the inflammatory discharge rich in fibrin coagulates on the conjunctival surface. A pseudomembrane lies superficially on the epithelial surface and can be peeled away without bleeding. In contrast, a true membrane incorporates conjunctival epithelium and/or granulation tissue
110 AAOP companion society meeting, USCAP 2010 Non-neoplastic conjunctival desease Milman T 4 and peels away with bleeding. The formation of pseudomembrane or a membrane often reflects the difference in the intensity of an inflammatory process, and both membranes and pseudomembranes may be present at the same time. The components of the exudate in membranes and pseudomembranes may point to an etiology of conjunctivitis. For example, acute membranes in immunologic and infectious disorders are composed of fibrinous exudate, neutrophils, and necrotic epithelial cells, while in ligneous conjunctivitis, lymphocytes, plasma cells, mast cells, and immunoglobulins predominate, with the background of extensive fibrin deposition and granulation tissue formation. Ligneous conjunctivitis Definition. Ligneous conjunctivitis is a rare, chronic, pseudomembranous disease, characterized by wood-like (pseudo)membranes developing on the ocular and extraocular mucosa. Although the term pseudomembrane is typically applied to ligneous lesion in clinical literature, it behaves as a true membrane by strict clinical and pathologic terminology. General features. Ligneous conjunctivitis typically presents in childhood as a chronic, bilateral, recurrent conjunctivitis, the hallmark of which is the formation of firm, woodlike, yellowish (pseudo)membranes. These are usually located on the superior tarsal conjunctiva, and less frequently on bulbar and inferior tarsal conjunctiva. Other mucous membranes can be less frequently involved, including oral cavity, respiratory tract, middle ear, and genital tract. Other conditions rarely associated with ligneous conjunctivitis include juvenile colloid milium and congenital occlusive hydrocephalus. Affected patients have homozygous and compound-heterozygous mutations in the type-1 plasminogen gene. Although mostly sporadic, familial cases with autosomal recessive inheritance pattern have been reported. While many reports describe spontaneous onset of disease, ligneous-like conjunctival changes can occasionally occur after ocular surgery. The condition has also been described in patients without plasminogen deficiency, who have been treated with antifibrinolytic medications, such as tranexamic acid. It is believed that mechanical injury or exposure to external irritants of mucosal tissues is followed by exudation of plasma proteins and immediate coagulation of fibin(ogen), the main constituent of (pseudo)membranes. This fibrin(ogen)-rich clot provides local hemostasis at the site of tissue injury, but also provides the substrate for the generation of fibrin matrix, which in turn is replaced by granulation tissue. Normally, fibrinolysis and remodeling of granulation tissue complete wound healing. Plasminogen deficiency results in defective fibrinolysis, thus manifesting in arrest of wound healing at the stage of extensive fibrin deposition and granulation tissue formation.
111 AAOP companion society meeting, USCAP 2010 Non-neoplastic conjunctival desease Milman T 5 Microscopic findings. 1. Abundant subepithelial deposits of amorphous, acellular, eosinopohilic, periodic acid- Schiff (PAS)-positive material, which consists of fibrin, immunoglobulin deposit (usually IgG), and mucopolysaccharides 2. Granulation tissue 3. Inflammatory infiltrate, which is rich in T-lymphocytes, although B-lymphocytes, plasma cells, and mast cells can also be observed 4. Occasionally, foreign material and bacteria have been demonstrated in the ligneous membranes, possibly providing the inciting stimulus for inflammatory response followed by ligneous membrane formation (debatable) 5. The surface of the ligneous membrane can lack normal epithelium and contains instead a collection of fibrin and inflammatory cells. This superficial layer may be scraped without bleeding, thus imparting a pseudomembrane characteristics to the superficial layer of the ligneous membrane. Treatment and prognosis. Ligneous conjunctivitis is usually a self limited disorder. Serious ocular complications can result, however, including secondary infection and corneal ulceration with perforation. Treatment modalitities include surgical excision of the membranes with or without adjunctive cryotherapy and amnionic membrane grafting, although recurrences are frequent. Anecdotal successes with topical corticosteroids, cyclosporine, heparin, purified plasminogen, and with intravenously administered purified plasminogen concentrate have been described. IV. DEGENERATIONS A. Conjunctivochalasis ( chalasis = relaxing, slackening in Greek) Definition. Isolated bilateral, condition in which redundant, non-edematous bulbar conjunctival tissue interposes between the globe and the lower eyelid, and protrudes over the lid margin. General features. Conjunctivochalasis typically presents after 5 th decade (average age ~70 years). The patients may be asymptomatic, or complain of dry eye, plerolacrima or epiphora. Few reported cases have been associated with nasolacrimal duct obstruction. In severe forms, exposure keratopathy and marginal corneal ulceration may occur. It is hypothesized that aging and actinic damage induce structural changes in the collagen and elastic fibers leading to conjunctival redundancy. Another theory postulates that inflammatory mediators and matrix metalloproteinases may contribute to the collagen and elastic fiber degradation leading to conjunctivochalasis. Increased levels of
112 AAOP companion society meeting, USCAP 2010 Non-neoplastic conjunctival desease Milman T 6 metalloproteinases could be induced by poor tear clearance, particularly in the patients with nasolacrimal duct obstruction. Microscopic findings. Several reports have identified varying histopathologic findings: 1. Fragmentation of elastic fibers and sparsely assembled collagen fibers in substantia propria; lymphangiectasis; no increased inflammation or epithelial changes*** 2. Increased chronic inflammatory infiltrate in the substantia propria 3. Actinic elastosis 4. Normal histology *** The first observation is consistent with our experience with conjunctivas bearing a clinical diagnosis of conjunctivochalasis. Treatment and prognosis. The condition is treated with resection of inferior limbal and bulbar conjunctiva. B. Pinguecula and pterygium Definition. Pingueculae and pterygia are common conjunctival lesions which typically occur in the temporal and nasal bulbar conjunctiva. Pinguecula appears as a yellowwhite, often vascularized nodule, while a pterygium presents as a wing-shaped vascularized fold of conjunctival tissue, which has invaded the superficial cornea. General features. Although pingueculae and pterygia traditionally have been viewed as conjunctival degenerations, this concept has been challenged by recent scientific evidence, which suggests that these lesions are non-malignant neoplasms. The pathogenesis of pingueculae and pterygia has been strongly correlated with environmental exposure (sunlight, wind, dust). Ultraviolet (UV) light (actinic exposure), in particular, is believed to be a strong inducer of these lesions. It is hypothesized that the optics of the anterior eye cause focusing of the scattered light at nasal or temporal limbus, accounting for the observed location of pingueculae and pterygia. The mechanisms proposed to explain growth of pterygia include UV-induced alteration of basal stem cells and resultant breakdown of limbal barrier, UV-induced loss of heterozygocity and loss of expression or function of tumor suppressor genes (e.g., P53), overexpression of cytokines (e. g., fibroblast growth factor, transforming growth factor-ß, tumor necrosis factor-α, vascular endothelial growth factor) which may lead to upregulation of matrix metalloproteinases, and viral (HSV, HPV) infection. Microscopic findings. Histopathologically, pingueculae and pterygia display actinic elastosis, increased vascularity and inflammatory infiltrate within the substantia propria. Involvement of the superficial cornea and destruction of Bowman s layer distinguish pterygia from pingueculae. Actinic elastosis is recognized by gray or basophilic amorphous, vermiform, or hyalin degeneration of collagen fibers. These regions stain
113 AAOP companion society meeting, USCAP 2010 Non-neoplastic conjunctival desease Milman T 7 with elastin (Verhoeff-van Giesen) stains, but the staining is not abolished by predigestion with elastase, supporting the conclusion that the material does not consist of true elastin fibers, but, rather, is elastin-like or elastotic. The conjunctival epithelium overlying pterygia or pingueculae may be normal or hyperplastic. Occasionally, pterygia and pingueculae can harbor ocular squamous surface neoplasia and benign and malignant melanocytic lesions, advocating for careful histopathological examinations of these lesions. Treatment and prognosis. Treatment for pterygia and pingueculae ranges from symptomatic relief with topical lubricants and nonsteroidal anti-inflammatory drugs, to surgical excision with limbal conjunctival autograft and/or amniotic membrane grafts. Adjuvant mitomycin-c, ß-irradiation, and anti-vascular endothelial growth factor agents are also occasionally used, particularly in pterygia with high risk of recurrence, and in recurrent pterygia. With sophisticated current surgical techniques the recurrence rate for primary pterygia is <10%. V. DEPOSITS The conjunctiva can be damaged by the use of topical and parenteral medications. Direct toxicity from active drug ingredients, drug metabolites, preservatives in drug vehicles, and deposition of drugs and their metabolites into the conjunctiva can occur. Compounds known to be actively accumulated in the conjunctiva include silver (basement membrane deposits), gold (all epithelial layers), mercury, amiodarone (epithelium), tetracycline and minocycline (within cystic inclusions), epinephrine (pigmented adrenochrome within cystic inclusions), quinacrine, and chorapromazine. Pigmentation of the conjunctiva has also been observed after long-term or high-dose therapy with antimalarial drugs and psychotropic medications. Several of drug-induced conjunctival deposits are discussed below. A. Tetracycline and minocycline-induced pigmentation Definition and general features. Tetracycline and tetracycline derivatives (especially minocycline) have been frequently associated with pigmentation of bones, teeth, skin, thyroid, and less frequently, of oral mucosa. Ocular manifestations of tetracycline and tetracycline derivatives-induced pigmentation are rare, and include scleral, retinal, and conjunctival pigmented deposits. Ocular manifestations usually appear after prolonged antibiotic use, but can be dose and duration independent. The mechanisms of pigmentation in various tissues differ, but typically include chelation with calcium or iron and oxidation of antibiotic to melanin-like pigment. Conjunctival deposits accumulate in pseudoglands of Henle possibly from degenerated conjunctival cells or their secretions. Microscopic findings. Pigmented and non-pigmented lamellated concretions are observed in pseudoglands of Henle. These concretions demonstrate yellow-green autofluorescence with blue light in unstained sections. Conjunctival concretions do not
Corneal specimens that influence clinical decisions
 Corneal specimens that influence clinical decisions Refractive surgery Corneal dystrophies Microbial infections J. Douglas Cameron, MD Chief, Ophthalmic Pathology Division Neuropathology Department Armed
Corneal specimens that influence clinical decisions Refractive surgery Corneal dystrophies Microbial infections J. Douglas Cameron, MD Chief, Ophthalmic Pathology Division Neuropathology Department Armed
Subject Index. Atopic keratoconjunctivitis (AKC) management 16 overview 15
 management 16 overview 15") Subject Index Acanthamoeba keratitis, see Infective keratitis Acute allergic conjunctivitis AKC, see Atopic keratoconjunctivitis Allergy acute allergic conjunctivitis 15 atopic keratoconjunctivitis 15
Subject Index Acanthamoeba keratitis, see Infective keratitis Acute allergic conjunctivitis AKC, see Atopic keratoconjunctivitis Allergy acute allergic conjunctivitis 15 atopic keratoconjunctivitis 15
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Autoimmune Diseases with Oral Manifestations
 Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
n Corneal epithelium is derived from surface ectoderm n Composed of stratified squamous epith. n 5% of total corneal thickness (50-90micro m thick)
") Cornea overview Dr. Sarita Tuladhar MD, Ophthalmology Gandaki Medical College Embryology CORNEA: n Corneal epithelium is derived from surface ectoderm n Corneal stroma, descement memb, bowman s layer,
Cornea overview Dr. Sarita Tuladhar MD, Ophthalmology Gandaki Medical College Embryology CORNEA: n Corneal epithelium is derived from surface ectoderm n Corneal stroma, descement memb, bowman s layer,
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Medical Affairs Policy
 Medical Affairs Policy Service: Corneal Treatments and Specialized Contact Lenses (Corneal remodeling, Corneal transplant, Corneal collagen crosslinking, Intrastromal Rings- INTACS, Keratoconus treatments,
Medical Affairs Policy Service: Corneal Treatments and Specialized Contact Lenses (Corneal remodeling, Corneal transplant, Corneal collagen crosslinking, Intrastromal Rings- INTACS, Keratoconus treatments,
Ocular Neoplasia What s Common? What s New? Richard R Dubielzig
 Ocular Neoplasia What s Common? What s New? Richard R Dubielzig Orbit 288 6% Tumors of the globe make up 3225 out of 6110 total neoplasms = 53%. Tumors of the conjunctiva make up 1192 out of 6110 total
Ocular Neoplasia What s Common? What s New? Richard R Dubielzig Orbit 288 6% Tumors of the globe make up 3225 out of 6110 total neoplasms = 53%. Tumors of the conjunctiva make up 1192 out of 6110 total
Degenerations. Conditions with cloudy cornea at birth or in infancy
 Dermoids The lesions are choristomas, which are congenital masses of tissue that have been dislocated from their normal position Limbal dermoids--overlapping the cornea and sclera, often inferotemporally
Dermoids The lesions are choristomas, which are congenital masses of tissue that have been dislocated from their normal position Limbal dermoids--overlapping the cornea and sclera, often inferotemporally
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Senile: flattening of vertical meridian, thinning of periphery, lack of luster
 Pterygia Etiology: triangular, fibrovascular, connective tissue overgrowths of bulbar conjunctiva onto cornea; distribution of ultraviolet energy- heat, wind, dust, dry atmosphere,higher prevalence nearer
Pterygia Etiology: triangular, fibrovascular, connective tissue overgrowths of bulbar conjunctiva onto cornea; distribution of ultraviolet energy- heat, wind, dust, dry atmosphere,higher prevalence nearer
CORNEAL CONDITIONS CORNEAL TRANSPLANTATION
 GENERAL INFORMATION CORNEAL CONDITIONS CORNEAL TRANSPLANTATION WHAT ARE CORNEAL CONDITIONS? The cornea is the clear outer layer of the eye. Shaped like a dome, it helps to protect the eye from foreign
GENERAL INFORMATION CORNEAL CONDITIONS CORNEAL TRANSPLANTATION WHAT ARE CORNEAL CONDITIONS? The cornea is the clear outer layer of the eye. Shaped like a dome, it helps to protect the eye from foreign
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pigmented lesions of the Oral cavity
 Oral medicine أ.م.د احسان عبد هللا كميل Pigmented lesions of the Oral cavity Pigmented oral lesions are a large group of disorders in which the dark or brown color is the essential clinical characteristic.
Oral medicine أ.م.د احسان عبد هللا كميل Pigmented lesions of the Oral cavity Pigmented oral lesions are a large group of disorders in which the dark or brown color is the essential clinical characteristic.
Atlas of Eyelid and Conjunctival Tumors
 Atlas of Eyelid and Conjunctival Tumors Jerry A. Shields, M.D. Director, Ocular Oncology Service Wills Eye Hospital Professor of Ophthalmology Thomas Jefferson University Philadelphia, Pennsylvania Carol
Atlas of Eyelid and Conjunctival Tumors Jerry A. Shields, M.D. Director, Ocular Oncology Service Wills Eye Hospital Professor of Ophthalmology Thomas Jefferson University Philadelphia, Pennsylvania Carol
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Among the benign intraepithelial melanocytic proliferations, Inflamed Conjunctival Nevi. Histopathological Criteria. Resident Short Reviews
 Resident Short Reviews Inflamed conjunctival nevi (ICN) may suggest malignancy because of their rapid growth and atypical histology. The objective of this study was to characterize the diagnostic features
Resident Short Reviews Inflamed conjunctival nevi (ICN) may suggest malignancy because of their rapid growth and atypical histology. The objective of this study was to characterize the diagnostic features
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Eye Care for Animals Micki Armour VMD DACVO THE CORNEA
 Eye Care for Animals Micki Armour VMD DACVO THE CORNEA ANATOMY 0.5-0.6mm thick 4 primary layers Epithelium (5-7 cell layers) Stroma (90% total thickness) Descemet s membrane Endothelium (1 layer) ANATOMY-
Eye Care for Animals Micki Armour VMD DACVO THE CORNEA ANATOMY 0.5-0.6mm thick 4 primary layers Epithelium (5-7 cell layers) Stroma (90% total thickness) Descemet s membrane Endothelium (1 layer) ANATOMY-
PAINFUL PAINLESS Contact lens user BOV
 Common Causes Allergies Infections Ocular Cornea, uveitis, endophthalmitis Orbital Orbital cellulitis Inflammation Uveitis Scleritis / episcleritis Glaucomas Trauma Foreign bodies Chemical injuries History
Common Causes Allergies Infections Ocular Cornea, uveitis, endophthalmitis Orbital Orbital cellulitis Inflammation Uveitis Scleritis / episcleritis Glaucomas Trauma Foreign bodies Chemical injuries History
Nasal mucosal melanosis may act as a harbinger of melanoma: A case report
 Nasal mucosal melanosis may act as a harbinger of melanoma: A case report The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters. Citation
Nasal mucosal melanosis may act as a harbinger of melanoma: A case report The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters. Citation
The Orbit. The Orbit OCULAR ANATOMY AND DISSECTION 9/25/2014. The eye is a 23 mm organ...how difficult can this be? Openings in the orbit
 The eye is a 23 mm organ...how difficult can this be? OCULAR ANATOMY AND DISSECTION JEFFREY M. GAMBLE, OD COLUMBIA EYE CONSULTANTS OPTOMETRY & UNIVERSITY OF MISSOURI DEPARTMENT OF OPHTHALMOLOGY CLINICAL
The eye is a 23 mm organ...how difficult can this be? OCULAR ANATOMY AND DISSECTION JEFFREY M. GAMBLE, OD COLUMBIA EYE CONSULTANTS OPTOMETRY & UNIVERSITY OF MISSOURI DEPARTMENT OF OPHTHALMOLOGY CLINICAL
Strategies for Anterior Segment Disease Management Mile Brujic, OD, FAAO 1409 Kensington Blvd Bowling Green, OH
 Strategies for Anterior Segment Disease Management Mile Brujic, OD, FAAO 1409 Kensington Blvd Bowling Green, OH 43402 brujic@prodigy.net 419-261-9161 Summary As optometry s scope of practice continues
Strategies for Anterior Segment Disease Management Mile Brujic, OD, FAAO 1409 Kensington Blvd Bowling Green, OH 43402 brujic@prodigy.net 419-261-9161 Summary As optometry s scope of practice continues
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY
 PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY") SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
Fitting Keratoconus and Other Complicated Corneas
 Fitting Keratoconus and Other Complicated Corneas Christine W Sindt OD FAAO Professor, Clinical Ophthalmology Director, Contact Lens Service University of Iowa Disclosure Consultant: ALCON Vision Care
Fitting Keratoconus and Other Complicated Corneas Christine W Sindt OD FAAO Professor, Clinical Ophthalmology Director, Contact Lens Service University of Iowa Disclosure Consultant: ALCON Vision Care
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Ocular Neoplasia CL Davis 9/08. Richard R Dubielzig
 Ocular Neoplasia CL Davis 9/08 Richard R Dubielzig 2135/5722 Canine Melanocytic Tumors Outside the Globe: 264 Conjunctival: 159 Eye Lid: 72 Skin: 33 Affecting the Globe: 1871 Anterior Uveal Melanocytoma:
Ocular Neoplasia CL Davis 9/08 Richard R Dubielzig 2135/5722 Canine Melanocytic Tumors Outside the Globe: 264 Conjunctival: 159 Eye Lid: 72 Skin: 33 Affecting the Globe: 1871 Anterior Uveal Melanocytoma:
A Case Report of Recurrent Conjunctival Squamous Cell Carcinoma M Zhao 1, W Lin 2 *, Z Liu 2 ABSTRACT
 A Case Report of Recurrent Conjunctival Squamous Cell Carcinoma M Zhao 1, W Lin 2 *, Z Liu 2 ABSTRACT A case of recurrent squamous cell carcinoma of the conjunctiva is presented here. A 13-yearsold male
A Case Report of Recurrent Conjunctival Squamous Cell Carcinoma M Zhao 1, W Lin 2 *, Z Liu 2 ABSTRACT A case of recurrent squamous cell carcinoma of the conjunctiva is presented here. A 13-yearsold male
Fleck. Pre-Descemet Dystrophies (generally good vision and comfort) Primary Pre-Descemet Dystrophy
 Primary Pre-Descemet Dystrophy") Fleck Etiology: bilateral, sometimes asymmetric, autosomal dominant opacities located in all levels of stroma as early as 1 st decade Slit lamp: well demarcated, small round gray-white doughnut-like, wreath-like
Fleck Etiology: bilateral, sometimes asymmetric, autosomal dominant opacities located in all levels of stroma as early as 1 st decade Slit lamp: well demarcated, small round gray-white doughnut-like, wreath-like
11/21/2016. Introduction. Diagnosis: Invasive mucosal melanoma. Mucosal melanoma diagnosis. Diagnosis: Invasive mucosal melanoma
 Introduction MUCOSAL MELANOMA AND PIGMENTED LESIONS OF MUCOSAL SURFACES Adriano Piris, M.D. Co-Director Mihm Cutaneous Pathology Consultative Service (MCPCS) Brigham and Women s Hospital, Harvard Medical
Introduction MUCOSAL MELANOMA AND PIGMENTED LESIONS OF MUCOSAL SURFACES Adriano Piris, M.D. Co-Director Mihm Cutaneous Pathology Consultative Service (MCPCS) Brigham and Women s Hospital, Harvard Medical
Conjunctivitis in Dogs
 Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Conjunctivitis in Dogs (Inflammation of the Moist Tissues of the Eye) Basics OVERVIEW
Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Conjunctivitis in Dogs (Inflammation of the Moist Tissues of the Eye) Basics OVERVIEW
CLINICAL PEARLS IN OCULAR ONCOLOGY
 CLINICAL PEARLS IN OCULAR ONCOLOGY IRIS NEVUS - Two kinds circumscribed and diffuse - Photodocumentation important to monitor growth - Risk Factors for iris nevus growth to melanoma (ABCDEF) A Age (young),
CLINICAL PEARLS IN OCULAR ONCOLOGY IRIS NEVUS - Two kinds circumscribed and diffuse - Photodocumentation important to monitor growth - Risk Factors for iris nevus growth to melanoma (ABCDEF) A Age (young),
a.superficial (adenoid layer).contain lymphoid tissue.
.contain lymphoid tissue.") Conjunctiva Dr. saifalshamarti Anatomy Microscopic: 1.Epithelium (non keratinized,includes goblet cell). 2.Epithelial basement membrane. 3.Stroma : a.superficial (adenoid layer).contain lymphoid tissue.
Conjunctiva Dr. saifalshamarti Anatomy Microscopic: 1.Epithelium (non keratinized,includes goblet cell). 2.Epithelial basement membrane. 3.Stroma : a.superficial (adenoid layer).contain lymphoid tissue.
PATIENT INFORMATION ON CORNEAL GRAFT
 PATIENT INFORMATION ON CORNEAL GRAFT (TRANSPLANT) SURGERY M ANANDAN What is the cornea? The clear window of the eye approximately 0.5mm thick and 12mm across. It lies in front of the fluid filled anterior
PATIENT INFORMATION ON CORNEAL GRAFT (TRANSPLANT) SURGERY M ANANDAN What is the cornea? The clear window of the eye approximately 0.5mm thick and 12mm across. It lies in front of the fluid filled anterior
FUCH S DYSTROPHY & CATARACT SURGERY TREATMENT ALGORITHM
 FUCH S DYSTROPHY & CATARACT SURGERY TREATMENT ALGORITHM ΙΟΑΝΝΙS Α. MALLIAS, MD, PHD Director of the Dept. of Ophthalmology, Mediterraneo Hospital, Glyfada, Athens, Greece Clinical Fellow in Cornea and
FUCH S DYSTROPHY & CATARACT SURGERY TREATMENT ALGORITHM ΙΟΑΝΝΙS Α. MALLIAS, MD, PHD Director of the Dept. of Ophthalmology, Mediterraneo Hospital, Glyfada, Athens, Greece Clinical Fellow in Cornea and
الطلاوة = Leukoplakia LEUKOPLAKIA
 LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
Ocular Pathology. I. Congenital and/or developmental. A. Trisomy 21. Hypertelorism (widely spaced eyes) Keratoconus (cone shaped cornea)
 Keratoconus (cone shaped cornea)") I. Congenital and/or developmental Robbins Pathologic Basis of Disease, 6 th Ed. A. Trisomy 21 Hypertelorism (widely spaced eyes) Keratoconus (cone shaped cornea) Focal hypoplasia of iris Cataracts frequently
I. Congenital and/or developmental Robbins Pathologic Basis of Disease, 6 th Ed. A. Trisomy 21 Hypertelorism (widely spaced eyes) Keratoconus (cone shaped cornea) Focal hypoplasia of iris Cataracts frequently
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Technicians & Nurses Program
 ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Meet Libby. Corneal Dysgenesis, Degeneration, and Dystrophies Definitions. Dr. Victor Malinovsky
 Meet Libby Corneal Dysgenesis, Degeneration, and Dystrophies 2006 Dr. Victor Malinovsky Definitions Dysgenesis: (congenital anomalies) A development disorder that results in a congenital malformation of
Meet Libby Corneal Dysgenesis, Degeneration, and Dystrophies 2006 Dr. Victor Malinovsky Definitions Dysgenesis: (congenital anomalies) A development disorder that results in a congenital malformation of
Histology of the Eye
 Histology of the Eye Objectives By the end of this lecture, the student should be able to describe: The general structure of the eye. The microscopic structure of:»cornea.»retina. EYE BULB Three coats
Histology of the Eye Objectives By the end of this lecture, the student should be able to describe: The general structure of the eye. The microscopic structure of:»cornea.»retina. EYE BULB Three coats
Unit I Problem 9 Histology: Basic Tissues of The Body
 Unit I Problem 9 Histology: Basic Tissues of The Body - What is the difference between cytology and histology? Cytology: it is the study of the structure and functions of cells and their contents. Histology:
Unit I Problem 9 Histology: Basic Tissues of The Body - What is the difference between cytology and histology? Cytology: it is the study of the structure and functions of cells and their contents. Histology:
04/09/2018. Squamous Cell Neoplasia and Precursor Lesions. Agenda. Squamous Dysplasia. Squamo-proliferative lesions. Architectural features
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
Conjunctivitis in Cats
 Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Conjunctivitis in Cats (Inflammation of the Moist Tissues of the Eye) Basics OVERVIEW
Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Conjunctivitis in Cats (Inflammation of the Moist Tissues of the Eye) Basics OVERVIEW
LENTIGO SIMPLEX. Epidemiology
 LENTIGO SIMPLEX Epidemiology The frequency of lentigo simplex in children and adults has not been determined. There does not appear to be a racial or gender predilection. Lentigo simplex is the most common
LENTIGO SIMPLEX Epidemiology The frequency of lentigo simplex in children and adults has not been determined. There does not appear to be a racial or gender predilection. Lentigo simplex is the most common
Dystrophies. Molecular Causes. Anterior Membrane Dystrophies (epithelium, basement membrane and Bowman s layer)
") Dystrophies Characteristics of corneal dystrophies About half the members of appropriate age to have the dystrophy( usually autosomal dominant): inherited Usually seen in the first or second decade of
Dystrophies Characteristics of corneal dystrophies About half the members of appropriate age to have the dystrophy( usually autosomal dominant): inherited Usually seen in the first or second decade of
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Distinction layer by layer. HRT II Rostock Cornea Module
 Distinction layer by layer HRT II Rostock Cornea Module Homogenously illuminated, undistorted images Movie capture Manual Pachymetry Epithelial and intra-corneal pachymetry Full corneal thickness Post-LASIK
Distinction layer by layer HRT II Rostock Cornea Module Homogenously illuminated, undistorted images Movie capture Manual Pachymetry Epithelial and intra-corneal pachymetry Full corneal thickness Post-LASIK
Course # Cutting Edge Cornea
 Course # 061 Cutting Edge Cornea 44 year old female with sudden onset right eye pain. Has happened 3 times previouslyevery time first thing in the morning Cutting Edge Cornea Terri Kim, M.D. Chairman,
Course # 061 Cutting Edge Cornea 44 year old female with sudden onset right eye pain. Has happened 3 times previouslyevery time first thing in the morning Cutting Edge Cornea Terri Kim, M.D. Chairman,
Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease:
 4. Associated with systemic disease:") Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease: Hematological GIT Behcet s HIV 5. Associated with dermatological diseases:
Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease: Hematological GIT Behcet s HIV 5. Associated with dermatological diseases:
Histopathology of Melanoma
 THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
Nasreen A. Syed, MD F.C. Blodi Eye Pathology Laboratory University of Iowa
 Nasreen A. Syed, MD F.C. Blodi Eye Pathology Laboratory University of Iowa No financial disclosures No discussion of off-label use of medications or unapproved devices 67 year old male referred to Oculoplastics
Nasreen A. Syed, MD F.C. Blodi Eye Pathology Laboratory University of Iowa No financial disclosures No discussion of off-label use of medications or unapproved devices 67 year old male referred to Oculoplastics
SEBACEOUS NEOPLASMS. Dr. Prachi Saraogi Clinical Fellow in Dermatology
 SEBACEOUS NEOPLASMS Dr. Prachi Saraogi Clinical Fellow in Dermatology Sebaceous neoplasms Sebaceous adenoma (Benign) Sebaceous carcinoma (Malignant) SEBACEOUS ADENOMA Benign tumours composed of incompletely
SEBACEOUS NEOPLASMS Dr. Prachi Saraogi Clinical Fellow in Dermatology Sebaceous neoplasms Sebaceous adenoma (Benign) Sebaceous carcinoma (Malignant) SEBACEOUS ADENOMA Benign tumours composed of incompletely
LARYNGEAL DYSPLASIA. Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital
 LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
Journal of Ophthalmic Medical Technology. Fuchs Dystrophy Amy Hischier
 Journal of Ophthalmic Medical Technology Volume 8, Number 1 October 2013 www.jomtonline.com Fuchs Dystrophy Amy Hischier Patient History: A 55 year old female complained that both of her eyes were red,
Journal of Ophthalmic Medical Technology Volume 8, Number 1 October 2013 www.jomtonline.com Fuchs Dystrophy Amy Hischier Patient History: A 55 year old female complained that both of her eyes were red,
Technicians & Nurses Program
 ASCRS ASOA Symposium & Congress Technicians & Nurses Program April 17-21, 2015 San Diego, California Clinical-Pathological Correlation of Common Periocular Lesions Todd Mondzelewski, MD Comprehensive Ophthalmology
ASCRS ASOA Symposium & Congress Technicians & Nurses Program April 17-21, 2015 San Diego, California Clinical-Pathological Correlation of Common Periocular Lesions Todd Mondzelewski, MD Comprehensive Ophthalmology
ICD-10-CM Cornea. Type RT LT OU SINGLE CODE UNSPECIFIED. Acute atopic conjunctivitis H10.11 H10.12 H10.13 X H10.10
 ICD-10-CM Cornea Conjunctiva Acute atopic conjunctivitis H10.11 H10.12 H10.13 H10.10 Acute chemical conjunctivitis H10.211 H10.212 H10.213 H10.219 Acute conjunctivitis, unspecified H10.31 H10.32 H10.33
ICD-10-CM Cornea Conjunctiva Acute atopic conjunctivitis H10.11 H10.12 H10.13 H10.10 Acute chemical conjunctivitis H10.211 H10.212 H10.213 H10.219 Acute conjunctivitis, unspecified H10.31 H10.32 H10.33
Childhood corneal neovascularization
 Miltos Balidis PhD, FEBOphth, ICOphth Sotiria Palioura MD,PhD Childhood corneal neovascularization Opacities Cornea clarity is essential for optimal vision at any age. In childhood, loss of corneal transparency
Miltos Balidis PhD, FEBOphth, ICOphth Sotiria Palioura MD,PhD Childhood corneal neovascularization Opacities Cornea clarity is essential for optimal vision at any age. In childhood, loss of corneal transparency
Anatomic Divisions. Ocular Surface. Intraocular. Orbital. Lacrimal. Eyelid
 Anatomic Divisions Ocular Surface Intraocular Orbital Lacrimal Eyelid Ocular Surface Melanocytic Squamous Neoplasia Lymphoid Melanocytic Nevi PAM (Primary Acquired Melanosis) Ocular Melanocytosis Melanoma
Anatomic Divisions Ocular Surface Intraocular Orbital Lacrimal Eyelid Ocular Surface Melanocytic Squamous Neoplasia Lymphoid Melanocytic Nevi PAM (Primary Acquired Melanosis) Ocular Melanocytosis Melanoma
Healing & Repair. Tissue Regeneration
 Healing & Repair Dr. Srikumar Chakravarthi Repair & Healing: Are they same? Repair :Regeneration of injured cells by cells of same type, as with regeneration of skin/oral mucosa (requires basement membrane)
Healing & Repair Dr. Srikumar Chakravarthi Repair & Healing: Are they same? Repair :Regeneration of injured cells by cells of same type, as with regeneration of skin/oral mucosa (requires basement membrane)
NEW OPPORTUNITIES OF USING THERAPEUTICAL CONTACT LENSES IN OCULAR SURGERY
 NEW OPPORTUNITIES OF USING THERAPEUTICAL CONTACT LENSES IN OCULAR SURGERY Authors: Prof univ. dr. Adriana Stănilă, Dr. Elena Mihai, Dr. Adrian Teodoru, Dr. IonuŃ Costache The Clinical Department of Op
NEW OPPORTUNITIES OF USING THERAPEUTICAL CONTACT LENSES IN OCULAR SURGERY Authors: Prof univ. dr. Adriana Stănilă, Dr. Elena Mihai, Dr. Adrian Teodoru, Dr. IonuŃ Costache The Clinical Department of Op
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Skin and Body Membranes Body Membranes Function of body membranes Cover body surfaces Line body cavities Form protective sheets around organs
 Skin and Body Membranes Body Membranes Function of body membranes Cover body surfaces Line body cavities Form protective sheets around organs Classification of Body Membranes Epithelial membranes Cutaneous
Skin and Body Membranes Body Membranes Function of body membranes Cover body surfaces Line body cavities Form protective sheets around organs Classification of Body Membranes Epithelial membranes Cutaneous
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Diploma examination. Dermatopathology: First paper. Tuesday 21 March Candidates must answer FOUR questions ONLY. Time allowed: Three hours
 Dermatopathology: First paper Tuesday 21 March 2017 1. Discuss the role of fluorescent in-situ hybridization (FISH) and emerging molecular techniques in the diagnosis of cutaneous melanocytic lesions,
Dermatopathology: First paper Tuesday 21 March 2017 1. Discuss the role of fluorescent in-situ hybridization (FISH) and emerging molecular techniques in the diagnosis of cutaneous melanocytic lesions,
Clinically Microscopically Pathogenesis: autoimmune not lifetime
 Vulvar Diseases: Can be divided to non-neoplastic and neoplastic diseases. The neoplastic diseases are much less common. Of those, squamous cell carcinoma is the most common. most common in postmenopausal
Vulvar Diseases: Can be divided to non-neoplastic and neoplastic diseases. The neoplastic diseases are much less common. Of those, squamous cell carcinoma is the most common. most common in postmenopausal
Dysplasia, Mimics and Other Controversies
 Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Ocular Anatomy for the Paraoptometric
 Ocular Anatomy for the Paraoptometric Minnesota Optometric Association Paraoptometric CE Friday September 30, 2016 Lindsay A. Sicks, OD, FAAO Assistant Professor, Illinois College of Optometry lsicks@ico.edu
Ocular Anatomy for the Paraoptometric Minnesota Optometric Association Paraoptometric CE Friday September 30, 2016 Lindsay A. Sicks, OD, FAAO Assistant Professor, Illinois College of Optometry lsicks@ico.edu
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT
 LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
What are some common conditions that affect the cornea?
 What are some common conditions that affect the cornea? Injuries After minor injuries or scratches, the cornea usually heals on its own. Deeper injuries can cause corneal scarring, resulting in a haze
What are some common conditions that affect the cornea? Injuries After minor injuries or scratches, the cornea usually heals on its own. Deeper injuries can cause corneal scarring, resulting in a haze
Amniotic Membrane Transplantation In Ocular Surface Disorders
 Orginal Article Amniotic Membrane Transplantation In Ocular Surface Disorders Khalid Iqbal Talpur, Faiz Muhammad Halepota, Muhammad Pak J Ophthalmol 2005, Vol. 22 No. 3.................................................................................................
Orginal Article Amniotic Membrane Transplantation In Ocular Surface Disorders Khalid Iqbal Talpur, Faiz Muhammad Halepota, Muhammad Pak J Ophthalmol 2005, Vol. 22 No. 3.................................................................................................
Skin and Body Membranes
 4 Skin and Body Membranes PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB Skin and Body Membranes
4 Skin and Body Membranes PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB Skin and Body Membranes
Chapter 6 Squamous Cell Carcinoma: Variants and Challenges
 Chapter 6 Squamous Cell Carcinoma: Variants and Challenges Michael B. Morgan EPIDEMIOLOGY: Second most common skin cancer, rare in the dark-skinned races. ETIOLOGY: Ultraviolet light, HPV infection. PATHOGENESIS:
Chapter 6 Squamous Cell Carcinoma: Variants and Challenges Michael B. Morgan EPIDEMIOLOGY: Second most common skin cancer, rare in the dark-skinned races. ETIOLOGY: Ultraviolet light, HPV infection. PATHOGENESIS:
Therapy of melanocytic conjunctival tumors
 DOI: 10.4149/BLL_2013_093 Bratisl Lek Listy 2013; 114 (8) CLINICAL STUDY Therapy of melanocytic conjunctival tumors Halas M Jr 1, Svetlosakova Z 1, Babal P 2 Department of Ophthalmology, Comenius University,
DOI: 10.4149/BLL_2013_093 Bratisl Lek Listy 2013; 114 (8) CLINICAL STUDY Therapy of melanocytic conjunctival tumors Halas M Jr 1, Svetlosakova Z 1, Babal P 2 Department of Ophthalmology, Comenius University,
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE DOCTORAL THESIS SUMMARY
 UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE DOCTORAL THESIS SUMMARY CLINICAL, HISTOPATHOLOGICAL AND IMMUNOHISTOCHEMICAL STUDY OF THE EPITHELIAL PRECANCEROUS LESIONS PRECURSORS OF
UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE DOCTORAL THESIS SUMMARY CLINICAL, HISTOPATHOLOGICAL AND IMMUNOHISTOCHEMICAL STUDY OF THE EPITHELIAL PRECANCEROUS LESIONS PRECURSORS OF
Lymphoid System: cells of the immune system. Answer Sheet
 Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT
 Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Premalignant lesions may expose to a promoting. factor & may be induced to undergo malignant. Carcinoma in situ displays the cytologic features of
 بسم رلاهللا Def. Premalignant lesions may expose to a promoting factor & may be induced to undergo malignant transformation. Carcinoma in situ displays the cytologic features of malignancy without invasion
بسم رلاهللا Def. Premalignant lesions may expose to a promoting factor & may be induced to undergo malignant transformation. Carcinoma in situ displays the cytologic features of malignancy without invasion
Introduction to Pemphigoid: Spectrum of Disease & Treatment
 Introduction to Pemphigoid: Spectrum of Disease & Treatment A Razzaque Ahmed, MD Center for Blistering Diseases Boston, MA A.Razzaque.Ahmed@tufts.edu centerforblisteringdiseases.com SPECTRUM OF PEMPHIGOID
Introduction to Pemphigoid: Spectrum of Disease & Treatment A Razzaque Ahmed, MD Center for Blistering Diseases Boston, MA A.Razzaque.Ahmed@tufts.edu centerforblisteringdiseases.com SPECTRUM OF PEMPHIGOID
Diseases of the vulva
 Diseases of the vulva 1. Bartholin Cyst - Infection of the Bartholin gland produces an acute inflammation within the gland (adenitis) and may result in an abscess. Bartholin duct cysts - Are relatively
Diseases of the vulva 1. Bartholin Cyst - Infection of the Bartholin gland produces an acute inflammation within the gland (adenitis) and may result in an abscess. Bartholin duct cysts - Are relatively
Principles of Anatomy and Physiology
 Principles of Anatomy and Physiology 14 th Edition CHAPTER 5 The Integumentary System Introduction The organs of the integumentary system include the skin and its accessory structures including hair, nails,
Principles of Anatomy and Physiology 14 th Edition CHAPTER 5 The Integumentary System Introduction The organs of the integumentary system include the skin and its accessory structures including hair, nails,
LESIONS OF THE ORAL CAVITY ORAL CAVITY. Oral Cavity Subsites 4/10/2013 LIPS TEETH GINGIVA ORAL MUCOUS MEMBRANES PALATE TONGUE ORAL LYMPHOID TISSUES
 LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
Ocul Oncol Pathol 2015;1:
 Received: November 19, 2014 Accepted after revision: January 9, 2015 Published online: April 1, 2015 2296 4681/15/0014 0231$39.50/0 Case Series and Brief Reports Unilateral Conjunctival in situ Squamous
Received: November 19, 2014 Accepted after revision: January 9, 2015 Published online: April 1, 2015 2296 4681/15/0014 0231$39.50/0 Case Series and Brief Reports Unilateral Conjunctival in situ Squamous
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Ulcerative Keratitis (Type of Inflammation of the Cornea) Basics
 Basics") Ulcerative Keratitis (Type of Inflammation of the Cornea) Basics OVERVIEW Keratitis is inflammation of the cornea; the cornea is the clear outer layer of the front of the eye The corneal epithelium is
Ulcerative Keratitis (Type of Inflammation of the Cornea) Basics OVERVIEW Keratitis is inflammation of the cornea; the cornea is the clear outer layer of the front of the eye The corneal epithelium is
John Rawstron Christchurch 2015
 John Rawstron Christchurch 2015 John Rawstron Christchurch 2015 Nasal and temporal pterygiae (medial and lateral) pingueculum Body Neck Head Cap/hood Iles de Fuchs Stocker s line Pathogenesis UV light
John Rawstron Christchurch 2015 John Rawstron Christchurch 2015 Nasal and temporal pterygiae (medial and lateral) pingueculum Body Neck Head Cap/hood Iles de Fuchs Stocker s line Pathogenesis UV light
Actinic keratosis (AK): Dr Sarma s simple guide
: Dr Sarma s simple guide") Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
CONJUNCTIVA NON NEOPLASTIC LESIONS
 CONJUNCTIVA NON NEOPLASTIC LESIONS Anat Stemmer-Rachamimov, MD Neuropathology Department Massachusetts General Hospital Boston, MA Learning objectives: 1) Review the normal histology and physiology of
CONJUNCTIVA NON NEOPLASTIC LESIONS Anat Stemmer-Rachamimov, MD Neuropathology Department Massachusetts General Hospital Boston, MA Learning objectives: 1) Review the normal histology and physiology of
COMBINED NEVI are composed
 CLINICAL SCIENCES Combined Nevi of the Conjunctiva J. rooks Crawford, MD; Edward L. Howes, Jr, MD; Devron H. Char, MD Objective: To report the clinical and histologic features of combined nevi of the conjunctiva,
CLINICAL SCIENCES Combined Nevi of the Conjunctiva J. rooks Crawford, MD; Edward L. Howes, Jr, MD; Devron H. Char, MD Objective: To report the clinical and histologic features of combined nevi of the conjunctiva,