VII convegno nazionale fondazione AMD Baveno23-25 ottobre 2014
|
|
|
- Walter Heath
- 5 years ago
- Views:
Transcription

1 VII convegno nazionale fondazione AMD Baveno23-25 ottobre 2014 SUBITO DE disfunzioni sessuali e rischio cardiovascolare. Il ruolo dell ipogonadismo Giovanni Corona MD, PhD Endocrinology Unit Medical Department, Ospedale Maggiore Bologna, Italy jocorona@libero.it

2 Subito-DE study The SUBITO-DE study is an observational, multicenter, prospective study involving 27 Italian diabetes centers. Male patients recently diagnosed with T2DM were consecutively interviewed by their attending physician at the diabetes care centers and asked whether they had experienced a change in their sexual function or found it unsatisfactory. Those responding positively were then invited to participate in the study
3 Corona et al J Endocrinol Invest 2013;36:868
4 Screening: Do you suffer from any sexual dysfunction? yes No Would you want to discuss the problem? Stop Yes: V1 No: Stop 18 months of follow up V2
5 Data analyzed General characteristics of the subject Smoking and alcohol consumption Clinical history Depressive symptoms ( CES- D) Assessment of ED severity ( IIEF -EF ) Clinical history of DE ( treatment, response to treatment ). Evaluation of ejaculatory disorders, and sexual desire Evaluation of suspected androgen deficiency defined on the basis of ANDROTEST and Testosterone levels
6 North Investigator Emanuele Fraticelli Gianpaolo Magro Carlo B.Giorda Annamaria Chiambretti/Riccardo Fornengo Giorgio Viviani Andrea Corsi /Alberto Aglialoro Gianpaolo Testori Donatella Zavaroni Roberto Mingardi Alessandra Sforza/Giovanni Corona Centre Bra (CN) Cuneo Chieri (TO) Chivasso (TO) Genova Genova Milano Piacenza Vicenza Bologna
7 Centre Investigator Fabio Baccetti Sergio Leotta Rocco Bulzomi Angela Sabbatini Lelio Morviducci Centre Massa Carrara Roma Roma Palestrina (RM) Roma
8 South Investigator Rossella Iannarelli Vincenzo Paciotti Andrea Del Buono Gerardo Corigliano Gennaro Clemente Luciano Improta Salvatore Turco Sandro Gentile Stefano Albano/Marcello Sciaraffia Pietro Pata Domenico Cucinotta Carmelo De Francesco Centre l'aquila Avezzano (AQ) Cellola (CE) Napoli Salerno Santagnello (NA) Napoli Napoli Taranto Messina Messina Messina
 Mean age 58.8±8.")
9 2 Milano Chivasso Vicenza Torino Piacenza Bra Bologna Cuneo Genova Massa Carrara 2 27 centre involved Patients screened=1503 Patients enrolled=499 (33%) Mean age 58.8±8.8 years 3 Roma Palestrina L Aquila Avezzano Cellole 4 Napoli Salerno Taranto 3 Messina
10 N. pz screened n=1503 N= % N= % N= % No ED ED Agree to be involved Not aggred

11 Type 1 diabetes Type 2 diabetes Age Total n. subjects %ED Total n. subjects %ED Fedele et al Int J Epidemiol 2000;29: 524

12 Yamada et al PLOS one 2012;7: e43763
13 Yamada et al PLOS one 2012;7: e43763
14 Yamada et al PLOS one 2012;7: e43763
15 Yamada et al PLOS one 2012;7: e43763
16 What is the role of hypogonadism in T2DM CV risk?

17 2013 J Sex Med. 2013;10:245.
18 Recommendation 1: Definition of Testosterone Deficiency (TD) -TD is a clinical AND biochemical syndrome associated with age and comorbidities, and characterized by a deficiency of testosterone and relevant symptoms. It may affect the function of multiple organ systems, and result in significant detriment in the quality of life, including alterations in sexual function (EBMl 2). -TD results from defects at various levels of the hypothalamuspituitary-testes axis: abnormality in the testes (primary TD), pituitary or hypothalamic failure (secondary or tertiary TD) or a combination of the two (mixed TD) (EBMl1). TD may also result from an impairment of T action because of decreased bioavailability of the hormone (due to SHBG variations) or because of androgen receptor alterations (EBMl2). Buvat et al., J Sex Med. 2013;10:245
19 Recommendation 7: Threshold levels for the biochemical diagnosis of TD There are no generally accepted lower limits of normal total testosterone. There is, however, general agreement that: TT > 12 nmol/l (3.5 ng/ml or 350 ng/dl) does not usually require substitution (EBMI1) Based on the data of young hypogonadal men, men with TT < 8 nmol/l (2.3 ng/ml or 230 ng/dl) usually benefit from T treatment (EBMI1) Between these levels: measuring FT by equilibrium dialysis or calculating it from TT and SHBG levels may be helpful in case of TT between 8 and 12 nmol/l. A lower limit of 225 pmol/l (65 pg/ml) is accepted by many (EBMI3) A Testosterone Therapy trial for 3-6 months may be envisaged in those patients who are symptomatic, while alternative causes of the symptoms have been excluded (EBMI5). Beyond that time, T therapy would be continued only in case of substantial benefit Buvat et al., J Sex Med. 2013;10:245
20 Measurement of bioactive or free testosterone

21 Corona et al., Int J Androl. 2011;34:528
22 RANDOM-EFFECTS POOLED MEAN DIFFERENCE OF TOTAL TESTOSTERONE BETWEEN T2DM CASES AND CONTROLS FROM CROSS-SECTIONAL STUDIES All=27 Source Daubresse et al., 1978 Shahwan et al., 1978 Andò et al., 1984 Phillips, 1984 Small et al., 1987 Semple et al., 1988 Barret-Connor et al., 1990 Barret-Connor, 1992 Andersson et al., 1994 Tibblin et al., 1996 Defay et al., 1998* Defay et al., 1998** Chearskul et al., 2000 Jang et al., 2001 Zietz et al., 2000 Abou-Seif et al., 2001 Corrales et al., 2004 Svartberg et al., 2004 Achemlal et al., 2005 Chen et al., 2005 Pitteloud et al., 2005 Crawford et al., 2007 Selvin et al., 2007 Ibanez et al., 2008 OVERALL NO ED Daubresse et al., 1978 Shahwan et al., 1978 Corona et al., 2004 Corona et al., 2005 Rhoden et al., 2005 Hamdan et al., 2008 OVERALL ED OVERALL Overall -15,00 TT mean differences (nmol/l) ,00-5,00 0,00 5,00 10,00 Diff. in means LL, 95% CI UL, 95% CI -4,60-9,85 0,65-3,40-10,62 3,82-3,20-7,72 1,32-1,60-5,91 2,71-4,80-8,54-1,06-0,70-3,99 2,59-1,50-2,74-0,26-2,70-4,76-0,64-6,60-11,96-1,24-2,30-4,03-0,57-6,70-11,14-2,26-3,80-5,64-1,96-3,70-6,34-1,06-2,90-5,44-0,36-2,50-3,06-1,94-4,09-4,86-3,32-2,40-6,19 1,39-2,00-3,38-0,62 1,70-1,45 4,85-2,10-3,91-0,29-4,90-8,07-1,73-3,30-4,20-2,40-3,60-5,89-1,31-9,70-13,71-5,69-3,00-3,61-2,38-1,00-6,06 4,06-2,75-9,21 3,71-6,50-7,67-5,33-2,10-3,02-1,18-1,92-3,10-0,74-1,60-6,58 3,38-2,96-5,18-0,73-2,99-3,59-2, TT lower in cases TT higher in controls Corona et al., Int J Androl. 2011;34:528
23 Corona et al., J Sex Med 2014;11:2065
24 Total Testosterone (ng/ml) Prevalence of hypogonadism 4 < < < %
25


26 Sweden Malmo Eight Countries/Cities in the European Male Ageing Study Estonia Tartu U.K. Manchester Russia Poland Lodz Belgium Leuven France Germany Hungary Szeged Spain Santiago Italy Florence n=3369
27 Wu et al., N Engl J Med. 2010;363:123
28 Testosterone totale (ng/ml) Prevalence of hypogonadism EMAS 4 < < < %
29 Testosterone and type 2 diabetes mellitus 1. Hypogonadism is associated with T2DM
30 What about pre-diabetes conditions?
31 Glucose abnormalities in a consecutive series of 4351 patients with ED IFG/DM 2.1% No IFG/DM Established DM Newly diagnosed DM IFG ( mg/dl) 59.2% 40.8% 19.6% 13.5% IFG ( mg/dl) 5.6% Corona et al J Sex Med. 2012;9:1669
32 % ANDROTEST score Total Testosterone (nomol/l) cft (nomol/l) Adj. r=-0.052; p=0.006 Adj. r=-0.054; p= TT < 8 nm TT < 10.4 nm TT < 12 nm Adj. r=0.053; p< < New ly Established 5 diagnosed Glycemia mg/dl DM < New ly Established diagnosed Glycemia mg/dl DM Corona et al J Sex Med. 2012;9:1669
33 Testosterone and type 2 diabetes mellitus 1. Hypogonadism is associated with MetS and T2DM 2. Hypogonadism is associated with pre-diabetic conditions
34 RANDOM-EFFECTS MODEL OF TOTAL TESTOSTERONE IN INCIDENT CASES OF T2DM IN PROSPECTIVE STUDIES Source -6,000 TT mean differences (nmol/l) -5,000-4,000-3,000-2,000-1,000 0,000 1, Diff. in means LL, 95% CI UL, 95% CI Haffner et al., ,700-2,037 0,637 Tibbling et al., ,700-5,501-1,899 Stellato et al., ,100-4,571-1,629 Laaksonen et al., ,600-4,462-0,738 OVERALL ,456-3,845-1,066 TT Favorable TT Adverse Corona et al., Int J Androl. 2011;34:528
35 Testosterone and type 2 diabetes mellitus 1. Hypogonadism is associated with MetS and T2DM 2. Hypogonadism is associated with pre-diabetic conditions 3. Hypogonadism predicts T2DM but T2DM predicts hypogonadism

36 Who came first? MetS Hypogonadism
37 Corona et al., J Endocrinol Invest. 2011;34:557.
38 Does hypogonadism increase CV risk?
39 Corona et al., Eur J Endocrinol. 2011;165:687
40 Weighted differences (with 95% confidence interval [CI]) of mean total testosterone between non-angiographically documented CHD and controls from cross-sectional studies Source Poggi et al., 1976 Ben-Halim etal., 1978 Entrican et al., 1978 Luria et al., 1982 Labropoulos et al., 1982 Labropoulos et al., 1982* Zumoff et al., 1982* Phillips et al., 1983 Aksut etal., 1986 Aksut et al., 1986* Franzen et al., 1986 Franzen et al., 1986* Lichatenstein et al., 1987 Small et al., 1987 Phillips et al., 1988 Barrett-Connor et al., 1988 Sewdarsen et al., 1990 Hauner et al., 1991 Rice et al., 1993 Hautanen et al., 1994 Marques-Vidal et al., 1995 Phillips et al., 1996 Tripathi et al., 1998* Tripathi et al., 1998** Tripathi et al., 1998*** Chearskul et al., 2000 Mikulec et al., 2004 Cao et al., 2010 Overall CHD non-angio documented TT mean differences (nmol/l) ,00-15,00-10,00-5,00 0,00 5,00 10,00 Diff. in mean LL, 95% CI UL, 95% CI -8,75-13,91-3,59 0,00-2,94 2,94 2,35-0,31 5,01 1,32-4,06 6,70 3,00 0,27 5,73 1,80-0,38 3,98 1,46-1,43 4,35 0,80-0,86 2,46-6,36-8,63-4,10-7,16-10,03-4,28 3,00 0,57 5,43 2,00-0,43 4,43-1,10-1,81-0,39-3,30-7,12 0,52-0,69-2,57 1,18-0,04-1,18 1,10-1,51-2,64-0,38-1,40-2,85 0,05-2,15-3,53-0,76 0,50-1,71 2,71-0,40-1,95 1,15 2,64-2,01 7,29-13,85-15,68-12,02-13,43-14,97-11,89-13,56-15,59-11,53-5,81-7,92-3,70 0,31-0,77 1,39-4,06-5,30-2,82-2,33-3,99-0,68 Overall CHD non-angio-documented Favours CHD Favors no CHD Corona et al., Eur J Endocrinol. 2011;165:687
41 Weighted differences (with 95% confidence interval [CI]) of mean total testosterone between angiographically documented CHD and controls from cross-sectional studies Source TT mean differences (nmol/l) ,00-10,00-5,00 0,00 5,00 10,00 Diff. in mean LL, 95% CI UL, 95% CI Luria et al., 1982 * 2,99-0,42 6,39 Zumoff et al., ,90-5,87 2,07 Barth et al., ,70-9,36-2,04 Hromadova et al., ,21-10,85-3,57 Sewdarsen et al., ,00-7,56-2,44 Chute et al., ,76-7,86-1,66 Hamalainen et al., ,70-4,36 2,96 Sewdarsen et al., ,80-6,88-0,72 Slowinska-Srzednicka et al., ,06-7,32 1,20 Zhao et al., ,56-7,80-3,32 Kabakci et al., ,74-0,28 3,76 English et al., ,00-4,09 0,09 Dobrzycki et al., ,30-11,97-6,63 Dunajska et al., ,60-7,25 0,05 Dunajska et al., 2004* -2,36-5,23 0,51 Fischer et al., ,60-2,08 0,88 Davoodi et al., ,78-0,64 2,20 He et al., ,28-2,08 1,53 Mohamad et al., ,50-6,48-2,52 Mohamad et al., 2007* -1,40-3,76 0,96 Turhan et al., ,48-5,76-1,20 Fallah et al., ,78-0,64 2,20 Overall Overall CHD CHD angio-documented -2, , , Favours CHD Favors no CHD Corona et al., Eur J Endocrinol. 2011;165:687
42 Weighted differences (with 95% confidence interval [CI]) of mean total testosterone between other CVD and controls from cross-sectional studies Source TT mean differences (nmol/l) ,00-12,00-10,00-8,00-6,00-4,00-2,00 0,00 2,00 4,00 Diff. in mean LL, 95% CI UL, 95% CI Taggart et al., ,10-2,15 2,35 Foresta et al., ,49-8,60-2,37 Elwan et al., ,87-4,67 2,93 Dash et al., ,60-12,26-0,94 Jeppesen et al., ,70-4,56-0,84 Price et al., ,30-3,52 0,92 Demirbag et al., ,02-11,73-4,31 Page et al., ,40-2,28-0,52 Overall other CVD Overall other CVD -2,71-4,26-1,15 Favours other CVD Favors no other CVD Corona et al., Eur J Endocrinol. 2011;165:687
43 Testosterone and type 2 diabetes mellitus 1. Hypogonadism is associated with MetS and T2DM 2. Hypogonadism is associated with pre-diabetic conditions 3. Hypogonadism predicts T2DM but T2DM predicts hypogonadism 4. Having MACE decreases T by 2-3 nmoles/l
44 Is any relationship with incident CV diasese?
45 Baseline weighted differences (with 95% confidence interval) of mean total testosterone (TT) between patients with incident overall mortality and controls TT mean differences (nmol/l) Source Diff. in mean LL, 95% CI UL, 95% CI Letonen et al., ,90-5,39-0,41 Khaw et al., ,90-1,38-0,42 Corona et al., ,10-3,87-0,33 OVERALL -1,53-2,69-0,37 Higher ovreall mortality Lower overall mortality Corona et al., Eur J Endocrinol. 2011;165:1
46 Baseline weighted differences (with 95% confidence interval) of mean total testosterone (TT) between patients with incident CV mortality and controls TT mean differences (nmol/l) Source Diff. in mean LL, 95% CI UL, 95% CI -7,00-6,00-5,00-4,00-3,00-2,00-1,00 0,00 1,00 Barrett-Connor et al., ,61-1,86 0,64 Khaw et al., ,00-1,66-0,34 Corona et al., ,00-6,53 0,53 OVERALL -0,97-1,55-0,40 Higher any CVD mortality Lower any CVD mortality Corona et al., Eur J Endocrinol. 2011;165:1
47 Baseline weighted differences (with 95% confidence interval) of mean total testosterone (TT) between patients with incident MACE and controls TT mean differences (nmol/l) Source Diff. in mean LL, 95% CI UL, 95% CI -12,00-10,00-8,00-6,00-4,00-2,00 0,00 2,00 4,00 Cauley et al., 1987 Phillips et al., 1988 Contoreggi et al., 1990 Yarnell et al., 1993 Hautanen et al 1994 Mikulec et al., 2004 Yeap et al., 2009 Corona et al., 2010 Overall 0,60-1,47 2,67-0,69-2,83 1,44 0,35-1,79 2,49 0,10-1,19 1,39 0,50-1,71 2,71-10,10-10,77-9,44-1,00-2,02 0,02-0,70-1,85 0,45-1,40-5,23 2,44 Higher any CVD incidence Lower any CVD incidence Corona et al., Eur J Endocrinol. 2011;165:1
48 Testosterone and type 2 diabetes mellitus 1. Hypogonadism is associated with MetS and T2DM 2. Hypogonadism is associated with pre-diabetic conditions 3. Hypogonadism predicts T2DM but T2DM predicts hypogonadism 4. Having MACE decreases T by 2-3 nmoles/l 5. T is associated with incident overall and CV mortality but not incident MACE in longitudinal studies
49 Any data in DM?
50 Subito DE: V2 data N= % N=43 N=6 8.2% 1.2% No V2 Yes V2 Dead Lost at follow up
51 V2 data: incident events N=43 8.2% N= % N=6;1.2% N=25; 5.6% N=15; 3.3% Dyslipidemia No V2 Yes V2 Arterial hypertension MACE
52 VERY HIGH DOSE OF TRT. CV-related events in: 4 of 14 subjects (29%) with T levels > 1000 ng/dl 7 of 46 subjects (15%) with T levels < 500 ng/dl COMPOSITE RISK FOR ADVERSE EVENTS (including peripheral oedema) ELDERLY MEN WITH LIMITED MOBILITY


53 Vigen et al., JAMA. 2013; 310:1829
54 Kaplan-Meier Survival Curves With Testosterone Therapy Evaluated as a Time-Varying Covariate Vigen et al., JAMA. 2013; 310:1829
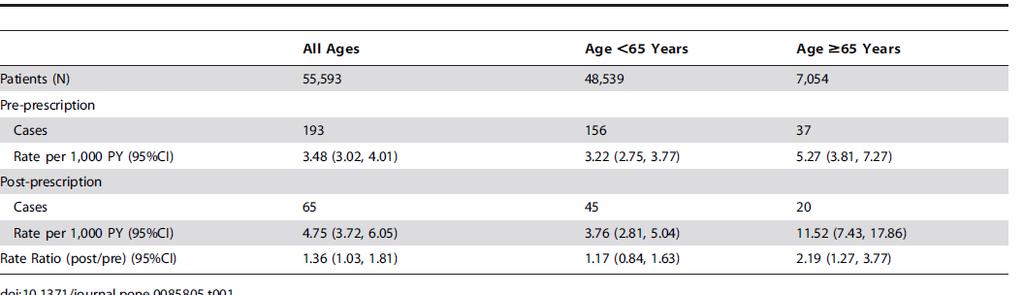
55 Cohort study of the risk of acute non-fatal myocardial infarction (MI) following an initial TT prescription (N = 55,593) in a large health-care database. Incidence rate of MI in the 90 days following the initial prescription (postprescription interval) compared with the rate in the one year prior to the initial prescription (pre-prescription interval) (post/pre). Finkle et al., PLoS ONE. 2014; 9: e85805
56
57


58 testosterone & heart Is testosterone administration associated with incidence of composite CV events? BMC Med. 2013; 11: 108. Published online 2013 April 18. doi: / PMCID: PMC Testosterone therapy and cardiovascular events among men: a systematic review and meta-analysis of placebo-controlled randomized trials Lin Xu, 1 Guy Freeman, 1 Benjamin J Cowling, 1 and C Mary Schooling 1,2 placebo-controlled, randomized studies 12 wks or more 27 trials 2994 men 180 adverse events
59 Xu et al., BMC Medicine 11:108, 2013
![[01-31-2014] The U.S. Food and Drug Administration (FDA) is investigating the risk of stroke, heart attack, and death in men taking FDA-approved testosterone products.](/docs-images/92/108289607/images/60-0.jpg "We have been monitoring this risk and decided to reassess this safety issue based on the recent publication of two separate studies that each suggested an increased risk of cardiovascular events")
60 [ ] The U.S. Food and Drug Administration (FDA) is investigating the risk of stroke, heart attack, and death in men taking FDA-approved testosterone products. We have been monitoring this risk and decided to reassess this safety issue based on the recent publication of two separate studies that each suggested an increased risk of cardiovascular events among groups of men prescribed testosterone therapy. We are providing this alert while we continue to evaluate the information from these studies and other available data, and will communicate our final conclusions and recommendations when the evaluation is complete.
61 Until evidence from large randomized trials becomes available, the Endocrine Society believes that patients should be made aware of the potential risk of cardiovascular events in middle-aged and older men who are taking or considering testosterone therapy for age-related decline in testosterone levels and symptoms.
62
63
64 Records identified through different sources N=2747 UNPUBLISHED Studies N=649 Ongoing N=202 Records removed: No Clinical Trials N=2287 No Human species N =2 No English language N=13 No Male subjects N=145 No results available N=372 No placebo N=26 W omen N=21 No T arm N=27 Full-text articles assessed for eligibility N=300 Full-text articles excluded: Women N=4 No T use included N=45 No RCT N=21 No placebo (or p-only) arm N=108 No T-only arm N=4 Study duplicates N=18 Study assessed for eligibility N=1 Studies included in qualitative synthesis N=101 Studies excluded (see table 6) N=26 Studies included in quantitative synthesis (meta-analysis) N=75 Corona et al., 2014
65 Primary end-point: MACE cardiovascular death, non-fatal myocardial infarction stroke, acute coronary syndromes and/or heart failure reported as serious adverse events Secondary end-points: all cardiovascular-related events (anything reported as such by the authors): events reported as cardiac disorders, cardiovascular complaints, cardiovascular event vascular disorders, cardiac or cardiovascular event description fell within the International Statistical Classification of Disease (ICD) version 10 chapter IX (I00 toi99) Corona et al., Expert Opin Drug Saf Aug 19:[Epub ahe
66 Is testosterone administration associated with CV outcomes? (MACE)
67 Source MH-OR LL UL p 0,00 0,01 Odds ratio for MACE 0,10 1,00 10,00 100, ,00 TS #Events # Patients Placebo #Events # Patients Copenaghen SG 1986 (27) 1,97 0,08 48,82 0,68 Hall et al., 1996 (30) 0,32 0,01 8,23 0,49 Sih et al., 1997 (32) 0,88 0,05 15,33 0,93 Snyder et al., 1999 (36) 2,04 0,18 23,17 0,57 English et al., 2000 (38) 3,12 0,12 80,39 0,49 Seidman et al., 2001 (43) 0,41 0,02 10,83 0,59 Steidle et al., 2003 (48) 2,83 0,11 70,27 0,53 Armory et al., 2004 (50) 3,13 0,12 80,68 0,49 Kenny et al., 2004 (52) 0,23 0,01 7,05 0,40 Svartberg et al., 2004 (56) 0,29 0,01 7,74 0,46 Brockenbrough et al., 2006 (59) 3,75 0,36 39,59 0,27 Malkin et al., 2006 (65) 2,17 0,19 25,01 0,53 Nair et al., 2006 (68) 5,70 0,26 123,78 0,27 Svartberg et al., 2008 (77) 3,16 0,12 82,64 0,49 Chapman et al., 2009 (80) 1,00 0,05 20,83 1,00 Legros et al., 2009 (81) 1,01 0,04 25,01 1,00 Aversa et al., 2010 (85) 0,08 0,00 2,07 0,13 Aversa et al., 2010 (86) 0,07 0,00 1,97 0,12 Basaria et al., 2010 (10) 13,39 0,74 240,78 0,08 Kalinchenko et al., 2010 (88) 0,21 0,01 5,15 0,34 Srinivas-Shankar et al., 2010 (89) 1,01 0,14 7,31 0,99 Ho et al., 2011 (91) 1,00 0,06 16,37 1,00 Jones et al., 2011 (92) 0,51 0,05 5,75 0,59 Kaufman et al., 2011 (93) 0,87 0,04 18,48 0,93 Behere et al., 2012 (95) 2,95 0,12 72,91 0,51 Hildreth et al., 2013 (97) 0,15 0,02 1,53 0,11 Overall 1,01 0,57 1,77 0, Placebo TS Corona et al., 2014
68 Source # Trials MH-OR LL UL p 0,00 Odds ratio for MACE 0,01 0,10 1,00 10, , ,00 TS #Events # Patients Placebo #Events # Patients AMI 14 0,68 0,30 1,52 0, Acute coronary syndrome 15 0,92 0,43 1,97 0, Stroke 5 0,82 0,24 2,83 0, New heart failure 3 1,64 0,25 10,63 0, CV mortality 13 1,14 0,49 2,66 0, Placebo TS Corona et al., Expert Opin Drug Saf Aug 19:[Epub ahe
69 Associated diaseses Source # Trials MH-OR LL UL p 0,00 Odds ratio for MACE 0,01 0,10 1,00 10,00 100, ,00 TS #Events # Patients Placebo #Events # Patients Elderly men 10 1,22 0,49 3,03 0,67 Men with CVD 2 2,48 0,35 17,45 0,36 Frail men 5 2,25 0,72 7,08 0,17 Men with metabolic diseases 4 0,19 0,04 0,85 0, Hypogonadism status Mixed population 14 1,26 0,58 2,73 0,56 TT < 12 nm 12 0,84 0,32 2,23 0, da qui Type of support Drug company not supported 12 0,94 0,39 2,24 0,88 Drug company supported 14 1,07 0,51 2,24 0, Trial duration 12 weeks 4 1,02 0,20 5,29 0,98 >12 weeks 22 1,01 0,55 1,84 0, Placebo TS Corona et al., 2014
70 Associated diaseses Source # Trials MH-OR LL UL p 0,00 Odds ratio for MACE 0,01 0,10 1,00 10,00 100, ,00 TS #Events # Patients Placebo #Events # Patients Elderly men 10 1,22 0,49 3,03 0,67 Men with CVD 2 2,48 0,35 17,45 0,36 Frail men 5 2,25 0,72 7,08 0,17 Men with metabolic diseases 4 0,19 0,04 0,85 0, Hypogonadism status Mixed population 14 1,26 0,58 2,73 0,56 TT < 12 nm 12 0,84 0,32 2,23 0, da qui Type of support Drug company not supported 12 0,94 0,39 2,24 0,88 Drug company supported 14 1,07 0,51 2,24 0, Trial duration 12 weeks 4 1,02 0,20 5,29 0,98 >12 weeks 22 1,01 0,55 1,84 0, Placebo TS Corona et al., 2014
71 Source MH-OR LL UL p Odds ratio for MACE in Metabolic disease 0,00 0,01 0,10 1,00 10,00 100, TS #Events # Patients Placebo #Events # Patients Aversa 2010 JSM 0,08 0,00 2,07 0, Aversa 2010 JEI 0,07 0,00 1,97 0, Kalinchenko ,21 0,01 5,15 0, Jones et al., ,51 0,05 5,75 0, Overall 0,19 0,04 0,85 0, Placebo TS Corona et al., 2014
72 Is testosterone administration associated with CV outcomes? (any adverse event)
73 Source MH-OR LL UL p Copenaghen SG 1986 (27) 2,22 0,78 6,31 0,13 Hall et al., 1996 (30) 0,19 0,01 4,08 0,29 Sih et al.,1997 (32) 0,88 0,05 15,33 0,93 Snyder et al., 1999 (36) 1,96 0,61 6,29 0,26 English et al.,2000 (38) 5,43 0,25 118,96 0,28 Seidman et al., 2001 (43) 0,41 0,02 10,83 0,59 Steidle et al., 2003 (48) 4,76 0,23 100,40 0,32 Armory et al., 2004 (50) 5,44 0,25 119,63 0,28 Kenny et al., 2004 (52) 0,23 0,01 7,05 0,40 Svartberg et al., 2004 (56) 0,29 0,01 7,74 0,46 Brockenbrough et al., 2006 (59) 1,20 0,34 4,18 0,77 Malkin et al., 2006 (65) 0,86 0,24 3,10 0,82 Merza et al.,2006 (67) 0,30 0,01 7,85 0,47 Nair et al., 2006 (68) 1,32 0,39 4,50 0,66 Okun et al., 2006 (69) 0,46 0,04 5,75 0,55 Emmelot-Vonk et al., 2008 (75) 2,35 0,59 9,33 0,22 Svartberg et al., 2008 (77) 3,16 0,12 82,64 0,49 Caminiti et al., 2009 (78) 2,06 0,18 23,83 0,56 Chapman et al., 2009 (80) 1,00 0,05 20,83 1,00 Legros et al., 2009 (81) 1,01 0,04 25,01 1,00 Aversa et al., 2010 (85) 0,08 0,00 2,07 0,13 Aversa et al., 2010 (86) 0,07 0,00 1,97 0,12 Basaria et al., 2010 (10) 6,05 2,22 16,51 0,00 Kalinchenko et al., 2010 (88) 0,12 0,01 2,59 0,18 Srinivas-Shankar et al., 2010 (89) 2,60 0,49 13,61 0,26 Ho et al., 2011 (91) 1,00 0,14 7,34 1,00 Jones et al.,2011 (92) 0,40 0,14 1,19 0,10 Kaufman et al., 2011 (93) 1,49 0,33 6,71 0,60 Hoyos et al., 2012 (94) 3,18 0,13 81,01 0,48 Hildreth et al., 2013 (97) 0,14 0,04 0,48 0,00 NCT ,88 0,05 16,74 0,93 Overall 1,07 0,69 1,65 0,76 0,00 Odds ratio for overall CV events 0,01 0,10 1,00 10,00 100, ,00 TS #Events # Patients Placebo #Events # Patients Placebo TS Corona et al., 2014
74
75 Associated diaseses Source # Trials MH-OR LL UL p 0,00 Odds ratio for overall CVD 0,01 0,10 1,00 10, ,00 TS #Events # Patients Placebo #Events # Patients Elderly men 11 1,13 0,58 2,22 0,71 Men with CVD 3 1,28 0,44 3,71 0,65 Frail men 5 2,62 1,38 4,96 0,00 Men with metabolic diseases 5 0,33 0,14 0,82 0, Hypogonadism status Mixed population 18 1,26 0,84 1,90 0,27 TT < 12 nm 13 0,80 0,30 2,15 0, Type of support Drug company not supported 14 1,33 0,82 2,15 0, Drug company supported 17 1,02 0,51 2,04 0, Trial duration 12 weeks 2 0,18 0,02 1,81 0, >12 weeks 29 1,14 0,73 1,77 0, Placebo TS Corona et al., 2014

76 Corona et al., 2014
77 Testosterone and type 2 diabetes mellitus 1. Hypogonadism is associated with MetS and T2DM 2. Hypogonadism is associated with pre-diabetic conditions 3. Hypogonadism predicts T2DM but T2DM predicts hypogonadism 4. Having MACE decreases T by 2-3 nmoles/l 5. T is associated with incident overall and CV mortality but not incident MACE in longitudinal studies 6. TRT does not increase CV risk : possible protective effects in metabolic subjects

78
79 EFFECTS OF TRT ON DM & MetS PATIENT RESULTS FROM META-ANALYSIS EVALUATION
80 Patients with metabolic syndrome and or type 2 diabetes Study (Ref.) Boyanov et al 2003 Kapoor et al., 2006 La Vignera et al., 2008 Heufelder et al., 2009 Aversa et al., 2010 Gopal et al., 2010 Jones et al., 2011 Aversa et al., 2011 Tishova et al., 2011 Location Sofia, Bulgaria Sheffield, UK Catania, Italy Munich, Germany Rome, Italy Mumbai, India Multicenter Rome, Italy Moscow, Russia # patients (ID/C) 24/24 12/12 7/5 16/16 32/10 11/11 103/102 40/10 105/65 Hypogonadism cut off Trial duration (weeks) TT TT TT TT TT cft TT TT TT <15 nm <12 nm <8 nm <12 nm <11 nm <225 pm < 11 nm <11 nm < 12 nm Drugs O-TU i.m T T gel 1% T gel 1% TU i.m T T gel 2% TU TU Dose 120 mg daily 200 mg/ 2weeks 50 mg/ daily 50 mg/ daily 1000 mg/ 12 weeks 200 mg/ 2weeks 60mg/ Daily 1000 mg/ 12 weeks 1000 mg/ 12 weeks Comparator No TRT group Placebo No TRT group No TRT group Placebo Placebo Placebo Placebo Placebo IDF-MetS Metabolic NCEP-ATPIII- T2DM with with or T2DM T2DM IDF-MetS T2DM characteristics MetS IDF-MetS without T2DM IDF-MetS IDF-MetS MetS n=483 patients; mean follow up 37 weeks Corona et al., Best Pract Clin Endocrinol & Metab 2013;27;557
81 Effects of TRT on metabolic parameter in patients with MetS Source -1,50 Glycaemia mean differences (mmol/l) -1,00-0, ,00 0,50 1,00 Diff. in mean LL, 95% CI UL, 95% CI p Heufelder et al., ,60-1,15-0,05 0,03 Aversa et al., ,60-1,35 0,15 0,12 Jones et al., ,31-1,33 0,71 0,55 Aversa et al., ,70-0,96-0,44 0,00 Tishova et al., ,04-0,49 0,41 0,86 Overall -0,48-0,78-0,19 0,00 Favours no TRT Favors TRT Corona et al., Best Pract Clin Endocrinol & Metab 2013;27;557
82 Effects of TRT on metabolic parameter in patients with MetS HOMA index mean differences Source ,00-5,00-4,00-3,00-2,00-1,00 0,00 1,00 2,00 3,00 Diff. in mean LL, 95% CI UL, 95% CI p La Vignera et al., ,22-3,62-0,81 0,00 Heufelder et al., ,22-3,08-1,35 0,00 Aversa et al., ,80-2,62-0,98 0,00 Jones et al., ,05-2,31 2,21 0,97 Aversa et al., ,85-5,04-0,66 0,01 Tishova et al., ,32-0,53-0,11 0,00 Overall -1,54-2,59-0,50 0,00 Favours TRT Favors no TRT Corona et al., Best Pract Clin Endocrinol & Metab 2013;27;557
83 Effects of TRT on metabolic parameter in patients with MetS Triglycerides mean differences (nmol/l) Source -1,20-1,00-0,80-0,60-0,40-0, ,00 0,20 0,40 0,60 0,80 Diff. in mean LL, 95% CI UL, 95% CI p La Vignera et al., ,48-0,82-0,14 0,01 Heufelder et al., ,80-1,08-0,52 0,00 Aversa et al., ,00-0,43 0,43 1,00 Jones et al., ,25-0,65 0,15 0,22 Aversa et al., ,10-0,79 0,59 0,78 Tishova et al., ,52-0,98-0,06 0,03 Overall -0,40-0,66-0,14 0,00 Favours TRT Favors no TRT Corona et al., Best Pract Clin Endocrinol & Metab 2013;27;557

84 Effects of TRT on metabolic parameter in patients with MetS Corona et al., Best Pract Clin Endocrinol & Metab 2013;27;557
85 Testosterone and type 2 diabetes mellitus 1. Hypogonadism is associated with MetS and T2DM 2. Hypogonadism is associated with pre-diabetic conditions 3. Hypogonadism predicts T2DM but T2DM predicts hypogonadism 4. Having MACE decreases T by 2-3 nmoles/l 5. T is associated with incident overall and CV mortality but not incident MACE in longitudinal studies 6. TRT does not increase CV risk : possible protective effects in metabolic subjects 7.TRT in MetS is able to improve glyco-metabolic control ( fasting glycaemia), insulin resistance ( triglycerides, HOMA), fat mass ( waist)
86 Patients with metabolic syndrome and or type 2 diabetes Study (Ref.) Boyanov et al 2003 Kapoor et al., 2006 La Vignera et al., 2008 Heufelder et al., 2009 Aversa et al., 2010 Gopal et al., 2010 Jones et al., 2011 Aversa et al., 2011 Tishova et al., 2011 Location Sofia, Bulgaria Sheffield, UK Catania, Italy Munich, Germany Rome, Italy Mumbai, India Multicenter Rome, Italy Moscow, Russia # patients (ID/C) 24/24 12/12 7/5 16/16 32/10 11/11 103/102 40/10 105/65 Hypogonadism cut off Trial duration (weeks) TT TT TT TT TT cft TT TT TT <15 nm <12 nm <8 nm <12 nm <11 nm <225 pm < 11 nm <11 nm < 12 nm Drugs O-TU i.m T T gel 1% T gel 1% TU i.m T T gel 2% TU TU Dose 120 mg daily 200 mg/ 2weeks 50 mg/ daily 50 mg/ daily 1000 mg/ 12 weeks 200 mg/ 2weeks 60mg/ Daily 1000 mg/ 12 weeks 1000 mg/ 12 weeks Comparator No TRT group Placebo No TRT group No TRT group Placebo Placebo Placebo Placebo Placebo IDF-MetS Metabolic characteristics T2DM T2DM NCEP-ATPIII- MetS T2DM with IDF-MetS IDF-MetS T2DM with or without IDF-MetS IDF-MetS T2DM Type 2 diabetes n=263 patients; mean follow up 28 weeks Corona et al., Best Pract Clin Endocrinol & Metab 2013;27;557

87 Effects of TRT on metabolic parameter in patients with T2DM Corona et al., Best Pract Clin Endocrinol & Metab 2013;27;557
88 Effects of TRT on metabolic parameter in patients with T2DM Source Glycaemia mean differences (mmol/l) ,00-3,00-2,00-1,00 0,00 1,00 2,00 Diff. in mean LL, 95% CI UL, 95% CI p Boyanov et al., ,00-3,09-0,91 0,00 Kapoor et al., ,35-3,33 0,63 0,18 Heufelder et al., ,60-1,15-0,05 0,03 Gopal et al., ,98-3,66-0,30 0,02 Jones et al., ,17-1,42 1,08 0,79 Overall -1,09-1,84-0,35 0,00 Favours TRT Favors no TRT Corona et al., Best Pract Clin Endocrinol & Metab 2013;27;557
89 Effects of TRT on metabolic parameter in patients with T2DM Source Triglycerides mean differences (nmol/l) ,00-1,50-1,00-0,50 0,00 0,50 1,00 Diff. in mean LL, 95% CI UL, 95% CI p Boyanov et al., ,51-0,92-0,10 0,02 Kapoor et al., ,20-1,23 0,83 0,70 Heufelder et al., ,80-1,08-0,52 0,00 Gopal et al., ,82-1,61-0,03 0,04 Jones et al., ,29-0,75 0,17 0,22 Overall -0,60-0,83-0,37 0,00 Favours TRT Favors no TRT Corona et al., Best Pract Clin Endocrinol & Metab 2013;27;557
90 Testosterone and type 2 diabetes mellitus 1. Hypogonadism is associated with MetS and T2DM 2. Hypogonadism is associated with pre-diabetic conditions 3. Hypogonadism predicts T2DM but T2DM predicts hypogonadism 4. Having MACE decreases T by 2-3 nmoles/l 5. T is associated with incident overall and CV mortality but not incident MACE in longitudinal studies 6. TRT does not increase CV risk : possible protective effects in metabolic subjects 7.TRT in MetS is able to improve glyco-metabolic control ( fasting glycaemia), insulin resistance ( triglycerides, HOMA), fat mass ( waist) 8. TRT in subjects with T2DM is able to improve glyco-metabolic control ( HbA1c, fasting glycaemia), insulin resistance ( triglycerides).
91 V1 Previous use of ED therapy (All 21%) Frequente Sildenafil Tadalfil Vardenafil PGE1 Testosterone Occasionale %
92 Efficacia PDE5ì V2 vs V1 Sildenafil Tadalfil Ottima Vardenafil Buona Scarsa %
93 V2 Previous use of ED therapy (All 38.2 vs 21%) Frequente Sildenafil Tadalfil Vardenafil PGE1 Testosterone Occasionale %
94 Ringraziamenti Prof. CB Giorda Prof. D Cucinotta Dott. P Guida Dott.ssa E Nada SUBITO-DE study group
Take-Home Messages: Androgens
 Take-Home Messages: Androgens Anthony J. Bella MD, FRCSC Greta and John Hansen Chair in Men s Health Research Division of Urology, Department of Surgery University of Ottawa SUMMARY SLAMS Symposium Clinical
Take-Home Messages: Androgens Anthony J. Bella MD, FRCSC Greta and John Hansen Chair in Men s Health Research Division of Urology, Department of Surgery University of Ottawa SUMMARY SLAMS Symposium Clinical
Testosterone Therapy in Men An update
 Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
IL RUOLO DEL DEFICIT DI TESTOSTERONE NELLA SINDROME METABOLICA E NELLA INSUFFICIENZA RENALE NEL MASCHIO ADULTO. VA Giagulli
 IL RUOLO DEL DEFICIT DI TESTOSTERONE NELLA SINDROME METABOLICA E NELLA INSUFFICIENZA RENALE NEL MASCHIO ADULTO VA Giagulli UOS di Endocrinologia e Malattie Metaboliche PT di Conversano ASL BA Male hypogonadism
IL RUOLO DEL DEFICIT DI TESTOSTERONE NELLA SINDROME METABOLICA E NELLA INSUFFICIENZA RENALE NEL MASCHIO ADULTO VA Giagulli UOS di Endocrinologia e Malattie Metaboliche PT di Conversano ASL BA Male hypogonadism
The reality of LOH-symptoms
 The reality of LOH-symptoms PRISM IV Bruges, Belgium September 25-26, 2014 Dr. Herman Leliefeld Androsmannenkliniek The Netherlands The reality of LOH symptoms male external & internal genitalia Testosterone
The reality of LOH-symptoms PRISM IV Bruges, Belgium September 25-26, 2014 Dr. Herman Leliefeld Androsmannenkliniek The Netherlands The reality of LOH symptoms male external & internal genitalia Testosterone
Hypogonadism* (män) Erytrocytos Kardiovaskulär risk
 Erytrocytos Kardiovaskulär risk") Hypogonadism* (män) Erytrocytos Kardiovaskulär risk *Lågt Testosteron och symtom Stefan Arver ANOVA, Karolinska Univ Sjukhuset Inst. F Medicin/Huddinge Karolinska Institutet Endokrindagar i Umeå 2019 1
Hypogonadism* (män) Erytrocytos Kardiovaskulär risk *Lågt Testosteron och symtom Stefan Arver ANOVA, Karolinska Univ Sjukhuset Inst. F Medicin/Huddinge Karolinska Institutet Endokrindagar i Umeå 2019 1
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA
 Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
Disclosures. Advisory Boards 6/10/2014
 Massachusetts Medical Society 12 th annual Men s Health Symposium 11 June 2014 Testosterone and Cardiovascular Disease Where Does The Real Answer Lie? Andre Guay MD, FACP, FACE, IF (Ret) Director, Center
Massachusetts Medical Society 12 th annual Men s Health Symposium 11 June 2014 Testosterone and Cardiovascular Disease Where Does The Real Answer Lie? Andre Guay MD, FACP, FACE, IF (Ret) Director, Center
Erectile Dysfunction, Cardiovascular Risk and
 Erectile Dysfunction, Cardiovascular Risk and Testosterone National Lipid Association (NLA) 2016 Fall Clinical Update August 26-28, 2016 Amelia Island, Fl Robert A. Kloner MD, PhD Director of the Cardiovascular
Erectile Dysfunction, Cardiovascular Risk and Testosterone National Lipid Association (NLA) 2016 Fall Clinical Update August 26-28, 2016 Amelia Island, Fl Robert A. Kloner MD, PhD Director of the Cardiovascular
Testosterone and PDE5 inhibitors in the aging male
 Testosterone and PDE5 inhibitors in the aging male Francesco Romanelli Department of Experimental Medicine Medical Pathophysiology, Food Science and Endocrinology Section Sapienza University of Rome 3005
Testosterone and PDE5 inhibitors in the aging male Francesco Romanelli Department of Experimental Medicine Medical Pathophysiology, Food Science and Endocrinology Section Sapienza University of Rome 3005
ENDOCRINOLOGICAL IMPLICATIONS AND COMPLICATIONS OF TESTOSTERONE REPLACEMENT IN AGEING MEN
 ENDOCRINOLOGICAL IMPLICATIONS AND COMPLICATIONS OF TESTOSTERONE REPLACEMENT IN AGEING MEN Frederick C.W. Wu Professor of Medicine and Endocrinology Andrology Research Unit, Centre for Endocrinology and
ENDOCRINOLOGICAL IMPLICATIONS AND COMPLICATIONS OF TESTOSTERONE REPLACEMENT IN AGEING MEN Frederick C.W. Wu Professor of Medicine and Endocrinology Andrology Research Unit, Centre for Endocrinology and
Update on diagnosis and complications of adult and elderly male hypogonadism
 Hypoandrogenism in the elderly: to treat or not to treat? 12 th Italian AME Meeting; 6 th joint Meeting with AAC Bari november 10th Update on diagnosis and complications of adult and elderly male hypogonadism
Hypoandrogenism in the elderly: to treat or not to treat? 12 th Italian AME Meeting; 6 th joint Meeting with AAC Bari november 10th Update on diagnosis and complications of adult and elderly male hypogonadism
Endocrine Update Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh
 Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Disclosures. Learning Objectives. Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease. None
 Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
PRISM Bruges June Herman Leliefeld Urologist. The Netherlands
 PRISM Bruges 25-26 June 2015 Herman Leliefeld Urologist The Netherlands Guidelines EAU 2015: a rich source of Knowledge! Epidemiology/ Aetiology / Pathology Diagnostic evaluation Disease management Follow-Up
PRISM Bruges 25-26 June 2015 Herman Leliefeld Urologist The Netherlands Guidelines EAU 2015: a rich source of Knowledge! Epidemiology/ Aetiology / Pathology Diagnostic evaluation Disease management Follow-Up
EUROPEAN SURVEY OF CARDIOVASCULAR DISEASE PREVENTION AND DIABETES EUROASPIRE IV. GUY DE BACKER Ghent University,Belgium
 EUROPEAN SURVEY OF CARDIOVASCULAR DISEASE PREVENTION AND DIABETES EUROASPIRE IV GUY DE BACKER Ghent University,Belgium ESC Congress 2012, aug.25-29th, Munich, Germany ESC Congress 2012, aug.25-29th, Munich,
EUROPEAN SURVEY OF CARDIOVASCULAR DISEASE PREVENTION AND DIABETES EUROASPIRE IV GUY DE BACKER Ghent University,Belgium ESC Congress 2012, aug.25-29th, Munich, Germany ESC Congress 2012, aug.25-29th, Munich,
An Idea Whose Time Has Come-Male Health Programs: An Opportunity For Clinical Expansion and Better Health
 An Idea Whose Time Has Come-Male Health Programs: An Opportunity For Clinical Expansion and Better Health KEVIN R. LOUGHLIN MD,MBA Harvard Medical School Boston, MA THE WEAKER SEX-MALES LIFE EXPECTANCY
An Idea Whose Time Has Come-Male Health Programs: An Opportunity For Clinical Expansion and Better Health KEVIN R. LOUGHLIN MD,MBA Harvard Medical School Boston, MA THE WEAKER SEX-MALES LIFE EXPECTANCY
Estrogens vs Testosterone for cardiovascular health and longevity
 Estrogens vs Testosterone for cardiovascular health and longevity Panagiota Pietri, MD, PhD, FESC Director of Hypertension Unit Athens Medical Center Athens, Greece Women vs Men Is there a difference in
Estrogens vs Testosterone for cardiovascular health and longevity Panagiota Pietri, MD, PhD, FESC Director of Hypertension Unit Athens Medical Center Athens, Greece Women vs Men Is there a difference in
Disclosures. Faculty 3/5/18. Testosterone, the FDA and CVD Risk Controversies. Matt Rosenberg, MD Director of Mid-Michigan Health Centers Jackson, MI
 Testosterone, the FDA and CVD Risk Controversies Faculty Matt Rosenberg, MD Director of Mid-Michigan Health Centers Jackson, MI 2 Disclosures Matt Rosenberg, MD serves on the advisory board for Bayer,
Testosterone, the FDA and CVD Risk Controversies Faculty Matt Rosenberg, MD Director of Mid-Michigan Health Centers Jackson, MI 2 Disclosures Matt Rosenberg, MD serves on the advisory board for Bayer,
TESTOSTERONE REPLACEMENT THERAPY. WHAT IS THE REAL RISK? WHAT TO DO IN PROSTATE CANCER?
 TESTOSTERONE REPLACEMENT THERAPY. WHAT IS THE REAL RISK? WHAT TO DO IN PROSTATE CANCER? TESTOSTERONE REPLACEMENT THERAPY (TRT) Nuno Tomada, MD, PhD Department of Urology of Hospital S. João Faculty of
TESTOSTERONE REPLACEMENT THERAPY. WHAT IS THE REAL RISK? WHAT TO DO IN PROSTATE CANCER? TESTOSTERONE REPLACEMENT THERAPY (TRT) Nuno Tomada, MD, PhD Department of Urology of Hospital S. João Faculty of
Point-Counterpoint: Late Onset Hypogonadism (LOH)
") Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
SCIENTIFIC STUDY REPORT
 PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
Present and future association between obesity and hypogonadism in Italian male
 ORIGINAL PAPER DOI: 10.4081/aiua.2014.1.26 Present and future association between obesity and hypogonadism in Italian male Valentina Boddi 1, Valeria Barbaro 2, Paul Mc Nieven 3, Mario Maggi 1, Carlo Maria
ORIGINAL PAPER DOI: 10.4081/aiua.2014.1.26 Present and future association between obesity and hypogonadism in Italian male Valentina Boddi 1, Valeria Barbaro 2, Paul Mc Nieven 3, Mario Maggi 1, Carlo Maria
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency
 Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Diagnosis and Clinical Evaluation of Hypogonadism in Adult Patients with Obesity and Diabetes
 Diagnosis and Clinical Evaluation of Hypogonadism in Adult Patients with Obesity and Diabetes Adrian Dobs, M.D., M.H.S. Professor of Medicine and Oncology The Johns Hopkins University School of Medicine
Diagnosis and Clinical Evaluation of Hypogonadism in Adult Patients with Obesity and Diabetes Adrian Dobs, M.D., M.H.S. Professor of Medicine and Oncology The Johns Hopkins University School of Medicine
NEW DEVELOPMENTS: T & CVD FDA & THE T TRIALS
 NEW DEVELOPMENTS: T & CVD FDA & THE T TRIALS 2017 UPDATE FDUS Martin Miner MD Clinical Professor of Family Medicine and Urology Co-Director The Men s Health Center The Miriam Hospital Warren Albert School
NEW DEVELOPMENTS: T & CVD FDA & THE T TRIALS 2017 UPDATE FDUS Martin Miner MD Clinical Professor of Family Medicine and Urology Co-Director The Men s Health Center The Miriam Hospital Warren Albert School
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Outline. Classic Androgen deficiency. Cardiovascular Risk and Testosterone Fact vs Fiction. Professor Robert I McLachlan AM, FRACP, PhD
 Health Ed Brisbane Saturday 27 th October 2018 Cardiovascular Risk and Testosterone Fact vs Fiction Professor Robert I McLachlan AM, FRACP, PhD Hudson Institute of Medical Research, Monash University Department
Health Ed Brisbane Saturday 27 th October 2018 Cardiovascular Risk and Testosterone Fact vs Fiction Professor Robert I McLachlan AM, FRACP, PhD Hudson Institute of Medical Research, Monash University Department
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Models of preventive care in clinical practice to achieve 25 by 25
 Models of preventive care in clinical practice to achieve 25 by 25 Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College
Models of preventive care in clinical practice to achieve 25 by 25 Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital
 Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital 1. Importance of Lowering LDL-Cholesterol in Diabetes Patients & Lipid Guidelines Prevalence of dyslipidemia in Korea Prevalence
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital 1. Importance of Lowering LDL-Cholesterol in Diabetes Patients & Lipid Guidelines Prevalence of dyslipidemia in Korea Prevalence
Androgen Pattern and Erectile Function in Newly Diagnosed Type 2 Diabetes
 Med. J. Cairo Univ., Vol. 84, No. 3, December: 341-347, 2016 www.medicaljournalofcairouniversity.net Androgen Pattern and Erectile Function in Newly Diagnosed Type 2 Diabetes AHMED I. EL-SAKKA, M.D.*;
Med. J. Cairo Univ., Vol. 84, No. 3, December: 341-347, 2016 www.medicaljournalofcairouniversity.net Androgen Pattern and Erectile Function in Newly Diagnosed Type 2 Diabetes AHMED I. EL-SAKKA, M.D.*;
Every obese male with type 2 diabetes should be screened for hypogonadism
 Every obese male with type 2 diabetes should be screened for hypogonadism FOR Professor T Hugh Jones Consultant Physician & Endocrinologist, Robert Hague Centre for Diabetes and Endocrinology, Barnsley
Every obese male with type 2 diabetes should be screened for hypogonadism FOR Professor T Hugh Jones Consultant Physician & Endocrinologist, Robert Hague Centre for Diabetes and Endocrinology, Barnsley
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Lipoprotein(a), PCSK9 Inhibition and Cardiovascular Risk: Insights from the FOURIER Trial
, PCSK9 Inhibition and Cardiovascular Risk: Insights from the FOURIER Trial") Lipoprotein(a), PCSK9 Inhibition and Cardiovascular Risk: Insights from the FOURIER Trial Michelle L. O Donoghue, Robert P. Giugliano, Anthony C. Keech, Estella Kanevsky, KyungAh Im, Peter S. Sever, Terje
Lipoprotein(a), PCSK9 Inhibition and Cardiovascular Risk: Insights from the FOURIER Trial Michelle L. O Donoghue, Robert P. Giugliano, Anthony C. Keech, Estella Kanevsky, KyungAh Im, Peter S. Sever, Terje
CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE. AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY. sul Paziente ad alto rischio CV*
 CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY sul Paziente ad alto rischio CV* Does reducing hyperglycemia protect against cardiovascular risk?
CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY sul Paziente ad alto rischio CV* Does reducing hyperglycemia protect against cardiovascular risk?
Dyslipidemia in women: Who should be treated and how?
 Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
9/2/2016. Faculty. Learning Objectives. Disclosures. Prevalence of Hypogonadism. Prevalence of HG (cont)
") Faculty Testosterone Replacement Therapies: Mitigating Cardiometabolic Risks Associated with Hypogonadism Pamela Ellsworth, MD Professor of Urology University of Massachusetts Medical School Vice Chair,
Faculty Testosterone Replacement Therapies: Mitigating Cardiometabolic Risks Associated with Hypogonadism Pamela Ellsworth, MD Professor of Urology University of Massachusetts Medical School Vice Chair,
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Recommendations on the diagnosis, treatment and monitoring of Testosterone deficiency (TD) in adult men
 in adult men") Recommendations on the diagnosis, treatment and monitoring of Testosterone deficiency (TD) in adult men Bruno Lunenfeld, George Mskhalaya, Svetlana Kalinchenko, Yulia Tishova, Michael Zitzmann, Stefan
Recommendations on the diagnosis, treatment and monitoring of Testosterone deficiency (TD) in adult men Bruno Lunenfeld, George Mskhalaya, Svetlana Kalinchenko, Yulia Tishova, Michael Zitzmann, Stefan
Alternative management of hypogonadism Tamoxifen. Emmanuele A. Jannini, MD Tor Vergata University of Rome ITALY
 Alternative management of hypogonadism Tamoxifen Emmanuele A. Jannini, MD Tor Vergata University of Rome ITALY eajannini@gmail.com What hypogonadism is? What hypogonadism is? It is an empty glass The two
Alternative management of hypogonadism Tamoxifen Emmanuele A. Jannini, MD Tor Vergata University of Rome ITALY eajannini@gmail.com What hypogonadism is? What hypogonadism is? It is an empty glass The two
Epidemiology of Diabetes, Impaired Glucose Homeostasis and Cardiovascular Risk. Eberhard Standl
 Epidemiology of Diabetes, Impaired Glucose Homeostasis and Cardiovascular Risk Eberhard Standl European Heart House Sophia Antipolis Thursday, June 17, 2010 IDF Diabetes Atlas 2009: Global Numbers Still
Epidemiology of Diabetes, Impaired Glucose Homeostasis and Cardiovascular Risk Eberhard Standl European Heart House Sophia Antipolis Thursday, June 17, 2010 IDF Diabetes Atlas 2009: Global Numbers Still
Carlo Patrono, MD, FESC. New York, 8 th December Catholic University School of Medicine, Rome, Italy. New York Cardiovascular Symposium
 Aspirin in Primary and Secondary Cardiovascular Disease Prevention. Still Four Questions: About Enteric-Coated, Indicated Doses, Use in Diabetes, Use in PVD Carlo Patrono, MD, FESC Catholic University
Aspirin in Primary and Secondary Cardiovascular Disease Prevention. Still Four Questions: About Enteric-Coated, Indicated Doses, Use in Diabetes, Use in PVD Carlo Patrono, MD, FESC Catholic University
Diabetes, Diet and SMI: How can we make a difference?
 Diabetes, Diet and SMI: How can we make a difference? Dr. Adrian Heald Consultant in Endocrinology and Diabetes Leighton Hospital, Crewe and Macclesfield Research Fellow, Manchester University Relative
Diabetes, Diet and SMI: How can we make a difference? Dr. Adrian Heald Consultant in Endocrinology and Diabetes Leighton Hospital, Crewe and Macclesfield Research Fellow, Manchester University Relative
Managing Testosterone Deficiency: A Practical Guide. John Grantmyre MD Professor of Urology Dalhousie University
 Managing Testosterone Deficiency: A Practical Guide John Grantmyre MD Professor of Urology Dalhousie University 1 2 Case Study #1 A 59-Year-Old Man with Erectile Dysfunction 3 Case History Robert is a
Managing Testosterone Deficiency: A Practical Guide John Grantmyre MD Professor of Urology Dalhousie University 1 2 Case Study #1 A 59-Year-Old Man with Erectile Dysfunction 3 Case History Robert is a
Testosterone Replacement Therapy for Hypogonadism: Learning Objectives. What Is the Evidence? Is It Safe? Case Study. Case Study contd.
 4 4:4pm Testosterone Therapy: Examining the Evidence SPEAKER Culley Carson, MD Presenter Disclosure Information The following relationships exist related to this presentation: Culley Carson, MD: Consultant
4 4:4pm Testosterone Therapy: Examining the Evidence SPEAKER Culley Carson, MD Presenter Disclosure Information The following relationships exist related to this presentation: Culley Carson, MD: Consultant
Supplementary Online Content
 Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Master Class in Preventive Cardiology. The New MI Phenotype OR. Klas Malmberg MD, PhD, FESC Karolinska Institutet, Stockholm Sweden
 Master Class in Preventive Cardiology The New MI Phenotype OR Klas Malmberg MD, PhD, FESC Karolinska Institutet, Stockholm Sweden The New MI Phenotype OR Coronary disease and glucose abnormalities Klas
Master Class in Preventive Cardiology The New MI Phenotype OR Klas Malmberg MD, PhD, FESC Karolinska Institutet, Stockholm Sweden The New MI Phenotype OR Coronary disease and glucose abnormalities Klas
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
LLL Session - Nutrition support in diabetes and dyslipidemia. Dyslipidemia: targeting the management of cardiovascular risk factors. M.
 ESPEN Congress Leipzig 2013 LLL Session - Nutrition support in diabetes and dyslipidemia Dyslipidemia: targeting the management of cardiovascular risk factors M. Leon Sanz (ES) Dyslipidemia: Targeting
ESPEN Congress Leipzig 2013 LLL Session - Nutrition support in diabetes and dyslipidemia Dyslipidemia: targeting the management of cardiovascular risk factors M. Leon Sanz (ES) Dyslipidemia: Targeting
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Statins in the Treatment of Type 2 Diabetes Mellitus: A Systematic Review.
 ISPUB.COM The Internet Journal of Cardiovascular Research Volume 7 Number 1 Statins in the Treatment of Type 2 Diabetes Mellitus: A Systematic Review. C ANYANWU, C NOSIRI Citation C ANYANWU, C NOSIRI.
ISPUB.COM The Internet Journal of Cardiovascular Research Volume 7 Number 1 Statins in the Treatment of Type 2 Diabetes Mellitus: A Systematic Review. C ANYANWU, C NOSIRI Citation C ANYANWU, C NOSIRI.
Testosterone Replacement Therapy and Cardiovascular Risk: A Review
 pissn: 2287-4208 / eissn: 2287-4690 World J Mens Health 2015 December 33(3): 130-142 http://dx.doi.org/10.5534/wjmh.2015.33.3.130 Review Article Testosterone Replacement Therapy and Cardiovascular Risk:
pissn: 2287-4208 / eissn: 2287-4690 World J Mens Health 2015 December 33(3): 130-142 http://dx.doi.org/10.5534/wjmh.2015.33.3.130 Review Article Testosterone Replacement Therapy and Cardiovascular Risk:
Metabolic Syndrome Update The Metabolic Syndrome: Overview. Global Cardiometabolic Risk
 Metabolic Syndrome Update 21 Marc Cornier, M.D. Associate Professor of Medicine Division of Endocrinology, Metabolism & Diabetes University of Colorado Denver Denver Health Medical Center The Metabolic
Metabolic Syndrome Update 21 Marc Cornier, M.D. Associate Professor of Medicine Division of Endocrinology, Metabolism & Diabetes University of Colorado Denver Denver Health Medical Center The Metabolic
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
A dro r gen e R e R p e lac a e c m e e m n e t t T her e a r p a y Androgen Replacement Therapy in the Aging O j b ecti t ve v s Male
 Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
Diabetes and Cardiovascular Risks in the Polycystic Ovary Syndrome
 Diabetes and Cardiovascular Risks in the Polycystic Ovary Syndrome John E. Nestler, M.D. William Branch Porter Professor of Medicine Chair, Department of Internal Medicine Virginia Commonwealth University
Diabetes and Cardiovascular Risks in the Polycystic Ovary Syndrome John E. Nestler, M.D. William Branch Porter Professor of Medicine Chair, Department of Internal Medicine Virginia Commonwealth University
HHS Public Access Author manuscript Int J Impot Res. Author manuscript; available in PMC 2015 September 01.
 Testosterone Therapy and Mortality Risk Michael L. Eisenberg, MD 1, Shufeng Li, MS 2, Danielle Herder, MD 3, Dolores J. Lamb, PhD 4, and Larry I. Lipshultz, MD 4 1 Assistant Professor, Departments of Urology
Testosterone Therapy and Mortality Risk Michael L. Eisenberg, MD 1, Shufeng Li, MS 2, Danielle Herder, MD 3, Dolores J. Lamb, PhD 4, and Larry I. Lipshultz, MD 4 1 Assistant Professor, Departments of Urology
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
A nationwide population-based study. Pai-Feng Hsu M.D. Shao-Yuan Chuang PhD
 The Association of Clinical Symptomatic Hypoglycemia with Cardiovascular Events and Total Death in Type 2 Diabetes Mellitus A nationwide population-based study Pai-Feng Hsu M.D. Shao-Yuan Chuang PhD Taipei
The Association of Clinical Symptomatic Hypoglycemia with Cardiovascular Events and Total Death in Type 2 Diabetes Mellitus A nationwide population-based study Pai-Feng Hsu M.D. Shao-Yuan Chuang PhD Taipei
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden
 Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Does TRT Induce Prostate Cancer?
 Does TRT Induce Prostate Cancer? Prism VI, Bruges, Belgium 21-22November 2014 Herman Leliefeld, Urologist, Utrecht The Netherlands Does TRT Induce Prostate Cancer? Why is it a controversial topic? Is there
Does TRT Induce Prostate Cancer? Prism VI, Bruges, Belgium 21-22November 2014 Herman Leliefeld, Urologist, Utrecht The Netherlands Does TRT Induce Prostate Cancer? Why is it a controversial topic? Is there
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Metastatic disease. 80% will die of prostate cancer 5 year survival only 25% No major advances in cure since 1942
 Prostate cancer Metastatic disease 80% will die of prostate cancer 5 year survival only 25% No major advances in cure since 1942 Impact of early prostate cancer 12 10 8 6 4 2 0 70-80 years 60-70 years
Prostate cancer Metastatic disease 80% will die of prostate cancer 5 year survival only 25% No major advances in cure since 1942 Impact of early prostate cancer 12 10 8 6 4 2 0 70-80 years 60-70 years
The Metabolic Syndrome Update The Metabolic Syndrome: Overview. Global Cardiometabolic Risk
 Update 2013 Marc Cornier, M.D. Associate Professor of Medicine Division of Endocrinology, Metabolism & Diabetes Anschutz Health and Wellness Center University of Colorado School of Medicine Denver Health
Update 2013 Marc Cornier, M.D. Associate Professor of Medicine Division of Endocrinology, Metabolism & Diabetes Anschutz Health and Wellness Center University of Colorado School of Medicine Denver Health
HORMONE THERAPY IN AGING MALE ATHLETES
 DISCLOSURES HORMONE THERAPY IN AGING MALE ATHLETES No relevant affiliations or financial interests When, Why and is it Safe? OBJECTIVES Summarize the benefits of optimizing hormone balance Examine the
DISCLOSURES HORMONE THERAPY IN AGING MALE ATHLETES No relevant affiliations or financial interests When, Why and is it Safe? OBJECTIVES Summarize the benefits of optimizing hormone balance Examine the
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Primary prevention of CVD Potential output:
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Primary prevention of CVD Potential output:
Supplementary Information for: Predictors of chronic kidney disease in type 1 diabetes: a longitudinal study from the AMD Annals initiative.
 Supplementary Information for: Predictors of chronic kidney disease in type 1 diabetes: a longitudinal study from the AMD Annals initiative. Authors: Pamela Piscitelli 1, Francesca Viazzi 2 ; Paola Fioretto
Supplementary Information for: Predictors of chronic kidney disease in type 1 diabetes: a longitudinal study from the AMD Annals initiative. Authors: Pamela Piscitelli 1, Francesca Viazzi 2 ; Paola Fioretto
Glucose Control and Prevention of Cardiovascular Disease
 Glucose Control and Prevention of Cardiovascular Disease Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Diabetes Update+, March
Glucose Control and Prevention of Cardiovascular Disease Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Diabetes Update+, March
A: Epidemiology update. Evidence that LDL-C and CRP identify different high-risk groups
 A: Epidemiology update Evidence that LDL-C and CRP identify different high-risk groups Women (n = 27,939; mean age 54.7 years) who were free of symptomatic cardiovascular (CV) disease at baseline were
A: Epidemiology update Evidence that LDL-C and CRP identify different high-risk groups Women (n = 27,939; mean age 54.7 years) who were free of symptomatic cardiovascular (CV) disease at baseline were
Disclosures. Speaker s bureau: Research grant: Advisory Board: Servier International, Bayer, Merck Serono, Novartis, Boehringer Ingelheim, Lupin
 Disclosures Speaker s bureau: Research grant: Advisory Board: Servier International, Bayer, Merck Serono, Novartis, Boehringer Ingelheim, Lupin Servier International, Boehringer Ingelheim Servier International,
Disclosures Speaker s bureau: Research grant: Advisory Board: Servier International, Bayer, Merck Serono, Novartis, Boehringer Ingelheim, Lupin Servier International, Boehringer Ingelheim Servier International,
Rikshospitalet, University of Oslo
 Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
Supplementary Online Material
 Supplementary Online Material Collet T-H, Gussekloo J, Bauer DC, et al; Thyroid Studies Collaboration. Subclinical hyperthyroidism and the risk of coronary heart disease and mortality. Arch Intern Med.
Supplementary Online Material Collet T-H, Gussekloo J, Bauer DC, et al; Thyroid Studies Collaboration. Subclinical hyperthyroidism and the risk of coronary heart disease and mortality. Arch Intern Med.
Glycemic control a matter of life and death
 Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study
 LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study") Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
How to treat: TRT modalities and formulations
 How to treat: TRT modalities and formulations Paul PIETTE, PharmD Senior Research Fellow Clinique Antoine Depage - Belgium ppiette@besins-healthcare.com Bruges 2014, May 15 th Testosterone-replacement
How to treat: TRT modalities and formulations Paul PIETTE, PharmD Senior Research Fellow Clinique Antoine Depage - Belgium ppiette@besins-healthcare.com Bruges 2014, May 15 th Testosterone-replacement
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
GALECTIN-3 PREDICTS LONG TERM CARDIOVASCULAR DEATH IN HIGH-RISK CORONARY ARTERY DISEASE PATIENTS
 GALECTIN-3 PREDICTS LONG TERM CARDIOVASCULAR DEATH IN HIGH-RISK CORONARY ARTERY DISEASE PATIENTS Table of Contents List of authors pag 2 Supplemental figure I pag 3 Supplemental figure II pag 4 Supplemental
GALECTIN-3 PREDICTS LONG TERM CARDIOVASCULAR DEATH IN HIGH-RISK CORONARY ARTERY DISEASE PATIENTS Table of Contents List of authors pag 2 Supplemental figure I pag 3 Supplemental figure II pag 4 Supplemental
Diabetes risk scores and death: predictability and practicability in two different populations
 Diabetes risk scores and death: predictability and practicability in two different populations Short Report David Faeh, MD, MPH 1 ; Pedro Marques-Vidal, MD, PhD 2 ; Michael Brändle, MD 3 ; Julia Braun,
Diabetes risk scores and death: predictability and practicability in two different populations Short Report David Faeh, MD, MPH 1 ; Pedro Marques-Vidal, MD, PhD 2 ; Michael Brändle, MD 3 ; Julia Braun,
GSK Medicine: Study Number: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Vitamin D supplementation of professionally active adults
 Vitamin D supplementation of professionally active adults VITAMIN D MINIMUM, MAXIMUM, OPTIMUM FRIDAY, SEPTEMBER 22 ND 2017 Samantha Kimball, PhD, MLT Research Director Pure North S Energy Foundation The
Vitamin D supplementation of professionally active adults VITAMIN D MINIMUM, MAXIMUM, OPTIMUM FRIDAY, SEPTEMBER 22 ND 2017 Samantha Kimball, PhD, MLT Research Director Pure North S Energy Foundation The
Testosterone treatment and cardiovascular and venous thromboembolism risk: what is new?
 Additional material is published online only. To view please visit the journal online (http:// dx. doi. org/ 10. 1136/ jim- 2017-000411). 1 Endocrinology Unit, Medical Department, Maggiore- Bellaria Hospital,
Additional material is published online only. To view please visit the journal online (http:// dx. doi. org/ 10. 1136/ jim- 2017-000411). 1 Endocrinology Unit, Medical Department, Maggiore- Bellaria Hospital,
SESSION 3 11 AM 12:30 PM
 SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
The Burden of the Diabetic Heart
 The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
Testosterone for the aging male; current evidence and recommended practice
 REVIEW Testosterone for the aging male; current evidence and recommended practice Roger D Stanworth T Hugh Jones Centre of Diabetes and Endocrinology, Barnsley Hospital NHS Foundation Trust, Barnsley,
REVIEW Testosterone for the aging male; current evidence and recommended practice Roger D Stanworth T Hugh Jones Centre of Diabetes and Endocrinology, Barnsley Hospital NHS Foundation Trust, Barnsley,
The clinical importance of testosterone in men with type 2 diabetes
 22 The clinical importance of testosterone in men with type 2 diabetes GEOFF HACKETT Although the association of low testosterone with type 2 diabetes is well established, testosterone levels are not routinely
22 The clinical importance of testosterone in men with type 2 diabetes GEOFF HACKETT Although the association of low testosterone with type 2 diabetes is well established, testosterone levels are not routinely
What Is the Low T Syndrome? Is Testosterone Supplementation Safe?
 What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or