IL RUOLO DEL DEFICIT DI TESTOSTERONE NELLA SINDROME METABOLICA E NELLA INSUFFICIENZA RENALE NEL MASCHIO ADULTO. VA Giagulli
|
|
|
- Lester Nash
- 6 years ago
- Views:
Transcription


1 IL RUOLO DEL DEFICIT DI TESTOSTERONE NELLA SINDROME METABOLICA E NELLA INSUFFICIENZA RENALE NEL MASCHIO ADULTO VA Giagulli UOS di Endocrinologia e Malattie Metaboliche PT di Conversano ASL BA
2 Male hypogonadism - classification Hypogonadism Primary hypogonadism Secondary hypogonadism Target organ resistance (T & LH +) Age-related hypogonadism LH -/+ T - Feminisation due to androgen resistance or Late onset hypogonadism LH + T - LH - T - 5-alpha-reductase deficiency Estrogen deficit due to aromatase deficiency The role of Diseases!!! Testicular causes Hypothalamic causes Pituitary causes Klinefelter syndrome Idiopathic hypogonado- Hypopituitarism Orchitis tropic hypogonadism Congenital or acquired Kallmann syndrome Pituitary tumors anorchia Constitutional delay of Testicular maldescent growth and development Testicular tumor Jockenhövel F: Male hypogonadism. UNI_MED Verlag Bremen 2004 Prepubertal forms Postpubertal forms
 20 15 12 10 8 0 Loss of libido P<0.001 Loss of vigour P<0.001 Obesity P<0.001 Feeling depressed P=0.")

3 Symptom-specific threshold testosterone levels for observed increase of prevalence in patients attending an andrology clinic Total testosterone (nmol/l) Loss of libido P<0.001 Loss of vigour P<0.001 Obesity P<0.001 Feeling depressed P=0.001 Disturbed sleep P=0.004 Lacking concentration P=0.002 Diabetes mellitus type 2 P<0.001 Hot flushes P<0.001 Erectile dysfunction P=0.003 Patients (n) Increasing prevalence of symptoms with decreasing testosterone concentrations Zitzmann et al. JCEM 2006;91:4335

4 Identification of late onset hypogonadism (EMAS) Wu et al NEJM 363:123-35; 2010 Prevalence: 0.1% 40-49y 0.6% 50-59y 3.2% 60-69y 5.1% 70-79y 4
5 Serum testosterone and SHBG vs age Kaufman &Vermeulen Endocr Rev 2005 according to Vermeulen et al JCEM,1996 5
6 FAT DISTRUBUTION AND DEPOSITION ACROSS THE LIVE IN MEN (E2 = 30 pg/ml) Lean ass cft= 2 ng/dl cft= 12 ng/dl Obese man T< 300 ng/dl SHBG = <30 nm/l cft=< 6 ng/dl cft= 4,5 ng/dl Fat mass PUBERTY T = < 200 ng/dl SHBG = 80 nm/l ADULT T = 600 ng/dl SHBG = 35 nm/l AGEING T = < 300 ng/dl SHBG = 55 nm/l Giagulli VA & Vermeulen A,1994 e 1996
7 Three Ways to Review Effects of Testosterone in Men 1. Evidence from Epidemiology and Observation 2. Evidence from Testosterone Deprivation 3. Evidence from Testosterone Treatment
8 JCEM,2012

9
10 Cross-sectional survey on 3200 community - dwelling men aged yr from a prospective cohort study in 8 European countries Wu et al., J Clin Endocrinol Metab. 2008;93:2737
 2,66nMol/=")
11 Random-Effects Pooled Mean Difference of Serum T Between Type 2 Diabetes Cases and Controls in Men (Ding EL et al JAMA,2006) 2,66nMol/= 77 ng/dl
12
13
14 Changes in Body Composition in 32 Men after Androgen Deprivation Therapy for Prostate Cancer for 48 weeks p=0.005 Baseline Basal 48 weeks p< p=0.005 p< Weight (kg) BMI (kg/m2) Fat mass (%) (DEXA) Lean mass (%) (DEXA) Smith MR et al. J Clin Endocrinol Metab 87(2): (2002)
15 GnRH Agonists are Associated with Significant Excess Risk of Diabetes, Coronary Heart Disease, Myocardial Infarction, and Sudden Cardiac Death Adjusted Hazard Ratios Excess Risk p value Diabetes 44 % <0.001 Coronary heart disease 16 % <0.001 Myocardial infarction 11 % 0.03 Sudden cardiac death 16 % Better Worse Saylor PJ and Smith MR J Urol 181: (2009)
16 Effects of Testosterone Therapy on Total Body Fat: a Meta-Analysis Baseline T < 10 nmol/l Morley et al. (1993) Sih et al. (1997) Boyanov et al. (2003) Steidle 1 et al. (2003) Steidle 2 et al. (2003) Page et al. (2005) Subtotal Baseline T > 10 nmol/l Marin et al. (1992) Snyder A et al. (1999) Kenny et al. (2001) Ly et al. (2001) Blackman et al. (2002) Wittert et al. (2003) Liu et al. (2003) Casaburi et al. (2004) Subtotal Glucocorticoid Treated Reid et al. (1996) Crawford et al. (2003) Overall Mean Difference (95%Cl) 1.86 (-5.09, 8.80) (-9.24, 0.10) (-9.25, 6.45) (-3.99, 2.19) -0.9 (-3.13, 1.33) (-10.97, 1.37) (-3.01, 0.09) 1.60 (-6.21, 3.01) (-4.66, 0.66) (-4.47, 1.67) (-6.81, 2.21) (-5.37, 3.17) (-5.27, 3.37) (-3.54, 0.94) (-7.68, 5.82) (-2.72, 0.28) (-7.48, 1.68) (-12.30, 6.30) (-2.49, 0.63) Total Fat Mass (kg) Isidori AM et al. Clin Endocrinol 63: (2005)
17 Effects of Testosterone Therapy on Total Fat Free Mass: a Meta-Analysis Baseline T < 10 nmol/l Boyanov et al. (2003) Steidle 1 et al. (2003) Steidle 2 et al. (2003) Page et al. (2005) Subtotal Baseline T > 10 nmol/l Marin et al. (1992) Tenover (1992) Clague et al. (1999) Snyder A et al. (1999) Ly et al. (2001) Kenny B et al. (2001) Blakman et al. (2002) Ferrando et al. (2003) Wittert et al. (2003) Liu et al. (2003) Casaburi et al. (2004) Subtotal Glucocorticoid Treated Reid et al. (1996) Crawford et al. (2003) Overall Mean Difference (95%Cl) (-5.00, 4.00) 0.80 (-2.10, 3.70) 0.90 (-1.73, 3.53) 3.98 (-0.21, 8.17) 1.16 (-0.49, 2.80) 0.40 (-5.98, 6.78) 1.90 (-2.35, 6.15) (-8.62, 7.02) 2.40 (0.153, 4.65) 1.20 (-3.19, 5.59) 0.80 (-2.48, 4.08) 1.50 (-2.20, 5.20) 6.20 (-2.83, 15.23) 1.65 (-2.30, 5.60) 2.90 (-1.86, 7.66) 2.09 (-3.99, 8.17) 1.80 (0.57, 3.03) 2.30 (-2.85, 7.45) 2.30 (-4.39, 8.99) 1.61 (0.65, 2.57) Total Fat Free Mass (kg) Isidori AM et al. Clin Endocrinol 63: (2005)
18 What is the possible mechanism causing hypogonadism in man affected by metabolic diseases and renal failure?
19 Normal physiology Preoptic area Leptin + Glicaemia
 c= p <0.01 vs nonobese d= p< 0.05 vs nonobese Functional Hypogonadism (?")
20 ANDROGENS AND INSULIN PLASMA LEVELS IN NONOBESE HEATHY MEN AND OBESE MEN (Giagulli VA et al, 1994) c= p <0.01 vs nonobese d= p< 0.05 vs nonobese Functional Hypogonadism (?)
 c= p <0.01 vs nonobese d= p< 0.")
21 INFLUENCE OF THE DEGREE OF OBESITY ON SERUM LH AND MEAN OF PULSE AND SUM OF PULSE AMPLITUDE (Giagulli et al 1994) c= p <0.01 vs nonobese d= p< 0.05 vs nonobese

22 Serum T, E, LH, FSH after Letrozolo 2,5mg/d in Hypogonadic Obese men (de Boer et al, 2005)


23 Inter.J End. 2014
24
25 Testis damage in chronic renal diseases (Clinical aspects)
26


27 Fertility in male with chronic kidney disease Xu HM et al, 2012
28 Testosterone Replacement Therapy

29 Current Testosterone Formulations on Market Giagulli et al Curr.Pharm.Design,2011
30

31
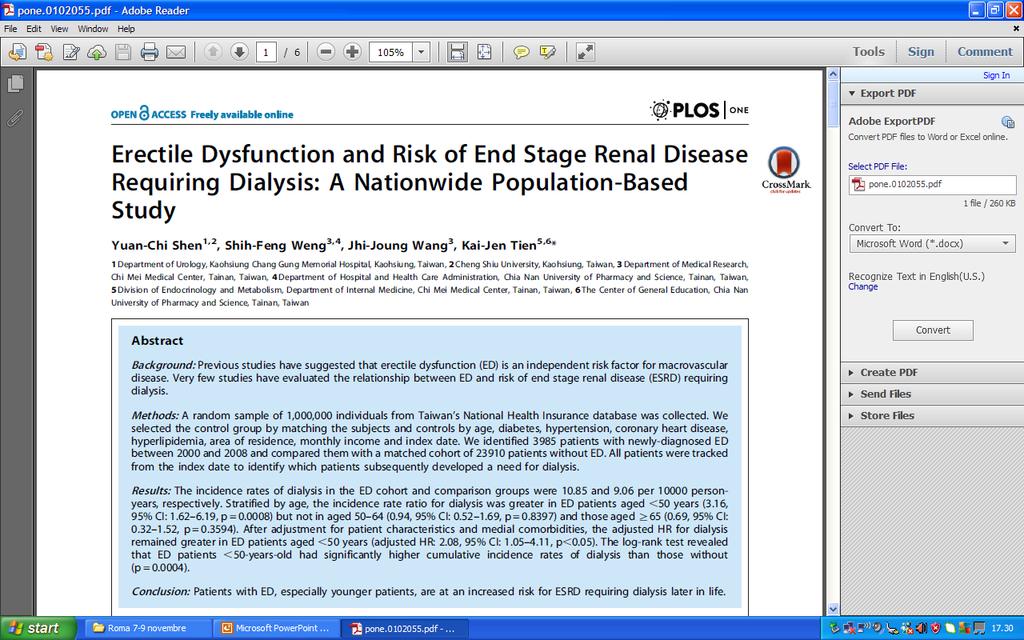
32 TESTOSTERONE THERAPY AND END-STAGE RENAL DISEASE TU os (240 mg/die x 3 mesi): < PRL e LH (Van Coevorden et al,1986) Differenti Tuttavia studi hanno i dati (RCTs) documentato in lettaratura che la terapia sono con T sulla DE è efficace veramente solo scarsi in caso e pertanto di ipogonadismo non franco (Canguven possono O et al essere 2010) considerati definitivi La somminstrazione di T migliora l eritropeotina e l anemia nei pazienti I distubi con biochinici insufficienza e quelli renale cronica di fase avanzata clinici dell ipogonadismo (Gaughan WJ 1997). nel paziente con stadio finale della insufficienza renale MIGLIORANO con il trapianto Iglesias P et al J Nephrol, 2012
 103 55.4±1.9 33 FT<146 pm Corona et al., (ITA-2004) 155 58.0± 8.9 34 TT < 12 nm Corona et al., (ITA-2006) 199 58.9± 8.2 24.5 TT < 10.4 nm Kapoor et al., (UK- 2007) 355 58.1±0.")
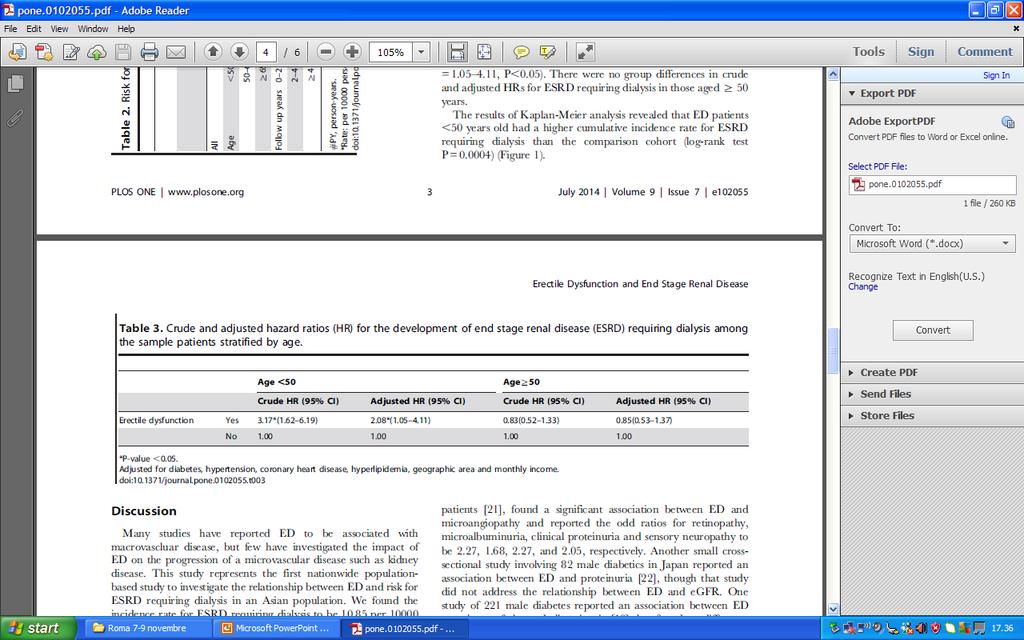
33 PREVALENCE of HYPOGONADISM IN T2 DM References n Age(years) % Criteria used Barrett-Connor et al. (US-1990) TT< 12nM Tan et al. (US-2002) 71 mean TT < 10.4 nm Dhindsa et al., (US-2004) ± FT<146 pm Corona et al., (ITA-2004) ± TT < 12 nm Corona et al., (ITA-2006) ± TT < 10.4 nm Kapoor et al., (UK- 2007) ± TT< 8 nm Kapoor et al., (UK- 2007) ± TT< 12 nm Kapoor et al., (UK- 2007) ± FT< 255 pm Grossman et al (AU- 2008) ± 1 43 TT < 10 nm
34

35 Corona et al., J Sex Med. 2014;11:1577 The effects of testosterone supplementation (TS) on male sexual functions in ED subjects are still more controversial. Another controversial issue is the effect of TS on PDE5i outcomes The aim of present study is to meta-analyse available data evaluating the effect TS on male sexual function and its therapeutic synergism with the combined use of PDE5i.
36 PUBLISHED studies Medline search N=1703 Review or Editorial N=4 No testosterone use included=649 No RCT studies N=755 Women N=5 Review n N=3 No data on sexual function N=245 UNPUBLISHED Studies N=31 Ongoing N=5 No testosterone use included=3 No data on sexual function N=9 No results available N=13 Case report N=1 40 Retrieved TOTAL N=41 N=1 Retrieved TS vs. placebo N=28 TS+PDE5ì vs. nothing or placebo + PED5ì N=12 TS vs. placebo N=1 Eugonadal N=5 Mixed N=5 Hypogonadal N=18 hypogonadal N=0 Mixed N=3 Eugonadal N=9 Hypogonadal N=1

")
")
37 Male sexual response cycle Motivation (libido) Arousal (erection) Orgasm (ejaculation)
38 Effect size (with 95%CI) of testosterone supplementation (TS) versus placebo on libido component Source Libido component standardized mean differences - 0,50 0,00 0,50 1,00 1,50 2,00 2,50 3, Diff. in mean LL, 95% CI UL, 95% CI p Overall eugonadal Overall mixed Overall hypogonadal Overall hypogonadal (TT <12 nm) Overall hypogonadal (TT < 8 nm) Overall pharmaceutical industry supported Overall pharmaceutical industry not supported 0,25-0,24 0,74 0,320 0,64 0,14 1,13 0,012 1,00 0,47 1,53 0,012 0,97 0,22 1,71 0,271 0,98 0,42 1,53 0,012 0,43 0,26 0,60 0,000 1,34 0,29 2,39 0,000 Overall , , , ,000 Placebo TS Corona et al., 2013 submitted
39 Conclusions T supplementation is able to improve libido but only in hypogonadal men (TT < 12 nm)
40 Effect size (with 95%CI) of testosterone supplementation (TS) versus placebo on overall erectile function component (including sexual and spontaneous erections) Source Overall erectile function component standardized mean differences Diff. in mean LL, 95% CI UL, 95% CI p - 0,50 0,00 0,50 1,00 1,50 2,00 2,50 Overall eugonadal Overall mixed Overall hypogonadal Overall hypogonadal (TT <12 nm) Overall hypogonadal (TT < 8 nm) Overall pharmaceutical industry supported 0,19-0,19 0,58 0,323 0,18-0,13 0,48 0,261 1,23 0,74 1,72 0,002 1,25 0,51 1,99 0,001 1,23 0,56 1,90 0,000 1,36 0,55 2,16 0,001 Overall pharmaceutical industry not supported 0,33 0,13 0,54 0,001 Overall Overall , , , ,001 Placebo TS
41 Conclusions T supplementation is able to improve libido but only in hypogonadal men (TT < 12 nm) T supplementation is able to improve erectile function but only in hypogonadal men (TT < 12 nm)
42 Effect size (with 95%CI) of testosterone supplementation (TS) versus placebo on erectile function component (including only sexual-related erections) Source Erectile function component standardized mean differences Diff. in mean LL, 95% CI UL, 95% CI p - 0,50 0,00 0,50 1,00 1,50 2,00 2,50 3,00 3,50 4,00 Overall oral formulations 1,77-0,19 3,73 0,076 Overall transdermal formulations 0,31 0,04 0,59 0,026 Overall parental formulations 0,46 0,18 0,74 0,001 Overall 0,75 0,37 1,12 0,000 Placebo TS
43 Conclusions T supplementation is able to improve libido but only in hypogonadal men (TT < 12 nm) T supplementation is able to improve erectile function but only in hypogonadal men (TT < 12 nm). No differences between transdermal and parental formulations
44 Effect size (with 95%CI) of testosterone supplementation (TS) versus placebo on orgasm component Source Orgasm component standardized mean differences Diff. in mean LL, 95% CI UL, 95% CI p - 5,00-4,00-3,00-2,00-1,00 0,00 1,00 2,00 3,00 4,00 5,00 Skakkebaek et al., ,46 0,52 2,40 0,00 Davidson et al., ,06-0,26 2,39 0,12 Kwan et al., ,58-0,26 3,41 0,09 Gluud et al., ,11-0,27 0,49 0,58 Carani et al., ,79-0,38 1,97 0,19 Schiavi et al., ,62 0,30 2,94 0,02 Cavallini et al., ,00 0,54 1,46 0,00 Chaing et al., ,97 0,31 1,62 0,00 Jones et al., ,05-0,24 0,34 0,74 Hackett et al., ,42 0,13 0,72 0,00 Overall ,68 0,34 1,02 0,00 Placebo TS

45 Recommendation 11: Combination therapy with T and PDE5- Is (EBMl1b). Evidence is emerging suggesting a therapeutic synergism with the combined use of Tth and PDE5-Is in men with ED and low T. These observations are preliminary and need additional studies. However, combination therapy can be considered in TD men who have not improved with T alone. In addition it is recommended to measure T in case of PDE5-Is failure if not previously done. Data suggests that the threshold level of T for optimal response to PDE5-Is is 3 ng/ml for TT and 52 pg/ml (180 pmol/l) for cft. J Sex Med. 2013;10:245.
46 Source Standardized mean differences - 2,00 0,00 2,00 4,00 6,00 8,00 10,00 12, Diff. in mean LL, 95% CI UL, 95% CI p Kalinchenko et al., 2003 Foresta eta la., 2004 Shamloul et al., 2005 Roschira et al 2006 Hwang et al., 2006 Garcia et al., 2009 Kim et al., 2013 Overall non placebo controlled 7,71 6,57 8,84 0,00 1,57 0,56 2,58 0,00 1,02 0,09 1,95 0,03 0,96 0,36 1,56 0,00 0,74 0,18 1,31 0,01 8,86 7,17 10,55 0,00 0,69 0,23 1,15 0,00 2,96 1,28 4,64 0,00 Aversa et al., ,98 3,21 6,76 0,00 Shabshig et al., 2004 Favours PDE5is Favours PDE5is + TS - 0,33-0,80 0,14 0,17 Buvat et al., ,20-0,10 0,50 0,20 Spitzer et al., ,17-0,19 0,53 0,36 HackeH et al., ,17-0,57 0,91 0,65 Overall placebo controlled 0,49-0,16 1,15 0,14
47 Source Standardized mean differences - 2,00 0,00 2,00 4,00 6,00 8,00 10,00 12, Diff. in mean LL, 95% CI UL, 95% CI p Kalinchenko et al., 2003 Foresta eta la., 2004 Shamloul et al., 2005 Roschira et al 2006 Hwang et al., 2006 Garcia et al., 2009 Kim et al., 2013 Overall non placebo controlled Aversa et al., 2003 Shabshig et al., 2004 Buvat et al., 2009 Spitzer et al., 2012 HackeH et al., 2013 Overall placebo controlled 7,71 6,57 8,84 0,00 1,57 0,56 2,58 0,00 1,02 0,09 1,95 0,03 0,96 0,36 1,56 0,00 0,74 0,18 1,31 0,01 8,86 7,17 10,55 0,00 0,69 0,23 1,15 0,00 2,96 1,28 4,64 0,00 4,98 3,21 6,76 0,00-0,33-0,80 0,14 0,17 0,20-0,10 0,50 0,20 0,17-0,19 0,53 0,36 0,17-0,57 0,91 0,65 0,49-0,16 1,15 0,14 Favours PDE5is Favours PDE5is + TS
48 Favours PDE5is Favours PDE5is + TS Source Standardized mean differences - 2,00 0,00 2,00 4,00 6,00 8,00 10,00 12, Diff. in mean LL, 95% CI UL, 95% CI p Kalinchenko et al., 2003 Foresta eta la., 2004 Shamloul et al., 2005 Roschira et al 2006 Hwang et al., 2006 Garcia et al., 2009 Kim et al., 2013 Overall non placebo controlled Aversa et al., ,71 6,57 8,84 0,00 1,57 0,56 2,58 0,00 1,02 0,09 1,95 0,03 0,96 0,36 1,56 0,00 0,74 0,18 1,31 0,01 8,86 7,17 10,55 0,00 0,69 0,23 1,15 0,00 2,96 1,28 4,64 0,00 4,98 3,21 6,76 0,00 Shabshig et al., 2004 Buvat et al., 2009 Spitzer et al., 2012 HackeH et al., 2013 Mixed eugonadal/hypogonadal subjects - 0,33-0,80 0,14 0,17 0,20-0,10 0,50 0,20 0,17-0,19 0,53 0,36 0,17-0,57 0,91 0,65 Overall placebo controlled 0,49-0,16 1,15 0,14
49 Change in IIEF scores with sildenafil alone or in combination with testosterone or placebo. Spitzer et al., Ann Int Med. 2012;157:681
50 Conclusions T supplementation is able to improve libido but only in hypogonadal men (TT < 12 nm) T supplementation is able to improve erectile function but only in hypogonadal men (TT < 12 nm). No differences between transdermal and parental formulations T supplementation is able to improve orgasm function particularly in subjects with low T levels More studies comparing PDE5i+T in hypogonadal subjects are advisable
51 Trial Flow Diagram Records identified through different sources n = 2747 Records removed: No clinical trials n = 2287 No human species n = 2 No english language n = 13 No male subsjects n = 145 Full-text articles assessed for eligibility n = 300 Full-text articles excluded: Women n = 4 No T use included n = 45 No RCT n = 21 No placebo (or p-only) arm n = 108 No T-only arm n = 4 Study duplicates n = 18 UNPUBLISHED Studies n = 649 Ongoing n = 202 No results available n = 372 No placebo n = 26 Women n = 21 No T arm n = 27 Study assessed for eligibility n = 1 Studies included in qualitative synthesis n = 101 RCT: Randomized clinical trials; T: Testosterone. Studies excluded (see table 6) n = 26 Studies included in quantitative synthesis (meta-analysis) n = 75 Corona G et al. Expert Opin Drug Saf, published online August 19, 2014
52 Odds Ratio for Major Adverse Cardiovascular Events (MACE) in Subjects Treated with Testosterone or Placebo MACE: cardiovascular death, non-fatal myocardial infarction, stroke, acute coronary syndromes, and/or heart failure Odds ratio for MACE TRT Placebo Source MH - OR LL UL p #Events # Patients #Events # Patients Copenhagen SG, 1986 (31) 1,97 0,08 48,82 0,68 Hall et al., 1996 (34) 0,32 0,01 8,23 0,49 Sih et al., 1997 (36) 0,88 0,05 15,33 0,93 Snyder et al., 1999 (40) 2,04 0,18 23,17 0,57 English et al., 2000 (42) 3,12 0,12 80,39 0,49 Seidman et al., 2001 (47) 0,41 0,02 10,83 0,59 Steidle et al., 2003 (52) 2,83 0,11 70,27 0,53 Armory et al., 2004 (54) 3,13 0,12 80,68 0,49 Kenn et al., 2004 (56) 0,23 0,01 7,05 0,40 Svartberg et al., 2004 (60) 0,29 0,01 7,74 0,46 Brockenbrough et al., 2006 (63) 3,75 0,36 39,59 0,27 Malkin et al., 2006 (69) 2,17 0,19 25,01 0,53 Nair et al., 2006 (72) 5,70 0,26 123,78 0,27 Svartberg et al., 2008 (81) 3,16 0,12 82,64 0,49 Chapman et al., 2009 (84) 1,00 0,05 20,83 1,00 Legros et al., 2009 (85) 1,01 0,04 25,01 1,00 Aversa et al., 2010 (89) 0,08 0,00 2,07 0,13 Aversa et al., 2010 (90) 0,07 0,00 1,97 0,12 Basaria et al., 2010 (11) 13,39 0,74 240,78 0,08 Kalinchenko et al., 2010 (92) 0,21 0,01 5,15 0,34 Srinivas- Shankar et al., 2010 (93) 1,01 0,14 7,31 0,99 Ho et al., 2011 (95) 1,00 0,06 16,37 1,00 Jones et al., 2011 (96) 0,51 0,05 5,75 0,59 Kaufman et al (97) 0,87 0,04 18,48 0,93 Behre et al (99) 2,95 0,12 72,91 0,51 Hildreth et al (100) 0,15 0,02 1,53 0,11 Overall 1,01 0,57 1,77 0,96 LL: Lower limit; MH-OR: Mantel-Haenszel odds ratio; UL: Upper limit Placebo TS Corona G et al. Expert Opin Drug Saf, published online August 19, 2014
53 Odds Ratio for Acute Myocardial Infarction (AMI), Acute Coronary Syndrome, Stroke, Heart Failure, and Cardiovascular (CV) Mortality in Subjects Treated with Testosterone or Placebo Source # Trials Odds ratio for MH-OR LL UL p 0.01 MACE TRT Placebo #Events # Patients #Events # Patients AMI 14 0,68 0,30 1,52 0, Acute coronary syndrome 15 0,92 0,43 1,97 0, Stroke 5 0,82 0,24 2,83 0, New heart failure 3 1,64 0,25 10,63 0, CV mortality 13 1,14 0,49 2,66 0, Placebo TS LL: Lower limit; MACE: Major adverse cardiovascular events; MH-OR: Mantel-Haenszel odds ratio; UL: Upper limit Corona G et al. Expert Opin Drug Saf, published online August 19, 2014
54 Odds Ratio for Major Adverse Cardiovascular Events (MACE) According to Baseline Characteristics in Subjects Treated with Testosterone or Placebo MACE: cardiovascular death, non-fatal myocardial infarction, stroke, acute coronary syndromes, and/or heart failure Source # Trials MH-OR LL UL p Odds ratio for TRT Placebo 0.01 MACE #Events # Patients #Events # Patients Associated diseases Elderly men 10 1,22 0,49 3,03 0,67 Men with CVD 2 2,48 0,35 17,45 0,36 Frail men 5 2,25 0,72 7,08 0,17 Men with metabolic diseases 4 0,19 0,04 0,85 0, Hypogonadism status Mixed population 14 1,26 0,58 2,73 0,56 TT < 12 nm 12 0,84 0,32 2,23 0, Type of support Drug company not supported 12 0,94 0,39 2,24 0,88 Drug company supported 14 1,07 0,51 2,24 0, Trial duration 12 weeks 4 1,02 0,20 5,29 0,98 >12 weeks 22 1,01 0,55 1,84 0, CVD: Cardiovascular diseases; LL: Lower limit; UL: Upper limit; MH-OR: Mantel-Haenszel odds ratio; TT: Total testosterone Placebo TS Corona G et al. Expert Opin Drug Saf, published online August 19, 2014
55 TRT and Prostatic Cancer Until now there has been no data showing a direct correlation between TRT and Prostatic Carcer (Morgantaler, 2006) However, to have a definitive evidence, Some meta-analysis there would be almost studies 6000 did hypogonadal not present men a significant difference who in have prostatic been treating carcer with between T for 5 yrs patients least. treated with TRT or (Cunningham placebo GR (Calof & Toma OM SM, et JCEM, al et 2010) al 2005, Fernadez-Barsells MM et al, 2010). Similar results were found by another Authors: Krieg et al 1993 Slater et al 2000 Heikkila et al 1999 Hsing et al 2001 Zitzmann et all, 2013
56 Hypogonadism, Metabolic diseases Chronic renal diseases and CVD CVD Obesity Metabolic Syndrome Chronic renal Diseases Diabetes Aging Male INSULIN RESISTANCE Hypotestosteronemia

57 Thanks for bearing with me
Take-Home Messages: Androgens
 Take-Home Messages: Androgens Anthony J. Bella MD, FRCSC Greta and John Hansen Chair in Men s Health Research Division of Urology, Department of Surgery University of Ottawa SUMMARY SLAMS Symposium Clinical
Take-Home Messages: Androgens Anthony J. Bella MD, FRCSC Greta and John Hansen Chair in Men s Health Research Division of Urology, Department of Surgery University of Ottawa SUMMARY SLAMS Symposium Clinical
Update on diagnosis and complications of adult and elderly male hypogonadism
 Hypoandrogenism in the elderly: to treat or not to treat? 12 th Italian AME Meeting; 6 th joint Meeting with AAC Bari november 10th Update on diagnosis and complications of adult and elderly male hypogonadism
Hypoandrogenism in the elderly: to treat or not to treat? 12 th Italian AME Meeting; 6 th joint Meeting with AAC Bari november 10th Update on diagnosis and complications of adult and elderly male hypogonadism
Testosterone Therapy in Men An update
 Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
What Is the Low T Syndrome? Is Testosterone Supplementation Safe?
 What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
An Idea Whose Time Has Come-Male Health Programs: An Opportunity For Clinical Expansion and Better Health
 An Idea Whose Time Has Come-Male Health Programs: An Opportunity For Clinical Expansion and Better Health KEVIN R. LOUGHLIN MD,MBA Harvard Medical School Boston, MA THE WEAKER SEX-MALES LIFE EXPECTANCY
An Idea Whose Time Has Come-Male Health Programs: An Opportunity For Clinical Expansion and Better Health KEVIN R. LOUGHLIN MD,MBA Harvard Medical School Boston, MA THE WEAKER SEX-MALES LIFE EXPECTANCY
The reality of LOH-symptoms
 The reality of LOH-symptoms PRISM IV Bruges, Belgium September 25-26, 2014 Dr. Herman Leliefeld Androsmannenkliniek The Netherlands The reality of LOH symptoms male external & internal genitalia Testosterone
The reality of LOH-symptoms PRISM IV Bruges, Belgium September 25-26, 2014 Dr. Herman Leliefeld Androsmannenkliniek The Netherlands The reality of LOH symptoms male external & internal genitalia Testosterone
ENDOCRINOLOGICAL IMPLICATIONS AND COMPLICATIONS OF TESTOSTERONE REPLACEMENT IN AGEING MEN
 ENDOCRINOLOGICAL IMPLICATIONS AND COMPLICATIONS OF TESTOSTERONE REPLACEMENT IN AGEING MEN Frederick C.W. Wu Professor of Medicine and Endocrinology Andrology Research Unit, Centre for Endocrinology and
ENDOCRINOLOGICAL IMPLICATIONS AND COMPLICATIONS OF TESTOSTERONE REPLACEMENT IN AGEING MEN Frederick C.W. Wu Professor of Medicine and Endocrinology Andrology Research Unit, Centre for Endocrinology and
Diagnosis and Clinical Evaluation of Hypogonadism in Adult Patients with Obesity and Diabetes
 Diagnosis and Clinical Evaluation of Hypogonadism in Adult Patients with Obesity and Diabetes Adrian Dobs, M.D., M.H.S. Professor of Medicine and Oncology The Johns Hopkins University School of Medicine
Diagnosis and Clinical Evaluation of Hypogonadism in Adult Patients with Obesity and Diabetes Adrian Dobs, M.D., M.H.S. Professor of Medicine and Oncology The Johns Hopkins University School of Medicine
Alternative management of hypogonadism Tamoxifen. Emmanuele A. Jannini, MD Tor Vergata University of Rome ITALY
 Alternative management of hypogonadism Tamoxifen Emmanuele A. Jannini, MD Tor Vergata University of Rome ITALY eajannini@gmail.com What hypogonadism is? What hypogonadism is? It is an empty glass The two
Alternative management of hypogonadism Tamoxifen Emmanuele A. Jannini, MD Tor Vergata University of Rome ITALY eajannini@gmail.com What hypogonadism is? What hypogonadism is? It is an empty glass The two
Outline. Classic Androgen deficiency. Cardiovascular Risk and Testosterone Fact vs Fiction. Professor Robert I McLachlan AM, FRACP, PhD
 Health Ed Brisbane Saturday 27 th October 2018 Cardiovascular Risk and Testosterone Fact vs Fiction Professor Robert I McLachlan AM, FRACP, PhD Hudson Institute of Medical Research, Monash University Department
Health Ed Brisbane Saturday 27 th October 2018 Cardiovascular Risk and Testosterone Fact vs Fiction Professor Robert I McLachlan AM, FRACP, PhD Hudson Institute of Medical Research, Monash University Department
Hypogonadism* (män) Erytrocytos Kardiovaskulär risk
 Erytrocytos Kardiovaskulär risk") Hypogonadism* (män) Erytrocytos Kardiovaskulär risk *Lågt Testosteron och symtom Stefan Arver ANOVA, Karolinska Univ Sjukhuset Inst. F Medicin/Huddinge Karolinska Institutet Endokrindagar i Umeå 2019 1
Hypogonadism* (män) Erytrocytos Kardiovaskulär risk *Lågt Testosteron och symtom Stefan Arver ANOVA, Karolinska Univ Sjukhuset Inst. F Medicin/Huddinge Karolinska Institutet Endokrindagar i Umeå 2019 1
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA
 Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
Hypogonadism 4/27/2018. Male Hypogonadism -- Definition. Epidemiology. Objectives HYPOGONADISM. Men with Hypogonadism. 95% untreated.
 Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
PRISM Bruges June Herman Leliefeld Urologist. The Netherlands
 PRISM Bruges 25-26 June 2015 Herman Leliefeld Urologist The Netherlands Guidelines EAU 2015: a rich source of Knowledge! Epidemiology/ Aetiology / Pathology Diagnostic evaluation Disease management Follow-Up
PRISM Bruges 25-26 June 2015 Herman Leliefeld Urologist The Netherlands Guidelines EAU 2015: a rich source of Knowledge! Epidemiology/ Aetiology / Pathology Diagnostic evaluation Disease management Follow-Up
Testosterone Replacement Therapy for Hypogonadism: Learning Objectives. What Is the Evidence? Is It Safe? Case Study. Case Study contd.
 4 4:4pm Testosterone Therapy: Examining the Evidence SPEAKER Culley Carson, MD Presenter Disclosure Information The following relationships exist related to this presentation: Culley Carson, MD: Consultant
4 4:4pm Testosterone Therapy: Examining the Evidence SPEAKER Culley Carson, MD Presenter Disclosure Information The following relationships exist related to this presentation: Culley Carson, MD: Consultant
Recognizing and Managing Testosterone Deficiency
 Recognizing and Managing Testosterone Deficiency J. Bruce Redmon, M.D. Professor Division of Endocrinology Departments of Medicine and Urologic Surgery Disclosure Information I have no financial relationships
Recognizing and Managing Testosterone Deficiency J. Bruce Redmon, M.D. Professor Division of Endocrinology Departments of Medicine and Urologic Surgery Disclosure Information I have no financial relationships
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency
 Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
Endocrine Update Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh
 Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Testosterone Treatment: Myths Vs Reality. Fadi Al-Khayer, M.D, F.A.C.E
 Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
GUIDELINES ON. Introduction. G.R. Dohle, S. Arver, C. Bettocchi, S. Kliesch, M. Punab, W. de Ronde
 GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
Disclosures. Advisory Boards 6/10/2014
 Massachusetts Medical Society 12 th annual Men s Health Symposium 11 June 2014 Testosterone and Cardiovascular Disease Where Does The Real Answer Lie? Andre Guay MD, FACP, FACE, IF (Ret) Director, Center
Massachusetts Medical Society 12 th annual Men s Health Symposium 11 June 2014 Testosterone and Cardiovascular Disease Where Does The Real Answer Lie? Andre Guay MD, FACP, FACE, IF (Ret) Director, Center
Point-Counterpoint: Late Onset Hypogonadism (LOH)
") Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
GUIDELINES ON MALE HYPOGONADISM
 GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
Prof. Dr. Michael Zitzmann Internal Medicine Endocrinology, Diabetology, Andrology University of Muenster, Germany
 Induction of fertility in hypogonadal men Prof. Dr. Michael Zitzmann Internal Medicine Endocrinology, Diabetology, Andrology University of Muenster, Germany Induction of fertility in hypogonadal men Prof.
Induction of fertility in hypogonadal men Prof. Dr. Michael Zitzmann Internal Medicine Endocrinology, Diabetology, Andrology University of Muenster, Germany Induction of fertility in hypogonadal men Prof.
6/14/2010. GnRH=Gonadotropin-Releasing Hormone.
 Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
Erectile Dysfunction, Cardiovascular Risk and
 Erectile Dysfunction, Cardiovascular Risk and Testosterone National Lipid Association (NLA) 2016 Fall Clinical Update August 26-28, 2016 Amelia Island, Fl Robert A. Kloner MD, PhD Director of the Cardiovascular
Erectile Dysfunction, Cardiovascular Risk and Testosterone National Lipid Association (NLA) 2016 Fall Clinical Update August 26-28, 2016 Amelia Island, Fl Robert A. Kloner MD, PhD Director of the Cardiovascular
ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN
 International Society for Sexual Medicine - www.issm.info ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN Version: September 2015 What is testosterone deficiency? Testosterone deficiency
International Society for Sexual Medicine - www.issm.info ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN Version: September 2015 What is testosterone deficiency? Testosterone deficiency
Men Getting Older Will Testosterone Keep Him Young?
 Men Getting Older Will Testosterone Keep Him Young? Alvin M. Matsumoto, M.D. Associate Director, GRECC V.A. Puget Sound Health Care System Professor, Department of Medicine Division of Gerontology and
Men Getting Older Will Testosterone Keep Him Young? Alvin M. Matsumoto, M.D. Associate Director, GRECC V.A. Puget Sound Health Care System Professor, Department of Medicine Division of Gerontology and
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY)
") HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
Testosterone and PDE5 inhibitors in the aging male
 Testosterone and PDE5 inhibitors in the aging male Francesco Romanelli Department of Experimental Medicine Medical Pathophysiology, Food Science and Endocrinology Section Sapienza University of Rome 3005
Testosterone and PDE5 inhibitors in the aging male Francesco Romanelli Department of Experimental Medicine Medical Pathophysiology, Food Science and Endocrinology Section Sapienza University of Rome 3005
Managing Testosterone Deficiency: A Practical Guide. John Grantmyre MD Professor of Urology Dalhousie University
 Managing Testosterone Deficiency: A Practical Guide John Grantmyre MD Professor of Urology Dalhousie University 1 2 Case Study #1 A 59-Year-Old Man with Erectile Dysfunction 3 Case History Robert is a
Managing Testosterone Deficiency: A Practical Guide John Grantmyre MD Professor of Urology Dalhousie University 1 2 Case Study #1 A 59-Year-Old Man with Erectile Dysfunction 3 Case History Robert is a
Hypogonadism in Men. CME Away India & Sri Lanka March 23 - April 7, 2018
 Hypogonadism in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Hypogonadism in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE
 Authoriser: Moya O Doherty Page 1 of 7 BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE The purpose of this protocol is to describe common tests used for the investigation
Authoriser: Moya O Doherty Page 1 of 7 BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE The purpose of this protocol is to describe common tests used for the investigation
A dro r gen e R e R p e lac a e c m e e m n e t t T her e a r p a y Androgen Replacement Therapy in the Aging O j b ecti t ve v s Male
 Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Testosterone Therapy in Men with Hypogonadism
 Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
THE RELEVANCE OF TESTOSTERONE THERAPY IN MANAGING PATIENTS WITH ERECTILE DYSFUNCTION
 THE RELEVANCE OF TESTOSTERONE THERAPY IN MANAGING PATIENTS WITH ERECTILE DYSFUNCTION Aksam A. Yassin MD PhD EdD FEBU Professor of Urology & Human Sexuality Institute of Urology & Andrology, Segeberger
THE RELEVANCE OF TESTOSTERONE THERAPY IN MANAGING PATIENTS WITH ERECTILE DYSFUNCTION Aksam A. Yassin MD PhD EdD FEBU Professor of Urology & Human Sexuality Institute of Urology & Andrology, Segeberger
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
VII convegno nazionale fondazione AMD Baveno23-25 ottobre 2014
 VII convegno nazionale fondazione AMD Baveno23-25 ottobre 2014 SUBITO DE disfunzioni sessuali e rischio cardiovascolare. Il ruolo dell ipogonadismo Giovanni Corona MD, PhD Endocrinology Unit Medical Department,
VII convegno nazionale fondazione AMD Baveno23-25 ottobre 2014 SUBITO DE disfunzioni sessuali e rischio cardiovascolare. Il ruolo dell ipogonadismo Giovanni Corona MD, PhD Endocrinology Unit Medical Department,
Late onset Hypogonadism. Dr KhooSay Chuan Department of Urology Penang General Hospital
 Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
EFFICACY AND SAFETY OF TESTOSTERONE THERAPY FOR LATE-ONSET HYPOGONADISM: AN UPDATE
 EFFICACY AND SAFETY OF TESTOSTERONE THERAPY FOR LATE-ONSET HYPOGONADISM: AN UPDATE Matthew Ho, PGY-2 Department of Urologic Sciences University of British Columbia OBJECTIVES 1. Review the characteristics
EFFICACY AND SAFETY OF TESTOSTERONE THERAPY FOR LATE-ONSET HYPOGONADISM: AN UPDATE Matthew Ho, PGY-2 Department of Urologic Sciences University of British Columbia OBJECTIVES 1. Review the characteristics
/04/ /0 Reprinted from Vol. 172, , August 2004 THE JOURNAL OF UROLOGY
 0022-5347/04/1722-0658/0 Reprinted from Vol. 172, 658 663, August 2004 THE JOURNAL OF UROLOGY Printed in U.S.A. Copyright 2004 by AMERICAN UROLOGICAL ASSOCIATION DOI: 10.1097/01.ju.0000132389.97804.d7
0022-5347/04/1722-0658/0 Reprinted from Vol. 172, 658 663, August 2004 THE JOURNAL OF UROLOGY Printed in U.S.A. Copyright 2004 by AMERICAN UROLOGICAL ASSOCIATION DOI: 10.1097/01.ju.0000132389.97804.d7
Update on Androgen Deficiency. Acknowledgments. Curatio PowerPoint TemplateControversies in Male Hypogonadism Bradley D.
 The General Practice Education Day Healthed / Generation Next August 22 nd Sydney Update on Androgen Deficiency Robert I. McLachlan, FRACP, PhD Director, Andrology Australia Principal Research Fellow,
The General Practice Education Day Healthed / Generation Next August 22 nd Sydney Update on Androgen Deficiency Robert I. McLachlan, FRACP, PhD Director, Andrology Australia Principal Research Fellow,
Every obese male with type 2 diabetes should be screened for hypogonadism
 Every obese male with type 2 diabetes should be screened for hypogonadism FOR Professor T Hugh Jones Consultant Physician & Endocrinologist, Robert Hague Centre for Diabetes and Endocrinology, Barnsley
Every obese male with type 2 diabetes should be screened for hypogonadism FOR Professor T Hugh Jones Consultant Physician & Endocrinologist, Robert Hague Centre for Diabetes and Endocrinology, Barnsley
NEW DEVELOPMENTS: T & CVD FDA & THE T TRIALS
 NEW DEVELOPMENTS: T & CVD FDA & THE T TRIALS 2017 UPDATE FDUS Martin Miner MD Clinical Professor of Family Medicine and Urology Co-Director The Men s Health Center The Miriam Hospital Warren Albert School
NEW DEVELOPMENTS: T & CVD FDA & THE T TRIALS 2017 UPDATE FDUS Martin Miner MD Clinical Professor of Family Medicine and Urology Co-Director The Men s Health Center The Miriam Hospital Warren Albert School
Androgen deficiency. Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital
 Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
Disclosures. Faculty 3/5/18. Testosterone, the FDA and CVD Risk Controversies. Matt Rosenberg, MD Director of Mid-Michigan Health Centers Jackson, MI
 Testosterone, the FDA and CVD Risk Controversies Faculty Matt Rosenberg, MD Director of Mid-Michigan Health Centers Jackson, MI 2 Disclosures Matt Rosenberg, MD serves on the advisory board for Bayer,
Testosterone, the FDA and CVD Risk Controversies Faculty Matt Rosenberg, MD Director of Mid-Michigan Health Centers Jackson, MI 2 Disclosures Matt Rosenberg, MD serves on the advisory board for Bayer,
Does TRT Induce Prostate Cancer?
 Does TRT Induce Prostate Cancer? Prism VI, Bruges, Belgium 21-22November 2014 Herman Leliefeld, Urologist, Utrecht The Netherlands Does TRT Induce Prostate Cancer? Why is it a controversial topic? Is there
Does TRT Induce Prostate Cancer? Prism VI, Bruges, Belgium 21-22November 2014 Herman Leliefeld, Urologist, Utrecht The Netherlands Does TRT Induce Prostate Cancer? Why is it a controversial topic? Is there
Present and future association between obesity and hypogonadism in Italian male
 ORIGINAL PAPER DOI: 10.4081/aiua.2014.1.26 Present and future association between obesity and hypogonadism in Italian male Valentina Boddi 1, Valeria Barbaro 2, Paul Mc Nieven 3, Mario Maggi 1, Carlo Maria
ORIGINAL PAPER DOI: 10.4081/aiua.2014.1.26 Present and future association between obesity and hypogonadism in Italian male Valentina Boddi 1, Valeria Barbaro 2, Paul Mc Nieven 3, Mario Maggi 1, Carlo Maria
Late onset hypogonadism
 Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Disclosures. Learning Objectives. Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease. None
 Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
Over the past decade, androgen replacement
 J. Andrew Hoover, MD; Jeffrey T. Kirchner, DO, FAAFP Department of Family and Community Medicine, Lancaster General Hospital, Pa jhoover4@lghealth.org The authors reported no potential conflict of interest
J. Andrew Hoover, MD; Jeffrey T. Kirchner, DO, FAAFP Department of Family and Community Medicine, Lancaster General Hospital, Pa jhoover4@lghealth.org The authors reported no potential conflict of interest
HORMONE THERAPY IN AGING MALE ATHLETES
 DISCLOSURES HORMONE THERAPY IN AGING MALE ATHLETES No relevant affiliations or financial interests When, Why and is it Safe? OBJECTIVES Summarize the benefits of optimizing hormone balance Examine the
DISCLOSURES HORMONE THERAPY IN AGING MALE ATHLETES No relevant affiliations or financial interests When, Why and is it Safe? OBJECTIVES Summarize the benefits of optimizing hormone balance Examine the
The clinical importance of testosterone in men with type 2 diabetes
 22 The clinical importance of testosterone in men with type 2 diabetes GEOFF HACKETT Although the association of low testosterone with type 2 diabetes is well established, testosterone levels are not routinely
22 The clinical importance of testosterone in men with type 2 diabetes GEOFF HACKETT Although the association of low testosterone with type 2 diabetes is well established, testosterone levels are not routinely
How to treat: TRT modalities and formulations
 How to treat: TRT modalities and formulations Paul PIETTE, PharmD Senior Research Fellow Clinique Antoine Depage - Belgium ppiette@besins-healthcare.com Bruges 2014, May 15 th Testosterone-replacement
How to treat: TRT modalities and formulations Paul PIETTE, PharmD Senior Research Fellow Clinique Antoine Depage - Belgium ppiette@besins-healthcare.com Bruges 2014, May 15 th Testosterone-replacement
Testosterone Therapy and the Prostate. Frans M.J. Debruyne Professor of Urology The Netherlands
 Testosterone Therapy and the Prostate Frans M.J. Debruyne Professor of Urology The Netherlands TRT- Risks Prostate ( Cancer, BPH )? Cardiac? Lipids? Polycythemia Sleep apnea Gynecomastia Edema Testosterone
Testosterone Therapy and the Prostate Frans M.J. Debruyne Professor of Urology The Netherlands TRT- Risks Prostate ( Cancer, BPH )? Cardiac? Lipids? Polycythemia Sleep apnea Gynecomastia Edema Testosterone
Assessment and management of male androgen disorders: an update
 Irene Chan Mark Ng Tang Fui Jeffrey D Zajac Mathis Grossmann Assessment and management of male androgen disorders: an update Background Male hypogonadism, caused by intrinsic pathology of the hypothalamic
Irene Chan Mark Ng Tang Fui Jeffrey D Zajac Mathis Grossmann Assessment and management of male androgen disorders: an update Background Male hypogonadism, caused by intrinsic pathology of the hypothalamic
Male hypogonadism & testosterone replacement therapy
 Male hypogonadism & testosterone replacement therapy Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard Adverse events should also be reported
Male hypogonadism & testosterone replacement therapy Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard Adverse events should also be reported
ANDROGEN DEFICIENCY/MALE HYPOGONADISM
 ANDROGEN DEFICIENCY/MALE HYPOGONADISM 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (androgen deficiency)
ANDROGEN DEFICIENCY/MALE HYPOGONADISM 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (androgen deficiency)
BAD TO THE BONE. Peter Jones, Rheumatologist QE Health, Rotorua. GP CME Conference Rotorua, June 2008
 BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
An Evidence-based Review of Clinical Trial Data
 An Evidence-based Review of Clinical Trial Data Karen K. Miller, MD Massachusetts General Hospital Harvard Medical School Boston, MA 1 Rationale for Investigating Androgen Administration in Women: Data
An Evidence-based Review of Clinical Trial Data Karen K. Miller, MD Massachusetts General Hospital Harvard Medical School Boston, MA 1 Rationale for Investigating Androgen Administration in Women: Data
Testosterone Deficiency Syndrome. Time for Proper Personalised Care
 Prof Geoffrey Hackett Good Hope Hospital Sutton Coldfield Testosterone Deficiency Syndrome Time for Proper Personalised Care BSSM Testosterone Guidelines 2017 www.bssm.org.uk Recommendations Diagnosis
Prof Geoffrey Hackett Good Hope Hospital Sutton Coldfield Testosterone Deficiency Syndrome Time for Proper Personalised Care BSSM Testosterone Guidelines 2017 www.bssm.org.uk Recommendations Diagnosis
Male History, Clinical Examination and Testing
 Male History, Clinical Examination and Testing Dirk Vanderschueren, MD, PhD Case Jan is 29 years old and consults for 1 year primary subfertility partner 28 years old and normal gynaecological investigation
Male History, Clinical Examination and Testing Dirk Vanderschueren, MD, PhD Case Jan is 29 years old and consults for 1 year primary subfertility partner 28 years old and normal gynaecological investigation
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel AXIRON transdermal solution FORTESTA transdermal gel NATESTO nasal gel STRIANT buccal mucoadhesive
TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel AXIRON transdermal solution FORTESTA transdermal gel NATESTO nasal gel STRIANT buccal mucoadhesive
Prior Authorization Criteria Update: Androgens, Topical and Parenteral
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
9/2/2016. Faculty. Learning Objectives. Disclosures. Prevalence of Hypogonadism. Prevalence of HG (cont)
") Faculty Testosterone Replacement Therapies: Mitigating Cardiometabolic Risks Associated with Hypogonadism Pamela Ellsworth, MD Professor of Urology University of Massachusetts Medical School Vice Chair,
Faculty Testosterone Replacement Therapies: Mitigating Cardiometabolic Risks Associated with Hypogonadism Pamela Ellsworth, MD Professor of Urology University of Massachusetts Medical School Vice Chair,
Didactic Series. Hypogonadism and HIV. Daniel Lee, MD UCSD Medical Center, Owen Clinic July 28, 2016
 Didactic Series Hypogonadism and HIV Daniel Lee, MD UCSD Medical Center, Owen Clinic July 28, 2016 This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department
Didactic Series Hypogonadism and HIV Daniel Lee, MD UCSD Medical Center, Owen Clinic July 28, 2016 This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department
Ian Eardley Department of Urology, Leeds Teaching Hospital Trust
 Ian Eardley Department of Urology, Leeds Teaching Hospital Trust Assessment of the man with ED Medical therapy for man with ED What to do when pills fail Sexual stimulus Neural pathways Neurotransmitter
Ian Eardley Department of Urology, Leeds Teaching Hospital Trust Assessment of the man with ED Medical therapy for man with ED What to do when pills fail Sexual stimulus Neural pathways Neurotransmitter
Androgen Pattern and Erectile Function in Newly Diagnosed Type 2 Diabetes
 Med. J. Cairo Univ., Vol. 84, No. 3, December: 341-347, 2016 www.medicaljournalofcairouniversity.net Androgen Pattern and Erectile Function in Newly Diagnosed Type 2 Diabetes AHMED I. EL-SAKKA, M.D.*;
Med. J. Cairo Univ., Vol. 84, No. 3, December: 341-347, 2016 www.medicaljournalofcairouniversity.net Androgen Pattern and Erectile Function in Newly Diagnosed Type 2 Diabetes AHMED I. EL-SAKKA, M.D.*;
Recommendations on the diagnosis, treatment and monitoring of Testosterone deficiency (TD) in adult men
 in adult men") Recommendations on the diagnosis, treatment and monitoring of Testosterone deficiency (TD) in adult men Bruno Lunenfeld, George Mskhalaya, Svetlana Kalinchenko, Yulia Tishova, Michael Zitzmann, Stefan
Recommendations on the diagnosis, treatment and monitoring of Testosterone deficiency (TD) in adult men Bruno Lunenfeld, George Mskhalaya, Svetlana Kalinchenko, Yulia Tishova, Michael Zitzmann, Stefan
Best Practices to Improve Patient Outcomes
 Best Practices Pearls Practical Primary Care Strategies for Diagnosing and Managing Hypogonadism in Men Utilize lab testing in appropriate patients who have complaints consistent with the often subtle
Best Practices Pearls Practical Primary Care Strategies for Diagnosing and Managing Hypogonadism in Men Utilize lab testing in appropriate patients who have complaints consistent with the often subtle
REPRODUCTIVE ENDOCRINOLOGY OF THE MALE
 Reproductive Biotechnologies Andrology I REPRODUCTIVE ENDOCRINOLOGY OF THE MALE Prof. Alberto Contri REPRODUCTIVE ENDOCRINOLOGY OF THE MALE SPERMATOGENESIS AND REPRODUCTIVE BEHAVIOR RELATED TO THE ACTIVITY
Reproductive Biotechnologies Andrology I REPRODUCTIVE ENDOCRINOLOGY OF THE MALE Prof. Alberto Contri REPRODUCTIVE ENDOCRINOLOGY OF THE MALE SPERMATOGENESIS AND REPRODUCTIVE BEHAVIOR RELATED TO THE ACTIVITY
Supplementary Online Content
 Supplementary Online Content Basaria S, Harman SM, Travison TG, et al. The effects of testosterone administration for three years on subclinical atherosclerosis progression in older men with low or low
Supplementary Online Content Basaria S, Harman SM, Travison TG, et al. The effects of testosterone administration for three years on subclinical atherosclerosis progression in older men with low or low
ANDROGEN DEFICIENCY/MALE HYPOGONADISM
 Medical Information to Support the Decisions of TUE Committees 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of
Medical Information to Support the Decisions of TUE Committees 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of
Testosterone for the aging male; current evidence and recommended practice
 REVIEW Testosterone for the aging male; current evidence and recommended practice Roger D Stanworth T Hugh Jones Centre of Diabetes and Endocrinology, Barnsley Hospital NHS Foundation Trust, Barnsley,
REVIEW Testosterone for the aging male; current evidence and recommended practice Roger D Stanworth T Hugh Jones Centre of Diabetes and Endocrinology, Barnsley Hospital NHS Foundation Trust, Barnsley,
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients
 Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
Sexual dysfunction of chronic kidney disease. Razieh salehian.md psychiatrist
 Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
MALE HYPOGONADISM: CHOOSING THE APPROPRIATE THERAPY. Michael S. Irwig, M.D. Director, Center for Andrology Division of Endocrinology & Metabolism
 MALE HYPOGONADISM: CHOOSING THE APPROPRIATE THERAPY Michael S. Irwig, M.D. Director, Center for Andrology Division of Endocrinology & Metabolism Disclosures Aromatase inhibitors & clomiphene citrate are
MALE HYPOGONADISM: CHOOSING THE APPROPRIATE THERAPY Michael S. Irwig, M.D. Director, Center for Andrology Division of Endocrinology & Metabolism Disclosures Aromatase inhibitors & clomiphene citrate are
Testosterone: Current Opinion and Controversy
 Testosterone: Current Opinion and Controversy Ravi Kacker, MD Metrowest Urology (508) 655 4422 Medical Office Building at Leonard Morse Hospital Disclosures MHB Labs President and CEO of Drug Development
Testosterone: Current Opinion and Controversy Ravi Kacker, MD Metrowest Urology (508) 655 4422 Medical Office Building at Leonard Morse Hospital Disclosures MHB Labs President and CEO of Drug Development
Options for Treatment of Hypogonadism in Men Desiring Fertility Preservation
 Options for Treatment of Hypogonadism in Men Desiring Fertility Preservation Natan Bar-Chama MD Director Male Reproductive Medicine and Surgery The Mount Sinai School of Medicine New York NY American Association
Options for Treatment of Hypogonadism in Men Desiring Fertility Preservation Natan Bar-Chama MD Director Male Reproductive Medicine and Surgery The Mount Sinai School of Medicine New York NY American Association
Androderm patch, AndroGel packets and pump, Axiron solution, First- Testosterone, First-Testosterone MC, Fortesta gel, Testim gel, Vogelxo
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.31 Subject: Testosterone Topical Page: 1 of 9 Last Review Date: September 23, 2016 Testosterone topical
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.31 Subject: Testosterone Topical Page: 1 of 9 Last Review Date: September 23, 2016 Testosterone topical
SMSNA Hypogonadism Colloquium: Update
 SMSNA Hypogonadism Colloquium: Update Arthur L. (Bud) Burnett, M.D., M.B.A., F.A.C.S. Patrick C. Walsh Distinguished Professor of Urology The James Buchanan Brady Urological Institute Johns Hopkins Medicine
SMSNA Hypogonadism Colloquium: Update Arthur L. (Bud) Burnett, M.D., M.B.A., F.A.C.S. Patrick C. Walsh Distinguished Professor of Urology The James Buchanan Brady Urological Institute Johns Hopkins Medicine
ANDROGEN DEFICIENCY Update on Evaluation and Management
 ANDROGEN DEFICIENCY Update on Evaluation and Management Kristen Gill Hairston, MD, MPH Associate Professor of Internal Medicine Section of Endocrinology and Metabolism Wake Forest University School of
ANDROGEN DEFICIENCY Update on Evaluation and Management Kristen Gill Hairston, MD, MPH Associate Professor of Internal Medicine Section of Endocrinology and Metabolism Wake Forest University School of
Testosterone levels in men with erectile dysfunction
 Original Article TESTOSTERONE LEVELS IN MEN WITH ED MARTÍNEZ-JABALOYAS et al. Testosterone levels in men with erectile dysfunction JOSÉ M. MARTÍNEZ-JABALOYAS, ALFONSO QUEIPO-ZARAGOZÁ*, FRANCISCO PASTOR-HERNÁNDEZ,
Original Article TESTOSTERONE LEVELS IN MEN WITH ED MARTÍNEZ-JABALOYAS et al. Testosterone levels in men with erectile dysfunction JOSÉ M. MARTÍNEZ-JABALOYAS, ALFONSO QUEIPO-ZARAGOZÁ*, FRANCISCO PASTOR-HERNÁNDEZ,
TESTOSTERONE DEFINITION
 DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
Sponsored by. Schering. Sidney Glina
 Sponsored by Schering Sidney Glina Testosterone and erectile dysfunction Sidney Glina Keywords Androgen Hormone replacement therapy Hypogonadism Impotence Testosterone Abstract The role of testosterone
Sponsored by Schering Sidney Glina Testosterone and erectile dysfunction Sidney Glina Keywords Androgen Hormone replacement therapy Hypogonadism Impotence Testosterone Abstract The role of testosterone
Testosterone Therapy in Men With Hypogonadism: An Endocrine Society* Clinical Practice Guideline
 CLINICAL PRACTICE GUIDELINE Testosterone Therapy in Men With Hypogonadism: An Endocrine Society* Clinical Practice Guideline Shalender Bhasin, 1 Juan P. Brito, 2 Glenn R. Cunningham, 3 Frances J. Hayes,
CLINICAL PRACTICE GUIDELINE Testosterone Therapy in Men With Hypogonadism: An Endocrine Society* Clinical Practice Guideline Shalender Bhasin, 1 Juan P. Brito, 2 Glenn R. Cunningham, 3 Frances J. Hayes,
Implantable Hormone Pellets
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Testosterone therapy in the new era of Food and Drug Administration oversight
 Review Article Testosterone therapy in the new era of Food and Drug Administration oversight Bethany Desroches 1, Taylor P. Kohn 2, Charles Welliver 3, Alexander W. Pastuszak 1,4 1 Scott Department of
Review Article Testosterone therapy in the new era of Food and Drug Administration oversight Bethany Desroches 1, Taylor P. Kohn 2, Charles Welliver 3, Alexander W. Pastuszak 1,4 1 Scott Department of
Primary Hypogonadism In Ghanaian Men With Type 2 Diabetes Mellitus
 Primary Hypogonadism In Ghanaian Men With Type 2 Diabetes Mellitus H. Asare-Anane, E.K. Ofori, F.A.Yeboah, E.A. Tagoe, S.B. Bani, A.T. Bawah, R.O Ateko Abstract-Emerging evidence links insulin resistance,
Primary Hypogonadism In Ghanaian Men With Type 2 Diabetes Mellitus H. Asare-Anane, E.K. Ofori, F.A.Yeboah, E.A. Tagoe, S.B. Bani, A.T. Bawah, R.O Ateko Abstract-Emerging evidence links insulin resistance,
Implantable Hormone Pellets
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Developing clinical stage small molecule therapeutics to treat hormonal and reproductive system disorders
 Developing clinical stage small molecule therapeutics to treat hormonal and reproductive system disorders Repros Disclaimer Any statements made by the Company that are not historical facts contained in
Developing clinical stage small molecule therapeutics to treat hormonal and reproductive system disorders Repros Disclaimer Any statements made by the Company that are not historical facts contained in
Testim 1 Gel: Review of Clinical Data
 European Urology Supplements European Urology Supplements 4 (2005) 24 30 Testim 1 Gel: Review of Clinical Data Tom A. McNicholas* Department of Urology, Lister Hospital, Corey s Mill Lane, Stevenage, Hertfordshire
European Urology Supplements European Urology Supplements 4 (2005) 24 30 Testim 1 Gel: Review of Clinical Data Tom A. McNicholas* Department of Urology, Lister Hospital, Corey s Mill Lane, Stevenage, Hertfordshire
Sexual Dysfunction. Jae Il Kang, Byeong Kuk Ham, Mi Mi Oh, Je Jong Kim, Du Geon Moon. DOI: /kju
 www.kjurology.org DOI:10.4111/kju.2011.52.6.416 Sexual Dysfunction Correlation between Serum Total Testosterone and the AMS and IIEF Questionnaires in Patients with Erectile Dysfunction with Testosterone
www.kjurology.org DOI:10.4111/kju.2011.52.6.416 Sexual Dysfunction Correlation between Serum Total Testosterone and the AMS and IIEF Questionnaires in Patients with Erectile Dysfunction with Testosterone
An Update on Men s Health and Sexual Function
 An Update on Men s Health and Sexual Function Lawrence Jenkins, MD, MBA Assistant Professor Clinical Department of Urology The Ohio State University Wexner Medical Center Outline Testosterone Deficiency
An Update on Men s Health and Sexual Function Lawrence Jenkins, MD, MBA Assistant Professor Clinical Department of Urology The Ohio State University Wexner Medical Center Outline Testosterone Deficiency
Long-Term Testosterone Therapy in Type 2 Diabetes Is Associated with Decreasing Waist Circumference and Improving Erectile Function
 Original Article pissn: 2287-4208 / eissn: 2287-4690 World J Mens Health Published online Sep 12, 2018 https://doi.org/10.5534/wjmh.180052m Long-Term Testosterone Therapy in Type 2 Diabetes Is Associated
Original Article pissn: 2287-4208 / eissn: 2287-4690 World J Mens Health Published online Sep 12, 2018 https://doi.org/10.5534/wjmh.180052m Long-Term Testosterone Therapy in Type 2 Diabetes Is Associated
Chapter 29: Male sexual dysfunction in type 2 diabetes
 South African Family Practice 08; 60():6-0 Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND.0] http://creativecommons.org/licenses/by-nc-nd/.0 S Afr Fam Pract
South African Family Practice 08; 60():6-0 Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND.0] http://creativecommons.org/licenses/by-nc-nd/.0 S Afr Fam Pract
The Sexual Medicine Society of North. Adult-Onset Hypogonadism SPECIAL ARTICLE
 SPECIAL ARTICLE Adult-Onset Hypogonadism Mohit Khera, MD, MBA, MPH; Gregory A. Broderick, MD; Culley C. Carson III, MD; Adrian S. Dobs, MD, MHS; Martha M. Faraday, PhD; Irwin Goldstein, MD; Lawrence S.
SPECIAL ARTICLE Adult-Onset Hypogonadism Mohit Khera, MD, MBA, MPH; Gregory A. Broderick, MD; Culley C. Carson III, MD; Adrian S. Dobs, MD, MHS; Martha M. Faraday, PhD; Irwin Goldstein, MD; Lawrence S.
66 M with erectile dysfunction and abnormal labs RAJESH JAIN ENDORAMA 10/29/2015
 66 M with erectile dysfunction and abnormal labs RAJESH JAIN ENDORAMA 10/29/2015 HPI 66 M presenting as a referral for erectile dysfunction and abnormal labs Has been seeing a facility specializing in
66 M with erectile dysfunction and abnormal labs RAJESH JAIN ENDORAMA 10/29/2015 HPI 66 M presenting as a referral for erectile dysfunction and abnormal labs Has been seeing a facility specializing in