Review Article Kidney Diseases Caused by Complement Dysregulation: Acquired, Inherited, and Still More to Come
|
|
|
- Cecil Warren
- 5 years ago
- Views:
Transcription
1 Clinical and Developmental Immunology Volume 2012, Article ID , 6 pages doi: /2012/ Review Article Kidney Diseases Caused by Complement Dysregulation: Acquired, Inherited, and Still More to Come Saskia F. Heeringa 1 and Clemens D. Cohen 2 1 Division of Internal Medicine, University Hospital Zurich, Raemistrasse 100, 8006 Zurich, Switzerland 2 Division of Nephrology, University Hospital Zurich, Raemistrasse 100, 8006 Zurich, Switzerland Correspondence should be addressed to Saskia F. Heeringa, saskia.heeringa@usz.ch Received 6 August 2012; Accepted 11 October 2012 Academic Editor: Michael A. Flierl Copyright 2012 S. F. Heeringa and C. D. Cohen. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Inherited and acquired dysregulation of the complement alternative pathway plays an important role in multiple renal diseases. In recent years, the identification of disease-causing mutations and genetic variants in complement regulatory proteins has contributed significantly to our knowledge of the pathogenesis of complement associated glomerulopathies. In these diseases defective complement control leading to the deposition of activated complement products plays a key role. Consequently, complement-related glomerulopathies characterized by glomerular complement component 3 (C3) deposition in the absence of local immunoglobulin deposits are now collectively described by the term C3 glomerulopathies. Therapeutic strategies for reestablishing complement regulation by either complement blockade with the anti-c5 monoclonal antibody eculizumab or plasma substitution have been successful in several cases of C3 glomerulopathies. However, further elucidation of the underlying defects in the alternative complement pathway is awaited to develop pathogenesis-specific therapies. 1. Introduction The central function of the kidney for whole body homeostasis is based on adequate blood flow and pressure, sufficient glomerular capillary surface for selective filtration, and subsequent secretion and reabsorption of solutes in the tubular system. The essential role of the glomerulus as a filtration unit can be estimated by the fact that most diseases leading to chronic kidney disease and end-stage renal disease with the need for dialysis or transplantation are caused by glomerulopathies. The glomerulus as a specialized capillary convolute is prone to any vascular damage and is affected as part of a generalized microangiopathy in common diseases such as diabetes mellitus or arterial hypertension. However, the glomerulus can also be affected by specific circulating factors, including antibodies against glomerular antigens, circulating immune complexes, or activated factors of a dysregulated complement system. The complement system as an essential component of the innate immune system plays an indispensable role in the elimination of invading microorganisms as a first line of defense [1, 2]. Furthermore, the complement system bridges innate and adaptive immunity. The cross-talk between toll-like receptors as another key component of the innate immune system and the complement system has been a key aspect of research as of their synergistic interaction to increase activation of inflammatory responses [3]. Complement activation runs through three major pathways (classic, alternative, and mannose-binding lectin) that all generate the enzyme complex C3-convertase which cleaves C3 into C3a and C3b. Herein, four main activation steps are distinguished: initiation of activation, activation and amplification of C3-convertase, activation of C5-convertase, and activation of the terminal pathway activity which is characterized by the assembly of the membrane attack complex (MAC) [4]. Importantly, the alternative pathway is constantly activated at low levels. Cascade progression and activation, however, is strictly controlled by complement regulating proteins such as complement factor H (CFH) and complement factor I (CFI): the two most important inhibitory proteins of the alternative pathway.
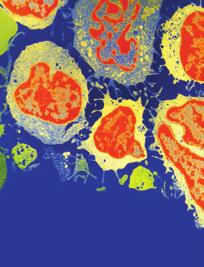
2 2 Clinical and Developmental Immunology Alternative complement pathway C3 C3a C3b Factor B Factor D C3bBbP = C3-convertase C5-convertase Fluid phase regulators: Factor I, Factor H, CFHR3 Membrane bound regulators: MCP, CRI Mutations/genetic variants in + Autoantibodies against: Complement regulating proteins + C3-convertase AP-dysregulation abnormal C3-convertase activity C5 Disease C5a C5b MAC Dense deposit disease C3 glomerulonephritis CFHR5 nephropathy Familial C3 glomerulopathy FSGS Figure 1: Dysregulation of the alternative complement cascade due to acquired or genetic factors leads to defective complement control causing a range of complement-associated glomerulopathies. C3 is cleaved to generate C3a and C3b. After binding of C3b to factor B, the complex is cleaved by factor D to form C3-convertase. The initial convertase constantly cleaves C3 at a low rate (referred to as tick-over of the alternative pathway). Binding of another C3b-fragment to C3-convertase creates a C5-convertase after which the pathway proceeds in the same manner as the classical pathway recruiting additional complement factors to ultimately form the membrane attack complex (MAC). The alternative pathway is strictly regulated by complement regulating proteins (listed in red). Mutations, genetic variations, or antibodies against complement regulating proteins or C3-convertase lead to abnormal C3-convertase activity. The subsequent deposition of activated complement products causes a range of complement-associated glomerulopathies. Abbreviations: C3; complement component 3, CFHR3; complement factor H related protein, AP; alternative pathway. Complement dysregulation has been early recognized to be a central event in many nephropathies, and peripheral markers for complement activation (especially serum levels of C3 and C4) are tested routinely for different acquired renal diseases, for example, postinfectious glomerulopathy and proliferative lupus nephritis, glomerular capillaritis due to cryoglobulinemia or cholesterol embolism. Moreover, an increasing number of inherited renal diseases and renal diseases due to acquired factors with genetic predisposition for complement dysregulation are discovered such as atypical hemolytic uremic syndrome (ahus) and membranoproliferative glomerulonephritis (MPGN) forms including dense deposit (DDD), C3 glomerulonephritis (C3GN) and CFHR5 nephropathy (Figure 1) [5, 6]. Mutations in CFH leading to CFH dysfunction and subsequently ahus are the best known disease-causing mutations, but mutations in several other genes coding for complement factors and regulatory proteins have been identified in complementrelated glomerulopathies (e.g., C3, CFI, CFHR1-5, MCP (membrane cofactor protein)). Genome-wide linkage analysis recently added novel polymorphisms and diseasecausing mutations in complement genes to the list of hereditary complement-related nephropathies [7, 8]. In the following minireview we give an overview of complementrelated glomerulopathies. Atypical HUS, a syndrome with prominent nonrenal, that is hematological and neurological manifestations, will not be discussed. 2. C3 Glomerulopathy Patients with MPGN due to complement dysregulation manifest with proteinuria, (micro)hematuria and a variable degree of renal insufficiency. Kidney biopsy results show an altered glomerular basement membrane with double
3 Clinical and Developmental Immunology 3 Table 1: C3 glomerulopathies. Diseases EM-findings Alternative pathway abnormalities Disease specific treatment options Dense deposit disease C3 glomerulonephritis CFHR5 nephropathy Familial C3 glomerulopathy (i) Osmophilic wavy dense deposits within GBM, mesangial matrix, tubular BM (i) Mesangial, subendothelial, subepithelial and intramembranous deposits (i) Mesangial, subendothelial, subepithelial deposits (i) MPGN type III (ii) Subendothelial, subepithelial deposits (i) Autoantibodies (C3Nef, FHAA, FBAA, C3-convertase AA) (ii) Mutations/genetic variations (CFH, CFI, CFB, MCP) (i) Mutations/genetic variations (CFH, CFI, MCP) (ii) Autoantibodies (C3Nef, FHAA) (i) CFHR5-mutation (i) Familial hybrid CFHR3-1 gene autosomal dominant inheritance (i) Infusion of fresh frozen plasma (ii) Plasmapheresis (iii) Eculizumab (iv) Immunosuppressive treatment (in case of autoantibodies) (i) Eculizumab (ii) Immunosuppressive treatment (in case of autoantibodies) (i) No treatment of proven efficacy (ii) Plasma exchange associated with good outcome (i) No treatment of proven efficacy Abbreviations: C3: complement component 3, CFHR5: complement factor H related protein 5, CFH: complement factor H, CFI: complement factor I, MCP: membrane cofactor protein, FHAA: factor H autoantibody, FBAA: factor B autoantibody, (G) BM; (glomerular) basement membrane, MCP: membrane cofactor protein. contours mostly due to subendothelial deposits, besides a variety of additional alterations such as hypercellularity and additional deposits [6]. As MPGN can be immunecomplex-mediated, specific immunofluorescence has to be employed when evaluating the renal biopsy to differentiate between immunglobulin-mediated MPGN and complement-mediated MPGN. Based on the localization of deposits in electron microscopy, MPGN has been classified into three different types: type I (subendothelial deposits), type II (intramembranous deposits), and type III (subendothelial and subepithelial deposits) [9]. Type I and III typically are immunglobulin-mediated diseases caused by the deposition of immune complexes as a result of for example circulating immune complexes, monoclonal gammopathies or chronic infections. MPGN II which is also called dense deposit disease, is characterized by complement component 3 (C3) containing dense deposits in the glomerular basement membrane that are a result of a dysregulation of the complement alternative pathway. As the inflammation is caused directly by the deposition of complement products, immunoglobulins are not involved and therefore not observed in immunofluorescence studies [6]. The subgrouping of MPGN has led to some confusion as all types of MPGN stain positive for C3 but immunglobulin staining can be negative even in some cases of MPGN I and III. Sethi et al. therefore proposed a classification driven by the findings on immunofluorescence, classifying MPGN as either immunoglobulin positive or negative [10]. Hence, immunoglobulin-negative but C3-positive MPGN is newly referred to as C3 glomerulopathy. Examples of C3 glomerulopathies are C3GN and DDD that can be distinguished by electron microscopical findings (see Table 1). C3GN appears to be a key example of a dysregulated alternative and terminal complement pathway in which the deposition of complement is triggered despite the absence of antibody deposition [5, 10, 11]. Besides the identification of several disease-causing mutations in alternative pathway inhibitors, some autoantibodies leading to the activation or blockage of alternative pathway proteins have also been identified as a cause of C3GN. In a recent study by Servais et al., patients with C3GN (and additional patients with other forms of MPGN) were screened for mutations and rare variants in CFH, CFI, and MCP [12]. Although genetic abnormalities found in patients with C3GN were similar to the ones reported in individuals affected by ahus, the genetic background predisposes specifically for the respective clinical and histological phenotype [12]. A rare, recently described variant of C3GN is CFHR5 nephropathy, a monogenic disease caused by mutations in the gene encoding complement factor-related protein 5 (CFHR5) [7]. CFHR5 is structurally related to CFH and possibly acts as a cofactor inhibiting C3-convertase [13]. In a cohort of patients with familial CFHR5 nephropathy sharing the same founder mutation, it was shown that the phenotype-spectrum among family members is broad [14]. As of this phenotypic heterogeneity, it is assumed that other factors like predisposing modifier genes and environmental factors as complementactivating infections also play a role in the development and phenotype of disease. CFHR5 is a member of the CFH related protein family, consisting of 5 proteins; CFHR1-5. Little is known about the function of these proteins, but there is increasing evidence that these protein families may either be involved in disease development or protection from complement dysregulation, respectively. CFHR1 inhibits C5-convertase activity and the formation of the terminal complex. CFHR3 also has complement regulatory activity as it inhibits C3-convertase [15]. Interestingly, a complete absence of both genes (ΔCFHR3-1) is not uncommon in the normal population. The deletion of CFHR3-1 has even been associated with protection from both complement- and age-related macular degeneration as well as IgA nephropathy,
4 4 Clinical and Developmental Immunology the most common mesangioproliferative glomerulonephritis with prominent mesangial IgA and secondary local complement activation [16]. In a recent study, a hybrid CFHR3-1 gene was shown to cause familial C3 glomerulopathy [17]. The authors suggested a possible dominant mechanism of this genetic alteration leading to an increased expression of both proteins, interfering with complement processing and leading to accumulation of C3 [17]. Dense deposit disease (DDD) is closely related to C3GN andrecentdatasuggestthatbothmayrepresentextremes in a continuous spectrum of complement-related MPGNs [6, 12]. Both diseases show similar features in light and immunofluorescence microscopy and they are distinguished by electron microscopy. Here, C3GN is characterized by mesangial, subendothelial, and intramembranous deposits, whereas DDD is characterized by osmophilic dense deposits along the glomerular and tubular basement membranes [18, 19]. By an advanced mass spectrometry approach on glomerular isolates, Sethi et al. detected activated components of the alternative pathway and of the terminal complement pathway in patients with DDD [20]. Because of a very high recurrence rate after kidney transplantation, a systemic cause of DDD has been early suggested. Hence, the identification of the first C3 nephritic factor (C3Nef) as an autoantibody that stabilizes C3-convertase, was a major achievement [21]. The presence of C3Nefs is the most common association with alternative pathway dysregulation in DDD [22]. Binding of C3Nef to the alternative C3- convertase increases its half-life leading to uncontrolled alternative pathway activation and a massive consumption of C3. However, C3Nef activity is not always associated with low C3 levels in plasma and C3Nef is not specific for DDD as it can be found in other diseases as well as in healthy individuals [23]. Less common causes for DDD are inhibitory CFH autoantibodies, CFH deficiency, or functional CFH-defects, the latter both due to genetic mutations leading to reduced CFH activity. Mutations that lead to a complete CFH deficiency are rare though, and most functional CFH defects go along with normal CFH levels in plasma [24, 25]. Interestingly, not all patients with a functional CFH defect develop DDD, as CFH deficiency can also lead to ahus and not all individuals with similar genetic variants develop the same phenotype [8]. In order to analyze the causes of alternative pathway dysregulation, several groups studied DDD cohorts employing functional and genetic tests [12, 22]. In these studies, a probable cause for complement dysregulation could be identified in about 80% of DDD patients [12, 22]. Detection of C3Nef was the most frequent single finding, but in some patients also autoantibodies against CFH or CFB were detected [22]. Gene variants in CFH were detected in 10 17% of DDD patients [12, 22]. Notably, a functional CFH defect frequently coexisted with the presence of C3Nef. Similarly, in C3GN the detection of C3Nef was the most common complement abnormality found in 45% patients with C3GN that were screened by Servais et al. [12]. Besides C3Nef, additional autoantibodies against CFH, CFB and to the individual components of C3-convertase (C3b and factor B) have been described in C3 glomerulopathies [12, 18, 26 28]. Anti-factor B autoantibody for example was found in a patient with DDD that was able to bind and thereby stabilize C3-convertase leading to an increased consumption of C3 [28]. This again indicates that DDD and C3GN have many pathogenetic and histological aspects in common and may represent extremes of a continuum. 3. Treatment In order to decrease proteinuria and improve blood pressure control, nonspecific treatment with angiotensin converting enzyme (ACE) inhibitors or angiotensin type II receptor blockers is recommended in all patients. With improved understanding of the pathogenesis of C3 glomerulopathies more specific therapies could be applied. In patients with C3Nef or autoantibodies to CFH or CFB immunosuppressive therapies including rituximab or plasma exchange have been reported to slow disease progression or to help to avoid recurrence after transplantation [19, 26]. With the increasing knowledge about the underlying mechanisms and the specific complement defects in C3 glomerulopathies, specific complement-targeting therapies have been successfully applied in several cases of DDD and C3GN. As can be expected, large-scale clinical studies are missing in these rare diseases. Especially eculizumab, a humanized anti-c5 monoclonal antibody, represents a promising agent as it blocks C5b-9 formation, the terminal event in the complement cascade. The antibody has been approved by both the U.S. Food and Drug Administration as well as the European Commission for the treatment of paroxysmal nocturnal hemoglobinuria and, more recently, atypical HUS. Eculizumab was even suggested to be an effective agent in children with enterohemorrhagic Escherichia coli (EHEC) infection-causedhus [29]. However, this was not evident in a case-control study reporting a mainly middle-aged population of a recent outbreak of EHEC induced HUS in northern Germany [30]. But for DDD and MPGN with CFHR1 deficiency, recent anecdotic reports suggest a treatment effect of eculizumab with stabilization of kidney function, decrease in proteinuria [31, 32], and even improvement in histopathological findings [33]. In a recent study reporting of three subjects with DDD and three subjects with C3GN who were treated with eculizumab for one year, response to treatment was seen in some but not all patients. Elevated serum membrane attack complex normalized on therapy, serum creatinine improved and proteinuria was reduced [34]. A very recent pathology report on C3GN patients treated with eculizumab showed de-novo monoclonal staining for IgG-kappa in the same distribution as C3 and C5b- 9 in all posttreatment protocol biopsies, indicating binding to C5 and glomerular deposition of eculizumab [35]. As the authors state, the long-term clinical significance of these therapy-induced immune deposits together with apparent drug-tissue interactions is not known. Beside eculizumab as target-specific but costly treatment option fresh frozen plasma (FFP) infusions were given to several cases with functional CFH deficits and resulted in the prevention
5 Clinical and Developmental Immunology 5 of further disease progression [36, 37]. In a recent case report of two unrelated patients with MPGN and MPGN II with combined autoantibodies for factor B and C3, one patient received immunosuppressive treatment leading to a significant decrease of both autoantibodies [26]. In order to guide such disease specific treatment, it may become important to evaluate the alternative complement pathway more comprehensively in patients that have a renal biopsy consistent with C3 glomerulopathy. Complement proteins (CFH, CFI, CFB), complement degradation products (C3c, C3d), soluble serum membrane attack complex (smac), and disease associated autoantibodies (C3 nephritic factor, anti-factor H, anti-factor B, anti-c3b [26]) might expand the diagnostic arsenal of complement specific markers in the future. 4. Conclusions In sum, the spectrum of renal disease phenotypes due to complement dysregulation is diverse. And it is still increasing: in a recent case report, Sethi et al. reported of single nucleotide polymorphisms in genes encoding CFH and C3 to be linked to the development of focal segmental glomerulosclerosis (FSGS), potentially extending the involvement of complement dysregulation to podocytopathies [38, 39]. Interestingly, this finding is in line with data from the European Renal cdna Bank indicating alteration of intraglomerular transcript levels of complement-related gene products in FSGS (own unpublished observation). As outlined above, several independent approaches such as Mendelian genetics, genome-wide association studies, transcriptomic and proteomic approaches as well as histopathology and functional studies underline the relevance of complement dysregulation in several kidney diseases, which currently undergo a redefinition. With the increasing insight into the pathophysiology, more specific complement targeting therapies may become available for the treatment of both ultrarare and more frequent complement-associated renal diseases. Acknowledgments C. D. Cohen was supported by the Else Kröner-Fresenius Foundation and the Swiss National Science Foundation in frame of the National Center of Competence in Research: Kidney Control of Homeostasis (NCCR Kidney.CH). References [1] M. J. Walport, Advances in immunology: complement (first of two parts), The New England Medicine, vol. 344, no. 14, pp , [2] M. J. Walport, Advances in immunology: complement (second of two parts), The New England Medicine, vol. 344, no. 15, pp , [3] B. Holst, A.-C. Raby, J. E. Hall, and M. O. Labéta, Complement takes its Toll: an inflammatory crosstalk between Toll-like receptors and the receptors for the complement anaphylatoxin C5a, Anaesthesia, vol. 67, no. 1, pp , [4] P. F. Zipfel and C. Skerka, Complement regulators and inhibitory proteins, Nature Reviews Immunology, vol. 9, no. 10, pp , [5] F. Fakhouri, V. Frémeaux-Bacchi, L. H. Noël,H.T.Cook,and M. C. Pickering, C3 glomerulopathy: a new classification, Nature Reviews Nephrology, vol. 6, no. 8, pp , [6] S. Sethi and F. C. Fervenza, Membranoproliferative glomerulonephritis a new look at an old entity, The New England Medicine, vol. 366, no. 12, pp , [7] D. P. Gale, E. G. de Jorge, H. T. Cook et al., Identification of a mutation in complement factor H-related protein 5 in patients of Cypriot origin with glomerulonephritis, The Lancet, vol. 376, no. 9743, pp , [8]J.Caprioli,P.Bettinaglio,P.F.Zipfeletal., Themolecular basis of familial hemolytic uremic syndrome: mutation analysis of factor H gene reveals a hot spot in short consensus repeat 20, the American Society of Nephrology, vol. 12, no. 2, pp , [9]E.C.Jackson,A.J.McAdams,C.F.Strife,J.Forristal,T. R. Welch, and C. D. West, Differences between membranoproliferative glomerulonephritis types I and III in clinical presentation, glomerular morphology, and complement perturbation, American Kidney Diseases, vol. 9, no. 2, pp , [10] S. Sethi, C. M. Nester, and R. J. H. Smith, Membranoproliferative glomerulonephritis and C3 glomerulopathy: resolving the confusion, Kidney International, vol. 81, no. 5, pp , [11] S. Sethi, F. C. Fervenza, Y. Zhang et al., Proliferative glomerulonephritis secondary to dysfunction of the alternative pathway of complement, Clinical the American Society of Nephrology, vol. 6, no. 5, pp , [12] A. Servais, L.-H. Noël, L. T. Roumenina et al., Acquired and genetic complement abnormalities play a critical role in dense deposit disease and other C3 glomerulopathies, Kidney International, vol. 82, no. 4, pp , [13] J. L. McRae, T. G. Duthy, K. M. Griggs et al., Human factor H- related protein 5 has cofactor activity, inhibits C3 convertase activity, binds heparin and C-reactive protein, and associates with lipoprotein, Immunology, vol. 174, no. 10, pp , [14] Y. Athanasiou, K. Voskarides, D. P. Gale et al., Familial C3 glomerulopathy associated with CFHR5 mutations: clinical characteristics of 91 patients in 16 pedigrees, Clinical Journal of the American Society of Nephrology, vol. 6, no. 6, pp , [15] L. G. Fritsche, N. Lauer, A. Hartmann et al., An imbalance of human complement regulatory proteins CFHR1, CFHR3 and factor H influences risk for age-related macular degeneration (AMD), Human Molecular Genetics, vol. 19, no. 23, pp , [16] A. G. Gharavi, K. Kiryluk, M. Choi et al., Genomewide association study identifies susceptibility loci for IgA nephropathy, Nature Genetics, vol. 43, no. 4, pp , [17] T. H. Malik, P. J. Lavin, E. G. De Jorge et al., A hybrid CFHR3-1 gene causes familial C3 glomerulopathy, the American Society of Nephrology, vol. 23, no. 7, pp , [18] S. Sethi, F. C. Fervenza, Y. Zhang et al., C3 glomerulonephritis: clinicopathological findings, complement abnormalities,
6 6 Clinical and Developmental Immunology glomerular proteomic profile, treatment, and follow-up, Kidney International, vol. 82, no. 4, pp , [19] R. J. H. Smith, C. L. Harris, and M. C. Pickering, Dense deposit disease, Molecular Immunology, vol. 48, no. 14, pp , [20] S. Sethi, J. D. Gamez, J. A. Vrana et al., Glomeruli of dense deposit disease contain components of the alternative and terminal complement pathway, Kidney International, vol. 75, no. 9, pp , [21] R. E. Spitzer, E. H. Vallota, J. Forristal et al., Serum C 3 lytic system in patients with glomerulonephritis, Science, vol. 164, no. 3878, pp , [22] Y. Zhang, N. C. Meyer, K. Wang et al., Causes of alternative pathway dysregulation in dense deposit disease, Clinical the American Society of Nephrology,vol.7,no.2,pp , [23] A. T. Gewurz, S. M. Imherr, S. Strauss, H. Gewurz, and C. Mold, C3 nephritic factor and hypocomplementaemia in a clinically healthy individual, Clinical and Experimental Immunology, vol. 54, no. 1, pp , [24] T. H. J. Goodship, I. Y. Pappworth, T. Toth et al., Factor H autoantibodies in membranoproliferative glomerulonephritis, Molecular Immunology, vol. 52, no. 3-4, pp , [25] C. Licht, U. Schlötzer-Schrehardt, M. Kirschfink, P. F. Zipfel, and B. Hoppe, MPGN II genetically determined by defective complement regulation? Pediatric Nephrology, vol. 22, no. 1, pp. 2 9, [26] Q. Chen, D. Müller, B. Rudolph et al., Combined C3b and factor B autoantibodies and MPGN type II, The New England Medicine, vol. 365, no. 24, pp , [27] T. S. Jokiranta, A. Solomon, M. K. Pangburn, P. F. Zipfel, and S. Meri, Nephritogenic λ light chain dimer: a unique human miniautoantibody against complement factor H, Immunology, vol. 163, no. 8, pp , [28] S. Strobel, M. Zimmering, K. Papp, J. Prechl, and M. Józsi, Anti-factor B autoantibody in dense deposit disease, Molecular Immunology, vol. 47, no. 7-8, pp , [29] L. Anne-Laure, M. Malina, V. Fremeaux-Bacchi et al., Eculizumab in severe shiga-toxin associated HUS, The New England Medicine, vol. 364, no. 26, pp , [30] J. Menne, M. Nitschke, R. Stingele et al., Validation of treatment strategies for enterohaemorrhagic Escherichia coli O104:H4 induced haemolytic uraemic syndrome: case-control study, British Medical Journal, vol. 345, no. 7869, Article ID e4565, [31] E. Daina, M. Noris, and G. Remuzzi, Eculizumab in a patient with dense-deposit disease, The New England Journal of Medicine, vol. 366, no. 12, pp , [32] S. Radhakrishnan, A. Lunn, M. Kirschfink et al., Eculizumab and refractory membranoproliferative glomerulonephritis, The New England Medicine, vol. 366, no. 12, pp , [33] M. Vivarelli, A. Pasini, and F. Emma, Eculizumab for the treatment of dense-deposit disease, The New England Journal of Medicine, vol. 366, no. 12, pp , [34] A. S. Bomback, R. J. Smith, G. R. Barile et al., Eculizumab for dense deposit disease and C3 glomerulonephritis, Clinical the American Society of Nephrology,vol.7,no.5,pp , [35] L. C. Herlitz, A. S. Bomback, G. S. Markowitz et al., Pathology after eculizumab in dense deposit disease and C3 GN, Journal of the American Society of Nephrology, vol. 23, no. 7, pp , [36] S. Habbig, M. J. Mihatsch, S. Heinen et al., C3 deposition glomerulopathy due to a functional factor H defect, Kidney International, vol. 75, no. 11, pp , [37] C. Licht, A. Weyersberg, S. Heinen et al., Successful plasma therapy for atypical hemolytic uremic syndrome caused by factor H deficiency owing to a novel mutation in the complement cofactor protein domain 15, American Journal of Kidney Diseases, vol. 45, no. 2, pp , [38] S. Sethi, F. C. Fervenza, Y. Zhang, and R. J. H. Smith, Secondary focal and segmental glomerulosclerosis associated with single-nucleotide polymorphisms in the genes encoding complement factor H and C3, American Kidney Diseases, vol. 60, no. 2, pp , [39] R. C. Wiggins, The spectrum of podocytopathies: a unifying view of glomerular diseases, Kidney International, vol. 71, no. 12, pp , 2007.
















7 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
C3 Glomerulopathy. Jun-Ki Park
 C3 Glomerulopathy Jun-Ki Park 03.08.11 For the last 30 years classification MPGN is based on glomerular findings by light microscopy with further specification on EM and staining for Ig and complement
C3 Glomerulopathy Jun-Ki Park 03.08.11 For the last 30 years classification MPGN is based on glomerular findings by light microscopy with further specification on EM and staining for Ig and complement
C3 Glomerulonephritis versus C3 Glomerulopathies?
 Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
From MPGN to C3G. F Fakhouri, Nantes, France. «Membranoproliferative» is a pathological feature. Mesangial expansion «Doubles contours»
 From MPGN to C3G F Fakhouri, Nantes, France Conflits d intérêt: consultant auprès d Alexion Pharmaceuticals «Membranoproliferative» is a pathological feature Mesangial expansion «Doubles contours» Immune
From MPGN to C3G F Fakhouri, Nantes, France Conflits d intérêt: consultant auprès d Alexion Pharmaceuticals «Membranoproliferative» is a pathological feature Mesangial expansion «Doubles contours» Immune
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Complement in vasculitis and glomerulonephritis. Andy Rees Clinical Institute of Pathology Medical University of Vienna
 Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Toward a working definition of C3 glomerulopathy by immunofluorescence
 http://www.kidney-international.org & 2013 International Society of Nephrology Toward a working definition of C3 glomerulopathy by immunofluorescence Jean Hou 1, Glen S. Markowitz 1, Andrew S. Bomback
http://www.kidney-international.org & 2013 International Society of Nephrology Toward a working definition of C3 glomerulopathy by immunofluorescence Jean Hou 1, Glen S. Markowitz 1, Andrew S. Bomback
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA
 C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA C3 Glomerulopathy Overview Discuss C3 Glomerulopathy (C3G) How did we get to the current classification
C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA C3 Glomerulopathy Overview Discuss C3 Glomerulopathy (C3G) How did we get to the current classification
H. Terence Cook. REVIEW C3 glomerulopathy [version 1; referees: 4 approved] Open Peer Review. Referee Status:
![H. Terence Cook. REVIEW C3 glomerulopathy [version 1; referees: 4 approved] Open Peer Review. Referee Status:](/thumbs/94/119185743.jpg "H. Terence Cook. REVIEW C3 glomerulopathy [version 1; referees: 4 approved] Open Peer Review. Referee Status:") REVIEW C3 glomerulopathy [version 1; referees: 4 approved] H. Terence Cook Department of Medicine, Imperial College London, Hammersmith, London, UK v1 First published: 10 Mar 2017, 6(F1000 Faculty Rev):248
REVIEW C3 glomerulopathy [version 1; referees: 4 approved] H. Terence Cook Department of Medicine, Imperial College London, Hammersmith, London, UK v1 First published: 10 Mar 2017, 6(F1000 Faculty Rev):248
Advances in Membranous and Membranoproliferative glomerulonephritis: Insights into Pathogenesis
 Advances in Membranous and Membranoproliferative glomerulonephritis: Insights into Pathogenesis Terry Cook, Imperial College, London Membranous Glomerulonephritis Membranous glomerulonephritis is characterised
Advances in Membranous and Membranoproliferative glomerulonephritis: Insights into Pathogenesis Terry Cook, Imperial College, London Membranous Glomerulonephritis Membranous glomerulonephritis is characterised
Membranoproliferative glomerulonephritis and C3 glomerulopathy: resolving the confusion
 http://www.kidney-international.org & 2012 International Society of Nephrology Membranoproliferative glomerulonephritis and C3 glomerulopathy: resolving the confusion Sanjeev Sethi 1, Carla M. Nester 2,3,4
http://www.kidney-international.org & 2012 International Society of Nephrology Membranoproliferative glomerulonephritis and C3 glomerulopathy: resolving the confusion Sanjeev Sethi 1, Carla M. Nester 2,3,4
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Article. Eculizumab for Dense Deposit Disease and C3 Glomerulonephritis
 CJASN epress. Published on March 8, 2012 as doi: 10.2215/CJN.12901211 Article Eculizumab for Dense Deposit Disease and C3 Glomerulonephritis Andrew S. Bomback,* Richard J. Smith, Gaetano R. Barile, Yuzhou
CJASN epress. Published on March 8, 2012 as doi: 10.2215/CJN.12901211 Article Eculizumab for Dense Deposit Disease and C3 Glomerulonephritis Andrew S. Bomback,* Richard J. Smith, Gaetano R. Barile, Yuzhou
Monoclonal gammopathies consist of. Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis REVIEW
 REVIEW Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis Sanjeev Sethi, MD, PhD, and S. Vincent Rajkumar, MD Abstract Monoclonal gammopathy is characterized by circulating monoclonal immunoglobulin
REVIEW Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis Sanjeev Sethi, MD, PhD, and S. Vincent Rajkumar, MD Abstract Monoclonal gammopathy is characterized by circulating monoclonal immunoglobulin
C3 Glomerulopathy. Rezan Topaloglu, MD Hacettepe University School of Medicine Department of Pediatric Nephrology Ankara, TURKEY
 C3 Glomerulopathy Rezan Topaloglu, MD Hacettepe University School of Medicine Department of Pediatric Nephrology Ankara, TURKEY Journey in history Some diseases have journey Diagnoses may change during
C3 Glomerulopathy Rezan Topaloglu, MD Hacettepe University School of Medicine Department of Pediatric Nephrology Ankara, TURKEY Journey in history Some diseases have journey Diagnoses may change during
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk
 R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Evidence Review: Title. Month/ Year. Evidence Review: Eculizumab in the treatment of recurrence of C3 glomerulopathy post-transplant
 Evidence Review: Title Month/ Year Evidence Review: Eculizumab in the treatment of recurrence of C glomerulopathy post-transplant October 2015 1 Standard Operating Procedure: NHS England Evidence Review:
Evidence Review: Title Month/ Year Evidence Review: Eculizumab in the treatment of recurrence of C glomerulopathy post-transplant October 2015 1 Standard Operating Procedure: NHS England Evidence Review:
C3 glomerulopathy: consensus report
 http://www.kidney-international.org & 2013 International Society of Nephrology OPEN C3 glomerulopathy: consensus report Matthew C. Pickering 1, Vivette D. D Agati 2, Carla M. Nester 3,4, Richard J. Smith
http://www.kidney-international.org & 2013 International Society of Nephrology OPEN C3 glomerulopathy: consensus report Matthew C. Pickering 1, Vivette D. D Agati 2, Carla M. Nester 3,4, Richard J. Smith
C3 Glomerulopathy: Clinicopathologic Features and Predictors of Outcome
 CJASN epress. Published on October 31, 2013 as doi: 10.2215/CJN.04700513 Article C3 Glomerulopathy: Clinicopathologic Features and Predictors of Outcome Nicholas R. Medjeral-Thomas,* Michelle M. O Shaughnessy,
CJASN epress. Published on October 31, 2013 as doi: 10.2215/CJN.04700513 Article C3 Glomerulopathy: Clinicopathologic Features and Predictors of Outcome Nicholas R. Medjeral-Thomas,* Michelle M. O Shaughnessy,
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation
 Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation Marius Miglinas Vilnius university hospital: Nephrology center, Center of Rare Kidney Diseases Vilnius university
Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation Marius Miglinas Vilnius university hospital: Nephrology center, Center of Rare Kidney Diseases Vilnius university
Article. Proliferative Glomerulonephritis Secondary to Dysfunction of the Alternative Pathway of Complement
 Article Proliferative Glomerulonephritis Secondary to Dysfunction of the Alternative Pathway of Complement Sanjeev Sethi,* Fernando C. Fervenza, Yuzhou Zhang, Samih H. Nasr,* Nelson Leung, Julie Vrana,*
Article Proliferative Glomerulonephritis Secondary to Dysfunction of the Alternative Pathway of Complement Sanjeev Sethi,* Fernando C. Fervenza, Yuzhou Zhang, Samih H. Nasr,* Nelson Leung, Julie Vrana,*
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Recurrence of C3G after renal transplantation. Moglie Le Quintrec Service de Néphrologie, Hôpital Foch CRC, UMRS 1138, Equipe complement and diseases
 Recurrence of C3G after renal transplantation Moglie Le Quintrec Service de Néphrologie, Hôpital Foch CRC, UMRS 1138, Equipe complement and diseases New MPGN classification C3G MPGN I DDD C3GN IF C3 deposits
Recurrence of C3G after renal transplantation Moglie Le Quintrec Service de Néphrologie, Hôpital Foch CRC, UMRS 1138, Equipe complement and diseases New MPGN classification C3G MPGN I DDD C3GN IF C3 deposits
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
C3 glomerulopathy in cystic fibrosis: a case report
 Santoro et al. BMC Nephrology (2018) 19:73 https://doi.org/10.1186/s12882-018-0880-y CASE REPORT C3 glomerulopathy in cystic fibrosis: a case report Domenico Santoro 1*, Rossella Siligato 1, Carmela Vadalà
Santoro et al. BMC Nephrology (2018) 19:73 https://doi.org/10.1186/s12882-018-0880-y CASE REPORT C3 glomerulopathy in cystic fibrosis: a case report Domenico Santoro 1*, Rossella Siligato 1, Carmela Vadalà
M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve.
 M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Prophylactic eculizumab prior to kidney transplantation for atypical hemolytic uremic
M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Prophylactic eculizumab prior to kidney transplantation for atypical hemolytic uremic
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Clinical Commissioning Policy: Eculizumab in the treatment of recurrence of C3 glomerulopathy postkidney transplant (all ages)
") Clinical Commissioning Policy: Eculizumab in the treatment of recurrence of C3 glomerulopathy postkidney transplant (all ages) Reference: NHS England: 16054/P NHS England INFORMATION READER BOX Directorate
Clinical Commissioning Policy: Eculizumab in the treatment of recurrence of C3 glomerulopathy postkidney transplant (all ages) Reference: NHS England: 16054/P NHS England INFORMATION READER BOX Directorate
Favorable effect of bortezomib in dense deposit disease associated with monoclonal gammopathy: a case report
 Hirashio et al. BMC Nephrology (2018) 19:108 https://doi.org/10.1186/s12882-018-0905-6 CASE REPORT Open Access Favorable effect of bortezomib in dense deposit disease associated with monoclonal gammopathy:
Hirashio et al. BMC Nephrology (2018) 19:108 https://doi.org/10.1186/s12882-018-0905-6 CASE REPORT Open Access Favorable effect of bortezomib in dense deposit disease associated with monoclonal gammopathy:
A Case of Myeloma Kidney With Glomerular C3 Deposition
 Case Report World J Nephrol Urol. 2018;7(3-4):73-77 A Case of Myeloma Kidney With Glomerular C3 Deposition Asif Khan a, c, Khine Lam b, Suzanne El-Sayegh b, Elie El-Charabaty b Abstract Manuscript submitted
Case Report World J Nephrol Urol. 2018;7(3-4):73-77 A Case of Myeloma Kidney With Glomerular C3 Deposition Asif Khan a, c, Khine Lam b, Suzanne El-Sayegh b, Elie El-Charabaty b Abstract Manuscript submitted
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular. Genetics
 / TTP/HUS/αHUS Pathology & Molecular. Genetics") Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Clinico-pathologic spectrum of C3 glomerulopathy-an Indian experience
 Viswanathan et al. Diagnostic Pathology (2015) 10:6 DOI 10.1186/s13000-015-0233-0 RESEARCH Open Access Clinico-pathologic spectrum of C3 glomerulopathy-an Indian experience Ganesh Kumar Viswanathan 1,
Viswanathan et al. Diagnostic Pathology (2015) 10:6 DOI 10.1186/s13000-015-0233-0 RESEARCH Open Access Clinico-pathologic spectrum of C3 glomerulopathy-an Indian experience Ganesh Kumar Viswanathan 1,
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Clinical Findings, Pathology, and Outcomes of C3GN after Kidney Transplantation
 CLINICAL RESEARCH www.jasn.org Clinical Findings, Pathology, and Outcomes of C3GN after Kidney ation Ladan Zand,* Elizabeth C. Lorenz,* Fernando G. Cosio,* Fernando C. Fervenza,* Samih H. Nasr, Manish
CLINICAL RESEARCH www.jasn.org Clinical Findings, Pathology, and Outcomes of C3GN after Kidney ation Ladan Zand,* Elizabeth C. Lorenz,* Fernando G. Cosio,* Fernando C. Fervenza,* Samih H. Nasr, Manish
Recent advances in pathogenesis & treatment of ahus
 Recent advances in pathogenesis & treatment of ahus Miquel Blasco Pelicano Nephrology and Kidney Transplant Unit Hospital Clínic, Barcelona Atypical Hemolytic Uremic Syndrome (ahus) Ultra-rare disease:
Recent advances in pathogenesis & treatment of ahus Miquel Blasco Pelicano Nephrology and Kidney Transplant Unit Hospital Clínic, Barcelona Atypical Hemolytic Uremic Syndrome (ahus) Ultra-rare disease:
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
HUS-MPGN-TTP. & related disorders
 ES-PCR 4 th International Conference HUS-MPGN-TTP & related disorders Current diagnosis and therapy of hemolytic uremic syndrome (HUS), membranoproliferative glomerulonephritis (MPGN), thrombotic thrombocytopenic
ES-PCR 4 th International Conference HUS-MPGN-TTP & related disorders Current diagnosis and therapy of hemolytic uremic syndrome (HUS), membranoproliferative glomerulonephritis (MPGN), thrombotic thrombocytopenic
Severe active C3 glomerulonephritis triggered by immune complexes and inactivated after eculizumab therapy
 Kersnik Levart et al. Diagnostic Pathology (2016) 11:94 DOI 10.1186/s13000-016-0547-6 CASE REPORT Open Access Severe active C3 glomerulonephritis triggered by immune complexes and inactivated after eculizumab
Kersnik Levart et al. Diagnostic Pathology (2016) 11:94 DOI 10.1186/s13000-016-0547-6 CASE REPORT Open Access Severe active C3 glomerulonephritis triggered by immune complexes and inactivated after eculizumab
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Clinical Commissioning Policy Proposition: A06X03 Eculizumab in the treatment of recurrence of C3 glomerulopathy postkidney
 Clinical Commissioning Policy Proposition: A06X03 Eculizumab in the treatment of recurrence of C3 glomerulopathy postkidney transplant All Ages First published: Month Year Prepared by NHS England Specialised
Clinical Commissioning Policy Proposition: A06X03 Eculizumab in the treatment of recurrence of C3 glomerulopathy postkidney transplant All Ages First published: Month Year Prepared by NHS England Specialised
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
Hemolytic uremic syndrome: Investigations and management
 Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
W J N. World Journal of Nephrology. Complement involvement in kidney diseases: From physiopathology to therapeutical targeting.
 W J N World Journal of Nephrology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5527/wjn.v4.i2.169 World J Nephrol 2015 May 6; 4(2): 169-184
W J N World Journal of Nephrology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5527/wjn.v4.i2.169 World J Nephrol 2015 May 6; 4(2): 169-184
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG)
") Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature
 Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Membranoproliferative Glomerulonephritis
 Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits in 5 renal allografts
 Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Gene Polymorphism of Complement Factor H in a Turkish Patient With Membranoproliferative Glomerulonephritis Type II
 Kidney Diseases Gene Polymorphism of Complement Factor H in a Turkish Patient With Membranoproliferative Glomerulonephritis Type II Betul Sozeri, 1 Sevgi Mir, 1 Afig Berdeli, 2 Nida Dincel, 1 Banu Sarsik
Kidney Diseases Gene Polymorphism of Complement Factor H in a Turkish Patient With Membranoproliferative Glomerulonephritis Type II Betul Sozeri, 1 Sevgi Mir, 1 Afig Berdeli, 2 Nida Dincel, 1 Banu Sarsik
Atypical hemolytic uremic syndrome (ahus)
") Sunday, July 12 10:00-18:30 Registration open I. Atypical hemolytic uremic syndrome (ahus) Chairs: Kronenberg, Speth 13:00 L1 ahus Role of complemet, overview Meri, FI 13:30 L2 ahus Role of lectin pathway
Sunday, July 12 10:00-18:30 Registration open I. Atypical hemolytic uremic syndrome (ahus) Chairs: Kronenberg, Speth 13:00 L1 ahus Role of complemet, overview Meri, FI 13:30 L2 ahus Role of lectin pathway
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
Pathogenesis of IgA Nephropathy. Shokoufeh Savaj MD Associate Professor of Medicine Firoozgar hospital- IUMS
 Pathogenesis of IgA Nephropathy Shokoufeh Savaj MD Associate Professor of Medicine Firoozgar hospital- IUMS History Immunoglobin A nephropathy was first described by Berger and Hinglais in 1968 in Paris
Pathogenesis of IgA Nephropathy Shokoufeh Savaj MD Associate Professor of Medicine Firoozgar hospital- IUMS History Immunoglobin A nephropathy was first described by Berger and Hinglais in 1968 in Paris
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
New insights in thrombotic microangiopathies : TTP and ahus
 New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Hemolytic uremic syndrome
 Hemolytic uremic syndrome Doyeun Oh Department of Internal Medicine CHA University School of Medicine Disclosures for Doyeun Oh Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau
Hemolytic uremic syndrome Doyeun Oh Department of Internal Medicine CHA University School of Medicine Disclosures for Doyeun Oh Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau
Accepted Manuscript. No more thrombotic thrombocytopenic purpura/hemolytic uremic syndrome please. Yeong-Hau H. Lien MD, PhD S (18)
") Accepted Manuscript No more thrombotic thrombocytopenic purpura/hemolytic uremic syndrome please Yeong-Hau H. Lien MD, PhD PII: S0002-9343(18)30965-3 DOI: https://doi.org/10.1016/j.amjmed.2018.10.009 Reference:
Accepted Manuscript No more thrombotic thrombocytopenic purpura/hemolytic uremic syndrome please Yeong-Hau H. Lien MD, PhD PII: S0002-9343(18)30965-3 DOI: https://doi.org/10.1016/j.amjmed.2018.10.009 Reference:
W J N. World Journal of Nephrology. Reclassification of membranoproliferative glomerulonephritis: Identification of a new GN: C3GN.
 W J N World Journal of Nephrology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5527/wjn.v5.i4.308 World J Nephrol 2016 July 6; 5(4): 308-320
W J N World Journal of Nephrology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5527/wjn.v5.i4.308 World J Nephrol 2016 July 6; 5(4): 308-320
Research Article Transplant Outcomes in Patients with Idiopathic Membranous Nephropathy
 International Nephrology Volume 2013, Article ID 818537, 4 pages http://dx.doi.org/10.1155/2013/818537 Research Article Transplant Outcomes in Patients with Idiopathic Membranous Nephropathy Claire Kennedy,
International Nephrology Volume 2013, Article ID 818537, 4 pages http://dx.doi.org/10.1155/2013/818537 Research Article Transplant Outcomes in Patients with Idiopathic Membranous Nephropathy Claire Kennedy,
Pathogenetic mechanisms in atypical HUS
 Pathogenetic mechanisms in atypical HUS Seppo Meri University & University Hospital Helsinki, Finland Antalya, Turkey Photo: Markku Kallio 21.10.2017 HUS after eating Kebab - 22 yo female - watery diarrhea
Pathogenetic mechanisms in atypical HUS Seppo Meri University & University Hospital Helsinki, Finland Antalya, Turkey Photo: Markku Kallio 21.10.2017 HUS after eating Kebab - 22 yo female - watery diarrhea
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Key Facts. About C3 Glomerulopathy or C3G 4 WHAT CAUSES C3G? 6 HOW COMMON IS C3G? 7 WHO IS AFFECTED? 9 SIGNS AND SYMPTOMS 12 KIDNEY BIOPSY
 WHAT IS CG? BREAKING DOWN THE TERM CG HOW YOUR KIDNEYS WORK WHAT CAUSES CG? WHAT IS THE COMPLEMENT SYSTEM? HOW COMMON IS CG? WHO IS AFFECTED? RELATIONSHIP OF MPGN TYPES I, II, III AND CG SIGNS AND SYMPTOMS
WHAT IS CG? BREAKING DOWN THE TERM CG HOW YOUR KIDNEYS WORK WHAT CAUSES CG? WHAT IS THE COMPLEMENT SYSTEM? HOW COMMON IS CG? WHO IS AFFECTED? RELATIONSHIP OF MPGN TYPES I, II, III AND CG SIGNS AND SYMPTOMS
TMA CASE STUDY. Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit
 TMA CASE STUDY Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit Cumulative fraction of patients free of events ahus is a catastrophic disease that can result in sudden & progressive
TMA CASE STUDY Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit Cumulative fraction of patients free of events ahus is a catastrophic disease that can result in sudden & progressive
glomerular capillary wall Pathogenic Mechanisms of Glomerular Diseases General Outline General Trend General Concepts
 General Outline Pathogenic Mechanisms of Glomerular Diseases Patrick H. Nachman, MD Professor University of North Carolina UNC Kidney Center Chapel Hill, NC USA Overview of Pathogenetic Mechanisms For
General Outline Pathogenic Mechanisms of Glomerular Diseases Patrick H. Nachman, MD Professor University of North Carolina UNC Kidney Center Chapel Hill, NC USA Overview of Pathogenetic Mechanisms For
RaDaR Inclusion and Exclusion Criteria. Diagnosis Inclusion Criteria Exclusion Criteria. Alport Syndrome definite or probable
 Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
TMA in HUS and TTP: new insights
 TMA in HUS and TTP: new insights Daan Dierickx University Hospitals Leuven, Department of Hematology, Belgium 20th Annual Meeting Belgian Society on Thrombosis and Haemostatis Antwerpen, 22 th November
TMA in HUS and TTP: new insights Daan Dierickx University Hospitals Leuven, Department of Hematology, Belgium 20th Annual Meeting Belgian Society on Thrombosis and Haemostatis Antwerpen, 22 th November
Atypical hemolytic uremic syndrome. Diana Karpman Department of Pediatrics Lund University
 Atypical hemolytic uremic syndrome Diana Karpman Department of Pediatrics Lund University Image courtesy of Dr. Sabine Leh, Haukeland University Hospital, Bergen Norway Hemolytic Uremic Syndrome Non-immune
Atypical hemolytic uremic syndrome Diana Karpman Department of Pediatrics Lund University Image courtesy of Dr. Sabine Leh, Haukeland University Hospital, Bergen Norway Hemolytic Uremic Syndrome Non-immune
Core Curriculum in Nephrology
 Core Curriculum in Nephrology Glomerular Diseases Dependent on Complement Activation, Including Atypical Hemolytic Uremic Syndrome, Membranoproliferative Glomerulonephritis, and C3 Glomerulopathy: Core
Core Curriculum in Nephrology Glomerular Diseases Dependent on Complement Activation, Including Atypical Hemolytic Uremic Syndrome, Membranoproliferative Glomerulonephritis, and C3 Glomerulopathy: Core
Soliris (eculizumab) DRUG.00050
 DRUG.00050") Market DC Soliris (eculizumab) DRUG.00050 Override(s) Prior Authorization Approval Duration 1 year Medications Soliris (eculizumab) APPROVAL CRITERIA Paroxysmal Nocturnal Hemoglobinuria I. Initiation of
Market DC Soliris (eculizumab) DRUG.00050 Override(s) Prior Authorization Approval Duration 1 year Medications Soliris (eculizumab) APPROVAL CRITERIA Paroxysmal Nocturnal Hemoglobinuria I. Initiation of
Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab
 TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
ahus A PATIENT S GUIDE To learn more about ahus, visit Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved.
 To learn more about ahus, visit www.ahussource.com ahus A PATIENT S GUIDE Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved. SOL 1169 BECOME EMPOWERED By learning more and taking control
To learn more about ahus, visit www.ahussource.com ahus A PATIENT S GUIDE Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved. SOL 1169 BECOME EMPOWERED By learning more and taking control
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
29th Annual Meeting of the Glomerular Disease Collaborative Network
 29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
Hemolytic Uremic Syndrome
 Hemolytic Uremic Syndrome Francesco Emma Division of Nephrology and Dialysis Bambino Gesù Children s Hospital, IRCCS Rome, Italy Hemolytic Uremic Syndrome (HUS) microangiopathic hemolytic anemia thrombocytopenia
Hemolytic Uremic Syndrome Francesco Emma Division of Nephrology and Dialysis Bambino Gesù Children s Hospital, IRCCS Rome, Italy Hemolytic Uremic Syndrome (HUS) microangiopathic hemolytic anemia thrombocytopenia
ACUTE GLOMERULONEPHRITIS. IAP UG Teaching slides
 ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
Diagnostic dilemmas in a girl with acute glomerulonephritis: Answers
 Pediatr Nephrol (2018) 33:65 69 DOI 10.1007/s00467-017-3626-3 CLINICAL QUIZ Diagnostic dilemmas in a girl with acute glomerulonephritis: Answers Farah A. Falix 1 & Michiel J. S. Oosterveld 1 & Sandrine
Pediatr Nephrol (2018) 33:65 69 DOI 10.1007/s00467-017-3626-3 CLINICAL QUIZ Diagnostic dilemmas in a girl with acute glomerulonephritis: Answers Farah A. Falix 1 & Michiel J. S. Oosterveld 1 & Sandrine
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS