C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
|
|
|
- Antonia Dixon
- 5 years ago
- Views:
Transcription

1 C3 GLOMERULOPATHIES Budapest Nephrology School Zoltan Laszik 1
2 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical course of C3 glomerulopathies Explore the underlying pathogenetic mechanisms of C3 glomerulopathies Venture into the unknown and therapy
3 Percutaneous needle kidney biopsies Historical context Iversen and Brun (1951), Denmark Alwall (1952), Sweden Kark and Muehrcke (1952), University of Illinois, Chicago Pirani (early 50 s), pathology interpretation, University of Illinois, Chicago

4 Light Microscopy (LM)

5 H&E PAS Trichrome Jones methenamine silver
 Subendothelial (at inner surface of glomerular basement membranes) Antibody against")
 Granular immunofluorescence Granular Linear or linear")
6 Antibody mediated glomerular injury Deposition of circulating immune complexes In situ binding of antibodies with or without immune complex formation Subepithelial (at outer surface of glomerular basement membranes) Subendothelial (at inner surface of glomerular basement membranes) Antibody against antigen on podocytes Anti-glomerular basement membrane antibody Mesangial Subepithelial immune complex formation (membranous glomerulonephritis) Anti-glomerular basement membrane glomerulonephritis (no immune complexes formed) Granular immunofluorescence Granular Linear or linear immunofluorescence

7 The hunt for the immune complexes
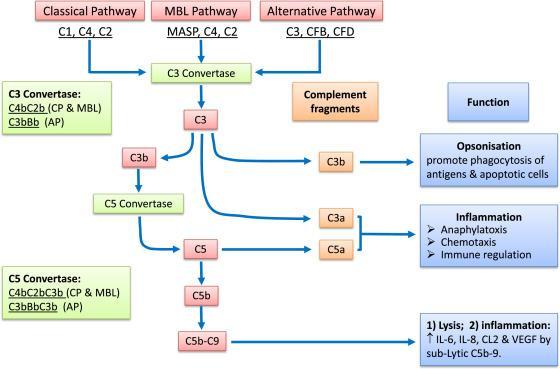
8 Mechanisms of glomerular diseases Binding of antibodies to cellular or extracellular glomerular constituents Glomerular immune complex deposition or in situ immune complex formation Binding of antigens to glomerular cells or matrix Complement activation via classical pathway Complement activation via alternative and mannose binding lectin pathway Local complement activation via alternative pathway due to complement dysregulation Glomerular recruitment of neutrophils and monocytes Glomerular injury via C5b-9 complex Glomerular injury via proteases and oxygen-derived free radicals f0030 Proteinuria, hematuria and structural damage
9 Mechanisms of glomerular diseases Immune mechanisms Circulating Immune Complexes Immune Complexes Formed In Situ Anti-GBM Antibody Mediated Caused by Abnormal Complement Activation Mediators of immune injury Complement and leukocytes Podocyte injury Nephron loss
10 Algorithm of Morphologic Interpretation of Glomerular Patterns The True Glomerulonephritides The Non-Glomerulonephritic Glomerulonephrophathies A. Is there glomerular hypercellularity (with narrowing of capillary lumens)? GLOMERULAR HYPERCELLULARITY (usually nephritic) or MINIMAL GLOMERULAR HYPERCELLULARITY (usually nephrotic) B. Is the hypercellularity: INTRA- CAPILLARY or EXTRA- CAPILLARY (crescents) Crescentic GN MESANGIUM NORMAL Minimal Change Nephrotic Syndrome DIFFUSE MESANGIAL PROMINENCE Diffuse Mesangial Hypercellularity or DIABETIC NEPHROPATHY SEGMENTAL MESANGIAL SCLEROSIS Focal segmental sclerosis MEMBRANOUS GLOMERULO- NEPHROPATHY C. Is the hypercellularity: DIFFUSE FOCAL Global or Segmental 1) Acute Postinfectious GN 2) Membranoproliferative GN (Types 1,2,3) or Focal GN (SLE, Collagenvascular diseases infective endocarditis etc.)
11 MPGN Previous classification MPGN Type I MPGN Type II or DDD MPGN Type III Light Microscopy Mesangial proliferation with GBM duplication (PMGN pattern) Diverse glomerular histology with/without PMGN PMGN Histological pattern Electron Microscopy (location of deposits) Mesangial and subendothelial Electro-dense mesangial and intramembranous Mesangials, subendothelials subepithelials and/or intramembranous Immunofluorescence C3 +/- lgg And/or lgg, C1 Isolated C3 lg negative Isolated C3 Isolated C3 lg negative C3 +/- lgg And/or lgg, C1 C3GN DDD C3GN Complement activation Classical Alternative Classical Current classification MPGN type I Glomerulopathies C3 MPGN type III
12 Membranoproliferative GN Types I, II and III Children and young adults Nephrotic and nephritic Rare Secondary forms older adults most commonly associated with hepatitis C

13 MPGN, 1 Endocapillary proliferation Mesangial matrix accumulation

14 MPGN, 1 Endocapillary proliferation Basement membrane reduplication

15 MPGN, 1 IgG/C3
16 MPGN, type I, secondary forms Infections Viral, bacterial, parasitic SLE Liver diseases Hepatitis (C & B) Cirrhosis or fibrosis (with or without hepatitis) Portosystemic shunt With dominant IgA2 deposits
17 Classic MPGN type 1 vs Cryoglobulinemic GN
18 Antibody mediated glomerular injury Deposition of circulating immune complexes In situ binding of antibodies with or without immune complex formation Subepithelial (at outer surface of glomerular basement membranes) Subendothelial (at inner surface of glomerular basement membranes) Antibody against antigen on podocytes Anti-glomerular basement membrane antibody Mesangial Subepithelial immune complex formation (membranous glomerulonephritis) Anti-glomerular basement membrane glomerulonephritis (no immune complexes formed) Granular immunofluorescence Granular Linear or linear immunofluorescence


19 Dense Deposit Disease (MPGN, Type 2)

20 Dense Deposit Disease (MPGN, Type II) C3
21 Dense deposit disease (DDD) (Type 2, MPGN) Recognized by transmission electron microscopy (1962) C3 glomerular deposition and low serum C3 levels attributed to the activation of the alternative pathway of complement (1975) In the 1980s, several reports in affected families indicated a genetic basis for some cases of DDD Berger J, Galle P. J Urol Nephrol (Paris) 1962; 68: Habib et al. Kidney Int 1975; 7:
22 Dense Deposit Disease (Type 2, MPGN) Clinical presentation Nephritic, proteinuria, hematuria, renal insufficiency Post tx recurrence common; outcome generally favorable Monoclonal gammopathy in older patients
23 Dense Deposit Disease (MPGN, Type 2) Etiology Associated with complement dysregulation C3NF (anti-c3 convertase)* Genetic Homozygous Factor H mutations Heterozygous Factor H, I, MCP mutations* Low serum C3 (but not C4) common, but does not correlate with disease activity Pediatr Nephrol (2011) 26:

24 C3 nephritic factor (C3NeF) Existence inferred from the accelerated C3 breakdown in vitro following the addition to normal human serum of serum obtained from patient with persistent hypocomplementemic GN Spitzer RE et al. Serum C 3 lytic system in patients with glomerulonephritis. Science 1969; 164:
25 DDD, IF & Mass Spec 41% C3 only (without Ig) 59% dominant C3 with up to 1+ IgM 80% dominant C3 of X2 orders of magnitude of intensity by IF greater than any other immune reactant Complement C3, MAC components, CFHR5, vitronectin and apolipoprotein E Absence of CFB consistent with AP C3 convertase formation with excessive C3 activation in the fluid phase, with subsequent deposition of C3 breakdown products Hou J et al. KI 2013 doi: /ki
26 Mechanisms of glomerular diseases f0030 Binding of antibodies to cellular or extracellular glomerular constituents Complement activation via classical pathway Glomerular injury via C5b-9 complex Glomerular immune complex deposition or in situ immune complex formation Complement activation via alternative and mannose binding lectin pathway Binding of antigens to glomerular cells or matrix Glomerular recruitment of neutrophils and monocytes Glomerular injury via proteases and oxygen-derived free radicals Proteinuria, hematuria and structural damage Local complement activation via alternative pathway due to complement dysregulation Immune mechanisms Circulating Immune Complexes Immune Complexes Formed In Situ Anti-GBM Antibody Mediated Caused by Abnormal Complement Activation Mediators of immune injury Complement and leukocytes Podocyte injury Nephron loss

27 MPGN type 3
28 MPGN Previous classification MPGN Type I MPGN Type II or DDD MPGN Type III Light Microscopy Mesangial proliferation with GBM duplication (PMGN pattern) Diverse glomerular histology with/without PMGN PMGN Histological pattern Electron Microscopy (location of deposits) Mesangial and subendothelial Electro-dense mesangial and intramembranous Mesangials, subendothelials subepithelials and/or intramembranous Immunofluorescence C3 +/- lgg And/or lgg, C1 Isolated C3 lg negative Isolated C3 Isolated C3 lg negative C3 +/- lgg And/or lgg, C1 C3GN DDD C3GN Complement activation Classical Alternative Classical Current classification MPGN type I Glomerulopathies C3 MPGN type III


29 C3 Glomerulonephritis C3 Servais A, Fremeaux-Bacchi V, et al. Primary glomerulonephritis with isolated C3 deposits: a new entity which shares common genetic risk factors with haemolytic uraemic syndrome. J Med Genet. (2007) 44:
30 MPGN Previous classification MPGN Type I MPGN Type II or DDD MPGN Type III Light Microscopy Mesangial proliferation with GBM duplication (PMGN pattern) Diverse glomerular histology with/without PMGN PMGN Histological pattern Electron Microscopy (location of deposits) Mesangial and subendothelial Electro-dense mesangial and intramembranous Mesangials, subendothelials subepithelials and/or intramembranous Immunofluorescence C3 +/- lgg And/or lgg, C1 Isolated C3 lg negative Isolated C3 Isolated C3 lg negative C3 +/- lgg And/or lgg, C1 C3GN DDD C3GN Complement activation Classical Alternative Classical Current classification MPGN type I Glomerulopathies C3 MPGN type III
31 C3 glomerulopathies dense deposit disease (DDD) (Formerly MPGN type 2) C3 glomerulonephritis (C3GN) FHR5 nephropathy
32 C3 glomerulopathies Key histological feature isolated complement C3 glomerular deposits with no or little immunoglobulins Etiology dysregulation of the alternative pathway of complement genetic defects and/or autoantibodies are identified in a proportion of patients
33 Autoantibodies in C3 glomerulopathies C3NeF Common in DDD, less so in C3GN Levels do not correlate with the course of nephritis in DDD Nonspecific frequent in MPGN Type 1 and rarely in LN or individuals without renal disease Other autoantibodies To CFB (one patient with DDD) - stabilizes AP C3 convertase To CFB and C3b (two patients with DDD) Anti-CFH monoclonal light chains or (possibly monoclonal) Ig, inhibitory (DDD and C3GN) CFH autoantibodies (C3GN)
34 C3 GN: Genetic abnormalities Original French C3GN series heterozygous mutations in the CFH, CFI and MCP genes Additional cases of DDD, C3GN, and MPGN Type 1 homozygous CFH, heterozygous CFH and CFI mutations DDD (50%), C3GN (27%) and MPGN Type 1 (17%) CFH, CFI, CD46 and C3 Servais A et al. KI 2012; 82: Zhao W et al. (2018). Genetic analysis of the complement pathway in C3 glomerulopathy. Nephrol Dial Transplant

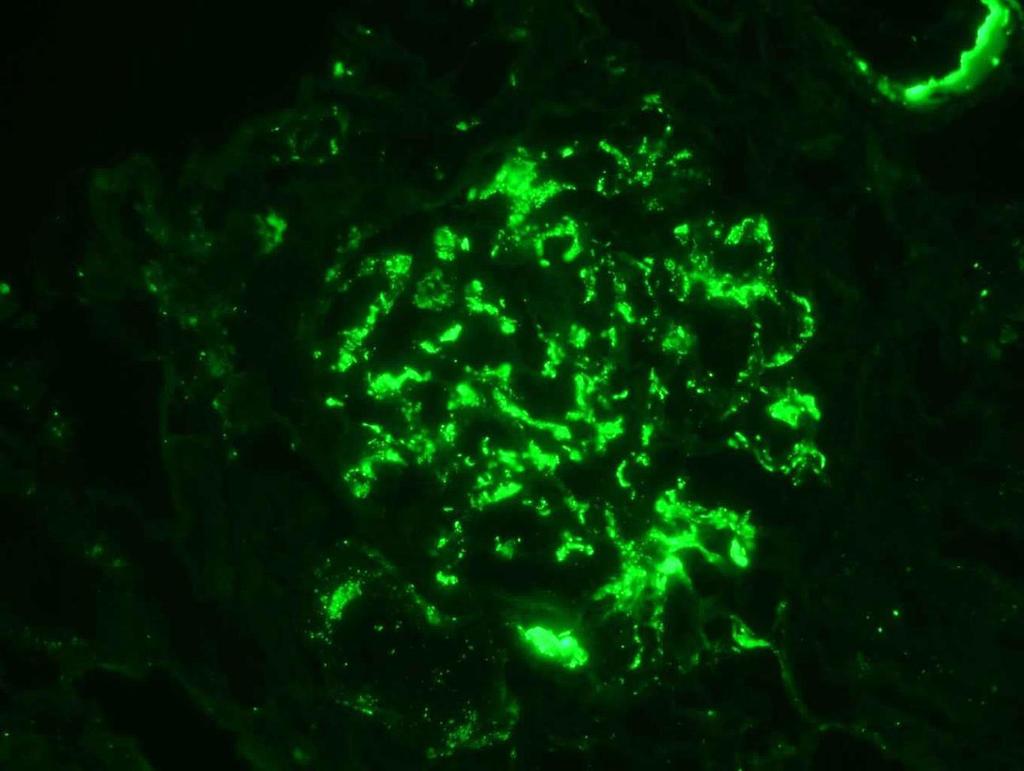
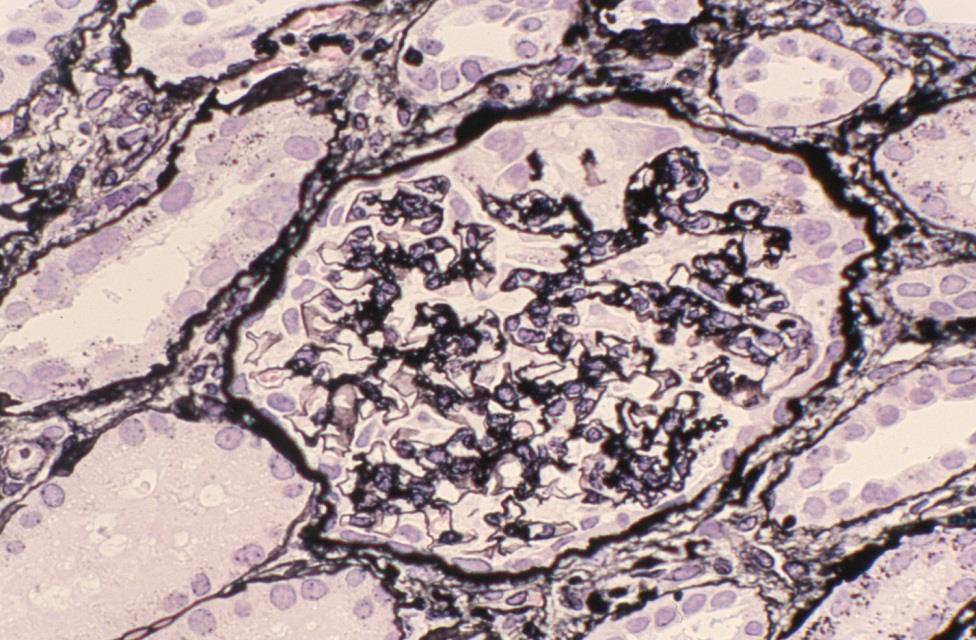
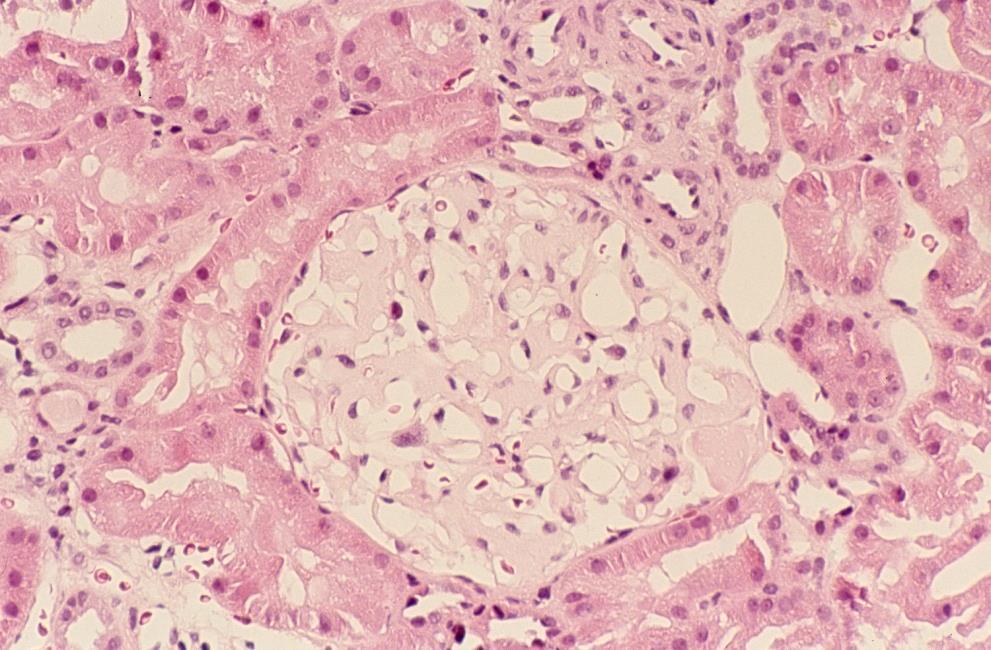
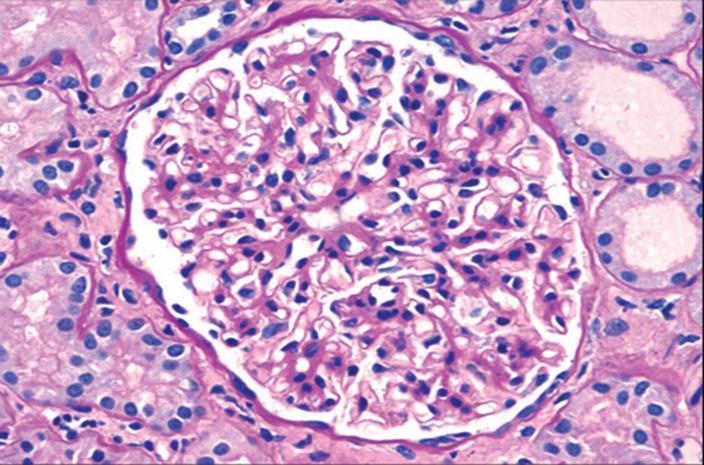
35 DDD vs. C3GN IF (C3c)

36 DDD vs. C3GN EM

37 DDD vs. C3GN EM
38 C3GN: Mesangial and subepithelial deposits


39 C3 GN with conventional mesangial deposits C3 GN with DDD-like mesangial deposits
40 C3 glomerulonephritis and dense deposit disease share a similar disease course in a large United States cohort of patients with C3 glomerulopathy Bomback, A. S., D. Santoriello, et al. (2018). Kidney Int 93(4):
 and dense deposit disease (42%).")
41 Over an average of 72 months of follow-up, remission occurred in 38% of patients with C3GN and 25% of patients with dense deposit disease. Progression to late-stage CKD and ESRD was common, with no differences between C3GN (39%) and dense deposit disease (42%).
42 C3 GN vs PIGN Differentiation of PIGN from C3 GN often cannot be made on the basis of morphology and clinical and laboratory data available at the time of biopsy Clinical and serologic follow up over several months to determine the course of urinary abnormalities and serum C3 levels If these parameters do not follow a typical course of PIGN (i.e., normalization of the decreased peripheral C3 level in 8 12 weeks), a diagnosis of C3 GN should be reconsidered and additional investigations performed Espinosa-Figueroa, J. L., M. Cano-Megias, et al. (2018). Recurrent postinfectious glomerulonephritis: an unusual evolution compatible with C3 glomerulopathy." BMJ Case Rep 2018.
43
44 Potential significance/caviats of C3/C5b-9 fragment detection Various C3 fragments (C3b, C3c, C3dg) can mediate distinct biological responses through their interactions with complement receptors Glomerular and tubular BM deposits of C5b-9 may persist in repeat renal biopsies of C3 GN and DDD 1 year after initiation of Eculizumab therapy despite the normalization of serum C5b- 9 levels C5b-9 may be present in glomeruli of normal kidneys
45 Case Challenge The patient is a 41-year-old woman with a history of systemic plasmacytosis (On prednisone last year for five months) Creatinine 1.3 Has low grade proteinuria (~1gr/24h) and no hematuria
46 Audience Response What would you do next? A. Do nothing B. Do a kidney biopsy C. I m not sure


47 Biopsy findings: C3 GN, mesangial variant C3


48 C3 GN, mesangial variant lambda kappa
49 Mesangial and subepithelial deposits
50 C3 GN: Morphologic manifestations Mild mesangial proliferative GN MPGN Crescentic GN

51

52 Recurrent C3GN post transplant
53 CFHR5 nephropathy (Familial C3GN) Caused heterozygous internal duplication of the CFHR5 gene in Cypriot families (autosomal dominant) Mesangioproliferative or MPGN pattern GN Subendothelial and mesangial deposits with occasional subepithelial deposits by EM Microscopic haematuria and episodes of synpharyngitic macroscopic haematuria (~50%) Serum C3 levels almost invariably normal Progression to ESKD common in adults (mostly in males) Ten patients with successful transplantation and one other with disease recurrence Gale DP et al. Lancet 2010; 376: Gale DP et al. Dis Model Mech 2011; 4:
54 Treatment BP control and antiproteinuric therapy (ACE inhibitors) Steroids, other immunosuppressants Long-term plasma infusion Administration of CFH (if it becomes available) Therapeutic inhibition of complement C3 or C5 successful and unsuccessful treatment with Eculizumab in both C3GN and DDD
55 C3 glomerulonephritis secondary to mutations in factors H and I: rapid recurrence in deceased donor kidney transplant effectively treated with eculizumab. Garg, N., Y. Zhang, et al. (2018). Nephrol Dial Transplant.
56 From: C3 glomerulonephritis secondary to mutations in factors H and I: rapid recurrence in deceased donor kidney transplant effectively treated with eculizumab Nephrol Dial Transplant. Published online January 23, doi: /ndt/gfx369 Nephrol Dial Transplant The Author(s) Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved.
 2018. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved.")
57 From: C3 glomerulonephritis secondary to mutations in factors H and I: rapid recurrence in deceased donor kidney transplant effectively treated with eculizumab Nephrol Dial Transplant. Published online January 23, doi: /ndt/gfx369 Nephrol Dial Transplant The Author(s) Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved.
58 From: C3 glomerulonephritis secondary to mutations in factors H and I: rapid recurrence in deceased donor kidney transplant effectively treated with eculizumab Nephrol Dial Transplant. Published online January 23, doi: /ndt/gfx369 Nephrol Dial Transplant The Author(s) Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved.
59 Recurrent allograft C3 glomerulonephritis and unsuccessful eculizumab treatment Kaartinen K et al Clin Immunol 187: C3Nef positive with C3 activation only - Analyzing C3Nef-mediated C3 and C5 activation separately could help in choosing the right patients for eculizumab therapy
60 Thank you!
61
C3 Glomerulopathy. Jun-Ki Park
 C3 Glomerulopathy Jun-Ki Park 03.08.11 For the last 30 years classification MPGN is based on glomerular findings by light microscopy with further specification on EM and staining for Ig and complement
C3 Glomerulopathy Jun-Ki Park 03.08.11 For the last 30 years classification MPGN is based on glomerular findings by light microscopy with further specification on EM and staining for Ig and complement
C3 Glomerulonephritis versus C3 Glomerulopathies?
 Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Complement in vasculitis and glomerulonephritis. Andy Rees Clinical Institute of Pathology Medical University of Vienna
 Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C3 Glomerulopathy. Rezan Topaloglu, MD Hacettepe University School of Medicine Department of Pediatric Nephrology Ankara, TURKEY
 C3 Glomerulopathy Rezan Topaloglu, MD Hacettepe University School of Medicine Department of Pediatric Nephrology Ankara, TURKEY Journey in history Some diseases have journey Diagnoses may change during
C3 Glomerulopathy Rezan Topaloglu, MD Hacettepe University School of Medicine Department of Pediatric Nephrology Ankara, TURKEY Journey in history Some diseases have journey Diagnoses may change during
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
From MPGN to C3G. F Fakhouri, Nantes, France. «Membranoproliferative» is a pathological feature. Mesangial expansion «Doubles contours»
 From MPGN to C3G F Fakhouri, Nantes, France Conflits d intérêt: consultant auprès d Alexion Pharmaceuticals «Membranoproliferative» is a pathological feature Mesangial expansion «Doubles contours» Immune
From MPGN to C3G F Fakhouri, Nantes, France Conflits d intérêt: consultant auprès d Alexion Pharmaceuticals «Membranoproliferative» is a pathological feature Mesangial expansion «Doubles contours» Immune
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA
 C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA C3 Glomerulopathy Overview Discuss C3 Glomerulopathy (C3G) How did we get to the current classification
C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA C3 Glomerulopathy Overview Discuss C3 Glomerulopathy (C3G) How did we get to the current classification
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Toward a working definition of C3 glomerulopathy by immunofluorescence
 http://www.kidney-international.org & 2013 International Society of Nephrology Toward a working definition of C3 glomerulopathy by immunofluorescence Jean Hou 1, Glen S. Markowitz 1, Andrew S. Bomback
http://www.kidney-international.org & 2013 International Society of Nephrology Toward a working definition of C3 glomerulopathy by immunofluorescence Jean Hou 1, Glen S. Markowitz 1, Andrew S. Bomback
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Membranoproliferative Glomerulonephritis
 Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
C3 glomerulopathy: consensus report
 http://www.kidney-international.org & 2013 International Society of Nephrology OPEN C3 glomerulopathy: consensus report Matthew C. Pickering 1, Vivette D. D Agati 2, Carla M. Nester 3,4, Richard J. Smith
http://www.kidney-international.org & 2013 International Society of Nephrology OPEN C3 glomerulopathy: consensus report Matthew C. Pickering 1, Vivette D. D Agati 2, Carla M. Nester 3,4, Richard J. Smith
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Review Article Kidney Diseases Caused by Complement Dysregulation: Acquired, Inherited, and Still More to Come
 Clinical and Developmental Immunology Volume 2012, Article ID 695131, 6 pages doi:10.1155/2012/695131 Review Article Kidney Diseases Caused by Complement Dysregulation: Acquired, Inherited, and Still More
Clinical and Developmental Immunology Volume 2012, Article ID 695131, 6 pages doi:10.1155/2012/695131 Review Article Kidney Diseases Caused by Complement Dysregulation: Acquired, Inherited, and Still More
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Recurrence of C3G after renal transplantation. Moglie Le Quintrec Service de Néphrologie, Hôpital Foch CRC, UMRS 1138, Equipe complement and diseases
 Recurrence of C3G after renal transplantation Moglie Le Quintrec Service de Néphrologie, Hôpital Foch CRC, UMRS 1138, Equipe complement and diseases New MPGN classification C3G MPGN I DDD C3GN IF C3 deposits
Recurrence of C3G after renal transplantation Moglie Le Quintrec Service de Néphrologie, Hôpital Foch CRC, UMRS 1138, Equipe complement and diseases New MPGN classification C3G MPGN I DDD C3GN IF C3 deposits
Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG)
") Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
ACUTE GLOMERULONEPHRITIS. IAP UG Teaching slides
 ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Membranoproliferative glomerulonephritis and C3 glomerulopathy: resolving the confusion
 http://www.kidney-international.org & 2012 International Society of Nephrology Membranoproliferative glomerulonephritis and C3 glomerulopathy: resolving the confusion Sanjeev Sethi 1, Carla M. Nester 2,3,4
http://www.kidney-international.org & 2012 International Society of Nephrology Membranoproliferative glomerulonephritis and C3 glomerulopathy: resolving the confusion Sanjeev Sethi 1, Carla M. Nester 2,3,4
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits in 5 renal allografts
 Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review
 Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
Advances in Membranous and Membranoproliferative glomerulonephritis: Insights into Pathogenesis
 Advances in Membranous and Membranoproliferative glomerulonephritis: Insights into Pathogenesis Terry Cook, Imperial College, London Membranous Glomerulonephritis Membranous glomerulonephritis is characterised
Advances in Membranous and Membranoproliferative glomerulonephritis: Insights into Pathogenesis Terry Cook, Imperial College, London Membranous Glomerulonephritis Membranous glomerulonephritis is characterised
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS
 GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
J Nephropharmacol. 2014; 3(2): Journal of Nephropharmacology
: Journal of Nephropharmacology") J Nephropharmacol. 2014; 3(2): 33 37. NPJ Journal of Nephropharmacology Pathological patterns of mesangioproliferative glomerulonephritis seen at a tertiary care center Ghadeer A. Mokhtar 1*, Sawsan Jalalah
J Nephropharmacol. 2014; 3(2): 33 37. NPJ Journal of Nephropharmacology Pathological patterns of mesangioproliferative glomerulonephritis seen at a tertiary care center Ghadeer A. Mokhtar 1*, Sawsan Jalalah
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Evidence Review: Title. Month/ Year. Evidence Review: Eculizumab in the treatment of recurrence of C3 glomerulopathy post-transplant
 Evidence Review: Title Month/ Year Evidence Review: Eculizumab in the treatment of recurrence of C glomerulopathy post-transplant October 2015 1 Standard Operating Procedure: NHS England Evidence Review:
Evidence Review: Title Month/ Year Evidence Review: Eculizumab in the treatment of recurrence of C glomerulopathy post-transplant October 2015 1 Standard Operating Procedure: NHS England Evidence Review:
Monoclonal gammopathies consist of. Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis REVIEW
 REVIEW Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis Sanjeev Sethi, MD, PhD, and S. Vincent Rajkumar, MD Abstract Monoclonal gammopathy is characterized by circulating monoclonal immunoglobulin
REVIEW Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis Sanjeev Sethi, MD, PhD, and S. Vincent Rajkumar, MD Abstract Monoclonal gammopathy is characterized by circulating monoclonal immunoglobulin
Pathogenesis of IgA Nephropathy. Shokoufeh Savaj MD Associate Professor of Medicine Firoozgar hospital- IUMS
 Pathogenesis of IgA Nephropathy Shokoufeh Savaj MD Associate Professor of Medicine Firoozgar hospital- IUMS History Immunoglobin A nephropathy was first described by Berger and Hinglais in 1968 in Paris
Pathogenesis of IgA Nephropathy Shokoufeh Savaj MD Associate Professor of Medicine Firoozgar hospital- IUMS History Immunoglobin A nephropathy was first described by Berger and Hinglais in 1968 in Paris
Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive Nephrotic Syndrome
 J Korean Med Sci 2009; 24 (Suppl 1): S44-9 ISSN 1011-8934 DOI: 10.3346/jkms.2009.24.S1.S44 Copyright The Korean Academy of Medical Sciences Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive
J Korean Med Sci 2009; 24 (Suppl 1): S44-9 ISSN 1011-8934 DOI: 10.3346/jkms.2009.24.S1.S44 Copyright The Korean Academy of Medical Sciences Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive
Immune profile of IgA-dominant diffuse proliferative glomerulonephritis
 Clin Kidney J (2014) 7: 479 483 doi: 10.1093/ckj/sfu090 Exceptional Case Immune profile of IgA-dominant diffuse proliferative glomerulonephritis Eric Wallace 1, Nicolas Maillard 2, Hiroyuki Ueda 2, Stacy
Clin Kidney J (2014) 7: 479 483 doi: 10.1093/ckj/sfu090 Exceptional Case Immune profile of IgA-dominant diffuse proliferative glomerulonephritis Eric Wallace 1, Nicolas Maillard 2, Hiroyuki Ueda 2, Stacy
Clinical Findings, Pathology, and Outcomes of C3GN after Kidney Transplantation
 CLINICAL RESEARCH www.jasn.org Clinical Findings, Pathology, and Outcomes of C3GN after Kidney ation Ladan Zand,* Elizabeth C. Lorenz,* Fernando G. Cosio,* Fernando C. Fervenza,* Samih H. Nasr, Manish
CLINICAL RESEARCH www.jasn.org Clinical Findings, Pathology, and Outcomes of C3GN after Kidney ation Ladan Zand,* Elizabeth C. Lorenz,* Fernando G. Cosio,* Fernando C. Fervenza,* Samih H. Nasr, Manish
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS
 MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
Post-infectious (bacterial) Glomerulonephritis
 Glomerulonephritis") Far East Regional Conference Russia Dialysis Society Khabarovsk, Russia October 30, 2015 Post-infectious (bacterial) Glomerulonephritis (An Update) William Couser, MD Affiliate Professor of Medicine University
Far East Regional Conference Russia Dialysis Society Khabarovsk, Russia October 30, 2015 Post-infectious (bacterial) Glomerulonephritis (An Update) William Couser, MD Affiliate Professor of Medicine University
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy?
 CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
Lab 3, case 1. Is this an example of nephrotic or nephritic syndrome? Why? Which portion of the nephron would you expect to be abnormal?
 Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
Clinico-pathologic spectrum of C3 glomerulopathy-an Indian experience
 Viswanathan et al. Diagnostic Pathology (2015) 10:6 DOI 10.1186/s13000-015-0233-0 RESEARCH Open Access Clinico-pathologic spectrum of C3 glomerulopathy-an Indian experience Ganesh Kumar Viswanathan 1,
Viswanathan et al. Diagnostic Pathology (2015) 10:6 DOI 10.1186/s13000-015-0233-0 RESEARCH Open Access Clinico-pathologic spectrum of C3 glomerulopathy-an Indian experience Ganesh Kumar Viswanathan 1,
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Journal of Nephropathology
 www.nephropathol.com DOI: 10.15171/jnp.2017.36 J Nephropathol. 2017;6(3):220-224 Journal of Nephropathology Proliferative glomerulonephritis with monoclonal IgG deposits; an unusual cause of de novo disease
www.nephropathol.com DOI: 10.15171/jnp.2017.36 J Nephropathol. 2017;6(3):220-224 Journal of Nephropathology Proliferative glomerulonephritis with monoclonal IgG deposits; an unusual cause of de novo disease
A Case of IgG2 Heavy Chain Deposition Disease in a Patient with Kappa Positive Plasma Cell Dyscrasia
 Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Glomerular Diseases. Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology
 Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Dense deposit disease with steroid pulse therapy
 Case Report Dense deposit disease with steroid pulse therapy Jun Odaka, Takahiro Kanai, Takane Ito, Takashi Saito, Jun Aoyagi, and Mariko Y Momoi Abstract Treatment of dense deposit disease DDD has not
Case Report Dense deposit disease with steroid pulse therapy Jun Odaka, Takahiro Kanai, Takane Ito, Takashi Saito, Jun Aoyagi, and Mariko Y Momoi Abstract Treatment of dense deposit disease DDD has not
29th Annual Meeting of the Glomerular Disease Collaborative Network
 29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
H. Terence Cook. REVIEW C3 glomerulopathy [version 1; referees: 4 approved] Open Peer Review. Referee Status:
![H. Terence Cook. REVIEW C3 glomerulopathy [version 1; referees: 4 approved] Open Peer Review. Referee Status:](/thumbs/94/119185743.jpg "H. Terence Cook. REVIEW C3 glomerulopathy [version 1; referees: 4 approved] Open Peer Review. Referee Status:") REVIEW C3 glomerulopathy [version 1; referees: 4 approved] H. Terence Cook Department of Medicine, Imperial College London, Hammersmith, London, UK v1 First published: 10 Mar 2017, 6(F1000 Faculty Rev):248
REVIEW C3 glomerulopathy [version 1; referees: 4 approved] H. Terence Cook Department of Medicine, Imperial College London, Hammersmith, London, UK v1 First published: 10 Mar 2017, 6(F1000 Faculty Rev):248
A Case of Myeloma Kidney With Glomerular C3 Deposition
 Case Report World J Nephrol Urol. 2018;7(3-4):73-77 A Case of Myeloma Kidney With Glomerular C3 Deposition Asif Khan a, c, Khine Lam b, Suzanne El-Sayegh b, Elie El-Charabaty b Abstract Manuscript submitted
Case Report World J Nephrol Urol. 2018;7(3-4):73-77 A Case of Myeloma Kidney With Glomerular C3 Deposition Asif Khan a, c, Khine Lam b, Suzanne El-Sayegh b, Elie El-Charabaty b Abstract Manuscript submitted
NEPHRITIC SYNDROME. By Dr Mai inbiek
 NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
considered for patients with cryoglobulinemic kidney diseases. (Weak)
") http://www.kidney-international.org & 2008 DIGO Guideline 5: Diagnosis and management of kidney diseases associated with HCV infection idney International (2008) 73 (Suppl 109), S69 S77; doi:10.1038/ki.2008.88
http://www.kidney-international.org & 2008 DIGO Guideline 5: Diagnosis and management of kidney diseases associated with HCV infection idney International (2008) 73 (Suppl 109), S69 S77; doi:10.1038/ki.2008.88
CASE OF THE WEEK 1
 www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
Diabetic Nephropathy. Introduction/Clinical Setting. Pathologic Findings Light Microscopy. J. Charles Jennette
 12 Diabetic Nephropathy J. Charles Jennette Introduction/Clinical Setting Diabetic nephropathy is a clinical syndrome in a patient with diabetes mellitus that is characterized by persistent albuminuria,
12 Diabetic Nephropathy J. Charles Jennette Introduction/Clinical Setting Diabetic nephropathy is a clinical syndrome in a patient with diabetes mellitus that is characterized by persistent albuminuria,
RENAL BIOPSIES in patients with the clinical
 RENAL BIOPSY TEACHING CASE Crescentic Glomerulonephritis With a Paucity of Glomerular Immunoglobulin Localization Alexis A. Harris, MD, Ronald J. Falk, MD, and J. Charles Jennette, MD RENAL BIOPSIES in
RENAL BIOPSY TEACHING CASE Crescentic Glomerulonephritis With a Paucity of Glomerular Immunoglobulin Localization Alexis A. Harris, MD, Ronald J. Falk, MD, and J. Charles Jennette, MD RENAL BIOPSIES in
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
IgA Nephropathy - «Maladie de Berger»
 IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
Dr. Ghadeer Mokhtar Consultant pathologists and nephropathologist, KAU
 Dr. Ghadeer Mokhtar Consultant pathologists and nephropathologist, KAU CLINICAL HISTORY A 4 year old Saudi girl presented to the ER with generalized body swelling, decrease urine output with passing dark
Dr. Ghadeer Mokhtar Consultant pathologists and nephropathologist, KAU CLINICAL HISTORY A 4 year old Saudi girl presented to the ER with generalized body swelling, decrease urine output with passing dark
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis with Monoclonal Immunoglobulin Deposits of Lambda Light Chain
 Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi
 Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
C3 Glomerulopathy: Clinicopathologic Features and Predictors of Outcome
 CJASN epress. Published on October 31, 2013 as doi: 10.2215/CJN.04700513 Article C3 Glomerulopathy: Clinicopathologic Features and Predictors of Outcome Nicholas R. Medjeral-Thomas,* Michelle M. O Shaughnessy,
CJASN epress. Published on October 31, 2013 as doi: 10.2215/CJN.04700513 Article C3 Glomerulopathy: Clinicopathologic Features and Predictors of Outcome Nicholas R. Medjeral-Thomas,* Michelle M. O Shaughnessy,
Atypical IgA Nephropathy
 Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases
 Kidney International, Vol. 65 (2004), pp. 2145 2152 Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases MARK HAAS and JOSEPH A. EUSTACE Department of Pathology
Kidney International, Vol. 65 (2004), pp. 2145 2152 Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases MARK HAAS and JOSEPH A. EUSTACE Department of Pathology
Overview of pediatric nephropathology
 Kidney Jnternat,onal, Vol. 33 (/988), pp. 1016 1032 Overview of pediatric nephropathology Principal discussant: FRED G. SILVA University of l'exas South u'estern Medical Center at Dallas, Dallas Texas
Kidney Jnternat,onal, Vol. 33 (/988), pp. 1016 1032 Overview of pediatric nephropathology Principal discussant: FRED G. SILVA University of l'exas South u'estern Medical Center at Dallas, Dallas Texas
Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft
 Article Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D. Cornell,* Mary E. Fidler,* Mark Boelkins, Fernando C. Fervenza, Fernando
Article Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D. Cornell,* Mary E. Fidler,* Mark Boelkins, Fernando C. Fervenza, Fernando
C1q nephropathy: a true immune complex disease or an immunologic epiphenomenon?
 NDT Plus (2009) 2: 285 291 doi: 10.1093/ndtplus/sfp055 Advance Access publication 9 May 2009 Case Report C1q nephropathy: a true immune complex disease or an immunologic epiphenomenon? Mordi Muorah 1,ManishD.Sinha
NDT Plus (2009) 2: 285 291 doi: 10.1093/ndtplus/sfp055 Advance Access publication 9 May 2009 Case Report C1q nephropathy: a true immune complex disease or an immunologic epiphenomenon? Mordi Muorah 1,ManishD.Sinha
Article. Eculizumab for Dense Deposit Disease and C3 Glomerulonephritis
 CJASN epress. Published on March 8, 2012 as doi: 10.2215/CJN.12901211 Article Eculizumab for Dense Deposit Disease and C3 Glomerulonephritis Andrew S. Bomback,* Richard J. Smith, Gaetano R. Barile, Yuzhou
CJASN epress. Published on March 8, 2012 as doi: 10.2215/CJN.12901211 Article Eculizumab for Dense Deposit Disease and C3 Glomerulonephritis Andrew S. Bomback,* Richard J. Smith, Gaetano R. Barile, Yuzhou