Practical challenges in CV risk management: When to start intervening in CVD?
|
|
|
- Myles Adams
- 5 years ago
- Views:
Transcription


1 The National Research Center for Preventive Medicine Ministry of Healthcare, Russian Federation Practical challenges in CV risk management: When to start intervening in CVD? Prof. Drapkina O.M., Eliashevich S.O.

2 The ESC Guidelines 2016 The ESC Guidelines represent the views of the ESC and were produced after careful consideration of the scientific and medical knowledge and the evidence available at the time of their publication. However, the ESC Guidelines do not override, in any way whatsoever, the individual responsibility of health professionals to make appropriate and accurate decisions in consideration of each patient s health condition and in consultation with that patient.

3 Two whales and intuition The total CV risk LDL-C level?

4 Recommendations for risk estimation

5 SCORE chart: 10-year risk of fatal cardiovascular disease in populations of countries at high cardiovascular risk
6 Simple principles of risk assessment Persons with documented CVD type 1 or type 2 diabetes very high levels of individual risk factors chronic kidney disease (CKD) are automatically at very high or high total CV risk. No risk estimation models are needed for them; they all need active management of all risk factors.

7 The additional impact of HDL-C on risk estimation for women in populations at high cardiovascular disease risk

8 Relative risk chart, derived from SCORE A particular problem relates to young people with high levels of risk factors; a low absolute risk may conceal a very high relative risk requiring intensive lifestyle advice. To motivate young people not to delay changing their unhealthy lifestyle, an estimate of their relative risk, illustrating that lifestyle changes can reduce relative risk substantially, may be helpful. ESC,2016

 The details should")
9 Low and moderate risk categories The heterogeneity of low and moderate risk group (SCORE 0 5%) The details should be in focus
10 The pilot study The aim: to assess criteria of the low-risk group heterogeneity (SCORE<1%) Inclusion % criteria: low-risk persons (SCORE <1%) aging 18 to 60 years; intima-media thickness <0.9 mm (according to ultrasound examination of the brachiocephalic arteries). Exclusion criteria: smoking over 1 year before the study, atherosclerosis-related cardiovascular pathologies; lipid-lowering therapy within 6 weeks; secondary arterial hypertension; thyroid pathologies; severe concomitant diseases (cardiac, respiratory, renal, and liver insufficiency, cancer, mental illness); pregnancy and lactation. n = 80 Group I Patients with abdominal obesity (AO) n=48 Group II Patients without signs of AO n=32
 mldl-c CRITERIA 0 10 20 30 40 50 60 mldl-c hscrp level General obesity Central obesity")
11 The detected criteria of the low-risk group heterogeneity Central obesity (60% of patients) General obesity (44 % of patients) hs CRP level ( 3 mg/l among 60% of patients) mldl-c CRITERIA mldl-c hscrp level General obesity Central obesity %


12 REGISTERS Prevalence of Overweight, % (BMI kg/m 2 ) According to WHO,
13 HIGH PREVALENCE OF THE MAIN RISK FACTORS OF NONCOMMUNICABLE DISEASES 60 % (n = 19,600, 12 regions) Женщины, Female N=11386 Мужчины, Male N=6919 Total Всего, N= Smoke Курение LPA НФА ESI ИПС PIFV НПОФ AH Повышенное TC Повышенный obesity Ожирение high glucose Повышенная АД ХС глюкоза ABP arterial blood pressure; TC total cholesterol; LFA low physical activity; ESI excessive salt intake; PIFV poor intake of fruit and vegetables Growth of Prevalence of Arterial Hypertension in Men 60 Мужчины Женщины 35 48, , , , ,1 20 % 30 % Growth of Obesity Prevalence Мужчины Женщины 30,8 26,4 26,9 11, НПВ (1993) ЭССЕ (2013) National Research Center for Preventive Medicine

14 Visceral obesity Increase in liver free fatty acids inflow (VLDL ) Glucose utilization in peripheral tissues hyperinsulinemia SMC proliferation with phenotypic changes Fasting hypertriglyceridemia HDL, LDL
15 Multifaced Metabolic Syndrome Thrombophilia Fatty tissue regulation disorder Hyperinsulinemia NAFLD Metabolic syndrome Visceral adiposopathy Insulin resistance Oxidative stress Hyperglycemia Hypertension Dyslipidemia Bonora E., Targher G. Increased risk of cardiovascular disease and chronic kidney disease in NAFLD. Nature Reviews Gastroenterology & Hepatology 2012: 9,

16 Examples of risk modifiers that are likely to have reclassification potential

17 Nontraditional markers of cardiovascular disease risk Routine assessment of circulating or urinary biomarkers is not recommended for refinement of CVD risk stratification (III class, B level).
 Biochemistry Ultrasound/ IMT CT/MRI/ fusion/ ±contrast Invasive (including intravascular US) Cheap, Allow risk")

18 How to catch an «athero» ASAP? Arterial stiffness/ functional tests (FMD) Biochemistry Ultrasound/ IMT CT/MRI/ fusion/ ±contrast Invasive (including intravascular US) Cheap, Allow risk stratification, Prognostic significance, etc BUT Sometimes so early, that it will have not had come into play? Indirect methods!! Simple, cheap, and very fast, Prognostic Significance and YOU CAN SEE IT! BUT Too late? Not reliable? Distrustful? You are able to see an virtual plaque BUT Dedicated, Limited availability, Distrustful [on early stages] fair accuracy (but not 100 %) BUT Young patients (and usually their physicians too) prefer to avoid it due to possible complications
19 The purpose to develop novel reliable noninvasive method of very early atherosclerotic lesions assessment.
20 ! Risk! Enrolled patients 10 patients with advanced symptomatic atherosclerosis (affected both cerebral, coronary, and carotid arteries); 11 patients with subclinical atherosclerosis (by duplex sonography or invasive tests); 10 patients with no evidence of atherosclerosis (assessed by duplex sonography and CT-angio/coronarography), normal intima-media thickness, but presented with dyslipidemia, smoking, and obesity; and 8 comparable healthy controls.
21 Patients characteristics Group / Parameter 1. Healthy controls 2. Pts with risk factors 3. Subclinical athero-s 4. Advanced athero-s Mean age, years 53 ± 8 52 ± 6 52 ± 4 50± 3 Mean blood pressure, mm Hg < 130 and 80 * 147 and and and 89** Myocardium mass (by Deveraux), gr Score risk (ESC), % 170 ± 16 * 230 ± ± ± 29** < 1 % * 4 ± 2 7 ± 4 > 15** * - p < 0,05 for comparison between groups 1 and (2 and 3) ** - p < 0,05 for comparison between groups 4 and (2 and 3)
22 Methods (1) Comprehensive clinical assessment Careful BP monitoring (blood pressure monitoring) Full blood biochemistry (including lipids, CRP, etc) ECG (including stress-test) Echocardiography with tissue doppler Microalbuminuria CT-angio / coronary angiography (In particular patients)
 evaluation Ultrasound transducer Cuff (forearm disposition)")
23 Methods (2) Flow-mediated dilation with parallel dual (US + photoplethysmograpic) assessment Vascular stiffness (RI, SI, Alx, etc) evaluation Ultrasound transducer Cuff (forearm disposition) Photoplethysmograpic sensor
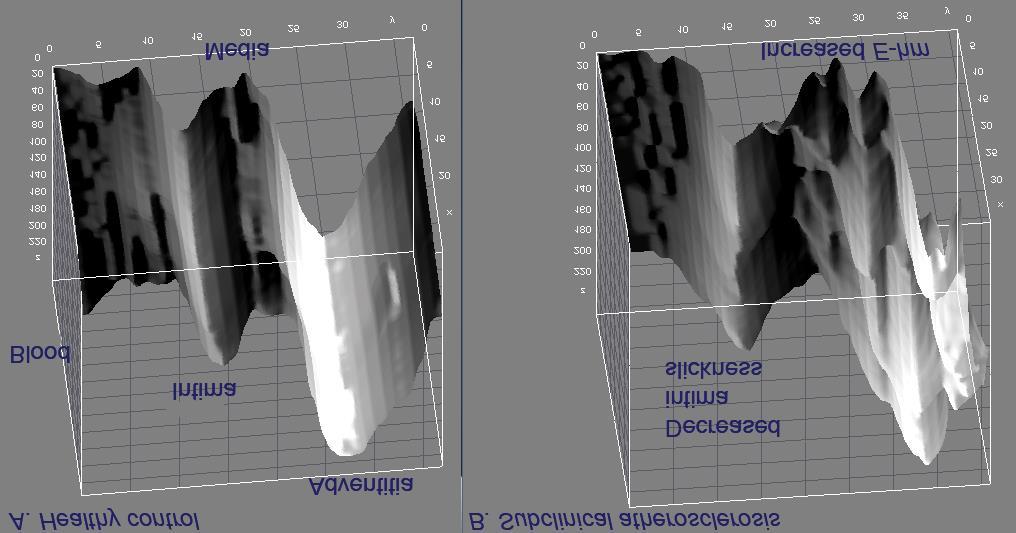
24 Methods: carotid ultrasound (1) High-resolution B-mode ultrasound imaging of common carotid artery structure and its pulse-motion (M-mode) were obtained in uniform regimen by single operator. Then gray-scale arterial wall images were 10-fold enlarged using fractal-based algorithm. After that shear stress, viscosity, stiffness and dimensions of common carotid artery layers (intima, media, adventitia) were assessed. Echo-heterogeneity of media and endothelium were evaluated by computed analysis with 3D-reconstruction of arterial wall.




25 Echo-heterogeneity of media IMT=0.84 mm IMT=0.67 mm 23 % 10 % E-hm = (maximal media echogenicity minimal media echogenicity) / 256 (levels in gray-scale) x 100 %

26 0.5 mm 0.5 mm 3D-reconstruction of the CCA wall

27 ,9 * 27,8 * * * * * - p < 0,05 20,1 * 13 11,7 E-hm,% FMD,% 3 4 8,5 9 6,5 IMT,mm x SCORE 3 7 % Patients 2 with risk factors, SCORE 4 % Healthy 1 controls, SCORE < 1 % Advanced atherosclerosis, SCORE > 15 % Subclinical atherosclerosis,
28 LDL-cholesterol, mg/dl healthy controls E-hm, %
29 LDL-cholesterol, mg/dl healthy controls - patients with risk factors E-hm threshold of 15 % permitted us to differentiate healthy controls from high-risk patients without overt atherosclerosis E-hm, %
30 LDL-cholesterol, mg/dl healthy controls - patients with risk factors - subclinical atherosclerosis r = 0.7, p < E-hm, %
31 LDL-cholesterol, mg/dl healthy controls - patients with risk factors - subclinical atherosclerosis - advanced atherosclerosis r = 0.7, p < 0.05 For IMT and LDL-cholesterol r = 0.4, p < E-hm, %
32 Study limitations Small sample Non-blinded, operator-dependent study, performed by single operator Difficulties associated with different ultrasound device application Morphological verification (autopsy) still in process Unknown prognostic significance
33 Conclusion Media echo-heterogeneity tightly correlates with LDL-cholesterol (r = 0.7, p < 0.05) and the threshold of 15 % allows to distinguish healthy controls from high-risk patients without overt atherosclerosis. The novel ultrasound postprocessing method of non-invasive subtle evaluation of common carotid artery intima and media characteristics might be used to catch atherosclerotic lesions at the earliest stage.
34 Treatment goals for LDL-C LDL-C is recommended as the primary target for treatment (I class, A level). LDL-C I class, B level 3 mmol/l Low and moderate risk I class, B level 2.6 mmol/l or a reduction of at least 50% High-risk IIa class, C level 1.8 mmol/l or a reduction of at least 50% Very high-risk

35 Possible intervention strategies as a function of total cardiovascular risk and LDL-C level

36 One goal, but different ways of achievement Low and moderate risk LDL-C 3 mmol/l Lifestyle modifications Drug therapy Lifestyle modifications plus drug therapy AHA/ACC guidelines have a wider indication for statin therapy than ESC guidelines
37 The primary prevention The absolute benefit from statin treatment may be less evident in patients in primary prevention, who are typically at lower risk. In Cochrane analysis (2013): all-cause mortality was reduced by 14%, CVD events by 27%, fatal and non-fatal coronary events by 27% and stroke by 22% per 1 mmol/l (40 mg/dl) LDL-C reduction. However, it should be emphasized that in subjects with lower risk, the absolute risk reduction is also lower. Thus statin use should be considered for primary prevention at high CV risk
38 It is sad but true Predictors of non-adherence with statins have been identified and include their use in individuals for primary prevention as compared with their use in patients with disease or with multiple risk factors, lower income, being elderly, complex polypharmacy, cost and forgetfulness due to a lack of symptoms and psychological co-morbidities.
39 CAC score improves coronary and CV risk assessment: More Evidence Medscape. Sep 26, The aim of this study was to assess the difference in indication for statin therapy by ESC versus AHA/ACC guidelines and to quantify the potential additional role of coronary artery calcification (CAC) score over updated guidelines in a primary prevention cohort individuals without cardiovascular disease or lipid-lowering therapy at baseline CAC score was assessed between 2000 and (8) years of age, 47% men Prospective study, a mean follow-up 10.4 years Mahabadi AA, Mohlenkamp S. Lehmann N, et al. CAC score improves coronary and CV risk assessment above statin indication by ESC and AHA/ACC primary prevention guidelines. JACC: Cardiovasc Imaging 2016

40 Statin Eligibility According to ESC and AHA/ACC Guidelines

41 CAC-Stratified Coronary and Cardiovascular Event Rate
42 Difference in Event Rate by CAC Score in Subjects With Potential Statin Therapy Coronary Calcium Scores Can Help Some 'Intermediate-Risk' Patients Avoid Statins
CVD Risk Assessment. Michal Vrablík Charles University, Prague Czech Republic
 CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
Association between arterial stiffness and cardiovascular risk factors in a pediatric population
 + Association between arterial stiffness and cardiovascular risk factors in a pediatric population Maria Perticone Department of Experimental and Clinical Medicine University Magna Graecia of Catanzaro
+ Association between arterial stiffness and cardiovascular risk factors in a pediatric population Maria Perticone Department of Experimental and Clinical Medicine University Magna Graecia of Catanzaro
Which CVS risk reduction strategy fits better to carotid US findings?
 Which CVS risk reduction strategy fits better to carotid US findings? Dougalis A, Soulaidopoulos S, Cholongitas E, Chalevas P, Vettas Ch, Doumtsis P, Vaitsi K, Diavasti M, Mandala E, Garyfallos A 4th Department
Which CVS risk reduction strategy fits better to carotid US findings? Dougalis A, Soulaidopoulos S, Cholongitas E, Chalevas P, Vettas Ch, Doumtsis P, Vaitsi K, Diavasti M, Mandala E, Garyfallos A 4th Department
Vascular disease. Structural evaluation of vascular disease. Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital
 Vascular disease. Structural evaluation of vascular disease Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital resistance vessels : arteries
Vascular disease. Structural evaluation of vascular disease Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital resistance vessels : arteries
Some good practices in an interagency approach to the prevention of NCDs in Russia
 National Research Center for Preventive Medicine of the Russian Federation WHO Collaborating Center on Development and Implementation of Non-communicable Disease Prevention Policy and Programs Collaborating
National Research Center for Preventive Medicine of the Russian Federation WHO Collaborating Center on Development and Implementation of Non-communicable Disease Prevention Policy and Programs Collaborating
ΛΟΙΜΩΞΗ HIV. Ιγνάτιος Οικονομίδης,MD,FESC Β Πανεπιστημιακή Καρδιολογική
 ΛΟΙΜΩΞΗ HIV Ιγνάτιος Οικονομίδης,MD,FESC Β Πανεπιστημιακή Καρδιολογική Κλινική, Νοσοκομείο «Αττικόν» Infection Acute Myocardial Infarction p er 100,000 HIV/AIDS discharg es 800 700 600 500 400 300 200
ΛΟΙΜΩΞΗ HIV Ιγνάτιος Οικονομίδης,MD,FESC Β Πανεπιστημιακή Καρδιολογική Κλινική, Νοσοκομείο «Αττικόν» Infection Acute Myocardial Infarction p er 100,000 HIV/AIDS discharg es 800 700 600 500 400 300 200
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary
 2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
Financial Disclosures. Coronary Artery Calcification. Objectives. Coronary Artery Calcium 6/6/2018. Heart Disease Statistics At-a-Glace 2017
 Coronary Artery Calcification Dharmendra A. Patel, MD MPH Director, Echocardiography Laboratory Associate Program Director Cardiovascular Disease Fellowship Program Erlanger Heart and Lung Institute UT
Coronary Artery Calcification Dharmendra A. Patel, MD MPH Director, Echocardiography Laboratory Associate Program Director Cardiovascular Disease Fellowship Program Erlanger Heart and Lung Institute UT
2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE
 2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE Massimo F Piepoli, MD, PhD, FESC, Piacenza, Italy on behalf of the 6 th Joint Task Force 2 3 Guidelines still based upon the principles of
2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE Massimo F Piepoli, MD, PhD, FESC, Piacenza, Italy on behalf of the 6 th Joint Task Force 2 3 Guidelines still based upon the principles of
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Intima-Media Thickness
 European Society of Cardiology Stockholm, 30th August 2010 Intima-Media Thickness Integration of arterial assessment into clinical practice Prof Arno Schmidt-Trucksäss, MD Institute of Exercise and Health
European Society of Cardiology Stockholm, 30th August 2010 Intima-Media Thickness Integration of arterial assessment into clinical practice Prof Arno Schmidt-Trucksäss, MD Institute of Exercise and Health
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
 Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Dyslipidemia in women: Who should be treated and how?
 Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Non alcoholic fatty liver disease and atherosclerosis Raul Santos, MD
 Non alcoholic fatty liver disease and atherosclerosis Raul Santos, MD Sao Paulo Medical School Hospital Sao Paulo, Brazil Disclosure Honoraria received for consult and/or speaker : Astra Zeneca, Amgen,
Non alcoholic fatty liver disease and atherosclerosis Raul Santos, MD Sao Paulo Medical School Hospital Sao Paulo, Brazil Disclosure Honoraria received for consult and/or speaker : Astra Zeneca, Amgen,
Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD
 Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD Sao Paulo Medical School Sao Paolo, Brazil Subclinical atherosclerosis in CVD risk: Stratification & management Prof.
Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD Sao Paulo Medical School Sao Paolo, Brazil Subclinical atherosclerosis in CVD risk: Stratification & management Prof.
Preclinical Detection of CAD: Is it worth the effort? Michael H. Crawford, MD
 Preclinical Detection of CAD: Is it worth the effort? Michael H. Crawford, MD 1 Preclinical? No symptoms No physical findings No diagnostic ECG findings No chest X-ray X findings No diagnostic events 2
Preclinical Detection of CAD: Is it worth the effort? Michael H. Crawford, MD 1 Preclinical? No symptoms No physical findings No diagnostic ECG findings No chest X-ray X findings No diagnostic events 2
Lipoprotein Particle Profile
 Lipoprotein Particle Profile 50% of people at risk for HEART DISEASE are not identified by routine testing. Why is LPP Testing The Most Comprehensive Risk Assessment? u Provides much more accurate cardiovascular
Lipoprotein Particle Profile 50% of people at risk for HEART DISEASE are not identified by routine testing. Why is LPP Testing The Most Comprehensive Risk Assessment? u Provides much more accurate cardiovascular
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
AN EARLY WARNING SYSTEM FOR CARDIOVASCULAR DISEASE
 AN EARLY WARNING SYSTEM FOR CARDIOVASCULAR DISEASE Good for your patients. Good for your practice. Using the AngioDefender system to complement your patients care routine enables you to: Improve your patient
AN EARLY WARNING SYSTEM FOR CARDIOVASCULAR DISEASE Good for your patients. Good for your practice. Using the AngioDefender system to complement your patients care routine enables you to: Improve your patient
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Weintraub, W et al NEJM March Khot, UN et al, JAMA 2003
 Global risk hscrp Should not be included in a Global Cardiovascular Risk Assessment. Jodi Tinkel, MD Assistant Professor Director of Cardiac Rehabilitation Associate Program Director, Cardiovascular Medicine
Global risk hscrp Should not be included in a Global Cardiovascular Risk Assessment. Jodi Tinkel, MD Assistant Professor Director of Cardiac Rehabilitation Associate Program Director, Cardiovascular Medicine
ASSeSSing the risk of fatal cardiovascular disease
 ASSeSSing the risk of fatal cardiovascular disease «Systematic Cerebrovascular and coronary Risk Evaluation» think total vascular risk Assess the risk Set the targets Act to get to goal revised; aupril
ASSeSSing the risk of fatal cardiovascular disease «Systematic Cerebrovascular and coronary Risk Evaluation» think total vascular risk Assess the risk Set the targets Act to get to goal revised; aupril
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Coronary Artery Calcium. Vimal Ramjee, MD FACC The Chattanooga Heart Institute
 Coronary Artery Calcium Vimal Ramjee, MD FACC The Chattanooga Heart Institute Disclosures I have no conflicts of interest to disclose. Objectives Recognize the utility of coronary artery calcium scoring
Coronary Artery Calcium Vimal Ramjee, MD FACC The Chattanooga Heart Institute Disclosures I have no conflicts of interest to disclose. Objectives Recognize the utility of coronary artery calcium scoring
Theoretical and practical questions in the evaluation of arterial function Miklós Illyés MD. Ph.D.
 Theoretical and practical questions in the evaluation of arterial function Miklós Illyés MD. Ph.D. TensioMed Arterial Stiffness Centre, Budapest Heart Institute, Faculty of Medicine, University of Pécs
Theoretical and practical questions in the evaluation of arterial function Miklós Illyés MD. Ph.D. TensioMed Arterial Stiffness Centre, Budapest Heart Institute, Faculty of Medicine, University of Pécs
Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients. Copyright. Not for Sale or Commercial Distribution
 CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
DYSLIPIDEMIA RECOMMENDATIONS
 DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
surtout qui n est PAS à risque?
 3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
PATIENTS AND METHODS:
 BACKGROUND: Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease characterized by erosive synovitis that involves peripheral joints and implicates an important influence in the quality
BACKGROUND: Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease characterized by erosive synovitis that involves peripheral joints and implicates an important influence in the quality
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
MEDICAL POLICY SUBJECT: CORONARY CALCIUM SCORING
 MEDICAL POLICY PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
Prevention of non-communicable diseases as a prerequisite for reducing mortality in the country
 Prevention of non-communicable diseases as a prerequisite for reducing mortality in the country Boytsov S.A. National Research Center for Preventive Medicine, Moscow 1970 1971 1972 1973 1974 1975 1976
Prevention of non-communicable diseases as a prerequisite for reducing mortality in the country Boytsov S.A. National Research Center for Preventive Medicine, Moscow 1970 1971 1972 1973 1974 1975 1976
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY
 THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
A study of brachial artery flow mediated dilatation and carotid intima media thickness in subjects having risk factors for coronary artery disease
 International Journal of Advances in Medicine http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20171037 A study of brachial
International Journal of Advances in Medicine http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20171037 A study of brachial
SCAPIS. Swedish CArdioPulmonary BioImage Study. SCAPIS outline. one of the largest cardiopulmonary research programs in Sweden
 SCAPIS Swedish CArdioPulmonary BioImage Study one of the largest cardiopulmonary research programs in Sweden SCAPIS outline Identification of vulnerable plaques CTA Ultrasound (carotid artery) MRI (carotid
SCAPIS Swedish CArdioPulmonary BioImage Study one of the largest cardiopulmonary research programs in Sweden SCAPIS outline Identification of vulnerable plaques CTA Ultrasound (carotid artery) MRI (carotid
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
The Metabolic Syndrome Update The Metabolic Syndrome Update. Global Cardiometabolic Risk
 The Metabolic Syndrome Update 2018 Marc Cornier, M.D. Professor of Medicine Division of Endocrinology, Metabolism & Diabetes Anschutz Health and Wellness Center University of Colorado School of Medicine
The Metabolic Syndrome Update 2018 Marc Cornier, M.D. Professor of Medicine Division of Endocrinology, Metabolism & Diabetes Anschutz Health and Wellness Center University of Colorado School of Medicine
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
Dyslipidaemia. Is there any new information? Dr. A.R.M. Saifuddin Ekram
 Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
CARDIOMETABOLIC SYNDROME
 CARDIOMETABOLIC SYNDROME Prof. Gerald Yonga FESC, FACC Dept of Medicine, Aga Khan University East Africa Introduction Years after the term metabolic syndrome was first coined, controversy continues over
CARDIOMETABOLIC SYNDROME Prof. Gerald Yonga FESC, FACC Dept of Medicine, Aga Khan University East Africa Introduction Years after the term metabolic syndrome was first coined, controversy continues over
CRP and fibrinogen imply clinical outcome of patients with type-2 diabetes. and coronary artery disease
 CRP and fibrinogen imply clinical outcome of patients with type-2 diabetes and coronary artery disease Marijan Bosevski 1, *, Golubinka Bosevska 1, Lily Stojanovska 2, Vasso Apostolopoulos 2, * 1 University
CRP and fibrinogen imply clinical outcome of patients with type-2 diabetes and coronary artery disease Marijan Bosevski 1, *, Golubinka Bosevska 1, Lily Stojanovska 2, Vasso Apostolopoulos 2, * 1 University
CardioHealth Station. powered by. Healthcare CardioHealth
 CardioHealth Station FDA cleared, in-office ultrasound imaging that helps you directly identify atherosclerotic cardiovascular disease (ASCVD) allowing you to make a more informed decision about your patients
CardioHealth Station FDA cleared, in-office ultrasound imaging that helps you directly identify atherosclerotic cardiovascular disease (ASCVD) allowing you to make a more informed decision about your patients
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Spotty Calcification as a Marker of Accelerated Progression of Coronary Atherosclerosis : Insights from Serial Intravascular Ultrasound
 Spotty Calcification as a Marker of Accelerated Progression of Coronary Atherosclerosis : Insights from Serial Intravascular Ultrasound Department of Cardiovascular Medicine Heart and Vascular Institute
Spotty Calcification as a Marker of Accelerated Progression of Coronary Atherosclerosis : Insights from Serial Intravascular Ultrasound Department of Cardiovascular Medicine Heart and Vascular Institute
Clinical Trial Synopsis TL-OPI-518, NCT#
 Clinical Trial Synopsis, NCT# 00225264 Title of Study: A Double-Blind, Randomized, Comparator-Controlled Study in Subjects With Type 2 Diabetes Mellitus Comparing the Effects of Pioglitazone HCl vs Glimepiride
Clinical Trial Synopsis, NCT# 00225264 Title of Study: A Double-Blind, Randomized, Comparator-Controlled Study in Subjects With Type 2 Diabetes Mellitus Comparing the Effects of Pioglitazone HCl vs Glimepiride
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies
 1. Evidence from genetic, epidemiologic and clinical studies") Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
How to detect early atherosclerosis ; focusing on techniques
 How to detect early atherosclerosis ; focusing on techniques Jang-Ho Bae, MD., PhD. Heart Center Konyang University Hospital Daejeon city, S. Korea Surrogates for Atherosclerosis Measures of endothelial
How to detect early atherosclerosis ; focusing on techniques Jang-Ho Bae, MD., PhD. Heart Center Konyang University Hospital Daejeon city, S. Korea Surrogates for Atherosclerosis Measures of endothelial
Endothelial function is impaired in women who had pre-eclampsia
 Endothelial function is impaired in women who had pre-eclampsia Christian Delles, Catriona E Brown, Joanne Flynn, David M Carty Institute of Cardiovascular and Medical Sciences University of Glasgow United
Endothelial function is impaired in women who had pre-eclampsia Christian Delles, Catriona E Brown, Joanne Flynn, David M Carty Institute of Cardiovascular and Medical Sciences University of Glasgow United
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
MOHAMMED R. ESSOP DIVISION OF CARDIOLOGY CH-BARAGWANATH HOSPITAL
 MOHAMMED R. ESSOP DIVISION OF CARDIOLOGY CH-BARAGWANATH HOSPITAL DEFINITION OF A SCREENING TEST TESTING FOR A DISEASE OR CONDITION IN ASYMPTOMATIC PERSONS TO IDENTIFY THE CONDITION BEFORE IT MANIFESTS
MOHAMMED R. ESSOP DIVISION OF CARDIOLOGY CH-BARAGWANATH HOSPITAL DEFINITION OF A SCREENING TEST TESTING FOR A DISEASE OR CONDITION IN ASYMPTOMATIC PERSONS TO IDENTIFY THE CONDITION BEFORE IT MANIFESTS
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu Indicator area: Pulse rhythm assessment for AF Indicator: NM146 Date: June 2017 Introduction There is evidence
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu Indicator area: Pulse rhythm assessment for AF Indicator: NM146 Date: June 2017 Introduction There is evidence
Put your Heart before your Head
 Put your Heart before your Head Alok K Gupta, MD, FAAFP, FASH Associate Professor, Outpatient Clinic since 1963, the US Congress has required the President to proclaim February "American Heart Month."
Put your Heart before your Head Alok K Gupta, MD, FAAFP, FASH Associate Professor, Outpatient Clinic since 1963, the US Congress has required the President to proclaim February "American Heart Month."
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Coronary artery disease (CAD) risk factors
 risk factors") Background Coronary artery disease (CAD) risk factors CAD Risk factors Hypertension Insulin resistance /diabetes Dyslipidemia Smoking /Obesity Male gender/ Old age Atherosclerosis Arterial stiffness precedes
Background Coronary artery disease (CAD) risk factors CAD Risk factors Hypertension Insulin resistance /diabetes Dyslipidemia Smoking /Obesity Male gender/ Old age Atherosclerosis Arterial stiffness precedes
2/20/2013. Why use imaging in CV prevention? Update on coronary CTA in 2013 Coronary CTA for 1 0 prevention: pros and cons Are we there yet?
 Evolving Role of Coronary CTA in Primary Cardiovascular Disease Prevention: Are We There Yet? Ron Blankstein, M.D., F.A.C.C. Co-Director, Cardiovascular Imaging Training Program Associate Physician, Preventive
Evolving Role of Coronary CTA in Primary Cardiovascular Disease Prevention: Are We There Yet? Ron Blankstein, M.D., F.A.C.C. Co-Director, Cardiovascular Imaging Training Program Associate Physician, Preventive
Total risk management of Cardiovascular diseases Nobuhiro Yamada
 Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
New Paradigms in Predicting CVD Risk
 New Paradigms in Predicting CVD Risk Imaging as an Integrator of Lifetime Risk Exposure Michael J. Blaha MD MPH Presented by: Michael J. Blaha September 24, 2014 1 Talk Outline Risk factors vs. Disease
New Paradigms in Predicting CVD Risk Imaging as an Integrator of Lifetime Risk Exposure Michael J. Blaha MD MPH Presented by: Michael J. Blaha September 24, 2014 1 Talk Outline Risk factors vs. Disease
KEY COMPONENTS. Metabolic Risk Cardiovascular Risk Vascular Inflammation Markers
 CardioMetabolic Risk Poor blood sugar regulation and unhealthy triglyceride and lipoprotein levels often present long before the diagnosis of type 2 Diabetes. SpectraCell s CardioMetabolic and Pre-Diabetes
CardioMetabolic Risk Poor blood sugar regulation and unhealthy triglyceride and lipoprotein levels often present long before the diagnosis of type 2 Diabetes. SpectraCell s CardioMetabolic and Pre-Diabetes
CARDIOVASCULAR DISEASE RISK TESTS
 CARDIOVASCULAR DISEASE RISK TESTS UnitedHealthcare Oxford Clinical Policy Policy Number: CARDIOLOGY 023.11 T2 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 APPLICABLE
CARDIOVASCULAR DISEASE RISK TESTS UnitedHealthcare Oxford Clinical Policy Policy Number: CARDIOLOGY 023.11 T2 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 APPLICABLE
Lupus as a risk factor for cardiovascular disease
 Lupus as a risk factor for cardiovascular disease SØREN JACOBSEN Department Rheumatology, Rigshospitalet Søren Jacobsen Main sponsors: Gigtforeningen Novo Nordisk Fonden Rigshospitalet Disclaimer: Novo
Lupus as a risk factor for cardiovascular disease SØREN JACOBSEN Department Rheumatology, Rigshospitalet Søren Jacobsen Main sponsors: Gigtforeningen Novo Nordisk Fonden Rigshospitalet Disclaimer: Novo
Landmesser U et al. Eur Heart J 2017; https://doi.org/ /eurheartj/ehx549
 2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
MPS and Calcium Score in asymptomatic patient F. Mut, J. Vitola
 MPS and Calcium Score in asymptomatic patient F. Mut, J. Vitola Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Quanta Diagnostico Nuclear Curitiba, Brazil Clinical history Male 63 y.o.,
MPS and Calcium Score in asymptomatic patient F. Mut, J. Vitola Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Quanta Diagnostico Nuclear Curitiba, Brazil Clinical history Male 63 y.o.,
Familial hypercholesterolaemia in children and adolescents
 Familial hypercholesterolaemia in children and adolescents Rationale and recommendations for early identification and treatment European Atherosclerosis Society Consensus Panel Slide deck adapted from:
Familial hypercholesterolaemia in children and adolescents Rationale and recommendations for early identification and treatment European Atherosclerosis Society Consensus Panel Slide deck adapted from:
Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY
 MCC-006 POST GRADUATE DIPLOMA IN CLINICAL CARDIOLOGY (PGDCC) 00269 Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY Time : 2 hours Maximum Marks : 60 Note : There will be multiple
MCC-006 POST GRADUATE DIPLOMA IN CLINICAL CARDIOLOGY (PGDCC) 00269 Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY Time : 2 hours Maximum Marks : 60 Note : There will be multiple
Autonomic nervous system, inflammation and preclinical carotid atherosclerosis in depressed subjects with coronary risk factors
 Autonomic nervous system, inflammation and preclinical carotid atherosclerosis in depressed subjects with coronary risk factors Carmine Pizzi 1 ; Lamberto Manzoli 2, Stefano Mancini 3 ; Gigliola Bedetti
Autonomic nervous system, inflammation and preclinical carotid atherosclerosis in depressed subjects with coronary risk factors Carmine Pizzi 1 ; Lamberto Manzoli 2, Stefano Mancini 3 ; Gigliola Bedetti
Η σημασία της αρτηριακής σκληρίας στην εκτίμηση της διαστολικής δυσλειτουργίας στην υπέρταση. Θεραπευτικές παρεμβάσεις
 Η σημασία της αρτηριακής σκληρίας στην εκτίμηση της διαστολικής δυσλειτουργίας στην υπέρταση. Θεραπευτικές παρεμβάσεις Ελένη Τριανταφυλλίδη Επιμελήτρια Α Β Πανεπιστημιακή Καρδιολογική Κλινική Αττικό Νοσοκομείο
Η σημασία της αρτηριακής σκληρίας στην εκτίμηση της διαστολικής δυσλειτουργίας στην υπέρταση. Θεραπευτικές παρεμβάσεις Ελένη Τριανταφυλλίδη Επιμελήτρια Α Β Πανεπιστημιακή Καρδιολογική Κλινική Αττικό Νοσοκομείο
Guidelines on cardiovascular risk assessment and management
 European Heart Journal Supplements (2005) 7 (Supplement L), L5 L10 doi:10.1093/eurheartj/sui079 Guidelines on cardiovascular risk assessment and management David A. Wood 1,2 * 1 Cardiovascular Medicine
European Heart Journal Supplements (2005) 7 (Supplement L), L5 L10 doi:10.1093/eurheartj/sui079 Guidelines on cardiovascular risk assessment and management David A. Wood 1,2 * 1 Cardiovascular Medicine
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Imaging Biomarkers: utilisation for the purposes of registration. EMEA-EFPIA Workshop on Biomarkers 15 December 2006
 Imaging Biomarkers: utilisation for the purposes of registration EMEA-EFPIA Workshop on Biomarkers 15 December 2006 Vascular Imaging Technologies Carotid Ultrasound-IMT IVUS-PAV QCA-% stenosis 2 ICH E
Imaging Biomarkers: utilisation for the purposes of registration EMEA-EFPIA Workshop on Biomarkers 15 December 2006 Vascular Imaging Technologies Carotid Ultrasound-IMT IVUS-PAV QCA-% stenosis 2 ICH E
HDL and Arterial Wall
 JIFA January 31th 2014 HDL and Arterial Wall P-J TOUBOUL INSERM698 Bichat University Conflict of Interest M Ath intellectual property owner Involvement in R & D for atherosclerosis software developments
JIFA January 31th 2014 HDL and Arterial Wall P-J TOUBOUL INSERM698 Bichat University Conflict of Interest M Ath intellectual property owner Involvement in R & D for atherosclerosis software developments
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines
 Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Diabetes and Heart Disease. Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center
 Diabetes and Heart Disease Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center No conflicts of interest or financial relationships to disclose. 2 What s the problem??
Diabetes and Heart Disease Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center No conflicts of interest or financial relationships to disclose. 2 What s the problem??
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Cardiac CT Angiography
 Cardiac CT Angiography Dr James Chafey, Radiologist Why do we need a better test for C.A.D? 1. CAD is the leading cause of death in the US CAD 31% Cancer 23% Stroke 7% 2. The prevalence of atherosclerosis
Cardiac CT Angiography Dr James Chafey, Radiologist Why do we need a better test for C.A.D? 1. CAD is the leading cause of death in the US CAD 31% Cancer 23% Stroke 7% 2. The prevalence of atherosclerosis
2013 Lipid Guidelines Practical Approach. Edward Goldenberg, MD FACC,FACP, FNLA Medical Director of Cardiovascular Prevention CCHS
 2013 Lipid Guidelines Practical Approach Edward Goldenberg, MD FACC,FACP, FNLA Medical Director of Cardiovascular Prevention CCHS EVIDENCE BASED MEDICINE Case #1 - LB 42 yo Asian/American female who was
2013 Lipid Guidelines Practical Approach Edward Goldenberg, MD FACC,FACP, FNLA Medical Director of Cardiovascular Prevention CCHS EVIDENCE BASED MEDICINE Case #1 - LB 42 yo Asian/American female who was
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Role of imaging in risk assessment models: the example of CIMT
 Role of imaging in risk assessment models: the example of CIMT Diederick E. Grobbee, MD, PhD, FESC Professor of Clinical Epidemiology Julius Center for Health Sciences and Primary Care, University Medical
Role of imaging in risk assessment models: the example of CIMT Diederick E. Grobbee, MD, PhD, FESC Professor of Clinical Epidemiology Julius Center for Health Sciences and Primary Care, University Medical
Prof. John Chapman, MD, PhD, DSc
 Prof. John Chapman, MD, PhD, DSc Director of the Dyslipidemia and Atherosclerosis Research Unit of the National Institute for Health and Medical Research (INSERM) at the Pitié-Salpétrière Hospital in Paris
Prof. John Chapman, MD, PhD, DSc Director of the Dyslipidemia and Atherosclerosis Research Unit of the National Institute for Health and Medical Research (INSERM) at the Pitié-Salpétrière Hospital in Paris
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
A: Epidemiology update. Evidence that LDL-C and CRP identify different high-risk groups
 A: Epidemiology update Evidence that LDL-C and CRP identify different high-risk groups Women (n = 27,939; mean age 54.7 years) who were free of symptomatic cardiovascular (CV) disease at baseline were
A: Epidemiology update Evidence that LDL-C and CRP identify different high-risk groups Women (n = 27,939; mean age 54.7 years) who were free of symptomatic cardiovascular (CV) disease at baseline were
Diabetes and Concomitant Cardiovascular Disease: Guideline Recommendations and Future Directions
 Diabetes and Concomitant Cardiovascular Disease: Guideline Recommendations and Future Directions Diabetes is one of the largest global health emergencies of 21 st century, with the number of people with
Diabetes and Concomitant Cardiovascular Disease: Guideline Recommendations and Future Directions Diabetes is one of the largest global health emergencies of 21 st century, with the number of people with
MEDICAL POLICY. 02/15/18 CATEGORY: Technology Assessment
 MEDICAL POLICY SUBJECT: CORONARY CALCIUM SCORING PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including
MEDICAL POLICY SUBJECT: CORONARY CALCIUM SCORING PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including
The Efficacy and Safety of Statins in the Primary Prevention of Cardiovascular Disease
 University of North Dakota UND Scholarly Commons Physician Assistant Scholarly Project Papers Department of Physician Studies 2018 The Efficacy and Safety of Statins in the Primary Prevention of Cardiovascular
University of North Dakota UND Scholarly Commons Physician Assistant Scholarly Project Papers Department of Physician Studies 2018 The Efficacy and Safety of Statins in the Primary Prevention of Cardiovascular
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Coronary Artery Calcium Scoring Mirvat Alasnag FACP, FRCP, FSCCT, FSCAI, FASE King Fahd Armed Forces Hospital, Jeddah. March 2017
 Coronary Artery Calcium Scoring Mirvat Alasnag FACP, FRCP, FSCCT, FSCAI, FASE King Fahd Armed Forces Hospital, Jeddah March 2017 Newspapers Referrals 62 year old female CT chest and abdomen following
Coronary Artery Calcium Scoring Mirvat Alasnag FACP, FRCP, FSCCT, FSCAI, FASE King Fahd Armed Forces Hospital, Jeddah March 2017 Newspapers Referrals 62 year old female CT chest and abdomen following