Diabetes and thyroid disorders in clinical practice today
|
|
|
- Lorena Newton
- 6 years ago
- Views:
Transcription
1 St Petersburg, Russia - April 25, 2015 Diabetes and thyroid disorders in clinical practice today IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION


2 Paolo Pozzilli Dept. Endocrinology and Diabetes, University Campus Bio-Medico of Rome, Italy Centre of Diabetes, St. Bartholomew's and The London School of Medicine Queen Mary University of London, UK Declared receipt of grants and contracts; honoraria or consultation fees.
3 St Petersburg, Russia - April 25, 2015 Type 2 diabetes, metabolic syndrome and thyroid diseases IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION
4 Highlights in Type 2 diabetes Metabolic syndrome Thyroid diseases
5 Obesity Trends* Among U.S. Adults BRFSS, 1991 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19%
6 Obesity Trends* Among U.S. Adults BRFSS, 1992 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19%
7 Obesity Trends* Among U.S. Adults BRFSS, 1993 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19%
8 Obesity Trends* Among U.S. Adults BRFSS, 1994 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19%
9 Obesity Trends* Among U.S. Adults BRFSS, 1995 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19%
10 Obesity Trends* Among U.S. Adults BRFSS, 1996 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19%
11 Obesity Trends* Among U.S. Adults BRFSS, 1997 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19% 20%
12 Obesity Trends* Among U.S. Adults BRFSS, 1998 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19% 20%
13 Obesity Trends* Among U.S. Adults BRFSS, 1999 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19% 20%
14 Obesity Trends* Among U.S. Adults BRFSS, 2000 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19% 20%
15 Obesity Trends* Among U.S. Adults BRFSS, 2001 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14 15% 19% 20% 24% 25%
16 Obesity Trends* Among U.S. Adults BRFSS, 2002 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14 15% 19% 20% 24% 25%
17 Obesity Trends* Among U.S. Adults BRFSS, 2003 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14 15% 19% 20% 24% 25%
18 Obesity Trends* Among U.S. Adults BRFSS, 2004 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14 15% 19% 20% 24% 25%
19 Obesity Trends* Among U.S. Adults BRFSS, 2005 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19% 20% 24% 25% 29% 30%
20 Obesity Trends* Among U.S. Adults BRFSS, 2006 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19% 20% 24% 25% 29% 30%
21 Obesity Trends* Among U.S. Adults BRFSS, 2007 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19% 20% 24% 25% 29% 30%
22 Obesity Trends* Among U.S. Adults BRFSS, 2008 (*BMI 30, or ~ 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19% 20% 24% 25% 29% 30%
23 Prevalence of Self-Reported Obesity Among Non- Hispanic White Adults,by State, BRFSS, % Data not reported* 15% <20% 20% <25% 25% <30% 30% <35% * Sample size <50 or the relative standard error (dividing the standard error by the prevalence) 30%.
24 Prevalence of Self-Reported Obesity Among Hispanic A by State, BRFSS, % Data not reported* 15% <20% 20% <25% 25% <30% 30% <35% * Sample size <50 or the relative standard error (dividing the standard error by the prevalence) 30%.
25 Prevalence of Self-Reported Obesity Among Non-Hispa Black Adults, by State, BRFSS, % Data not reported* 15% <20% 20% <25% 25% <30% 30% <35% * Sample size <50 or the relative standard error (dividing the standard error by the prevalence) 30%.
26 Factor structure of the metabolic syndrom Insulin Resistance Fasting Insulin Fasting Glucose Obesity Body Mass Index Waist/Hip Ratio Lipids HDL Cholesterol Triglycerides Blood pressure Systolic BP Diastolic BP Adapted from Shen et al. Am J Epidemiol, 157: , 2003

27 Genetic factors Tessuto Visceral adiposo sottocutaneo adipose tissue FFA TNF- PAI-1 ILs Insulin resistance Environmental factors Glucose uptake Gluconeogenesis VLDL syntesis Hypertriglyceridemia Hyperglycemia Hyperinsulinemia



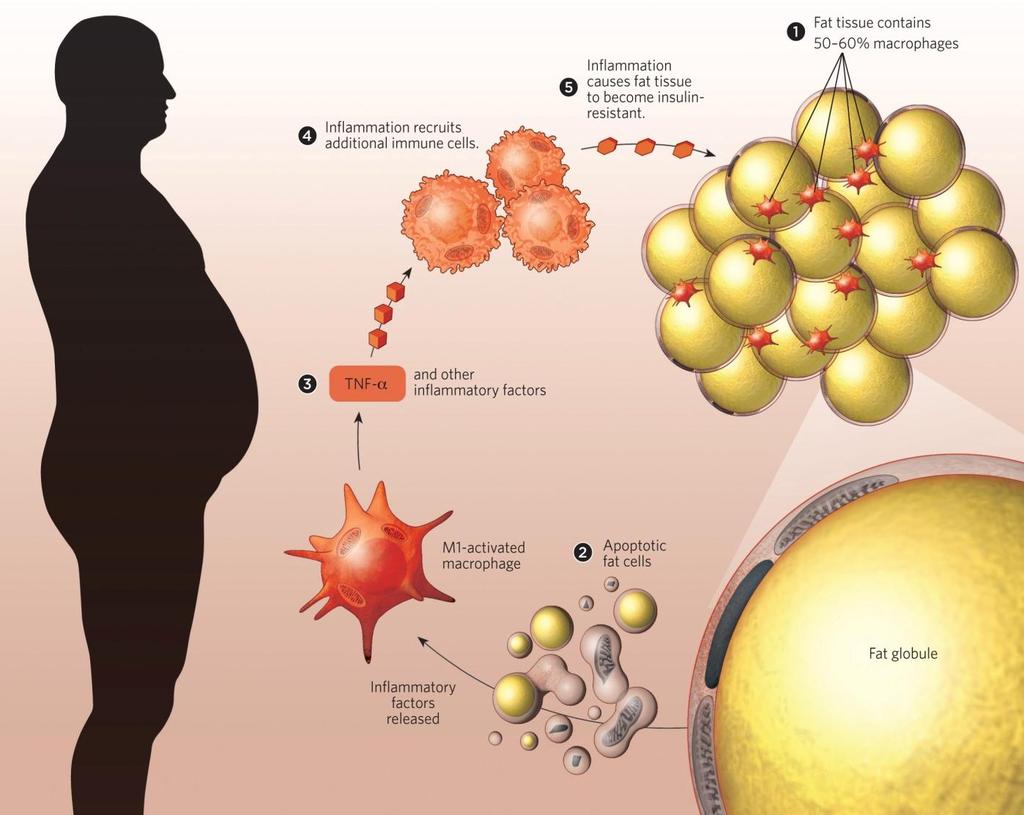

28 Insulin resistance Adipose tissue FFA
29 Relationship between visceral fat and insulin sensitivity Total glucose (mmol/min/kg FFM) Bonora E et al, Ital Cardiol, r = p< Visceral fat amount (cm 2 )

 gender; 2)")

30 The variability of waist circumference Fox K et al., Int J Obes Relat Metab Disord, 1993 Waist circumference is subject to interoperator variability and is influenced by: 1) gender; 2) race or ethnicity Waist circumference explains only 25% to 50% of the variation in intra-abdominal adipose tissue.



31 The study findings suggest a close relationship among wrist circumference, its bone component, and insulin resistance in overweight/obese children and adolescents, opening new perspectives in the prediction of cardiovascular disease. Buzzetti R. et al., Circulation, 2011




32 Wrist circumference as a predictor of T2D Incidence of diabetes during 8.8 years of follow-up ( Noudeh et al. JCEM 2013)

33 Type 2 diabetes and personalized therapy






34 T2DM is a COMPLEX disease with a COMPLEX therapy! Detemir Glargine Degludec U 300 Lispro Aspart Glulisine Regular human Biosimilar insulin INSULIN Glicazide Glibenclamide Glimepiride Glyburide SULFONYLUREAS Pioglitazone TZDs Nateglinide Repaglinide Metformin GLINIDES BIGUANIDES Sitagliptin Saxagliptin Vildagliptin Linagliptin Alogliptin DPP-IV INHIBITORS Exenatide Exenatide LAR Liraglutide Lixisenatide Dulaglutide LAR Albiglutide LAR Senaglutide INCRETINS Acarbose Miglitol ALPHA GLUCOSIDASES INHIBITORS Dapagliflozin Ertugliflozin Canagliflozin Empagliflozin Sotagliflozin SGLT2 INHIBITORS
 CARMELINA (n estimated=8.300) CAROLINA (n estimated=6.")
 TECOS (n=14.")
35 DPP-4I and cardiovascular outcomes NCT (n= 5.000) CARMELINA (n estimated=8.300) CAROLINA (n estimated=6.000) SAVOR TIMI 53 (n=18.206) EXAMINE (n= 5.380) TECOS (n=14.000) Clinicaltrials.gov
 EXSCEL (n estimated= 14.000) LEADER (n=9.")
36 GLP-1A and cardiovascular outcomes SUSTAIN 6 (n=3.297) REWIND (n estimated=9.622) ELIXA (n=6.075) EXSCEL (n estimated= ) LEADER (n=9.340) Clinicaltrials.gov
 EMPA REG (n= 7.")
 CANVAS (n estimated= 4.")
37 SGLT-2 and cardiovascular outcomes MK (n estimated=3.900) EMPA REG (n= 7.000) DECLARE TIMI (n estimated=17.150) CANVAS (n estimated= 4.365) Clinicaltrials.gov
 - + - + - + <6 <6.5 <6.5 6.")
:239-44.")
38 The A1C and ABCD(E)* of glycaemia management in type 2 diabetes: a physician's personalized approach AGE (years) >70 COMPLICATIONS DURATION>10yrs HbA1c (%) <6 <6.5 < <7 7-8 HbA1c 9% Insulin treatment HbA1c< 9% METFORMIN Physicia n should choose drug a ccording to pa tie nt's risk of w e ight ga in, hypoglyca e mia, ca rdio-re na l complica tions Pozzilli P, Leslie RD, Chan J, De Fronzo R, Monnier L, Raz I, Del Prato S. Diabetes Metab Res Rev May;26(4): *Khazrai YM, Buzzetti R, Del Prato S, Cahn A, Raz I, Pozzilli P. J Diabetes Complications Mar 11. pii: S1056-





39 ADA/EASD position statement 2015 Towards personalized glycaemic targets Diabetes Care, Volume 38, supplement 1, January 2015




40 Maddaloni E.& Pozzilli P. Endocrine, January 2014 The «SMART» diabetologist afety Primum non nocere The challenge for diabetologist is to choose the best safe approach with concerns to potential adverse effects and benefits of intensive glucose control. ultifactorial pproach isk herapy In diabetic patients relevant cardiovascular risk factors other than hyperglycaemia always coexist. There is a universal agreement that anti-hyperglycaemic therapy should be pursued within a multifactorial risk reduction framework A careful evaluation of the risk reduction that could really be achieved should always be performed. However the risk of macrovascular complications starts to increase very early, even in the pre-diabetic stages, claiming for precocious management strategies. Therapy of diabetes is becoming increasingly complex, due to the complexity of pathophysiology and to the wide therapeutic options. A non univocal, but just a smart approach could be the key to turn therapeutic complexity from a problem into an opportunity.



41 complex human behaviour It is important that patients learn to manage and cope with their disease and gain greater control over actions and decisions affecting their health. Healthcare professionals should aim to encourage and increase patients perception about their ability to take informed decisions about disease management and to improve patient self-esteem and feeling of self-efficacy to become agents of their own health. Khazrai YM et al., JDC 2015
42 A ge B ody weight C omplications D uration of disease E mpowerment / economics Patient perspective Normal glycaemia Easy to use Safe and tolerable Immediate benefit Inexpensive Physician perspective Durability Easy to prescribe Reduce complications Long-term benefit Preserve beta-cells





43 Considerations for personalizing medicine in T2DM therapy Efficacy Cost Age Safety and tolerability Personalized Therapy Occupation Patient wishes Diabetes Duration Concomitant Diseases Body Weight The A1C and ABCD of glycaemia management in type 2 diabetes: a physician's personalized approach. Pozzilli P, Leslie RDG, Chan J, De Fronzo R, Monnier L, Raz I, Del Prato S: Diabetes Metab Res Rev 26:239-44, 2010
44 Thyroid and other diseases associated with diabetes
45 Prevalence of autoimmune thyroid and other diseases associated with type 1 diabetes Barker JM et al, JCEM, 2011; Hollowell JC, JCEM, 2012; Van den Driessche et al, J Med, 2009; Bowes J, Rheumat, 2008 T1DM (%) General population (%) Coeliac disease Hashimoto 3-8 <1 Graves disease 1 1 Addison disease < Autoimmune gastritis Pernicious anemia Multiple sclerosis Vitiligo Rheumatoid Arthritis Systemic Lupus Erithematosus
46 Prevalence autoantibodies in type 1 diabetes and in general population Barker JM et al, JCEM, 2006; Alonso N et al, Nat Rev, 2009 Autoantigen T1DM (%) General population (%) Celiac disease ttg Hashimoto TPO TG Graves'disease TRAb 5 1 Addison disease 21-OH 1-2 Rare Autoimmune gastritis APCA



47 Prevalence of organ-specific autoantibodies in NIRAD /LADA and T2D patients High titre GADA p<0.001 p<0.004 Low titre GADA T2DM p<0.03 p< p= TPO 21-OH ttg APC Zampetti S et al., J Clin Endocrinol Metab 97: , 2012

48 Conclusions Interaction between obesity, diabetes and autoimmune thyroid and other diseases is more than an association of different conditions but a pathophysiological cluster which requires precise characterization for the implementation of the most suitable therapy.
49 St Petersburg, Russia - April 25, 2015 Diabetes and thyroid disorders in clinical practice today IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Newer Therapies for Type 2 Diabetes
 Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Type 2 Diabetes Management: Case 1: Reducing Hypoglycemic Risk Case 2: Reducing Cardiovascular Risk
 Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Keep Calm and Focus on the Evidence for the Management of Diabetes. Diabetes Update 2018
 Keep Calm and Focus on the Evidence for the Management of Diabetes Diabetes Update 2018 Nicole C.Pezzino, PharmD, BCACP, CDE Assistant Professor, Wilkes University Pharmacist, Weis Markets Nicole.pezzino@wilkes.edu
Keep Calm and Focus on the Evidence for the Management of Diabetes Diabetes Update 2018 Nicole C.Pezzino, PharmD, BCACP, CDE Assistant Professor, Wilkes University Pharmacist, Weis Markets Nicole.pezzino@wilkes.edu
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Physiology of Normoglycemia
 Case 1 45 year-old male patient seen at the clinic (Medicine). Workplace stress (financial analyst); occasionally goes jogging. Two-year duration of T2DM. No previous cardiovascular events. Coexisting
Case 1 45 year-old male patient seen at the clinic (Medicine). Workplace stress (financial analyst); occasionally goes jogging. Two-year duration of T2DM. No previous cardiovascular events. Coexisting
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs
 Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
Clinical Cases in Diabetes Management. Joseph Cook D.O.
 Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Novel anti-diabetic therapies
 Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
CV outcomes Studies and Implications for diabetes management. Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH
 CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
Silvio E. Inzucchi MD Section of Endocrinology Yale School of Medicine
 Gegia Chapter of the American Association of Clinical Endocrinologists, 2017 Annual Meeting January 28, 2017 Silvio E. Inzucchi MD Section of Endocrinology Yale School of Medicine DIABETES MANAGEMENT GUIDELINES
Gegia Chapter of the American Association of Clinical Endocrinologists, 2017 Annual Meeting January 28, 2017 Silvio E. Inzucchi MD Section of Endocrinology Yale School of Medicine DIABETES MANAGEMENT GUIDELINES
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
3. Cardiovascular Disease?
 Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Clinical Guidelines. Management of adult patients with diabetes undergoing endoscopic procedures
 Clinical Guidelines Management of adult patients with diabetes undergoing endoscopic s Document Detail Document type Clinical Guideline Management of adult Patients with diabetes Undergoing Document name
Clinical Guidelines Management of adult patients with diabetes undergoing endoscopic s Document Detail Document type Clinical Guideline Management of adult Patients with diabetes Undergoing Document name
Yes! Is Type 2 diabetes the same in kids as in adults? And No! Youth-onset type 2 diabetes 5/16/2018 LEST WE THINK THIS IS NOT AN IMPORTANT PROBLEM
 Youth-onset type 2 diabetes PHIL ZEITLER MD, PHD SECTION OF ENDOCRINOLOGY DEPARTMENT OF PEDIATRICS UNIVERSITY OF COLORADO DEPARTMENT OF ENDOCRINOLOGY CHILDREN S HOSPITAL COLORADO LEST WE THINK THIS IS
Youth-onset type 2 diabetes PHIL ZEITLER MD, PHD SECTION OF ENDOCRINOLOGY DEPARTMENT OF PEDIATRICS UNIVERSITY OF COLORADO DEPARTMENT OF ENDOCRINOLOGY CHILDREN S HOSPITAL COLORADO LEST WE THINK THIS IS
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Type 2 diabetes & Cardiovascular disease. update. Barcelona, March 15th 2018
 Type 2 diabetes & Cardiovascular disease update Barcelona, March 15th 2018 Francesc Xavier Cos Claramunt Sant Martí de Provençals. Head of Innovation and Health in Barcelona city Assoc.ProfUniversitatAutonomade
Type 2 diabetes & Cardiovascular disease update Barcelona, March 15th 2018 Francesc Xavier Cos Claramunt Sant Martí de Provençals. Head of Innovation and Health in Barcelona city Assoc.ProfUniversitatAutonomade
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION
 SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
Canadian Journal of Diabetes
 Can J Diabetes 42 (2018) S88 S103 Contents lists available at ScienceDirect Canadian Journal of Diabetes journal homepage: www.canadianjournalofdiabetes.com 2018 Clinical Practice Guidelines Pharmacologic
Can J Diabetes 42 (2018) S88 S103 Contents lists available at ScienceDirect Canadian Journal of Diabetes journal homepage: www.canadianjournalofdiabetes.com 2018 Clinical Practice Guidelines Pharmacologic
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Therapeutic strategy to reduce Glucagon secretion
 Clinical focus on glucagon: α-cell as a companion of β-cell Therapeutic strategy to reduce Glucagon secretion Sunghwan Suh Dong-A University Conflict of interest disclosure None Committee of Scientific
Clinical focus on glucagon: α-cell as a companion of β-cell Therapeutic strategy to reduce Glucagon secretion Sunghwan Suh Dong-A University Conflict of interest disclosure None Committee of Scientific
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18
 Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18 No conflicts of interest Objectives for this talk Update on non-insulin drug therapy fro type 2 DM Appropriate use of insulin in type 2 DM ADA
Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18 No conflicts of interest Objectives for this talk Update on non-insulin drug therapy fro type 2 DM Appropriate use of insulin in type 2 DM ADA
2018 Diabetes Update
 2018 Diabetes Update Jennifer D. Smith, PharmD, BCACP, BC-ADM, CDE Susan Cornell, PharmD, CDE, FAPhA, FAADE Midwestern University Chicago College of Pharmacy Target Audience: Pharmacists ACPE#: 0202-0000-18-043-L01-P
2018 Diabetes Update Jennifer D. Smith, PharmD, BCACP, BC-ADM, CDE Susan Cornell, PharmD, CDE, FAPhA, FAADE Midwestern University Chicago College of Pharmacy Target Audience: Pharmacists ACPE#: 0202-0000-18-043-L01-P
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
Session 10: Drugs. GLP-1 receptor agonists
 Session 10: Drugs GLP-1 receptor agonists Dr. Manel Mata La Mina Primary Health Care Centre. Barcelona. Catalonian Institute of Health. Grup DAP_Cat, Barcelona Research Support Unit. IDIAP-Jordi Gol. CIBERDEM.
Session 10: Drugs GLP-1 receptor agonists Dr. Manel Mata La Mina Primary Health Care Centre. Barcelona. Catalonian Institute of Health. Grup DAP_Cat, Barcelona Research Support Unit. IDIAP-Jordi Gol. CIBERDEM.
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Obesity and diabetes threaten European quality of life and regional health and social care budgets
 Obesity and diabetes threaten European quality of life and regional health and social care budgets Professor Mike Lean 3rd May 2017 Type 2 Diabetes in the 21 st Century A New Treatment Paradigm Professor
Obesity and diabetes threaten European quality of life and regional health and social care budgets Professor Mike Lean 3rd May 2017 Type 2 Diabetes in the 21 st Century A New Treatment Paradigm Professor
Update on Cardiovascular Outcome Trials in Diabetes. Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013
 Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Update Diabetes Therapie. Marc Y Donath
 Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Disclosures of Interest. Publications Diabetologia Key points to emphasize
 Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Disclaimers 22/03/2018. Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2
 Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
DR. SUBHASH K. WANGNOO
 Photograph DR. SUBHASH K. WANGNOO M.D, D.M, FRCP (London) Senior Consultant, Endocrinologist & Diabetologist Apollo Centre for Obesity, Diabetes and Endocrinology Indraprastha Apollo Hospital, Sarita Vihar,
Photograph DR. SUBHASH K. WANGNOO M.D, D.M, FRCP (London) Senior Consultant, Endocrinologist & Diabetologist Apollo Centre for Obesity, Diabetes and Endocrinology Indraprastha Apollo Hospital, Sarita Vihar,
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Diabetes and Heart Failure: The Role of SGLT2 Inhibitors
 22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Diabetes Mellitus case studies. Jana Vinklerová
 Diabetes Mellitus case studies Jana Vinklerová Definition of diabetes (metabolic disorder) Chronically raised blood glucose (hyperglycaemia) Insulin/Glucagon Insulin is responsible for lowering glucose
Diabetes Mellitus case studies Jana Vinklerová Definition of diabetes (metabolic disorder) Chronically raised blood glucose (hyperglycaemia) Insulin/Glucagon Insulin is responsible for lowering glucose
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
New Measure Recommended for Endorsement by PQA
 New Measure Recommended for Endorsement by PQA Measure: Statin Use in Persons with Diabetes Description: The percentage of patients ages 40 75 years who were dispensed a medication for diabetes that receive
New Measure Recommended for Endorsement by PQA Measure: Statin Use in Persons with Diabetes Description: The percentage of patients ages 40 75 years who were dispensed a medication for diabetes that receive
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
Diabetes mellitus. Treatment
 Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
Joslin Diabetes Center Management of Diabetes in 2013: The Need to Combine Art and Science Weight Management in the Patient With Diabetes
 Long-term Weight Management in Patients With Diabetes: The Why WAIT Model Osama Hamdy, MD, PhD, FACE Medical Director, Obesity Clinical Program Director of Inpatient Diabetes Management Joslin Diabetes
Long-term Weight Management in Patients With Diabetes: The Why WAIT Model Osama Hamdy, MD, PhD, FACE Medical Director, Obesity Clinical Program Director of Inpatient Diabetes Management Joslin Diabetes
Evaluating the Cardiovascular Benefits of Antidiabetic Medications
 Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
ANTIDIABETIC THERAPY 2018: PHARMACOLOGIC OPTIONS. Andrew Reikes, MD, FACE Clinical Professor of Medicine UC Irvine School of Medicine
 ANTIDIABETIC THERAPY 2018: PHARMACOLOGIC OPTIONS Andrew Reikes, MD, FACE Clinical Professor of Medicine UC Irvine School of Medicine Disclosure Spouse works for GlaxoSmithKline as recruiter and owns GSK
ANTIDIABETIC THERAPY 2018: PHARMACOLOGIC OPTIONS Andrew Reikes, MD, FACE Clinical Professor of Medicine UC Irvine School of Medicine Disclosure Spouse works for GlaxoSmithKline as recruiter and owns GSK
Individualizing Management of T2DM in the Hospital Setting to Reduce Macro and Microvascular Complications
 Individualizing Management of T2DM in the Hospital Setting to Reduce Macro and Microvascular Complications This CME activity is provided by Integrity Continuing Education. This CEU/CNE activity is co-provided
Individualizing Management of T2DM in the Hospital Setting to Reduce Macro and Microvascular Complications This CME activity is provided by Integrity Continuing Education. This CEU/CNE activity is co-provided
Michael Mansfield Consultant Leeds Teaching Hospitals
 Easing, fixing and avoiding diabetic hyperglycaemia: new drugs, new approaches Michael Mansfield Consultant Leeds Teaching Hospitals Declaration: no significant gifts, fees, funding from pharma Topics:
Easing, fixing and avoiding diabetic hyperglycaemia: new drugs, new approaches Michael Mansfield Consultant Leeds Teaching Hospitals Declaration: no significant gifts, fees, funding from pharma Topics:
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Noninsulin Treatment of Diabetes: What the PCP Needs to Know
 Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
COPYRIGHT. Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely?
 Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018
 GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
Diabetes Management: A diagnostic perspective
 Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Halting the Rise, Newest Non- Insulin Options for Lowering A1c
 Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure?
 UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
CANA DAPA EMPA. Change in Baseline Body Weight (kg) *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg, EMPA=10 or 25 mg.
 *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg, EMPA=10 or 25 mg.") CANA DAPA EMPA Change in Baseline Body Weight (kg) 2 1 0-1 -2-3 -4-5 PBO SGLT2 inhibitor (low dose)* SGLT2 inhibitor (high dose)* *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg,
CANA DAPA EMPA Change in Baseline Body Weight (kg) 2 1 0-1 -2-3 -4-5 PBO SGLT2 inhibitor (low dose)* SGLT2 inhibitor (high dose)* *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg,
Halting the Rise, Newest Non- Insulin Options for Lowering A1c
 Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
razionale della combinazione insulina/glp-1 RAs
 Insulina e GLP-1 RAS: insieme o separati? razionale della combinazione insulina/glp-1 RAs Catania Mercure Catania Excelsior 10 ottobre 2017 Andrea Giaccari andrea.giaccari@unicatt.it Centro per le Malattie
Insulina e GLP-1 RAS: insieme o separati? razionale della combinazione insulina/glp-1 RAs Catania Mercure Catania Excelsior 10 ottobre 2017 Andrea Giaccari andrea.giaccari@unicatt.it Centro per le Malattie
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
La lezione dei trials di safety cardiovascolare. Edoardo Mannucci
 La lezione dei trials di safety cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer
La lezione dei trials di safety cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer
Diabetes management in liver and kidney disease
 Diabetes management in liver and kidney disease Epidemiology 1 Clinical case A 59 year old man with alcoholic cirrhosis; portal hypertension; mild encephalopathy Fasting plasma glucose - 103, March 2016;
Diabetes management in liver and kidney disease Epidemiology 1 Clinical case A 59 year old man with alcoholic cirrhosis; portal hypertension; mild encephalopathy Fasting plasma glucose - 103, March 2016;
Jeopardy: Update on Diabetes Pharmacotherapy
 Jeopardy: Update on Diabetes Pharmacotherapy Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Objectives Describe the mechanism of action
Jeopardy: Update on Diabetes Pharmacotherapy Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Objectives Describe the mechanism of action
Objectives. Why is Glucose Control Important? 11/2/2016. Jeopardy: Update on Diabetes Pharmacotherapy
 Jeopardy: Update on Diabetes Pharmacotherapy Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University Chicago College of Pharmacy Objectives Describe the mechanism of action
Jeopardy: Update on Diabetes Pharmacotherapy Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University Chicago College of Pharmacy Objectives Describe the mechanism of action
Drug Class Update with New Drug Evaluation: Non-insulin Diabetes Treatments (SGLT-2 Inhibitors and GLP-1 Receptor Agonists)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP
 Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Diabetes Update July 6, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period
 Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich
Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Should Psychiatrists be diagnosing (and treating) metabolic syndrome
 metabolic syndrome") Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Intensification of Diabetic Therapy. Case studies
 Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Peter Stein, MD Janssen Research and Development
 New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
New Strategies for Cardiovascular Risk reduction in Diabetes
 New Strategies for Cardiovascular Risk reduction in Diabetes Dr. Godwin LEUNG Tat Chi MB ChB(HK), MRCP (UK), FHKCP, FHKAM (Medicine) FRCP (Glasg), FACC Specialist in Cardiology % event as first CV event
New Strategies for Cardiovascular Risk reduction in Diabetes Dr. Godwin LEUNG Tat Chi MB ChB(HK), MRCP (UK), FHKCP, FHKAM (Medicine) FRCP (Glasg), FACC Specialist in Cardiology % event as first CV event
Newer Diabetes Treatments Drug Class Update with New Drug Evaluation: Semaglutide and Ertugliflozin
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight