DIFFERENTIAL DIAGNOSIS OF NEUROGENIC DISORDERS & MYOPATHIES
|
|
|
- Sherman Collins
- 6 years ago
- Views:
Transcription
1 DIFFERENTIAL DIAGNOSIS OF NEUROGENIC DISORDERS & MYOPATHIES NEUROPATHY MYOPATHY Weakness distal proximal Sensory dysfunction + 0 Loss of reflexes early late Serum enzymes +/- +++ CSF protein may be elevated normal Electromyography neurogenic myopathic
2 CLASSIFICATION OF PERIPHERAL NERVE DISEASES Myelinopathy y Acute inflammatory polyneuropathy (Guillain-Barré syndrome or GBS) Chronic inflammatory demyelinating polyneuropathy (CIDP) Charcot-Marie-Tooth, type 1 (CMT-1) Axonopathy Wallerian degeneration (trauma, vasculitis etc.) Distal axonopathies (dying back neuropathies) Neuronopathy Amyotrophic lateral sclerosis (ALS)
3 CLINICAL ROLE OF NERVE BIOPSY IS VERY LIMITED Identify the cause of a neuropathy (vasculitis, amyloidosis). Nerve conduction o studies are more useful than nerve biopsy for dis- tinguishing between a demyelinating neuropathy and an axonal disorder.
4 PATHOLOGICAL ANALYSIS OF SURAL NERVE BIOPSY ROUTINE HISTOLOGY SEMITHIN PLASTIC SECTIONS TEASED MYELINATED FIBERS ELECTRON MICROSCOPY
5 SURAL NERVE, SEMITHIN PLASTIC SECTION (TOLUIDINE BLUE)
6 TEASED MYELINATED FIBER: TEASED MYELINATED FIBER: NORMAL
7 PERIPHERAL NERVE, ELECTRON MICROGRAPH
8 SEQUENCE OF SEGMENTAL DEMYELINATION & REMYELINATION Prox. Dist. Conduction block of action po- tentials Conduction slowing
9 NERVE STIMULATION EVOKES ACTION POTENTIAL IN HAND MUSCLE J. Neurol. Neurosurg. Psychiatry 2005;76; NORMAL COMPOUND MUSCLE ACTION POTENTIAL REDUCED AMPLITUDE OF CMAP
10 TEASED MYELINATED FIBER: TEASED MYELINATED FIBER: SEGMENTAL REMYELINATION
11 SAME TEASED FIBER AT SAME TEASED FIBER AT HIGHER MAGNIFICATION
12 SEQUENCE OF SEGMENTAL AXONAL DEGENERATION & REGENERATION Proximal Distal
13 TEASED MYELINATED FIBER: AXONAL DEGENERATION
14 CLASSIFICATION OF PERIPHERAL NERVE DISEASES Myelinopathy y Acute inflammatory polyneuropathy (Guillain-Barré syndrome or GBS) Chronic inflammatory demyelinating polyneuropathy (CIDP) Charcot-Marie-Tooth, type 1 (CMT-1) Axonopathy Wallerian degeneration (trauma, vasculitis etc.) Distal axonopathies (dying back neuropathies) Neuronopathy Amyotrophic lateral sclerosis (ALS)
15 ACUTE INFLAMMATORY POLYNEUROPATHY (GUILLAIN-BARRE A SYNDROME OR GBS) Rapidly progressive neuropathy, chiefly motor, reaching maximum weakness usually within 1 to 2 weeks. Severe respiratory weakness is a major danger and may require treatment in an intensive care unit. An acute infectious illness precedes weakness in two thirds, consisting of influenza-like symptoms or diarrhea. The res- piratory disorder is linked to infection by viruses whereas diarrhea is often caused by Campylobacter jejuni. R t k k th P th di Recovery takes weeks or months. Permanent handicap occurs in 15%-20% of patients.
16 GBS: DIAGNOSIS & TREATMENT Electrophysiology: early block of conduction of action potentials along motor nerves. Slowing of conduction veloc- ity develops later as segmental remyelination appears. Electrodiagnostic studies often show evidence of co-existing axonal degeneration, usually of mild degree. Cerebrospinal fluid typically y has mildly elevated pro- tein and no cells. Sural nerve biopsy does not have a role in diagnosis but has provided information about etiology and pathogenesis. Plasmapheresis or intravenous gamma globulin speeds recovery.
17 PATHOLOGY OF GUILLAIN-BARRÉ SYNDROME Immune complexes (C3, IgG, IgM) are detectable on the surface of myelin sheaths in the early stage. Sparse T cells, chiefly CD4 subset, infiltrate endoneurium. Monocytes and macrophages appear to attack myelin shea Myelinated fibers show segmental demyelination during the first few days. Segmental remyelination occurs subsequently. The lesions have a perivenular distribution and tend to affect the DRG, nerve roots and adjacent nerves where blood nerve barrier is normally more permeable than elsewhere.
18 GBS, DORSAL ROOT GANGLION, H&E
19 GBS, MOTOR NERVE, H&E
20 GBS, MOTOR NERVE, SEMITHIN SECTION
21 GBS, ELECTRON MICROGRAPH
22 GBS, SEGMENTAL REMYELINATION
23 GBS, C3 COMPONENT ON MYELIN SHEATHS
24 EVIDENCE FOR AUTOIMMUNE ETIOLOGY IN GUILLAIN-BARRE SYNDROME Demyelinating neuropathy can be induced in experimental animals by immunization i with myelin, purified myelin protein or galactocerebroside. Antibody titers to nerve myelin in patients correlate with disease activity. The antibodies recognize specific glycolipids or glycoproteins of peripheral myelin in a minority of patients. Immune complexes are found at surface of myelin sheaths Plasmapheresis or intravenous gamma globulin speeds recovery when treatment is started early.
25 AXONAL VARIANT OF GUILLAIN- BARRE SYNDROME Clinical syndrome resembles Guillain-Barre syndrome, but is often purely motor. It is common in Asia and other countries but accounts for only 5% of patients in the US or Europe.
26 AXONAL VARIANT OF GBS, Possible molecular l mimicry i The patients often have elevated serum autoantibodies that recognize the terminal oligosaccharide of GM1 & GD1a ganglioside. The chemical structure of lipopolysaccharide of C. jejuni j has the same oligosaccharide id chain present in GD1a and GM1. This suggests that the immune response to C. jejuni induces antibodies that crossreact to a self- antigen of the axolemma. This axonal variant of t i
27 CLASSIFICATION OF PERIPHERAL NERVE DISEASES Myelinopathy y Acute inflammatory polyneuropathy (Guillain-Barré syndrome or GBS) Chronic inflammatory demyelinating polyneuropathy (CIDP) Charcot-Marie-Tooth, type 1 (CMT-1) Axonopathy Wallerian degeneration (trauma, vasculitis etc.) Distal axonopathies (dying back neuropathies) Neuronopathy Amyotrophic lateral sclerosis (ALS)
28 CHRONIC INFLAMMATORY DEMYELINAT- ING POLYNEUROPATHY (CIDP) Chronic progressive or relapsing neuropathy, motor > sensory. An antecedent infectious illness is uncommon. Electrophysiology: conduction block and slowing of velocity. Pathology: segmental demyelination and remyelination, onion bulbs, fibrosis and little or no lymphocytic infiltration of tissue. Probably an autoimmune disorder of myelin but pathogenesis is not well understood. Patients respond to plasmapheresis, intravenous gamma globulin or corticosteroid treatment.
29 ONION BULB
30 CIDP WITH ONION BULBS
31 CLASSIFICATION OF PERIPHERAL NERVE DISEASES Myelinopathy y Acute inflammatory polyneuropathy (Guillain-Barré syndrome or GBS) Chronic inflammatory demyelinating polyneuropathy (CIDP) Charcot-Marie-Tooth, type 1 (CMT-1) Axonopathy Wallerian degeneration (trauma, vasculitis etc.) Distal axonopathies (dying back neuropathies) Neuronopathy Amyotrophic lateral sclerosis (ALS)
32 CHARCOT-MARIE-TOOTH, TYPE I Slowly progressive distal limb weakness begins in first decade with great variation in onset; few sensory complaints. Autosomal dominant, mutations commonly affect PMP22. Neurological exam: Atrophy of distal leg muscles (stork leg appearance). Palpable nerve enlargement in 50%. Pes cavus and hammer toes is common. Electrophysiology: l Uniform slowing of conduction velocity. No conduction block. Pathology: similar to CIDP.
33 Lou Gehrig
34 AMYOTROPHIC LATERAL SCLEROSIS (LOU GEHRIG S DISEASE) Progressive weakness, muscle wasting and fasciculations; often asymmetrical in the beginning. Symptoms usually begin after the age of 40. Hyperactive tendon reflexes, clonus and Babinski signs. Electromyogram: Signs of denervation in muscle. Normal or slightly reduced conductions. Most are sporadic; about 10% are familial. Death occurs usually within 3 to 5 years from onset.
35 ALS: FASCICULATIONS & BABINSKY REFLEXES
36 ALS: LOWER MOTOR NEURON PATHOLOGY Loss of motor neurons in ventral horns and nuclei of cranial nerve V, VII, IX-XII. Sparing of motor nuclei of cranial nerves III, IV & VI and Onuf s nucleus. Surviving motor neurons show atrophy & inclusions. Few chromatolytic-like nerve cells. Little or no evidence of axonal regeneration.
37 ALS: LOSS OF MOTOR NEURONS IN VENTRAL HORN
38 ALS & SARCOIDOSIS, SPINAL CORD, TDP-43
39 ALS, SKEIN-LIKE INCLUSIONS, UBIQUITIN
40 SKEIN-LIKE INCLUSIONS Intracytoplasmic t aggregates of granules and loosely- arranged fibrils (skein-like inclusions) occur in motor neurons of spinal cord and brain stem. Rare in Betz motor cells of precentral gyrus. Invisible in routine histology (H&E) and are not argyrophilic. The inclusions are composed of TDP-43, a protein that is normally expressed in the nucleus. The skein-like inclusions are ubiquinated. Sensitivity: %; specificity: >95%.
41 ALS, NEUROFILAMENT PROTEIN
42 ALS: UPPER MOTOR NEURON PATHOLOGY Loss of fbetz cells (upper motor neurons) )in precentral gyrus. Pyramidal degeneration with gradually increasing myelin pallor in a caudal direction due to loss of axons. The tract degeneration is marked by macrophages (removing myelin debris) and numerous activated microglia.
43 ALS, MYELIN PALLOR IN PYRAMIDAL TRACT, LFB-PAS






44 ALS, PYRAMIDAL TRACT, CD68
45 PATHOGENESIS OF ALS Mutations of the Cu/Zn superoxide dismutase (SOD1) cause ALS of 20% of familial cases. Expression of mutant human SOD1 in transgenic mice produces MND by a toxic or gain of function mechanism. This mouse model has yielded two major hypotheses of toxicity: aberrant oxidation intracellular aggregates g glutamate toxicity disrupted glutamate toxicity, disrupted calcium homeostasis, abnormal nitration and glycation of proteins, apoptotic death
46 AIMS OF MUSCLE BIOPSY Distinguish a neurogenic disorder from a myopathy. Screen inherited it myopathies for molecular analysis. Subclassify acquired myopathies.
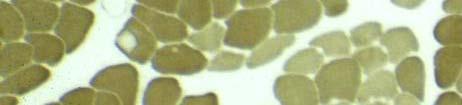
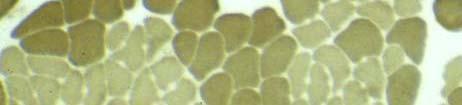
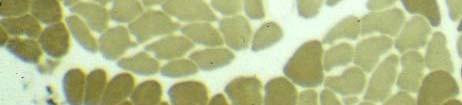
47 CRYOSECTIONS OF SKELETAL MUSCLE, H&E
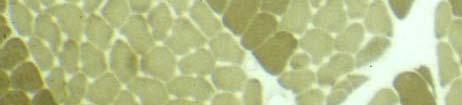
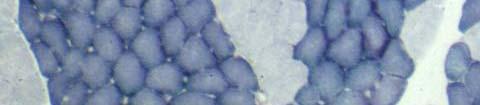
48 CRYOSECTIONS OF SKELETAL MUSCLE, ATPase
49 MODIFIED GOMORI TRICHROME SUCCINATE DE- HYDROGENASE
50 DIAGNOSTIC HISTOLOGICAL FEATURES OF A NEUROGENIC DISORDER LARGE GROUPS OF ATROPHIC FIBERS FIBER TYPE GROUPING TARGET FIBERS
51 GROUPS OF ATROPHIC MYOFIBERS, H&E




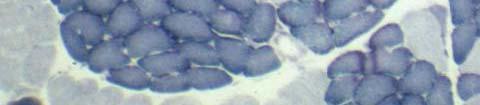
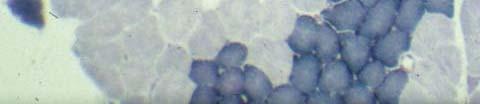
52 FIBER TYPE GROUPING NADH-DEHY- DROGENASE ATPase
53 TARGET FIBERS, NADH DEHYDROGENASE
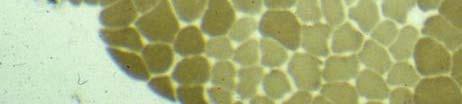
54 DIAGNOSTIC HISTOLOGICAL FEATURES OF MYOPATHIES ABSENCE OF NEUROGENIC ABNORMALITIES NECROTIC MUSCLE FIBERS BASOPHILIC (REGENERATING) MYOFIBERS FIBROSIS OF THE ENDOMYSIUM SPECIAL PATHOLOGICAL FEATURES (INFLAMMATORY SPECIAL PATHOLOGICAL FEATURES (INFLAMMATORY CELLS, RAGGED RED FIBERS ETC.)
55 NECROTIC FIBER, H&E
56 REGENERATING FIBER, H&E
57 Gowers, 1879 GOWER S SIGN
58 DUCHENNE MUSCULAR DYSTROPHY X-linked recessive inheritance Onset of weakness noticeable at 2-5 years of age. Progressive weakness, proximal>distal Hypertrophy of calves High serum creatine kinase activity Fatal in 3rd decade
59 DUCHENNE DYSTROPHY, H&E
60 DUCHENNE DYSTROPHY, LATER STAGE
61 DUCHENNE MUSCULAR DYSTROPHY Dystrophin is a 427 kd protein that binds to the inner face of the surface membrane. The protein has amino acid sequence ence similarities with alpha-actinin, an actin binding protein. The protein links actin to the surface membrane and the basal lamina acting through dystrogly- can and merosin (alpha 2-laminin). Interrupting this linkage causes the surface Interrupting this linkage causes the surface membrane to be unstable leading to fiber injury.
62 Duggan et al. Mutations in the sarcoglycan genes in patients with myopathy. N Engl J Med 1997;336:618
63 DUCHENNE DYSTROPHY, SPECTRIN
64 DUCHENNE DYSTROPHY, DYSTROPHIN
65 INFLAMMATORY MYOPATHIES Polymyositis Inclusion body myositis Dermatomyositis
66 POLYMYOSITIS
67 DIAGNOSTIC FEATURES OF POLYMYOSITIS Subacute progressive weakness, proximal>distal. Usually adults, women more common than men. Elevated serum creatine kinase activity. Electromyogram: myopathic potentials, spontaneous activity. Muscle biopsy: inflammatory myopathy affecting chiefly the endomysium. Usually respond to glucocorticoids.
68 POLMYOSITIS, H&E
69 POLMYOSITIS, PARAFFIN SECTION, H&E
70 POLMYOSITIS, IMMUNOPEROXIDASE, CD8
71 POLYMYOSITIS: PATHOLOGY Necrotic fibers and regenerating fibers randomly distributed throughout the muscle specimen. CD8 cytotoxic cells infiltrate pre- dominantly the endomysium with invasion of rare myofibers. Little fibrosis or myofiber hypertrophy, consistent ste t with a subacute disorder. de
72 INCLUSION BODY MYOSITIS
73 DIAGNOSTIC FEATURES OF IBM Most common inflammatory myopathy in patients over the age of 50 years and affects mostly men. Slowly progressive weakness, proximal and distal. Mildly elevated serum creatine kinase or normal. Electromyogram: myopathic potentials, spontaneous activity. Muscle biopsy: resembles polymyosits, but chronic and exhibits rimmed vacuoles and amyloid inclusions. Usually does not respond to glucocorticoids.
74 INCLUSION BODY MYOSITIS, H&E
75 IBM, RIMMED VACUOLES, H&E
76 IBM, EOSINOPHILIC INCLUSION IN A RIMMED VACUOLE
77 IBM, CONGO RED, FLUORESCENCE, RHODAMINE OPTICS
78 ELECTRON MICROSCOPY, nm FILAMENTS
79 IBM PATHOLOGY IBM resembles polymyositis but has hypertrophic fibers and prominent endomysial fibrosis indicating it is chronic. Rimmed vacuoles. Congophilic fibrillar inclusions, composed of abnormal (? paired-helical) filaments. Lymphocytic infiltration suggests an autoimmune disorder, but disorder is usually unresponsive to immunosuppression.
80 DERMATOMYOSITIS
81 DIAGNOSTIC FEATURES OF DERMATOMYOSITIS Subacute progressive weakness, proximal>distal. Children and adults, women more common than men. Characteristic rash on face, chest & extensor surfaces. Elevated serum creatine kinase activity. Electromyogram: myopathic potentials, spontaneous activity. Muscle biopsy: inflammatory myopathy affecting chiefly the perimysium with perifascicular atrophy. Usually respond to glucocorticoids or IVGG.
82 DERMATOMYOSITIS, PERIFASCICULAR ATROPHY, H&E
83 DERMATOMYOSITIS: LYMPHO- CYTE PHENOTYPES CD4 T cells and B cells located chiefly in connective tissue and around vessels of perimysium. Inconstant and usually sparse CD8 T cells y p located mainly in endomysium.
84 DM, IMMUNE COMPLEXES (C5b-9) IN BLOOD VESSEL WALL
85 TUBULORETICULAR AGGREGATE IN ENDOTHELIAL CELL
86 DERMATOMYOSITIS: PATHOLOGY Perifascicular atrophy of muscle fibers, with or with- out necrotic fibers or regenerating fibers. Immune complexes of immunoglobulins and comple- ment components in the walls of blood vessels. Endothelial tubuloreticular aggregates. Reduced number of capillaries at periphery of fascicle. Lymphocytes are often sparse and located in chiefly perimysium.
87 INFLAMMATORY MYOPATHIES: PATHOPHYSIOLOGY Polymyositis and inclusion body myositis (IBM) have autoaggressive CD8 lymphocytes that appear to attack myofibers and suggest an autoimmune role. However, a major question exists about the etiology and patho- genesis of fibm. Dermatomyositis is thought to be caused by auto- antibodies, possibly targeting an antigen of the endothelium. The pathological findings suggest that myofiber injury may be caused by ischemia.
88 HYPOTONIA IN INFANCY DISEASE INHERITED PROGNOSIS Werdnig-Hoffmann Autosomal Fatal disease recessive Central core disease Autosomal Not pro- dominant gressive Nemaline myopathy y Variable Variable Mitochondrial disorder Maternal or Variable autosomal
89 WERDNIG-HOFFMANN DISEASE
90 CENTRAL CORE DISEASE, NADH DEHYDROGENASE
91 MITOCHONDRIAL MYOPATHY
92 MUTATIONS OF mtdna RAGGED RED FIBER
93 CYTOCHROME C OXIDASE DEFICIENT MYOFIBER
94 RRF, SUCCINATE DEHYDROGENASE
CLASSIFICATION OF PERIPHERAL NERVE DISEASES
 DIFFERENTIAL DIAGNOSIS OF NEUROGENIC DISORDERS & MYOPATHIES NEUROPATHY MYOPATHY Weakness distal proximal Sensory loss + 0 Loss of reflexes early late CSF protein elevated normal Electromyography neurogenic
DIFFERENTIAL DIAGNOSIS OF NEUROGENIC DISORDERS & MYOPATHIES NEUROPATHY MYOPATHY Weakness distal proximal Sensory loss + 0 Loss of reflexes early late CSF protein elevated normal Electromyography neurogenic
Amyloid neuropathy: (A) scattered Congo Red positive material in endoneurium displays apple green birefringence under polarized light.
 scattered Congo Red positive material in endoneurium displays apple green birefringence under polarized light.") Cơ vân Cơ vân Cơ vân (cắt dọc) Amyloid neuropathy: (A) scattered Congo Red positive material in endoneurium displays apple green birefringence under polarized light. (A, Congo Red). Amyloid neuropathy:
Cơ vân Cơ vân Cơ vân (cắt dọc) Amyloid neuropathy: (A) scattered Congo Red positive material in endoneurium displays apple green birefringence under polarized light. (A, Congo Red). Amyloid neuropathy:
Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases
 Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases Peripheral neuropathies according to which part affected Axonal Demyelinating with axonal sparing Many times: mixed features
Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases Peripheral neuropathies according to which part affected Axonal Demyelinating with axonal sparing Many times: mixed features
Clinical Aspects of Peripheral Nerve and Muscle Disease. Roy Weller Clinical Neurosciences University of Southampton School of Medicine
 Clinical Aspects of Peripheral Nerve and Muscle Disease Roy Weller Clinical Neurosciences University of Southampton School of Medicine Normal Nerves 1. Anterior Horn Cell 2. Dorsal root ganglion cell 3.
Clinical Aspects of Peripheral Nerve and Muscle Disease Roy Weller Clinical Neurosciences University of Southampton School of Medicine Normal Nerves 1. Anterior Horn Cell 2. Dorsal root ganglion cell 3.
Immune Mediated Neuropathies
 Immune Mediated Neuropathies Hernan Gatuslao, M.D. Assistant Professor Department of Neurology Virginia Commonwealth University School of Medicine AIDP and CIDP Acute inflammatory demyelinating polyneuropathy
Immune Mediated Neuropathies Hernan Gatuslao, M.D. Assistant Professor Department of Neurology Virginia Commonwealth University School of Medicine AIDP and CIDP Acute inflammatory demyelinating polyneuropathy
Introduction and aims of the study
 Introduction and aims of the study 1 Chapter 1 Motor neuron diseases include the most incapacitating and life-threatening illnesses but also rather benign disorders with only mild symptoms and slow progression.
Introduction and aims of the study 1 Chapter 1 Motor neuron diseases include the most incapacitating and life-threatening illnesses but also rather benign disorders with only mild symptoms and slow progression.
PRIMARY DISEASES OF MYELIN. By: Shifaa Al Qa qa
 PRIMARY DISEASES OF MYELIN By: Shifaa Al Qa qa Most diseases of myelin are primarily white matter disorders??? Myelinated axons most diseases of CNS myelin do not involve the peripheral nerves to any significant
PRIMARY DISEASES OF MYELIN By: Shifaa Al Qa qa Most diseases of myelin are primarily white matter disorders??? Myelinated axons most diseases of CNS myelin do not involve the peripheral nerves to any significant
Diseases of Muscle and Neuromuscular Junction
 Diseases of Muscle and Neuromuscular Junction Diseases of Muscle and Neuromuscular Junction Neuromuscular Junction Muscle Myastenia Gravis Eaton-Lambert Syndrome Toxic Infllammatory Denervation Atrophy
Diseases of Muscle and Neuromuscular Junction Diseases of Muscle and Neuromuscular Junction Neuromuscular Junction Muscle Myastenia Gravis Eaton-Lambert Syndrome Toxic Infllammatory Denervation Atrophy
Case 1: History of J.H. Outside Evaluation. Outside Labs. Question #1
 Case 1: History of J.H. 64 yo man seen at UCSF 6-256 25-07. 9 months ago onset progressive weakness of arms and legs, with muscle atrophy in arms. 4 months ago red scaly rash on face, back of hands and
Case 1: History of J.H. 64 yo man seen at UCSF 6-256 25-07. 9 months ago onset progressive weakness of arms and legs, with muscle atrophy in arms. 4 months ago red scaly rash on face, back of hands and
An autoimmune perspective on neuromuscular diseases
 An autoimmune perspective on neuromuscular diseases Colin Chalk MD,CM FRCPC Montreal General Hospital McGill University Schlomchik 2001 The proportion of neuromuscular patients who have an autoimmune cause
An autoimmune perspective on neuromuscular diseases Colin Chalk MD,CM FRCPC Montreal General Hospital McGill University Schlomchik 2001 The proportion of neuromuscular patients who have an autoimmune cause
Peripheral Neuropathies
 Peripheral Neuropathies ELBA Y. GERENA MALDONADO, MD ACTING ASSISTANT PROFESSOR UNIVERSITY OF WASHINGTON MEDICAL CENTER Objectives Definition Neurophysiology Evaluation of polyneuropathies Cases Summary
Peripheral Neuropathies ELBA Y. GERENA MALDONADO, MD ACTING ASSISTANT PROFESSOR UNIVERSITY OF WASHINGTON MEDICAL CENTER Objectives Definition Neurophysiology Evaluation of polyneuropathies Cases Summary
Muscle Pathology Surgical Pathology Unknown Conference. November, 2008 Philip Boyer, M.D., Ph.D.
 Muscle Pathology Surgical Pathology Unknown Conference November, 2008 Philip Boyer, M.D., Ph.D. Etiologic Approach to Differential Diagnosis Symptoms / Signs / Imaging / Biopsy / CSF Analysis Normal Abnormal
Muscle Pathology Surgical Pathology Unknown Conference November, 2008 Philip Boyer, M.D., Ph.D. Etiologic Approach to Differential Diagnosis Symptoms / Signs / Imaging / Biopsy / CSF Analysis Normal Abnormal
III./10.4. Diagnosis. Introduction. A.) Laboratory tests. Laboratory tests, electrophysiology, muscle biopsy, genetic testing, imaging techniques
 Laboratory tests. Laboratory tests, electrophysiology, muscle biopsy, genetic testing, imaging techniques") III./10.4. Diagnosis Laboratory tests, electrophysiology, muscle biopsy, genetic testing, imaging techniques After studying this chapter, you will become familiar with the most commonly used diagnostic
III./10.4. Diagnosis Laboratory tests, electrophysiology, muscle biopsy, genetic testing, imaging techniques After studying this chapter, you will become familiar with the most commonly used diagnostic
Genetic diagnosis of limb girdle muscular dystrophy type 2A, A Case Report
 Genetic diagnosis of limb girdle muscular dystrophy type 2A, A Case Report Roshanak Jazayeri, MD, PhD Assistant Professor of Medical Genetics Faculty of Medicine, Alborz University of Medical Sciences
Genetic diagnosis of limb girdle muscular dystrophy type 2A, A Case Report Roshanak Jazayeri, MD, PhD Assistant Professor of Medical Genetics Faculty of Medicine, Alborz University of Medical Sciences
Neonatal Hypotonia. Encephalopathy acute No encephalopathy. Neurology Chapter of IAP
 The floppy infant assumes a frog legged position. On ventral suspension, the baby can not maintain limb posture against gravity and assumes the position of a rag doll. Encephalopathy acute No encephalopathy
The floppy infant assumes a frog legged position. On ventral suspension, the baby can not maintain limb posture against gravity and assumes the position of a rag doll. Encephalopathy acute No encephalopathy
Il ruolo della diagnostica di laboratorio
 Cremona 9 giugno 2017 DIAGNOSI DIFFERENZIALE DELLE MALATTIE DEL SISTEMA NERVOSO PERIFERICO Il ruolo della diagnostica di laboratorio No conflicts of interest Wang Y et al. Mediators of Inflammatory 2015
Cremona 9 giugno 2017 DIAGNOSI DIFFERENZIALE DELLE MALATTIE DEL SISTEMA NERVOSO PERIFERICO Il ruolo della diagnostica di laboratorio No conflicts of interest Wang Y et al. Mediators of Inflammatory 2015
Critical Illness Polyneuropathy CIP and Critical Illness Myopathy CIM. Andrzej Sladkowski
 Critical Illness Polyneuropathy CIP and Critical Illness Myopathy CIM Andrzej Sladkowski Potential causes of weakness in the ICU-1 Muscle disease Critical illness myopathy Inflammatory myopathy Hypokalemic
Critical Illness Polyneuropathy CIP and Critical Illness Myopathy CIM Andrzej Sladkowski Potential causes of weakness in the ICU-1 Muscle disease Critical illness myopathy Inflammatory myopathy Hypokalemic
Evaluation of Peripheral Neuropathy. Evaluation of Peripheral Neuropathy - Introduction
 Evaluation of Peripheral Neuropathy Chris Edwards, MD Ochsner Neurology, Main Campus Evaluation of Peripheral Neuropathy - Introduction A very common complaint in the clinic Presentation is variable Multiple
Evaluation of Peripheral Neuropathy Chris Edwards, MD Ochsner Neurology, Main Campus Evaluation of Peripheral Neuropathy - Introduction A very common complaint in the clinic Presentation is variable Multiple
Immunopathology of Guillain- Barré syndrome. L. Magy Service de Neurologie Centre de Référence 'Neuropathies Périphériques Rares' CHU Limoges, France
 Immunopathology of Guillain- Barré syndrome L. Magy Service de Neurologie Centre de Référence 'Neuropathies Périphériques Rares' CHU Limoges, France What is Guillain-Barré syndrome? An immune-mediated
Immunopathology of Guillain- Barré syndrome L. Magy Service de Neurologie Centre de Référence 'Neuropathies Périphériques Rares' CHU Limoges, France What is Guillain-Barré syndrome? An immune-mediated
A Practical Approach to Polyneuropathy SLOCUM DICKSON ANNUAL TEACHING DAY NOVEMBER 4, 2017
 A Practical Approach to Polyneuropathy SLOCUM DICKSON ANNUAL TEACHING DAY NOVEMBER 4, 2017 Disclosures Research support from Cytokinetics, Inc Catalyst, Inc Editorial fees from UptoDate. Objectives Describe
A Practical Approach to Polyneuropathy SLOCUM DICKSON ANNUAL TEACHING DAY NOVEMBER 4, 2017 Disclosures Research support from Cytokinetics, Inc Catalyst, Inc Editorial fees from UptoDate. Objectives Describe
AII-type: Select the most appropriate answer
 AII-type: Select the most appropriate answer ( )1. Choose one best answer for the following pathologic pictures. A. choroid cyst B. choroid papilloma C. pontine glioma D. ependymoma E. metastatic tumor
AII-type: Select the most appropriate answer ( )1. Choose one best answer for the following pathologic pictures. A. choroid cyst B. choroid papilloma C. pontine glioma D. ependymoma E. metastatic tumor
CNS third year med students Summary of midterm material H Awad
 CNS third year med students 2018 Summary of midterm material H Awad Dear All This presentation summaries the main important topics covered in the midterm material ( lectures 1-6) There will be two questions
CNS third year med students 2018 Summary of midterm material H Awad Dear All This presentation summaries the main important topics covered in the midterm material ( lectures 1-6) There will be two questions
Movement Disorders. Psychology 372 Physiological Psychology. Background. Myasthenia Gravis. Many Types
 Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
MOTOR NEURONE DISEASE
 MOTOR NEURONE DISEASE Dr Arun Aggarwal Department of Rehabilitation Medicine, RPAH Department of Neurology, Concord Hospital. Motor Neurone Disease Umbrella term in UK and Australia (ALS in USA) Neurodegenerative
MOTOR NEURONE DISEASE Dr Arun Aggarwal Department of Rehabilitation Medicine, RPAH Department of Neurology, Concord Hospital. Motor Neurone Disease Umbrella term in UK and Australia (ALS in USA) Neurodegenerative
Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists
 & electromyography (EMG) for non-neurologists") Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists What is NCS/EMG? NCS examines the conduction properties of sensory and motor peripheral nerves. For both
Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists What is NCS/EMG? NCS examines the conduction properties of sensory and motor peripheral nerves. For both
Making sense of Nerve conduction & EMG
 Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
Distal chronic spinal muscular atrophy involving the hands
 Journal ofneurology, Neurosurgery, and Psychiatry, 1978, 41, 653-658 Distal chronic spinal muscular atrophy involving the hands D. J. O'SULLIVAN AND J. G. McLEOD From St Vincent's Hospital, and Department
Journal ofneurology, Neurosurgery, and Psychiatry, 1978, 41, 653-658 Distal chronic spinal muscular atrophy involving the hands D. J. O'SULLIVAN AND J. G. McLEOD From St Vincent's Hospital, and Department
Electron microscopy in the investigation and diagnosis of muscle disease
 Electron microscopy in the investigation and diagnosis of muscle disease Roy Weller Clinical Neurosciences University of Southampton School of Medicine Normal Muscle Normal Muscle The Sarcomere The names
Electron microscopy in the investigation and diagnosis of muscle disease Roy Weller Clinical Neurosciences University of Southampton School of Medicine Normal Muscle Normal Muscle The Sarcomere The names
Case Report An Unusual Case of Recurrent Guillain-Barre Syndrome of a Different Subtype Five Years after Initial Diagnosis
 Case Reports in Neurological Medicine Volume 2013, Article ID 356157, 4 pages http://dx.doi.org/10.1155/2013/356157 Case Report An Unusual Case of Recurrent Guillain-Barre Syndrome of a Different Subtype
Case Reports in Neurological Medicine Volume 2013, Article ID 356157, 4 pages http://dx.doi.org/10.1155/2013/356157 Case Report An Unusual Case of Recurrent Guillain-Barre Syndrome of a Different Subtype
5.1 Alex.
 5.1 Alex http://tinyurl.com/neuromakessense Alex is a 20-year-old full-time national serviceman. His only past medical history is asthma, presents to A&E with a 4-day history of bilateral finger weakness
5.1 Alex http://tinyurl.com/neuromakessense Alex is a 20-year-old full-time national serviceman. His only past medical history is asthma, presents to A&E with a 4-day history of bilateral finger weakness
Muscular Dystrophy. Biol 405 Molecular Medicine
 Muscular Dystrophy Biol 405 Molecular Medicine Duchenne muscular dystrophy Duchenne muscular dystrophy is a neuromuscular disease that occurs in ~ 1/3,500 male births. The disease causes developmental
Muscular Dystrophy Biol 405 Molecular Medicine Duchenne muscular dystrophy Duchenne muscular dystrophy is a neuromuscular disease that occurs in ~ 1/3,500 male births. The disease causes developmental
muscle biopsy How to do it
 How to do it muscle biopsy Gillian Hall Department of Clinical Neurosciences, Western General Hospital, Edinburgh EH4 2XU. Email: ghall@skull.dcn.ed.ac.uk INTRODUCTION Good clinical evaluation remains
How to do it muscle biopsy Gillian Hall Department of Clinical Neurosciences, Western General Hospital, Edinburgh EH4 2XU. Email: ghall@skull.dcn.ed.ac.uk INTRODUCTION Good clinical evaluation remains
A Case of Acute Sensory Neuropathy Associated with Contrast Enhancement of the Cauda Equina on Magnetic Resonance Imaging
 61 Case Report St. Marianna Med. J. Vol. 33, pp. 61 66, 2005 A Case of Acute Sensory Neuropathy Associated with Contrast Enhancement of the Cauda Equina on Magnetic Resonance Imaging Toshinari Kobayashi
61 Case Report St. Marianna Med. J. Vol. 33, pp. 61 66, 2005 A Case of Acute Sensory Neuropathy Associated with Contrast Enhancement of the Cauda Equina on Magnetic Resonance Imaging Toshinari Kobayashi
Thank you to: L Magy, L Richard, N Couade, F Maquin
 «Crash course in the interpretation of peripheral nerve biopsies: which nerve to biopsy, tissue fixation: paraffin, semi thins, EM (common stains and immunos), identifying degenerating and regenerating
«Crash course in the interpretation of peripheral nerve biopsies: which nerve to biopsy, tissue fixation: paraffin, semi thins, EM (common stains and immunos), identifying degenerating and regenerating
Disorders of Muscle. Disorders of Muscle. Muscle Groups Involved in Myopathy. Needle Examination of EMG. History. Muscle Biopsy
 Disorders of Muscle Disorders of Muscle Zakia Bell, M.D. Associate Professor of Neurology and Physical Medicine & Rehabilitation Virginia Commonwealth University Cardinal symptom of diseases of the muscle
Disorders of Muscle Disorders of Muscle Zakia Bell, M.D. Associate Professor of Neurology and Physical Medicine & Rehabilitation Virginia Commonwealth University Cardinal symptom of diseases of the muscle
MR Imaging of the Cauda Equina in Charcot-Marie-Tooth disease
 MR Imaging of the Cauda Equina in Charcot-Marie-Tooth disease Poster No.: C-0741 Congress: ECR 2015 Type: Scientific Exhibit Authors: Y. Tatewaki, S. Nishiyama, Y. Kato, T. Murata, S. Mugikura, L. Li,
MR Imaging of the Cauda Equina in Charcot-Marie-Tooth disease Poster No.: C-0741 Congress: ECR 2015 Type: Scientific Exhibit Authors: Y. Tatewaki, S. Nishiyama, Y. Kato, T. Murata, S. Mugikura, L. Li,
IVIG (intravenous immunoglobulin) Bivigam, Carimune NF, Flebogamma, Gammagard, Gammagard S/D, Gammaked, Gammaplex, Gamunex-C, Octagam, Privigen
 Bivigam, Carimune NF, Flebogamma, Gammagard, Gammagard S/D, Gammaked, Gammaplex, Gamunex-C, Octagam, Privigen") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following documented indications: 1. Primary Immunodeficiency Disease (PID) with ONE of the a. Hypogammaglobulinemia,
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following documented indications: 1. Primary Immunodeficiency Disease (PID) with ONE of the a. Hypogammaglobulinemia,
Multifocal motor neuropathy: diagnostic criteria that predict the response to immunoglobulin treatment
 Multifocal motor neuropathy: diagnostic criteria that predict the response to immunoglobulin treatment 7 MMN RM Van den Berg-Vos, H Franssen, JHJ Wokke, HW Van Es, LH Van den Berg Annals of Neurology 2000;
Multifocal motor neuropathy: diagnostic criteria that predict the response to immunoglobulin treatment 7 MMN RM Van den Berg-Vos, H Franssen, JHJ Wokke, HW Van Es, LH Van den Berg Annals of Neurology 2000;
Pathology of Neuromuscular Disease Part 1: muscle
 Pathology of Neuromuscular Disease Part 1: muscle Zarife Sahenk, MD. PhD. Research Institute at Nationwide Children s Hospital Center for gene therapy, Neuromuscular Program Experimental & Clinical Neuromuscular
Pathology of Neuromuscular Disease Part 1: muscle Zarife Sahenk, MD. PhD. Research Institute at Nationwide Children s Hospital Center for gene therapy, Neuromuscular Program Experimental & Clinical Neuromuscular
Chapter 12b. Overview
 Chapter 12b Spinal Cord Overview Spinal cord gross anatomy Spinal meninges Sectional anatomy Sensory pathways Motor pathways Spinal cord pathologies 1 The Adult Spinal Cord About 18 inches (45 cm) long
Chapter 12b Spinal Cord Overview Spinal cord gross anatomy Spinal meninges Sectional anatomy Sensory pathways Motor pathways Spinal cord pathologies 1 The Adult Spinal Cord About 18 inches (45 cm) long
A CASE OF GIANT AXONAL NEUROPATHY HEMANANTH T SECOND YEAR POST GRADUATE IN PAEDIATRICS INSTITUTE OF SOCIAL PAEDIATRICS GOVERNMENT STANLEY HOSPITAL
 A CASE OF GIANT AXONAL NEUROPATHY HEMANANTH T SECOND YEAR POST GRADUATE IN PAEDIATRICS INSTITUTE OF SOCIAL PAEDIATRICS GOVERNMENT STANLEY HOSPITAL CASE HISTORY Nine year old male child Second born Born
A CASE OF GIANT AXONAL NEUROPATHY HEMANANTH T SECOND YEAR POST GRADUATE IN PAEDIATRICS INSTITUTE OF SOCIAL PAEDIATRICS GOVERNMENT STANLEY HOSPITAL CASE HISTORY Nine year old male child Second born Born
Neuroimmunology. Innervation of lymphoid organs. Neurotransmitters. Neuroendocrine hormones. Cytokines. Autoimmunity
 Neuroimmunology Innervation of lymphoid organs Neurotransmitters Neuroendocrine hormones Cytokines Autoimmunity CNS has two ways of contacting and regulating structures in the periphery Autonomic
Neuroimmunology Innervation of lymphoid organs Neurotransmitters Neuroendocrine hormones Cytokines Autoimmunity CNS has two ways of contacting and regulating structures in the periphery Autonomic
Faculty Disclosure. Sanjay P. Singh, MD, FAAN. Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion
 Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
CIDP + MMN - how to diagnose and treat. Dr Hadi Manji
 CIDP + MMN - how to diagnose and treat Dr Hadi Manji Outline Introduction CIDP Diagnosis Clinical features MRI Nerve conduction tests Lumbar puncture Nerve biopsy Treatment IV Ig Steroids Plasma Exchnage
CIDP + MMN - how to diagnose and treat Dr Hadi Manji Outline Introduction CIDP Diagnosis Clinical features MRI Nerve conduction tests Lumbar puncture Nerve biopsy Treatment IV Ig Steroids Plasma Exchnage
Supplementary Online Content
 Supplementary Online Content Stevens O, Claeys KG, Poesen K, Veroniek S, Van Damme P. Diagnostic challenges and clinical characteristics of hepatitis E virus associated Guillain- Barré syndrome. JAMA Neurol.
Supplementary Online Content Stevens O, Claeys KG, Poesen K, Veroniek S, Van Damme P. Diagnostic challenges and clinical characteristics of hepatitis E virus associated Guillain- Barré syndrome. JAMA Neurol.
DOWNLOAD OR READ : MYOPATHIES AND MUSCLE DISEASES HANDBOOK OF CLINICAL NEUROLOGY PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : MYOPATHIES AND MUSCLE DISEASES HANDBOOK OF CLINICAL NEUROLOGY PDF EBOOK EPUB MOBI Page 1 Page 2 myopathies and muscle diseases handbook of clinical neurology myopathies and muscle diseases
DOWNLOAD OR READ : MYOPATHIES AND MUSCLE DISEASES HANDBOOK OF CLINICAL NEUROLOGY PDF EBOOK EPUB MOBI Page 1 Page 2 myopathies and muscle diseases handbook of clinical neurology myopathies and muscle diseases
Patogenesi e terapia della Neuropatia Motoria Multifocale
 26 Settembre 2014 Patogenesi e terapia della Neuropatia Motoria Multifocale Francesca Gallia Neurologia 2, Ist. Clin. Humanitas Rozzano, Milano Multifocal Motor Neuropathy Rare disorder characterized by:
26 Settembre 2014 Patogenesi e terapia della Neuropatia Motoria Multifocale Francesca Gallia Neurologia 2, Ist. Clin. Humanitas Rozzano, Milano Multifocal Motor Neuropathy Rare disorder characterized by:
Lumbosacral plexus lesion Lumbosacral plexus disorders G54.1 Neuralgic amyotrophy Neuralgic amyotrophy G
 ICD-9-CM and ICD-10-CM NEUROMUSCULAR DIAGNOSIS CODES Focal Neuropathy ICD-9-CM ICD-10-CM Mononeuropathy G56.00 Carpal tunnel syndrome 354.00 Other median nerve lesion 354.10 Lesion of ulnar nerve 354.20
ICD-9-CM and ICD-10-CM NEUROMUSCULAR DIAGNOSIS CODES Focal Neuropathy ICD-9-CM ICD-10-CM Mononeuropathy G56.00 Carpal tunnel syndrome 354.00 Other median nerve lesion 354.10 Lesion of ulnar nerve 354.20
ELEVATION OF CREATINE KINASE IN AMYOTROPHIC LATERAL SCLEROSIS
 20 1 ELEVATION OF CREATINE KINASE IN AMYOTROPHIC LATERAL SCLEROSIS Po ten tial Confusion with Pol y m y osi ti s THOMAS M. HARRINGTON, MARC D. COHEN, JOHN D. BARTLESON, and WILLIAM W. GINSBURG Serum creatine
20 1 ELEVATION OF CREATINE KINASE IN AMYOTROPHIC LATERAL SCLEROSIS Po ten tial Confusion with Pol y m y osi ti s THOMAS M. HARRINGTON, MARC D. COHEN, JOHN D. BARTLESON, and WILLIAM W. GINSBURG Serum creatine
Comparison of electrophysiological findings in axonal and demyelinating Guillain-Barre syndrome
 Iranian Journal of Neurology Original Paper Iran J Neurol 2014; 13(3): 138-143 Comparison of electrophysiological findings in axonal and demyelinating Guillain-Barre syndrome Received: 9 Mar 2014 Accepted:
Iranian Journal of Neurology Original Paper Iran J Neurol 2014; 13(3): 138-143 Comparison of electrophysiological findings in axonal and demyelinating Guillain-Barre syndrome Received: 9 Mar 2014 Accepted:
Guillain-Barré Syndrome
 Guillain-Barré Syndrome Ouch! www.philippelefevre.com Guillain-Barré Syndrome Acute post-infective polyneuropathy Heterogeneous condition with several variant forms Lipid A Neuronal Ganglioside Pathogenesis
Guillain-Barré Syndrome Ouch! www.philippelefevre.com Guillain-Barré Syndrome Acute post-infective polyneuropathy Heterogeneous condition with several variant forms Lipid A Neuronal Ganglioside Pathogenesis
Case Report Central Nervous System Demyelination in a Charcot-Marie-Tooth Type 1A Patient
 Case Reports in Neurological Medicine Volume 2013, Article ID 243652, 4 pages http://dx.doi.org/10.1155/2013/243652 Case Report Central Nervous System Demyelination in a Charcot-Marie-Tooth Type 1A Patient
Case Reports in Neurological Medicine Volume 2013, Article ID 243652, 4 pages http://dx.doi.org/10.1155/2013/243652 Case Report Central Nervous System Demyelination in a Charcot-Marie-Tooth Type 1A Patient
A family study of Charcot-Marie-Tooth disease
 Joturnal of Medical Genetics, 1982, 19, 88-93 A family study of Charcot-Marie-Tooth disease A P BROOKS* AND A E H EMERY From the University Department of Human Genetics, Western General Hospital, Edinburgh
Joturnal of Medical Genetics, 1982, 19, 88-93 A family study of Charcot-Marie-Tooth disease A P BROOKS* AND A E H EMERY From the University Department of Human Genetics, Western General Hospital, Edinburgh
Fundamentals of the Nervous System and Nervous Tissue. Nervous System. Basic Divisions of the Nervous System C H A P T E R 12.
 C H A P T E R 12 Fundamentals of the Nervous System and Nervous Tissue Nervous System Sensory input Integration Motor output Figure 12.1 Basic Divisions of the Nervous System Brain CNS Spinal cord Nerves
C H A P T E R 12 Fundamentals of the Nervous System and Nervous Tissue Nervous System Sensory input Integration Motor output Figure 12.1 Basic Divisions of the Nervous System Brain CNS Spinal cord Nerves
Genetics of Inclusion Body Myositis
 Genetics of Inclusion Body Myositis Thomas Lloyd, MD, PhD Associate Professor of Neurology and Neuroscience Co-director, Johns Hopkins Myositis Center Sporadic IBM (IBM) Age at onset usually > 50 Prevalence
Genetics of Inclusion Body Myositis Thomas Lloyd, MD, PhD Associate Professor of Neurology and Neuroscience Co-director, Johns Hopkins Myositis Center Sporadic IBM (IBM) Age at onset usually > 50 Prevalence
Jonathan Katz, MD CPMC
 Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC First, a bit of background Classic CIDP--TREATABLE MADSAM/Asymmetric Neuropathy Chronic Length Dependent Neuropathy-
Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC First, a bit of background Classic CIDP--TREATABLE MADSAM/Asymmetric Neuropathy Chronic Length Dependent Neuropathy-
DSS-1. No financial disclosures
 DSS-1 No financial disclosures Clinical History 9 year old boy with past medical history significant for cerebral palsy, in-turning right foot, left clubfoot that was surgically corrected at 3 years of
DSS-1 No financial disclosures Clinical History 9 year old boy with past medical history significant for cerebral palsy, in-turning right foot, left clubfoot that was surgically corrected at 3 years of
Infection-Associated Neurological Syndromes
 Infection-Associated Neurological Syndromes Anand P, MD PhD Medical Director, BloodCenter of Wisconsin Assistant Professor, Medical College of Wisconsin ASFA Annual Meeting San Antonio, TX, May 8th, 2015
Infection-Associated Neurological Syndromes Anand P, MD PhD Medical Director, BloodCenter of Wisconsin Assistant Professor, Medical College of Wisconsin ASFA Annual Meeting San Antonio, TX, May 8th, 2015
Index. Note: Page numbers of article titles are in boldface type.
 Neurol Clin N Am 20 (2002) 605 617 Index Note: Page numbers of article titles are in boldface type. A ALS. See Amyotrophic lateral sclerosis (ALS) Amyotrophic lateral sclerosis (ALS) active denervation
Neurol Clin N Am 20 (2002) 605 617 Index Note: Page numbers of article titles are in boldface type. A ALS. See Amyotrophic lateral sclerosis (ALS) Amyotrophic lateral sclerosis (ALS) active denervation
A Tale of Five Demyelinating Neuropathies
 Objectives A Tale of Five Demyelinating Neuropathies Tahseen Mozaffar, MD FAAN Professor and Vice Chair of Neurology Director, UC Irvine-MDA ALS and Neuromuscular Center Director, Neurology Residency Training
Objectives A Tale of Five Demyelinating Neuropathies Tahseen Mozaffar, MD FAAN Professor and Vice Chair of Neurology Director, UC Irvine-MDA ALS and Neuromuscular Center Director, Neurology Residency Training
Post-MDT leprosy neuropathy: differentially diagnosing reactional neuritis and relapses.
 Sérgio Luiz Gomes Antunes Márcia Rodrigues Jardim Robson Vital Teixeira José Augusto da Costa Nery Anna Maria Sales, Euzenir Nunes Sarno Post-MDT leprosy neuropathy: differentially diagnosing reactional
Sérgio Luiz Gomes Antunes Márcia Rodrigues Jardim Robson Vital Teixeira José Augusto da Costa Nery Anna Maria Sales, Euzenir Nunes Sarno Post-MDT leprosy neuropathy: differentially diagnosing reactional
High resolution ultrasound in peripheral neuropathies
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 5 Advanced neurosonology - Level 3 High resolution ultrasound in peripheral neuropathies
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 5 Advanced neurosonology - Level 3 High resolution ultrasound in peripheral neuropathies
EDX in Myopathies Limitations. EDX in Myopathies Utility Causes of Myopathy. Myopathy: Issues for Electromyographers
 Electrodiagnostic Assessment of Myopathy Myopathy: Issues for Electromyographers Often perceived as challenging Ian Grant Division of Neurology QEII Health Sciences Centre Halifax NS CNSF EMG Course June
Electrodiagnostic Assessment of Myopathy Myopathy: Issues for Electromyographers Often perceived as challenging Ian Grant Division of Neurology QEII Health Sciences Centre Halifax NS CNSF EMG Course June
Diagnosis and Management of Immune-mediated Neuropathies
 Continuing Medical Education 39 Diagnosis and Management of Immune-mediated Neuropathies Sung-Tsang Hsieh Abstract- Immune-mediate neuropathies, or inflammatory neuropathies are neuropathies due to the
Continuing Medical Education 39 Diagnosis and Management of Immune-mediated Neuropathies Sung-Tsang Hsieh Abstract- Immune-mediate neuropathies, or inflammatory neuropathies are neuropathies due to the
Chapter 5 Inclusion Body Myositis
 Chapter 5 Inclusion Body Myositis Lawrence J. Kagen Abstract Inclusion body myositis is an insidious, slowly progressive myopathy of middle-aged and older individuals. Because of these characteristics,
Chapter 5 Inclusion Body Myositis Lawrence J. Kagen Abstract Inclusion body myositis is an insidious, slowly progressive myopathy of middle-aged and older individuals. Because of these characteristics,
Compound Action Potential, CAP
 Stimulus Strength UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY INTRODUCTION TO NEUROPHYSIOLOGY Spring, 2013 Textbook of Medical Physiology by: Guyton & Hall, 12 th edition
Stimulus Strength UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY INTRODUCTION TO NEUROPHYSIOLOGY Spring, 2013 Textbook of Medical Physiology by: Guyton & Hall, 12 th edition
CLINICAL AND LABORATORY FEATURES OF NEUROPATHIES WITH SERUM IgM BINDING TO TS-HDS
 CLINICAL AND LABORATORY FEATURES OF NEUROPATHIES WITH SERUM IgM BINDING TO TS-HDS ALAN PESTRONK, MD, 1,2 ROBERT E. SCHMIDT, MD, PhD, 2 RATI M. CHOKSI, MS, 1 R. BRIAN SOMMERVILLE, MD, 1 and MUHAMMAD T.
CLINICAL AND LABORATORY FEATURES OF NEUROPATHIES WITH SERUM IgM BINDING TO TS-HDS ALAN PESTRONK, MD, 1,2 ROBERT E. SCHMIDT, MD, PhD, 2 RATI M. CHOKSI, MS, 1 R. BRIAN SOMMERVILLE, MD, 1 and MUHAMMAD T.
Pedro A. Mendez-Tellez, MD
 Critical Illness Polyneuropathy and Myopathy: Epidemiology and Risk Factors Pedro A. Mendez-Tellez, MD Johns Hopkins University Baltimore, Maryland, USA pmendez@jhmi.edu Conflict of Interest I have no
Critical Illness Polyneuropathy and Myopathy: Epidemiology and Risk Factors Pedro A. Mendez-Tellez, MD Johns Hopkins University Baltimore, Maryland, USA pmendez@jhmi.edu Conflict of Interest I have no
12 Anatomy and Physiology of Peripheral Nerves
 12 Anatomy and Physiology of Peripheral Nerves Introduction Anatomy Classification of Peripheral Nerves Sensory Nerves Motor Nerves Pathologies of Nerves Focal Injuries Regeneration of Injured Nerves Signs
12 Anatomy and Physiology of Peripheral Nerves Introduction Anatomy Classification of Peripheral Nerves Sensory Nerves Motor Nerves Pathologies of Nerves Focal Injuries Regeneration of Injured Nerves Signs
ALS and Hyperexcitability. Anai Hamasaki, MD Neurophysiology Fellow - KUMC March 10 th, 2017
 ALS and Hyperexcitability Anai Hamasaki, MD Neurophysiology Fellow - KUMC March 10 th, 2017 Overview History What we know What supports our theories What we don't know Future directions ALS History Jean-Martin
ALS and Hyperexcitability Anai Hamasaki, MD Neurophysiology Fellow - KUMC March 10 th, 2017 Overview History What we know What supports our theories What we don't know Future directions ALS History Jean-Martin
Biology 3201 Nervous System # 7: Nervous System Disorders
 Biology 3201 Nervous System # 7: Nervous System Disorders Alzheimer's Disease first identified by German physician, Alois Alzheimer, in 1906 most common neurodegenerative disease two thirds of cases of
Biology 3201 Nervous System # 7: Nervous System Disorders Alzheimer's Disease first identified by German physician, Alois Alzheimer, in 1906 most common neurodegenerative disease two thirds of cases of
Spinal Cord Organization. January 12, 2011
 Spinal Cord Organization January 12, 2011 Spinal Cord 31 segments terminates at L1-L2 special components - conus medullaris - cauda equina no input from the face Spinal Cord, Roots & Nerves Dorsal root
Spinal Cord Organization January 12, 2011 Spinal Cord 31 segments terminates at L1-L2 special components - conus medullaris - cauda equina no input from the face Spinal Cord, Roots & Nerves Dorsal root
BIOH111. o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system
 BIOH111 o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system Endeavour College of Natural Health endeavour.edu.au 1 TEXTBOOK AND REQUIRED/RECOMMENDED
BIOH111 o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system Endeavour College of Natural Health endeavour.edu.au 1 TEXTBOOK AND REQUIRED/RECOMMENDED
Electrophysiology in the Guillain-Barré Syndrome: Study of 30 Cases
 Journal of Bangladesh College of Physicians and Surgeons Vol. 24, No. 2, May 2006 Electrophysiology in the Guillain-Barré Syndrome: Study of 30 Cases NC KUNDU Summary: Thirty consecutive patients diagnosed
Journal of Bangladesh College of Physicians and Surgeons Vol. 24, No. 2, May 2006 Electrophysiology in the Guillain-Barré Syndrome: Study of 30 Cases NC KUNDU Summary: Thirty consecutive patients diagnosed
Muscle Weakness Or Paralysis With Compromise Of Peripheral Nerve
 Muscle Weakness Or Paralysis With Compromise Of Peripheral Nerve Muscle weakness or complete paralysis may be secondary to an interruption in the communication between the brain and nerve cells in the
Muscle Weakness Or Paralysis With Compromise Of Peripheral Nerve Muscle weakness or complete paralysis may be secondary to an interruption in the communication between the brain and nerve cells in the
A. Subdivisions of the Nervous System: 1. The two major subdivisions of the nervous system:
 BIO 211: ANATOMY & PHYSIOLOGY I 1 Ch 10 A Ch 10 B CHAPTER 10 NERVOUS SYSTEM 1 BASIC STRUCTURE and FUNCTION Dr. Lawrence G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill.
BIO 211: ANATOMY & PHYSIOLOGY I 1 Ch 10 A Ch 10 B CHAPTER 10 NERVOUS SYSTEM 1 BASIC STRUCTURE and FUNCTION Dr. Lawrence G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill.
Nervous Tissue and Histology of CNS
 Nervous Tissue and Histology of CNS Functions of Nervous System Like the CPU of a computer, the nervous system is the master controlling system of the body. It is designed to constantly and rapidly adjust
Nervous Tissue and Histology of CNS Functions of Nervous System Like the CPU of a computer, the nervous system is the master controlling system of the body. It is designed to constantly and rapidly adjust
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 4: Myelin diseases of the CNS
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 4: Myelin diseases of the CNS ILOS 1. to understand differences and similarities between diseases of myelin in CNS and PNS. 2. to understand
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 4: Myelin diseases of the CNS ILOS 1. to understand differences and similarities between diseases of myelin in CNS and PNS. 2. to understand
Clinical, Electrophysiological and Histopathological Diagnosis of Chronic Polyradiculoneuropathy
 Clinical, Electrophysiological and Histopathological Diagnosis of Chronic Polyradiculoneuropathy Hamdy N.A. El-Tallawy 1, Essam S. Darwish 1, Samyaa Ashour 2, Seyam S. Salem 3, Hesham S. Atta 4, Tarek
Clinical, Electrophysiological and Histopathological Diagnosis of Chronic Polyradiculoneuropathy Hamdy N.A. El-Tallawy 1, Essam S. Darwish 1, Samyaa Ashour 2, Seyam S. Salem 3, Hesham S. Atta 4, Tarek
Miller Fisher Syndrome A variant of Guillan Barré Syndrome. Sarah I. Sheikh, BM BCh, MRCP
 Miller Fisher Syndrome A variant of Guillan Barré Syndrome Sarah I. Sheikh, BM BCh, MRCP History of GBS 1859 Jean Baptiste Octave Landry de Thézillat (1826-1865) published his observation on ascending
Miller Fisher Syndrome A variant of Guillan Barré Syndrome Sarah I. Sheikh, BM BCh, MRCP History of GBS 1859 Jean Baptiste Octave Landry de Thézillat (1826-1865) published his observation on ascending
Myopathy in Post-Radiation Cervico-Scapular Syndrome
 http://escholarship.umassmed.edu/neurol_bull Myopathy in Post-Radiation Cervico-Scapular Syndrome Anna Kogan, Galyna Pushchinska, and Roberta Seidman Department of Neurology Stony Brook University Hospital
http://escholarship.umassmed.edu/neurol_bull Myopathy in Post-Radiation Cervico-Scapular Syndrome Anna Kogan, Galyna Pushchinska, and Roberta Seidman Department of Neurology Stony Brook University Hospital
1/22/2019. Nerve conduction studies. Learning objectives: Jeffrey Allen MD University of Minnesota Minneapolis, MN
 Jeffrey Allen MD University of Minnesota Minneapolis, MN February 9, 2019 Learning objectives: Describe electrophysiologic features of peripheral nerve demyelination Identify electrophysiology findings
Jeffrey Allen MD University of Minnesota Minneapolis, MN February 9, 2019 Learning objectives: Describe electrophysiologic features of peripheral nerve demyelination Identify electrophysiology findings
Sensory Pathways & Somatic Nervous System. Chapter 15
 Sensory Pathways & Somatic Nervous System Chapter 15 How Does Brain Differentiate Sensations? Pain impulses make brain aware of injuries and infections. Impulses from eye, ear, nose and tongue make brain
Sensory Pathways & Somatic Nervous System Chapter 15 How Does Brain Differentiate Sensations? Pain impulses make brain aware of injuries and infections. Impulses from eye, ear, nose and tongue make brain
ZKV and Guillain-Barré Syndrome. Silvia N. Tenembaum Pediatric Neurologist
 ZKV and Guillain-Barré Syndrome Silvia N. Tenembaum Pediatric Neurologist ZIKA VIRUS- BACKGROUND INFORMATION Arbovirus (Arthropod-borne virus) 1- Flaviviridae family: Dengue (DENV) West Nile (WNV) Yellow
ZKV and Guillain-Barré Syndrome Silvia N. Tenembaum Pediatric Neurologist ZIKA VIRUS- BACKGROUND INFORMATION Arbovirus (Arthropod-borne virus) 1- Flaviviridae family: Dengue (DENV) West Nile (WNV) Yellow
Index. Phys Med Rehabil Clin N Am 14 (2003) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Phys Med Rehabil Clin N Am 14 (2003) 445 453 Index Note: Page numbers of article titles are in boldface type. A Acid maltase deficiencies, electrodiagnosis of, 420, 422 Acquired peripheral neuropathy,
Phys Med Rehabil Clin N Am 14 (2003) 445 453 Index Note: Page numbers of article titles are in boldface type. A Acid maltase deficiencies, electrodiagnosis of, 420, 422 Acquired peripheral neuropathy,
Motor tracts Both pyramidal tracts and extrapyramidal both starts from cortex: Area 4 Area 6 Area 312 Pyramidal: mainly from area 4 Extrapyramidal:
 Motor tracts Both pyramidal tracts and extrapyramidal both starts from cortex: Area 4 Area 6 Area 312 Pyramidal: mainly from area 4 Extrapyramidal: mainly from area 6 area 6 Premotorarea: uses external
Motor tracts Both pyramidal tracts and extrapyramidal both starts from cortex: Area 4 Area 6 Area 312 Pyramidal: mainly from area 4 Extrapyramidal: mainly from area 6 area 6 Premotorarea: uses external
Once a vessel is torn, blood accumulating under arterial pressure can dissect the tightly applied dura away from the inner skull surface producing a
 Once a vessel is torn, blood accumulating under arterial pressure can dissect the tightly applied dura away from the inner skull surface producing a hematoma that compresses the brain surface. - Clinically,
Once a vessel is torn, blood accumulating under arterial pressure can dissect the tightly applied dura away from the inner skull surface producing a hematoma that compresses the brain surface. - Clinically,
Medical Immunology Practice Questions-2016 Autoimmunity + Case Studies
 Medical Immunology Practice Questions-2016 Autoimmunity + Case Studies Directions: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement.
Medical Immunology Practice Questions-2016 Autoimmunity + Case Studies Directions: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement.
Chapter 13 PNS and reflex activity
 Chapter 13 PNS and reflex activity I. Peripheral nervous system A. PNS links CNS to the body B. Sensory: the afferent division C. Motor: the efferent division D. Ganglia: collections of cell bodies in
Chapter 13 PNS and reflex activity I. Peripheral nervous system A. PNS links CNS to the body B. Sensory: the afferent division C. Motor: the efferent division D. Ganglia: collections of cell bodies in
Treatment of multifocal motor neuropathy with interferon-β1a
 Treatment of multifocal motor neuropathy with interferon-β1a 12 MMN RM Van den Berg-Vos, LH Van den Berg, H Franssen, PA Van Doorn, ISJ Martina, JHJ Wokke Adapted from Neurology 2000; 54: 1518-1521. Chapter
Treatment of multifocal motor neuropathy with interferon-β1a 12 MMN RM Van den Berg-Vos, LH Van den Berg, H Franssen, PA Van Doorn, ISJ Martina, JHJ Wokke Adapted from Neurology 2000; 54: 1518-1521. Chapter
Nerve pathologic features differentiate POEMS syndrome from CIDP
 Piccione et al. Acta Neuropathologica Communications (2016) 4:116 DOI 10.1186/s40478-016-0389-1 RESEARCH Nerve pathologic features differentiate POEMS syndrome from CIDP Ezequiel A. Piccione 1, Janean
Piccione et al. Acta Neuropathologica Communications (2016) 4:116 DOI 10.1186/s40478-016-0389-1 RESEARCH Nerve pathologic features differentiate POEMS syndrome from CIDP Ezequiel A. Piccione 1, Janean
Charcot-Marie-Tooth Disease (CMT) Sometimes known as Hereditary Motor and Sensory neuropathy (HMSN) or Peroneal Muscular Atrophy (PMA)
 Sometimes known as Hereditary Motor and Sensory neuropathy (HMSN) or Peroneal Muscular Atrophy (PMA)") Version: 2 Published: January 2004 Updated: December 2009 Date of review: November 2011 Author: Dr.Hilton-Jones MD, FRCP, FRCPE Clinical Director, Oxford MDC Muscle and Nerve Centre, and revised by Dr.
Version: 2 Published: January 2004 Updated: December 2009 Date of review: November 2011 Author: Dr.Hilton-Jones MD, FRCP, FRCPE Clinical Director, Oxford MDC Muscle and Nerve Centre, and revised by Dr.
Multifocal motor neuropathy: long-term clinical and electrophysiological assessment of intravenous immunoglobulin maintenance treatment
 Multifocal motor neuropathy: long-term clinical and electrophysiological assessment of intravenous immunoglobulin maintenance treatment 11 MMN RM Van den Berg-Vos, H Franssen, JHJ Wokke, LH Van den Berg
Multifocal motor neuropathy: long-term clinical and electrophysiological assessment of intravenous immunoglobulin maintenance treatment 11 MMN RM Van den Berg-Vos, H Franssen, JHJ Wokke, LH Van den Berg
PhD. Authors/faculty
 Multifocal Motor Neuropathy Eduardo Nobile-Orazio, MD, PhD,Alberto Cappellari, MD,and Alberto Priori, MD, PhD No one involved in the planning of this CME activity has any y relevant financial relationships
Multifocal Motor Neuropathy Eduardo Nobile-Orazio, MD, PhD,Alberto Cappellari, MD,and Alberto Priori, MD, PhD No one involved in the planning of this CME activity has any y relevant financial relationships
Department of Neurology/Division of Anatomical Sciences
 Spinal Cord I Lecture Outline and Objectives CNS/Head and Neck Sequence TOPIC: FACULTY: THE SPINAL CORD AND SPINAL NERVES, Part I Department of Neurology/Division of Anatomical Sciences LECTURE: Monday,
Spinal Cord I Lecture Outline and Objectives CNS/Head and Neck Sequence TOPIC: FACULTY: THE SPINAL CORD AND SPINAL NERVES, Part I Department of Neurology/Division of Anatomical Sciences LECTURE: Monday,
Objectives. Non-Traumatic Muscle Pathologies. Abnormal Muscle Signal Intensity. Inflammatory Myositis. Polymyostis / Dermatomyositis.
 Non-Traumatic Muscle Pathologies Ali Naraghi Division of Musculoskeletal Radiology Joint Department of Medical Imaging University of Toronto Objectives Define the range of non-traumatic pathologies affecting
Non-Traumatic Muscle Pathologies Ali Naraghi Division of Musculoskeletal Radiology Joint Department of Medical Imaging University of Toronto Objectives Define the range of non-traumatic pathologies affecting
The Nervous System. Functions of the Nervous System input gathering To monitor occurring inside and outside the body Changes =
 The Nervous System Functions of the Nervous System input gathering To monitor occurring inside and outside the body Changes = To process and sensory input and decide if is needed output A response to integrated
The Nervous System Functions of the Nervous System input gathering To monitor occurring inside and outside the body Changes = To process and sensory input and decide if is needed output A response to integrated
Inclusion body myositis
 Pathology Feature William R. Hart, M.D. Section Editor Inclusion body myositis A possible chronic persistent muscle infection mumps virus 1 Samuel M. Chou, M.D., Ph.D. Inclusion body myositis was diagnosed
Pathology Feature William R. Hart, M.D. Section Editor Inclusion body myositis A possible chronic persistent muscle infection mumps virus 1 Samuel M. Chou, M.D., Ph.D. Inclusion body myositis was diagnosed
Biology 218 Human Anatomy
 Chapter 17 Adapted form Tortora 10 th ed. LECTURE OUTLINE A. Overview of the Nervous System (p. 537) 1. The nervous system and the endocrine system are the body s major control and integrating centers.
Chapter 17 Adapted form Tortora 10 th ed. LECTURE OUTLINE A. Overview of the Nervous System (p. 537) 1. The nervous system and the endocrine system are the body s major control and integrating centers.