Dementia Update Kenneth B Pugar, DO, dfacn. Dayton Center for Neurological Disorders. Frustration, Progress, and Hope
|
|
|
- Lynette Strickland
- 6 years ago
- Views:
Transcription
1 Dementia Update 2016 Frustration, Progress, and Hope Kenneth B Pugar, DO, dfacn Dayton Center for Neurological Disorders

2
3

4

5
6 Facts and figures Types and definitions Pathophysiology Treatment failures Risk factors Hope Preventative strategies Early detection Biomarkers Treatment Future
7
8 In fact Women are at the epicenter of the AD crisis 2/3 of the 5 million seniors with AD are women In all people > 71yo 16% of the women have AD 11% of the men have AD At age 65, women without AD have a 1 in 6 chance of developing AD during the remainder of their lives, compared with a 1 in 11 chance in men
9 Why? Women have a higher life expectancy (81 vs 76) After the age of 80, the risk of developing AD is the same between the 2 sexes But in the age group, the risk for women is 2 times that of men Men are more likely to die earlier of heart disease, hypertension, or diabetes, before they develop AD. Those that survive are assumed to have a more robust cardiovascular system, and that has been shown to be protective against dementia Women have a 70% higher risk of depression In the pre-feminist era, women had less education and less stimulating jobs; perhaps less social interactions APOe4 allele seems to carry a greater risk for women than men. There is some evidence to suggest it may interact with estrogen.
10
11 Reported at 2016 AAIC from a Mayo Clinic Jacksonville study of 1,600 pts in a brain bank review: Men are more likely to be: Misdiagnosed Underdiagnosed Affected at a younger age Have a shorter disease duration More likely to have symptoms involving speech and movement Less affected with memory symptoms early in the course of their disease
12
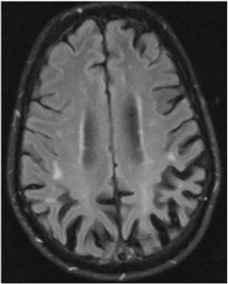
13 Dementia Types Cortical AD FTD PCA Vascular Small vessel ischemic Multi infarct Lewy Body PDD DLB Mixed Other CJD NPH HD WKS CTE
14
15 Definitions Alzheimer s Disease A new definition, proposed by a group of international experts The aim is to achieve earlier diagnosis, even before the onset of proven dementia Is now considered a disease of a continuum of stages involving degenerative and regressive or retrogressive stages of mental capacity
16 The progression of AD is separated into 3 phases: 1. Preclinical Stage The patient has no outward symptoms but imaging and biomarker tests identify changes that are occurring within the brain 2. Mild Cognitive Impairment Some outward signs of change begin to occur. There is some memory loss but patient is still capable of independent living. 3. Alzheimer s Disease These patients meet the established criteria for dementia Mild Moderate Severe
17
18
19
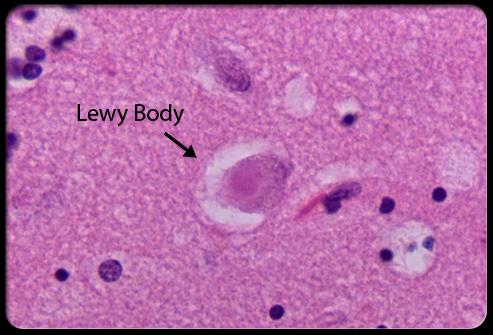
20 DLB Affects 1.3 million Americans is the most misdiagnosed dementia Early and accurate Dx can be life saving; i.e. avoid Rx that can: Exacerbate psychosis Precipitate NMS Needs to be distinguished from idiopathic PD Less response to dopaminergics More dopaminergic side-effects
21 DLB Diagnostic Criteria PROBABLE: Dementia (1 year rule) At least one of the following: Fluctuating attention and concentration Recurrent, well-formed visual hallucinations Spontaneous parkinsonian motor signs SUGGESTIVE: REM sleep behavioral disorder Severe neuroleptic sensitivity Low dopamine transport uptake in the basal ganglia (SPECT or PET)
22 PDD An accurate prior Dx of PD Dementia causing a decline in function severe enough to impair the patient in daily activities involving at least one of the following cognitive domains: Attention Executive function Visual-spatial ability Memory Language Apathy Personality change Hallucinations Delusions Excessive sleepiness
23
24
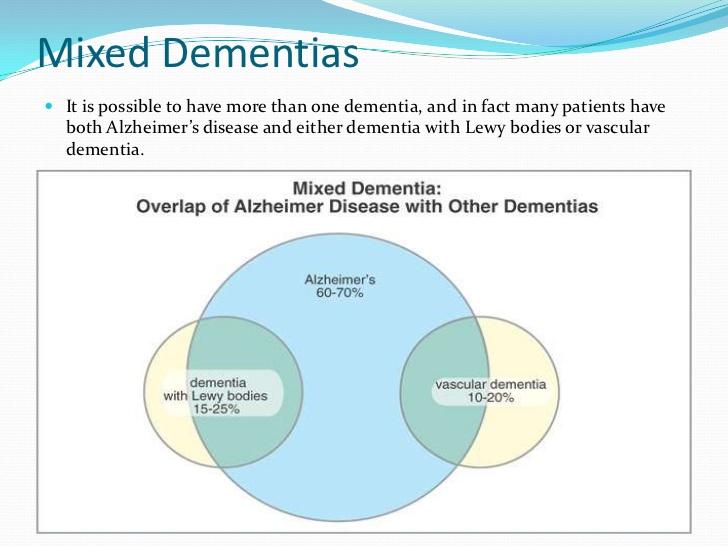
25 Mixed Dementia Are very common Specific proteinopathies predispose an individual to other protein misfoldings Vascular disease is a risk factor for the propagation of other known dementia pathologies
26 Mixed Dementia Lancet June 13, 2016 A post mortem study of 478 pts with AD showed: 39% had moderate to severe atherosclerosis 35% had arteriosclerosis Many pts with DLB were also found to have plaques and tangles Most pts with vascular dementia also had plaques and tangles Many pts with AD also were found to have Lewy Bodies
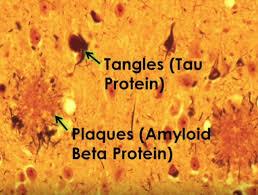
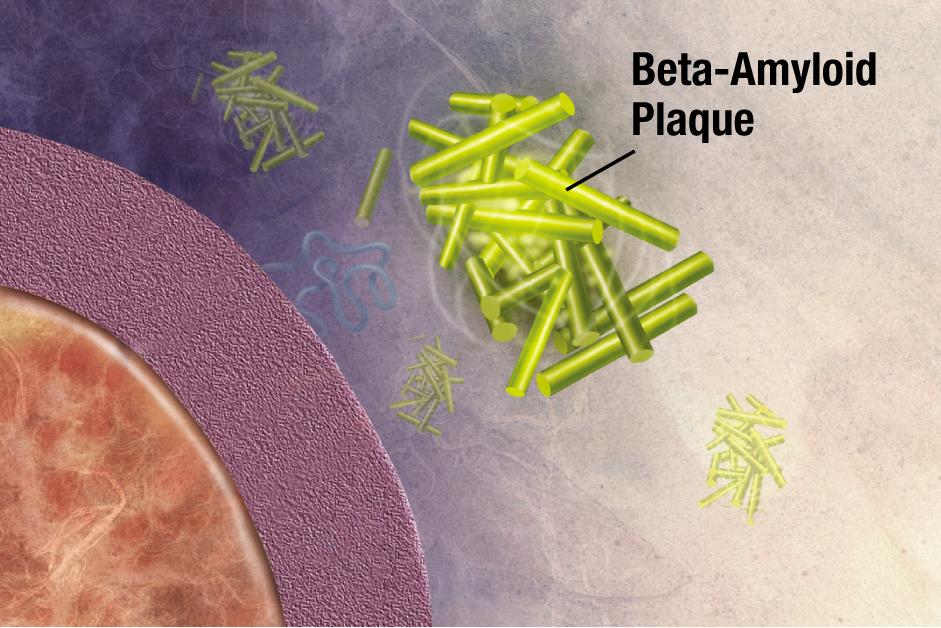
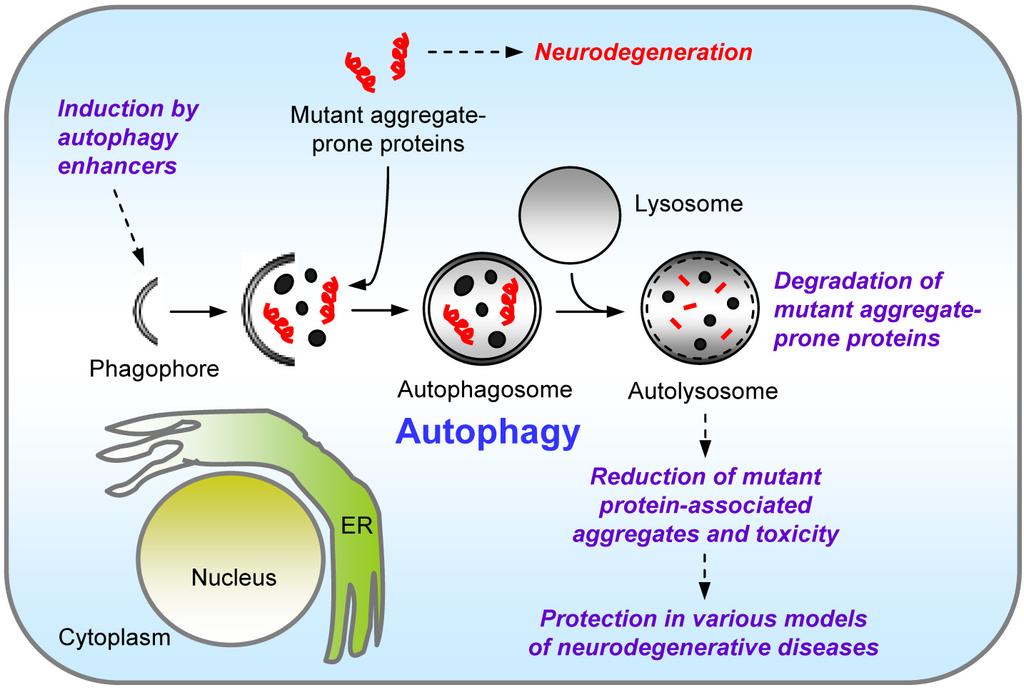
27 Pathologic Processes and Targets Beta Amyloid Tau Inflammation Immunological dysfunction Insulin resistance Mitochondrial dysfunction Autophagy
28
29
30
31
32
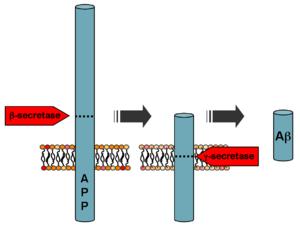
33 Flaws in the Amyloid Theory Some individuals have large amounts of amyloid loads but no AD There is a poor correlation between the amount of AB and the severity of the AD Numerous interventions have demonstrated amyloid removal: Vaccines Monoclonal antibodies that attack amyloid (Solanezumab) (Aducanumab) Beta secretase inhibitors Gamma secretase inhibitors *ALL OF THESE AGENTS FAILED IN CLINICAL TRIALS
34 Newest Research A soluble, 2-molecule aggregate (dimer) of beta-amyloid protein fragments may initiate the disease The soluble monomers and the insoluble plaque cores had no effect The dimers impaired memories of newly learned behaviors The dimers reduced the density of dendritic spines by 47%, thus directly altering synapses
35 Small, diffusible amyloid beta oligomers (amyloid derived diffusible ligands) are now thought to be highly toxic to neurons Neurological dysfunction evoked by ADDL s occurred well in advance of cellular degeneration. They seem to have an immediate effect on hippocampal signal transduction.
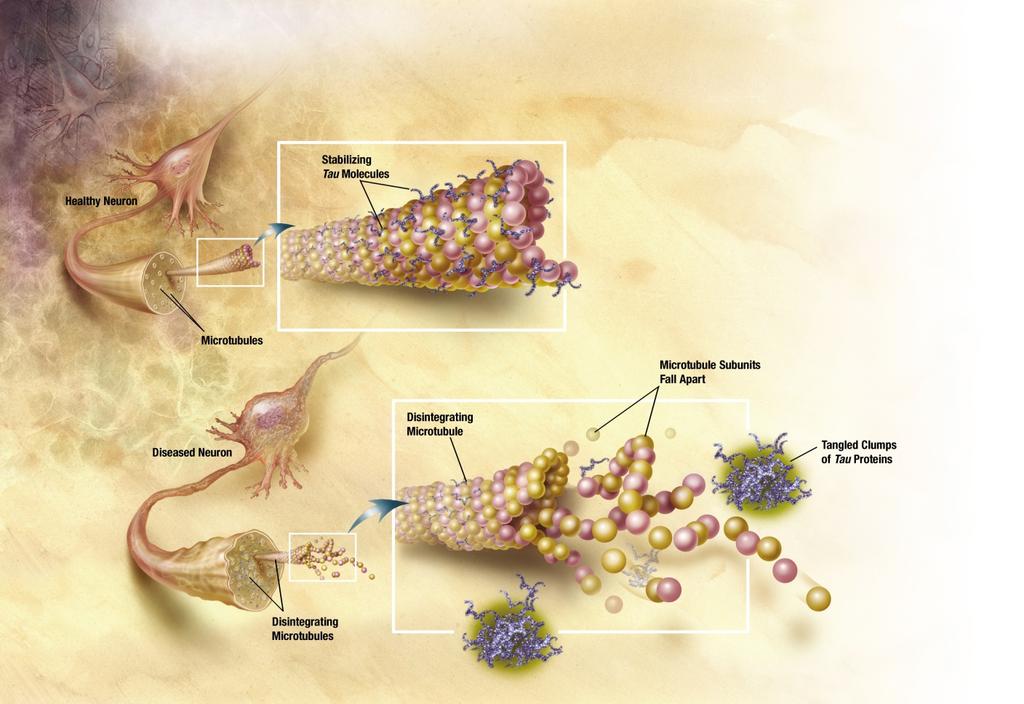
36 Tau
37 Tau is a collection of microtubule associated proteins (MAP) expressed from a single gene on chromosome 17
38 Tau is the basic component of neurofibrillary degeneration. Tau aggregation, in the form of filaments (either helical, twisted, or straight) have been implicated in more than 20 neurodegenerative disorders, including; AD, PSP, CBD, *FTD, and *FTDP-17.
39 NFT s are the result of degeneration of microtubules. Tangles occur when tau protein, which normally stabilizes microtubules, converts from a soluble to an insoluble form a process known as hyperhposphorylation.
40 Tau and Prions The tau protein in located on chromosome 17 This protein can be corrupted by strains of miscoded proteins that act very similarly to prions Prions are composed of normal proteins that are misfolded In the CNS, different misfoldings (prion strains) have been identified these can be transmitted like a virus and are strain specific Scientists took 28 patients with known tauopathies to post. Clinically, they had one of 5 forms that were identified by a unique tau-prion strand. In every patient with AD, the exact same tau-prion strand was identified. The same held true in other clinical tauopathies. Treatment options Antibodies to remove the prions Block prion movement between cells Stop cells from making new copies of the prion protein
41
42 UNFORTUNATELY A recently completed phase 3 trial of a potent tau aggregation inhibitor (LMTM) was negative. LMTM, (a derivative of methylene blue) failed to slow the rate of decline in cognition or in daily functioning
43 So Is amyloid beta: A culprit? A conspirator? A bystander? And where does tau fit in?
44 So It is now apparent, that removing amyloid from a clinically affected brain seems to offer no benefit Yet, there are many studies that show that amyloid deposition is a predictor of, and possibly a prerequisite for, future disease Recent studies have shown that neurodegeneration alone did not confer a significantly different risk of developing AD than the control group Yet, some studies suggest that levels of tau more closely coordinate with cognitive decline than do levels of amyloid
45 Lancet Neurology: 15: 10, Sept 2016 A+ N+ > A+ N- > SNAP = A-N+ The presence of both amyloid and neurodegeneration confers the highest risk Neurodegeneration seems to act as a compounding factor Neurodegeneration alone did not confer a significantly different risk from the control group SNAP: Suspected Non-Alzheimer s Pathology

46 It Takes 2 to Tango Tau and amyloid in combination seems to show a strong connection with the burdens of AD and declining function These misfolded proteins are thought to independently coexist with preferences in different parts of the brain
47
48 The brain does not exist in a vacuum. It dwells in our bodies where it is in constant conversation with our body s other great communicator, i.e. the immune system.
49 LilrB2 A molecule found to be important in the immune system has now been found to play an important role in the brain This molecule works at the synapse acting like a brake to slow the ferocity of the immune response Amyloid-beta has a high affinity for LilrB2 at the synapse thus, taking off the brake, allowing the immune response to deteriorate the synapse Therefore, blocking amyloid-beta from binding to LilbR2 may be a viable treatment strategy to prevent cognitive decline
50 C1q A protein typically associated with immune function was found to have a 300 fold uptick in prevalence in old brains compared to young This is seen especially at the synapses, and especially in the hippocampus Microglia produce C1q in the brain, and this protein is essential in initiating the complement system Astrocytes produce numerous other proteins that join C1q in the formation of the complement cascade as part of our immune response Buildup of C1q at the synapse may not be directly toxic, but it is thought to leave the brain vulnerable. When any number of stresses occur, the astrocytes can be triggered to release the other components and initiate the destructive cascade that injures/destroys the synapse. Work is ongoing to develop drugs that block this complement cascade ADDL s promote C1q deposition at the synapse
51 Solanezumab A humanized monoclonal antibody that preferentially binds to soluble forms of amyloid In preclinical studies it dramatically promoted amyloid clearance from the brain Recently released data from a phase 3 clinical trial showed that this agent FAILED to improve cognition or functional ability
52 Aducanumab Biogen monoclonal antibody that was just granted fast track designation Like previously studied monoclonals, it is thought to help clear the brain of beta-amyloid plaques Currently being studies in patients with early and mild forms of AD
53 IVIg 18 month GAP trial (gammaglobulin Alzheimer s partnership) Showed no significant difference in the rates of cognitive or functional decline compared to placebo (this in contrast to the highly favorable results suggested in the phase 2 trials)

54
55
56 Insulin Resistance Diabetes Doubles the risk for AD A meta-analysis of 19 longitudinal studies looked at the association of DM with relative risk for AD, vascular dementia, any dementia, and MCI. Their conclusion: AD 1.46 Vascular dementia 2.48 Any dementia 1.51 MCI 1.21
57 Insulin Resistance In pts > 65 years old Prevalence of DM: 8.5% Prevalence of Dementia: 6.4% It is estimated that Type II DM or abnormal fasting blood glucose may be present in up to 80% of patients with a diagnosis of AD It has been clearly demonstrated that patients with AD have decreased ability to metabolize glucose in the hippocampus and other areas of the brain
58 Insulin Resistance Ties back into the ADDL (amyloid-derived diffusible ligand) hypothesis ADDL s bind at the synapse and lead to a dramatic loss in the number of available insulin receptors High brain insulin levels also lead to insulin resistance Up to 30% of all adults > 60 years old may have insulin resistance and most are unaware Brain insulin levels may be 300x normal this can lead to insulin resistance, even with normal blood glucose levels
59 IDE (Insulin Degrading Enzyme) Is a protease that not only degrades insulin but also beta amyloid in fact, it appears to be the only protease involved in beta amyloid degradation. Beta-amyloid competes with insulin to be degraded by IDE. An increase in CNS insulin levels may inhibit beta amyloid degradation by IDE Therefore, optimized brain insulin levels promote beta amyloid clearance and thus may have a protective role in AD.
60 Strategies to Treat Insulin Resistance Diet low fat, low sugar, Mediterranean diet High fat, high sugar diets led to increased amyloid production Aerobic exercise Lower visceral (belly) fat Subcutaneous fat may actually be beneficial
61 Nasal Insulin - SNIFF study: NIA, USC, Wake Forest The Study of Nasal Insulin and the Fight Against Forgetfulness The results from a small preliminary study looked promising This ongoing study is investigation the effects that nasal insulin has on: Cognition, memory, and ADLs Entorhinal cortex and hippocampal atrophy CSF biomarkers
62 Could inducing ketosis to address brain glucose hypometabolism offer any benefit?
63 Revisiting Brain Inflammation in Alzheimer s Disease
64
65 Autophagy is the neuron s recycling system and it has been shown to be impaired in AD This can lead to inflammation and cell destruction In cerebral inflammation, microglia, (close cousins of pathogen eating macrophages), swarm around plaques and tangles This is thought to be helpful in gobbling up amyloid and damaged cells and cellular debris But, can this immunologic enthusiasm also cause harm to healthy cells? Conditions that are known to accelerate dementia such as head trauma and systemic infections are also known to cause inflammation
66 Most NSAI studies have shown no benefit in the treatment or prevention of AD, and one study actually suggested harm There is however a more recent study that suggested that naproxen showed benefit TREM 2 agents which suppress inflammatory responses by repression of microglia mediated cytokine production, are currently under investigation Specific IL-12 and IL-23 blockers are currently being investigated
67 Risk Factors Advancing age for every 5-year age group beyond 65, the percentage of patients with AD doubles Family history DM HTN Obesity Hypercholesterolemia in midlife Metabolic Syndrome Pts in their 40s with total cholesterol were 1.5 times more likely to develop AD than those with cholesterol less than 198
68 Risk Factors (cont) Downs Syndrome Head injury Decrease in exercise Heavy drinkers (more than 2 drinks per day) developed AD 4.8 years sooner Heavy smokers (more than 1 pack per day) developed AD 2.3 years sooner A cognitive complaint Unmarried in midlife Depression
69 Education Less than 12 years of education: 15% increased risk compared to those with years of education 35% increased risk compared to those with more than 15 years of education Is this due to an increase in cognitive reserve or due to social cofactors? Even when cofactors are taken into account, fewer years of education does increase the risk of developing AD. African Americans > Caucasians But this seems to be due to cofactors, particularly years of education,

70
71 Genetic Factors in the Development of Alzheimer s Disease Chromosome 1 mutations on the presenilin-2 gene Chromosome 14 mutations on the presenilin-1 (gamma secretase) gene Chromosome 19 ApoE allele Chromosome 21 mutations on the APP gene
72 Reasons for Optimism? Are we seeing less dementia than expected? Studies now suggest that the dementia rate is decreasing in some wealthy countries CFAS II (Cognitive Function in Aging Study) suggested that the dementia prevalence in the UK was lower than previously expected Lancet, July 11, 2013 David Green published research in Legacy that showed similar declines in England, Sweden, Germany, and the Netherlands
73 In the US, a multi-year study funded by the federal government followed up on new dementia cases, in people over the age of 60, in 5- year blocks of time Baseline rate for comparison % drop in new cases % drop in new cases % drop in new cases * In addition, the average age for dementia diagnosis rose from 80yo in the first group to 85yo in the last one.
74 Prevention AD is not a fate without the possibility of change We have now identified modifiable risk factors. If behavior can be altered or actions be taken early enough, some targeted interventions can have a major impact on delaying or preventing AD symptoms in vulnerable individuals. Since age is the #1 risk factor for AD, it is thought that delaying the onset of AD by 5 years may prevent 50% of all cases
75 Exercise and Diet FINGER study: a 2-year study of 1,260 participants aged randomized into 2 groups. The control group received regular medical attention and the study group had Nutritional guidance Management of heart health risk factors Regular exercise (cardiovascular and weight training) Diet heavy in fruits, vegetables, and fish and low in saturated fats Conclusion: after 2 years the intervention group scored significantly better on a comprehensive cognitive exam and on specific tests of memory, executive function, planning, judgment, problem-solving, and cognitive processing speed A 7-year extended follow-up is ongoing and will measure the incidence of AD in both groups
76 Exercise and Diet Another recent study published in the Annals of Internal Medicine, Feb 2013: 20,000 pts enrolled in their 40 s and 50 s were followed into their 70 s and 80 s. Conclusion: patients who were physically fit / physically active in mid-life were 40% less likely to develop dementia or AD compared to their counterparts who were not Annals of Internal Medicine, 2006, Volume 134, pp 73-81: Looked at 1,740 participants over the age of 65. Conclusion: Those who exercised vigorously (3-4 times per week) had a 34% reduction in the development of dementia in elderly persons compared with those who didn t
77 AAIC 2016 Data - A Study of 3536 Patients Concluded: Vascular intervention does not appear to affect dementia incidence in patients who are cognitively healthy
78 On the Other Hand Neurology 86:20 May 17, 2016 LTPA Leisure Time Physical Activity Was shown in this study of 1228 pts to be protective against decline in cognitive performance Low level LTPA was associated with a greater level of cognitive performance decline especially in processing speed and episodic memory
79
80 Downstream Benefits? SSRIs 11% of US adult population 23% of women in their 40 s and 50 s Can reduce the amyloid-beta burden in key regions of the brain (Science, May 2014) Specifically, citalopram (which is the most selective for increasing serotonin) Patients who have used SSRIs during a 5-year period have fewer amyloid deposits compared to a control group. Activation of serotonin receptors reduces amyloid-beta production and activates intracellular signaling pathways. (Proceedings of the National Academy of Science, 2011)
81 Statins Statins Over 15 million Americans are currently on statins NIH guidelines indicate that 35 million Americans should be In February 2012, the FDA issued a statement based on anecdotal reports warning of possible adverse mental affects associated with statin use. * BUT Annals of Internal Medicine, Nov 19, 2013 concluded in a well designed study that statins are NOT linked to memory loss or dementia. Moreover Rotterdam study, 2008 Prospective study of almost 7,000pts followed for years showed that statins are associated with a reduced risk of AD, regardless of lipophilicity. Non-statin cholesterol lowering agents were not. A Johns Hopkins study, published in Mayo Clinic Proceedings, Oct 2013 Concluded that the long-term use of statins reduced dementia risk by 29%. High potency (artorvastatin and rosuvastatin) seems to be more important than solubiilty. The conclusion from an article published in Circulation were that the benefits of statins largely outweighed the risks
82 Metformin The most commonly prescribed drug for the treatment of type-2 DM Presentation to the Alzheimer s Association International Conference, 2013 Compared to people taking sulfonylureas, those taking metformin has a 20% reduced risk of developing AD over the 5 year study period This was an observational, retrospective, population-based study. It showed an association, NOT cause and effect. On the other hand, another study showed that metformin use overactivates AMPK (adenosine monophosphate activated protein kinase), and enzyme that promotes Alzheimer changes (Neuron, 2013) J. Alzheimer s Dis 2014; 41(1): 61-8 Controlling for age, education, diabetes duration FBS, and vascular and nonvascular risk factors metformin use showed a significant inverse association with cognitive impairment in longitudinal analysis, with use for more than 6 years showing the lowest incidents of cognitive impairment
83 The Importance of Early Detection More and more data is consistent with the paradigm that interventions aimed at preventing cognitive decline need to occur before symptoms manifest Amyloid begins its neural stranglehold up to 30 years prior to symptom onset If the pathologic substrates of AD can be removed early in the process, can Alzheimer s be delayed? Be prevented? Perhaps combination therapies with early pharmacologic interventions to remove or prevent amyloid, tau, and inflammation along with lifestyle modifications and other preventative strategies can make a difference.
84 Biomarkers Amyloid Measures Neuronal Injury Measures Other Preclinical Screens
 Florbetapir")
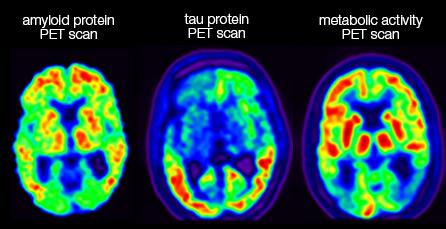
85 Amyloid Measures Amyloid PET Brain Imaging PIB (Pittsburgh Compound B) Florbetapir (Amyvid)
86 Amyloid Measures Amyloid PET If a person with dementia does not have amyloid buildup, then the cause is very unlikely to be AD If amyloid buildup is seen in a patient with memory impairment, then the likelihood that this symptom is secondary to AD is significantly increased If a person without memory complaints has amyloid buildup, it does NOT mean that they will develop AD
87 Amyloid Measures CSF Analysis Decrease amyloid beta 42
88 Amyloid Measures Non-Invasive Detetection of Beta- Amyloid in the Retina A very promising development presented at last year s AAIC by the Australian National Science Agency In preliminary published results in 40 patients, the test could differentiate between AD and non-ad with 100% sensitivity and 80.6% specificity This optical imaging exam appears to detect changes that occur years prior to clinical diagnosis The process involves staining amyloid plaques in the retina with curcumin (a component of the spice turmeric)

89
90 Amyloid Measures ADx Imaging Alzeca Biosciences study published in Journal of Alz Disease ADx is a nanoparticle that can be given IV that can carry an encapsulated agent across the BBB to bind precisely to amyloid plaques Researches were able to obtain precise, high resolution images of amyloid plaques using conventional MRI If substantiated in larger studies, this would result in amyloid detection being more available and affordable

91 Neuronal Injury Measures FDG-PET
92 Neuronal Injury Measures Increase CSF phosophorylated tau
93 Neuronal Injury Measures Specific Lipid Panels - Another Promising Biomarker Researchers looked at 4,600 potential metabolites of CNS cell breakdown They discovered that 10 lipids were significantly altered in the plasma of cognitively normal adults who would then go on to develop the clinical symptoms of AD It is thought that this 10-lipid phospholipid biomarker panel reflects the breakdown of neural cell membranes in those individuals destined to develop advanced MCI or AD Interestingly, APOe4 was not one of these lipids This panel predicted clinical AD based on the patient s performance on cognitive skills tests, rather than distinguishing among causes of impairment such as vascular dementia vs AD This is based on work being done at the Rochester Medical Center

94 Neuronal Injury Measures
95
96 Other Preclinical Screens UPSIT (University of Pennsylvania Smell Identification Test) Recent research from Harvard was presented at the 2014 AAIC in Denmark Inexpensive and easy to administer Poor UPSIT scores correlated with lower cognitive scores and was confirmed by other physical markers of AD, including atrophy (which represents neurodegeneration) and amyloid deposits A second study from the UFCOM found that among 757 participants, lower scores on UPSIT were associated with the transition to dementia and AD
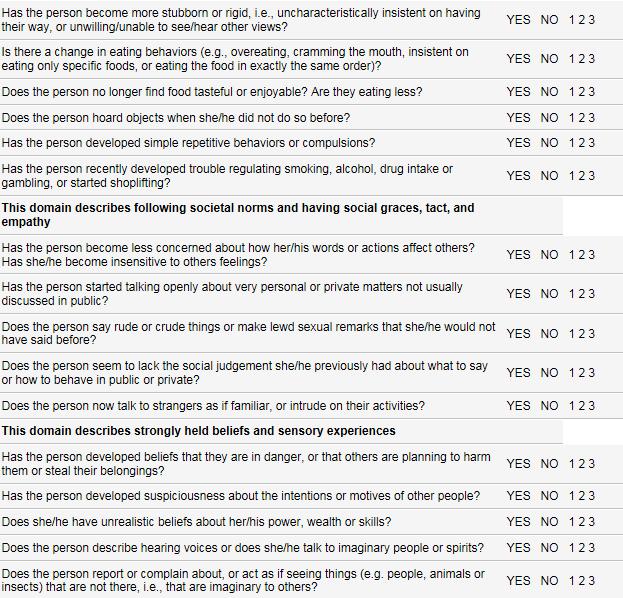
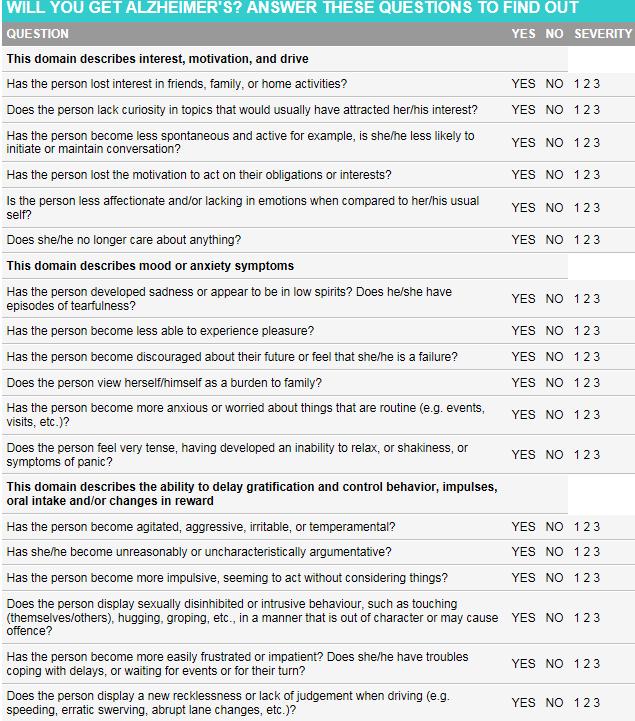
97 Other Preclinical Screens Mild Behavioral Impairment (MBI) Is a predictor of neurodegeneration and progression to dementia AMJ Psychiatry [5] showed: Agitation > apathy > anxiety > irritability > depression Predicted future dementia
98
99 Current Treatments Cognex (tacrine) Exelon (rivastigmine) Namenda (memantine) Aricept (donepezil) Reminyl (galantamine) Cognex is a registered trademark of Warner-Lambert Company. Aricept is a registered trademark of Eisai Company Ltd. Exelon is a registered trademark of Novartis AG. Reminyl is a registered trademark of Janssen Pharmaceutica. Namenda is a registered trademark of Forest Laboratories Inc.
100 Benefits of Combined Cholinesterase Inhibitor and Memantine Treatment in Moderate-Severe AD Alzheimer s Dementia, May 2013 Conclusion: Treatment with combination therapy produces consistent benefits that appear to increase over time and that are beyond those of cholinesterase treatment alone JAMA Conclusion: Combination therapy showed positive results in all measures, i.e. cognition, global status, function, and behavior
101 The Future Nasal insulin SNIFF study: utilizing intranasal insulin did seem to improve glucose metabolism in the hippocampus and frontal lobes without affecting blood glucose levels Anti-APOe monoclonal antibodies Is APOe a therapeutic target? Blood transfusions Blood from young mice transfused into older mice seems to lead to better cognitive performance (Science, Sept 2014) Brain derived neurotropic factor Neural stem cells Can up-regulate neprilysin (a protein that breaks down beta-amyloid) TC-2153 (Journal of Alzheimer s Disease, May 2014) Reversed AD symptoms in mice Blocks the effects of STEP (striatal enriched tyrosine phosphate); STEP prevents synaptic strengthening in the brain
102
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
The Aging Brain The Aging Brain
 The Aging Brain The Aging Brain R. Scott Turner, MD, PhD Director, Memory Disorders Program Professor, Department of Neurology Georgetown University Washington, DC memory.georgetown.edu rst36@georgetown.edu
The Aging Brain The Aging Brain R. Scott Turner, MD, PhD Director, Memory Disorders Program Professor, Department of Neurology Georgetown University Washington, DC memory.georgetown.edu rst36@georgetown.edu
Alzheimer's Disease A mind in darkness awaiting the drink of a gentle color.
 Alzheimer's Disease A mind in darkness awaiting the drink of a gentle color. Mary ET Boyle, Ph. D. Department of Cognitive Science UCSD Gabriel García Márquez One Hundred Years of Solitude Alois Alzheimer
Alzheimer's Disease A mind in darkness awaiting the drink of a gentle color. Mary ET Boyle, Ph. D. Department of Cognitive Science UCSD Gabriel García Márquez One Hundred Years of Solitude Alois Alzheimer
Alzheimer s Disease Update: From Treatment to Prevention
 Alzheimer s Disease Update: From Treatment to Prevention Jeffrey M. Burns, MD Edward H. Hashinger Professor of Medicine Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science
Alzheimer s Disease Update: From Treatment to Prevention Jeffrey M. Burns, MD Edward H. Hashinger Professor of Medicine Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science
Alzheimer s Disease without Dementia
 Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diabetes Mellitus and Dementia. Andrea Shelton & Adena Zadourian
 Diabetes Mellitus and Dementia Andrea Shelton & Adena Zadourian Abstract Diabetes mellitus increases the risk for developing dementia...but there is inconsistency with the subtypes of dementia Diabetes
Diabetes Mellitus and Dementia Andrea Shelton & Adena Zadourian Abstract Diabetes mellitus increases the risk for developing dementia...but there is inconsistency with the subtypes of dementia Diabetes
Dementia and Healthy Ageing : is the pathology any different?
 Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.
, also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.") CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
Alzheimer s Disease. Fact Sheet. Fact Sheet. Fact Sheet. What Causes AD?
 2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Neuro degenerative PET image from FDG, amyloid to Tau
 Neuro degenerative PET image from FDG, amyloid to Tau Kun Ju Lin ( ) MD, Ph.D Department of Nuclear Medicine and Molecular Imaging Center, Chang Gung Memorial Hospital ( ) Department of Medical Imaging
Neuro degenerative PET image from FDG, amyloid to Tau Kun Ju Lin ( ) MD, Ph.D Department of Nuclear Medicine and Molecular Imaging Center, Chang Gung Memorial Hospital ( ) Department of Medical Imaging
8/14/2018. The Evolving Concept of Alzheimer s Disease. Epochs of AD Research. Diagnostic schemes have evolved with the research
 The Evolving Concept of Alzheimer s Disease David S. Geldmacher, MD, FACP Warren Family Endowed Chair in Neurology Department of Neurology UAB School of Medicine Epochs of AD Research Epoch Years Key Event
The Evolving Concept of Alzheimer s Disease David S. Geldmacher, MD, FACP Warren Family Endowed Chair in Neurology Department of Neurology UAB School of Medicine Epochs of AD Research Epoch Years Key Event
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Claims & Underwriting. You already told us that story! Maria C. Carrillo, Ph.D. Sr. Director, Medical & Scientific Relations Alzheimer s Association
 Claims & Underwriting Alzheimer s & Cognitive Impairment: You already told us that story! Maria C. Carrillo, Ph.D. Sr. Director, Medical & Scientific Relations Alzheimer s Association 1 OVERVIEW Impact
Claims & Underwriting Alzheimer s & Cognitive Impairment: You already told us that story! Maria C. Carrillo, Ph.D. Sr. Director, Medical & Scientific Relations Alzheimer s Association 1 OVERVIEW Impact
Imaging of Alzheimer s Disease: State of the Art
 July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
#CHAIR2015. Miami, Florida. September 24 26, JW Marriott Miami. Sponsored by
 #CHAIR2015 September 24 26, 2015 JW Marriott Miami Miami, Florida Sponsored by Case Challenge Workshop Alzheimer s Disease Anand Kumar, MD University of Illinois at Chicago, College of Medicine Chicago,
#CHAIR2015 September 24 26, 2015 JW Marriott Miami Miami, Florida Sponsored by Case Challenge Workshop Alzheimer s Disease Anand Kumar, MD University of Illinois at Chicago, College of Medicine Chicago,
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
Fact Sheet Alzheimer s disease
 What is Alzheimer s disease Fact Sheet Alzheimer s disease Alzheimer s disease, AD, is a progressive brain disorder that gradually destroys a person s memory and ability to learn, reason, make judgements,
What is Alzheimer s disease Fact Sheet Alzheimer s disease Alzheimer s disease, AD, is a progressive brain disorder that gradually destroys a person s memory and ability to learn, reason, make judgements,
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Dementia. Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 Dementia Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine What is Dementia? Dementia is a general term referring to a decline in cognitive/mental functioning; this decline
Dementia Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine What is Dementia? Dementia is a general term referring to a decline in cognitive/mental functioning; this decline
11/12/2018. Acknowledgements. Risk factors for Alzheimer s disease
 Is it Possible to Reduce My Risk for Alzheimer's Disease? An Overview of Current Risk Reduction Strategies Dorothy Farrar Edwards PhD, Professor of Medicine and Kinesiology Core Leader: Outreach, Recruitment
Is it Possible to Reduce My Risk for Alzheimer's Disease? An Overview of Current Risk Reduction Strategies Dorothy Farrar Edwards PhD, Professor of Medicine and Kinesiology Core Leader: Outreach, Recruitment
WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together. Presented by
 WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together Presented by Our agenda for today Understanding behavioral symptoms in people living with dementia Briefly review key strategies
WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together Presented by Our agenda for today Understanding behavioral symptoms in people living with dementia Briefly review key strategies
Understanding Symptoms, Causes, and Risks for Alzheimer s Disease
 Understanding Symptoms, Causes, and Risks for Alzheimer s Disease Gene E. Alexander, Ph.D., Professor of Psychology, Neuroscience, and Physiological Sciences; Director, Brain Imaging, Behavior & Aging
Understanding Symptoms, Causes, and Risks for Alzheimer s Disease Gene E. Alexander, Ph.D., Professor of Psychology, Neuroscience, and Physiological Sciences; Director, Brain Imaging, Behavior & Aging
Type 2 Diabetes and Brain Disease in Older Adults. Erin L. Abner, PhD, MPH Asst. Professor University Of Kentucky
 Type 2 Diabetes and Brain Disease in Older Adults Erin L. Abner, PhD, MPH Asst. Professor University Of Kentucky Disclosures to Participants Requirements for Successful Completion: For successful completion,
Type 2 Diabetes and Brain Disease in Older Adults Erin L. Abner, PhD, MPH Asst. Professor University Of Kentucky Disclosures to Participants Requirements for Successful Completion: For successful completion,
Introduction, use of imaging and current guidelines. John O Brien Professor of Old Age Psychiatry University of Cambridge
 Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Objective 4/22/2019. Interaction of Cardiovascular Disease and Alzheimer s Disease: Implications for Cardiopulmonary Rehabilitation.
 Interaction of Cardiovascular Disease and Alzheimer s Disease: Implications for Cardiopulmonary Rehabilitation Dereck Salisbury, PhD Assistant Professor, Clinical Exercise Physiologist Director: Laboratory
Interaction of Cardiovascular Disease and Alzheimer s Disease: Implications for Cardiopulmonary Rehabilitation Dereck Salisbury, PhD Assistant Professor, Clinical Exercise Physiologist Director: Laboratory
Interaction of Cardiovascular Disease and Alzheimer s Disease: Implications for Cardiopulmonary Rehabilitation
 Interaction of Cardiovascular Disease and Alzheimer s Disease: Implications for Cardiopulmonary Rehabilitation Dereck Salisbury, PhD Assistant Professor, Clinical Exercise Physiologist Director: Laboratory
Interaction of Cardiovascular Disease and Alzheimer s Disease: Implications for Cardiopulmonary Rehabilitation Dereck Salisbury, PhD Assistant Professor, Clinical Exercise Physiologist Director: Laboratory
TUESDAY, MARCH 26, 2019 WEDNESDAY, MARCH 27, 2019
 KEY: PRE CONFERENCE SYMPOSIUM SPONSORED SYMPOSIUM SYMPOSIUM PLENARY LECTURE FORUM OTHER EVENT *PRE-REGISTRATION IS REQUIRED FOR THE INFORMAL NETWORKING WITH PROFESSOR LUNCH SESSION TUESDAY, MARCH 26, 2019
KEY: PRE CONFERENCE SYMPOSIUM SPONSORED SYMPOSIUM SYMPOSIUM PLENARY LECTURE FORUM OTHER EVENT *PRE-REGISTRATION IS REQUIRED FOR THE INFORMAL NETWORKING WITH PROFESSOR LUNCH SESSION TUESDAY, MARCH 26, 2019
Sleep Cycle Shift and its effects on Cognitive Function
 Sleep Cycle Shift and its effects on Cognitive Function MARY ET BOYLE, PH. D. DEPARTMENT OF COGNITIVE SCIENCE UCSD Sleep wake cycle is regulated by the circadian system. Superchiasmatic Nucleus in the
Sleep Cycle Shift and its effects on Cognitive Function MARY ET BOYLE, PH. D. DEPARTMENT OF COGNITIVE SCIENCE UCSD Sleep wake cycle is regulated by the circadian system. Superchiasmatic Nucleus in the
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
TUESDAY, MARCH 26, 2019 WEDNESDAY, MARCH 27, 2019
 KEY: PRE CONFERENCE SYMPOSIUM SPONSORED SYMPOSIUM SYMPOSIUM PLENARY LECTURE FORUM OTHER EVENT *PRE-REGISTRATION IS REQUIRED FOR THE INFORMAL NETWORKING WITH PROFESSOR LUNCH SESSION TUESDAY, MARCH 26, 2019
KEY: PRE CONFERENCE SYMPOSIUM SPONSORED SYMPOSIUM SYMPOSIUM PLENARY LECTURE FORUM OTHER EVENT *PRE-REGISTRATION IS REQUIRED FOR THE INFORMAL NETWORKING WITH PROFESSOR LUNCH SESSION TUESDAY, MARCH 26, 2019
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Stephen Salloway, M.D., M.S. Disclosure of Interest
 Challenges in the Early Diagnosis of Alzheimer s Disease Stephen Salloway, MD, MS Professor of Neurology and Psychiatry Alpert Medical School, Brown University 2 nd Annual Early Alzheimer s Educational
Challenges in the Early Diagnosis of Alzheimer s Disease Stephen Salloway, MD, MS Professor of Neurology and Psychiatry Alpert Medical School, Brown University 2 nd Annual Early Alzheimer s Educational
What s New in Dementia?
 What s New in Dementia? Howard Rosen Professor, Department of Neurology UCSF and Aging Center Disclosure Biogen pharmaceuticals Small grant for clinical trials planning Dementia is a growing source of
What s New in Dementia? Howard Rosen Professor, Department of Neurology UCSF and Aging Center Disclosure Biogen pharmaceuticals Small grant for clinical trials planning Dementia is a growing source of
Brain Health and Risk Factors for Dementia
 Welcome To Brain Health and Risk Factors for Dementia Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa April 4, 2018 10:00 11:00
Welcome To Brain Health and Risk Factors for Dementia Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa April 4, 2018 10:00 11:00
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
The role of the vascular system in dementia
 The role of the vascular system in dementia James AR Nicoll Professor of Neuropathology, University of Southampton Consultant Neuropathologist, Southampton General Hospital What does the vascular system
The role of the vascular system in dementia James AR Nicoll Professor of Neuropathology, University of Southampton Consultant Neuropathologist, Southampton General Hospital What does the vascular system
3/7/2017. Alzheimer s and Dementia Research: An Advanced Discussion. Alzheimer s and Dementia Research: An Advanced Discussion
 Alzheimer s and Dementia Research: An Advanced Discussion Brad Boeve, MD Department of Neurology Mayo Clinic Alzheimer s and Dementia Research: An Advanced Discussion Theoretical Constructs in Aging/Dementia
Alzheimer s and Dementia Research: An Advanced Discussion Brad Boeve, MD Department of Neurology Mayo Clinic Alzheimer s and Dementia Research: An Advanced Discussion Theoretical Constructs in Aging/Dementia
Memory Matters: Learning Objectives: Synapses, Age, and Health. Neuronal Synapses DISCLOSURE DECLARATION. Cognition and Normal Aging
 Standard Deviations from Mean Memory Matters: Preventing and Treating Late-Life, Cognitive Decline Daniel L. Murman, MD, MS Director, Behavioral and Geriatric Neurology Program Professor & Vice Chair,
Standard Deviations from Mean Memory Matters: Preventing and Treating Late-Life, Cognitive Decline Daniel L. Murman, MD, MS Director, Behavioral and Geriatric Neurology Program Professor & Vice Chair,
ALZHEIMER S DISEASE FACTOIDS & STATISTICS
 ALZHEIMER S DISEASE FACTOIDS & STATISTICS ~ 4 million affected in US alone 6-8% if 65+ years old, 30-50% if 80+ By 2030, in US >65 million people >65+ (---> ~14 million with AD) AD is one of the top 10
ALZHEIMER S DISEASE FACTOIDS & STATISTICS ~ 4 million affected in US alone 6-8% if 65+ years old, 30-50% if 80+ By 2030, in US >65 million people >65+ (---> ~14 million with AD) AD is one of the top 10
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
Drug Update. Treatments for Cognitive Impairment in the Older Adult. William Solan, M.D. Karen Sanders, Ph.D. Northwest Hospital Seattle
 Drug Update Treatments for Cognitive Impairment in the Older Adult William Solan, M.D. Karen Sanders, Ph.D. Northwest Hospital Seattle Current Drug Treatments for Alzheimer s Disease Cholinesterase Inhibitors:
Drug Update Treatments for Cognitive Impairment in the Older Adult William Solan, M.D. Karen Sanders, Ph.D. Northwest Hospital Seattle Current Drug Treatments for Alzheimer s Disease Cholinesterase Inhibitors:
TUESDAY, MARCH 28, 2017 WEDNESDAY, MARCH 29, 2017 WELCOME RECEPTION (VIENNA CITY HALL)
") KEY: PRE CONFERENCE SYMPOSIUM SPONSORED SYMPOSIUM SYMPOSIUM PLENARY LECTURE FORUM OTHER EVENT *PRE-REGISTRATION IS REQUIRED FOR THE INFORMAL NETWORKING WITH PROFESSOR LUNCH SESSION TUESDAY, MARCH 28, 2017
KEY: PRE CONFERENCE SYMPOSIUM SPONSORED SYMPOSIUM SYMPOSIUM PLENARY LECTURE FORUM OTHER EVENT *PRE-REGISTRATION IS REQUIRED FOR THE INFORMAL NETWORKING WITH PROFESSOR LUNCH SESSION TUESDAY, MARCH 28, 2017
Moving Targets: An Update on Diagnosing Dementia in the Clinic
 Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Overview of neurological changes in Alzheimer s disease. Eric Karran
 Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Personal Reflections on the Design and Delivery of Services to Those with Cognitive Disorders
 Personal Reflections on the Design and Delivery of Services to Those with Cognitive Disorders Dr. David B. Hogan Brenda Strafford Foundation Chair in Geriatric Medicine University of Calgary None to declare
Personal Reflections on the Design and Delivery of Services to Those with Cognitive Disorders Dr. David B. Hogan Brenda Strafford Foundation Chair in Geriatric Medicine University of Calgary None to declare
TGF-ß1 pathway as a new pharmacological target for neuroprotection in AD. Filippo Caraci
 Department of Clinical and Molecular Biomedicine Section of Pharmacology and Biochemistry Department of Educational Sciences University of Catania TGF-ß1 pathway as a new pharmacological target for neuroprotection
Department of Clinical and Molecular Biomedicine Section of Pharmacology and Biochemistry Department of Educational Sciences University of Catania TGF-ß1 pathway as a new pharmacological target for neuroprotection
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
New life Collage of nursing Karachi
 New life Collage of nursing Karachi Presenter: Zafar ali shah Faculty: Raja khatri Subject: Pathophysiology Topic :Alzheimer s Disease Post RN BScN semester 2 nd Objective Define Alzheimer s Describe pathophysiology
New life Collage of nursing Karachi Presenter: Zafar ali shah Faculty: Raja khatri Subject: Pathophysiology Topic :Alzheimer s Disease Post RN BScN semester 2 nd Objective Define Alzheimer s Describe pathophysiology
9.01 Introduction to Neuroscience Fall 2007
 MIT OpenCourseWare http://ocw.mit.edu 9.01 Introduction to Neuroscience Fall 2007 For information about citing these materials or our Terms of Use, visit: http://ocw.mit.edu/terms. 9.01 Recitation (R02)
MIT OpenCourseWare http://ocw.mit.edu 9.01 Introduction to Neuroscience Fall 2007 For information about citing these materials or our Terms of Use, visit: http://ocw.mit.edu/terms. 9.01 Recitation (R02)
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
Dementia Basics. Welcome! What to expect and how to handle a dementia diagnosis. In partnership with Scripps Health.
 Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
! slow, progressive, permanent loss of neurologic function.
 UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
2018 ALZHEIMER S DISEASE FACTS AND FIGURES. Includes a Special Report on the Financial and Personal Benefits of Early Diagnosis
 2018 ALZHEIMER S DISEASE FACTS AND FIGURES Includes a Special Report on the Financial and Personal Benefits of Early Diagnosis About this report 2018 Alzheimer s Disease Facts and Figures is a statistical
2018 ALZHEIMER S DISEASE FACTS AND FIGURES Includes a Special Report on the Financial and Personal Benefits of Early Diagnosis About this report 2018 Alzheimer s Disease Facts and Figures is a statistical
Cheyenne 11/28 Neurological Disorders II. Transmissible Spongiform Encephalopathy
 Cheyenne 11/28 Neurological Disorders II Transmissible Spongiform Encephalopathy -E.g Bovine4 Spongiform Encephalopathy (BSE= mad cow disease), Creutzfeldt-Jakob disease, scrapie (animal only) -Sporadic:
Cheyenne 11/28 Neurological Disorders II Transmissible Spongiform Encephalopathy -E.g Bovine4 Spongiform Encephalopathy (BSE= mad cow disease), Creutzfeldt-Jakob disease, scrapie (animal only) -Sporadic:
Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre
 Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre Today Introduction to CT Introduction to MRI Introduction to nuclear medicine Imaging the dementias The Brain ~ 1.5
Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre Today Introduction to CT Introduction to MRI Introduction to nuclear medicine Imaging the dementias The Brain ~ 1.5
What We Can Do To Prevent or Reduce the Risk for Dementia
 What We Can Do To Prevent or Reduce the Risk for Dementia Colloquium on Health and Wellness October 10 th, 2018 Frank M. Longo, MD, PhD Professor and Chair Department of Neurology and Neurological Sciences
What We Can Do To Prevent or Reduce the Risk for Dementia Colloquium on Health and Wellness October 10 th, 2018 Frank M. Longo, MD, PhD Professor and Chair Department of Neurology and Neurological Sciences
A Dynamic Model of Care for Late Onset Cognitive Impairment. Linda CW Lam Department of Psychiatry The Chinese University of Hong Kong
 A Dynamic Model of Care for Late Onset Cognitive Impairment Linda CW Lam Department of Psychiatry The Chinese University of Hong Kong Outline The pathogenesis of Late life cognitive impairment A framework
A Dynamic Model of Care for Late Onset Cognitive Impairment Linda CW Lam Department of Psychiatry The Chinese University of Hong Kong Outline The pathogenesis of Late life cognitive impairment A framework
UNDERSTANDING ALZHEIMER S AND DEMENTIA
 UNDERSTANDING ALZHEIMER S AND DEMENTIA Geri T., living with Alzheimer's, and her husband and care partner, Jim T. THE IMPACT OF ALZHEIMER S AND DEMENTIA Currently, an estimated 50 million people worldwide
UNDERSTANDING ALZHEIMER S AND DEMENTIA Geri T., living with Alzheimer's, and her husband and care partner, Jim T. THE IMPACT OF ALZHEIMER S AND DEMENTIA Currently, an estimated 50 million people worldwide
Alzheimer s Disease - Dementia
 - Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
- Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
Alzheimer s disease is an
 Alzheimer s Disease FACT SHEET Alzheimer s disease is an irreversible, progressive brain disease that slowly destroys memory and thinking skills, and eventually even the ability to carry out the simplest
Alzheimer s Disease FACT SHEET Alzheimer s disease is an irreversible, progressive brain disease that slowly destroys memory and thinking skills, and eventually even the ability to carry out the simplest
Diagnosis before NIA AA The impact of FDG PET in. Diagnosis after NIA AA Neuropathology and PET image 2015/10/16
 The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
Chapter 15: Late Life and Psychological Disorders
 \ Chapter 15: Late Life and Psychological Disorders 1. Ageism refers to a. the physical deterioration that accompanies old age. b. the intellectual deterioration that frequently occurs as a person ages.
\ Chapter 15: Late Life and Psychological Disorders 1. Ageism refers to a. the physical deterioration that accompanies old age. b. the intellectual deterioration that frequently occurs as a person ages.
Evaluation and Treatment of Dementia
 Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Dementia Past, Present and Future
 Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Neuroinflammation in preclinical AD: in vivo evidence
 Neuroinflammation in preclinical AD: in vivo evidence Barbara Bendlin, PhD Assistant Professor UW-Madison Dept. of Medicine, Geriatrics bbb@medicine.wisc.edu Overview Background Preclinical effects of
Neuroinflammation in preclinical AD: in vivo evidence Barbara Bendlin, PhD Assistant Professor UW-Madison Dept. of Medicine, Geriatrics bbb@medicine.wisc.edu Overview Background Preclinical effects of
Regulatory Challenges across Dementia Subtypes European View
 Regulatory Challenges across Dementia Subtypes European View Population definition including Early disease at risk Endpoints in POC studies Endpoints in pivotal trials 1 Disclaimer No CoI The opinions
Regulatory Challenges across Dementia Subtypes European View Population definition including Early disease at risk Endpoints in POC studies Endpoints in pivotal trials 1 Disclaimer No CoI The opinions
Update on functional brain imaging in Movement Disorders
 Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen. Dr. Michael Plopper. Dr. Guerry Peavy
 1 Anne State 2 3 Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen Dr. Michael Plopper Dr. Guerry Peavy 4 Michael Lobatz, MD Medical Director, Neurosciences Medical Director, Rehabilitation
1 Anne State 2 3 Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen Dr. Michael Plopper Dr. Guerry Peavy 4 Michael Lobatz, MD Medical Director, Neurosciences Medical Director, Rehabilitation
Understanding Alzheimer s Disease
 Understanding Alzheimer s Disease Alzheimer s disease is an irreversible, progressive brain disorder that slowly impacts memory, thinking, skills and, eventually, the ability to carry out the simplest
Understanding Alzheimer s Disease Alzheimer s disease is an irreversible, progressive brain disorder that slowly impacts memory, thinking, skills and, eventually, the ability to carry out the simplest
1 in 3 seniors dies with Alzheimer s or another dementia.
 2013 Alzheimer s disease facts and figures Includes a Special Report on long-distance caregivers 1 in 3 seniors dies with Alzheimer s or another dementia. Out-of-pocket expenses for long-distance caregivers
2013 Alzheimer s disease facts and figures Includes a Special Report on long-distance caregivers 1 in 3 seniors dies with Alzheimer s or another dementia. Out-of-pocket expenses for long-distance caregivers
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
The Impact of Type 2 Diabetes on Cognition
 The Impact of Type 2 Diabetes on Cognition Laura D. Baker, PhD Associate Professor of Medicine & Public Health Sciences Associate Director, Wake Forest Alzheimer s Disease Center Wake Forest School of
The Impact of Type 2 Diabetes on Cognition Laura D. Baker, PhD Associate Professor of Medicine & Public Health Sciences Associate Director, Wake Forest Alzheimer s Disease Center Wake Forest School of
WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES
 WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 1 CMS Medicare-Medicaid Coordination Office (MMCO) Established by Section 2602 of the Affordable Care Act Purpose:
WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 1 CMS Medicare-Medicaid Coordination Office (MMCO) Established by Section 2602 of the Affordable Care Act Purpose:
Dementia. Amber Eker, MD. Assistant Professor Near East University Department of Neurology
 Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social
Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social
Current Treatments for Dementia and Future Prospects. James Warner St Charles Hospital, London
 Current Treatments for Dementia and Future Prospects James Warner St Charles Hospital, London Dementia Cognitive Non-cognitive (BPSD) Memory orientation language other cognitive abilities praxis planning
Current Treatments for Dementia and Future Prospects James Warner St Charles Hospital, London Dementia Cognitive Non-cognitive (BPSD) Memory orientation language other cognitive abilities praxis planning
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
Research and possible future brain health treatments
 Research and possible future brain health treatments Cheryl Brandi, DNSc, ARNP, NP-C Roskamp Institute Clinic July 21, 2016 brandi, roskamp institute 1 The Roskamp Institute Not for profit biomedical research
Research and possible future brain health treatments Cheryl Brandi, DNSc, ARNP, NP-C Roskamp Institute Clinic July 21, 2016 brandi, roskamp institute 1 The Roskamp Institute Not for profit biomedical research
Brain imaging for the diagnosis of people with suspected dementia
 Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
Shaping the Future of Dementia Care. Cheryl Miller, Phoebe Ministries Staff Development Coordinator
 Shaping the Future of Dementia Care Cheryl Miller, Phoebe Ministries Staff Development Coordinator Objectives By the end of this session attendees will be able to: 1. List three modifiable risk factors
Shaping the Future of Dementia Care Cheryl Miller, Phoebe Ministries Staff Development Coordinator Objectives By the end of this session attendees will be able to: 1. List three modifiable risk factors
Round table: Moderator; Fereshteh Sedaghat, MD, PhD Brain Mapping in Dementias and Non-invasive Neurostimulation
 Round table: Moderator; Fereshteh Sedaghat, MD, PhD Brain Mapping in Dementias and Non-invasive Neurostimulation 1. Reflection of Mild Cognitive Impairment (MCI) and Dementias by Molecular Imaging, PET
Round table: Moderator; Fereshteh Sedaghat, MD, PhD Brain Mapping in Dementias and Non-invasive Neurostimulation 1. Reflection of Mild Cognitive Impairment (MCI) and Dementias by Molecular Imaging, PET
AT RISK, SCI, EMCI: THE ALPHABET SOUP OF PRECLINICAL AND PRODROMAL ALZHEIMER DISEASE
 AT RISK, SCI, EMCI: THE ALPHABET SOUP OF PRECLINICAL AND PRODROMAL ALZHEIMER DISEASE Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology Mary Quiceno, MD discloses she has received honoraria
AT RISK, SCI, EMCI: THE ALPHABET SOUP OF PRECLINICAL AND PRODROMAL ALZHEIMER DISEASE Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology Mary Quiceno, MD discloses she has received honoraria
The Primary Care Guide To Understanding The Role Of Diabetes As A Risk Factor For Cognitive Loss Or Dementia In Adults
 The Primary Care Guide To Understanding The Role Of Diabetes As A Risk Factor For Cognitive Loss Or Dementia In Adults. Introduction Glucose intolerance is common in older individuals and this metabolic
The Primary Care Guide To Understanding The Role Of Diabetes As A Risk Factor For Cognitive Loss Or Dementia In Adults. Introduction Glucose intolerance is common in older individuals and this metabolic
Mild Cognitive Impairment Symposium January 19 and 20, 2013
 Highlights of Biomarker and Clinical Outcomes in Recent AD Treatment Trials Stephen Salloway, MD, MS Professor of Neurology and Psychiatry Alpert Medical School, Brown University Mild Cognitive Impairment
Highlights of Biomarker and Clinical Outcomes in Recent AD Treatment Trials Stephen Salloway, MD, MS Professor of Neurology and Psychiatry Alpert Medical School, Brown University Mild Cognitive Impairment
USE OF BIOMARKERS TO DISTINGUISH SUBTYPES OF DEMENTIA. SGEC Webinar Handouts 1/18/2013
 Please visit our website for more information http://sgec.stanford.edu/ SGEC Webinar Handouts 1/18/2013 2013 WEBINAR SERIES STATE OF THE SCIENCE: DEMENTIA EVALUATION AND MANAGEMENT AMONG DIVERSE OLDER
Please visit our website for more information http://sgec.stanford.edu/ SGEC Webinar Handouts 1/18/2013 2013 WEBINAR SERIES STATE OF THE SCIENCE: DEMENTIA EVALUATION AND MANAGEMENT AMONG DIVERSE OLDER
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Neurocognitive Disorders Research to Emerging Therapies
 Neurocognitive Disorders Research to Emerging Therapies Edward Huey, MD Assistant Professor of Psychiatry and Neurology The Taub Institute for Research on Alzheimer s Disease and the Aging Brain Columbia
Neurocognitive Disorders Research to Emerging Therapies Edward Huey, MD Assistant Professor of Psychiatry and Neurology The Taub Institute for Research on Alzheimer s Disease and the Aging Brain Columbia