Diabetes for GP CME 2009
|
|
|
- Bertram Ellis
- 5 years ago
- Views:
Transcription
1 Diabetes for GP CME 2009 The good, the bad and the ugly Dr Paul Drury Medical and Clinical Director, Auckland Diabetes Centre
2 Some of the areas to cover New NZ data on epidemiology New trials: ACCORD, ADOPT, ADVANCE, VA... New targets: HbA1c New treatments and old : metformin and incretins New toxicities and concerns, need for CV studies New NZ renal data from ANZDATA New risk issues
3 The pyramid (or iceberg) of metabolic syndrome ca 2009 More DM implies more IGT, IFG and Metabolic syndrome US figures horrifying. Diabetes Abnormal glucose tolerance (IGT and IFG) Clear evidence from multiple studies esp AUSDIAB Metabolic syndrome
4 Models and Forecasts 2002 and 2006/7 NZ Prevalence (all in 1000s) Mean Lower Upper Column1 Expon. (Column1)
5 Diagnosed and undiagnosed diabetes in NZ Tradition Maori 2003 Known Unknown European 2003 Pacific 2003 Recent data from Sundborn et al, NZMJ 2007
6 What s possibly happening mid 2009? Ignore exact numbers Main drivers demographic obesity screening Undiagnosed Diagnosed Prevention won t work for years, if at all
7 The pyramid or iceberg of metabolic syndrome and vascular risk Macrovascular risk Microvascular risk Diabetes Abnormal glucose tolerance (IGT and IFG) Metabolic syndrome So no need for retinal screening for IGT etc
8 Controversies in Screening & Diagnosis After selection by clinical risk scores what is best test? Casual plasma glucose o Variable; o Poor sensitivity; Fasting plasma glucose o Reliable; o Misses IGT; o Inconvenient; Glucose Tolerance Test HbA1c o As good as Fasting plasma glucose (FPG)? As screen? As diagnosis?
9 HbA1c things likely to change Assuming a standardised assay may be reported in mmol/l: 1. A rise in cardiovascular events occurs with rising HbA1c well below the diabetic range Approximately 10% risk for 1% HbA1c rise 2. If aim of screening is to identify people at high risk of vascular disease could HbA1c be added to CV risk tables? 3. Proposal (JCEM July 2008) HbA1c > 6.0% - re-screen with FPG or OGTT HbA1c 6.5% - confirm possible diagnosis of diabetes with fasting/random glucose 4. Average Blood Glucose (eag) for communication
10 Relationship of HbA1c with estimated average glucose We may be moving to reporting estimated average glucose eag (mmol/l) HbA1c (%)
11 Who to risk assess NZGG 2003 Possible changes for 2010? Or even more aggressive? Men Women Asymptomatic people, without other known risk factors Age 45 Age 55 Māori, Pacific people and people from the Indian sub-continent Those with at higher risk of CVD or developing diabetes Age 35? Now 30 Age 35? Now 30 Age 45? Now 40 Age 45? Now 40 People with diabetes or IGT or IGF or?? MetS At diagnosis 11

12
13 HbA1c and vascular events There is strong evidence regarding the relationship between HbA1c and microvascular events e.g. DCCT, Kumamoto, UKPDS. But What about macrovascular events in Type 2 Diabetes? o In UKPDS HbA1c % resulted in 18% in events (NS) o Meta-analysis analysis suggests 16% increase in CV events per 1% HbA1c o Local actual Get Checked data shows 8% increase 13
14 Adjusted hazard ratios of association between HbA1c and risk of first CVD event (95% CIs) Elley et al, 2008 I n press P< % increase in CV event rate per 1% increase in HbA1c (Previous estimate around 15%) From NZ Get Checked data Many/most patients on cardioprotective medication Effect present in both sexes (not significantly different)
15 Targets for HbA1c in 2009? What are your targets for: 1. A 66-year old overweight but asymptomatic Caucasian man with newly-diagnosed type 2 diabetes on screening? HbA1c 8% two months later on lifestyle measures alone. 2. A 47-year old Maori woman, diabetic for 9 years, with HbA1c 9%, ACR 34.8 and previous marked hypos on insulin. Not optimal adherence.
16 Targets for HbA1c in 2009? 7%? ADA, NZGG 6.5%? EASD, AACE?? Does one size fit all?? Around 6-6 7%? But not if CVD or very high risk Hypo risk may be more important than we think
17 ACCORD Study (NEJM June 2008) T2 Diabetes aged > 40 years + C/V risk or CV Disease 10,000 patients Baseline: Aged 62 years BMI 32 BP 136/75 HbA1c 8.3% (10 year duration) Previous C/V event 35% High use of statin, ACE-I, aspirin 17
18 ACCORD results June 2008 The Action to Control Cardiovascular Risk in Diabetes Study Group. N Engl J Med 2008;358:
19 ACCORD results June 2008
20 ACCORD Study (NEJM June 2008) Results: (prematurely stopped after 3.5 years) Intensive Standard HbA1c 6.4% 7.5% Insulin Use 77% 55% TZD Use 92% 58% Hypos (needing assistance) 16% 5% Non Fatal MI/CVA or CV Death n = 352 n = 372 Total Mortality Fatal MI Fatal CHF Unexpected Death Effect apparently not attributable to any single/combo drugs 20
21 ADVANCE Study (NEJM June 2008) T2 Diabetes aged > 55 years + 1 risk factor 11,000 patients Baseline: Aged 66 years BMI 28 Mean HbA1c 7.5% (8 year duration) Previous macrovascular event 35% Microalbuminuria 27% Statin use 28% 21

22 ADVANCE results June 2008
23 ADVANCE results June 2008 The ADVANCE Collaborative Group. N Engl J Med 2008;358:
24 ADVANCE Study (NEJM June 2008) Results: (after 5 years) Intensive Standard HbA1c 6.5% (80% < 7%) 7.3% (50% < 7%) Insulin Use 40% 24% TZD Use 17% 11% Sulphonylurea 92% 58% Metformin 74% 67% Statin 45% 47% CV Death n = 253 n = 289 Major CV event n = 557 n= 590 Coronary events New or worsening nephropathy
25 ADVANCE Study (NEJM June 2008) Suggests the current target of 7% and not lower is reasonable for those with: 8-10 years T2DM and/or established CV disease As long as BP/Lipids controlled + aspirin This was less well done than in ACCORD and higher mortality in ADVANCE 25
26 Targets for HbA1c in 2009? What are your targets for: 1. A 66-year old overweight but asymptomatic Caucasian man with newly-diagnosed type 2 diabetes on screening? HbA1c 8% two months later on lifestyle measures alone. 2. A 47-year old Maori woman, diabetic for 9 years, with HbA1c 9%, ACR 34.8 and previous marked hypos on insulin. Not optimal adherence.
27
28 Diabetes drugs old and new - and HbA1c reductions adapted from NEJM review Nathan, 2007 Insulin Hypo 1922 >2.5% Inhaled insulin % Sulphonylureas Hypo % Phenformin 1957-? 1.5% Metformin 1960s 1.5% Alpha-glucosidase inhibs (acarbose) % Glinides e.g. repaglinide Hypo % Troglitazone % Rosiglitazone % Pioglitazone % GLP analogues % Amylin analogues % DPP-4 inhibitors % Diet and exercise (UKPDS)???? 2%
29 Type 2 DM Which Drug is Best to Start? ADOPT Study 2006: (NEJM December 2006) 4360 patients given either Rosiglitazone, Metformin or Glyburide as monotherapy. At 4 yrs HbA1c < 7% HbA1c maintained < 7% Rosi 40% 60 mths Met 36% 45 mths Gly 26% 33 mths But only 60% completed study. 29
30 ADOPT - Adverse Events Rosi Metf Glyburide CV Events n= CHF 1.5% (22) 1.3% (19) 0.6% (9) Oedema 14% 7.2% 8.5% Hypos (Self reported) 9.2% 11.6% 38.9% GI Events 23% 38% 22% Weight gain kg kg kg Fractures 6.3% (92) 4.1% (59) 3.4% (49) Costs - -
31 Metformin Pros: Many years of experience Reduces insulin resistance Weight neutral No hypoglycaemia Reduces risk of CV events (stroke esp. plus MI in obese subset in UKPDS) Cost is low Cons: G.I. intolerance in 5-20% But lactic acidosis is rare N.B.? Cautious reduction in dose when egfr 40ml/min STOP once egfr ml/min Mild in B 12 levels Slow release and combos available elsewhere, but not in NZ Better tolerability and fewer tablets
32 Sulphonylurea as Monotherapy Sulphonylurea: OK if BMI < 25 (consider LADA) OK if BMI > 25 and Metformin cannot be used. Pros: Promotes insulin release Generally well tolerated Variable in renal impairment Low cost Cons: Hypoglycaemia Can be severe Weight gain Earlier ß Cell failure? Avoid in elderly/frail ( ADOPT Study 2006)
33 Glitazones Pioglitazone (Actos); Rosiglitazone (Avandia) Insulin sensitizers. Only Actos currently funded in N.Z. No longer specialist only approval. Take ages e.g. months to work, but not always Monotherapy Dual Therapy Met. Intol With Met or SU and BMI >33 or S.U. intol May use with insulin if > 1.5u/kg but best avoided here. 33 Best left to specialists as higher risk of HF
34 Glitazones Pros: Cons: Good insulin sensitisers Equipotent with other oral agents. Additive effect on HbA1c Actos has benefit of Triglyceride and HDL CRP and may BP. May preserve ß cell function longer than other oral agents. (ADOPT Study) Reduces fat in liver Weight gain common. Oedema ankle 2-5%. Heart failure in 2-3% not cardiodepressant but contraindicated in heart failure. Cost high CV outcomes still unclear. No long term reduction in C/V events proven. Rosi relation to MI currently questioned but no signal from large RECORD study yet. (Meta analysis by Nissen et al NEJM 2007). Increase in non-vertebral # in women - recently demonstrated (2-2.5 x risk ).
35 Pioglitazone (Actos) - how to use Start at 15mg, to 30mg soon max dose 45mg but often needed in large patients!. Watch for early weight gain, SOB, ankle swelling. May not have any clinical effect for 4-6 weeks and maximal effect at 6-8 months... or more Patient may give up if not educated well about slow action Not always easy to decide who will respond best, but usually the most insulin resistant (truncally obese).
36 Acarbose Pros α-glucosidase inhibitor slows CHO breakdown Post-prandial in glucose in HbA1c by ca 0.5% Reduction in CV mortality when used for IGT (STOP NIDDM) Useful if significant CHO in diet? Start 25mg pre-dinner and build to mg t.d.s. Cons Significant GI. side effects. Specialist approval to start.
37 What are Incretins? Incretins are gut hormones that help the body response to elevated glucose Incretins (GLP-1 and GIP) are naturally occurring hormones released in response to meals. GLP-1 analogues are now available e.g. exenatide. When glucose levels are elevated, GLP-1 and GIP signal ß cells to increase insulin release and GLP-1 signals α-cells to suppress glucagon release The physiologic activity of incretins is limited by the enzyme dipeptidyl peptidase 4 (DPP-4), which rapidly degrades incretins after their release. DPP-4 inhibitors are now available e.g. Sitagliptin.

38 Gila Monster World s largest lizard holds key to diabetes treatment in its mouth 38
39 Incretin Effect After Oral vs IV Glucose is diminished in Type 2 Diabetes Venous plasma glucose (mmol/l) IR insulin (mu/l) Healthy controls (n=8) Oral glucose (50 g/400 ml) Normal incretin effect Type 2 diabetes (n=14) Isoglycemic intravenous glucose * * * * * * * Venous plasma glucose (mmol/l) IR insulin (mu/l) Diminished incretin effect * * * Time (minutes) Time (minutes) *p 0.05 vs. respective value after oral load, IR=immunoreactive Adapted from Nauck M et al Diabetologia 1986;29:







40 GLP-1 Effects in Humans Understanding the Glucoregulatory Role of Incretins GLP-1 secreted upon the ingestion of food Promotes satiety and reduces appetite Alpha cells: Postprandial glucagon secretion Beta cells: Enhances glucosedependent insulin secretion Liver: Glucagon reduces hepatic glucose output Stomach: Helps regulate gastric emptying Adapted from Flint A, et al. J Clin Invest. 1998;101: ; Adapted from Larsson H, et al. Acta Physiol Scand. 1997;160: ; Adapted from Nauck MA, et al. Diabetologia. 1996;39: ; Adapted from Drucker DJ. Diabetes. 1998;47:
 GIP (3 42) GLP-1 (9 36) GIP and GLP-1 actions Adapted from Deacon CF et al Diabetes 1995;44:1126 1131; Kieffer TJ et al Endocrinology 1995;136:3585 3596; Ahrén B Curr Diab Rep")
41 In Vitro and In Vivo DPP-4 Inhibition Increases Levels of Biologically Active Incretins GLP-1 and GIP Intestinal GIP and GLP-1 release Meal DPP-4 enzyme DPP-4 inhibitor GIP (1 42) GLP-1 (7 36) Rapid degradation (minutes) GIP (3 42) GLP-1 (9 36) GIP and GLP-1 actions Adapted from Deacon CF et al Diabetes 1995;44: ; Kieffer TJ et al Endocrinology 1995;136: ; Ahrén B Curr Diab Rep 2003;3: ; Deacon CF et al J Clin Endocrinol Metab 1995;80: ; Weber AE J Med Chem 2004;47:
42 Incretin Drugs available in U.S. and Europe and now NZ But not funded Exenatide (Exendin), LA prep and others in hand Binds to GLP receptor. Injected b.d. often some nausea initially. Weight loss of 4-5kg. HbA1c by %, possibly more with newer agents No hypos. Not funded ideal after 2 oral agents instead of insulin? Perhaps available in daily and once weekly injections soon
43 Incretin Drugs available in U.S. and Europe and now NZ But not funded DPP IV Inhibitors, e.g. Sitagliptin GLP by inhibiting breakdown Oral medication HbA1c by % No hypos Weight neutral Not funded Works well with Metformin Perhaps ideal for elderly or in those where hypoglycaemia likely e.g. renal impairment
44 Poor control in type 2 diabetes If patient has poor control and many of the following then they are VERY likely to have ß cell failure: Longer duration of diabetes e.g. > 7 years Initial high HbA1c at presentation Very high HbA1c > 9-10% Have needed progressive increases in oral medication over the years Are losing weight Poor diet, limited exercise and /or poor compliance are also possible or likely but Unlikely to be the whole explanation
45 Declining Beta-Cell Function Associated with Increasing Hyperglycemia UKPDS Beta-cell function (%) Diet/conventional therapy (n=110) Metformin (n=159) Sulfonylurea (n=511) HbA 1c (%) Diet/conventional therapy (n=297) Metformin (n=251) Insulin or sulfonylurea (n=695) Years Years Beta-cell function assessed by HOMA HbA 1c results shown from obese patients UKPDS=United Kingdom Prospective Diabetes Study; HbA 1c =glycosylated hemoglobin Adapted from UKPDS Group Diabetes 1995;44:
46 So why don t we use insulin earlier? Better glycaemic control. Reduces lipotoxcity ( NEFA, TG). Conserves B cell function. Improves endothelial function.
47 Clinical Inertia in T2DM Management in Auckland Choe & Cutfield 2008 Study of 2240 patients in 1 1 care in S.W. Auckland in on 2 oral agents: 954 (42.6%) of these had HbA1c 8% Nearly 2 year s later: 451 out of 605 patients with second HbA1c 8 were still not on insulin 47
48 Overcoming Barriers Introduce concept of insulin early, not as threat. Pain Demonstrate how to inject early with appropriate education; usually painless. Inconvenience Quality of Life Hypos Weight gain Cultural issues keep regimen simple e.g. Nocturnal NPH by pen. Does not reduce / May increase. minimal. use with Metformin / Review food plan. involve family, friends, church leaders. CHANGE ATTITUDES of Health Professionals.
49
50
51 Cardiovascular risk in diabetes Basically same as anyone else BUT Current equations, even NZGG, don t adequately allow for: Ethnicity (also deprivation) Maori + 30%, East Asian -20% Microalbuminuria Macroalbuminuria Poor glycaemic control Newer data show significant and major effect of: Reduced renal function, even marginal, as egfr Lesser effect of glycaemic control (if on CV Rx) Increasing evidence of increasing benefit from Duration of anti-risk treatment
52 Microvascular and macrovascular risk vs HbA1c UKPDS data type Microvascular Macrovascular 50 Risk HbA1c (%) HbA1c (%)
53 Attack the Risk Factors and overall risk - but which drugs? BP: ACE inhibitor / A2 antagonist but NOT both Thiazide Ca 2t antagonists B-BlockerBlocker Lipids: STATIN for most if TG > 3.0 +(-) STATIN to LDL if target not reached but... Fibrate if TG > 3.0 Ezetemibe to Aspirin: If C.V. risk > 15% at 5 years or DM with 1 risk factor or DM > 10 years duration or > 50 years age. But new data..
54 Previous prognosis of diabetic nephropathy from type 1 cohorts
55 Type 1 diabetes and nephropathy incidence
56 Type 1 DM and risk of death from ESRD
57 New type 1 DM RRT patients New Zealand ANZDATA
58 New RRT patients New Zealand ANZDATA uncorrected numbers All Type 1 Type
59 New RRT NZ by ethnicity ANZDATA uncorrected numbers Caucasoid Maori Pacific Asian
60 NZ diabetes on dialysis (end 2006) by age ANZDATA uncorrected numbers Causasoid Maori Pacific Asian 20 0 <
61 Comparison of ethnicities All diabetic population New DM RRT patients 2006 Caucasoid Maori Pacific Asian Caucasoid Maori Pacific Asian
62 New Patient ESRF Rates: ANZDATA Diabetes consistently 40-45% of NZ new RRT Uncorrected for diabetes prevalence 130 Incident RRT rate (per million per year) Year Australia NZ Is that a plateau or not? 2007 data now shows no sig rise Given rising prevalence are we winning?
63 Albuminuria mortality rates (UKPDS data) Microalbuminuria predates proteinuria May predate renal impairment Also very powerful CV risk factor, tho so is renal function alone (egfr) Mortality (%) Normoalbuminuria Microalbuminuria Macroalbuminuria Clinical nephropathy ESRF
64 Original Article Effect of a Multifactorial Intervention on Mortality in Type 2 Diabetes Peter Gæde, M.D., D.M.Sc., Henrik Lund-Andersen, M.D., D.M.Sc., Hans- Henrik Parving, M.D., D.M.Sc., and Oluf Pedersen, M.D., D.M.Sc. N Engl J Med Volume 358(6): February 7, 2008
65 Intensified Multifactorial Intervention Steno 2 Study ( NEJM 2008) 160 patients with type 2 diabetes and microalbuminuria Intensive group treat to target for first 8 years, then all intensive nsive All offered aspirin/ace inhibitor (85-90%), + statin intensive Intensive Conventional Baseline At 7 yrs 13 yrs 7 yrs 13 yrs BP 146/85 131/73 140/74 146/78 146/73 LDL Smoking 40% 31% 22% 27% 18% HbA1c % 7.7% 9.0% 8.0%

66
67 Kaplan-Meier Estimates of the Risk of Death from Any Cause and from Cardiovascular Causes and the Number of Cardiovascular Events, According to Treatment Group Gaede P et al. N Engl J Med 2008;358:
68 Some brief issues on risk Several studies fail to confirm efficacy of ASP in type 2 DM with no CV event e.g. primary prevention ineffective? In contrast STATINS are beneficial, though absolute risk reduction dependent on absolute risk (20% reduction of 5% is not a lot) Overall CV event rates in all T2DM recent studies have been well below predictions e.g. FIELD, CARDS, POPADAD May be benefit of METFORMIN separate from BG lowering effect. Should almost everyone have METF? Fenofibrate may have some specific actions on eye disease and on amputation May be long lag period before maximal benefit from intervention
69 My thanks to Dr Rick Cutfield and Prof Tim Cundy for slides Thank you for your interest and attention
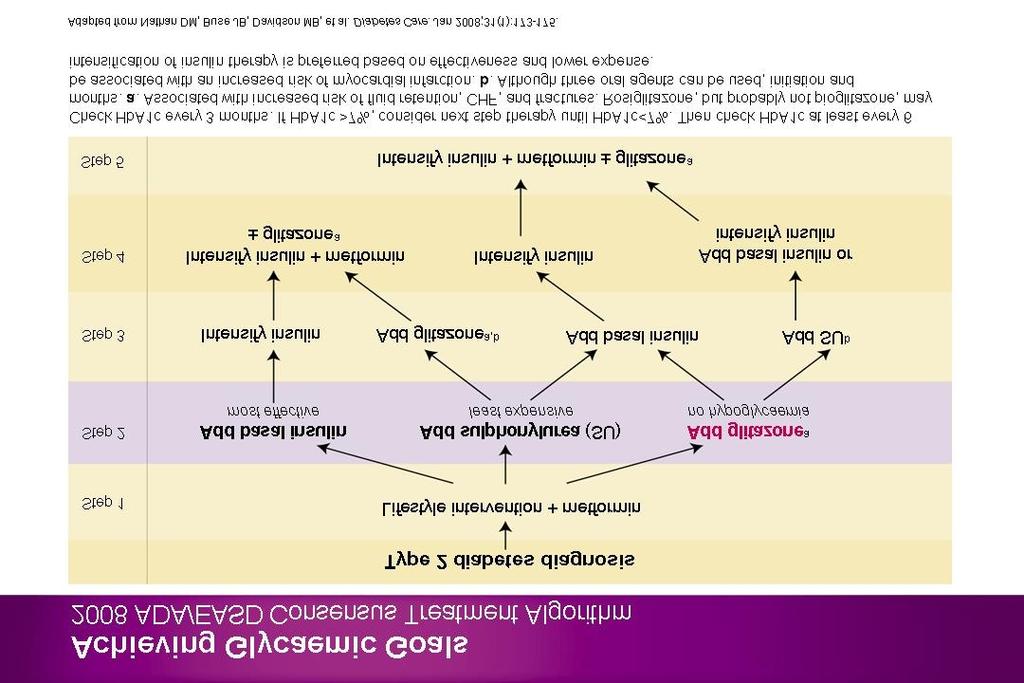
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Optimal glucose control. DM Treatment. Glucose Control one out of many. Many guidelines: Confusing. Theorectically easy
 DM Treatment How to Achieve Optimal Glycaemic Control The Tung Wah Eastern Hospital Experience of DM Share Care Experience Optimal glucose control Theorectically easy More challenging in the real world
DM Treatment How to Achieve Optimal Glycaemic Control The Tung Wah Eastern Hospital Experience of DM Share Care Experience Optimal glucose control Theorectically easy More challenging in the real world
Mr Rab Burtun. Dr David Kim. 8:30-10:30 WS #2: Diabetes Basic 11:00-13:00 WS #9: Diabetes Basic (Repeated)
") Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
Should Psychiatrists be diagnosing (and treating) metabolic syndrome
 metabolic syndrome") Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
CURRENT CONTROVERSIES IN DIABETES CARE
 CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
Pathogenesis of Type 2 Diabetes
 9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Glycemic control what can be achieved with life-style and when and how to use pharmacological agents?
 Glycemic control what can be achieved with life-style and when and how to use pharmacological agents? Eberhard Standl Munich Diabetes Research Institute At the Munich Helmholtz Center Pathogenetic key
Glycemic control what can be achieved with life-style and when and how to use pharmacological agents? Eberhard Standl Munich Diabetes Research Institute At the Munich Helmholtz Center Pathogenetic key
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Diabetes Risk Assessment and Treatment
 Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Pre-diabetes. Pharmacological Approaches to Delay Progression to Diabetes
 Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
DPP-4 inhibitor. The new class drug for Diabetes
 DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Dr Tahseen A. Chowdhury Royal London Hospital. New Guidelines in Diabetes: NICE or Nasty?
 Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville
 Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Current Diabetes Care for Internists:2011
 Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Diabetes in the UK: Update on Diabetes Treatment and Care. Why is diabetes increasing? Obesity Increased waist circumference.
 Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
DIABETES IN 2007 What snew
 DIABETES IN 2007 What snew 1 Objectives 1. Review recently published clinical trials in diabetes What does this mean to us? 1. Discuss novel concepts in the treatment of diabetes What should we expect?
DIABETES IN 2007 What snew 1 Objectives 1. Review recently published clinical trials in diabetes What does this mean to us? 1. Discuss novel concepts in the treatment of diabetes What should we expect?
Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy
 Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy Melpomeni Peppa Assistant Professor of Endocrinology 2 nd Dept of Internal Medicine-Propaedeutic, Athens
Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy Melpomeni Peppa Assistant Professor of Endocrinology 2 nd Dept of Internal Medicine-Propaedeutic, Athens
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
 What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Diabetes: What is the scope of the problem?
 Diabetes: What is the scope of the problem? Elizabeth R. Seaquist MD Division of Endocrinology and Diabetes Department of Medicine Director, General Clinical Research Center Pennock Family Chair in Diabetes
Diabetes: What is the scope of the problem? Elizabeth R. Seaquist MD Division of Endocrinology and Diabetes Department of Medicine Director, General Clinical Research Center Pennock Family Chair in Diabetes
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus. Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre
 Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
CURRENT STATEGIES IN DIABETES MELLITUS DIABETES. Recommendations for Adults CURRENT STRATEGIES IN DIABETES MELLITUS. Diabetes Mellitus: U.S.
 CURRENT STATEGIES IN DIABETES MELLITUS Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Diabetes Mellitus: U.S. Impact ~1 Million Type 1 DIABETES 16.7 Million IFG (8.3%) 12.3
CURRENT STATEGIES IN DIABETES MELLITUS Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Diabetes Mellitus: U.S. Impact ~1 Million Type 1 DIABETES 16.7 Million IFG (8.3%) 12.3
CURRENT ISSUES IN DIABETES MANAGEMENT
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2011 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2011 BMI
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dr A Pokrajac MD MSc MRCP Consultant
 Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
la prise en charge du diabète de
 N21 XIII Congrès National de Diabétologie, 29 mai 2011, Alger Intérêt et place des Anti DPP4 dans la prise en charge du diabète de type 2 Nicolas PAQUOT, MD, PhD CHU Sart-Tilman, Université de Liège Belgique
N21 XIII Congrès National de Diabétologie, 29 mai 2011, Alger Intérêt et place des Anti DPP4 dans la prise en charge du diabète de type 2 Nicolas PAQUOT, MD, PhD CHU Sart-Tilman, Université de Liège Belgique
MANAGEMENT OF TYPE 2 DIABETES
 MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glycemic control A combination of life style interaction and the use of drugs
 Multifactorial management to reduce cardiovascular risk in patients with diabetes mellitus Glycemic control A combination of life style interaction and the use of drugs Eberhard Standl Munich Diabetes
Multifactorial management to reduce cardiovascular risk in patients with diabetes mellitus Glycemic control A combination of life style interaction and the use of drugs Eberhard Standl Munich Diabetes
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
GLP-1 Receptor Agonists and SGLT-2 Inhibitors. Debbie Hicks
 GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017
 TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes. Overview. Prevalence of Overweight in the U.S.
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Diabetes update - Diagnosis and Treatment
 Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
Newer and Expensive treatment of diabetes. Endocrinology Visiting Associate Professor Institute of Medicine TUTH
 Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Changing Diabetes: The time is now!
 Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
효과적인경구혈당강하제의조합은? 대한당뇨병학회제 17 차연수강좌 ( ) 가천의대길병원내분비대사내과
 가천의대길병원내분비대사내과") 효과적인경구혈당강하제의조합은? 대한당뇨병학회제 17 차연수강좌 (2011.10.30.) 가천의대길병원내분비대사내과 박이병 내용 배경 경구혈당강하제의병합이왜필요한가? (WHY?) 경구혈당강하제의병합은언제시작하나? (WHEN?) 경구혈당강하제의병합은어떻게하는것이좋은가?(HOW) 맺음말 배경 : drugs for treating diabetes In 1995 :
효과적인경구혈당강하제의조합은? 대한당뇨병학회제 17 차연수강좌 (2011.10.30.) 가천의대길병원내분비대사내과 박이병 내용 배경 경구혈당강하제의병합이왜필요한가? (WHY?) 경구혈당강하제의병합은언제시작하나? (WHEN?) 경구혈당강하제의병합은어떻게하는것이좋은가?(HOW) 맺음말 배경 : drugs for treating diabetes In 1995 :
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP
 Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP KEY POINTS sitagliptin (Januvia) is a DPP-4 inhibitor that blocks the breakdown of the
Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP KEY POINTS sitagliptin (Januvia) is a DPP-4 inhibitor that blocks the breakdown of the
GLP-1-based therapies in the management of type 2 diabetes
 GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
Glycemic control a matter of life and death
 Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Injectable GLP 1 therapy: weight loss effects seen in obesity with and without diabetes
 Injectable GLP 1 therapy: weight loss effects seen in obesity with and without diabetes Dr Masud Haq Consultant Lead in Diabetes & Endocrinology Maidstone & Tunbridge Wells NHS Trust & The London Preventative
Injectable GLP 1 therapy: weight loss effects seen in obesity with and without diabetes Dr Masud Haq Consultant Lead in Diabetes & Endocrinology Maidstone & Tunbridge Wells NHS Trust & The London Preventative
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
FUNDING: MICIS mandated by Maine Legislature, funded by fees collected from pharmaceutical companies as a cost of doing business in the state.
 GOAL: To improve clinical outcomes by delivering upto-date, evidence-based prescribing information, using data and guidelines developed by noncommercial sources FUNDING: MICIS mandated by Maine Legislature,
GOAL: To improve clinical outcomes by delivering upto-date, evidence-based prescribing information, using data and guidelines developed by noncommercial sources FUNDING: MICIS mandated by Maine Legislature,
INJECTABLE THERAPIES IN DIABETES. Barbara Ann McKee Diabetes Specialist Nurse
 INJECTABLE THERAPIES IN DIABETES Barbara Ann McKee Diabetes Specialist Nurse 1 Aims of the session Describe the different injectable agents for diabetes and when they would be used. Describe some common
INJECTABLE THERAPIES IN DIABETES Barbara Ann McKee Diabetes Specialist Nurse 1 Aims of the session Describe the different injectable agents for diabetes and when they would be used. Describe some common
CURRENT ISSUES IN DIABETES MANAGEMENT
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact DIABETES
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact DIABETES
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Diabetes Update July 6, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Addressing Addressing Challenges in Type 2 Challenges in Type 2 Diabetes Diabetes Speaker:
 Addressing Challenges in Type 2 Diabetes Geneva Briggs, PharmD,, BCPS Addressing Challenges in Type 2 Diabetes Speaker: Dr. Geneva Clark Briggs, a board-certified Pharmacotherapy Specialist, received her
Addressing Challenges in Type 2 Diabetes Geneva Briggs, PharmD,, BCPS Addressing Challenges in Type 2 Diabetes Speaker: Dr. Geneva Clark Briggs, a board-certified Pharmacotherapy Specialist, received her
Julie White, MS Administrative Director Boston University School of Medicine Continuing Medical Education
 MENTOR QI Diabetes Performance Improvement Initiative, Getting Patients to Goal in Glycemic Control: Current Data Julie White, MS Administrative Director Boston University School of Medicine Continuing
MENTOR QI Diabetes Performance Improvement Initiative, Getting Patients to Goal in Glycemic Control: Current Data Julie White, MS Administrative Director Boston University School of Medicine Continuing
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number