A Case of Immunotactoid Glomerulopathy with Rapid Progression to End-Stage Renal Disease
|
|
|
- Oscar Douglas
- 5 years ago
- Views:
Transcription
1 Case Study TheScientificWorldJOURNAL (2009) 9, ISSN X; DOI /tsw A Case of Immunotactoid Glomerulopathy with Rapid Progression to End-Stage Renal Disease Shikha Jain 1, * and Darshika Chhabra 2 1 Department of Internal Medicine, University of Illinois, Chicago; 2 Department of Nephrology, Northwestern University, Chicago sjain03@gmail.com; darshika@gmail.com Received August 16, 2009; Revised December 4, 2009; Accepted December 4, 2009; Published December 16, 2009 Immunotactoid glomerulopathy (IGN) is a rare immunoglobulin deposition disease. It is often mistaken for cryoglobulinemia or amyloidosis due to the similarities on biopsy findings. The disease progresses to end-stage renal disease (ESRD) within 7 months to 10 years. This is the first case reported of a patient with a diagnosis of IGN who developed acute kidney injury (AKI) and ESRD within 1 week of initial presentation. KEYWORDS: immunotactoid glomerulopathy, acute kidney injury, end-stage renal disease, immunoglobulin INTRODUCTION Immunoglobulin (Ig)-mediated kidney disorders are divided into two categories: those that result from the deposition of intact Ig molecules into the kidney and those caused by deposition of components of Ig molecules, such as light or heavy chains or chain fragments. Disorders due to intact Ig deposition include IgA nephropathy, membranous lupus, and anti-gbm (glomerular basement membrane) disease. These pathologies are caused by polyclonal Ig molecules that interact directly with kidney antigens or form preformed immune complexes. In contrast, disorders due to deposition of Ig components are monoclonal, and the pathogenic proteins are produced by clonal populations of plasma cells or B lymphocytes. Immunotactoid glomerulopathy (IGN) is a rare disease that falls into the category of Ig component deposition disorders. CASE PRESENTATION A 78-year-old man with multiple medical problems, including hypertension, hyperlipidemia, dementia, and benign prostatic hypertrophy, presented with a 2-day history of anuria. The patient s son noted that he had also exhibited worsening lethargy and oliguria over the past week. The physical exam revealed a thin, slightly disoriented man in no acute distress. On admission, blood pressure was 201/96 and the patient was able to follow commands. The remainder of the physical exam was unremarkable. A Foley catheter was placed with no urine output. Pertinent initial labs included blood urea nitrogen (BUN) 136 mg/dl, creatinine (Cr) 20.1 mg/dl, estimated glomerular filtration rate (egfr) <10 ml/min (baseline 25 mg/dl, *Corresponding author w ith author. Published by TheScientificWorld;
. He was noted to have an anion gap metabolic acidosis with bicarbonate of 20.")
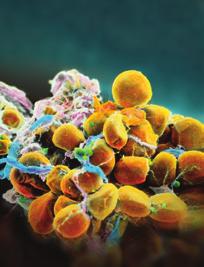
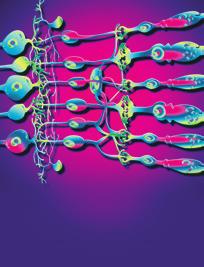
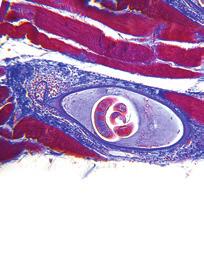
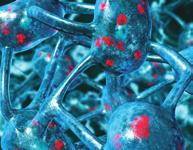
2 1.2 mg/dl, >60 ml/min, respectively, 1 week prior). The patient was hyperkalemic, with a potassium of 5.6 mmol/l, and thrombocytopenic, with a platelet count of 71,000/μl (baseline 200,000/μl, 147,000/μl 1 week prior). He was noted to have an anion gap metabolic acidosis with bicarbonate of 20.6 mmol/l and an anion gap of 18 mmol/l. There was no history of nephrotoxic agents or new medications to explain the patient s rapid decline in renal function. Initial noncontrast computed tomography (CT) revealed a rightsided lung infiltrate, possible acute cholecystitis, and a nonobstructive calculus in the parenchyma of the left kidney. Bilateral pelvic calcifications of indeterminate relationship to the distal ureters were also noted, however, no hydronephrosis was appreciated. Renal ultrasound showed bilateral medical renal disease and mild-to-moderate right midrenal arterial stenosis. Examination of urine sediment was significant for white and red blood cells, protein, and positive for nitrite and large leukocyte esterase. During the course of hospitalization, urine culture was noted to be negative. The patient s mental status continued to worsen and urine output did not respond to multiple fluid challenges. The patient s hyperkalemia continued to worsen and hemodialysis was initiated within 24 h of presentation. Further laboratory testing was sent and findings of significance include hypocomplementemia (C3: 76 mg/dl, repeat 90 mg/dl; C4: 5 mg/dl, repeat 7 mg/dl); serum protein electrophoresis (SPEP) revealed hypoproteinemia and hypoalbuminemia, with no evidence of monoclonal spike. Urine protein electrophoresis (UPEP) was not sent secondary to anuria. Serologic tests were negative for anti-gbm antibody, Hepatitis B Surface Antigen/Antibody and Hepatitis C Antibody, antinuclear antibody (ANA), cryoglobulins, and myeloperoxidase (MPO) antibody. Hemolytic-uremic syndrome (HUS) and thrombotic thrombocytopenic purpura (TTP) workup was negative as well. The patient underwent right kidney biopsy on his 4 th day of hospitalization, which showed multiple globally sclerosed glomeruli and severe endocapillary proliferation with neutrophil infiltrates and podocyte hyperplasia (Fig. 1). Some glomeruli showed massive eosinophilic subepithelial deposits in a global or segmental pattern (Fig. 2). Congo red stain was negative for amyloid deposits. On immunofluorescence (IF), two glomeruli showed weak staining for IgG and C3 along capillary walls (Figs. 3 and 4). Electron microscopy (EM) revealed glomeruli with large subepithethial deposits varying in size and focal subendothelial, mesangial, and podocyte cytoplasm deposits (Figs. 5 and 6). These deposits were organized and randomly arranged in nonbranching microtubules, with a thick wall and an electron-lucent core measuring nm in diameter (Figs. 7 and 8). Deposits included nonorganized mixed granular and organized tubular types. Podocytes showed severe swelling and foot process effacement. There were no findings suggestive of acute tubular necrosis (ATN). Differential diagnosis of the biopsy included IGN, cryoglobulinemia glomerulonephritis, lupus nephritis, and acute postinfectious glomerulonephritis. The features of organized microtubules and the dominant subepithelial localization of the deposits were most consistent with a diagnosis of IGN. FIGURE 1. H&E stain: endocapillary hypercellularity with neutrophil infiltrate. 1349


.")


3 FIGURE 2. Trichrom stain: endocapillary hypercellularity and large subepithelial deposits (red). FIGURE 3. IF: IgG. FIGURE 4. IF: C3. FIGURE 5. EM: diffuse subepithelial deposits. FIGURE 6. EM: focal mesangial deposits. 1350


4 FIGURE 7. EM: subepithelial deposit with microtubule ultrastructure. FIGURE 8. EM: measurements of microtubules. DISCUSSION IGN is a rare disease that falls into the category of Ig component deposition disorders and EM is the gold standard for diagnosis[1,2]. It is interesting to note that unlike the other pathologies that are described in this group, the Ig components found in IGN are often not monoclonal, and in many cases, the deposits contain intact Ig molecules rather than solely light or heavy chains. IGN is categorized into this particular group due the similarities it shares with the amyloid syndromes such as the fibril-forming capacity of the pathogenic proteins. However, unlike amyloid, IGN does not stain with Congo red or thioflavine-t, and it has been postulated that many cases previously diagnosed as Congo-red negative amyloidosis were in fact IGN. The morphologic uniformity of the fibrils seen in individual IGN patients, as well as the presence of a lymphoproliferative disorder in some, has raised the question of whether a monoclonal component is necessary for fibril formation. It has also been suggested that the polyclonality of IGN may be due to the incorporation of Ig molecules into a fibril with a monoclonal core [1]. Fibrillary glomerulopathy (FGN) is considered by some to be a subset within the diagnosis of IGN due to the amyloid-like fibrils and similar EM findings. In a study of 14 IGN and nine FGN patients, clinical symptoms, including hypertension, nephrotic syndrome, and hematuria, as well as mean diameter of substructures, were similar when comparing the two pathologies. At diagnosis, there was no significant difference between the two groups when comparing age, serum Cr levels, incidence of microscopic hematuria, hypertension, and renal failure[3]. However, the two diseases have been shown to be morphologically different[3]. EM in patients with IGN show extracellular microtubule deposits arranged in densely packed parallel arrays with well-defined borders. These microtubles are >30 nm in diameter, have a central lumen, are electron lucent, and are predominantly found in the subepithelial space and mesangium. Deposition is almost always limited to the kidney. Renal biopsies of patients with FGN display randomly arranged extracellular fibrils that are 30 nm in diameter, with poorly defined borders and no central lumen. These deposits are unbranched and are predominantly mesangial and subepithelial as in IGN; however, in some cases, fibrils extend through the lamina densa of the GBM in patients with FGN[4]. Immunofluorescence in IGN shows circulating paraprotein or monoclonal Ig deposition in the glomeruli and is positive for IgG, C3, and κ and λ light chains. The deposits may be extensive as to give the appearance of linear IgG deposition similar to that seen in anti-gbm antibody disease. IgG4 has been shown to be the predominant IgG in deposits[3]. Immunologically, patients may have low titers of often- 1351
5 speckled ANA with normal levels of complements. As in our patient, serologic workup is usually unremarkable, although one patient in the Bridoux study did have low levels of C3 and C4 as in this patient. Presentation Most cases of IGN are idiopathic. The average age of presentation is approximately 45 years, however it ranges from years. Patients present with features similar to other primary renal diseases associated with nephrotic range proteinuria. In approximately 60 70% of cases, patients have microscopic hematuria and 50% of patients are hypertensive with renal insufficiency. In most cases, patients develop end-stage renal disease (ESRD) within 2 6 years. A study done on patients with FGN showed that the time to ESRD varied depending on histology on light microscopy. Median times were as follows[7]: 7 months, diffuse sclerosing 20 months, diffuse proliferative 44 months, membranoproliferative 80 months, mesangial proliferative/sclerosing 87 months, membranous Our patient is different from all of the cases thus far presented in the literature as he progressed to ESRD within 1 week of initial symptoms. His BUN and Cr increased in this time from 25 to 136 mg/dl and 1.2 to 20 mg/dl, respectively. Of the cases of IGN cited to date, all of the patients have shown a much more prolonged progression to ESRD. Although the biopsy did not show evidence for ATN, the presence of concurrent pulmonary and biliary tract processes may have set the stage for renal ischemic injury that was not appreciated on the sampled kidney tissue. Of note, studies have also shown that IGN can be associated with chronic lymphocytic leukemia (CLL) or B-cell lymphoma, and association with neoplasia has been shown to be more pronounced in patients with circulating monoclonal paraprotein. Hepatitis C, cryoglobulinemia, and systemic lupus erythematosus have also been shown to be associated with IGN[5]. In 1992, Alpers found that six of 11 patients with larger microtubules had associated dysproteinemia or lymphoproliferative disorder compared to one of 86 patients with smaller microtubules[6]. Rosenstock et al. showed an indistinguishable clinical picture between the two groups when separating IGN and FGN on the basis of fibril size; however, at presentation, patients with larger microtubules were more likely to have associated lymphoproliferative disorders and paraproteinemia[7]. In 1993, Fogo et al. found that patients with more organized arrays of larger microtubules were more likely to have hematopoietic disorders than patients with small, randomly oriented fibrils. In the Bridoux study, six IGN patients carried a diagnosis of CLL, one patient was diagnosed with small lymphocytic non-hodgkin s lymphoma, and three patients had small amounts of urinary Bence-Jones proteins[8]. Treatment Unfortunately, there have been no successful controlled trials to help provide guidance for appropriate therapy in patients with IGN and, thus far, no treatment has been proven to be effective. Both plasmapharesis and prednisone have been utilized with no obvious positive effects. In a study of 16 patients treated with prednisone and/or cytotoxic agents only, two patients experienced partial remission of proteinuria, with the remaining 14 patients having no response. The partial remission seen in these two patients was most likely related to a nonspecific reversal of the acute inflammatory process[9]. In the Bridoux study, 10 of 12 nephrotic IGN patients with an underlying lymphoproliferative disease and/or paraproteinemia showed complete or partial remission of nephrotic syndrome after chemotherapy was 1352
6 completed[3]. As most patients progress to ESRD, dialysis or renal transplantation is necessary. Recurrent disease in the graft is a common occurrence (four of eight patients in one study), but the rate of progression is typically slower than in a native kidney transplant; thus, transplantation is not contraindicated[10]. In our case, given the variable responses to treatments documented in the literature with none proven to be effective, the age of our patient, his comorbidities, and the fact that he developed ESRD, the decision was made not to treat with any cytotoxic agents/steroids. CONCLUSION The differential diagnosis of IGN includes a multitude of pathologies, including cryoglobulinemia GN, lupus nephritis, acute postinfectious GN, and amyloidosis. IGN is often misdiagnosed as cryoglobulinemia as both diseases have features that overlap, such as the organized deposition of the microtubules. However, patients with IGN do not display lesions typical of cryoglobulinemia, such as dominant intracapillary hyaline thrombi or crystal inclusions within endothelial cells. A higher frequency of monoclonal Ig deposits are found in the subepithelium and intramembranously in the kidney in patients with IGN compared to cryoglobunemia as well[3]. In this case, the distinction could not be made based on morphologic features by EM. However, our patient s cryoglobulins were negative on initial and repeat testing. Lupus nephritis was excluded as ANA was negative and the patient displayed no other clinical signs of lupus. The presence of such small amounts of subendothelial deposits is also not compatible with Class IV lupus nephritis. Acute postinfectious GN specimens typically display dominant subepithelial hump deposits that are granular and nonorganized. The biopsy did not stain with Congo red, thus amyloidosis was ruled out. EM in this case revealed glomeruli with large subepithelial deposits of varying sizes. These deposits were randomly arranged in nonbranching microtubules with a thick wall and an electron-lucent core measuring nm in diameter. The deposits also included nonorganized mixed granular and tubular types. These features were pathognomonic for IGN. IGN is a diagnosis that is often missed or overlooked as it presents in a similar manner to many other renal diseases and cannot be confirmed without biopsy. Our patient presented with IGN that progressed to ESRD rapidly. Thus far in the literature, IGN and FGN have been described by a subacute progression to ESRD ranging from 7 months to 10 years. This is the first case reported of a patient with a diagnosis of IGN who developed acute kidney injury (AKI) and ESRD within 1 week of initial presentation. REFERENCES 1. Dember, L.M. (2006.) Light chains, casts, sheets and fibrils: monoclonal immunoglobulin diseases and immunotactoid/fibrillary glomerulopathy. Clin. J. Am. Soc. Nephrol. 1, Iskandar, S.S., Falk, R.J., and Jennette, J.C. (1992) Clinical and pathologic features of fibrillary glomerulonephritis. Kidney Int. 42, Bridoux, F., Hugue, V., Coldefy, O., et al. (2002) Fibrillary glomerulonephritis and immunotactoid (microtubular) glomerulopathy are associated with distinct immunologic features. Kidney Int. 62, Korbet, S.M., Schwartz, M.M., and Lewis, E.J. (2006) Immuotactoid glomerulopathy (fibrillary glomerulonephritis). Clin. J. Am. Soc. Nephrol. 1, Touchard, G., Preud'homme, J.L., Aucouturier, P., et al. (1989) Nephrotic syndrome associated with chronic lymphocytic leukemia: an immunological and pathological study. Clin. Nephrol. 31(2), Alpers, C.E. (1992) Immunotactoid (microtubular) glomerulopathy: an entity distinct from fibrillary glomerulonephritis. Am. J. Kidney Dis. 19, Rosenstock, J.L., Markowitz, G.S., Valeri, A.M., et al. (2003) Fibrillary and immunotactoid glomerulonephritis: distinct entities with different clinical and pathologic features. Kidney Int. 63, Fogo, A., Qureshi, N., and Horn, R.G. (1993) Morphologic and clinical features of fibrillary glomerulonephritis versus immunotactoid glomerulopathy. Am. J. Kidney Dis. 22, D'Agati, V., Sacchi, G., Truong, L., et al. (1991) Fibrillary glomerulopathy: defining the disease spectrum. J. Am. Soc. Nephrol. 2,
7 10. Pronovost, P.H., Brady, H.R., Gunning, M.E., et al. (1996) Clinical features, predictors of disease progression and results of renal transplantation in fibrillary/immunotactoid glomerulopathy. Nephrol. Dial. Transplant. 11, This article should be cited as follows: Jain, S. and Chhabra, D. (2009) A case of immunotactoid glomerulopathy with rapid progression to end-stage renal disease. TheScientificWorldJOURNAL 9, DOI /tsw








8 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
A Case of IgG2 Heavy Chain Deposition Disease in a Patient with Kappa Positive Plasma Cell Dyscrasia
 Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Article. Laser Microdissection and Proteomic Analysis of Amyloidosis, Cryoglobulinemic GN, Fibrillary GN, and Immunotactoid Glomerulopathy
 Article Laser Microdissection and Proteomic Analysis of Amyloidosis, Cryoglobulinemic GN, Fibrillary GN, and Immunotactoid Glomerulopathy Sanjeev Sethi,* Jason D. Theis,* Julie A. Vrana,* Fernando C. Fervenza,
Article Laser Microdissection and Proteomic Analysis of Amyloidosis, Cryoglobulinemic GN, Fibrillary GN, and Immunotactoid Glomerulopathy Sanjeev Sethi,* Jason D. Theis,* Julie A. Vrana,* Fernando C. Fervenza,
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis with Monoclonal Immunoglobulin Deposits of Lambda Light Chain
 Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Mr. I.K 58 years old
 Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
ACUTE GLOMERULONEPHRITIS. IAP UG Teaching slides
 ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG)
") Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits in 5 renal allografts
 Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
Immune profile of IgA-dominant diffuse proliferative glomerulonephritis
 Clin Kidney J (2014) 7: 479 483 doi: 10.1093/ckj/sfu090 Exceptional Case Immune profile of IgA-dominant diffuse proliferative glomerulonephritis Eric Wallace 1, Nicolas Maillard 2, Hiroyuki Ueda 2, Stacy
Clin Kidney J (2014) 7: 479 483 doi: 10.1093/ckj/sfu090 Exceptional Case Immune profile of IgA-dominant diffuse proliferative glomerulonephritis Eric Wallace 1, Nicolas Maillard 2, Hiroyuki Ueda 2, Stacy
Rituximab treatment for fibrillary glomerulonephritis
 Nephrol Dial Transplant (2014) 29: 1925 1931 doi: 10.1093/ndt/gfu189 Advance Access publication 27 May 2014 Rituximab treatment for fibrillary glomerulonephritis Jonathan Hogan, Michaela Restivo, Pietro
Nephrol Dial Transplant (2014) 29: 1925 1931 doi: 10.1093/ndt/gfu189 Advance Access publication 27 May 2014 Rituximab treatment for fibrillary glomerulonephritis Jonathan Hogan, Michaela Restivo, Pietro
Jo Abraham MD Division of Nephrology University of Utah
 Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Lab 3, case 1. Is this an example of nephrotic or nephritic syndrome? Why? Which portion of the nephron would you expect to be abnormal?
 Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Journal of Nephropathology
 www.nephropathol.com DOI: 10.15171/jnp.2017.36 J Nephropathol. 2017;6(3):220-224 Journal of Nephropathology Proliferative glomerulonephritis with monoclonal IgG deposits; an unusual cause of de novo disease
www.nephropathol.com DOI: 10.15171/jnp.2017.36 J Nephropathol. 2017;6(3):220-224 Journal of Nephropathology Proliferative glomerulonephritis with monoclonal IgG deposits; an unusual cause of de novo disease
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
29th Annual Meeting of the Glomerular Disease Collaborative Network
 29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
Membranoproliferative Glomerulonephritis
 Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Nephritic vs. Nephrotic Syndrome
 Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
LECTURE IN INTERNAL MEDICINE PROPAEDEUTICS 2017/2018
 SIGNS AND SYMPTOMS OF URINARY SYSTEM DISEASES (urinary syndrome, nephrotic syndrome, nephritic syndrome, urinary tract obstruction syndrome, hypertensive syndrome) LECTURE IN INTERNAL MEDICINE PROPAEDEUTICS
SIGNS AND SYMPTOMS OF URINARY SYSTEM DISEASES (urinary syndrome, nephrotic syndrome, nephritic syndrome, urinary tract obstruction syndrome, hypertensive syndrome) LECTURE IN INTERNAL MEDICINE PROPAEDEUTICS
Clinical pathological correlations in AKI
 Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
29 Glomerular disease: an overview
 29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
DIABETES MELLITUS. Kidney in systemic diseases. Slower the progression: Pathology: Patients with diabetes mellitus are prone to other renal diseases:
 Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
A PREGNANT FEMALE WITH FIBRILLARY GLOMERULONEPHRITIS AND LIVER CIRRHOSIS
 Case Report 201 A PREGNANT FEMALE WITH FIBRILLARY GLOMERULONEPHRITIS AND LIVER CIRRHOSIS Chi-Yuan Hung *, Chi-Jen Wu *, Han-Hsiang Chen *, Jui-Chi Yeh *, Tsang-En Wang **, Jeffrey Tzen ***, Yi-Chou Chen
Case Report 201 A PREGNANT FEMALE WITH FIBRILLARY GLOMERULONEPHRITIS AND LIVER CIRRHOSIS Chi-Yuan Hung *, Chi-Jen Wu *, Han-Hsiang Chen *, Jui-Chi Yeh *, Tsang-En Wang **, Jeffrey Tzen ***, Yi-Chou Chen
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review
 Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft
 Article Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D. Cornell,* Mary E. Fidler,* Mark Boelkins, Fernando C. Fervenza, Fernando
Article Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D. Cornell,* Mary E. Fidler,* Mark Boelkins, Fernando C. Fervenza, Fernando
Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT
 The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME
 CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
Ascites, a New Cause for Bilateral Hydronephrosis: Case Report
 Case Study TheScientificWorldJOURNAL (2009) 9, 1035 1039 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2009.112 Ascites, a New Cause for Bilateral Hydronephrosis: Case Report D. Jain*, S. Dorairajan, and
Case Study TheScientificWorldJOURNAL (2009) 9, 1035 1039 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2009.112 Ascites, a New Cause for Bilateral Hydronephrosis: Case Report D. Jain*, S. Dorairajan, and
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Biopsy Features of Kidney Allograft Rejection Banff B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy?
 CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab
 TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
Alterations of Renal and Urinary Tract Function
 Alterations of Renal and Urinary Tract Function Chapter 29 Urinary Tract Obstruction Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract The obstruction
Alterations of Renal and Urinary Tract Function Chapter 29 Urinary Tract Obstruction Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract The obstruction
Functions of the kidney:
 Diseases of renal system : Normal anatomy of renal system : Each human adult kidney weighs about 150 gm, the ureter enters the kidney at the hilum, it dilates into a funnel-shaped cavity, the pelvis, from
Diseases of renal system : Normal anatomy of renal system : Each human adult kidney weighs about 150 gm, the ureter enters the kidney at the hilum, it dilates into a funnel-shaped cavity, the pelvis, from
Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases
 Kidney International, Vol. 65 (2004), pp. 2145 2152 Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases MARK HAAS and JOSEPH A. EUSTACE Department of Pathology
Kidney International, Vol. 65 (2004), pp. 2145 2152 Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases MARK HAAS and JOSEPH A. EUSTACE Department of Pathology
DIABETIC NEPHROPATHY is a major
 KIDNEY BIOPSY TEACHING CASES Nodular Glomerulopathy in a 50-Year-Old Diabetic Man Erika R. Bracamonte, MD, Peter Hullman, MD, and Kelly D. Smith, MD, PhD INDEX WORDS: Diabetes; membranoproliferative glomerulonephritis;
KIDNEY BIOPSY TEACHING CASES Nodular Glomerulopathy in a 50-Year-Old Diabetic Man Erika R. Bracamonte, MD, Peter Hullman, MD, and Kelly D. Smith, MD, PhD INDEX WORDS: Diabetes; membranoproliferative glomerulonephritis;
Proliferative Glomerulonephritis with Monoclonal IgG Deposits
 JASN Express. Published on May 21, 2009 as doi: 10.1681/ASN.2009010110 Proliferative Glomerulonephritis with Monoclonal IgG Deposits Samih H. Nasr,* Anjali Satoskar, Glen S. Markowitz,* Anthony M. Valeri,
JASN Express. Published on May 21, 2009 as doi: 10.1681/ASN.2009010110 Proliferative Glomerulonephritis with Monoclonal IgG Deposits Samih H. Nasr,* Anjali Satoskar, Glen S. Markowitz,* Anthony M. Valeri,
Renal Disease. Please refer to the assignment page Three online modules TBLs
 Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
CJASN epress. Published on September 28, 2010 as doi: /CJN
 CJASN epress. Published on September 28, 2010 as doi: 10.2215/CJN.05750710 Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D.
CJASN epress. Published on September 28, 2010 as doi: 10.2215/CJN.05750710 Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D.
Immunotactoid Glomerulopathy
 DISEASE OF THE MONTH J Am Soc Nephrol 13: 1390 1397, 2002 Immunotactoid Glomerulopathy MELVIN M. SCHWARTZ,* STEPHEN M. KORBET, and EDMUND J. LEWIS *Department of Pathology and the Section of Nephrology,
DISEASE OF THE MONTH J Am Soc Nephrol 13: 1390 1397, 2002 Immunotactoid Glomerulopathy MELVIN M. SCHWARTZ,* STEPHEN M. KORBET, and EDMUND J. LEWIS *Department of Pathology and the Section of Nephrology,
Complement in vasculitis and glomerulonephritis. Andy Rees Clinical Institute of Pathology Medical University of Vienna
 Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors of Renal Outcome
 International Scholarly Research Network ISRN Pediatrics Volume 2011, Article ID 507298, 5 pages doi:10.5402/2011/507298 Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors
International Scholarly Research Network ISRN Pediatrics Volume 2011, Article ID 507298, 5 pages doi:10.5402/2011/507298 Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors
Monoclonal gammopathies consist of. Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis REVIEW
 REVIEW Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis Sanjeev Sethi, MD, PhD, and S. Vincent Rajkumar, MD Abstract Monoclonal gammopathy is characterized by circulating monoclonal immunoglobulin
REVIEW Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis Sanjeev Sethi, MD, PhD, and S. Vincent Rajkumar, MD Abstract Monoclonal gammopathy is characterized by circulating monoclonal immunoglobulin
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS
 GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
C3 Glomerulonephritis versus C3 Glomerulopathies?
 Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
ESRD Dialysis Prevalence - One Year Statistics
 Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Dense deposit disease with steroid pulse therapy
 Case Report Dense deposit disease with steroid pulse therapy Jun Odaka, Takahiro Kanai, Takane Ito, Takashi Saito, Jun Aoyagi, and Mariko Y Momoi Abstract Treatment of dense deposit disease DDD has not
Case Report Dense deposit disease with steroid pulse therapy Jun Odaka, Takahiro Kanai, Takane Ito, Takashi Saito, Jun Aoyagi, and Mariko Y Momoi Abstract Treatment of dense deposit disease DDD has not
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS
 MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
Membranous nephropathy. By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University
 Membranous nephropathy By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University Membranous nephropathy Definition: Immune complex glomerular disease in which immune deposits of IgG and complement
Membranous nephropathy By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University Membranous nephropathy Definition: Immune complex glomerular disease in which immune deposits of IgG and complement
Tuesday Conference 7/23/2013. Hasan Fattah
 Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi
 Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
A Case of Myeloma Kidney With Glomerular C3 Deposition
 Case Report World J Nephrol Urol. 2018;7(3-4):73-77 A Case of Myeloma Kidney With Glomerular C3 Deposition Asif Khan a, c, Khine Lam b, Suzanne El-Sayegh b, Elie El-Charabaty b Abstract Manuscript submitted
Case Report World J Nephrol Urol. 2018;7(3-4):73-77 A Case of Myeloma Kidney With Glomerular C3 Deposition Asif Khan a, c, Khine Lam b, Suzanne El-Sayegh b, Elie El-Charabaty b Abstract Manuscript submitted
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. HIV and the Kidney. Leah Haseley, MD. Presentation prepared by: LH NW AETC ECHO June 2012
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and the Kidney Leah Haseley, MD Presentation prepared by: LH NW AETC ECHO June 2012 Etiology of renal disease in HIV 1985- The virus 1995- The antivirals
NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and the Kidney Leah Haseley, MD Presentation prepared by: LH NW AETC ECHO June 2012 Etiology of renal disease in HIV 1985- The virus 1995- The antivirals
A case of heavy chain deposition disease complicated by acquired angioedema.
 Case Report http://www.alliedacademies.org/pathology-and-disease-biology/ A case of heavy chain deposition disease complicated by acquired angioedema. Rafia Chaudhry 1 *, Gautam Bhave 2, Rachel Fissell
Case Report http://www.alliedacademies.org/pathology-and-disease-biology/ A case of heavy chain deposition disease complicated by acquired angioedema. Rafia Chaudhry 1 *, Gautam Bhave 2, Rachel Fissell