All the New Medications: What Should I. Lauren LaBryer, MD Endocrinologist Oklahoma Heart Institute
|
|
|
- Rosemary Robbins
- 5 years ago
- Views:
Transcription
1 All the New Medications: What Should I Choose for NIDDM Lauren LaBryer, MD Endocrinologist Oklahoma Heart Institute
2 None Disclosures
3 Objectives To become familiar with the new medication classes for the treatment of Type 2 diabetes mellitus Become familiar with the advantages and disadvantages of the new classes of diabetes medications
4 Outline Background A1C Goals and Outcomes Case Presentation Review new medication classes DPP4 Inhibitors GLP1 Receptor Agonists GLP1 Receptor Agonist + Basal insulin combined SGLT2 Inhibitors Review case presentations Summary
5 Background
6 Prevalence of Diabetes and Prediabetes in the United States 140 Undiagnosed DM Persons (milli ions) Diagnosed DM Prediabetes Diabetes 9.1% of US population Prediabetes 37% of US population CDC. National diabetes fact sheet, CDC. National diabetes fact sheet, CDC. National diabetes statistics report,
7 Increase in Diabetes Parallels the Increase in Obesity in the United States Obesity* Diabetes 45 96% increase 12 43% increase (%) Population ( Population (%) *BMI 30 kg/m 2. CDC. National diabetes statistics report, Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, Mokdad AH, et al. JAMA. 1999;282: ; Mokdad AH, et al. Diabetes Care. 2000;23: ; Ogden CL, et al. JAMA. 2014;311:
8 Diabetes Morbidity and Mortality 7th leading cause of death in US Leading cause of blindness Most frequent cause of kidney failure Accounts for ~60% of nontraumatic lower limb amputations Doubles risk of periodontal disease Double risk of developing depression Increases patients susceptibility to acute illness Worsens the prognosis of patients with acute illness CDC. National diabetes statistics report, CDC. National diabetes fact sheet,
9 Relationship of A1C Goals and Outcome Microvascular complications 38% reduction in risk with every 1% reduction in A1C Macrovascular complications Reduction in risk with early, intensive treatment High-risk patients, intensive control may increase risk UKPDS Lancet 1998; HolmannNew EnglJ2008; Patel New EnglJ2008; Stratton BMJ 2008; Gerstein New EnglJ 2011.
10 Microvascular Complications Increase With Increasing A1C Diabetes Control and Complications Trial Relative Risk Retinopathy Nephropathy Neuropathy Microalbuminuria A1C (%) Skyler JS. Endocrinol Metab Clin North Am. 1996;25:
11 Intensive Glycemic Control Reduces Longterm Macrovascular Risk UKPDS T2D, newly diagnosed (N=4209) Proportion With MI Randomized treatment 15% risk reduction P= Years Conventional Intensive T2D, type 2 diabetes; UKPDS, United Kingdom Prospective Diabetes Study. Holman RR, et al. N Engl J Med. 2008;359:
12


13 Targets for Glycemic Control
14 DDP4 Inhibitors New Medication Classes GLP-1 Receptor Agonist (RA) GLP-1 RA + Basal insulin combination SGLT2 Inhibitors It is nowpossible to treat Type 2 diabetes mellitus effectively with a low risk for hypoglycemia, weight loss, robust lowering of A1C, a reduction in the need or frequency of self-monitored blood glucose levels, and even cardiac death reduction.
15
16 Case 1 52 year old man here for follow-up of Type 2 DM. His diabetes was diagnosed 4 years ago. A1C is 7.2%. Medications: Metformin1000 mg PO BID Atorvastatin20 mg QD Lisinopril10 mg PO QD ASA 81 mg PO QD For the last 3 months, he has been working on improving diet and increasing exercise. No history of pancreatitis. No personal or family history of medullary thyroid cancer. No recurrent yeast infections.
17 PMH: DM2 HTN Mixed hyperlipidemia Obesity (BMI 32) Case 1 CAD s/p stent 2 years ago BP 130/75 Normal BMP. Lipids at goal. Eye exam and vaccinations up-to-date Sensation to monofilament decreased on diabetic foot exam
18 Case 1 What is next best step in his diabetes management? A. No change in medication. A1C at goal. B. Add sulfonylurea (e.g., glipizide) C. Add SGLT-2 Inhibitor D. Add DPP-4 Inhibitor E. Add GLP-1 Receptor Agonist
19 Case 2 47 year old woman with Type 2 DM. A1C is 6.9%, however, she reports frequent low blood glucose levels (40 s-50 s mg/dl) in the afternoon associated with missed meals at work. No lows overnight or in the morning. She is also very frustrated with her weight. Trying to follow a low carbdiet with reduced portion sizes but has only lost 2 lbs over last 3 months. No history of pancreatitis. No personal or family history of medullary thyroid cancer. No history of yeast infections.
20 Case 2 Medications: Metformin500 mg PO BID Lantus10 units SQ QHS Glimepiride1 mg PO QD Atorvastatin10 mg PO QD Losartan100 mg PO QD ASA 81 mg PO QD
21 PMH: DM2 HTN Mixed HLD Diabetic kidney disease Case 2 BMI 34 egfr 40 BP: 116/65 Recent normal eye exam, up-to-date on vaccinations, normal diabetic foot exam
22 Case 2 What would you do for this individual? A. No change. A1C is at goal. B. Stop glimepiride. C. Stop glimepiride. Add GLP-1 receptor agonist D. Stop glimeperide. Add DPP-4 Inhibitor E. Stop glimeperide. Add SGLT-2 Inhibitor
23 Case 3 69 year old man here for follow-up of Type 2 DM. A1C 8.4%. Medications: Metformin 1000 mg PO BID Rosuvastatin 10 mg PO BID ASA 81 mg PO BID Lisinopril20 mg PO QD He reports a needle phobia and does not want any type of injectable therapy. He lives alone. Previously had lower A1C on SU, however, due to recurrent hypoglycemia the SU was discontinued. He reports irregular eating schedule.
24 Case 3 No history of pancreatitis. No personal or family history of medullary thyroid cancer. No history of yeast infections. PMH: DM2 Mild non-proliferative diabetic retinopathy, stable Peripheral neuropathy Mixed HLD HTN OSA on CPAP CAD s/p CABG
25 BP 140/80 BMI: 42 Case 3 Normal BMP. Lipids at goal. Up-to-date on eye exam and vaccinations
26 Case 3 What would you offer this patient? A. Restart SU at lower dose B. Start GLP-1 Agonist C. Start DPP-4 Inhibitor D. Start SGLT-2 Inhibitor E. Start a SGLT-2 and DPP-4 Inhibitor


27 GLP-1 & DPP-4 GLP-1 & DPP-4 GLP-1 & DPP-4 SGLT-2 GLP-1 & DPP-4 GLP-1


28 Normal Physiology: GLP-1 and DPP4
29 DPP-4 Inhibitors FDA-Approved Agents Alogliptin(Nesina) Linagliptin(Tradjenta) Saxagliptin(Onglyza) Sitagliptin(Januvia) Key Features Oral administration Increase endogenous GLP-1 levels Increase glucose-dependent insulin secretion Suppress glucagon production DPP-4, dipeptidyl peptidase 4; GIP, glucose-dependent insulinotropic polypeptide; GLP-1, glucagon-like peptide 1. Garber AJ, et al. Endocr Pract. 2016;22:
30 Glucose Control with DPP-4 Inhibitors Placebo-Adjusted Change from Baseline (Not Head-to-Head Trials) Monotherapy Add-on to Metformin Add-on to SU Alo 1 Lin 2 Sax 3 Sit 4 Alo 5 Lin 6 Sax 7 Sit 8 Alo 9 Lin 10, * Sax 11 Sit 12, A1C 0.5%-0.8% Baseline A1C (%) Placebo-adjuste d A1C (%) *SU + metformin. With or without metformin. Absolute change from baseline (active-controlled trial) DeFronzo RA, et al. Diabetes Care. 2008;31: Del Prato S, et al. Diabetes Obes Metab. 2011;13: Rosenstock J, et al. Curr Med Res Opin. 2009;25: Nauck MA, et al. Diabetes Obes Metab. 2007;9: Nauck MA, et al. Int J Clin Pract. 2009;63: Taskinen MR, et al. Diabetes Obes Metab. 2011;13: DeFronzo RA, et al. Diabetes Care. 2009;32: Charbonnel B, et al. Diabetes Care. 2006;29: Pratley RE, et al. Diabetes Obes Metab. 2009;11: Owens DR, et al. Diabet Med. 2011;28: Chacra AR, et al. Int J Clin Pract. 2009;63: Hermansen K, et al. Diabetes Obes Metab. 2007;9:
31 Weight Change with DPP-4 Inhibitors Absolute Change from Baseline (Not Head-to-Head Trials) Monotherapy Add-on to Metformin Add-on to SU Alo 1 Lin 2 Sax 3 Sit 4 Alo 5 Lin 6 Sax 7 Sit 8 Alo 9 Lin 10, * Sax 11 Sit 12, Weight (kg) NR Weight neutral NR NR, value not reported. *SU + metformin. With or without metformin. 1. DeFronzo RA, et al. Diabetes Care. 2008;31: Del Prato S, et al. Diabetes Obes Metab. 2011;13: Rosenstock J, et al. Curr Med Res Opin. 2009;25: Nauck MA, et al. Diabetes Obes Metab. 2007;9: Nauck MA, et al. Int J Clin Pract. 2009;63: Taskinen MR, et al. Diabetes Obes Metab. 2011;13: DeFronzo RA, et al. Diabetes Care. 2009;32: Charbonnel B, et al. Diabetes Care. 2006;29: Pratley RE, et al. Diabetes Obes Metab. 2009;11: Owens DR, et al. Diabet Med. 2011;28: Chacra AR, et al. Int J Clin Pract. 2009;63: Hermansen K, et al. Diabetes Obes Metab. 2007;9:
32 Hypoglycemia with DPP-4 Inhibitors Percentage of Patients Reporting Hypoglycemia (Not Head-to-Head Trials) Monotherapy Add-on to Metformin Add-on to SU Alo 1 Lin 2 Sax 3 Sit 4 Alo 5 Lin 6 Sax 7 Sit 8 Alo 9 Lin 10, * Sax 11 Sit 12, Patients (%) Rare hypoglycemia alone Consider decreasing dose of SU or insulin if in combination NR, value not reported. *SU + metformin. With or without metformin. 1. DeFronzo RA, et al. Diabetes Care. 2008;31: Del Prato S, et al. Diabetes Obes Metab. 2011;13: Rosenstock J, et al. Curr Med Res Opin. 2009;25: Nauck MA, et al. Diabetes Obes Metab. 2007;9: Nauck MA, et al. Int J Clin Pract. 2009;63: Taskinen MR, et al. Diabetes Obes Metab. 2011;13: DeFronzo RA, et al. Diabetes Care. 2009;32: Charbonnel B, et al. Diabetes Care. 2006;29: Pratley RE, et al. Diabetes Obes Metab. 2009;11: Owens DR, et al. Diabet Med. 2011;28: Chacra AR, et al. Int J Clin Pract. 2009;63: Hermansen K, et al. Diabetes Obes Metab. 2007;9:
33 Cardiovascular Outcome Trials


34 DDP4 Inhibitor CV Outcome Trials Jan 2018
35 Sulphonylureacompared to DPP-4 Inhibitors in combination with metformin All T2DM patients in Sweden Model adjusted for age, sex, CVD drugs, prior CVD diagnosis Met + SU = 40,736 Met + DPP4i = 12, 024 More hypoglycemia, CV events and mortality in SU-treated patients Erikson, JW et al DiabRes ClinPract ; 39-47
36 Stay Tuned CAROLINA TRIAL Cardiovascular Outcome Study of Linagliptin vs Glimepiride Ongoing, randomized trial Started date: 10/2010 Estimated Completion date: 2/2019 N = 6041 Reported patient characteristics: Median duration Type 2 DM: 6.2 years 60% male; 40% female Mean A1C 7.2% 34.5% had previous CV complications Marx, N et al. DiabVascDisRes May;12(3):
37 Stay Tuned CAROLINA TRIAL Primary Outcome: 3 point MACE CV death non-fatal MI non-fatal stroke Marx, N et al. DiabVascDisRes May;12(3):
38 Adverse Effects of DPP-4 Inhibitors Generally well tolerated Side-effects Headache Nausea, diarrhea, abdominal pain Peripheral edema Rare side-effects Acute pancreatitis sitagliptin Acute renal failure Bone fractures saxagliptin Angioedema
39 Safety Considerations with DPP-4 Inhibitors Pancreatitis No causal relationship established Discontinue if pancreatitis suspected No evidence of increased pancreatitic risk with incretins vs other agents Pancreatic cancer No evidence of increased pancreatic risk with incretins vs other agents Further assessments required from long duration controlled studies or epidemiological databases CHF Potentially increased risk of CHF hospitalization with alogliptin and saxagliptin Renal impairment Dose adjustment and periodic monitoring of kidney function in moderate-severe CKD EXCEPT linagliptin which is NOT renally excreted Garber AJ, et al. Endocr Pract. 2016;22: White W, et al. N Engl J Med. 2013;369: Scirica BM, et al. Circulation. 2014;130: ADA/EASD/IDF statement concerning the use of incretin therapy and pancreatic disease [news release]. Alexandria, VA: American Diabetes Association, European Association for the Study of Diabetes, International Diabetes Federation; June 28,
40 Key Points Once daily, oral therapy Clinically significant A1C reductions ( %) No/low hypoglycemia Consider reduction of dose of SU or insulin if used in combination Complementary mechanism of action with many drugs Don t use with GLP-1 receptor agonist Very well tolerated No weight gain, no hypoglycemia, no edema, minimal GI sx DPP-4 Inhibitors are safe in patients with CV disease.? Saxagliptin and alogliptin increase risk of hospitalizations for heart failure Need dose adjustment for moderate-severe CKD Except for linagliptin
41 GLP-1 Receptor Agonists FDA-Approved Agents Albiglutide(Tanzeum) Dulaglutide(Trulicity) Exenatide(Byetta) Exenatide ER (Bydureon) Liraglutide(Victoza) Lixisenatide(Aldyxin) Key Features Injectable administration Mimic action of native GLP-1 Increase glucose-dependent insulin secretion Suppress glucagon production Slow gastric emptying ER, extended release; GLP-1, glucagon-like peptide 1. Garber AJ, et al. Endocr Pract. 2016;22:

42 GLP-1 RA Dosing Daily dosing Once weekly dosing


43 Glucose Control with GLP-1 Receptor Agonists Head-to-Head Trials A1C 0.5%- 1.5% Trujillo, J et al. Therapeutic Advances in Endocrinology and Metabolism2015, 6(1): 19 28


44 Weight Change with GLP-1 Receptor Agonists Head-to-Head Trials Weight 2-6 lb Weight loss maintained Trujillo, J et al. Therapeutic Advances in Endocrinology and Metabolism2015, 6(1): 19 28
45 Hypoglycemia with GLP-1 Receptor Agonists Percentage of Patients Reporting Hypoglycemia (Not Head-to-Head Trials) Monotherapy Add-on to Metformin Add-on to SU Alb 1 Dul 2 Exe 3 Exe ER 4 Lir 5 Lix 6 Alb 7 Dul 8 Exe 9 Exe ER 10 Lir 11 Lix 12 Alb 13, * Exe 14 Exe ER 15, Lir 16 Patients (%) Rare hypoglycemia alone Consider decreasing dose of SU or insulin if in combination *Metformin with or without SU or TZD. Metformin with or without SU. 1. Nauck M, et al. Diabetes. 2013;62(suppl 2): Abstr. 55-LB. 2. Umpierrez G, et al. Diabetes Care. 2014;37: Moretto TJ, et al. Clin Ther. 2008;30: Russell-Jones D, et al. Diabetes Care. 2012;35: Garber A, et al. Lancet. 2009;373: Fonseca VA, et al. Diabetes Care. 2012;35: Ahrén B, et al. Diabetes Care. 2014;37: Dungan KM, et al. Lancet. 2014;384: DeFronzo RA et al. Diabetes Care. 2005;28: Bergenstal RM, et al. Lancet. 2010;376: Pratley RE, et al. Lancet. 2010;375: Rosenstock J, et al. Diabetes Care. 2013;36: Pratley RE, et al. Lancet Diabetes Endocrinol. 2014;2: Buse JB, et al. Diabetes Care. 2004;27: Diamant M, et al. Lancet. 2010;375: Marre M, et al. Diabet Med. 2009;26:
46 Cardiovascular Outcome Trials


47 April
48 LEADER (Liraglutide) Cardiovascular Outcome Trial CV death, MI, stroke Marso, S. et al N EnglJ Med 2016; 375(4): Liraglutide NOT FDA approved for CV death prevention
49 Adverse Effects with GLP-1 RA GI N/V, diarrhea or constipation Common Usually dose dependent and transient Usually reduced with dose titration Caution in patients with gastroparesis
50 Safety Considerations with GLP-1 RA Pancreatitis No causal relationship established Discontinue if pancreatitis suspected No evidence of increased pancreatic risk with incretins vs. other agents Pancreatic cancer No evidence of increased pancreatic risk with incretins vs. other agents Further assessments required from long duration controlled studies or epidemiological databases Medullary Thyroid Cancer Animal data showed increased incidence of C-cell tumors with liraglutide and exenatide ER treatment, but confirmatory population studies are lacking Labeling for liraglutide and exenatide ER: Patients should be counseled regarding MTC and the signs/symptoms of thyroid tumors Contraindicated in patients with personal/family history of MTC or MEN Type 2 Renal impairment Exenatide is contraindicated in patients with severe renal insufficiency or ESRD Liraglutide safe in moderate renal impairment Dulaglutide is safe in renal impairment Garber AJ, et al. Endocr Pract. 2016;22: White W, et al. N Engl J Med. 2013;369: Scirica BM, et al. Circulation. 2014;130: ADA/EASD/IDF statement concerning the use of incretin therapy and pancreatic disease [news release]. Alexandria, VA: American Diabetes Association, European Association for the Study of Diabetes, International Diabetes Federation; June 28,
51 Key Points Once daily or once weekly SQ injection Impressive clinically significant A1C reductions ( %) Both fasting and prandial blood glucose reductions No hypoglycemia Consider reduction of dose of SU or insulin if used in combination Sustained weight loss Slight decrease in SBP Beta-cell preservation Complementary mechanism of action with many drugs Don t use with DPP-4 Inhibitors GI side effects Less with weekly dosing Don t use if history of MTC/MEN2 Caution if history of pancreatitis or gastroparesis
52 Basal insulin + GLP-1 -Now available as combination injection
53 Basal insulin + GLP-1 Combination IGlarLixi(Soliqua) released Jan 2017 IDegLira(Xultophy) expected released June 2017

54 IGlarLixi
55 IGlarLixi 1 unit of IGlarLixi= 1 unit of Lantus mcg lixisenatide Dosing: If uncontrolled on basal insulin < 30 units/day Start 15 units of IGlarLixi If uncontrolled on basal insulin > 30 units/day Start 30 units of IGlarLixi Max dose 60 units Give within 1 hour of 1 st meal of the day Titrate weekly by 2-4 units until goal fasting glucose reached
56 IDegLira(Xultophy) Significant reduction in A1C relative to individual components
57 No weight gain when IDegLiraadded to Metformin +/-Pioglitazone
58 IDegLiraSafety Profile Safety profile consistent with individual components Some component adverse effects mitigated Confirmed hypoglycemia rates with IDegLira Consistently lower than with basal insulin Higher than GLP-1 RA or placebo Higher than GLP-1 RA or placebo GI AEs with IDegLira Lower than with GLP-1 RA Higher than with basal insulin alone No confirmed cases of pancreatitis CV safety reflective of components No cases of MTC
59 SGLT2 Inhibitors
60 SGLT2 Inhibitors FDA-Approved Agents Canagliflozin(Invokana) Dapagliflozin(Farxiga) Empagliflozin(Jardiance) Key Features Oral administration Inhibit reabsorption of glucose into the bloodstream from renal fluid SGLT2, sodium-glucose cotransporter 2. DeFronzo RA, et al. Diabetes Obes Metab. 2012;14:5-14.
61 Pathophysiology

62 Renal Glucose Threshold Effect of SGLT2 Inhibitor New TmG SGLT2 Inhibitor TmG Normal TmG Diabetes
63 Glucose Control with SGLT2 Inhibitors A1C 1% Muhammad A. Abdul-Ghani et al. Am J Physiol Renal Physiol 2015;309:F889-F900
64 Weight (kg) -0.5 Weight Change with SGLT2 Inhibitors Absolute Change from Baseline (Not Head-to-Head Trials) Monotherapy Add-on to Metformin Add-on to Insulin +/- OAs Can 1 Dap 2 Emp 3 Can 4 Dap 5 Emp 6 Can 7 Dap 8 Emp lb weight loss Stenlof K, et al. Diabetes Obes Metab. 2013;15: Ferrannini E, et al. Diabetes Care. 2010;33: Roden M, et al. Lancet Diabetes Endocrinol. 2013;1: Cefalu WT, et al. Lancet. 2013;382: Nauck MA, et al. Diabetes Care. 2011;34: Haring HU, et al. Diabetes Care. 2014;37: Yale J-F, et al. Diabetes Obes Metab. 2013;15: Wilding JPH, et al. Ann Intern Med. 2012;156: Rosenstock J, et al. Diabetes Care. 2014;37:
65 Patients (%) Hypoglycemia with SGLT2 Inhibitors Percentage of Patients Reporting Hypoglycemia (Not Head-to-Head Trials) Monotherapy Add-on to Metformin Add-on to Insulin +/- OAs Can 1 Dap 2 Emp 3 Can 4 Dap 5 Emp 6 Can 7 Dap 8 Emp 9 Rare hypoglycemia alone Consider decreasing dose of SU or insulin if in combination < Stenlof K, et al. Diabetes Obes Metab. 2013;15: Ferrannini E, et al. Diabetes Care. 2010;33: Roden M, et al. Lancet Diabetes Endocrinol. 2013;1: Cefalu WT, et al. Lancet. 2013;382: Nauck MA, et al. Diabetes Care. 2011;34: Haring HU, et al. Diabetes Care. 2014;37: Yale J-F, et al. Diabetes Obes Metab. 2013;15: Wilding JPH, et al. Ann Intern Med. 2012;156: Rosenstock J, et al. Diabetes Care. 2014;37:
66 Cardiovascular Outcomes Trials


67


68
69 EMPA-REG Baseline Characteristics Baseline Characteristics Placebo N= 2, 333 Empaglafozin N = 4,687 Mean Age (years) 63 (+/-9) 63 (+/-9) Male (%) Race % - - White Asian Black/ AfricanAmerican 5 5 MeanBMI 31 +/ /-5
70 EMPA-REG Baseline Characteristics Baseline Characteristics Placebo N= 2, 333 Empaglafozin N = 4,687 Established CVD* (%) CAD History of MI History of stroke PAD 21 21
71 CV death stroke MI EMPA-REG Outcome
72 EMPA-REG Cardiovascular Outcome Study CV death stroke MI 14% relative risk reduction 1.6% Absolute risk reduction ZinmanB et al. N EnglJ Med. 2015; 373:
73 EMPA-REG Cardiovascular Outcome Study 38% relative risk reduction 2.2% Absolute risk reduction FDA approved to reduce the risk of CV death in adults with Type 2 DM and established CV disease


74 Number Needed to Treat To Prevent Death in High CV risk Group 1. 4S Investigator, Lancet 1994; 344: HOPE Investigator. N EnglJ Med 2000; 342:
75 Number Needed to Treat To Prevent Death NNT = over years to prevent1 CV death 1. 4S Investigator, Lancet 1994; 344: HOPE Investigator. N EnglJ Med 2000; 342:
76 Is it a Class Effect?
77 Awaiting results of CANVAS and DECLARE, but
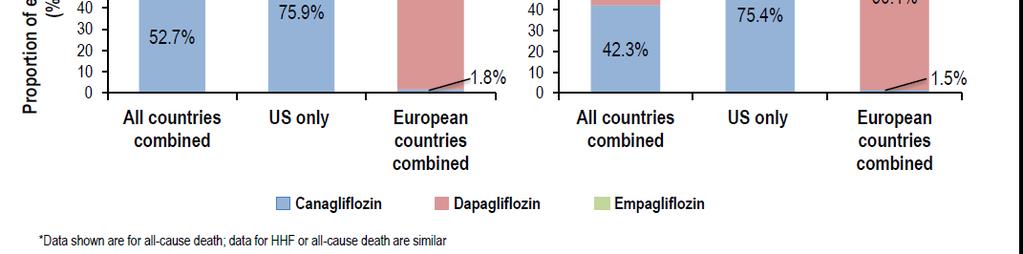
78 CVD REAL
79 CVD-REAL Trial


80
81
82


83


84

85


86

87

88
89 Renal Benefit of SGLT2 Inhibitors?
90 EMPA-REG Outcome Trial Assessment of renal outcome was pre-specified objective Main renal outcomes Incident or worsening nephropathy defined as: Doubling of serum Cr with egfr<45 ml/min/1.73m2 or Initiation of renal replacement therapy or Death due to renal disease
91
92
93 Adverse Effects of SGLT-2 Inhibitors Genital Mycotic Infection (Yeast infections) Empa-reg study: 6.5% developed vs. 1.8% placebo Rare cause of discontinuation (0.8%) Avoid use in patients with recurrent yeast infections Treat if necessary Hypotension Avoid use in patients with low blood pressure or tendency for volume depletion Counsel patients to stay well hydrated LDL-C Small increases in LDL-C have been observed
94 Safety Considerations SGLT-2 Inhibitors Renal Impairment Monitor renal function Dapaglifozin Avoid use if egfr< 60 ml/min/1.73 m 2 Canaglifozin Avoid if egfr< 45 ml/min/1.73 m 2 Empagliflozin Avoid if egfr< 45 ml/min/1.73 m 2 Bone fractures Increased incidence of bone fractures in canagliflozinand dapaglifozin clinic trials Canagliflozinlabeling includes specific warning about bone fractures
95 Safety Considerations SGLT-2 Inhibitors DKA Potentially increased risk of diabetic ketoacidosisin patients with insulin deficiency and/or those undergoing acute metabolic stress Bladder cancer Increased incidence of bladder cancers in patients receiving dapagliflozin Dapagliflozinlabeling recommends not using in patients with active bladder cancer and should be used with caution in patients with a history of bladder cancer
96 Key Points Once daily, oral therapy Clinically significant A1C reductions (~1%) Increased reduction in more uncontrolled DM Significant weight loss Blood pressure improvements Empagliflozin has FDA approval for CV death prevention Class effect????
97 Key Points Low risk hypoglycemia Consider reduction of dose of SU or insulin if used in combination Complementary mechanism of action with many drugs Very well tolerated Increased risk of GU infections: Don t use if already an issue Treat if needed Avoid use if GFR < 45 Or if egfr< 60 for dapaglifozin Potential renal protection??
98 Case 1 52 year old man here for follow-up of Type 2 DM. His diabetes was diagnosed 4 years ago. A1C is 7.2%. Medications: Metformin1000 mg PO BID Atorvastatin20 mg QD Lisinopril10 mg PO QD ASA 81 mg PO QD For the last 3 months, he has been working on improving diet and increasing exercise. No history of pancreatitis. No personal or family history of medullary thyroid cancer. No recurrent yeast infections.
99 PMH: DM2 HTN Mixed hyperlipidemia Obesity (BMI 32) Case 1 CAD s/p stent 2 years ago BP 130/75 Normal BMP. Lipids at goal. Eye exam and vaccinations up-to-date Sensation to monofilament decreased on diabetic foot exam
100 Case 1 What is next best step in his diabetes management? A. No change in medication. A1C at goal. B. Add sulfonylurea (e.g., glipizide) C. Add SGLT-2 Inhibitor D. Add DPP-4 Inhibitor E. Add GLP-1 Receptor Agonist
101 Case 1 What is next best step in his diabetes management? A. No change in medication. A1C at goal. B. Add sulfonylurea C. Add SGLT-2 Inhibitor Likely my first choice in this patient D. Add DPP-4 Inhibitor E. Add GLP-1 Receptor Agonist Great alternative
102 Case 2 47 year old woman with Type 2 DM. A1C is 6.9%, however, she reports frequent low blood glucose levels (40 s-50 s mg/dl) in the afternoonassociated with missed meals at work. No lows overnight or in the morning. She is also very frustrated with her weight. Trying to follow a low carbdiet with reduced portion sizes but has only lost 2 lbs over last 3 months. No history of pancreatitis. No personal or family history of medullary thyroid cancer. No history of yeast infections.
103 Case 2 Medications: Metformin500 mg PO BID Lantus10 units SQ QHS Glimepiride1 mg PO QD Atorvastatin10 mg PO QD Losartan100 mg PO QD ASA 81 mg PO QD
104 PMH: DM2 HTN Mixed HLD Diabetic kidney disease Case 2 BMI 34 egfr 40 BP: 116/65 Recent normal eye exam, up-to-date on vaccinations, normal diabetic foot exam
105 Case 2 What would you do for this individual? A. No change. A1C is at goal. B. Stop glimepiride. C. Stop glimepiride. Add GLP-1 receptor agonist D. Stop glimeperide. Add DPP-4 Inhibitor E. Stop glimeperide. Add SGLT-2 Inhibitor
106 Case 2 What would you do for this individual? A. No change. A1C is at goal. B. Stop glimepiride. C. Stop glimepiride. Add GLP-1 Receptor agonist D. Stop glimeperide. Add DPP-4 Inhibitor E. Stop glimeperide. Add SGLT-2 Inhibitor
107 Case 3 69 year old man here for follow-up of Type 2 DM. A1C 8.4%. Medications: Metformin 1000 mg PO BID Rosuvastatin 10 mg PO BID ASA 81 mg PO BID Lisinopril20 mg PO QD He reports a needle phobia and does not want any type of injectable therapy. He lives alone. Previously had lower A1C on SU, however, due to recurrent hypoglycemia the SU was discontinued. He reports irregular eating schedule.
108 Case 3 No history of pancreatitis. No personal or family history of medullary thyroid cancer. No history of yeast infections. PMH: DM2 Non-proliferative diabetic retinopathy Peripheral neuropathy Mixed HLD HTN OSA on CPAP CAD s/p CABG
109 BP 140/80 BMI: 42 Case 3 Normal BMP. Lipids at goal. Up-to-date on eye exam and vaccinations
110 Case 3 What would you offer this patient? A. Restart SU at lower dose B. Start GLP-1 Agonist C. Start DPP-4 Inhibitor D. Start SGLT-2 Inhibitor E. Start a SGLT-2 and DPP-4 Inhibitor
111 Case 3 What would you offer this patient? A. Restart SU at lower dose B. Start GLP-1 Agonist C. Start DPP-4 Inhibitor D. Start SGLT-2 Inhibitor E. Start a SGLT-2 and DPP-4 Inhibitor
112 Summary Goal A1C <6.5%, but need to individualize Achieving goal reduces complications Metformin first line 2 nd line: GLP-1 RA, SGLT2i, DPP4i
113 Summary GLP-1 Receptor Agonist Promote weight loss Reduce BP Low risk hypoglycemia Cardiac benefits? SGLT-2 Inhibitor Promote weight loss Reduce BP Low risk hypoglycemia Cardiac death reduction Renal protection?
Speaker Disclosures 6/17/ :07 AM. Management of Type 2 Diabetes: From Pathophysiology to Pharmacology
 Speaker Disclosures Management of Type 2 Diabetes: From Pathophysiology to Pharmacology Barry S. Horowitz, MD, FACE, FACP Clinical Research: Eli Lilly, NovoNordisk, Amgen, Pfizer, Sanofi, GSK, Lexicon,
Speaker Disclosures Management of Type 2 Diabetes: From Pathophysiology to Pharmacology Barry S. Horowitz, MD, FACE, FACP Clinical Research: Eli Lilly, NovoNordisk, Amgen, Pfizer, Sanofi, GSK, Lexicon,
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies. Module D
 Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Ertugliflozin (Steglatro ) 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy
 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy") Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL
 Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
OBESITY IN TYPE 2 DIABETES
 OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
DIABETES UPDATE NON INSULIN THERAPY
 American College of Physicians (ACP) Northern California Chapter Scientific Meeting Walnut Creek (2017) DIABETES UPDATE NON INSULIN THERAPY FOCUS ON: INCRETIN THERAPY (DPP41, GLP1-RA) & SGLT2 INHIBITORS
American College of Physicians (ACP) Northern California Chapter Scientific Meeting Walnut Creek (2017) DIABETES UPDATE NON INSULIN THERAPY FOCUS ON: INCRETIN THERAPY (DPP41, GLP1-RA) & SGLT2 INHIBITORS
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD. Disclosures. Objectives 9/1/2015
 Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Type 2 Diabetes Management: Case 1: Reducing Hypoglycemic Risk Case 2: Reducing Cardiovascular Risk
 Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
California Chapter of the American Association of Clinical Endocrinologists AACE Presents: Hot Topics in Diabetes and Endocrinology for Primary Care
 California Chapter of the American Association of Clinical Endocrinologists AACE Presents: Hot Topics in Diabetes and Endocrinology for Primary Care New Advances in Pharmacotherapy in Management of Patients
California Chapter of the American Association of Clinical Endocrinologists AACE Presents: Hot Topics in Diabetes and Endocrinology for Primary Care New Advances in Pharmacotherapy in Management of Patients
Jaiwant Rangi, MD, FACE
 California Chapter of American Association of Clinical Endocrinologists Presents HOT TOPICS IN DIABETES AND ENDOCRINOLOGY FOR PRIMARY CARE Diabetes Update Non Insulin Therapy Focus on: Incretin Therapy
California Chapter of American Association of Clinical Endocrinologists Presents HOT TOPICS IN DIABETES AND ENDOCRINOLOGY FOR PRIMARY CARE Diabetes Update Non Insulin Therapy Focus on: Incretin Therapy
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018
 GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
California Chapter of the American Association of Clinical Endocrinologists AACE Presents: Hot Topics in Diabetes and Endocrinology for Primary Care
 California Chapter of the American Association of Clinical Endocrinologists AACE Presents: Hot Topics in Diabetes and Endocrinology for Primary Care New Advances in Pharmacotherapy in Management of Patients
California Chapter of the American Association of Clinical Endocrinologists AACE Presents: Hot Topics in Diabetes and Endocrinology for Primary Care New Advances in Pharmacotherapy in Management of Patients
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors. Bryce Fukunaga PharmD April 25, 2018
 Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM
 Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
What s the Goal? Individualizing Glycemic Targets. Matthew Freeby M.D. December 3 rd, 2016
 What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Incredible Incretins Abby Frye, PharmD, BCACP
 Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Metformin although effective has become obsolete
 Metformin although effective has become obsolete Does not address core needs as well as other agents (ominous octet) Does not address metabolic parameters (blood pressure, Hgb A1C) as well as other agents
Metformin although effective has become obsolete Does not address core needs as well as other agents (ominous octet) Does not address metabolic parameters (blood pressure, Hgb A1C) as well as other agents
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S.
 GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Diabetes Risk Assessment and Treatment
 Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
Joshua Settle, PharmD Clinical Pharmacist Baptist Medical Center South ALSHP Fall Meeting September 30, 2016
 Joshua Settle, PharmD Clinical Pharmacist Baptist Medical Center South jjsettle@baptistfirst.org ALSHP Fall Meeting September 30, 2016 Objectives Describe the current information concerning newly approved
Joshua Settle, PharmD Clinical Pharmacist Baptist Medical Center South jjsettle@baptistfirst.org ALSHP Fall Meeting September 30, 2016 Objectives Describe the current information concerning newly approved
Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii
 Individualized Diabetes Treatment for the Elderly Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii Extremely Relevant Baby Boomers are aging! ¼ of people age
Individualized Diabetes Treatment for the Elderly Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii Extremely Relevant Baby Boomers are aging! ¼ of people age
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Halting the Rise, Newest Non- Insulin Options for Lowering A1c
 Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c
 Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Therapeutic strategy to reduce Glucagon secretion
 Clinical focus on glucagon: α-cell as a companion of β-cell Therapeutic strategy to reduce Glucagon secretion Sunghwan Suh Dong-A University Conflict of interest disclosure None Committee of Scientific
Clinical focus on glucagon: α-cell as a companion of β-cell Therapeutic strategy to reduce Glucagon secretion Sunghwan Suh Dong-A University Conflict of interest disclosure None Committee of Scientific
WITH SO MANY NEW CLASSES OF MEDICATIONS OUT THERE
 UPDATE ON THE NEW DIABETES MEDICATIONS AND HOW TO INCORPORATE INTO YOUR PRACTICE Amy DeGueme, MD, ECNU Madison Medical Affiliates 3/15/19 WITH SO MANY NEW CLASSES OF MEDICATIONS OUT THERE Which ones to
UPDATE ON THE NEW DIABETES MEDICATIONS AND HOW TO INCORPORATE INTO YOUR PRACTICE Amy DeGueme, MD, ECNU Madison Medical Affiliates 3/15/19 WITH SO MANY NEW CLASSES OF MEDICATIONS OUT THERE Which ones to
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Top HF Trials to Impact Your Practice
 Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Medication for the Management of Diabetes Mechanism of. Duration of Daily Dosing Action
 Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
Disclaimers 22/03/2018. Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2
 Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
Presented By: Creative Educational Concepts, Inc. Lexington, KY
 Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of April 2015. The content and views presented in this educational activity are those of the
Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of April 2015. The content and views presented in this educational activity are those of the
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
THE NEW-ISH DIABETES MEDICINES
 THE NEW-ISH DIABETES MEDICINES Using GLP1s and SGLT2s FINANCIAL DISCLOSURES None Brent Jones, MD Endocrinology Madison Medical Affiliates January 31, 2019 OBJECTIVES Gain familiarity with GLP1 receptor
THE NEW-ISH DIABETES MEDICINES Using GLP1s and SGLT2s FINANCIAL DISCLOSURES None Brent Jones, MD Endocrinology Madison Medical Affiliates January 31, 2019 OBJECTIVES Gain familiarity with GLP1 receptor
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Type 2 Diabetes Novel Therapies and Difficult Cases
 Type 2 Diabetes Novel Therapies and Difficult Cases Matt Dowell, DO Type 2 Diabetes - An Epidemic Is Here 1 Age-Adjusted Prevalence of Diagnosed Diabetes Among US Adults 2005 Missing data
Type 2 Diabetes Novel Therapies and Difficult Cases Matt Dowell, DO Type 2 Diabetes - An Epidemic Is Here 1 Age-Adjusted Prevalence of Diagnosed Diabetes Among US Adults 2005 Missing data
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
GLP-1-based therapies in the management of type 2 diabetes
 GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
AACE Diabetes Algorithm- Focus on: SGLT2-inhibitors and GLP1-ra Therapies
 California Chapter of the American Association of Clinical Endocrinologists Presents: Hot Topics in Diabetes and Endocrinology for Primary Care AACE Diabetes Algorithm- Focus on: SGLT2-inhibitors and GLP1-ra
California Chapter of the American Association of Clinical Endocrinologists Presents: Hot Topics in Diabetes and Endocrinology for Primary Care AACE Diabetes Algorithm- Focus on: SGLT2-inhibitors and GLP1-ra
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC
 MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
3/8/2011. Julie M. Sease, Pharm D, BCPS, CDE Associate Professor of Pharmacy Practice Presbyterian College School of Pharmacy
 Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
GLP-1. GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4.
 GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
Injectable Agents for Type 2 Diabetes. Richard Christensen, MD AACE Diabetes Day, Boise, ID September 2017
 Injectable Agents for Type 2 Diabetes Richard Christensen, MD AACE Diabetes Day, Boise, ID September 2017 Financial Disclosures Sanofi speaker honoraria No other relevant financial disclosures Injectable
Injectable Agents for Type 2 Diabetes Richard Christensen, MD AACE Diabetes Day, Boise, ID September 2017 Financial Disclosures Sanofi speaker honoraria No other relevant financial disclosures Injectable