Update on Agents for Type 2 Diabetes
|
|
|
- Melvyn Horton
- 5 years ago
- Views:
Transcription
1 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific concerns, adverse drug reactions, and contraindications Discuss the role and timing of combination therapy in achieving A1C goals Explain the implications of recent, large randomized clinical trials on clinical decision-making
2

3 Approach to Management of Hyperglycemia ADA. V. Diabetes Care. Diabetes Care. 2014;37(suppl 1):S25. Figure 1. Adapted with permission from Ismail-Beigi F, et al. Ann Intern Med 2011;154:



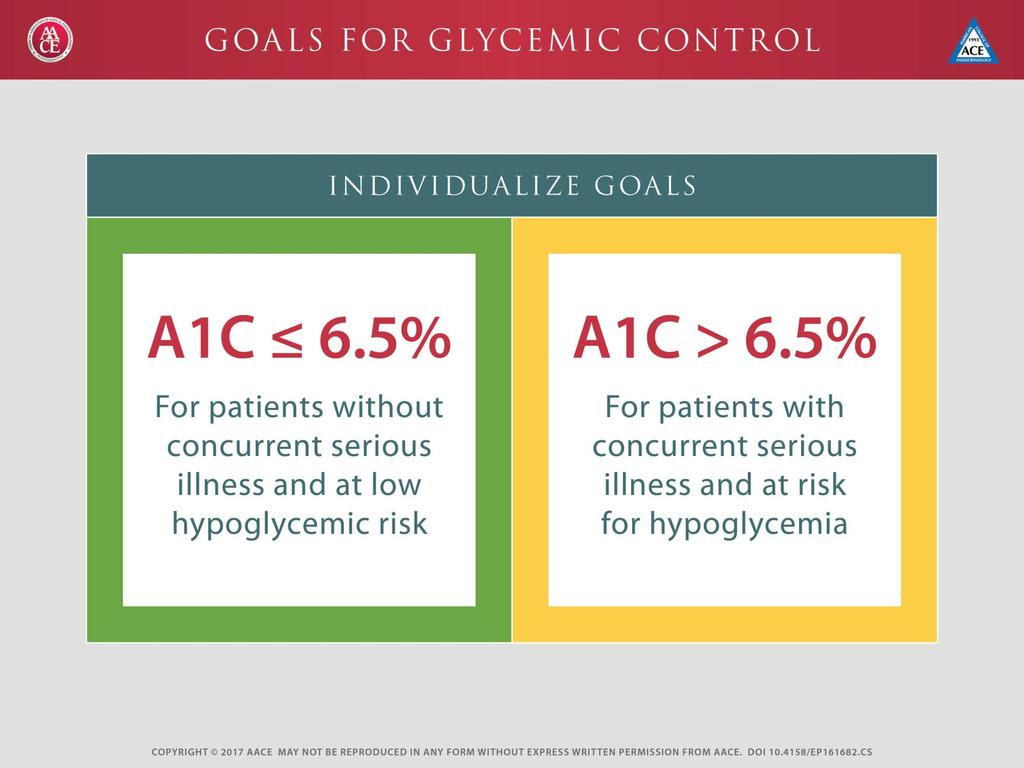
4 Glycemic Management of Type 2 Diabetes: Treatment Goals Lowering A1C Preventing Hypoglycemia Individualized Algorithm
:773-95.")
5 Main Pathophysiological Defects in T2DM Islet b-cell The Ominous Octet Impaired insulin secretion Decreased incretin effect Increased lipolysis Islet a-cell Increased glucagon secretion Increased glucose reabsorption Increased hepatic glucose production Defronzo RA. Diabetes Apr;58(4): Neurotransmitter dysfunction Decreased glucose uptake


6 Pathogenesis of Type 2 Diabetes Insulin Resistance: Receptor And Post-receptor Defects Increased Glucose Production Insufficient Glucose Disposal Glucose X Liver Peripheral Tissues (skeletal muscle) Pancreas Impaired Insulin Secretion DeFronzo et al. Diabetes Care. 1992;15:
7 Hepatic Insulin Resistance: Increased Hepatic Glucose Output DeFronzo RA. Diabetes 1988;37: FPG=Fasting Plasma Glucose

8 Current Antihyperglycemic Medications Glinides Sulfonylureas TZDs Insulin replacement therapy Restore postprandial insulin patterns Generalized insulin secretagogue Reduce peripheral insulin resistance Biguanide Reduces hepatic insulin resistance GLP-1 analogs Stimulate beta-cells Suppress glucagon 12 groups with different mechanisms of action SGLT-2 inhibitors Block renal glucose reabsorption DPP-4 inhibitors Restore GLP-1 Levels Amylin analog Suppresses glucagon a-glucosidase inhibitors Delay CHO absorption Colesevelam Bile acid sequestrant Bromocriptine Hypothalamic pituitary reset CHO = carbohydrate; DPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1; SGLT-2 = sodium-dependent glucose cotransporters-2; TZD = thiazolidinedione.
9

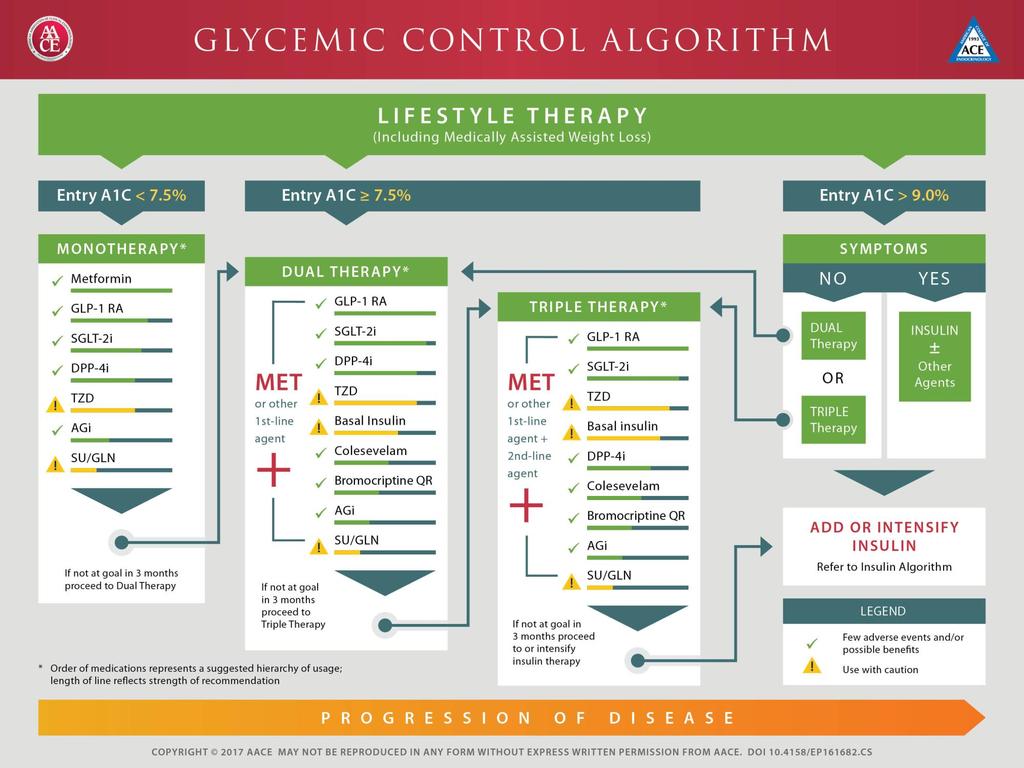
10 Algorithm to Achieve Glycemic Goals Baseline A1C 6.5% - 7.5% Monotherapy may be effective in this range Metformin first choice for monotherapy if no contraindications Consider DPP-4 if PP and FPG, GLP-1 if PP, TZD if metabolic syndrome or NAFLD, AGI if PP Do not recommend secretagogue (SU or glinide) in this range due to risk of hypoglycemia; short-lived effect If monotherapy is unsuccessful, move on to dual oral rx; often need to augment reduction in PP BG to get to goal in this A1C range DPP-4 = dipeptidyl peptidase-4; PP = post-prandial; FPG = fasting plasma glucose; GLP-1 = glucagon-like peptide-1; TZD = thiazolidinedione; NAFLD = non-alcoholic fatty liver disease; AGI = alpha-glucosidase inhibitor; SU = sulfonylurea; A1C = glycated hemoglobin; SGLT-2 = sodium glucose transport-2 AACE Comprehensive Diabetes Management Algorithm Endocr Pract. 2013;19(3):

11 Algorithm to Achieve Glycemic Goals Baseline A1C 7.6%-9.0% Dual therapy with metformin provides superior glycemic control over metformin alone. If dual oral rx is unsuccessful, consider triple therapy If triple oral rx fails to achieve A1C goal, initiate insulin GLP-1 RA = glucagon-like peptide-1 receptor agonist DPP4-I = dipeptidyl peptidase 4 inhibitor TZD = thiazolidinedione SGLT-2 = sodium glucose cotransporter 2 inhibitor QR = quick-release AG-I = alpha-glucosidase inhibitor SU = sulfonylurea GLN = glinide AACE Comprehensive Diabetes Management Algorithm Endocr Pract. 2013;19(3):

12 Algorithm to Achieve Glycemic Goals Baseline A1C >9.0% If patient is asymptomatic with recent onset of disease and drug naïve, may consider starting with dual or triple oral regimens If symptomatic, start insulin Once A1C has improved to <7.5%, consider initiation of dual oral therapy with tapering and possible discontinuation of insulin rx AACE Comprehensive Diabetes Management Algorithm Endocr Pract. 2013;19(3):









13 Targeted Sites of Action of Oral Anti-Hyperglycemic Drug Classes Liver Skeletal Muscle Pancreas Gut Fat Kidney Brain Biguanides TZDs DPP-IV inhibitors Sulfonylureas TZDs Insulin DPP-IV Inhibitors Sulfonylureas Glinides TZDs Amylin α-glucosidase inhibitors Biguanides Colesevelam GLP-1 RA TZDs SGLT-2 inhibitors Bromocriptine Glucose production Glucose uptake Insulin release Glucose absorption Insulin sensitivity Glucose reabsorption Glucose production DPP = dipeptidyl peptidase; SGLT-2 = Sodium-glucose co-transporter 2; TZD = thiazolidinediones Fonseca V. Clin Ther. 2014;36: Sonne DP. Eur J Endocrinol Inzucchi S, et al. Diabetes Care. 2012;35: ; Diabetologia. 2012;55:
14 Clinical Considerations Combining therapeutic agents with different modes of action may be advantageous In many if not most patients (unless contraindicated or intolerance has been demonstrated), use metformin, which increases insulin sensitivity, and/or insulin sensitizers such as TZDs, as part of the therapeutic regimen Dosage of secretagogues or insulin should be adjusted as blood glucose levels decline when used in combination with metformin, TZD, DPP-4 inhibitors, and/or incretin mimetics (GLP-1 agonists) TZD = thiazolidinediones; DPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1 AACE Comprehensive Diabetes Management Algorithm Endocr Pract. 2013;19(3): Sitagliptin [package insert]. Whitehouse Station, NJ; Merck Co. Inc.; Saxagliptin [package insert]. Princeton, NJ; Bristol Meyers Squibb; 2009; Linagliptin [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals
15 Clinical Considerations The weight gain associated with thiazolidinediones in some patients may be partly offset by combination therapy with metformin If A1C is elevated and preprandial blood glucose measurements are at target levels, carefully assess postprandial glucose levels Individualize treatment regimens! AACE Comprehensive Diabetes Management Algorithm Endocr Pract. 2013;19(3): ;
16 Effect of Glucose-lowering Drugs on Patient Weight Therapeutic Options Weight Sulfonylurea 1,2 TZD 3,4 Insulin 5,6 Metformin 7 DPP-4 inhibitor 8 GLP-1 receptor agonist 9 SGLT-2 Inhibitors 10 A1C = glycated hemoglobin; DPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1; SGLT-2 = sodium glucose co-transporter-2; TZD = thiazolidinedione 1. Malone M. Ann Pharmacother. 2005;39: Glipizide [package insert]. New York, NY; Pfizer; Pioglitazone [package insert]. Deerfield, IL: Takeda Pharmaceuticals America; Rosiglitazone [package insert]. Research Triangle Park, NC; GlaxoSmithKline; Nathan DM, et al. Diabetes Care. 2008;31(1): Holman RR. NEJM. 2007;357(17): Metformin[package insert]. Princeton NJ; Bristol Meyers Squibb; Sitagliptin [package insert]. Whitehouse Station, NJ; Merck and Co.; Drucker DJ, et al. J Clin Invest. 2007;117(1): Invokana [Package Insert] Janssen Pharmaceuticals, Inc. Titusville, NJ
17 Risk of Hypoglycemia Plays a significant role in choice of agents in AACE algorithm For patients at highest risk of hypoglycemia, may consider close evaluation of agents chosen as well as therapeutic goal Patients with type 2 diabetes at highest risk of low blood glucose include those with: Diabetes duration >15 years Advanced macrovascular disease Hypoglycemia unawareness Limited life expectancy Severe comorbidities AACE Comprehensive Diabetes Management Algorithm Endocr Pract. 2013;19(3): ; AACE Algorithm for Glycemic Control, Endocr Pract. 2009;15(6):
18 Biguanides Metformin Mechanism Insulin sensitivity Hepatic glucose production FPG more than PPG Efficacy A1C 1%-2% Advantages Disadvantages Contraindications No weight gain or hypoglycemia, potential weight loss GI side effects Lactic acidosis (rare) Renal disease; CHF Combinations available with SU, TZD, repaglinide, and DPP-4 inhibitors A1C = glycated hemoglobin; CHF = congestive heart failure; DPP-4 = dipeptidyl peptidase-4; FPG = fasting plasma glucose; GI = gastrointestinal; PPG = post-prandial glucose; SU = sulfonylurea; TZD = thiazolidinedione Metformin [package insert]. Princeton NJ; Bristol Myers Squibb; 2009.
19 Mechanism Sulfonylureas and Glinides Glipizide, Glimepiride, Glyburide Repaglinide, Nateglinide Insulin secretion FPG PPG Efficacy Advantages Moderate Strong short term efficacy Disadvantages Contraindications Weight gain, hypoglycemia, tend to lose efficacy after several years Avoid in severe hepatic and renal impairment Combinations available with metformin, TZD FPG = fasting plasma glucose; PPG = post-prandial glucose; TZD = thiazolidinedione Glyburide [package insert]. New York, NY; Pfizer; Glipizide [package insert]. New York, NY; Pfizer; Glimepiride [package insert]. Scoppito, Italy; Aventis Pharma S.p.A; Kahn SE, et al. NEJM. 2006;355:23.
20 Thiazolidinediones Pioglitazone, Rosiglitazone Mechanism Insulin sensitivity, especially at muscle, lowers both FPG and PPG, but effect may be delayed Efficacy Moderate ( A1C 1.0%-1.5%) Advantages No hypoglycemia, no reliance on renal excretion Disadvantages Contraindications Fluid retention, edema, heart failure, weight gain, slow onset of action, bone fractures, macular edema, osteoporosis, anemia, and bladder cancer Class III or IV CHF or hepatic impairment w/alt >2.5 times upper normal limits Combinations available with metformin and sulfonylurea A1C = glycated hemoglobin; ALT = alanine aminotransferase; CHF = congestive heart failure; FPG = fasting plasma glucose; PPG = postprandial plasma glucose. Pioglitazone [package insert]. Deerfield, IL: Takeda Pharmaceuticals America, Rosiglitazone Prescribing Information. Research Triangle Park, NC: GlaxoSmithKline, 2013.
21 Bays HE, et al. Arch Intern Med. 2008;168: Fonseca VA, et al. Diabetes Care. 2008; 31: Fonseca V, et al. Diabetes Obes Metab. 2010;12(5); Goldberg RB, et al. Arch Intern Med. 2008;168: ; Colesevelam [package insert]. Parsippany, NJ; Daiichi Sankyo, Mechanism Bile Acid Sequestrants Colesevelam Efficacy Modest ( A1C 0.5%) Advantages Disadvantages Raises cholecystokinin, which slows gastric emptying and post-prandial glucose Exact mechanism unknown, may be mediated via TGR5, and/or farnesoid X receptor (FXR/bile acid receptor) effects on intestinal glucose LDL-C (also FDA approved for LDL-C reduction) weight neutral, no hypoglycemia, can complement statin treatment in lowering LDL and cardiac event risk Constipation, nausea, dyspepsia, myalgia, pharyngitis, triglycerides, drug interactions Contraindications History of bowel obstruction, TGs >500 mg/dl; history of hypertriglyceridemiainduced pancreatitis A1C = glycated hemoglobin; LDL-C = low-density lipoprotein cholesterol; TG = triglyceride
 -0.")


22 Effects of Colesevelam on A1C Levels in Add-On Therapy Trials: 0.5% Reductions GLOWS Week 12 Metformin Week 26 Sulfonylurea Week 26 Insulin Week 16 Mean Change in A1C (%) * P n = >1, * -0.54* -0.54* -0.50* Zieve FJ et al. Clin Ther. 2007;29:74. Bays H et al. Presented at: AACE 16th Annual Meeting & Clinical Congress; April Abstract 204. Fonseca VA et al. Presented at: AACE 16th Annual Meeting & Clinical Congress; April Abstract 409. Goldberg RB et al. Presented at: AHA Scientific Sessions; November 2006; Chicago, IL. Poster
23 Strategies for Enhancing GLP-1 Action GLP-1 receptor agonists (injectable therapies) Short acting: exenatide BID, liraglutide, lixisenatide Long acting: exenatide QR, albiglutide, dulaglutide Under investigation: semaglutide and ITCA 650 DPP-4 inhibitors (oral therapies) Inhibit actions of DPP-4 Sitagliptin, saxagliptin, linagliptin, alogliptin

24 Summary of Incretin Actions on Different Target Tissues Drucker D. J. Cell Metabolism 2006
25 Inhibition of DPP-4 Increases Active Incretin Levels, Enhancing Downstream Incretin Actions Active GIP Active GLP-1 Increased insulin secretion Decreased glucagon release DPP-4 DPP-4 inhibitor Inactive GIP Inactive GLP-1 Glucose control improved Umpierrez et al. Endocrine Practice 2014
26 GLP1-RA Increase Active Incretin Levels Normal Physiology Active GLP-1 DPP-4 Inactive GLP-1 GLP-1 RA DPP-4 inhibitor Resistance Increased circulating GLP-1 levels Increased insulin secretion Decreased glucagon release Glucose control improved GLP-1 = glucagon-like peptide-1; GLP1-RA = glucagon-like peptide-1 receptor agonist; DPP-4 = dipeptidyl peptidase 4 Umpierrez et al. Endocrine Practice 2014
27 Characteristics of DPP-4 Inhibitors Alogliptin, Linagliptin, Saxagliptin, Sitagliptin Mechanism Inhibit enzymatic degradation of GLP-1 and GIP; glucose-dependent Efficacy Decrease A1C levels 0.6% 0.9% Dosing Side effects Main risk Once daily Headaches, nasopharyngitis Viral infection; long-term safety unknown A1C = glycated hemoglobin; GIP = gastric inhibitory polypeptide; GLP-1 = glucagon-like peptide-1 Rosenstock J, et al. Curr Opin Endocrinol Diabetes Obes. 2007;14: Nathan DM, et al. Diabetes Care. 2008;31:
28 Summary of DPP-4 Inhibitors Average A1C Change in Clinical Trials DPP-4 Inhibitor Monotherapy Initial with Metformi n Add-on to Metformin Add on to SU Add on to TZD Initial with TZD Alogliptin Linagliptin (SU + Met) Saxagliptin Sitagliptin Nesina (alogliptin) prescribing information. Deerfield, IL: Takeda Pharmaceuticals America, Inc.; 2013.
29 Summary of DPP-4 Inhibitors Alogliptin, Linagliptin, Saxagliptin, Sitagliptin Mechanism Inhibit enzymatic degradation of GLP-1 and GIP; glucose-dependent Efficacy Decrease A1C levels 0.6% 0.9% Dosing Side effects Main risk Once daily Headaches, nasopharyngitis Viral infection; long-term safety unknown A1C = glycated hemoglobin; GIP = gastric inhibitory polypeptide; GLP-1 = glucagon-like peptide-1 Rosenstock J, et al. Curr Opin Endocrinol Diabetes Obes. 2007;14: Nathan DM, et al. Diabetes Care. 2008;31:

30 1. Stenlöf K, et al. Diabetes Obes Metab. 2013;15: Ferrannini E, et al. Diabetes Care. 2010;33: Roden M, et al. Lancet Diabetes Endocrinol. 2013;1: Efficacy of SGLT2 Inhibitors as Monotherapy a CANA 1 PBO DAPA 2 PBO 5 10 EMPA 3 PBO a Phase 3 trials, BL A1C 7.8% to 8.1%, weeks. P<0.001 vs PBO for all

31 Weight Effects with SGLT2 Inhibitors a as Monotherapy Roden M et al. Lancet Diabetes Endocrinol. 2013;1: Stenlöf K et al. Diabetes Obes Metab. 2013;15: Ferrannini E et al. Diabetes Care. 2010;33: US FDA. Drugs@FDA.
32 Renal Glucose Transport in Type 2 Diabetes With increasing plasma glucose, filtered glucose increases in linear relationship When transport system becomes saturated, excess glucose is excreted in urine Renal threshold for glucose is 180 mg/dl in normal glucosetolerant individuals In patients with type 2 diabetes, transport maximum for glucose increases and glucosuria occurs at more elevated glucose levels Glucose reabsorption is enhanced, leading to worsening hyperglycemia Handelsman Y. Endocrine Pract, Bays, H. Diabetes Therapy, 2013; Goldstein DE et al. Diabetes Care, 2004.
33 Mechanism of action: SGLT2 Inhibitors Decrease re-absorption of glucose in the proximal convoluted tubule Decrease renal threshold so urinary glucose excretion occurs at lower plasma glucose concentration FDA-approved Canagliflozin Dapagliflozin Empagliflozin FDA = U.S. Food and Drug Administration; SGLT-2 = sodium-dependent glucose cotransporters-2. Bays, H. Diabetes Therapy, 2013.
34 SGLT 2 Inhibition: Meeting Unmet Needs in Diabetes Care Corrects a Novel Pathophysiologic Defect Reduces A1C Promotes Weight Loss Improves Glycemic Control and CVRFs Complements Action of Other Antidiabetic Agents Reduces Blood Pressure No Hypoglycemia Reversal of Glucotoxicity CVRF=Cardiovascular Risk Factor
35 Mechanism SGLT2 Inhibitors Canagliflozin, Dapagliflozin, Empagliflozin Inhibits sodium-glucose transport protein subtype 2 (SGLT2) which is responsible for at least 90% of glucose reabsorption in the kidney causing blood glucose is eliminated in the urine Efficacy Modest ( A1C %) Advantages Disadvantages Contraindications Insulin-independent glucose reduction, Low risk of hypoglycemia, Weight loss (to 4% BW), Blood pressure-lowering Osmotic diuresis causing Polyuria and lightheadedness, Bacterial urinary tract infections ( 5%), Fungal genital infections ( 10%), Increased LDL cholesterol, Hyperkalemia (canagliflozin), Bladder cancer concerns (dapagliflozin) History of genital fungal infections, caution in chronic kidney disease Invokana [Package Insert] Janssen Pharmaceuticals, Inc. Titusville, NJ.; Lavalle-gonzález FJ, Januszewicz A, Davidson J, et al. Diabetologia. 2013; Stenlöf K, Cefalu WT, Kim KA, et al. Diabetes Obes Metab. 2013;15(4):372-82; Burki TK. Lancet. 2012;379(9815):507.
36 SGLT2 Inhibitors Safety: Adverse Reactions The most frequent adverse effects of SGLT2 inhibitors (occurring in 5% patients) are female genital mycotic and urinary tract infections Patients may also experience increased urination, dehydration, or nasopharyngitis SGLT2 = sodium-glucose cotransporter-2 Empagliflozin/Jardiance PI 2016.; Dapagliflozin/Farxiga PI 2016.; Canagliflozin/Invokana PI 2016.
37 SGLT2 Inhibitors Safety: Warnings and Precautions SGLT2 inhibitor use may be associated with hypotension, ketoacidosis, impaired renal function, hypoglycemia, and increased LDL-C Patients should be closely monitored, particularly those with a history of, or at risk for, these conditions Dapagliflozin should not be used in patients with a history of bladder cancer Canagliflozin may be associated with hyperkalemia and bone fracture Bone fracture risk should be considered before use, and potassium levels should be monitored during use LDL-C = low-density lipoprotein cholesterol; SGLT2 = sodium-glucose cotransporter-2 Empagliflozin/Jardiance PI 2016.; Dapagliflozin/Farxiga PI 2016.; Canagliflozin/Invokana PI 2016.
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors. Bryce Fukunaga PharmD April 25, 2018
 Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Update on Oral Agents for T2DM and Obesity
 Update on Oral Agents for T2DM and Obesity This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved,
Update on Oral Agents for T2DM and Obesity This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved,
Treatment of Type 2 Diabetes: What Have We Learned? AACE Diabetes Algorithm. ADOPT Trial 6/13/2012
 Treatment of Type 2 Diabetes: What Have We Learned? Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering needed, patientspecific
Treatment of Type 2 Diabetes: What Have We Learned? Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering needed, patientspecific
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
SGLT2 Inhibitors
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: SGLT2 Inhibitors Page: 1 of 7 Last Review Date: June 22, 2018 SGLT2 Inhibitors Description Invokana
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: SGLT2 Inhibitors Page: 1 of 7 Last Review Date: June 22, 2018 SGLT2 Inhibitors Description Invokana
Update on Oral Agents for T2DM and Obesity
 AACE 2016 To AACE Update on Oral Agents for T2DM and Obesity This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C
AACE 2016 To AACE Update on Oral Agents for T2DM and Obesity This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
RPCC Pharmacy Forum. The Type 2 Diabetes Issue. Type 2 Diabetes: The Basics
 Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
SGLT2 Inhibitors
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: SGLT2 Inhibitors Page: 1 of 7 Last Review Date: November 30, 2018 SGLT2 Inhibitors Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: SGLT2 Inhibitors Page: 1 of 7 Last Review Date: November 30, 2018 SGLT2 Inhibitors Description
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Oral Medication for the Management of Diabetes Mechanism of. Duration of Daily Dosing Action
 Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA 2012 Virginia Mason Medical
 Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Peter Stein, MD Janssen Research and Development
 New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
SESSION 4 12:30pm 1:45pm
 SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Thiazolidinedione Step Therapy Program
 Thiazolidinedione Step Therapy Program Policy Number: 5.01.580 Last Review: 7/2018 Origination: 07/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide
Thiazolidinedione Step Therapy Program Policy Number: 5.01.580 Last Review: 7/2018 Origination: 07/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide
GLP-1. GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4.
 GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
AACE/ACE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM. Sherwin D Souza, MD, FACE
 AACE/ACE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM Sherwin D Soza, MD, FACE Prediabetes Treatment Algorithm T2DM = type 2 diabetes mellits BP = blood pressre CVD = cardiovasclar disease
AACE/ACE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM Sherwin D Soza, MD, FACE Prediabetes Treatment Algorithm T2DM = type 2 diabetes mellits BP = blood pressre CVD = cardiovasclar disease
OBJECTIVES 4/7/2014. Diabetes Update Overview of the Diabetes Epidemic in the United States. ISHP Annual Spring Meeting
 Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Ertugliflozin (Steglatro ) 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy
 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy") Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
STEP THERAPY CRITERIA
 CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
Drug Class Review Newer Diabetes Medications and Combinations
 Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
CANA DAPA EMPA. Change in Baseline Body Weight (kg) *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg, EMPA=10 or 25 mg.
 *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg, EMPA=10 or 25 mg.") CANA DAPA EMPA Change in Baseline Body Weight (kg) 2 1 0-1 -2-3 -4-5 PBO SGLT2 inhibitor (low dose)* SGLT2 inhibitor (high dose)* *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg,
CANA DAPA EMPA Change in Baseline Body Weight (kg) 2 1 0-1 -2-3 -4-5 PBO SGLT2 inhibitor (low dose)* SGLT2 inhibitor (high dose)* *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg,
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
9/12/2014. Main Pathophysiological Defect in T1DM. Main Pathophysiological Defects in T2DM. Personalizing Diabetes Care: The Alphabet Soup of Options
 9/12/2014 Baptist Health South Florida 13th Annual Primary Focus Symposium June 28, 2014 Silvio Inzucchi MD Section of Endocrinology Yale University School of Medicine Half-Century of HTN & T2DM Medications
9/12/2014 Baptist Health South Florida 13th Annual Primary Focus Symposium June 28, 2014 Silvio Inzucchi MD Section of Endocrinology Yale University School of Medicine Half-Century of HTN & T2DM Medications
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
GLYXAMBI (empagliflozin-linagliptin) oral tablet
 oral tablet") GLYXAMBI (empagliflozin-linagliptin) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
GLYXAMBI (empagliflozin-linagliptin) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
DIABETES UPDATE 2018
 DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
9/16/2013. Sherwin D Souza, M.D.
 Sherwin D Souza, M.D. Burden of disease in 2013 Type 2 DM Glucose Management Goals-understand the new guidelines by ADA/ AACE Drugs available for management of diabetes in 2013 (non insulin and insulin
Sherwin D Souza, M.D. Burden of disease in 2013 Type 2 DM Glucose Management Goals-understand the new guidelines by ADA/ AACE Drugs available for management of diabetes in 2013 (non insulin and insulin
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
3/22/2017. Type 2 Diabetes Pathophysiology and Pharmacology Review. Accreditation Statement
 Type 2 Diabetes Pathophysiology and Pharmacology Review Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA This
Type 2 Diabetes Pathophysiology and Pharmacology Review Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA This
Diabetes Medications: Oral Anti-Hyperglycemic Medications
 Diabetes Medications: Oral Anti-Hyperglycemic Medications Medication Types 1. Biguanides 2. Sulfonylureas 3. Thiazolidinediones (TZDs) 4. Alpha-Glucosidase Inhibitors 5. D-Phenylalanine Meglitinides 6.
Diabetes Medications: Oral Anti-Hyperglycemic Medications Medication Types 1. Biguanides 2. Sulfonylureas 3. Thiazolidinediones (TZDs) 4. Alpha-Glucosidase Inhibitors 5. D-Phenylalanine Meglitinides 6.
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Type 2 Diabetes Management: Case 1: Reducing Hypoglycemic Risk Case 2: Reducing Cardiovascular Risk
 Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
New Therapies for Diabetes
 Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Diabetes update - Diagnosis and Treatment
 Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
SGLT2 Inhibitors
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.19 Subject: SGLT2 Inhibitors Page: 1 of 6 Last Review Date: September 15, 2016 SGLT2 Inhibitors Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.19 Subject: SGLT2 Inhibitors Page: 1 of 6 Last Review Date: September 15, 2016 SGLT2 Inhibitors Description
3/8/2011. Julie M. Sease, Pharm D, BCPS, CDE Associate Professor of Pharmacy Practice Presbyterian College School of Pharmacy
 Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Diabetes Mellitus: Overview and Guidelines
 Diabetes Mellitus: Overview and Guidelines Rezvan Salehidoost, M.D., Endocrinologist Abidi Diabetes Master Class IMPORTANCE? Why is it interesting to do research in diabetes J. Olefsky, JAMA 2001:285:628-632
Diabetes Mellitus: Overview and Guidelines Rezvan Salehidoost, M.D., Endocrinologist Abidi Diabetes Master Class IMPORTANCE? Why is it interesting to do research in diabetes J. Olefsky, JAMA 2001:285:628-632
SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk
 Managing Diabetes & CVD: Expling New Evidence & Opptunities ESC Congress, London, UK 30 August, 2015 SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk Silvio E. Inzucchi MD Yale
Managing Diabetes & CVD: Expling New Evidence & Opptunities ESC Congress, London, UK 30 August, 2015 SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk Silvio E. Inzucchi MD Yale
Initiating the conversation
 Patient Case Study: Janice Janice - Medical History 6-year-old Hispanic woman comes to see you. She has not been to the doctor in almost 2 years. She reports feeling tired and has clearly gained weight
Patient Case Study: Janice Janice - Medical History 6-year-old Hispanic woman comes to see you. She has not been to the doctor in almost 2 years. She reports feeling tired and has clearly gained weight
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018
 Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Joshua Settle, PharmD Clinical Pharmacist Baptist Medical Center South ALSHP Fall Meeting September 30, 2016
 Joshua Settle, PharmD Clinical Pharmacist Baptist Medical Center South jjsettle@baptistfirst.org ALSHP Fall Meeting September 30, 2016 Objectives Describe the current information concerning newly approved
Joshua Settle, PharmD Clinical Pharmacist Baptist Medical Center South jjsettle@baptistfirst.org ALSHP Fall Meeting September 30, 2016 Objectives Describe the current information concerning newly approved
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Noninsulin Treatment of Diabetes: What the PCP Needs to Know
 Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Updates in Diabetes Care
 Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
FARXIGA (dapagliflozin) Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)
 Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)") Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL
 Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Newer and Expensive treatment of diabetes. Endocrinology Visiting Associate Professor Institute of Medicine TUTH
 Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Innovative, Unusual Therapies for DM-2: Insulin U-500, Bromocriptine, Colesevelam, and SGLT2 inhibitors. April 3 rd, 2014
 Innovative, Unusual Therapies for DM-2: Insulin U-500, Bromocriptine, Colesevelam, and SGLT2 inhibitors April 3 rd, 2014 KM Pantalone Associate Staff Endocrinology Speaker Bureau: Disclosures Bristol-Myers
Innovative, Unusual Therapies for DM-2: Insulin U-500, Bromocriptine, Colesevelam, and SGLT2 inhibitors April 3 rd, 2014 KM Pantalone Associate Staff Endocrinology Speaker Bureau: Disclosures Bristol-Myers
Julie White, MS Administrative Director Boston University School of Medicine Continuing Medical Education
 MENTOR QI Diabetes Performance Improvement Initiative, Getting Patients to Goal in Glycemic Control: Current Data Julie White, MS Administrative Director Boston University School of Medicine Continuing
MENTOR QI Diabetes Performance Improvement Initiative, Getting Patients to Goal in Glycemic Control: Current Data Julie White, MS Administrative Director Boston University School of Medicine Continuing
Exploring Non-Insulin Therapies in Type 1 Diabetes
 Exploring Non-Insulin Therapies in Type 1 Diabetes Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Disclosures Dr. Cornell: Advanced
Exploring Non-Insulin Therapies in Type 1 Diabetes Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Disclosures Dr. Cornell: Advanced
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.