Cardiovascular Disease Risk Factors and Blood Pressure Control in Ambulatory Care Visits to Physician Offices in the U.S.
|
|
|
- Moris Hudson
- 5 years ago
- Views:
Transcription
1 Cardiovascular Disease Risk Factors and Blood Pressure Control in Ambulatory Care Visits to Physician Offices in the U.S. Item Type Thesis Authors Couch, Christopher Rights Copyright is held by the author. Digital access to this material is made possible by the College of Medicine - Phoenix, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 24/08/ :01:30 Link to Item
2 Cardiovascular Disease Risk Factors and Blood Pressure Control in Ambulatory Care Visits to Physician Offices in the U.S. A Thesis submitted to The University of Arizona College of Medicine- Phoenix in partial fulfillment of the requirements for the Degree of Doctor of Medicine Christopher Couch 2011
3 Dedication The University of Arizona College of Medicine Phoenix and its inaugural class of Acknowledgements Doug Campos-Outcalt, MD, MPA. Howard Silverman, MD, MS. Suleman Hamid. Jeffrey Kriseman. Brett Overby. 2
4 Abstract Background: Cardiovascular disease is the leading cause of mortality in the U.S. Risk factors identified for coronary artery disease, cerebrovascular disease, and kidney disease include uncontrolled blood pressure, diabetes, renal disease, hyperlipidemia, obesity, and tobacco use. The threshold for pharmacologic treatment of hypertension in patients with diabetes or chronic kidney disease is 130/80 mmhg. It may be of benefit to extend these criteria to individuals who have other cardiovascular disease risk factors and no diagnosis of hypertension. Blood pressure recommendations in this population have largely been unstudied. This study investigates blood pressure control in this nonhypertensive population. Methods: We analyzed 2006 National Ambulatory Medical Care Survey (NAMCS) data to determine blood pressure control at physician office visits in the U.S. among patients with cardiovascular disease risk factors and no diagnosis of hypertension. Physician office visits with a documented diagnosis of hypertension were excluded from our study. Characteristics of the non-hypertensive population were indentified and were classified by blood pressure above or below 140/90 mmhg. Cardiovascular disease risk factors examined were diabetes, 3
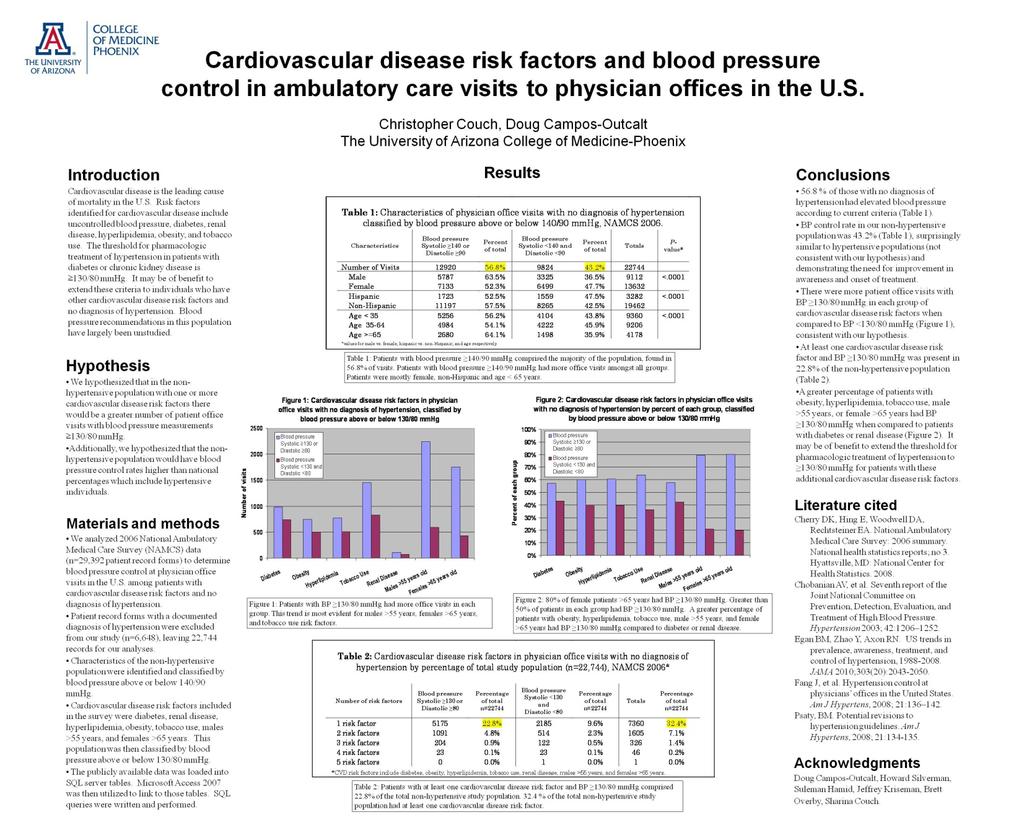
5 renal disease, hyperlipidemia, obesity, tobacco use, males >55 years, and females >65 years. This population was then divided into two groups, those with blood pressure above or below 130/80 mmhg. Results: We found 22,744 records (77.4% of visits) with no diagnosis of hypertension out of 29,392 total records, with 43.2% of the nonhypertensive population having BP <140/90 mmhg. Males fulfilled criteria for hypertension ( 140/90 mmhg) more frequently than females (63.5% vs. 52.3%, P-value <.001). Patients were mostly younger than 65 years. Males >55 years was the most prevalent CVD risk factor, with 79.2% of these with BP 130/80 mmhg. Second most prevalent risk factor was tobacco use at 10.1% of non-hypertensive visits, and BP was 130/80 mmhg in 63.6% of these visits. Hyperlipidemia in 5.6% of total visits, with BP 130/80 mmhg in 60.5%. Obesity was documented in 5.5% of non-hypertensive population, with BP 130/80 mmhg in 60.0%. Visits with one risk factor with BP 130/80 mmhg were found in 22.8% of our nonhypertensive study population. Conclusions: 56.8 % of those without a diagnosis of hypertension had elevated blood pressure recorded at their physician visit. BP control rate in our non-hypertensive population was 43.2%, surprisingly 4
6 similar to hypertensive populations and demonstrating the need for improvement in awareness and onset of treatment. There were more patient office visits with BP 130/80 mmhg in each group of cardiovascular disease risk factors when compared to BP <130/80 mmhg. At least one cardiovascular disease risk factor and BP 130/80 mmhg was present in 22.8% of the non-hypertensive population. A greater percentage of patients with obesity, hyperlipidemia, tobacco use, male >55 years, or female >65 years had BP 130/80 mmhg when compared to patients with diabetes or renal disease. It may be of benefit to extend the threshold for pharmacologic treatment of hypertension to 130/80 mmhg for patients with these additional cardiovascular disease risk factors. More studies are needed that evaluate blood pressure goals amongst non-hypertensive patients with multiple cardiovascular disease risk factors. 5
7 Table of Contents Abstract. 3 List of tables.7 Introduction..8 Research materials and methods...12 Results..15 Discussion Future directions Conclusions..26 References Tables Poster
8 List of tables 1. Table 1: Characteristics of physician office visits with no diagnosis of hypertension, NAMCS Table 2: Characteristics of physician office visits with no diagnosis of hypertension by percentage of total study population, NAMCS Table 3: Cardiovascular disease risk factors in physician office visits with no diagnosis of hypertension, NAMCS Table 4: Blood pressure control in physician office visits by number of cardiovascular disease risk factors, NAMCS Table 5: Cardiovascular disease risk factors in physician office visits with no diagnosis of hypertension by percentage of total study population, NAMCS
9 Introduction Background Cardiovascular disease is the leading cause of mortality in the United States (1). Hypertension is associated with an elevated risk for coronary artery disease, cerebrovascular disease, and kidney disease (2). Antihypertensive therapy and lifestyle modifications have been demonstrated to significantly decrease major cardiovascular events (3). Approximately one-third of the United States population has hypertension, which include both diagnosed and undiagnosed individuals (2). Approximately two-thirds of these individuals are untreated or not achieving optimal control (2). According to the Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7) hypertension is defined as a systolic blood pressure above 140 mmhg or a diastolic above 90 mmhg (2). If blood pressure does not fall into the recommended range after appropriate lifestyle modifications have been made, antihypertensive pharmacologic therapy is indicated in order to achieve optimal control. According to an analysis of a 2003 and 2004 national dataset, 44% of individuals with diagnosed hypertension are achieving recommended control (4). 8
10 The National Health and Nutrition Examination Survey (NHANES) reported hypertensive individuals controlled (<140/90 mmhg) in 34% of cases (5). A more recent NHANES analysis demonstrated hypertension control rates of 50%, meeting the goal recommended by Healthy People 2010 (6, 7). There is still much room for improvement. In addition to hypertension, there are a variety of risk factors for cardiovascular disease. According to JNC-7, some of the established risk factors include cigarette smoking, obesity (body mass index 30 kg/m 2 ), physical inactivity, dyslipidemia, diabetes mellitus, microalbuminuria or estimated GFR <60 ml/min, age >55 years for men or >65 years for women, and family history of premature cardiovascular disease (men <55 years or women <65 years) (2). Antihypertensive therapy is an essential tool utilized to prevent cardiovascular events, such as a myocardial infarction or stroke. The current recommendations suggest starting pharmacologic therapy in those patients with multiple blood pressure measurements above 140/90 mmhg (2). Multiple drug trials have demonstrated the benefit of hypertension control in patients with diabetes for preventing 9
11 cardiovascular disease and minimizing the progression of diabetic nephropathy (8, 9, 10). In addition, good blood pressure control in patients with chronic kidney disease protects against worsening renal function and cardiovascular disease (14). The recommended blood pressure goal, and standard of care, for patients with diabetes or chronic kidney disease is less than 130/80 mmhg (2, 11, 12, 13). Significance The current criteria, which simply utilizes a blood pressure cutoff for initiating antihypertensives, does not take into account a patient s cumulative risk for cardiovascular disease. In addition to an office blood pressure measurement, it has been suggested that a patient s cardiovascular risk be assessed to identify the need for pharmacologic therapy (14). Antihypertensive therapy could be indicated in patients that do not necessarily meet the current definition of hypertension. For example, individuals with one or more cardiovascular disease risk factors without documented hypertension and considered normotensive according to the current criteria may decrease their risk for a cardiovascular event with the initiation of antihypertensive therapy. Randomized controlled studies assessing blood pressure goals in this patient population are lacking (15). 10
12 As described above, patients with diabetes or chronic kidney disease are recommended to maintain blood pressure below 130/80 mmhg. It may be of benefit to extend the threshold for antihypertensive therapy of 130/80 mmhg to individuals who have the following cardiovascular disease risk factors: obesity, tobacco use, hyperlipidemia, males >55 years, and females >65 years. Aims/Goals/Hypothesis Using the 2006 National Ambulatory Medical Care Survey (NAMCS) data, published by the Centers of Disease Control and Prevention in 2008, we investigated blood pressure control at physician office visits in the non-hypertensive population (16, 17). We performed analyses of this dataset to evaluate blood pressure control rates with documented cardiovascular disease risk factors. The risk factors included in the NAMCS data are age, smoking status, obesity, diabetes, hyperlipidemia, and renal disease (16, 17). Risk factors not included in the dataset are family history of early cardiovascular disease and physical inactivity (16, 17). We hypothesized that in the non-hypertensive population with one or more cardiovascular disease risk factors there would be a greater number of patient office visits with blood pressure 11
13 measurements 130/80 mmhg. Additionally, we hypothesized that the non-hypertensive population would have blood pressure control rates higher than national percentages which include hypertensive individuals. Given the lack of research evaluating blood pressure control in this non-hypertensive patient population our cross-sectional study provides preliminary analyses. Research Materials and Methods The 2006 NAMCS data was published by the CDC in August 2008, and is available for the public to utilize for research purposes. This national survey has been conducted annually since 1989, completed by nonfederal, office-based physicians in the United States. The data represents a random sampling of patient visits to physicians over a one week period. Data includes patients' symptoms, physicians' diagnoses, and medications ordered or provided. It also includes demographic characteristics of patients, services provided, information on diagnostic procedures and patient management, as well as planned future treatment. All collected data has been de-identified, and no provider or patient information is included (16, 17). 12
14 The NAMCS data is accessible via the National Center for Health Statistics (NCHS) website, (16, 17, 18). Using the downloadable 2006 NAMCS dataset we studied the aforementioned cardiovascular disease risk factors in relation to blood pressure control as documented in the patient record form. The publicly available data was loaded into SQL server tables. Microsoft Access 2007 was then utilized to link to those tables. SQL queries were then written and performed according to the criteria as outlined here. Patient visits with a documented diagnosis of hypertension were excluded from our study. These visits were identified because the physician had checked hypertension under diagnosis for visit, or the diagnosis was coded as ICD-9-CM Cardiovascular disease risk factors including age, tobacco use, obesity, diabetes, hyperlipidemia, and renal disease were identified using the following methods. The survey includes date of birth to determine age. Tobacco use is identified if current tobacco use, was checked, the reason for the visit was smoking problems, or the diagnosis for the visit was coded as ICD-9-CM for tobacco use disorder. Obesity was defined using ICD-9-CM 278, or diagnosis for 13
15 visit obesity. (Height and weight was provided on survey for potential BMI calculation, although data completion for height value was found to be incomplete in the majority of data records.) Diabetes was defined using ICD-9-CM 250, reason for visit diabetes mellitus, or checking diabetes under diagnosis for visit. Hyperlipidemia was identified using ICD-9-CM or by checking hyperlipidemia under diagnosis for visit. Renal disease was defined using ICD-9-CM (chronic kidney disease, stage III), (chronic kidney disease, stage IV), (chronic kidney disease, stage V), (end stage renal disease), (chronic kidney disease, unspecified), or (renal failure, unspecified), reason for visit kidney dialysis, or by checking chronic renal failure under diagnosis for visit. Blood pressure measurements are included in the vital signs section of the survey, with both systolic and diastolic measurements. Using this dataset we looked at blood pressure control in physician office visits with no diagnosis of hypertension. We further characterized this group by sex, age, and ethnicity. Our second analysis included cardiovascular disease risk factors as described above in patients without a diagnosis of hypertension. This group was classified according to blood pressure measurements, 130/80 and 14
16 <130/80. In addition, we performed analyses for patients with one to five risk factors, covering all appropriate combinations. These were classified according to blood pressure measurements 130/80 or <130/80. Statistical analyses performed included the use of contingency tables and chi-square tests for the specified comparisons as outlined below. These include male versus female, Hispanic versus non- Hispanic, and age as described in the characteristics of our study population. Additionally, we performed comparisons of the number of cardiovascular disease risk factors present in our study population to include one versus two risk factors, one versus three risk factors, etc. as demonstrated below. Results As documented in the National Ambulatory Medical Care Survey, 2006 Summary, 29,392 patient record forms (PRFs) were completed (16). Hypertension related visits comprised 22.4% of visits (16). According to our criteria for hypertension as described above, we found 22,744 PRFs (table 1) without a diagnosis of hypertension, 77.4% of total visits for Despite the fact that hypertension was not 15
17 reported, 56.8% of our study population had blood pressure measurements 140 mmhg systolic or 90 mmhg diastolic, meeting the criteria for hypertension. We found 43.2% of patients with adequately controlled blood pressures measuring <140/90 mmhg. Amongst further classification of this population separated by sex, ethnicity and age we found more than half of visits in each sub-group to meet criteria for hypertension, (blood pressures 140 mmhg systolic or 90 mmhg diastolic )with a range from 52.3% (females) up to 64.1% (age 65).. Females comprised the majority of the population without a reported diagnosis of hypertension at 59.9% of patient visits (table 2). A higher proportion of males (63.5%) without a reported diagnosis of hypertension were found to meet the criteria for hypertension (according to documented blood pressure) than females, (52,3%)(table 1). The non-hispanic population comprised 85.6% of visits without a reported diagnosis of hypertension (table 2). Age distribution demonstrated patients without a reported diagnosis of hypertension were more likely to be younger than 65, comprising 41.2% of visits for <35 years, 40.5% of visits for 35 to 64 years and 18.4% of visits for 65 years. 16
18 Further classifying our non-hypertensive population by cardiovascular disease risk factors as previously described (table 3, table 4, and table 5) we found that males >55 years was the most prevalent risk factor, found in 12.5% of all non-hypertensive visits, with 79.2% of these having blood pressure 130/80 mmhg. The second most prevalent risk factor was tobacco use at 10.1% of nonhypertensive visits, with blood pressure 130/80 mmhg in 63.6% of these visits. Diabetes was present in 7.6% of all visits, and 57.0% of those with diabetes had blood pressure 130/80 mmhg. Obese individuals comprised 5.5% of the non-hypertensive population, with blood pressure 130/80 mmhg in 60.0% of this population. Reported hyperlipidemia was found in 5.6% of all visits, with blood pressure 130/80 mmhg in 60.5% of this population. Renal disease was the least prevalent risk factor in our non-hypertensive population at 0.8% of visits, with blood pressure 130/80 mmhg found in 57.7% of visits. The final cardiovascular disease risk factor that we examined was females >65 years which comprised 9.6% of all visits, and was found to be the largest group with blood pressure 130/80 mmhg at 80.2%. Patient visits with multiple cardiovascular disease risk factors were classified by blood pressure measurements (table 4 and table 5). 17
19 Visits with a minimum of one documented risk factor comprised 32.4% of non-hypertensive related visits, with blood pressure 130/80 mmhg found in 70.3% of this subset. Two risk factors were present in 7.1% of visits, and blood pressure 130/80 mmhg was found in 68.0% of this population. Three risk factors were found in 1.4% of visits, with blood pressure 130/80 mmhg found in 62.6% of visits. Four risk factors comprised only 0.2% of visits without a diagnosis of hypertension, and blood pressure 130/80 mmhg was found in 50.0% of this group. We only found one PRF out of 22,744 with five risk factors and no diagnosed hypertension. Discussion Our analysis demonstrates a substantial number of visits (56.8% with blood pressure 140 mmhg systolic or 90 mmhg diastolic) without a documented diagnosis of hypertension, who in fact meet the current criteria, as per JNC-7 (2). Reasons for this finding may be explained by the fact that these blood pressures may have been the first documented elevated measurement. As per JNC-7, hypertension is officially diagnosed with two or more accurate measurements 140/90 mmhg (2). NAMCS data captures only a single physician 18
20 office visit making it difficult to ascertain if the documented elevation had been found in previous visits. Other explanations may include the following: the physician decided not to address the elevated blood pressure at that particular visit, the elevated blood pressure was overlooked by the clinician, or a previous diagnosis of hypertension was mistakenly not included in the survey section 5b, provider s diagnosis for this visit. Given the fact that our population is comprised of unreported or undiagnosed hypertension, blood pressure control rates were found to be much worse than national estimates, which include patients with diagnosed hypertension. NHANES demonstrated 50.1% of hypertensive patients to have controlled blood pressure (<140/90 mmhg) (6). Surprisingly, our study, which was comprised of patient visits without a reported diagnosis of hypertension, found only 43.2% to have adequately controlled blood pressure. While this is similar to control rates for NHANES , which was 44.8%, we anticipated better control rates in our non-hypertensive population (6). Classification by sex demonstrates men to have more poorly controlled blood pressure than women (63.5% vs. 52.3% respectively, p- value <.001). This is consistent with prior studies that suggest men to 19
21 be less aware of hypertension, and therefore more often undiagnosed than women (6). Women are more likely to seek medical care than men (8). This may help to explain men s lack of awareness of hypertension. Another reason for the high percentage of males with uncontrolled blood pressure may be that the data represents a greater portion of initial visits by males to a physician office, with the first evidence of elevated blood pressure. Subsequent visits may confirm the elevated blood pressure and ultimately result in a diagnosis of hypertension and the onset of treatment. Our analysis of ethnicity demonstrates Hispanics to have marginally better blood pressure control rates than non-hispanics, at 47.5% and 42.5% respectively (p-value <.001). Our findings are not consistent with NHANES , which demonstrates Hispanics to be less aware of hypertension and more poorly controlled when compared to non-hispanics (6). As described in previous studies blood pressures tends to increase with age (2, 6). In the NHANES study patients older than 60 years of age were more aware of hypertension and more often treated, although this age group was less often controlled when compared to younger patients (6). Consistent with previous studies, 20
22 hypertension control rates for patients 65 years in our nonhypertensive population were amongst the worst, at 35.9% with blood pressures <140/90 mmhg. According to the current recommendations for blood pressure control for diabetes and chronic kidney disease of <130/80 mmhg, our analysis demonstrates a significant percentage of these patients without a diagnosis of hypertension to have uncontrolled blood pressure, 57.0% and 57.7% respectively. This leaves room for much improvement. Hypertension was not diagnosed at the time of these blood pressure readings. This may be due to the clinician overlooking a marginally elevated measurement in the majority of visits. In an analysis of NAMCS data by Fang and colleagues, blood pressure control rates for diabetics were 22.4% (4). As mentioned, our study found control rates for diabetics to be 43.0%, much better than this previous analysis; however, their analysis included diabetics with a diagnosis of hypertension. Our analysis excluded those with a diagnosis of hypertension which may explain the better control rates. Chronic kidney disease was not assessed in the study by Fang. Regardless of the comparison to prior studies, both groups in our 21
23 analysis demonstrate poor hypertension control rates as per current recommendations. Our hypothesis of finding a greater number of patient office visits with blood pressure 130/80 mmhg in the non-hypertensive population with one or more cardiovascular disease risk factors was verified (table 3). For visits with documented obesity, hyperlipidemia, or tobacco use, uncontrolled blood pressure as per our proposed criteria of 130/80 mmhg was found in greater than 60% of visits in each group. Females >65 years were the most uncontrolled at 80.2%, while males >55 years were uncontrolled in 79.2% of visits. Proposed revisions to hypertension guidelines as mentioned here may indicate the initiation of antihypertensive medications in a considerable number of patients. Our analysis looking at multiple cardiovascular disease risk factors demonstrates significant results. We found 22.8% of our nonhypertensive population to have at least one cardiovascular disease risk factor (diabetes, obesity, hyperlipidemia, tobacco use, renal disease, male >55 years, or female >65 years) with blood pressure 130 systolic or 80 diastolic. This represents 5,175 visits of which initiating antihypertensives would be indicated according to our 22
24 revised criteria. Those visits with at least two risk factors and blood pressure 130/80 comprised 4.8% of total visits. Three risk factors comprised 0.9% of visits, and four risk factors comprised 0.1%. This downward trend probably represents that hypertension is more likely to be diagnosed as a patient has an increasing number of cardiovascular disease risk factors. Limitations to our study include the lack of comparative analyses to the hypertensive population. Our study was intended to focus on physician office visits without a diagnosis of hypertension, and to assess blood pressure control rates. It would have been useful to have data from the hypertensive group for comparison purposes. The method by which the blood pressure measurement was obtained at each visit was not standardized or verified. Per JNC-7 the correct method for blood pressure measurement is to take the average of two blood pressures on one arm after the patient has been seated quietly for five minutes (2). It is unlikely that this was performed at each study site. NAMCS data is limited for a number of reasons. The data represents physician office visits, not complete patient analyses over time. The patient population represented here are those seeking 23
25 medical care, and thus do not represent the entire U.S. population. The data is not longitudinal in nature, making it difficult in our analyses to determine if the elevated blood pressures were the first documented evidence of hypertension. Per JNC-7 the diagnosis of hypertension requires the average of two or more properly measured, seated, BP readings on each of two or more office visits (2). It would be useful to determine if hypertension was in fact diagnosed at a subsequent visit, or if an elevated measurement had been documented previously. Other limitations to our study include that our analyses did not assess pharmacologic therapy and blood pressure control. It is unknown whether our study population includes those already on antihypertensive medications. We could have excluded these individuals from our study and further validated our results. Future Directions Given the lack of studies addressing blood pressure goals amongst non-hypertensive patients with multiple cardiovascular disease risk factors, our study demonstrates the need for additional analyses. Randomized controlled studies evaluating the use of 24
26 antihypertensives in this patient population with marginally elevated blood pressures ( 130/80 mmhg) would provide the most useful results. Our study demonstrates a large population that would meet these criteria. Patients that use tobacco, are obese, or have hyperlipidemia would most likely be affected by these studies, as they comprise the majority of this population. Additional studies that would prove useful may also include evaluations of the timing of diagnosis of hypertension at physician offices in the U.S. Our study demonstrates a significant lack of an official diagnosis of hypertension at a single visit despite meeting established criteria. A longitudinal analysis would prove extremely useful in assessing the timing of a hypertension diagnosis. This may be a better assessment of our study population and provide valuable data concerning the effectiveness of interventions. If new data were obtained we would redesign the survey to be more specific for our intended analyses. Blood pressure measurements would be standardized. The reporting of patient specific data would be more accurate to avoid unreported risk factors. For example, height and weight would be documented for every patient allowing an accurate BMI calculation and subsequent reporting of obesity. 25
27 Additionally, our data would be longitudinal in nature, thus allowing us to follow patients over time. Conclusions It has been demonstrated that the awareness, treatment, and control of hypertension in the U.S. has improved over the last decade (6, 19). It has been suggested that this may be explained by increased availability and tolerability of antihypertensives, increased use of electronic systems providing feedback reminders to both patients and clinicians, and the increasing use of nonphysician healthcare professionals in the management team (20). Despite the improved statistics, early diagnosis and treatment of hypertension are important for the prevention of cardiovascular events. While our study does not report blood pressure control rates meeting the Healthy People 2010 goal of 50%, the suggested explanations for improved awareness, treatment, and control may very well be reflected in future analyses of NAMCS data. If guidelines for antihypertensive therapy included both a cardiovascular disease risk analysis and a blood pressure measurement, many more individuals would meet criteria for 26
28 treatment. Our study demonstrates a significant number of physician office visits in the U.S. in 2006 that would meet these revised guidelines for antihypertensive therapy. This would significantly impact healthcare spending, increasing the number of individuals on antihypertensive therapy. This may be viewed as an early intervention to a probable future diagnosis of hypertension in this high risk population. Additionally, this could be a preventive measure for future cardiovascular events, thus decreasing their incidence over time. 27
29 References 1. Xu J, Kochanek KD, Murphy SL, Tejada-Vera B. Deaths: Final Data for Natl Vital Stat Rep. 2007; 58(19): Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jones DW, Materson BJ, Oparil S, Wright JT, Roccella EJ. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003; 42: Blood Pressure Lowering Treatment Trialists', Collaboration, Turnbull, F, Neal, B, et al. Effects of different regimens to lower blood pressure on major cardiovascular events in older and younger adults: meta-analysis of randomised trials. BMJ 2008; 336: Fang J, Alderman MH, Keenan NL, Ayala C, Croft JB. Hypertension control at physicians offices in the United States. Am J Hypertens, 2008; 21: Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, JAMA 2010;303(20): U.S. Department of Health and Human Services. Healthy People 2010 Midcourse Review. Washington, DC: U.S. Government Printing Office,
30 8. Hansson, L, Zanchetti, A, Carruthers, SG, et al. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. HOT Study Group. Lancet 1998; 351: Patel, A, ADVANCE Collaborative Group, MacMahon, S, et al. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet 2007; 370: Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ 1998; 317: Bakris GL, Williams M, Dworkin L, Elliott WJ, Epstein M, Toto R, Tuttle K, Douglas J, Hsueh W, Sowers J. Preserving renal function in adults with hypertension and diabetes: a consensus approach. National Kidney Foundation Hypertension and Diabetes Executive Committees Working Group. Am J Kidney Dis. 2000;36(3): Executive summary: Standards of medical care in diabetes Diabetes Care 2010; 33 Suppl 1:S Kidney Disease Outcomes Quality Initiative, (K/DOQI). K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. Am J Kidney Dis 2004; 43:S1. 29
31 14. Psaty, BM. Potential revisions to hypertension guidelines. Am J Hypertens, 2008; 21: Mancia, G, De Backer, G, Dominiczak, A, et al Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2007; 28: Cherry DK, Hing E, Woodwell DA, Rechtsteiner EA. National Ambulatory Medical Care Survey: 2006 summary. National health statistics reports; no 3. Hyattsville, MD: National Center for Health Statistics Centers for Disease Control and Prevention, National Center for Health Statistics. Public Use Data File Documentation: 2006 National Ambulatory Medical Care Survey. Hyattsville, MD: National Center for Health Statistics, Centers for Disease Control and Prevention. National Center for Health Statistics. Ambulatory Healthcare Data Hajjar I, Kotchen TA. Trends in prevalence, awareness, treatment, and control of hypertension in the United States, JAMA 2003;290: Chobanian AV. Improved hypertension control. JAMA 2010;303(20):
32 31 Table 1: Characteristics of physician office visits with no diagnosis of hypertension, NAMCS 2006 Characteristics Blood pressure Systolic 140 or Diastolic 90 Percent Blood pressure Systolic <140 and Diastolic <90 Percent Totals P- value* Number of Visits % % Male % % 9112 <.0001 Female % % Hispanic % % 3282 <.0001 Non-Hispanic % % Age < % % 9360 <.0001 Age % % 9206 Age >= % % 4178 *values for male vs. female, hispanic vs. non-hispanic, and age respectively
33 Male % % % Female % % % Hispanic % % % Non-Hispanic % % % Age < % % % Age % % % Age >= % % % 32 Table 2: Characteristics of physician office visits with no diagnosis of hypertension by percentage of total study population, NAMCS 2006 Characteristics Blood pressure Systolic 140 or Diastolic 90 Percent of total n=22744 Blood pressure Systolic <140 and Diastolic <90 Percent of total n=22744 Totals Percent of total n=22744
34 33 Table 3: Cardiovascular disease risk factors in physician office visits with no diagnosis of hypertension, NAMCS 2006 Risk factor Blood pressure Systolic 130 or Diastolic 80 Percent Blood pressure Systolic <130 and Diastolic <80 Percent Totals Diabetes % % 1720 Obesity % % 1249 Hyperlipidemia % % 1277 Tobacco Use % % 2289 Renal Disease % % 182 Males >55 years old % % 2836 Females >65 years old % % 2184
35 34 Table 4: Blood pressure control in physician office visits by number of cardiovascular disease risk factors*, NAMCS Number of risk factors Blood pressure Systolic 130 or Diastolic 80 Percent Blood pressure Systolic <130 and Diastolic <80 Percent Totals P- value** 1 risk factor % % 7360 < risk factors % % risk factors % % risk factors % % 46 5 risk factors 0 0.0% % 1 *cardiovascular disease risk factors include: diabetes, obesity, tobacco use, renal disease, males >55 and females >65 **value for one vs. two risk factors, and one vs. three risk factors, etc.
36 Table 5: Cardiovascular disease risk factors in physician office visits with no diagnosis of hypertension by percentage of total study population, NAMCS 2006 Number of risk factors 1 risk factor % % % 2 risk factors % % % 3 risk factors % % % 4 risk factors % % % 5 risk factors 0 0.0% 1 0.0% 1 0.0% 35 Risk factor Blood pressure Systolic 130 or Diastolic 80 Percentage of total n=22744 Blood pressure Systolic <130 and Diastolic <80 Percentage of total n=22744 Totals Percentage of total n=22744 Diabetes % % % Obesity % % % Hyperlipidemia % % % Tobacco Use % % % Renal Disease % % % Males >55 years old % % % Females >65 years old % % %
37 36
Analytical Methods: the Kidney Early Evaluation Program (KEEP) The Kidney Early Evaluation program (KEEP) is a free, community based health
 The Kidney Early Evaluation program (KEEP) is a free, community based health") Analytical Methods: the Kidney Early Evaluation Program (KEEP) 2000 2006 Database Design and Study Participants The Kidney Early Evaluation program (KEEP) is a free, community based health screening program
Analytical Methods: the Kidney Early Evaluation Program (KEEP) 2000 2006 Database Design and Study Participants The Kidney Early Evaluation program (KEEP) is a free, community based health screening program
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Target Blood Pressure Attainment in Diabetic Hypertensive Patients: Need for more Diuretics? Waleed M. Sweileh, PhD
 Target Blood Pressure Attainment in Diabetic Hypertensive Patients: Need for more Diuretics? Waleed M. Sweileh, PhD Associate Professor, Clinical Pharmacology Corresponding author Waleed M. Sweileh, PhD
Target Blood Pressure Attainment in Diabetic Hypertensive Patients: Need for more Diuretics? Waleed M. Sweileh, PhD Associate Professor, Clinical Pharmacology Corresponding author Waleed M. Sweileh, PhD
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
 Touyz, R. M., and Dominiczak, A. F. (2016) Hypertension guidelines: is it time to reappraise blood pressure thresholds and targets? Hypertension, 67(4), pp. 688-689. There may be differences between this
Touyz, R. M., and Dominiczak, A. F. (2016) Hypertension guidelines: is it time to reappraise blood pressure thresholds and targets? Hypertension, 67(4), pp. 688-689. There may be differences between this
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Blood Pressure Assessment Practices of Dental Hygienists
 Blood Pressure Assessment Practices of Dental Hygienists Abstract An estimated 50 million Americans have high blood pressure (HBP), with 30% of them unaware of their condition. Both the American Dental
Blood Pressure Assessment Practices of Dental Hygienists Abstract An estimated 50 million Americans have high blood pressure (HBP), with 30% of them unaware of their condition. Both the American Dental
ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ
 ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ USADA can grant a Therapeutic Use Exemption (TUE) in compliance with the World Anti- Doping Agency International Standard for TUEs. The TUE application process
ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ USADA can grant a Therapeutic Use Exemption (TUE) in compliance with the World Anti- Doping Agency International Standard for TUEs. The TUE application process
Cardiovascular disease (CVD), including stroke, is the
, including stroke, is the") Review: Clinical Cardiology: New Frontiers Hypertensive Therapy: Part I Veronica Franco, MD; Suzanne Oparil, MD; Oscar A. Carretero, MD Cardiovascular disease (CVD), including stroke, is the most common
Review: Clinical Cardiology: New Frontiers Hypertensive Therapy: Part I Veronica Franco, MD; Suzanne Oparil, MD; Oscar A. Carretero, MD Cardiovascular disease (CVD), including stroke, is the most common
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Prevalence of Pre Hypertension Among the Women Aged Years in Coastal and Non Coastal Areas
 2016 IJSRST Volume 2 Issue 5 Print ISSN: 2395-6011 Online ISSN: 2395-602X Themed Section: Science and Technology Prevalence of Pre Hypertension Among the Women Aged 20-60 Years in Coastal and Non Coastal
2016 IJSRST Volume 2 Issue 5 Print ISSN: 2395-6011 Online ISSN: 2395-602X Themed Section: Science and Technology Prevalence of Pre Hypertension Among the Women Aged 20-60 Years in Coastal and Non Coastal
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
In the Literature 1001 BP of 1.1 mm Hg). The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi
. The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi") Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
The Hypertension Clinic is a part of the Internal Medicine
 Original Article Hypertension Registry at the Bangkok Hospital Medical Center: The First 7 Months Experience OBJECTIVE: The Hypertension Registry at the Bangkok Hospital Medical Center was established
Original Article Hypertension Registry at the Bangkok Hospital Medical Center: The First 7 Months Experience OBJECTIVE: The Hypertension Registry at the Bangkok Hospital Medical Center was established
The target blood pressure in patients with diabetes is <130 mm Hg
 Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
ORIGINAL INVESTIGATION. Effects of Prehypertension on Admissions and Deaths
 ORIGINAL INVESTIGATION Effects of Prehypertension on Admissions and Deaths A Simulation Louise B. Russell, PhD; Elmira Valiyeva, PhD; Jeffrey L. Carson, MD Background: The Joint National Committee on Prevention,
ORIGINAL INVESTIGATION Effects of Prehypertension on Admissions and Deaths A Simulation Louise B. Russell, PhD; Elmira Valiyeva, PhD; Jeffrey L. Carson, MD Background: The Joint National Committee on Prevention,
Hypertension is a major risk factor for
 OPTIMAL RISK MANAGEMENT OF THE HYPERTENSIVE PATIENT WITH MULTIPLE RISK FACTORS * Keith C. Ferdinand, MD, FACC ABSTRACT To determine the risk of cardiovascular disease in patients with hypertension, it
OPTIMAL RISK MANAGEMENT OF THE HYPERTENSIVE PATIENT WITH MULTIPLE RISK FACTORS * Keith C. Ferdinand, MD, FACC ABSTRACT To determine the risk of cardiovascular disease in patients with hypertension, it
The problem of uncontrolled hypertension
 (2002) 16, S3 S8 2002 Nature Publishing Group All rights reserved 0950-9240/02 $25.00 www.nature.com/jhh The problem of uncontrolled hypertension Department of Public Health and Clinical Medicine, Norrlands
(2002) 16, S3 S8 2002 Nature Publishing Group All rights reserved 0950-9240/02 $25.00 www.nature.com/jhh The problem of uncontrolled hypertension Department of Public Health and Clinical Medicine, Norrlands
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Declaration of conflict of interest
 Declaration of conflict of interest Prevalence and main features of resistant hypertension in Central and Eastern Europe: data from the G. Brambilla 1, G. Seravalle 2, R. Cifkova 3, C. Farsang 4, S. Laurent
Declaration of conflict of interest Prevalence and main features of resistant hypertension in Central and Eastern Europe: data from the G. Brambilla 1, G. Seravalle 2, R. Cifkova 3, C. Farsang 4, S. Laurent
EXAMINING THE EDUCATION GRADIENT IN CHRONIC ILLNESS
 EXAMINING THE EDUCATION GRADIENT IN CHRONIC ILLNESS PINKA CHATTERJI, HEESOO JOO, AND KAJAL LAHIRI Department of Economics, University at Albany: SUNY February 6, 2012 This research was supported by the
EXAMINING THE EDUCATION GRADIENT IN CHRONIC ILLNESS PINKA CHATTERJI, HEESOO JOO, AND KAJAL LAHIRI Department of Economics, University at Albany: SUNY February 6, 2012 This research was supported by the
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
NIH Public Access Author Manuscript JAMA Intern Med. Author manuscript; available in PMC 2015 August 01.
 NIH Public Access Author Manuscript Published in final edited form as: JAMA Intern Med. 2014 August ; 174(8): 1397 1400. doi:10.1001/jamainternmed.2014.2492. Prevalence and Characteristics of Systolic
NIH Public Access Author Manuscript Published in final edited form as: JAMA Intern Med. 2014 August ; 174(8): 1397 1400. doi:10.1001/jamainternmed.2014.2492. Prevalence and Characteristics of Systolic
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Chapter 1: CKD in the General Population
 Chapter 1: CKD in the General Population Overall prevalence of CKD (Stages 1-5) in the U.S. adult general population was 14.8% in 2011-2014. CKD Stage 3 is the most prevalent (NHANES: Figure 1.2 and Table
Chapter 1: CKD in the General Population Overall prevalence of CKD (Stages 1-5) in the U.S. adult general population was 14.8% in 2011-2014. CKD Stage 3 is the most prevalent (NHANES: Figure 1.2 and Table
Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico
 Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico G. Mazzanti UO Cardiologia Ospedale SS. Annunziata, Cento (FE) AUSL di Ferrara Antiplatelet therapy Aspirin Aspirin:
Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico G. Mazzanti UO Cardiologia Ospedale SS. Annunziata, Cento (FE) AUSL di Ferrara Antiplatelet therapy Aspirin Aspirin:
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Quality ID #122: Adult Kidney Disease: Blood Pressure Management National Quality Strategy Domain: Effective Clinical Care
 Quality ID #122: Adult Kidney Disease: Blood Pressure Management National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Intermediate
Quality ID #122: Adult Kidney Disease: Blood Pressure Management National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Intermediate
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Hypertension is an important global public
 IN THE LITERATURE Blood Pressure Target in Individuals Without Diabetes: What Is the Evidence? Commentary on Verdecchia P, Staessen JA, Angeli F, et al; on behalf of the Cardio-Sis Investigators. Usual
IN THE LITERATURE Blood Pressure Target in Individuals Without Diabetes: What Is the Evidence? Commentary on Verdecchia P, Staessen JA, Angeli F, et al; on behalf of the Cardio-Sis Investigators. Usual
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Know Your Number Aggregate Report Single Analysis Compared to National Averages
 Know Your Number Aggregate Report Single Analysis Compared to National s Client: Study Population: 2242 Population: 3,000 Date Range: 04/20/07-08/08/07 Version of Report: V6.2 Page 2 Study Population Demographics
Know Your Number Aggregate Report Single Analysis Compared to National s Client: Study Population: 2242 Population: 3,000 Date Range: 04/20/07-08/08/07 Version of Report: V6.2 Page 2 Study Population Demographics
Prevalence of Comorbidities and Their Influence on Blood Pressure Goal Attainment in Geriatric Patients
 Original Paper Prevalence of Comorbidities and Their Influence on Blood Pressure Goal Attainment in Geriatric Patients CME Credit 1 www.lejacq.com/cme John D. Bisognano, MD, PhD; 1 Kevin A. Townsend, MS,
Original Paper Prevalence of Comorbidities and Their Influence on Blood Pressure Goal Attainment in Geriatric Patients CME Credit 1 www.lejacq.com/cme John D. Bisognano, MD, PhD; 1 Kevin A. Townsend, MS,
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
EFFICACY & SAFETY OF ORAL TRIPLE DRUG COMBINATION OF TELMISARTAN, AMLODIPINE AND HYDROCHLOROTHIAZIDE IN THE MANAGEMENT OF NON-DIABETIC HYPERTENSION
 EFFICACY & SAFETY OF ORAL TRIPLE DRUG COMBINATION OF TELMISARTAN, AMLODIPINE AND HYDROCHLOROTHIAZIDE IN THE MANAGEMENT OF NON-DIABETIC HYPERTENSION Khemchandani D. 1 and * Arif A. Faruqui 2 1 Bairagarh,
EFFICACY & SAFETY OF ORAL TRIPLE DRUG COMBINATION OF TELMISARTAN, AMLODIPINE AND HYDROCHLOROTHIAZIDE IN THE MANAGEMENT OF NON-DIABETIC HYPERTENSION Khemchandani D. 1 and * Arif A. Faruqui 2 1 Bairagarh,
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
HYPERTENSION IS A MAJOR RISK
 ORIGINAL CONTRIBUTION Trends in Prevalence, Awareness, Treatment, and Control of Hypertension in the United States, 1988-2000 Ihab Hajjar, MD, MS Theodore A. Kotchen, MD Context Prior analyses of National
ORIGINAL CONTRIBUTION Trends in Prevalence, Awareness, Treatment, and Control of Hypertension in the United States, 1988-2000 Ihab Hajjar, MD, MS Theodore A. Kotchen, MD Context Prior analyses of National
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Chapter 2: Identification and Care of Patients With Chronic Kidney Disease
 Chapter 2: Identification and Care of Patients With Chronic Kidney Disease Introduction The examination of care in patients with chronic kidney disease (CKD) is a significant challenge, as most large datasets
Chapter 2: Identification and Care of Patients With Chronic Kidney Disease Introduction The examination of care in patients with chronic kidney disease (CKD) is a significant challenge, as most large datasets
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Type 2 diabetes mellitus with hypertension at primary healthcare level in Malaysia: are they managed according to guidelines?
 O r i g i n a l A r t i c l e Singapore Med J 2005; 46(3) : 127 Type 2 diabetes mellitus with hypertension at primary healthcare level in Malaysia: are they managed according to guidelines? G C Chan ABSTRACT
O r i g i n a l A r t i c l e Singapore Med J 2005; 46(3) : 127 Type 2 diabetes mellitus with hypertension at primary healthcare level in Malaysia: are they managed according to guidelines? G C Chan ABSTRACT
Diabetes: Staying Two Steps Ahead. The prevalence of diabetes is increasing. What causes Type 2 diabetes?
 Focus on CME at the University of University Manitoba of Manitoba : Staying Two Steps Ahead By Shagufta Khan, MD; and Liam J. Murphy, MD The prevalence of diabetes is increasing worldwide and will double
Focus on CME at the University of University Manitoba of Manitoba : Staying Two Steps Ahead By Shagufta Khan, MD; and Liam J. Murphy, MD The prevalence of diabetes is increasing worldwide and will double
As a major risk factor for cardiovascular (CV)
") R e v i e w P a p e r Assessment of Global Risk: A Foundation for a New, Better Definition of Hypertension Thomas D. Giles, MD The prevalence of individuals with increased blood pressure (BP) is growing.
R e v i e w P a p e r Assessment of Global Risk: A Foundation for a New, Better Definition of Hypertension Thomas D. Giles, MD The prevalence of individuals with increased blood pressure (BP) is growing.
Endorama. 5/7/15 Luke J. Laffin MD
 Endorama 5/7/15 Luke J. Laffin MD 58 year-old male with history of DM2, HTN, and CKD Presented to us in clinic in 7/2014 HTN since his 30s, DM2 and CKD for >10 years Multiple anti-hypertensives tried in
Endorama 5/7/15 Luke J. Laffin MD 58 year-old male with history of DM2, HTN, and CKD Presented to us in clinic in 7/2014 HTN since his 30s, DM2 and CKD for >10 years Multiple anti-hypertensives tried in
The Road to Renin System Optimization: Renin Inhibitor
 The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
The prevalence of hypertension in a representative
 CLINICAL STRATEGIES FOR OPTIMAL HYPERTENSION MANAGEMENT Roger S. Blumenthal, MD * ABSTRACT In the United States, approximately 25% of the adult population older than 40 years has hypertension. Americans
CLINICAL STRATEGIES FOR OPTIMAL HYPERTENSION MANAGEMENT Roger S. Blumenthal, MD * ABSTRACT In the United States, approximately 25% of the adult population older than 40 years has hypertension. Americans
When should blood pressure be lowered? Should treatment be guided by blood pressure values or total cardiovascular risk?
 OF JOURNAL HYPERTENSION JH R RESEARCH Journal of HYPERTENSION RESEARCH www.hypertens.org/jhr Editorial J Hypertens Res (2016) 2(2):47 51 When should blood pressure be lowered? Should treatment be guided
OF JOURNAL HYPERTENSION JH R RESEARCH Journal of HYPERTENSION RESEARCH www.hypertens.org/jhr Editorial J Hypertens Res (2016) 2(2):47 51 When should blood pressure be lowered? Should treatment be guided
Controlling Hypertension in Primary Care: Hitting a moving target?
 Controlling Hypertension in Primary Care: Hitting a moving target? David J. Hyman, MD,MPH Professor of Medicine and Family & Community Medicine Chief, Section General Medicine Baylor College of Medicine
Controlling Hypertension in Primary Care: Hitting a moving target? David J. Hyman, MD,MPH Professor of Medicine and Family & Community Medicine Chief, Section General Medicine Baylor College of Medicine
Prevalence, awareness of hypertension in rural areas of Kurnool
 Original article: Prevalence, awareness of hypertension in rural areas of Kurnool Dr. Sudhakar Babu*, Dr.Aruna MS** *Associate Professor, Dept of Community Medicine, Vishwa Bharathi Medical College Kurnool,
Original article: Prevalence, awareness of hypertension in rural areas of Kurnool Dr. Sudhakar Babu*, Dr.Aruna MS** *Associate Professor, Dept of Community Medicine, Vishwa Bharathi Medical College Kurnool,
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
S150 KEEP Analytical Methods. American Journal of Kidney Diseases, Vol 55, No 3, Suppl 2, 2010:pp S150-S153
 S150 KEEP 2009 Analytical Methods American Journal of Kidney Diseases, Vol 55, No 3, Suppl 2, 2010:pp S150-S153 S151 The Kidney Early Evaluation program (KEEP) is a free, communitybased health screening
S150 KEEP 2009 Analytical Methods American Journal of Kidney Diseases, Vol 55, No 3, Suppl 2, 2010:pp S150-S153 S151 The Kidney Early Evaluation program (KEEP) is a free, communitybased health screening
Trends in Prevalence, Awareness, Management, and Control of Hypertension Among United States Adults, 1999 to 2010
 Journal of the American College of Cardiology Vol. 60, No. 7, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2012.04.026
Journal of the American College of Cardiology Vol. 60, No. 7, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2012.04.026
Pharmacy Student Self-Perception of Weight and Relationship to Counseling Patients on Lifestyle Modification
 RESEARCH American Journal of Pharmaceutical Education 2014; 78 (2) Article 35. Pharmacy Student Self-Perception of Weight and Relationship to Counseling Patients on Lifestyle Modification Allen Antworth,
RESEARCH American Journal of Pharmaceutical Education 2014; 78 (2) Article 35. Pharmacy Student Self-Perception of Weight and Relationship to Counseling Patients on Lifestyle Modification Allen Antworth,
Chapter 4: Cardiovascular Disease in Patients with CKD
 Chapter 4: Cardiovascular Disease in Patients with CKD The prevalence of cardiovascular disease (CVD) was 65.8% among patients aged 66 and older who had chronic kidney disease (CKD), compared to 31.9%
Chapter 4: Cardiovascular Disease in Patients with CKD The prevalence of cardiovascular disease (CVD) was 65.8% among patients aged 66 and older who had chronic kidney disease (CKD), compared to 31.9%
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
USRDS UNITED STATES RENAL DATA SYSTEM
 USRDS UNITED STATES RENAL DATA SYSTEM Chapter 2: Identification and Care of Patients With CKD Over half of patients from the Medicare 5 percent sample have either a diagnosis of chronic kidney disease
USRDS UNITED STATES RENAL DATA SYSTEM Chapter 2: Identification and Care of Patients With CKD Over half of patients from the Medicare 5 percent sample have either a diagnosis of chronic kidney disease
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
2014 HYPERTENSION GUIDELINES
 2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
None. Disclosure: Relationships with Industry Conflicts of Interests. Learning Objectives: Participants will be able to:
 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions
 Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
ADHD and Adverse Health Outcomes in Adults
 Thomas J. Spencer, MD This work was supported in part by a research grant from Shire (Dr. Spencer) and by the Pediatric Psychopharmacology Council Fund. Disclosures Dr. Spencer receives research support
Thomas J. Spencer, MD This work was supported in part by a research grant from Shire (Dr. Spencer) and by the Pediatric Psychopharmacology Council Fund. Disclosures Dr. Spencer receives research support
KEEP 2009 Summary Figures
 S4 29 Summary Figures American Journal of Kidney Diseases, Vol 55, No 3, Suppl 2, 21:pp S4-S57 S41 Definitions DATA ANALYSES DIABETES Self-reported diabetes, self reported diabetic retinopathy, receiving
S4 29 Summary Figures American Journal of Kidney Diseases, Vol 55, No 3, Suppl 2, 21:pp S4-S57 S41 Definitions DATA ANALYSES DIABETES Self-reported diabetes, self reported diabetic retinopathy, receiving
 Choice of therapy in esse... http://www.uptodate.co... Page 1 of 28 Official reprint from UpToDate www.uptodate.com Print Back Choice of therapy in essential hypertension: Recommendations Authors Norman
Choice of therapy in esse... http://www.uptodate.co... Page 1 of 28 Official reprint from UpToDate www.uptodate.com Print Back Choice of therapy in essential hypertension: Recommendations Authors Norman
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
Chapman University Digital Commons. Chapman University. Michael S. Kelly Chapman University,
 Chapman University Chapman University Digital Commons Pharmacy Faculty Articles and Research School of Pharmacy 12-30-2016 Assessment of Achieved Systolic Blood Pressure in Newly Treated Hypertensive Patients
Chapman University Chapman University Digital Commons Pharmacy Faculty Articles and Research School of Pharmacy 12-30-2016 Assessment of Achieved Systolic Blood Pressure in Newly Treated Hypertensive Patients
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Cardiovascular Disease in Tennessee. Audrey M Bauer, DVM, MPH Surveillance, Epidemiology and Evaluation Tennessee Department of Health
 Cardiovascular Disease in Tennessee Audrey M Bauer, DVM, MPH Surveillance, Epidemiology and Evaluation Tennessee Department of Health Practical Strategies in Medication Adherence for Cardiac and Stroke
Cardiovascular Disease in Tennessee Audrey M Bauer, DVM, MPH Surveillance, Epidemiology and Evaluation Tennessee Department of Health Practical Strategies in Medication Adherence for Cardiac and Stroke
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Guideline scope Hypertension in adults (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Hypertension in adults (update) This guideline will update the NICE guideline on hypertension in adults (CG127). The guideline will be
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Hypertension in adults (update) This guideline will update the NICE guideline on hypertension in adults (CG127). The guideline will be
Department of Family Medicine, Kulliyyah of Medicine, International Islamic University Malaysia, Kuantan, Pahang b
 Prevalence of Hypertension and Glycaemic Control in Adult Type-2 Diabetes Patients: A Preliminary Retrospective Cohort Study in Kuantan, Pahang, Malaysia Fa iza Abdullah a, Tin Myo Han b, Mohd Basri Mat
Prevalence of Hypertension and Glycaemic Control in Adult Type-2 Diabetes Patients: A Preliminary Retrospective Cohort Study in Kuantan, Pahang, Malaysia Fa iza Abdullah a, Tin Myo Han b, Mohd Basri Mat
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
A n aly tical m e t h o d s
 a A n aly tical m e t h o d s If I didn t go to the screening at Farmers Market I would not have known about my kidney problems. I am grateful to the whole staff. They were very professional. Thank you.
a A n aly tical m e t h o d s If I didn t go to the screening at Farmers Market I would not have known about my kidney problems. I am grateful to the whole staff. They were very professional. Thank you.
Clinical Issues Research Implemented April 2010
 Hypertension General Management Principals (from the JNC7) In persons older than 50 years, systolic blood pressure greater than 140 mmhg is a much more important cardiovascular disease (CVD) risk factor
Hypertension General Management Principals (from the JNC7) In persons older than 50 years, systolic blood pressure greater than 140 mmhg is a much more important cardiovascular disease (CVD) risk factor
DECLARATION OF CONFLICT OF INTEREST. None to declare
 DECLARATION OF CONFLICT OF INTEREST None to declare Sympathetic nerve traffic, insulin resistance and baroreflex control of circulation in patients with resistant hypertension Gino Seravalle Marco Volpe
DECLARATION OF CONFLICT OF INTEREST None to declare Sympathetic nerve traffic, insulin resistance and baroreflex control of circulation in patients with resistant hypertension Gino Seravalle Marco Volpe
Director of the Israeli Institute for Quality in Medicine Israeli Medical Association July 1st, 2016
 The differential effect of Atherosclerosis on end organ damage in adult and elderly patients with CVRF: New Algorithm for Hypertension Diagnosis and Treatment R. Zimlichman, FAHA, FASH, FESC, FESH Chief
The differential effect of Atherosclerosis on end organ damage in adult and elderly patients with CVRF: New Algorithm for Hypertension Diagnosis and Treatment R. Zimlichman, FAHA, FASH, FESC, FESH Chief
The control of hypertension in the. Reaching for Aggressive Blood Pressure Goals: Role of Angiotensin Receptor Blockade in Combination Therapy REPORTS
 REPORTS Reaching for Aggressive Blood Pressure Goals: Role of Angiotensin Receptor Blockade in Combination Therapy By Richard V. Milani, MD Abstract Elevated blood pressure, particularly systolic blood
REPORTS Reaching for Aggressive Blood Pressure Goals: Role of Angiotensin Receptor Blockade in Combination Therapy By Richard V. Milani, MD Abstract Elevated blood pressure, particularly systolic blood
ABSTRACT KEYWORDS: The prevalence of hypertension varies from percentages in all
 85 P a g e International Standard Serial Number (ISSN): 2319-8141 International Journal of Universal Pharmacy and Bio Sciences 6(6): November-December 2017 INTERNATIONAL JOURNAL OF UNIVERSAL PHARMACY AND
85 P a g e International Standard Serial Number (ISSN): 2319-8141 International Journal of Universal Pharmacy and Bio Sciences 6(6): November-December 2017 INTERNATIONAL JOURNAL OF UNIVERSAL PHARMACY AND
Chronic Disease Challenges and Solutions
 Chronic Disease Challenges and Solutions Janet Collins, PhD Director, Division of Nutrition, Physical Activity and Obesity, CDC Council of State Governments Kansas City, MO September 18, 2013 Centers for
Chronic Disease Challenges and Solutions Janet Collins, PhD Director, Division of Nutrition, Physical Activity and Obesity, CDC Council of State Governments Kansas City, MO September 18, 2013 Centers for
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension)
") Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Dysglycaemia and Hypertension. Dr E M Manuthu Physician Kitale
 Dysglycaemia and Hypertension Dr E M Manuthu Physician Kitale None Disclosures DM is MI equivalent MR FIT Objective was to assess predictors of CVD mortality among men with and without diabetes and
Dysglycaemia and Hypertension Dr E M Manuthu Physician Kitale None Disclosures DM is MI equivalent MR FIT Objective was to assess predictors of CVD mortality among men with and without diabetes and
Lowering blood pressure in 2003
 UPDATE CLINICAL UPDATE Lowering blood pressure in 2003 John P Chalmers and Leonard F Arnolda Institute for International Health, University of Sydney, Sydney, NSW. John P Chalmers, MD, FRACP, Professor
UPDATE CLINICAL UPDATE Lowering blood pressure in 2003 John P Chalmers and Leonard F Arnolda Institute for International Health, University of Sydney, Sydney, NSW. John P Chalmers, MD, FRACP, Professor
Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly
 Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly Paul Muntner, PhD MHS Professor and Vice Chair Department of Epidemiology University of Alabama
Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly Paul Muntner, PhD MHS Professor and Vice Chair Department of Epidemiology University of Alabama
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
KEEP Summary Figures S40. Am J Kidney Dis. 2012;59(3)(suppl 2):S40-S64
(suppl 2):S40-S64") 211 Summary Figures S4 Am J Kidney Dis. 212;59(3)(suppl 2):S4-S64 Definitions DATA ANALYSES DIABETES Self-reported diabetes, self reported diabetic retinopathy, receiving medication for diabetes, or elevated
211 Summary Figures S4 Am J Kidney Dis. 212;59(3)(suppl 2):S4-S64 Definitions DATA ANALYSES DIABETES Self-reported diabetes, self reported diabetic retinopathy, receiving medication for diabetes, or elevated
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Recent Hypertension Guidelines
 Recent Hypertension Guidelines Lawrence J. Fine, MD, DrPH, FAHA Division of Cardiovascular Sciences NHLBI/NIH February 19, 2014 Disclosures: Member of Panel Appointed to the Eighth Joint National Committee
Recent Hypertension Guidelines Lawrence J. Fine, MD, DrPH, FAHA Division of Cardiovascular Sciences NHLBI/NIH February 19, 2014 Disclosures: Member of Panel Appointed to the Eighth Joint National Committee
RATIONALE. chapter 4 & 2012 KDIGO
 http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
Firenze 22 settembre 2007
 Istituto di di medicina dello sport di di Firenze AMES Prevenzione cardiovascolare e cambiamenti negli stili di vita Firenze 22 settembre 2007 Orientamenti attuali per un intervento farmacologico e non
Istituto di di medicina dello sport di di Firenze AMES Prevenzione cardiovascolare e cambiamenti negli stili di vita Firenze 22 settembre 2007 Orientamenti attuali per un intervento farmacologico e non