How to Use the ADA Type 2 Diabetes Treatment Algorithm. Eric L. Johnson, MD Jay Shubrook, Jr., DO, FACOFP
|
|
|
- Peregrine Robinson
- 5 years ago
- Views:
Transcription


1 How to Use the ADA Type 2 Diabetes Treatment Algorithm Eric L. Johnson, MD Jay Shubrook, Jr., DO, FACOFP 8 ACOFP 55th Annual Convention & Scientific Seminars
2 ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please check where applicable and sign below. Provide additional pages as necessary. Name of CME Activity: ACOFP 55th Annual Convention and Scientific Seminars Dates and Location of CME Activity: March 22-25, 2018 JW Marriott Name of Faculty/Moderator: DISCLOSURE OF FINANCIAL RELATIONSHIPS WITHIN 12 MONTHS OF DATE OF THIS FORM A. Neither I nor any member of my immediate family has a financial relationship or interest with any proprietary entity producing health care goods or services. B. I have, or an immediate family member has, a financial relationship or interest with a proprietary entity producing health care goods or services. Please check the relationship(s) that applies. Research Grants Stock/Bond Holdings (excluding mutual funds) Speakers Bureaus* Ownership Consultant for Fee Employment Partnership Others, please list: Please indicate the name(s) of the organization(s) with which you have a financial relationship or interest, and the specific clinical area(s) that correspond to the relationship(s). If more than four relationships, please list on separate piece of paper: Organization With Which Relationship Exists Clinical Area Involved *If you checked Speakers Bureaus in item B, please continue: Did you participate in company-provided speaker training related to your proposed Topic? Yes: No: Did you travel to participate in this training? Yes: No: Did the company provide you with slides of the presentation in which you were trained as a speaker? Yes: No: Did the company pay the travel/lodging/other expenses? Yes: No: Did you receive an honorarium or consulting fee for participating in this training? Yes: No: Have you received any other type of compensation from the company? Please specify: Yes: No: When serving as faculty for ACOFP, will you use slides provided by a proprietary entity for your presentation and/or lecture handout materials? Yes: No: Will your Topic1 involve information or data obtained from commercial speaker training? Yes: No: DISCLOSURE OF UNLABELED/INVESTIGATIONAL USES OF PRODUCTS A. The content of my material(s)/presentation(s) in this CME activity will not include discussion of unapproved or investigational uses of products or devices. B. The content of my material(s)/presentation in this CME activity will include discussion of unapproved or investigational uses of products or devices as indicated below: I have read the ACOFP policy on full disclosure. If I have indicated a financial relationship or interest, I understand that this information will be reviewed to determine whether a conflict of interest may exist, and I may be asked to provide additional information. I understand that failure or refusal to disclose, false disclosure, or inability to resolve conflicts will require the ACOFP to identify a replacement. Signature: Date: Eric L. Johnson, MD Please this form to joank@acofp.org or fax to NO LATER THAN JANUARY 26, 2018
3
4 How to Use ADA s Type 2 Diabetes Treatment Algorithm Jay H. Shubrook DO FACOFP Professor Primary Care Department Director of Clinical Research and Diabetes Services Touro University California Eric L. Johnson, M.D. Associate Professor University of North Dakota School of Medicine and Health Sciences Assistant Medical Director Altru Diabetes Center Disclosures Dr. Johnson: Numerous clinical multicenter diabetes studies at Altru Site since 2003 Novo Nordisk Speakers Bureau Medtronic Speakers Bureau Advisory panels Novo Nordisk, Sanofi I have type 1 diabetes and I use insulin products 1
5 Disclosures Jay H. Shubrook Advisory Board Eli Lilly Novo Nordisk Intarcia Clinical Trials Eli Lilly Astra Zeneca Theracos Management of Hyperglycemia in T2DM 1. Patient-centered care 2. Anti-hyperglycemic therapy 3. Implementation strategies 4. Other considerations 2

6 Learning Objectives Recognize drug-specific and patient factors of antihyperglycemic agents to support patientprovider shared decision making Demonstrate when and how to intensify therapy Identify opportunities to refer patients to Diabetes Self-Management Education Ominous Octet 3
7 Patient-Centered Approach...providing care that is respectful of and responsive to individual patient preferences, needs, and values - ensuring that patient values guide all clinical decisions. Gauge patient s preferred level of involvement Explore therapeutic choices Consider using decision aids Shared decision making Lifestyle choices ultimately lie with the patient Diabetes Care 2012;35: ; Diabetologia 2012;55: Glycemic Recommendations: Individualized Treatment A1C <7.0% * Preprandial capillary plasma glucose mg/dl * ( mmol/l) Peak postprandial capillary plasma glucose <180 mg/dl * (<10.0 mmol/l) * More or less stringent glycemic goals may be appropriate for individual patients. Goals should be individualized based on duration of diabetes, age/life expectancy, comorbid conditions, known CVD or advanced microvascular complications, hypoglycemia unawareness, and individual patient considerations. Postprandial glucose measurements should be made 1 2 h after the beginning of the meal, generally peak levels in patients with diabetes 4
 Nutrition therapy Physical activity Smoking cessation counseling Psychosocial care American Diabetes Association Standards of Medical Care in Diabetes. 4.")
8 Approach to the Management of Hyperglycemia Lifestyle Management Lifestyle management is a fundamental aspect of diabetes care and includes Diabetes self-management education (DSME) Diabetes self-management support (DSMS) Nutrition therapy Physical activity Smoking cessation counseling Psychosocial care American Diabetes Association Standards of Medical Care in Diabetes. 4. Lifestyle Management. Diabetes Care 2018;41(Suppl. 1): S38-S50 5

9 Anti-Hyperglycemic Therapy in T2DM Therapeutic options: Oral Agents & Non-Insulin Injectables Most Popular in U.S. and Europe Metformin SGLT-2 Inhibitors GLP-1 Receptor Agonists DPP-4 Inhibitors Thiazolidinediones Sulfonylureas Less Commonly Used Meglitinides A-Glucosidase Inhibitors Colesevelam Dopamine-2 Agonists Amylin Mimetics Metformin Efficacy Hypoglycemia Weight Change Cost Oral/SQ High No Neutral (Potential for Modest Loss) Low Oral 6
10 Metformin CV Effects Renal Effects ASCVD CHF Progression of DKD Dosing/Use Considerations Potential Benefit Neutral Neutral Contraindicated with egrf <30 Additional Considerations Gastrointestinal side effects common (diarrhea, nausea) Potential for B12 deficiency Sulfonylureas (2 nd Generation) Compounds: Glyburide; Glipizide; Glimepiride Efficacy Hypoglycemia Weight Change Cost Oral/SQ High Yes Gain Low Oral 7
11 Sulfonylureas (2 nd Generation) CV Effects Renal Effects ASCVD CHF Progression of DKD Dosing/Use Considerations Neutral Neutral Neutral Glyburide: not recommended Glipizide & glimepiride: initiate conservatively to avoid hypoglycemia Additional Considerations FDA Special Warning on increased risk of cardiovascular mortality based on studies of an older sulfonylurea (tolbutamide) SGLT-2 Inhibitors Compounds: Canagliflozin; Dapagliflozin; Empagliflozin Efficacy Hypoglycemia Weight Change Cost Oral/SQ Intermediate No Loss High Oral 8
12 SGLT-2 Inhibitors CV Effects Renal Effects ASCVD CHF Progression of DKD Dosing/Use Considerations Benefit: canagliflozin, empagliflozin Benefit: canagliflozin, empagliflozin Benefit: canagliflozin, empagliflozin Canagliflozin: Not recommended with egrf <45 Dapagliflozin: Not recommended with egrf <60; contraindicated with egrf <30 Empagliflozin: contraindicated with egrf <30 SGLT-2 Inhibitors Additional Considerations FDA Black Box: risk of amputation (canagliflozin) Risk of bone fractures (canagliflozin) DKA risk (all agents, rare in T2DM) Genitourinary infections Risk of volume depletion, hypotension Increase LDL cholesterol 9
13 GPL-1RAs Compounds: Exenatide; Exenatide extended release; lixisenatide, liraglutide; semaglutide; dulaglutide Efficacy High Hypoglycemia Weight Change Cost Oral/SQ No Loss High SQ GPL-1RAs CV Effects Renal Effects ASCVD CHF Progression of DKD Dosing/Use Considerations Neutral: lixisenatide, exenatide extended release Benefit: liraglutide Neutral Benefit: liraglutide Exenatide: not indicated with egrf<30 Lixisenatide: caution with egrf <30 Increased risk of side effects in patients with renal impairment 10
14 GPL-1RAs Additional Considerations FDA Black Box: Risk of thyroid c-cell tumors (liraglutide, dulaglutide, exenatide extended release) Gastrointestinal side effects common (nausea, vomiting, diarrhea) Injection site reactions Acute pancreatitis risk DPP-4 Inhibitors Compounds: Sitagliptin; Saxagliptin; Linagliptin; Alogliptin Efficacy Intermediate Hypoglycemia Weight Change Cost Oral/SQ No Neutral High Oral 11
15 DPP-4 Inhibitors CV Effects Renal Effects ASCVD CHF Progression of DKD Dosing/Use Considerations Neutral Potential Risk: saxagliptin, alogliptin Neutral Renal dose adjustment required; can be used in renal impairment Additional Considerations Potential risk of acute pancreatitis Joint pain Thiazolidinediones (TZDs) Compounds: Pioglitazone; Rosiglitazone Efficacy High Hypoglycemia Weight Change Cost Oral/SQ No Gain Low Oral 12
16 Thiazolidinediones (TZDs) CV Effects Renal Effects ASCVD CHF Progression of DKD Dosing/Use Considerations Potential Benefit: pioglitazone Increased Risk Neutral No dose adjustment required Generally not recommended in renal impairment due to potential fluid retention Thiazolidinediones (TZDs) Additional Considerations FDA Black Box: Congestive Heart Failure (pioglitazone, rosiglitazone) Fluid retention (edema; heart failure) Benefit in NASH Risk of bone fractures Bladder cancer (pioglitazone) Increase LDL cholesterol (rosiglitazone) 13
17 Insulin Efficacy Highest Hypoglycemia Weight Change Cost Oral/SQ Yes Gain Human Insulin: Low Analogs: High SQ Insulin CV Effects Renal Effects ASCVD CHF Progression of DKD Dosing/Use Considerations Neutral Neutral Neutral Lower Insulin doses required with a decrease in egrf; titrate per clinical response Additional Considerations Injection site reactions Higher risk of hypoglycemia with a human insulin (NPH or premixed formulations) vs. analogs 14
: S73-S85 Considerations in Designing an Optimal Glucose Lowering Drug Regimen for Patients Age Weight Sex / racial / ethnic / genetic differences Comorbidities Coronary artery disease Heart")
18 Individualizing Treatment Medical Care in Diabetes. Diabetes Care 2018; 41 (Suppl. 1): S73-S85 Considerations in Designing an Optimal Glucose Lowering Drug Regimen for Patients Age Weight Sex / racial / ethnic / genetic differences Comorbidities Coronary artery disease Heart Failure Chronic kidney disease Liver dysfunction Hypoglycemia-prone Identifying and addressing barriers to medication adherence Cost Side effects 15

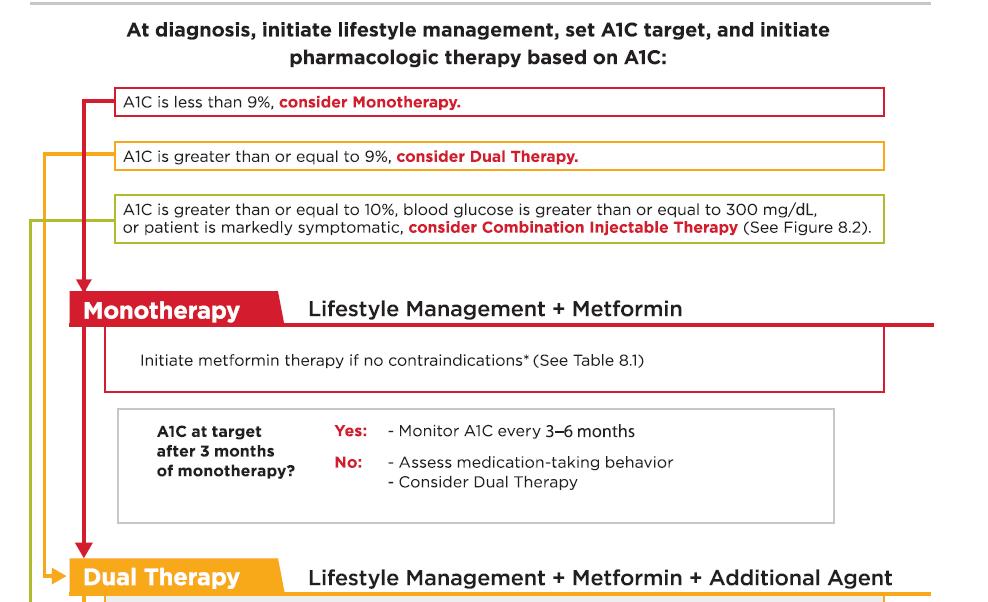
19 Antihyperglycemic Therapy in Adults with T2DM Antihyperglycemic Therapy in Adults with T2DM 16

20 Antihyperglycemic Therapy in Adults with T2DM Case 1 JW is a 42 year old male who presents for a work physical. He denies any specific symptoms or concerns. You had mentioned a couple of years ago that he had pre-diabetes and he should lose weight and there was a class he could take but he has not found the time to do this. Med hx/surg hx: none Meds: omeprazole OTC prn Allergies: none 17
21 Case 1: Physical exam Obese male BMI 32 Bp 142/88 Mild athlete s foot Exam otherwise normal Labs HbA1c = 7.5% Glucose (fasting) 138 mg/dl High trigs (258) low HDL 28 Labs otherwise normal Case 1: Question 1 What is your A1c goal for this patient? A. < 6.5% B < 7.0% C. < 7.5% D < 8.0% 18
22 Case 1: Question 2 What is the treatment plan for this patient? We will assume that he will be offered diabetes educaton A. therapeutic lifestyle change (TLC) B. TLC + metformin C. TLC + other oral medication D. TLC + insulin Case 1: Question 3 Which of the following conditions would make you not want to use metformin? A. peripheral neuropathy B. Stage 3 CKD C. Stage 4 CKD D. Stage 3 heart failure E. Cirrhosis 19
23 Case 1: Question 4 What is your next pharmacologic option for this patient? If A1c not at goal in 3 months?) Sulfonylurea DPP-4 inhibitor GLP-1 RA SGLT-2 inhibitor TZD Alpha-glucosidase inhibitor What About The Patient with Established Atherosclerotic Cardiovascular Disease (ASCVD)? 20
24 Impact of Intensive Therapy for Diabetes: Summary of Major Clinical Trials Study Microvasc CVD Mortality UKPDS DCCT / EDIC* ACCORD ADVANCE VADT Kendall DM, Bergenstal RM. International Diabetes Center 2009 UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:854. Holman RR et al. N Engl J Med. 2008;359:1577. DCCT Research Group. N Engl J Med 1993;329;977. Nathan DM et al. N Engl J Med. 2005;353:2643. Gerstein HC et al. N Engl J Med. 2008;358:2545. Patel A et al. N Engl J Med 2008;358:2560. Duckworth W et al. N Engl J Med 2009;360:129. (erratum: Moritz T. N Engl J Med 2009;361:1024). Writing Group for the DCCT/EDIC Research Group. JAMA. 2015;313(1): * in T1DM Initial Trial Long Term Follow-up Cardiovascular Benefit of Diabetes Medications 21
25 SUSTAIN-6 New GLP-1 agonist just approved December 2017, not on algorithm yet 26% risk reduction in the primary outcome, a composite of nonfatal heart attacks, nonfatal strokes, and cardiovascular death N Engl J Med. 2016;375(19): LEADER Liraglutide T2DM at higher CVD risk 22% risk reduction of cardiovascular death 22% risk reduction of nephropathy 12% risk reduction of non-fatal heart attacks,11% risk reduction of non-fatal strokes but neither statistically significant 13% reduction of primary CVD endpoints N Engl J Med 2016; 375:
26 EMPA-REG Empagliflozin T2DM patients with high CVD risk Reduced the primary major adverse cardiac event (MACE) end point (CV death, nonfatal myocardial infarction, nonfatal stroke) by 14% 38% reduction in CV mortality No significant decrease in nonfatal myocardial infarction or stroke. 35% reduction in hospitalization for heart failure without affecting hospitalization for unstable angina N Engl J Med 2015; 373: CANVAS Canagliflozin T2DM patients with high CV risk 14% reduction in CV endpoints 40% reduction in renal composite endpoints Higher risk of distal amputations N Engl J Med 2017; 377:
27 Pharmacologic Therapy For T2DM: ASCVD Recommendations In patients with T2DM and established ASCVD: antihyperglycemic therapy should begin with lifestyle management and metformin subsequently incorporate an agent proven to reduce major adverse CV events and CV mortality (currently empagliflozin and liraglutide), after considering drug-specific and patient factors (Table 8.1). A the antihyperglycemic agent canagliflozin may be considered to reduce major adverse CV events, based on drug-specific and patient factors (Table 8.1). C Case 2 MT is a 58 y/o Hispanic female Type 2 diabetes x 11 years with dyslipidemia, hypertension, albuminuria, non-painful peripheral neuropathy, obesity, NAFLD, history of MI 3 years ago Current medications: Metformin 1000mg BID Glipizide 10mg daily Pioglitazone 30mg daily Lisinopril 20mg daily Metoprolol XL 25mg daily Atorvastatin 80mg daily Aspirin 81mg daily 24
28 Case 2: Question 1 In this patient with established ASCVD, what should we consider beyond initial metformin therapy? A. TZD B. DPP-IV inhibitor C. GLP-1 RA (liraglutide) D. SGLT-2 inhibitor (canagliflozin, empagliflozin) E. either C or D Case 2: Question 2 In this patient with established ASCVD, what should we consider beyond initial metformin therapy? A. TZD B. DPP-IV inhibitor C. GLP-1 RA (liraglutide) D. SGLT-2 inhibitor (canagliflozin, empagliflozin) E. either C or D Answer: E 25
29 Case 2 Physical exam Nonproliferative retinopathy, normal heart and lung sounds, obese, decreased vibratory and filament sensation in otherwise healthy appearing feet Concerns Many blood sugars in 200 s-300 s, but occasional less than 70 mg/dl Fatigue Difficulty losing weight Labs A1C 10.2% Lipids target (on moderate statin dose), serum creatinine 0.9, GFR 54, hepatic function minor transaminase elevation, urine albumin 110 (normal <30) What next? Case 2 Recall current standards of care recommend SGLT-2 inhibitor (empagliflozin, canagliflozin) or GLP-1 agonist (liraglutide) in the setting of established cardiovascular disease Empagliflozin and liraglutide have FDA indication One of patients main complaints is difficulty losing weight, both of these drug classes are more weight-neutral or -loss 26
30 Case 2 Could do any of the following in the setting of established CVD Add liraglutide (GLP-1 RA) Add empagliflozin (or canagliflozin) (SGLT-2 inhibitor) Both GLP-1 RA or SGLT-2 inhibitor for maximal weight loss Would definitely Continue metformin (renal function is OK) Refer to diabetes educator and dietician Review activity level/exercise prescription Could consider Stop glipizide Stop pioglitazone Insulin Therapy in T2DM The progressive nature of T2DM should be regularly and objectively explained to T2DM patients. Avoid using insulin as a threat, describing it as a failure or punishment. Give patients a self-titration algorithm. 27
 Rapid analogues (lispro, aspart, glulisine) Biosimilar Insulin Basaglar (a biosimilar version of")

31 Combination Injectable Therapy in T2DM Therapeutic Options: Insulins Human Insulins Neutral protamine Hagedorn (NPH) Regular human insulin Insulin Analogues Basal analogues (glargine, detemir, degludec) Rapid analogues (lispro, aspart, glulisine) Biosimilar Insulin Basaglar (a biosimilar version of insulin glargine); long-acting Pre-mixed formulations Pre-mixed formulations Diabetes Care 2012;35: ; Diabetologia 2012;55: Diabetes Care 2015;38: ; Diabetologia 2015; /s
 Long (Glargine) 0 2 4 6 8 10 12 14 16 18 20 22 24 Hours After Injection Approach to Starting and Adjusting Insulin in")
32 Insulin level 3/15/2018 Anti-Hyperglycemic Therapy: Insulins Rapid (Lispro, Aspart, Glulisine) Short (Regular) Long (Detemir) (Degludec) Long (Glargine) Hours After Injection Approach to Starting and Adjusting Insulin in T2DM 29



33 Approach to Starting and Adjusting Insulin in T2DM Approach to Starting and Adjusting Insulin in T2DM 30
34 Case 3 GM is a 64 y/o white male Diagnosed with type 2 diabetes after 2 fasting blood sugars of 154 mg/dl and 142 mg/dl and A1C of 6.8% Saw Diabetes Educator and Dietician at diagnosis Pre-existing HTN (on Lisinopril 10mg) Dyslipidemia (on atorvastatin 40mg) no history of ASCVD ASA 81 mg daily (over 50 + DM) Case 3 Physical Exam BP 132/78, pulse 80, BMI 34 Fundi normal Obese Feet healthy appearing other than benign calluses Lipids in target (measure of compliance), hepatic and renal chemistries all normal 31
35 Case 3 Current Diabetes Medications: Metformin 1000mg BID Glimepiride 4mg daily Basal insulin 40 units daily A1C 8.2% Fasting blood glucose values 110 s-130 s 2 hour post-prandial glucose values 220 s-250 s What next? Case 3 What would be an appropriate choice for this patient? A. DPP-IV inhibitor B. Higher dose of sulfonylurea C. GLP-1 RA D. Rapid acting insulin 32

36 Case 3 What would be an appropriate choice for this patient? A. DPP-IV inhibitor B. Higher dose of sulfonylurea C. GLP-1 RA D. Rapid acting insulin Answer: C or D Options Case 3 Add rapid acting insulin to largest meal of the day 33
 Switch to premix Case 3 Patient should see Diabetes Educator (again) and Dietician for regimen")

37 Case 3 Add GLP-1 RA (or switch to combination GLP-1 RA + basal insulin) (lirglutide + degludec or lixisenatide + glargine) Switch to premix Case 3 Patient should see Diabetes Educator (again) and Dietician for regimen change/instruction and lifestyle evaluation If not reaching targets, consider multiple daily injections of insulin per algorithm Could consider stopping sulfonylurea may not be adding a lot of benefit, or could contribute to hypoglycemia 34

38 Key Points Individualize glycemic targets & BG-lowering therapies Lifestyle foundation of any T2DM therapy program Unless contraindicated, metformin is optimal first-line drug In patients with ASCVD and T2D, subsequent treatment should incorporate agent proven to CV events and/or CV mortality Ultimately, many patients will require insulin therapy alone or in combination with other agents to maintain BG control Shared decision making (focus on his/her preferences, needs & values) Comprehensive CV risk reduction - a major focus of therapy Diabetes Care 2012;35: ; Diabetologia 2012;55: Diabetes Care 2015;38: ; American Diabetes Association Standards of Medical Care in Diabetes. Diabetes Care 2018; 41 (Suppl. 1): S73-S85 Inzucchi SE et al. Diabetologia 2015;58(3): Case 4 TG, a 58-year-old African American, has had T2D for 8 years Currently being treated for hypertension (12 years) and dyslipidemia (10 years) Concerned about uncontrolled blood glucose level, a recent increase in weight (5 lbs) Non-smoker and only occasionally consumes alcohol Walks minutes, three times a week Diet has improved over last 5 years after consult with RD, but she admits to having a sweet tooth (Continued ) 35
39 Physical exam: Case 4 General examination normal, No pallor, cyanosis, clubbing or lymphadenopathy Height, 5 2 (157 cm); weight, 152 lbs (69 kg) BMI, 27.8 kg/m² BP, 132/86 mmhg Pulse 80/min, regular, peripheral pulses well felt Systemic examination- normal Foot examination is normal Fundus examination :Grade I non proliferative diabetic retinopathy Medication history: Glimepiride 2 mg daily BID Metformin sustained release preparations 1000 mg daily Telmisartan 40 mg daily Atorvastatin 10 mg at night Aspirin 81 mg at night (Continued ) Labs: A1C 8.3 % Case 4 Lipids TC 190, TG s 210, HDL 35, LDL 101 Fasting blood glucose values 130 s-160 s Post-prandial blood glucose values 190 s-220 s GFR 65, serum creatinine 1.2, hepatic chemistries normal Urine normal (no albuminuria) 36
40 Case 4 From the lab results, which plasma glucose patterns of hyperglycemia are present? A. Fasting B. Preprandial C. Postprandial D. Nocturnal E. B and C above Case 4 A drug from which of the following drug classes could you suggest to intensify Mrs. G s treatment to manage her hyperglycemia? A. GLP-1 receptor agonist B. DPP-4 inhibitor C. SGLT2 inhibitor D. Basal insulin E. A, B, C, or D above 37
41 Case 4: Think-Pair-Share What option you would have tried first? Would you discontinue the sulfonylurea or add the GLP-1 receptor agonist to the metformin/sulfonylurea? What if this patient had chronic kidney disease (GFR <40)? What if this patient had ASCVD? Thank You! 38
Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS
 Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Know Your Diabetes by Heart: Diabetes and Cardiovascular Disease. Eric L. Johnson, MD February 19, 2019
 Know Your Diabetes by Heart: Diabetes and Cardiovascular Disease Eric L. Johnson, MD February 19, 2019 WELCOME AND REMINDERS Use chat for questions and comments Slides and recording will be available on
Know Your Diabetes by Heart: Diabetes and Cardiovascular Disease Eric L. Johnson, MD February 19, 2019 WELCOME AND REMINDERS Use chat for questions and comments Slides and recording will be available on
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Clinical Cases in Diabetes Management. Joseph Cook D.O.
 Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Clinical Practice Guidelines
 Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Keep Calm and Focus on the Evidence for the Management of Diabetes. Diabetes Update 2018
 Keep Calm and Focus on the Evidence for the Management of Diabetes Diabetes Update 2018 Nicole C.Pezzino, PharmD, BCACP, CDE Assistant Professor, Wilkes University Pharmacist, Weis Markets Nicole.pezzino@wilkes.edu
Keep Calm and Focus on the Evidence for the Management of Diabetes Diabetes Update 2018 Nicole C.Pezzino, PharmD, BCACP, CDE Assistant Professor, Wilkes University Pharmacist, Weis Markets Nicole.pezzino@wilkes.edu
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017
 TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link?
 Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
WITH SO MANY NEW CLASSES OF MEDICATIONS OUT THERE
 UPDATE ON THE NEW DIABETES MEDICATIONS AND HOW TO INCORPORATE INTO YOUR PRACTICE Amy DeGueme, MD, ECNU Madison Medical Affiliates 3/15/19 WITH SO MANY NEW CLASSES OF MEDICATIONS OUT THERE Which ones to
UPDATE ON THE NEW DIABETES MEDICATIONS AND HOW TO INCORPORATE INTO YOUR PRACTICE Amy DeGueme, MD, ECNU Madison Medical Affiliates 3/15/19 WITH SO MANY NEW CLASSES OF MEDICATIONS OUT THERE Which ones to
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Noninsulin Treatment of Diabetes: What the PCP Needs to Know
 Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Quick Reference Guide
 2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Disclosures of Interest. Publications Diabetologia Key points to emphasize
 Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
AUGUST 25-27, 2017 UPDATE & BOARD REVIEW. acofp INTENSIVE. Diabetes Review. Colleen Cagno, MD INNOVATIVE COMPREHENSIVE HANDS-ON
 acofp INTENSIVE UPDATE & BOARD REVIEW AUGUST 25-27, 2017 Loews Chicago O'Hare Hotel Rosemont, IL INNOVATIVE COMPREHENSIVE HANDS-ON Diabetes Review Colleen Cagno, MD acofp Am eric an College of Osteopathi
acofp INTENSIVE UPDATE & BOARD REVIEW AUGUST 25-27, 2017 Loews Chicago O'Hare Hotel Rosemont, IL INNOVATIVE COMPREHENSIVE HANDS-ON Diabetes Review Colleen Cagno, MD acofp Am eric an College of Osteopathi
Evaluating the Cardiovascular Benefits of Antidiabetic Medications
 Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
Diabetes Mellitus in Older Adults. Presenter Disclosure Information
 Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Disclosures. Type 2 Diabetes. The New Epidemic: How Did We Get Here and What's to Come? Summary:
 Type 2. The New Epidemic: How Did We Get Here and What's to Come? Robert J. Rushakoff, MD Professor of Medicine University of California, San Francisco None Disclosures robert.rushakoff@ucsf.edu Type 2.
Type 2. The New Epidemic: How Did We Get Here and What's to Come? Robert J. Rushakoff, MD Professor of Medicine University of California, San Francisco None Disclosures robert.rushakoff@ucsf.edu Type 2.
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Diabetes Update July 6, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
CURRENT CONTROVERSIES IN DIABETES CARE
 CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
Cardiovascular Impact of Medications for Treating Type 2 Diabetes
 Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Disclaimers 22/03/2018. Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2
 Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks
 Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
New Drugs for Diabetes
 NEW DRUGS FOR DIABETES Which Ones, For Which Patients? Disclosure Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu No relevant financial relationships
NEW DRUGS FOR DIABETES Which Ones, For Which Patients? Disclosure Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu No relevant financial relationships
Canadian Journal of Diabetes
 Can J Diabetes 42 (2018) S88 S103 Contents lists available at ScienceDirect Canadian Journal of Diabetes journal homepage: www.canadianjournalofdiabetes.com 2018 Clinical Practice Guidelines Pharmacologic
Can J Diabetes 42 (2018) S88 S103 Contents lists available at ScienceDirect Canadian Journal of Diabetes journal homepage: www.canadianjournalofdiabetes.com 2018 Clinical Practice Guidelines Pharmacologic
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Vascular complications
 Vascular complications December 8, 2018 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships
Vascular complications December 8, 2018 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
9/12/2014. Main Pathophysiological Defect in T1DM. Main Pathophysiological Defects in T2DM. Personalizing Diabetes Care: The Alphabet Soup of Options
 9/12/2014 Baptist Health South Florida 13th Annual Primary Focus Symposium June 28, 2014 Silvio Inzucchi MD Section of Endocrinology Yale University School of Medicine Half-Century of HTN & T2DM Medications
9/12/2014 Baptist Health South Florida 13th Annual Primary Focus Symposium June 28, 2014 Silvio Inzucchi MD Section of Endocrinology Yale University School of Medicine Half-Century of HTN & T2DM Medications
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Diabetes Family Medicine Board Review
 Diabetes Family Medicine Board Review Sarah Kim, MD Associate Clinical Professor of Clinical Medicine, UCSF Division of Endocrinology, SFGH March 21, 2018 No disclosures Diabetes Test Topics Majority Type
Diabetes Family Medicine Board Review Sarah Kim, MD Associate Clinical Professor of Clinical Medicine, UCSF Division of Endocrinology, SFGH March 21, 2018 No disclosures Diabetes Test Topics Majority Type
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Learning Objectives. Outline 4/3/2018. Treatment Strategies to Maximize the Value of Diabetes Medications
 Treatment Strategies to Maximize the Value of Diabetes Medications Presenters: Jennifer Toy, PharmD, BCACP and Crystal Zhou, PharmD, APh AHSCP, BCACP Learning Objectives 1. Discuss which patients may benefit
Treatment Strategies to Maximize the Value of Diabetes Medications Presenters: Jennifer Toy, PharmD, BCACP and Crystal Zhou, PharmD, APh AHSCP, BCACP Learning Objectives 1. Discuss which patients may benefit
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
3/8/2011. Julie M. Sease, Pharm D, BCPS, CDE Associate Professor of Pharmacy Practice Presbyterian College School of Pharmacy
 Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Incredible Incretins Abby Frye, PharmD, BCACP
 Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Cardiovascular Outcome Trials of Diabetes Medications: Translating Results into Practice
 Presenter Disclosure Information Cardiovascular Outcome Trials of Diabetes Medications: Translating Results into Practice Carol Hatch Wysham, MD Clinical Professor of Medicine University of Washington
Presenter Disclosure Information Cardiovascular Outcome Trials of Diabetes Medications: Translating Results into Practice Carol Hatch Wysham, MD Clinical Professor of Medicine University of Washington
OBESITY IN TYPE 2 DIABETES
 OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
DIABETES UPDATE 2018
 DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department