Treating the elderly patients with type 2 diabetes mellitus
|
|
|
- Blanche Bradley
- 5 years ago
- Views:
Transcription

1 Treating the elderly patients with type 2 diabetes mellitus Niki Katsiki MSc, PhD, MD, FRSPH IASO/EASO Scope Member EASD Diabetes & Cardiovascular Disease Group Member Member of the Executive Board of the Hellenic Atherosclerosis Society Specialized in Internal Medicine and Diabetes Greece
2 Declaration of interest Associate Editor of Angiology Associate Editor of Clinical Lipidology Associate Editor of the Hellenic College of Treatment of Atherosclerosis forthe Open Cardiovascular Medicine Journal Section Editor of Archives of Medical Science Book Review and News and Views Editor of Current Vascular Pharmacology Editorial Board Member of Metabolism Clinical and Experimental and Current Medical Research and Opinion 2
3 Declaration of interest NK has given talks, attended conferences and participated in trials sponsored by Amgen, Angelini, Astra-Zeneca, Boehringer Ingelheim, Galenica, MSD, Novartis, Novo Nordisk, Sanofi and WinMedica 3
4 Why discuss treatment in the elderly? 4
5 Elderly? Oxford dictionary: following middle-age, the age of pension (!) «Τhe span of time between retirement and the beginning of ageimposed physical, emotional, and cognitive limitations» Clinical trials: > 65 years 5

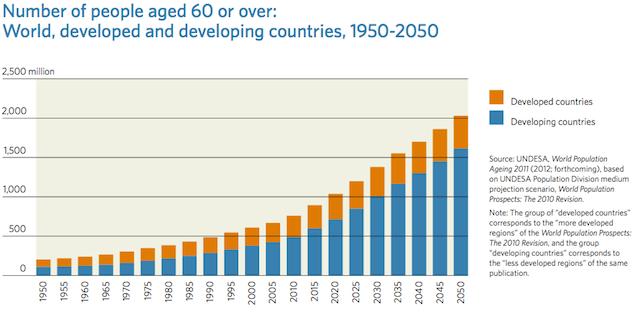
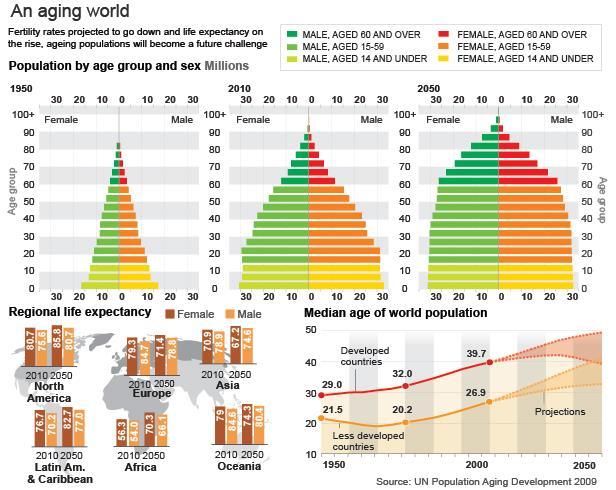
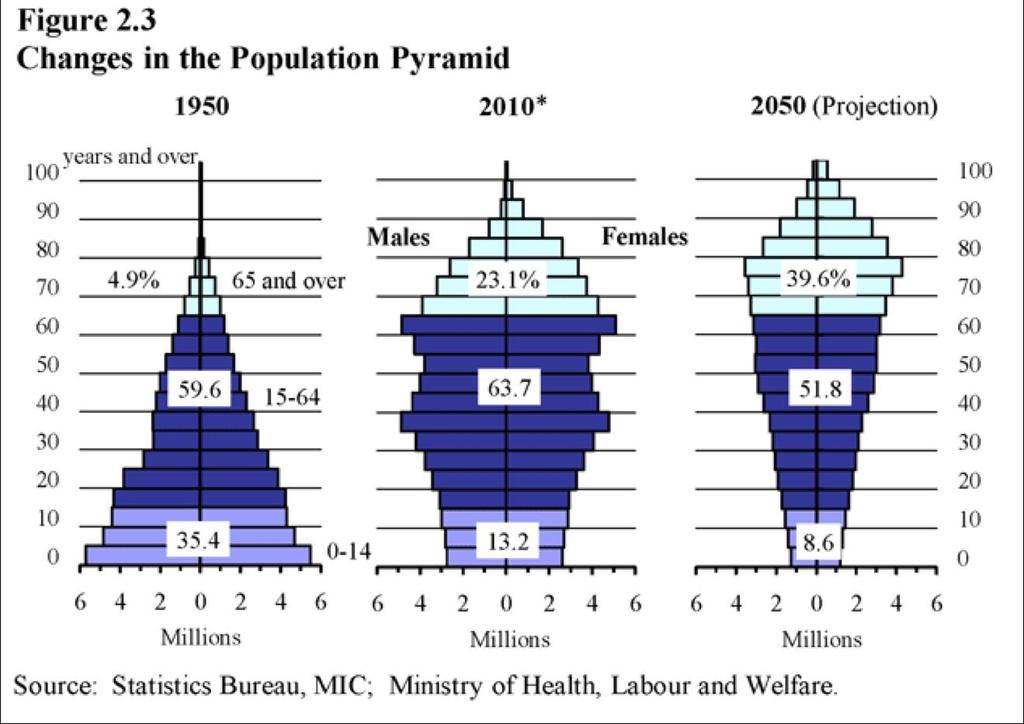
6 Aging of the population 6
7 7
8 8
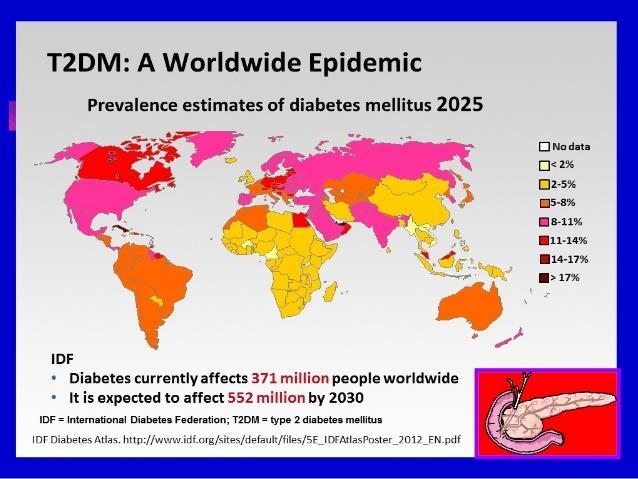
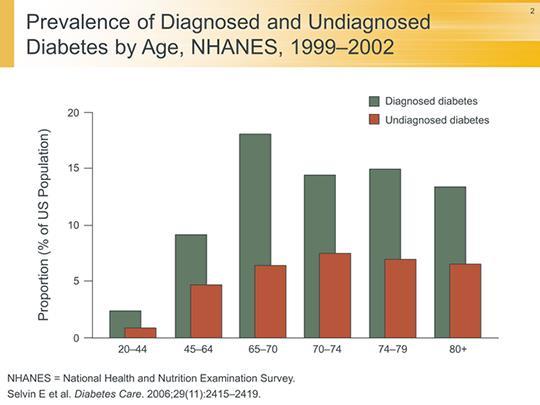
9 Why discuss T2DM in the elderly? 9
10 10
11 11

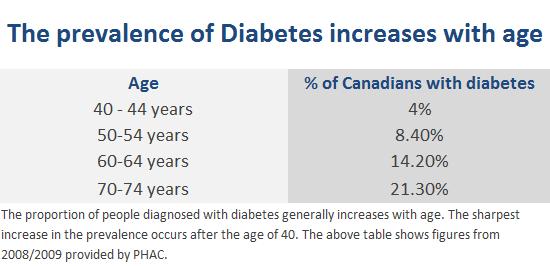
12 Prevalence of T2DM in Canada 12
13 13
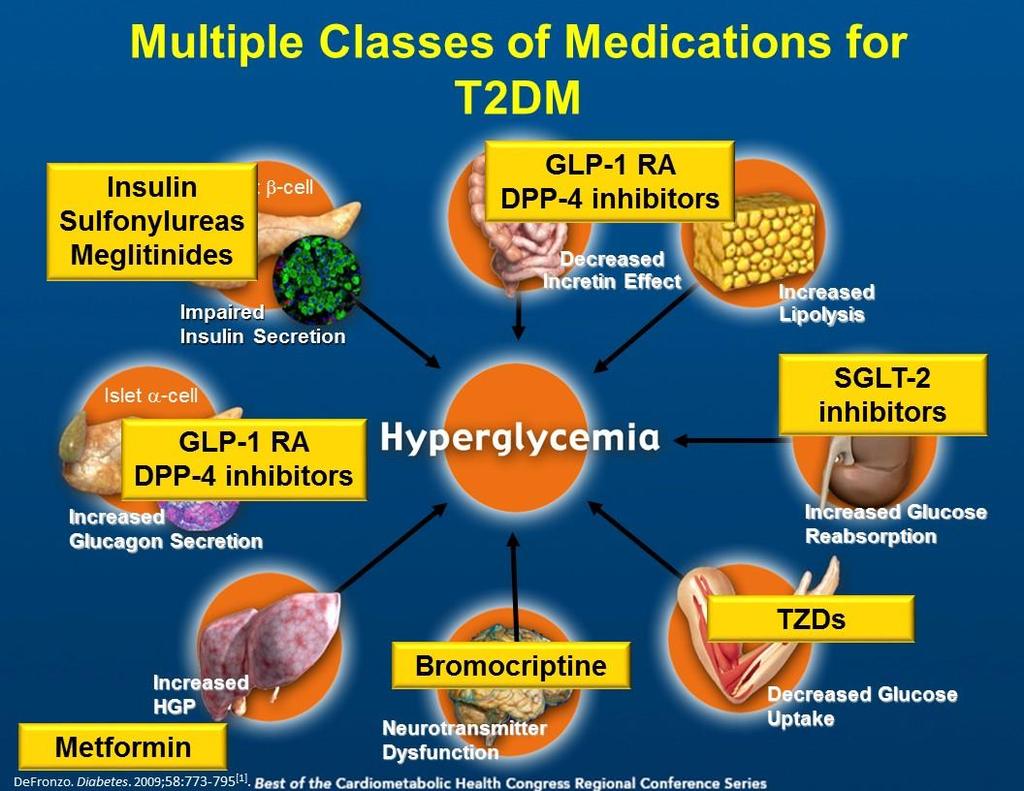
14 Pathophysiology of T2DM in the elderly 14

15 Glucose Intolerance of Aging Chang AM et al. Am J Physiol Endocrinol Metab 2003; E
:19-29 16")
16 Curr Vasc Pharmacol 2017;15(1):
17 Glucose increases gradually after the age of years Every 10 years: FBG increases by about 1 mg/dl PPG increase by 6-13 mg/dl Davidson MB. Metabolism

18 Other characteristics of the elderly More frequent complications 18
19 Other characteristics of the elderly Increased all-cause mortality Verona Study Muggeo M et al

20 Corriere M et al Curr Diab Rep 2013; 13:










21 COMPLEX INTERACTIONS in ELDERLY PATIENTS with T2DM Morbidity and Functional Disability HYPOGLYCEMIA COMPLIANCE QUALITY of LIFE CAD CVD PVD COGNITIVE DYSFUNCTION DEPRESSION POLYPHARMACY NEUROPATHY RETINOPATHY NEUROPATHY FALLS URINARY INCONTINENCE PHYSICAL DISABILITY T2DM MORBIDITY MORTALITY 21
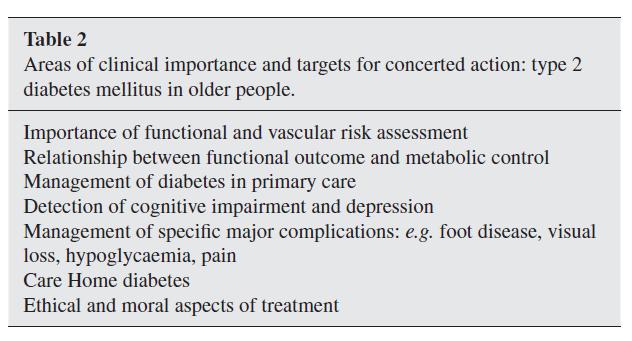
22 Clinical features of T2DM in the elderly 22

23 Clinical presentation of T2DM in the elderly e.g. silent MI Campbell IW Value Health 2000;3:3-6 23

24 Treatment of T2DM in the elderly 24


25 Why treat T2DM in the elderly? Prevention of micro- and macrovascular diabetic complications Improvement of quality of life Increase survival 25
26 26

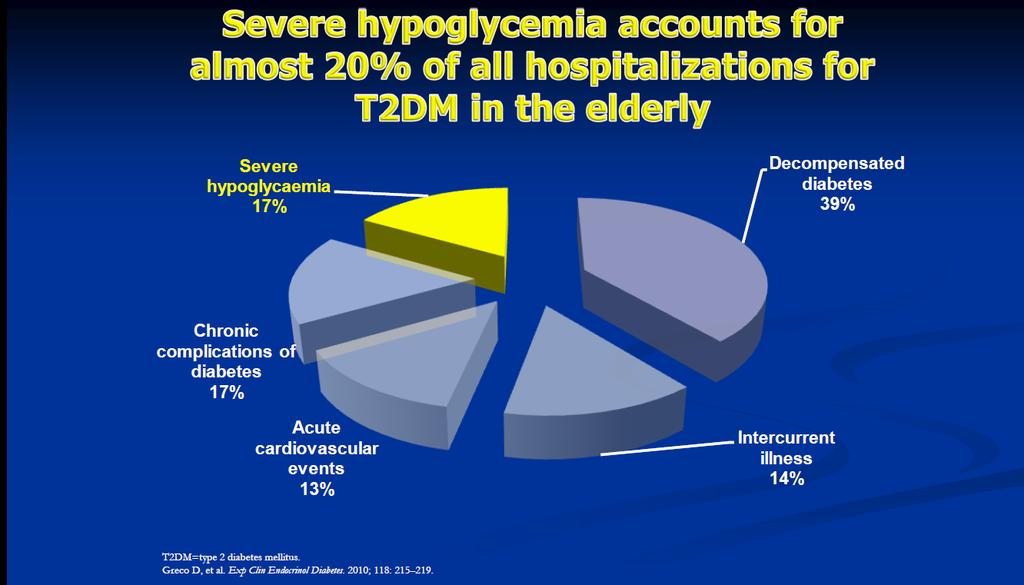
27 Hypoglycaemia 27
28 Hypoglycaemia in the elderly Elderly T2DM patients are prone to hypoglycaemia due to old age (characterized by defective mechanisms of response to hypoglycaemia and lack of hypoglycaemia awareness), polypharmacy and co-morbidities (such as renal impairment) Malnutrition and the use of insulin and/or sulfonylureas (SUs), and especially glyburide, further increase the risk of hypoglycaemia Hypoglycaemia may present with non-specific symptoms in the elderly, thus hampering the early diagnosis of a hypoglycaemic episode Strict glycaemic control in older patients with T2DM on SUs or insulin may lead to severe hypoglycaemic episodes requiring hospitalization. In contrast, other antidiabetic drugs have a low risk of hypoglycaemia such as metformin, pioglitazone and incretinbased therapies Mitrakou A, Katsiki N, Lalic NM. Curr Vasc Pharmacol. 2017;15(1):

29 Older patients have less perception of hypos 29
30 30
31 Hypoglycaemia harmful effects Hypoglycaemia has been linked to: increased morbidity (e.g. CVD, falls and dementia) and mortality, especially in the elderly; potential mechanisms include electrophysiological and proinflammatory changes as well as increased oxygen demand and myocardial workload (due to the activation of the sympathoadrenal nervous system) Large DM outcome trials suggested that severe hypoglycaemia may predict CVD events worse outcomes after a fall (i.e. head injuries and fractures) and a higher rate of use of emergency and long-term health care settings cognitive and physical dysfunction, poor quality of life, less adherence to drug therapy and increased frailty with poor long-term outcomes worsening of glycaemic control Mitrakou A, Katsiki N, Lalic NM. Curr Vasc Pharmacol 2017; 15:
32 Hypoglycaemia in the elderly Strongest predictors of severe hypoglycaemia in the elderly are advanced age, recent hospitalisation and polypharmacy Lifestyle measures and careful selection of antidiabetic drugs to prevent hypoglycaemia Education is the key to preventing recurrent or severe hypoglycaemia (close coordination of care between the patient, physician and all other healthcare providers in identifying the cause of hypoglycaemia in elderly patients, treating hypoglycaemia and preventing further episodes) Prevention of hypoglycaemia has the potential to improve psychosocial aspects of elderly health, including enhanced quality of life, boosted confidence, improved compliance with antidiabetic regimens and avoidance of long-term complications Chelliah A et al Drugs Aging 2004; 21:
33 Standards of Medical Care in Diabetes
34 Older Adults 26% of patients aged >65 have diabetes Older adults have higher rates of premature death, functional disability & coexisting illnesses At greater risk for polypharmacy, cognitive impairment, urinary incontinence, injurious falls & persistent pain Screening for complications should be individualized and periodically revisited At higher risk for depression American Diabetes Association Standards of Medical Care in Diabetes. Older adults. Diabetes Care 2016; 39 (Suppl. 1): S81-S85
35 Recommendations: Older Adults Glycemic goals for some older adults might be relaxed but hyperglycemia leading to symptoms or risk of acute hyperglycemic complications should be avoided in all patients Hypoglycemia should be avoided in older adults with diabetes It should be screened for and managed by adjusting glycemic targets and pharmacologic interventions American Diabetes Association Standards of Medical Care in Diabetes. Older adults. Diabetes Care 2016; 39 (Suppl. 1): S81-S85
36 Recommendations: Older Adults Patients with DM in long-term care facilities need careful assessment to establish a glycemic goal & to make appropriate choices of glucoselowering agents Other CV risk factors should be treated in older adults with consideration of the time frame of benefit and the individual patient o Treatment of HTN is indicated in virtually all older adults o Lipid-lowering and aspirin therapy may benefit those with life expectancy at least equal to the time frame of primary or secondary prevention trials American Diabetes Association Standards of Medical Care in Diabetes. Older adults. Diabetes Care 2016; 39 (Suppl. 1): S81-S85
37 Recommendations: Older Adults When palliative care is needed, strict BP control may not be necessary and withdrawal of therapy may be appropriate Intensity of lipid management can be relaxed and withdrawal of lipid-lowering therapy may be appropriate Screening for complications should be individualized, but attention should be paid to complications that would lead to functional impairment American Diabetes Association Standards of Medical Care in Diabetes. Older adults. Diabetes Care 2016; 39 (Suppl. 1): S81-S85
38 Recommendations: Older Adults Screening for geriatric syndromes may be appropriate in older adults with limitations in basic and instrumental activities of daily living Older adults with DM should be considered a high-priority population for depression screening and treatment Overall comfort, prevention of distressing symptoms & preservation of quality of life and dignity are primary goals for diabetes management at the end of life American Diabetes Association Standards of Medical Care in Diabetes. Older adults. Diabetes Care 2016; 39 (Suppl. 1): S81-S85
39 Recommendations: Hypertension/ Blood Pressure Control Patients with confirmed BP >140/90 mmhg should, in addition to lifestyle therapy, have prompt initiation and timely subsequent titration of pharmacological therapy to achieve blood pressure goals In older adults, pharmacological therapy to achieve treatment goals of <130/70 are not recommended Lifestyle intervention including: o o o o Weight loss if overweight DASH-style diet including reduced sodium, increased potassium Moderation of alcohol intake Increased physical activity American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2016; 39 (Suppl. 1): S60-S71
40 Recommendations: Hypertension/ Blood Pressure Control Treatment: Pharmacological therapy for patients with diabetes and HTN includes: o either an ACE inhibitor or angiotensin II receptor blocker o if one class is not tolerated, substitute the other Multiple drug therapy (two or more agents at maximal doses) generally required to achieve BP targets American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2016; 39 (Suppl. 1): S60-S71
41 Recommendations for Statin Treatment in People with Diabetes Age Risk Factors Statin Intensity * <40 years years >75 years None ASCVD risk factor(s)** ASCVD None ASCVD risk factors ACS & LDL >50 who can t tolerate high dose statin None ASCVD risk factors ASCVD ACS & LDL >50 who can t tolerate high dose statin None Moderate or high High Moderate High Moderate + ezetimibe Moderate Moderate or high High Moderate + ezetimibe * In addition to lifestyle therapy. ** ASCVD risk factors include LDL cholesterol 100 mg/dl (2.6 mmol/l), high blood pressure, smoking, overweight and obesity, and family history of premature ASCVD. American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2016; 39 (Suppl. 1): S60-S71
42 Recommendations: Lipid Management Consider therapy with statin and fenofibrate for men with both trigs 204 mg/dl (2.3 mmol/l) and HDL 34 mg/dl (0.9 mmol/l) Combination therapy (statin/niacin) hasn t demonstrated additional CV benefit over statins alone, may raise risk of stroke & is not generally recommended American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2016; 39 (Suppl. 1): S60-S71
43 Recommendations: Antiplatelet Agents Consider aspirin therapy ( mg/day) As a primary prevention strategy in those with type 1 or type 2 diabetes at increased cardiovascular risk (10- year risk >10%) Includes most men or women with diabetes age 50 years who have at least one additional major risk factor, including: o o o o o Family history of premature ASCVD Hypertension Smoking Dyslipidemia Albuminuria American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2016; 39 (Suppl. 1): S60-S71
44 Recommendations: Antiplatelet Agents Use aspirin therapy ( mg/day) as secondary prevention in those with diabetes and history of ASCVD For patients w/ ASCVD & aspirin allergy, clopidogrel (75 mg/day) should be used Dual antiplatelet therapy is reasonable for up to a year after an acute coronary syndrome American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2016; 39 (Suppl. 1): S60-S71

45 Approach to the Management of Hyperglycemia Patient/Disease Features Risks associated with hypoglycemia & other drug adverse effects Disease Duration more stringent low newly diagnosed A1C 7% less stringent high long-standing Life expectancy Important comorbidities Established vascular complications long absent absent Few/mild Few/mild short severe severe Patient attitude & expected treatment efforts Resources & support system highly motivated, adherent, excellent self-care capabilities readily available less motivated, nonadherent, poor self-care capabilities limited American Diabetes Association Standards of Medical Care in Diabetes. Glycemic targets. Diabetes Care 2016; 39 (Suppl. 1): S39-S46

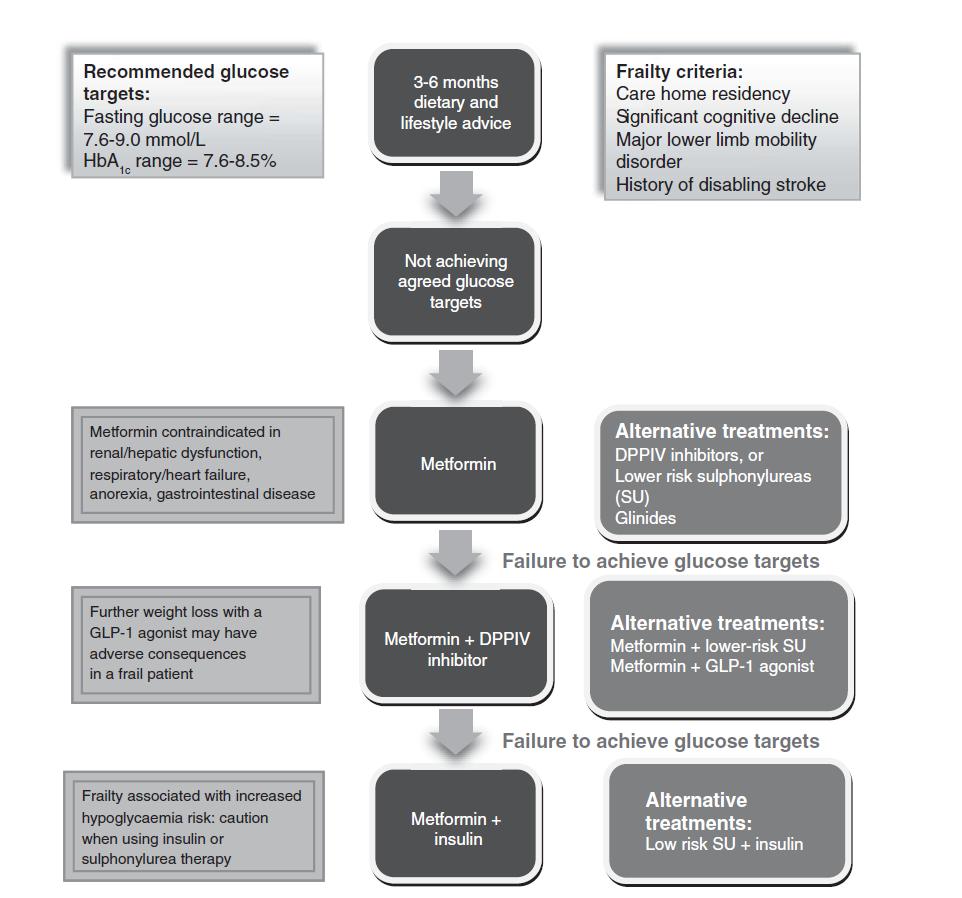
46 Treatment targets for the elderly
47 47
48 48
49 49
50 50

51 51
52 Metformin HbA1c reduction: 1-2% Advantages Weight neutral Low cost No hypos Disadvantages GI side effects Lactic acidosis Contraindications: heart, liver and renal failure (GFR < 30 ml/min) 52
53 Acarbose HbA1c reduction: % Advantages Weight neutral Improvement in PPG No hypos Disadvantages GI side effects Contraindications: renal failure (GFR < 25 ml/min) 53
54 SUs HbA1c reduction: 1-2% Advantages High efficacy Low cost Disadvantages Weight gain Hypos Ischemic preconditioning Contraindications: renal failure (GFR < 30 ml/min) 54
55 Meglitinides HbA1c reduction: % Advantages Improvement in PPG Flexibility Disadvantages Hypos Weight gain Contraindications: renal failure (GFR < 15 ml/min) 55
56 Pioglitazone HbA1c reduction: % Advantages CV benefits (PROActive trial) Low cost No hypos Disadvantages Weight gain/edema Bone fractures Contraindications: heart and renal failure (GFR < 5 ml/min) 56
57 DPP-4 inhibitors HbA1c reduction: % Advantages Weight neutral No hypos CV safety (TECOS, EXAMINE and SAVOR-TIMI trials) Disadvantages Cost Weight gain Dose adjustment in renal failure (GFR < 50 ml/min), except for linagliptin Heart failure (saxagliptin) 57
58 GLP-1 receptor agonists HbA1c reduction: % Advantages Weight reduction No hypos Metabolic effects CV reduction (LEADER and SUSTAIN trials)- safety (EXCSEL trial) Disadvantages Cost Injectable GI side effects Contraindications: renal failure (GFR < 30 ml/min) 58
59 SGLT2 inhibitors HbA1c reduction: % Advantages Weight reduction No hypos Metabolic effects: BP, lipids, uric acid CV reduction (EMPA-REG OUTCOME and CANVAS Program trials) Disadvantages Cost Genital infections Contraindications: renal failure (GFR < 60 ml/min) Caution: diuretics, dehydration 59
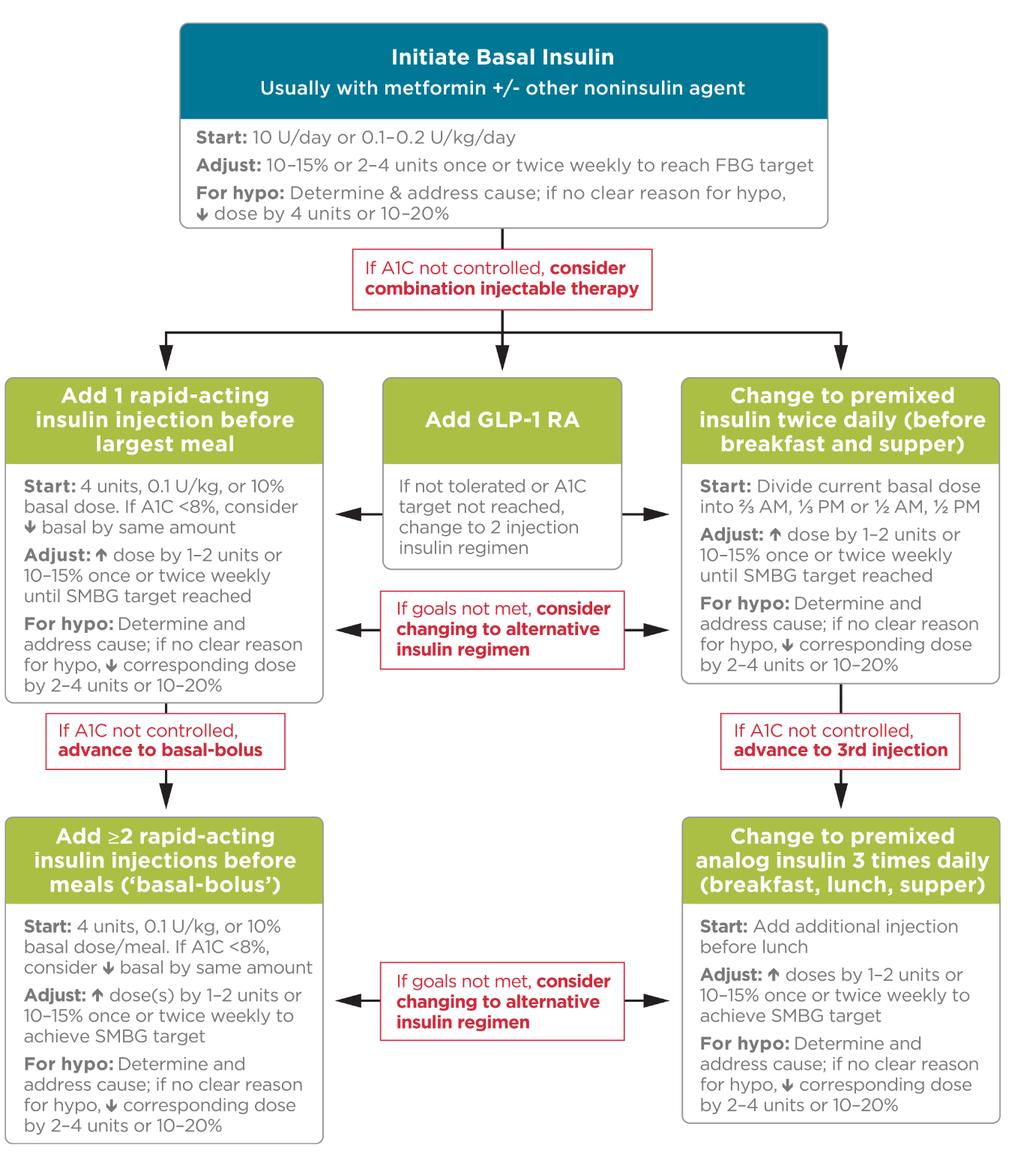
60 Insulin therapy Basal, basal-plus, basal-bolus, premixed Advantages Efficacy Can be used in heart, liver and renal failure Disadvantages Hypos Education of the patient + care provider Fear of the needle/hypos Follow-up 60

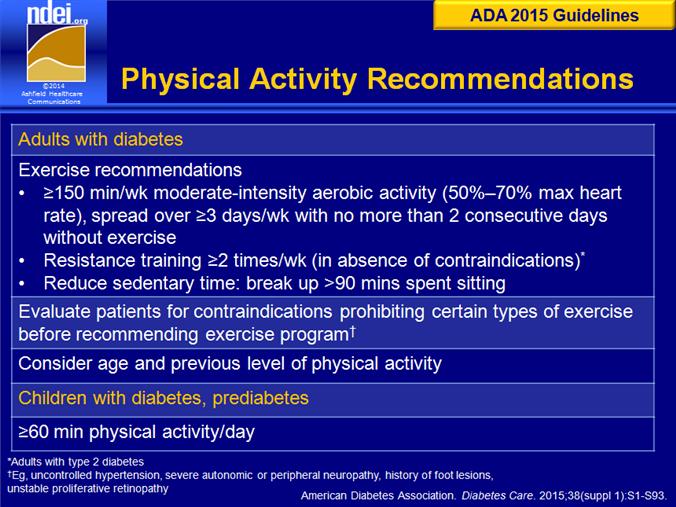
61 Foundations of Care 1. Self Management Education 2. Nutrition 3. Counseling 4. Physical Activity 5. Smoking Cessation 6. Immunizations 7. Psychosocial Care 8. Medications American Diabetes Association Standards of Medical Care in Diabetes. Foundations of care and the comprehensive medical evaluation. Diabetes Care 2016; 39 (Suppl. 1): S23-S35

62 Cl Clin Interv Aging 2008;3:
63 63
64 64
65 Diabetes treatment considerations with aging PHYSIOLOGY Postprandial Hyperglycemia Increased risk of Hypoglycemia Age related PK and PD changes SELF MANAGEMENT ABILITY Competing priorities Polypharmacy Depression Physical limitations ENVIRONMENT Meal planning Physical activity Safety DIABETES TREATMENT Hyperglycemia affects cognition Hypoglycemia affects cognition Benefit of treatment over lifespan Risks of treatment 65
66 The good physician treats the disease; the great physician treats the patient who has the disease William Osler
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Mellitus in Older Adults. Presenter Disclosure Information
 Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Quick Reference Guide
 2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Standards of Medical Care in Diabetes 2016
 Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2018
 Standards of Medical Care in Diabetes 2018 Eric L. Johnson, M.D. Associate Professor University of North Dakota School of Medicine and Health Sciences Assistant Medical Director Altru Diabetes Center Grand
Standards of Medical Care in Diabetes 2018 Eric L. Johnson, M.D. Associate Professor University of North Dakota School of Medicine and Health Sciences Assistant Medical Director Altru Diabetes Center Grand
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications
 American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
Diabetes Update: Diabetes Management In Primary Care. Jonathon M. Firnhaber, MD, FAAFP
 Diabetes Update: Diabetes Management In Primary Care Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Critically evaluate the evidence emerging within diabetes research as it applies to recommendations
Diabetes Update: Diabetes Management In Primary Care Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Critically evaluate the evidence emerging within diabetes research as it applies to recommendations
Finding the sweet spot: Individualized targets for older adults with Type 2 DM
 Finding the sweet spot: Individualized targets for older adults with Type 2 DM Samuel C. Durso, M.D., M.B.A. Mason F. Lord Professor of Medicine Director, Division of Geriatric Medicine and Gerontology
Finding the sweet spot: Individualized targets for older adults with Type 2 DM Samuel C. Durso, M.D., M.B.A. Mason F. Lord Professor of Medicine Director, Division of Geriatric Medicine and Gerontology
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Μεταβλητότητα γλυκόζης και καρδιά
 Μεταβλητότητα γλυκόζης και καρδιά Nίκη Κατσίκη MSc, PhD, MD, FRSPH IASO/EASO Scope Member EASD Diabetes & Cardiovascular Disease Group Member Μέλος ΔΣ της Ελληνικής Εταιρείας Αθηροσκλήρωσης Ειδική Παθολόγος,
Μεταβλητότητα γλυκόζης και καρδιά Nίκη Κατσίκη MSc, PhD, MD, FRSPH IASO/EASO Scope Member EASD Diabetes & Cardiovascular Disease Group Member Μέλος ΔΣ της Ελληνικής Εταιρείας Αθηροσκλήρωσης Ειδική Παθολόγος,
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii
 Individualized Diabetes Treatment for the Elderly Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii Extremely Relevant Baby Boomers are aging! ¼ of people age
Individualized Diabetes Treatment for the Elderly Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii Extremely Relevant Baby Boomers are aging! ¼ of people age
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Standards of Medical Care In Diabetes
 Standards of Medical Care In Diabetes - 2017 Robert E. Ratner, MD, FACP, FACE Professor of Medicine Georgetown University School of Medicine Disclosed no conflict of interest Standards of Care Professional.diabetes.org/SOC
Standards of Medical Care In Diabetes - 2017 Robert E. Ratner, MD, FACP, FACE Professor of Medicine Georgetown University School of Medicine Disclosed no conflict of interest Standards of Care Professional.diabetes.org/SOC
Diabetes in the Elderly 1, 2, 3
 Diabetes in the Elderly 1, 2, 3 WF Mollentze Feb 2010 Diabetes in the elderly differs from diabetes in younger people Prevalence: o Diabetes increases with age affecting approximately 10% of people over
Diabetes in the Elderly 1, 2, 3 WF Mollentze Feb 2010 Diabetes in the elderly differs from diabetes in younger people Prevalence: o Diabetes increases with age affecting approximately 10% of people over
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
Standards of Care in Diabetes What's New? Veronica Brady, FNP-BC, PhD, BC-ADM,CDE Karmella Thomas, RD, LD,CDE
 Standards of Care in Diabetes 2016-- What's New? Veronica Brady, FNP-BC, PhD, BC-ADM,CDE Karmella Thomas, RD, LD,CDE Terminology No longer using the term diabetic. Diabetes does not define people. People
Standards of Care in Diabetes 2016-- What's New? Veronica Brady, FNP-BC, PhD, BC-ADM,CDE Karmella Thomas, RD, LD,CDE Terminology No longer using the term diabetic. Diabetes does not define people. People
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Current Clinical Practice Guideline for Diabetes Management
 Current Clinical Practice Guideline for Diabetes Management Chaicharn Deerochanawong M.D. Professor of Medicine, i Rangsit Medical University it Diabetes and Endocrinology Unit Department of Medicine Rajavithi
Current Clinical Practice Guideline for Diabetes Management Chaicharn Deerochanawong M.D. Professor of Medicine, i Rangsit Medical University it Diabetes and Endocrinology Unit Department of Medicine Rajavithi
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Management of DM in Older Adults: It s not all about sugar! Who needs treatment for DM? Peggy Odegard, Pharm.D., BCPS, CDE
 Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Diabetes Mellitus: Overview and Guidelines
 Diabetes Mellitus: Overview and Guidelines Rezvan Salehidoost, M.D., Endocrinologist Abidi Diabetes Master Class IMPORTANCE? Why is it interesting to do research in diabetes J. Olefsky, JAMA 2001:285:628-632
Diabetes Mellitus: Overview and Guidelines Rezvan Salehidoost, M.D., Endocrinologist Abidi Diabetes Master Class IMPORTANCE? Why is it interesting to do research in diabetes J. Olefsky, JAMA 2001:285:628-632
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Pre-diabetes. Pharmacological Approaches to Delay Progression to Diabetes
 Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL
 Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Dr Tahseen A. Chowdhury Royal London Hospital. New Guidelines in Diabetes: NICE or Nasty?
 Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 5 PURPOSE To assure that DOP inmates with Diabetes are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers are to follow these guidelines when treating
PAGE 1 of 5 PURPOSE To assure that DOP inmates with Diabetes are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers are to follow these guidelines when treating
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
Rational Goal-Setting and Management of Diabetes in the Elderly
 Rational Goal-Setting and Management of Diabetes in the Elderly Michael Shannon, MD Medical Director, Physicians of Southwest Washington Clinical Assistant Professor, University of Washington Outline of
Rational Goal-Setting and Management of Diabetes in the Elderly Michael Shannon, MD Medical Director, Physicians of Southwest Washington Clinical Assistant Professor, University of Washington Outline of
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol
 Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Case study: Lean adult with no complications, newly diagnosed with type 2 diabetes
 Case study: Lean adult with no complications, newly diagnosed with type 2 diabetes Authored by Clifford Bailey and James LaSalle on behalf of the Global Partnership for Effective Diabetes Management. The
Case study: Lean adult with no complications, newly diagnosed with type 2 diabetes Authored by Clifford Bailey and James LaSalle on behalf of the Global Partnership for Effective Diabetes Management. The
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Older Adults & Optimal Outcome. Individualizing Diabetes Management. Mary Moyer Janci BC-FNP BC-ADM CDE Teaching Associate Diabetes Care Center UWMC
 Older Adults & Optimal Outcome Individualizing Diabetes Management Mary Moyer Janci BC-FNP BC-ADM CDE Teaching Associate Diabetes Care Center UWMC What is Diabetes? METABOLIC DISEASE Food breakdown (carbohydrates,
Older Adults & Optimal Outcome Individualizing Diabetes Management Mary Moyer Janci BC-FNP BC-ADM CDE Teaching Associate Diabetes Care Center UWMC What is Diabetes? METABOLIC DISEASE Food breakdown (carbohydrates,
Diabetes: a key problem in elderly
 Diabetes: a key problem in elderly 노인인구의급격한증가 자료 : 통계청. 고령자통계. 2005 Prevalence of diagnosed and undiagnosed diabetes and IGT by age and sex, KOREA Park Y, et al. Diabetes Care. 18(4):545-8, 1995 2005 년도우리나라당뇨병유병률
Diabetes: a key problem in elderly 노인인구의급격한증가 자료 : 통계청. 고령자통계. 2005 Prevalence of diagnosed and undiagnosed diabetes and IGT by age and sex, KOREA Park Y, et al. Diabetes Care. 18(4):545-8, 1995 2005 년도우리나라당뇨병유병률
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
Current Diabetes Care for Internists:2011
 Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
2013 ESC Guidelines on Diabetes, Pre-diabetes and Cardiovascular Diseases Developed in Collaboration with EASD
 2013 ES Guidelines on Diabetes, Pre-diabetes and ardiovascular Diseases Developed in ollaboration with ESD Paul Valensi Department of Endocrinology Diabetology Nutrition Jean Verdier Hospital Paris-Nord
2013 ES Guidelines on Diabetes, Pre-diabetes and ardiovascular Diseases Developed in ollaboration with ESD Paul Valensi Department of Endocrinology Diabetology Nutrition Jean Verdier Hospital Paris-Nord
Diabetes Complications Guideline Based Screening, Management, and Referral
 Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Know Your Diabetes by Heart: Diabetes and Cardiovascular Disease. Eric L. Johnson, MD February 19, 2019
 Know Your Diabetes by Heart: Diabetes and Cardiovascular Disease Eric L. Johnson, MD February 19, 2019 WELCOME AND REMINDERS Use chat for questions and comments Slides and recording will be available on
Know Your Diabetes by Heart: Diabetes and Cardiovascular Disease Eric L. Johnson, MD February 19, 2019 WELCOME AND REMINDERS Use chat for questions and comments Slides and recording will be available on
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017
 TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
Diabetes and Heart Disease. Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center
 Diabetes and Heart Disease Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center No conflicts of interest or financial relationships to disclose. 2 What s the problem??
Diabetes and Heart Disease Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center No conflicts of interest or financial relationships to disclose. 2 What s the problem??
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Diabetes Update July 6, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Modified version focused on CCNC Quality Measures and Feedback Processes
 Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy
 Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy Melpomeni Peppa Assistant Professor of Endocrinology 2 nd Dept of Internal Medicine-Propaedeutic, Athens
Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy Melpomeni Peppa Assistant Professor of Endocrinology 2 nd Dept of Internal Medicine-Propaedeutic, Athens
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Philippine Practice Guidelines for the Diagnosis & Management of Type 2 Diabetes Mellitus
 Philippine Practice Guidelines for the Diagnosis & Management of Type 2 Diabetes Mellitus Iris Thiele Isip Tan MD, MSc, FPCP, FPSEM Chief, Medical Informatics Unit Associate Professor IV, UP College of
Philippine Practice Guidelines for the Diagnosis & Management of Type 2 Diabetes Mellitus Iris Thiele Isip Tan MD, MSc, FPCP, FPSEM Chief, Medical Informatics Unit Associate Professor IV, UP College of
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks
 Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Disclosures of Interest. Publications Diabetologia Key points to emphasize
 Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Evaluating the Cardiovascular Benefits of Antidiabetic Medications
 Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
Diabetic Management of the Cardiac Patient
 Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus
 Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY?
 MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
Diagnosis and Management of Type 2 Diabetes Mellitus in Adults
 Quality Improvement Support: Diagnosis and Management of Type 2 Diabetes Mellitus in Adults The Aims and Measures section is intended to provide guideline users with a menu of measures for multiple purposes,
Quality Improvement Support: Diagnosis and Management of Type 2 Diabetes Mellitus in Adults The Aims and Measures section is intended to provide guideline users with a menu of measures for multiple purposes,
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Glucose Control and Prevention of Cardiovascular Disease
 Glucose Control and Prevention of Cardiovascular Disease Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Diabetes Update+, March
Glucose Control and Prevention of Cardiovascular Disease Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Diabetes Update+, March
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Cardiovascular risk reduction in diabetes Lipids (NICE CG181)
") Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Alia Gilani Health Inequalities Pharmacist
 Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals