Standards of Medical Care in Diabetes 2018
|
|
|
- Kristopher Gregory
- 5 years ago
- Views:
Transcription


1 Standards of Medical Care in Diabetes 2018 Eric L. Johnson, M.D. Associate Professor University of North Dakota School of Medicine and Health Sciences Assistant Medical Director Altru Diabetes Center Grand Forks, ND
2 Thank you American Diabetes Association for slides
3 Evidence Grading System
4 1. Improving Care and Promoting Health in Populations
5 Chronic Care Model (CCM) The CCM includes Six Core Elements to optimize the care of patients with chronic disease: 1. Delivery system design 2. Self-management support 3. Decision support 4. Clinical information systems 5. Community resources & policies 6. Health systems Improving Care and Promoting Health in Population: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S7-S12
6 Support Patient Self-Management Implement a systematic approach to support patient behavior change efforts, including: High-quality diabetes self-management education and support (DSMES) Clinical content & skills Behavioral strategies (goal setting, problem solving, etc.) Engagement with psychosocial concerns Addressing barriers to medication taking Improving Care and Promoting Health in Population: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S7-S12
7 Health Inequities Health inequities related to diabetes and its complications are well documented and are heavily influenced by social determinants of health Social determinants of health are defined as: The economic, environmental, political, and social conditions in which people live Responsible for a major part of health inequality worldwide Improving Care and Promoting Health in Population: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S7-S12
8 2. Classification and Diagnosis of Diabetes

9 Criteria for the Diagnosis of Diabetes Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S13-S27

10 Categories of Increased Risk for Diabetes (Prediabetes) Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S13-S27

11 Testing for Diabetes or Prediabetes in Asymptomatic Adults Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S13-S27
12
13 Prediabetes: Recommendations (2) If tests are normal, repeat testing carried out at a minimum of 3-year intervals is reasonable. C To test for prediabetes, fasting plasma glucose, 2-h plasma glucose during 75-g oral glucose tolerance test, and A1C are equally appropriate. B In patients with prediabetes, identify and, if appropriate, treat other cardiovascular disease risk factors. B Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S13-S27
14 Gestational Diabetes Mellitus (GDM): Recommendations Test for undiagnosed diabetes at the 1 st prenatal visit in those with risk factors, using standard diagnostic criteria. B Test for GDM at weeks of gestation in pregnant women not previously known to have diabetes. A Test women with GDM for persistent diabetes at 4 12 weeks postpartum, using the OGTT and clinically appropriate nonpregnancy diagnostic criteria. E Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S13-S27
15 Gestational Diabetes Mellitus (GDM): Recommendations (2) Women with a history of GDM should have lifelong screening for the development of diabetes or prediabetes at least every 3 years. B Women with a history of GDM found to have prediabetes should receive intensive lifestyle interventions or metformin to prevent diabetes. A Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S13-S27

16 Screening and Diagnosis of GDM: One-Step Strategy Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S13-S27

17 Screening and Diagnosis of GDM: Two-Step Strategy Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S13-S27
18 3. Comprehensive Medical Evaluation and Assessment of Comorbidities
19 Components of the Comprehensive Diabetes Evaluation Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S28-S37

20 Components of the Comprehensive Diabetes Evaluation Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S28-S37

21 Components of the Comprehensive Diabetes Evaluation * 65 years Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S28-S37

22 Components of the Comprehensive Diabetes Evaluation Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S28-S37
,.")
23 Components of the Comprehensive Diabetes Evaluation May be needed more frequently in patients with known chronic kidney disease or with changes in medications that affect kidney function and serum potassium. # May also need to be checked after initiation or dose changes of medications that affect these laboratory values (i.e., diabetes medications, blood pressure medications, cholesterol medications, or thyroid medications),. In people without dyslipidemia and not on cholesterol-lowering therapy, testing may be less frequent. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S28-S37


24 Components of the Comprehensive Diabetes Evaluation May be needed more frequently in patients with known chronic kidney disease or with changes in medications that affect kidney function and serum potassium. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S28-S37
25 4. Lifestyle Management
26 Diabetes Self-Management Education & Support: Recommendations (2) Effective DSMES should be patient centered, may be given in group or individualized settings or using technology, and should help guide clinical decisions. A Because DSMES can improve outcomes and reduce costs B, adequate reimbursement by third-party payers is recommended. E Lifestyle Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S38-S50
27 DSMES Delivery Four critical time points for DSMES delivery: 1. At diagnosis 2. Annually for assessment of education, nutrition, and emotional needs 3. When new complicating factors (health conditions, physical limitations, emotional factors, or basic living needs) arise that influence selfmanagement; and 4. When transitions in care occur Lifestyle Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S38-S50
28 Goals of Nutrition Therapy 1. To promote and support healthful eating patterns, emphasizing a variety of nutrient-dense foods in appropriate portion sizes, to improve overall health and to: Achieve and maintain body weight goals Attain individualized glycemic, blood pressure, and lipid goals Delay or prevent the complications of diabetes 2. To address individual nutrition needs based on personal & cultural preferences, health literacy & numeracy, access to healthful foods, willingness and ability to make behavioral changes, & barriers to change Lifestyle Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S38-S50
29 Goals of Nutrition Therapy (2) 3. To maintain the pleasure of eating by providing nonjudgmental messages about food choices 4. To provide an individual with diabetes the practical tools for developing healthful eating patterns rather than focusing on individual macronutrients, micronutrients, or single foods Lifestyle Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S38-S50
30 Physical Activity: Recommendations Children and adolescents with diabetes or prediabetes should engage in 60 min/day or more of moderate- or vigorousintensity aerobic activity, with vigorous muscle-strengthening and bone-strengthening activities at least 3 days/week. C Most adults with type 1 C and type 2 B diabetes should engage in 150 min or more of moderate-to-vigorous intensity aerobic activity per week, spread over at least 3 days/week, with no more than 2 consecutive days without activity. Shorter durations (minimum 75 min/week) of vigorous-intensity or interval training may be sufficient for younger and more physically fit individuals. Lifestyle Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S38-S50
31 Recommendations: Physical Activity (2) Adults with type 1 C and type 2 B diabetes should engage in 2-3 sessions/week of resistance exercise on nonconsecutive days. All adults, and particularly those with type 2 diabetes, should decrease the amount of time spent in daily sedentary behavior. B Prolonged sitting should be interrupted every 30 min for blood glucose benefits, particularly in adults with type 2 diabetes. C Flexibility training and balance training are recommended 2 3 times/week for older adults with diabetes. Yoga and tai chi may be included based on individual preferences to increase flexibility, muscular strength, and balance. C Lifestyle Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S38-S50
32 Recommendations: Smoking Cessation Advise all patients not to use cigarettes and other tobacco products A or e-cigarettes. E Include smoking cessation counseling and other forms of treatment as a routine component of diabetes care. B Lifestyle Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S38-S50
33 Psychosocial Issues: Recommendations Psychosocial care should be integrated with a collaborative, patient-centered approach and provided to all people with diabetes, with the goals of optimizing health outcomes and health-related quality of life (QOL). A Psychosocial screening and follow-up may include, but are not limited to, attitudes about diabetes, expectations for medical management and outcomes, affect or mood, general and diabetesrelated QOL, available resources (financial, social, and emotional), and psychiatric history. E Lifestyle Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S38-S50
34 Psychosocial Issues: Recommendations (2) Providers should consider assessment for symptoms of diabetes distress, depression, anxiety, disordered eating, and cognitive capacities using patient-appropriate standardized and validated tools at the initial visit, at periodic intervals, and when there is a change in disease, treatment, or life circumstance. Including caregivers and family members in this assessment is recommended. B Consider screening older adults (aged 65 years) with diabetes for cognitive impairment and depression. B Lifestyle Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S38-S50
35 5. Prevention or Delay of Type 2 Diabetes
36 Prevention or Delay of T2DM: Recommendations At least annual monitoring for the development of diabetes in those with prediabetes is suggested. E Patients with prediabetes should be referred to an intensive behavioral lifestyle intervention program modeled on the Diabetes Prevention Program to achieve and maintain 7% loss of initial body weight and increase moderate-intensity physical activity (such as brisk walking) to at least 150 min/week. A Prevention or Delay of Type 2 Diabetes: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S51-S54
37 6. Glycemic Targets
38 Question All persons with diabetes should have a target A1C of <7% A. Yes B. No Answer: B. A1C targets should be individualized
39 A1C Goals in Adults: Recommendations A reasonable A1C goal for many nonpregnant adults is <7% (53 mmol/mol). A Providers might reasonably suggest more stringent A1C goals (such as <6.5%) for select individual patients if this can be achieved without significant hypoglycemia or other adverse effects of treatment (i.e., polypharmacy). Appropriate patients might include those with short duration of diabetes, type 2 diabetes treated with lifestyle or metformin only, long life expectancy, or no significant cardiovascular disease. C Glycemic Targets: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S55-S64
40 A1C Goals in Adults: Recommendations (2) Less stringent goals (such as <8% [64 mmol/mol]) may be appropriate for patients with a history of severe hypoglycemia, limited life expectancy, advanced microvascular or macrovascular complications, or longstanding diabetes in whom the goal is difficult to achieve despite diabetes self-management education, appropriate glucose monitoring, and effective doses of multiple glucose-lowering agents including insulin. B Glycemic Targets: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S55-S64

41 Summary of Glycemic Recommendations Glycemic Targets: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S55-S64
42 9. Cardiovascular Disease and Risk Management
43 Cardiovascular Disease ASCVD is the leading cause of morbidity & mortality for those with diabetes. Largest contributor to direct/indirect costs Common conditions coexisting with type 2 diabetes (e.g., hypertension, dyslipidemia) are clear risk factors for ASCVD. Diabetes itself confers independent risk Control individual cardiovascular risk factors to prevent/slow CVD in people with diabetes. Systematically assess all patients with diabetes for cardiovascular risk factors. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S86-S104
44 Hypertension/BP Control: Recommendations Screening and Diagnosis: Blood pressure (BP) should be measured at every routine clinical visit. Patients found to have elevated BP( 140/90) should have BP confirmed using multiple readings, including measurements on a separate day, to diagnose hypertension. B All hypertensive patients with diabetes should monitor their BP at home. B Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S86-S104
45 Hypertension/BP Control: Recommendations (2) Treatment Goals Most people with diabetes and hypertension should be treated to a systolic BP goal of <140 mmhg and a diastolic BP goal of <90 mmhg. A Lower systolic and diastolic BP targets, such as 130/80 mmhg, may be appropriate for individuals at high risk of CVD, if they can be achieved without undue treatment burden. C In pregnant patients with diabetes and preexisting hypertension who are treated with antihypertensive therapy, BP targets of / mmhg are suggested in the interest of optimizing long-term maternal health and minimizing impaired fetal growth. E Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S86-S104
46 Hypertension/BP Control: Recommendations (4) Pharmacologic Interventions Patients with confirmed office-based blood pressure 140/90 mmhg should, in addition to lifestyle therapy, have prompt initiation and timely titration of pharmacologic therapy to achieve BP goals. A Patients with confirmed office-based blood pressure 160/100 mmhg should, in addition to lifestyle therapy, have prompt initiation and timely titration of two drugs or a single-pill combination of drugs demonstrated to reduce CV events in patients with diabetes. A Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S86-S104
47 Hypertension/BP Control: Recommendations (5) Pharmacologic Interventions Treatment for hypertension should include drug classes demonstrated to reduce CV events in patients with diabetes: A ACE Inhibitors Angiotensin receptor blockers (ARBs) Thiazide-like diuretics Dihydropyridine calcium channel blockers Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S86-S104
48 Hypertension/BP Control: Recommendations (7) Pharmacologic Interventions An ACE inhibitor or ARB, at the maximumly tolerated dose indicated for BP treatment, is the recommended first-line treatment for hypertension in patients with diabetes and urinary albumin-to-creatinine ratio 300 mg/g creatinine A or mg/g creatinine B. If one class is not tolerated, the other should be substituted. B For patients treated with an ACE inhibitor, ARB, or diuretic, serum creatinine/estimated glomerular filtrated rate and serum potassium levels should be monitored at least annually. B Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S86-S104
49 Lipid Management: Recommendations (2) Ongoing Therapy and Monitoring with Lipid Panel In adults not taking statins or other lipid-lowering therapy, it is reasonable to obtain a lipid profile at the time of diabetes diagnosis, at an initial medical evaluation, and every 5 years thereafter if under the age of 40 years, or more frequently if indicated. E Obtain a lipid profile at initiation of statins or other lipidlowering therapy, 4-12 weeks after initiation or a change in dose, and annually thereafter as it may help to monitor the response to therapy and inform adherence. E Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S86-S104
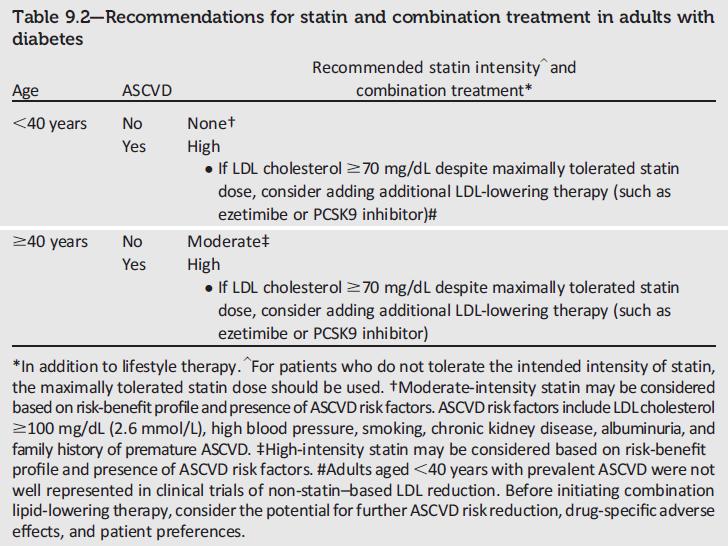
50 Question All adults with diabetes should be on a statin A. Yes B. No Answer: B- no. Adults over 40 with at least one risk factor for ASCVD should be on statins, or those with ASCVD
51

52 High- and Moderate-Intensity Statin Therapy Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S86-S104
53 Antiplatelet Agents: Recommendations (2) Aspirin therapy ( mg/day) may be considered as a primary prevention strategy in those with type 1 or type 2 diabetes who are at increased CV risk. This includes most men and women with diabetes aged 50 years who have at least one additional major risk factor (family history of premature ASCVD, hypertension, dyslipidemia, smoking, or albuminuria) and are not at increased risk of bleeding. A Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S86-S104
54 10. Microvascular Complications and Foot Care
55 Diabetic Kidney Disease (DKD): Recommendations Screening At least once a year, assess urinary albumin (e.g., spot urinary albumin-to-creatinine ratio) and estimated glomerular filtration rate (egfr): In patients with type 1 diabetes with duration of 5 years B In all patients with type 2 diabetes B In all patients with comorbid hypertension B Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S105-S118
56 Diabetic Kidney Disease (DKD): Recommendations (2) Treatment Optimize glucose control to reduce the risk or slow progression of DKD. A Optimize blood pressure control to reduce the risk or slow progression of DKD. A For people with nondialysis-dependent DKD, dietary protein intake should be ~0.8 g/kg body weight per day (the recommended daily allowance). For patients on dialysis, higher levels of dietary protein intake should be considered. B Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S105-S118
57 Diabetic Kidney Disease (DKD): Recommendations (3) Treatment In nonpregnant patients with diabetes and hypertension, either an ACE inhibitor or ARB is recommended for those with modestly elevated urinary albumin-to-creatinine ratio (UACR) ( mg/g creatinine) B and is strongly recommended for those with UACR 300 mg/g creatinine and/or egfr <60 ml/min/1.73m 2. A Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S105-S118
58 Diabetic Kidney Disease (DKD): Recommendations (4) Treatment Periodically monitor serum creatinine and potassium levels for the development of increased creatinine or changes in potassium when ACE inhibitors, ARBs, or diuretics are used. B Continued monitoring of UACR in patients with albuminuria treated with an ACE inhibitor or ARB is reasonable to assess the response to treatment and progression of DKD. E Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S105-S118
59 Diabetic Retinopathy: Recommendations To reduce the risk or slow the progression of diabetic retinopathy: Optimize glycemic control. A Optimize blood pressure and serum lipid control. A Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S105-S118
60 Diabetic Retinopathy: Recommendations (2) Screening: Initial dilated and comprehensive eye examination by an ophthalmologist or optometrist: Adults with type 1 diabetes, within 5 years of diabetes onset. B Patients with type 2 diabetes at the time of diabetes diagnosis. B Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S105-S118
61 Neuropathy: Overview Early recognition and management is important because: 1. Diabetic neuropathy (DN) is a diagnosis of exclusion. 2. Numerous treatment options exist. 3. Up to 50% of diabetic peripheral neuropathy (DPN) may be asymptomatic. 4. Recognition & treatment may improve symptoms, reduce sequelae, and improve quality of life. Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S105-S118
62 Screening: Neuropathy: Recommendations All patients should be assessed for DPN starting at diagnosis for T2DM and 5 years after diagnosis of T1DM and at least annually thereafter. B Assessment for distal symmetric polyneuropathy should include a careful history and assessment of either temperature or pinprick sensation (smallfiber function) and vibration sensation using a 128-Hz tuning fork (for large-fiber function). All patients should have annual 10-g monofilament testing to identify feet at risk for ulceration and amputation. B Symptoms and signs of autonomic neuropathy should be assessed in patients with microvascular complications. E Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S105-S118
63 Neuropathy: Recommendations (2) Treatment: Optimize glucose control to prevent or delay the development of neuropathy in patients with T1DM A and to slow the progression in patients with T2DM. B Assess and treat patients to reduce pain related to DPN B and symptoms of autonomic neuropathy and to improve quality of life. E Either pregabalin or duloxetine are recommended as initial pharmacologic treatments for neuropathic pain in diabetes. A Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S105-S118
64 11. Older Adults
65 Older Adults 26% of patients >65 years of age have diabetes. Older adults have higher rates of premature death, functional disability & coexisting illnesses. At greater risk for polypharmacy, cognitive impairment, urinary incontinence, injurious falls & persistent pain. Screening for complications should be individualized and periodically revisited. At higher risk for depression. Older Adults: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S119-S125
66 Older Adults: Recommendations Consider the assessment of medical, psychological, functional, and social geriatric domains in older adults to provide a framework to determine targets and therapeutic approaches for diabetes management. C Screening for geriatric syndromes may be appropriate in older adults experiencing limitations in their basic and instrumental activities of daily living as they may affect diabetes self-management and be related to health-related quality of life. C Older Adults: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S119-S125
67 Older Adults: Recommendations (4) Treatment Goals: Older adults who are otherwise healthy with few coexisting chronic illnesses and intact cognitive function and functional status should have lower glycemic goals (A1C <7.5%), while those with multiple coexisting chronic illnesses, cognitive impairment, or functional dependence should have less stringent glycemic goals (A1C < %). C Glycemic goals for some older adults might reasonably be relaxed as part of individualized care, but hyperglycemia leading to symptoms or risk of acute hyperglycemic complications should be avoided in all patients. C Older Adults: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S119-S125
68 Older Adults: Recommendations (5) Treatment Goals: Screening for diabetes complications should be individualized in older adults. Particular attention should be paid to complications that would lead to functional impairment. C Treatment of hypertension to individualized target levels is indicated in most older adults. C Older Adults: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S119-S125
69 Older Adults: Recommendations (6) Treatment Goals: Treatment of other CV risk factors should be individualized in older adults considering the time frame of benefit. Lipid-lowering therapy and aspirin therapy may benefit those with life expectancies at least equal to the time frame of primary prevention or secondary intervention trials. E Older Adults: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S119-S125
70 Older Adults: Recommendations (7) Pharmacologic Therapy: In older adults at increased risk of hypoglycemia, medication classes with low risk of hypoglycemia are preferred. B Overtreatment of diabetes is common in older adults and should be avoided. B Deintensification (or simplification) of complex regimens is recommended to reduce the risk of hypoglycemia, if it can be achieved within the individualized A1C target. B Older Adults: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S119-S125
71 Older Adults: Recommendations (8) Treatment in Skilled Nursing Facilities and Nursing Homes: Consider diabetes education for the staff of long-term care facilities to improve the management of older adults with diabetes. E Patients with diabetes residing in long-term care facilities need careful assessment to establish glycemic goals and to make appropriate choices of glucose-lowering agents based on their clinical and functional status. E Older Adults: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S119-S125
72 14. Diabetes Care in the Hospital
73 Diabetes Care in the Hospital: Recommendations Perform an A1C on all patients with diabetes or hyperglycemia (blood glucose >140 mg/dl) admitted to the hospital if not performed in the prior 3 months. B Insulin should be administered using validated written or computerized protocols that allow for predefined adjustments in the insulin dosage based on glycemic fluctuations. E Diabetes Care in the Hospital: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S144-S151
74 Diabetes Care in the Hospital: Recommendations (2) Glycemic Targets: Insulin therapy should be initiated for treatment of persistent hyperglycemia starting at a threshold 180 mg/dl. Once insulin therapy is started, a target glucose range of mg/dl is recommended for the majority of critically ill patients and noncritically ill patients. A More stringent goals, such as mg/dl, may be appropriate for selected patients, if this can be achieved without significant hypoglycemia. C Diabetes Care in the Hospital: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S144-S151
75 Diabetes Care in the Hospital: Recommendations (3) Antihyperglycemic Agent Use: A basal bolus correction insulin regimen, with the addition of nutritional insulin in patients who have good nutritional intake, is the preferred treatment for noncritically ill patients. A Sole use of sliding scale insulin the inpatient hospital setting is strongly discouraged. A Diabetes Care in the Hospital: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S144-S151
76 Diabetes Care in the Hospital: Recommendations (4) Hypoglycemia: A hypoglycemia management protocol should be adopted and implemented by each hospital or hospital system. A plan for preventing and treating hypoglycemia should be established for each patient. Episodes of hypoglycemia in the hospital should be documented in the medical record and tracked. E The treatment regimen should be reviewed and changed as necessary to prevent further hypoglycemia when a blood glucose value is 70 mg/dl (3.9 mmol/l). C Diabetes Care in the Hospital: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S144-S151
Standards of Medical Care In Diabetes
 Standards of Medical Care In Diabetes - 2017 Robert E. Ratner, MD, FACP, FACE Professor of Medicine Georgetown University School of Medicine Disclosed no conflict of interest Standards of Care Professional.diabetes.org/SOC
Standards of Medical Care In Diabetes - 2017 Robert E. Ratner, MD, FACP, FACE Professor of Medicine Georgetown University School of Medicine Disclosed no conflict of interest Standards of Care Professional.diabetes.org/SOC
Standards of Medical Care in Diabetes 2016
 Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
What s New in the Standards of Medical Care in Diabetes? Dr. Jason Kruse, DO Broadlawns Medical Center
 What s New in the Standards of Medical Care in Diabetes? Dr. Jason Kruse, DO Broadlawns Medical Center Learning Objectives By the end of this presentation, participants should be able to: Discuss updates
What s New in the Standards of Medical Care in Diabetes? Dr. Jason Kruse, DO Broadlawns Medical Center Learning Objectives By the end of this presentation, participants should be able to: Discuss updates
STATE OF THE STATE: TYPE II DIABETES
 STATE OF THE STATE: TYPE II DIABETES HENRY DRISCOLL, MD, CHIEF of ENDOCRINOLOGY MARSHALL U, CHERTOW DIABETES CENTER, HUNTINGTON VAMC HEATHER VENOY, RD, LD, CDE DIETITIAN, DIABETES EDUCATOR, CHERTOW DIABETES
STATE OF THE STATE: TYPE II DIABETES HENRY DRISCOLL, MD, CHIEF of ENDOCRINOLOGY MARSHALL U, CHERTOW DIABETES CENTER, HUNTINGTON VAMC HEATHER VENOY, RD, LD, CDE DIETITIAN, DIABETES EDUCATOR, CHERTOW DIABETES
Modified version focused on CCNC Quality Measures and Feedback Processes
 Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Diabetes Review Chris Paras, D.O. Assistant Prof of Medicine, NYIT & Touro COM Designated Institutional Official & Assoc. Clinical Dean, Brookdale
 Diabetes Review Chris Paras, D.O. Assistant Prof of Medicine, NYIT & Touro COM Designated Institutional Official & Assoc. Clinical Dean, Brookdale University Hospital Diabetes Care 2018 Jan; 41 Objectives
Diabetes Review Chris Paras, D.O. Assistant Prof of Medicine, NYIT & Touro COM Designated Institutional Official & Assoc. Clinical Dean, Brookdale University Hospital Diabetes Care 2018 Jan; 41 Objectives
Executive Summary: Standards of Medical Care in Diabetes 2010
 E X E C U T I V E S U M M A R Y Executive Summary: Standards of Medical Care in Diabetes 2010 Current criteria for the diagnosis of diabetes A1C 6.5%: The test should be performed in a laboratory using
E X E C U T I V E S U M M A R Y Executive Summary: Standards of Medical Care in Diabetes 2010 Current criteria for the diagnosis of diabetes A1C 6.5%: The test should be performed in a laboratory using
American Diabetes Association: Standards of Medical Care in Diabetes 2015
 American Diabetes Association: Standards of Medical Care in Diabetes 2015 Synopsis of ADA standards relevant to the 11 th Scope of Work under Task B.2 ASSESSMENT OF GLYCEMIC CONTROL Recommendations: Perform
American Diabetes Association: Standards of Medical Care in Diabetes 2015 Synopsis of ADA standards relevant to the 11 th Scope of Work under Task B.2 ASSESSMENT OF GLYCEMIC CONTROL Recommendations: Perform
DIABETES MEASURES GROUP OVERVIEW
 2014 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN DIABETES MEASURES GROUP: #1. Diabetes: Hemoglobin A1c Poor Control #2. Diabetes: Low Density Lipoprotein (LDL-C)
2014 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN DIABETES MEASURES GROUP: #1. Diabetes: Hemoglobin A1c Poor Control #2. Diabetes: Low Density Lipoprotein (LDL-C)
Clinical Practice Guidelines for Diabetes Management
 Clinical Practice Guidelines for Diabetes Management Diabetes is a disease in which blood glucose levels are above normal. Over the years, high blood glucose damages nerves and blood vessels, which can
Clinical Practice Guidelines for Diabetes Management Diabetes is a disease in which blood glucose levels are above normal. Over the years, high blood glucose damages nerves and blood vessels, which can
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications
 American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
Standards of Medical Care in Diabetes
 Standards of Medical Care in Diabetes - 2018 1. Improving Care and Promoting Health in Populations Diabetes and Population Health: Recommendations Ensure treatment decisions are timely, rely on evidence-based
Standards of Medical Care in Diabetes - 2018 1. Improving Care and Promoting Health in Populations Diabetes and Population Health: Recommendations Ensure treatment decisions are timely, rely on evidence-based
An Update on the Standards of Medical Care in Diabetes 2017, With an Eye Toward 2018
 An Update on the Standards of Medical Care in Diabetes 2017, With an Eye Toward 2018 Erika Gebel Berg, PhD Director, Scientific and Medical Affairs Corresponding Author, ADA s Standards of Medical in Diabetes
An Update on the Standards of Medical Care in Diabetes 2017, With an Eye Toward 2018 Erika Gebel Berg, PhD Director, Scientific and Medical Affairs Corresponding Author, ADA s Standards of Medical in Diabetes
2019 Standards of Medical Care in Diabetes: What is New and Why
 2019 Standards of Medical Care in Diabetes: What is New and Why Jane E.B. Reusch, MD ADA President of Medicine & Science Professor of Medicine, Division of Endocrinology, Metabolism and Diabetes and Associate
2019 Standards of Medical Care in Diabetes: What is New and Why Jane E.B. Reusch, MD ADA President of Medicine & Science Professor of Medicine, Division of Endocrinology, Metabolism and Diabetes and Associate
Standards of Care in Diabetes What's New? Veronica Brady, FNP-BC, PhD, BC-ADM,CDE Karmella Thomas, RD, LD,CDE
 Standards of Care in Diabetes 2016-- What's New? Veronica Brady, FNP-BC, PhD, BC-ADM,CDE Karmella Thomas, RD, LD,CDE Terminology No longer using the term diabetic. Diabetes does not define people. People
Standards of Care in Diabetes 2016-- What's New? Veronica Brady, FNP-BC, PhD, BC-ADM,CDE Karmella Thomas, RD, LD,CDE Terminology No longer using the term diabetic. Diabetes does not define people. People
Diabetes Summary of Medical Guidelines
 Diabetes Summary of Medical Guidelines Key concepts in setting glycemic controls: goals should be individualized; certain populations (children, pregnant women, and elderly) require special considerations;
Diabetes Summary of Medical Guidelines Key concepts in setting glycemic controls: goals should be individualized; certain populations (children, pregnant women, and elderly) require special considerations;
Diabetes Mellitus: Evaluation and Care Management
 Diabetes Mellitus: Evaluation and Care Management Michael King, MD Assistant Professor Residency Program Director University of Kentucky Dept. of Family & Community Medicine Learning Objectives 1. Review
Diabetes Mellitus: Evaluation and Care Management Michael King, MD Assistant Professor Residency Program Director University of Kentucky Dept. of Family & Community Medicine Learning Objectives 1. Review
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
STANDARDS OF MEDICAL CARE IN DIABETES 2014
 STANDARDS OF MEDICAL CARE IN DIABETES 2014 I. CLASSIFICATION AND DIAGNOSIS Classification of Diabetes Type 1 diabetes β-cell destruction Type 2 diabetes Progressive insulin secretory defect Other specific
STANDARDS OF MEDICAL CARE IN DIABETES 2014 I. CLASSIFICATION AND DIAGNOSIS Classification of Diabetes Type 1 diabetes β-cell destruction Type 2 diabetes Progressive insulin secretory defect Other specific
Executive Summary: Standards of Medical Care in Diabetes 2009
 Executive Summary Executive Summary: Standards of Medical Care in Diabetes 2009 Current Criteria for the Diagnosis of Diabetes Fasting plasma glucose (FPG) 126 mg/dl (7.0 mmol/l). Fasting is defined as
Executive Summary Executive Summary: Standards of Medical Care in Diabetes 2009 Current Criteria for the Diagnosis of Diabetes Fasting plasma glucose (FPG) 126 mg/dl (7.0 mmol/l). Fasting is defined as
Diabetic Retinopathy and Neuropathy: 2018 Clinical Practice Guidelines
 Diabetic Retinopathy and Neuropathy: 2018 Clinical Practice Guidelines Richard Arakaki, M.D. Phoenix Area Diabetes Consultant August 9 th 2018 Disclose no conflict of interest Complications and Co-morbidities
Diabetic Retinopathy and Neuropathy: 2018 Clinical Practice Guidelines Richard Arakaki, M.D. Phoenix Area Diabetes Consultant August 9 th 2018 Disclose no conflict of interest Complications and Co-morbidities
Clinical Practice Guideline Key Points
 Clinical Practice Guideline Key Points Clinical Practice Guideline 2008 Key Points Diabetes Mellitus Provided by: Highmark Endocrinology Clinical Quality Improvement Committee In accordance with Highmark
Clinical Practice Guideline Key Points Clinical Practice Guideline 2008 Key Points Diabetes Mellitus Provided by: Highmark Endocrinology Clinical Quality Improvement Committee In accordance with Highmark
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Update on Diabetes Standards-What Community Physicians Should Know. Kevin Miller D.O.
 Update on Diabetes Standards-What Community Physicians Should Know. Kevin Miller D.O. Know The ABC Targets A1C BP LDL Cholesterol AACE Recommendations for A1C Testing A1C levels may be misleading in several
Update on Diabetes Standards-What Community Physicians Should Know. Kevin Miller D.O. Know The ABC Targets A1C BP LDL Cholesterol AACE Recommendations for A1C Testing A1C levels may be misleading in several
Diabetes Complications Guideline Based Screening, Management, and Referral
 Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care
: Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care") Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
The American Diabetes
 Standards of Medical Care in Diabetes 2016 Abridged for Primary Care Providers American Diabetes Association This is an abridged version of the American Diabetes Association Position Statement: Standards
Standards of Medical Care in Diabetes 2016 Abridged for Primary Care Providers American Diabetes Association This is an abridged version of the American Diabetes Association Position Statement: Standards
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process
 MEASURE TYPE: Process") Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Management of Chronic Conditions 2019 COLLECTION
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Management of Chronic Conditions 2019 COLLECTION
9/28/2012. Sponsored By: NDSU College of Pharmacy, Nursing and Allied Sciences
 Sponsored By: NDSU College of Pharmacy, Nursing and Allied Sciences By PresenterMedia.com Faculty: Wendy Brown Pharm.D, PA-C, AE-C Associate Professor Pharmacy Practice About the Patient Clinical Coordinator
Sponsored By: NDSU College of Pharmacy, Nursing and Allied Sciences By PresenterMedia.com Faculty: Wendy Brown Pharm.D, PA-C, AE-C Associate Professor Pharmacy Practice About the Patient Clinical Coordinator
UPDATED APRIL 26, 2018 This slide deck contains content created, reviewed, and approved by the American Diabetes Association. You are free to use the
 UPDATED APRIL 26, 2018 This slide deck contains content created, reviewed, and approved by the American Diabetes Association. You are free to use the slides in presentations without further permission
UPDATED APRIL 26, 2018 This slide deck contains content created, reviewed, and approved by the American Diabetes Association. You are free to use the slides in presentations without further permission
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Standards of Medical Care in Diabetes 2019 Abridged for Primary Care Providers
 Standards of Medical Care in Diabetes 2019 Abridged for Primary Care Providers American Diabetes Association This is an abridged version of the American Diabetes Association s Standards of Medical Care
Standards of Medical Care in Diabetes 2019 Abridged for Primary Care Providers American Diabetes Association This is an abridged version of the American Diabetes Association s Standards of Medical Care
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES
 RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
Standards of Medical Care for Patients With Diabetes Mellitus
 Standards of Medical Care for Patients With Diabetes Mellitus American Diabetes Association Originally approved 1988. Most recent review/revision, October 2002. Abridged from Diabetes Care 26 (Suppl. 1):S33
Standards of Medical Care for Patients With Diabetes Mellitus American Diabetes Association Originally approved 1988. Most recent review/revision, October 2002. Abridged from Diabetes Care 26 (Suppl. 1):S33
Key Elements in Managing Diabetes
 Key Elements in Managing Diabetes Presentor Disclosure No conflicts of interest to disclose Presented by Susan Cotey, RN, CDE Lennon Diabetes Center Stephanie Tubbs Jones Health Center Cleveland Clinic
Key Elements in Managing Diabetes Presentor Disclosure No conflicts of interest to disclose Presented by Susan Cotey, RN, CDE Lennon Diabetes Center Stephanie Tubbs Jones Health Center Cleveland Clinic
Treating the elderly patients with type 2 diabetes mellitus
 Treating the elderly patients with type 2 diabetes mellitus Niki Katsiki MSc, PhD, MD, FRSPH IASO/EASO Scope Member EASD Diabetes & Cardiovascular Disease Group Member Member of the Executive Board of
Treating the elderly patients with type 2 diabetes mellitus Niki Katsiki MSc, PhD, MD, FRSPH IASO/EASO Scope Member EASD Diabetes & Cardiovascular Disease Group Member Member of the Executive Board of
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
The American Diabetes
 Standards of Medical Care in Diabetes 2015 Abridged for Primary Care Providers American Diabetes Association This is an abridged version of the American Diabetes Association Position Statement: Standards
Standards of Medical Care in Diabetes 2015 Abridged for Primary Care Providers American Diabetes Association This is an abridged version of the American Diabetes Association Position Statement: Standards
Donna Amundson, RN, BSN, CDE Director of the Sanford Diabetes Center Bismarck, ND
 Donna Amundson, RN, BSN, CDE Director of the Sanford Diabetes Center Bismarck, ND Discuss the core principles of quality management for diabetes care and education Identify the 6 core elements of the Chronic
Donna Amundson, RN, BSN, CDE Director of the Sanford Diabetes Center Bismarck, ND Discuss the core principles of quality management for diabetes care and education Identify the 6 core elements of the Chronic
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Indiana Medicaid Drug Utilization Review Board Newsletter
 Indiana Medicaid Drug Utilization Review Board Newsletter Volume 12 Issue 4 October 2009 Indiana Medicaid DUR Board Room W382 Indiana State Government Center, South 402 West Washington Street Indianapolis,
Indiana Medicaid Drug Utilization Review Board Newsletter Volume 12 Issue 4 October 2009 Indiana Medicaid DUR Board Room W382 Indiana State Government Center, South 402 West Washington Street Indianapolis,
Diabetes Updates. Disclosures
 Diabetes Updates Dr. Thanh D. Hoang, DO, FACP, FACE Walter Reed National Military Medical Center Associate Professor of Medicine Uniformed Services University of the Health Sciences March 2018 Disclosures
Diabetes Updates Dr. Thanh D. Hoang, DO, FACP, FACE Walter Reed National Military Medical Center Associate Professor of Medicine Uniformed Services University of the Health Sciences March 2018 Disclosures
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND CLASSIFICATION OF DIABETES
 Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND CLASSIFICATION OF DIABETES Objectives u At conclusion of the lecture the participant will be able to: 1. Differentiate between the classifications of diabetes
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND CLASSIFICATION OF DIABETES Objectives u At conclusion of the lecture the participant will be able to: 1. Differentiate between the classifications of diabetes
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D.
 Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
2018 Standard of Medical Care Diabetes and Pregnancy
 2018 Standard of Medical Care Diabetes and Pregnancy 2018 Standard of Medical Care Diabetes and Pregnancy Marjorie Cypress does not have any relevant financial relationships with any commercial interests
2018 Standard of Medical Care Diabetes and Pregnancy 2018 Standard of Medical Care Diabetes and Pregnancy Marjorie Cypress does not have any relevant financial relationships with any commercial interests
Diabetes is a chronic illness that requires
 P O S I T I O N S T A T E M E N T Standards of Medical Care for Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION Diabetes is a chronic illness that requires continuing medical care and patient
P O S I T I O N S T A T E M E N T Standards of Medical Care for Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION Diabetes is a chronic illness that requires continuing medical care and patient
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Diabetes is a chronic illness that
 Standards of Medical Care for Patients With Diabetes Mellitus Originally approved 1988. Most recent review/revision, October 2001 Abridged from Diabetes Care 25:213 229, 2002. Full text of this position
Standards of Medical Care for Patients With Diabetes Mellitus Originally approved 1988. Most recent review/revision, October 2001 Abridged from Diabetes Care 25:213 229, 2002. Full text of this position
Guideline for Management of Type 2 Diabetes Mellitus: Kingdome of Bahrain Ministry of Health 2016
 Guideline for Management of Type 2 Diabetes Mellitus: Kingdome of Bahrain Ministry of Health 2016 1. Screening and diagnosis: Detection type 2 Diabetes are usually based on a two-step approach: Step 1:
Guideline for Management of Type 2 Diabetes Mellitus: Kingdome of Bahrain Ministry of Health 2016 1. Screening and diagnosis: Detection type 2 Diabetes are usually based on a two-step approach: Step 1:
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
Energy balance. Changing rate of energy expenditure
 Energy balance Changing rate of energy expenditure 2 Physical activity and exercise Physical activity Occupational activity Physical Activity Exercise (business, work) Leisure activity (Recreational activities,
Energy balance Changing rate of energy expenditure 2 Physical activity and exercise Physical activity Occupational activity Physical Activity Exercise (business, work) Leisure activity (Recreational activities,
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Dr Aftab Ahmad Consultant Diabetologist at Royal Liverpool University Hospital Regional Diabetes Network Lead
 Dr Aftab Ahmad Consultant Diabetologist at Royal Liverpool University Hospital Regional Diabetes Network Lead Today s Presentation HbA1c & diagnosing Diabetes What is Impaired Glucose & IGR? Implications
Dr Aftab Ahmad Consultant Diabetologist at Royal Liverpool University Hospital Regional Diabetes Network Lead Today s Presentation HbA1c & diagnosing Diabetes What is Impaired Glucose & IGR? Implications
STANDARDS OF MEDICAL CARE IN DIABETES 2012
 STANDARDS OF MEDICAL CARE IN DIABETES 2012 Section Table of Contents ADA Evidence Grading System of Clinical Recommendations Slide No. I. Classification and Diagnosis 4-11 II. Testing for Diabetes in Asymptomatic
STANDARDS OF MEDICAL CARE IN DIABETES 2012 Section Table of Contents ADA Evidence Grading System of Clinical Recommendations Slide No. I. Classification and Diagnosis 4-11 II. Testing for Diabetes in Asymptomatic
Microvascular Complications
 Comprehensive education course for Asian diabetes educators Microvascular Complications Keimyung University Dongsan Medical Center Mi Kyung Kim Conflict of interest disclosure None Committee of Scientific
Comprehensive education course for Asian diabetes educators Microvascular Complications Keimyung University Dongsan Medical Center Mi Kyung Kim Conflict of interest disclosure None Committee of Scientific
Chapter 37: Exercise Prescription in Patients with Diabetes
 Chapter 37: Exercise Prescription in Patients with Diabetes American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York:
Chapter 37: Exercise Prescription in Patients with Diabetes American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York:
National Strategy. for Control and Prevention of Non - communicable Diseases in Kingdom of Bahrain
 Kingdom of Bahrain Ministry of Health National Strategy for Control and Prevention of Non - communicable Diseases in Kingdom of Bahrain 2014 2025 Behavioural Risk Factors Tobacco Use Unhealthy Diets Physical
Kingdom of Bahrain Ministry of Health National Strategy for Control and Prevention of Non - communicable Diseases in Kingdom of Bahrain 2014 2025 Behavioural Risk Factors Tobacco Use Unhealthy Diets Physical
Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic
 Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic Sanford Center for Aging 775-784-4744 med.unr.edu/aging Diabetes Management Series: From Selfmanagement
Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic Sanford Center for Aging 775-784-4744 med.unr.edu/aging Diabetes Management Series: From Selfmanagement
Diabetes Mellitus in Older Adults. Presenter Disclosure Information
 Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
ILSI NA - Canadian Diabetes Association Workshop on Carbohydrate Quality
 ILSI NA - Canadian Diabetes Association Workshop on Carbohydrate Quality Sacha Uelmen, RDN, CDE Director, Nutrition American Diabetes Association Arlington, VA Presentation Title 1 Discussion Points Review
ILSI NA - Canadian Diabetes Association Workshop on Carbohydrate Quality Sacha Uelmen, RDN, CDE Director, Nutrition American Diabetes Association Arlington, VA Presentation Title 1 Discussion Points Review
Exercise in Diabetes Mellitus. Pranisa Luengratsameerung,MD
 Exercise in Diabetes Mellitus By Pranisa Luengratsameerung,MD What is the Diabetes Mellitus? action Insulin Defect release Abnormal glucose metabolism Symptoms Polyuria (frequent urination) Polyphasia
Exercise in Diabetes Mellitus By Pranisa Luengratsameerung,MD What is the Diabetes Mellitus? action Insulin Defect release Abnormal glucose metabolism Symptoms Polyuria (frequent urination) Polyphasia
Understanding the Diabetes Care Process Pfizer Medical Affairs
 Understanding the Diabetes Care Process Pfizer Medical Affairs Overview of Diabetes 1 Diabetes is a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion,
Understanding the Diabetes Care Process Pfizer Medical Affairs Overview of Diabetes 1 Diabetes is a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion,
RCHC Clinical Guidelines Type 2 Diabetes; Adults
 RCHC Clinical Guidelines Type 2 Diabetes; Adults Screening for diabetes in asymptomatic adults 1 Population: Aged > 45 years; Aged < 45 years who are overweight (BMI> 25kg/m 2 ) and have an additional
RCHC Clinical Guidelines Type 2 Diabetes; Adults Screening for diabetes in asymptomatic adults 1 Population: Aged > 45 years; Aged < 45 years who are overweight (BMI> 25kg/m 2 ) and have an additional
Diabetes Update: Diabetes Management In Primary Care. Jonathon M. Firnhaber, MD, FAAFP
 Diabetes Update: Diabetes Management In Primary Care Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Critically evaluate the evidence emerging within diabetes research as it applies to recommendations
Diabetes Update: Diabetes Management In Primary Care Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Critically evaluate the evidence emerging within diabetes research as it applies to recommendations
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND THE OLDER ADULT
 Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND THE OLDER ADULT Objectives u At conclusion of the presentation the participant will: 1. Discuss challenges to glycemic control unique in the older population
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND THE OLDER ADULT Objectives u At conclusion of the presentation the participant will: 1. Discuss challenges to glycemic control unique in the older population
Quick Reference Guide
 2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
Diabetes mellitus is a disease defined by abnormalities of
 AHA/ADA Scientific Statement Primary Prevention of Cardiovascular Diseases in People With Diabetes Mellitus A Scientific Statement From the American Heart Association and the American Diabetes Association
AHA/ADA Scientific Statement Primary Prevention of Cardiovascular Diseases in People With Diabetes Mellitus A Scientific Statement From the American Heart Association and the American Diabetes Association
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
Management of DM in Older Adults: It s not all about sugar! Who needs treatment for DM? Peggy Odegard, Pharm.D., BCPS, CDE
 Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Physical Activity/Exercise Prescription with Diabetes
 Physical Activity/Exercise Prescription with Diabetes B R AD H I NTERMEYER C E P A C SM S A NFORD H E ALTH C A RDIAC R E H AB A N D D I ABE TES E XE RCISE The adoption and maintenance of physical activity
Physical Activity/Exercise Prescription with Diabetes B R AD H I NTERMEYER C E P A C SM S A NFORD H E ALTH C A RDIAC R E H AB A N D D I ABE TES E XE RCISE The adoption and maintenance of physical activity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Hypertension JNC 8 (2014)
") Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
DIABETES MEASURES GROUP OVERVIEW
 2016 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2016 PQRS MEASURES IN DIABETES MEASURES GROUP: #1 Diabetes: Hemoglobin A1c Po Control #110 Preventive Care and Screening: Influenza
2016 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2016 PQRS MEASURES IN DIABETES MEASURES GROUP: #1 Diabetes: Hemoglobin A1c Po Control #110 Preventive Care and Screening: Influenza
Each year, the American Diabetes
 Expanded ABCs of Diabetes Samuel L. Abbate, MD, CDE Each year, the American Diabetes Association (ADA) publishes clinical practice recommendations that include standards of care for patients with diabetes
Expanded ABCs of Diabetes Samuel L. Abbate, MD, CDE Each year, the American Diabetes Association (ADA) publishes clinical practice recommendations that include standards of care for patients with diabetes
Guidelines for Improving the Care of the Older Person with Diabetes Mellitus
 Guidelines for Improving the Care of the Older Person with Diabetes Mellitus California Healthcare Foundation/American Geriatrics Society Panel on Improving Care for Elders with Diabetes This guideline
Guidelines for Improving the Care of the Older Person with Diabetes Mellitus California Healthcare Foundation/American Geriatrics Society Panel on Improving Care for Elders with Diabetes This guideline
2016 Diabetes Practice Guidelines
 2016 Diabetes Practice Guidelines SOURCE(S): 1. American Diabetes Association. Standards of Medical Care in Diabetes 2016. Diabetes Care January 2016 Volume 39, Supplement 1. Diagnosis Diabetes can be
2016 Diabetes Practice Guidelines SOURCE(S): 1. American Diabetes Association. Standards of Medical Care in Diabetes 2016. Diabetes Care January 2016 Volume 39, Supplement 1. Diagnosis Diabetes can be
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Section 1: 1: Trends. Section 2: 2: Comparisons to to Overall Portland Area Area Results for for
 Section 1: 1: Trends 1 Patients in the Diabetes Register 2 Gender of Patients with Diabetes 2 Age of Patients with Diabetes 3 Diabetes Type 3 Duration of Diabetes 4 Weight Control 5 Hemoglobin A1c 6 Blood
Section 1: 1: Trends 1 Patients in the Diabetes Register 2 Gender of Patients with Diabetes 2 Age of Patients with Diabetes 3 Diabetes Type 3 Duration of Diabetes 4 Weight Control 5 Hemoglobin A1c 6 Blood
Finding the sweet spot: Individualized targets for older adults with Type 2 DM
 Finding the sweet spot: Individualized targets for older adults with Type 2 DM Samuel C. Durso, M.D., M.B.A. Mason F. Lord Professor of Medicine Director, Division of Geriatric Medicine and Gerontology
Finding the sweet spot: Individualized targets for older adults with Type 2 DM Samuel C. Durso, M.D., M.B.A. Mason F. Lord Professor of Medicine Director, Division of Geriatric Medicine and Gerontology
8/5/2017. Disclosure to Participants. Learning Outcomes. Terry Compton MS, APRN, CDE. Seniors with Diabetes: Why Are They Different?
 Terry Compton MS, APRN, CDE Diabetes Education Program Manager St. Tammany Parish Hospital Covington, LA Sara (Mandy) Reece PharmD, CDE, BC-ADM, FAADE Diabetes Educator Vice Chair and Associate Professor,
Terry Compton MS, APRN, CDE Diabetes Education Program Manager St. Tammany Parish Hospital Covington, LA Sara (Mandy) Reece PharmD, CDE, BC-ADM, FAADE Diabetes Educator Vice Chair and Associate Professor,
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks
 Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
 Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Measure Owner Designation. AMA-PCPI is the measure owner. NCQA is the measure owner. QIP/CMS is the measure owner. AMA-NCQA is the measure owner
 2011 EHR Measure Specifications The specifications listed in this document have been updated to reflect clinical practice guidelines and applicable health informatics standards that are the most current
2011 EHR Measure Specifications The specifications listed in this document have been updated to reflect clinical practice guidelines and applicable health informatics standards that are the most current
Nutritional Recommendations for the Diabetes Managements
 In the name of God Nutritional for the Diabetes Managements Zohreh Mazloom. PhD Shiraz University of Medical Sciences School of Nutrition and Food Sciences Department of Clinical Nutrition OVERVIEW Healthful
In the name of God Nutritional for the Diabetes Managements Zohreh Mazloom. PhD Shiraz University of Medical Sciences School of Nutrition and Food Sciences Department of Clinical Nutrition OVERVIEW Healthful
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Solomon SD, Uno H, Lewis EF, et al. Erythropoietic response
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Solomon SD, Uno H, Lewis EF, et al. Erythropoietic response
Diabetes in Renal Patients. Contents. Understanding Diabetic Nephropathy
 Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Presenter Disclosure Information
 Prediabetes & Type 2 Diabetes Prevention Cari Ritter, PA-C Presenter Disclosure Information In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Prediabetes & Type 2 Diabetes Prevention Cari Ritter, PA-C Presenter Disclosure Information In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Diabetes in the Elderly 1, 2, 3
 Diabetes in the Elderly 1, 2, 3 WF Mollentze Feb 2010 Diabetes in the elderly differs from diabetes in younger people Prevalence: o Diabetes increases with age affecting approximately 10% of people over
Diabetes in the Elderly 1, 2, 3 WF Mollentze Feb 2010 Diabetes in the elderly differs from diabetes in younger people Prevalence: o Diabetes increases with age affecting approximately 10% of people over
Personal Diabetes Passport
 Personal Diabetes Passport Contact information: Name: Physician: Diabetes Education Centre: Dietitian: Ophthalmologist: Chiropodist: Type of Diabetes: Type 1 (T1DM) Increased risk for diabetes Type 2(T2DM)
Personal Diabetes Passport Contact information: Name: Physician: Diabetes Education Centre: Dietitian: Ophthalmologist: Chiropodist: Type of Diabetes: Type 1 (T1DM) Increased risk for diabetes Type 2(T2DM)
Complications of Diabetes: Screening and Prevention
 Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy