State of the Art Multimodal Monitoring
|
|
|
- Adrian Garrison
- 5 years ago
- Views:
Transcription
1 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD
2 Disclosures I have no financial relationships to disclose with makers of the products here discussed.
3 Outline I Brief Overview ICP monitoring. II Microdialysis III Brief Overview about brain tissue oxygen monitoring P bt O 2 (licox) IV Near Infrared Spectroscopy (NIRS) V Quantitative EEG

4 Monitoring the Brain in Coma Black box No reliable exam Need to determine if the tissue is in crisis
5 Decreased substrate delivery Hypotension - Vasospasm Hypoxia Aggravate hemorrhage or edema Hypertension Cellular toxicity Hyperglycemia Increased metabolism Fever Seizures Secondary Brain Insults
6 Limitations of the GCS & NIHSS Does not directly assess brainstem function Does not evaluate alterations in respiratory pattern Verbal component cannot be tested in comatose or intubated patients Underestimates LOC, especially in dominant hemisphere lesions

7 ICP monitors


8 Monroe-Kellie Doctrine cont d 125 cc 1200 cc cc 50/150 cc Mass Mass


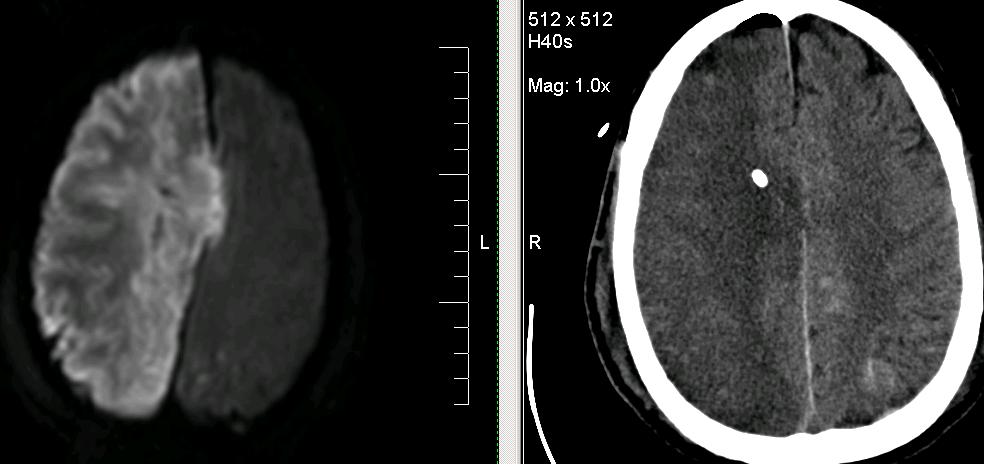
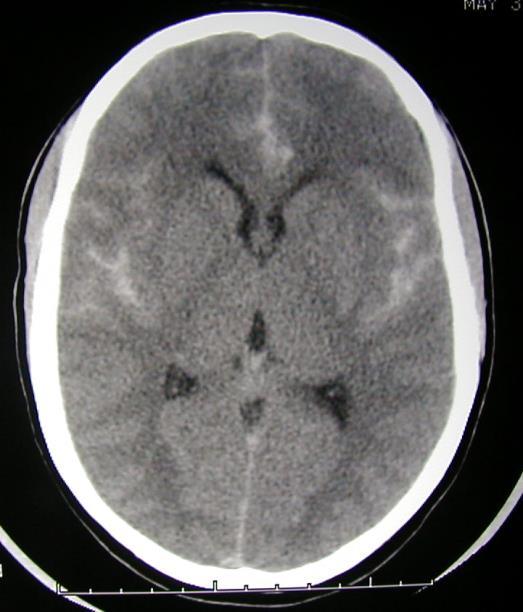
9 Subdural 13 mm Shift Left to right
 indicating uncal herniation.")
10 Patients with a malignant MCA infarction may show ICP values < 20 mm Hg despite marked MLS (> 5 mm), large brain infarctions, and neurological deterioration (pupillary abnormalities) indicating uncal herniation. Consequently, ICP monitoring cannot substitute for strict clinical and neuroradiological follow-up in these patients.
11 BEST-TRIP Trial Multicenter RCT (Chesnut et al) in which 324 patients with severe TBI were randomized to A) ICP/CPP monitoring group and B) Imaging and clinical examination group Primary outcome: composite of survival time, impaired consciousness, and functional status at 3 months and 6 months and neuropsychological status at 6 months
12 Kaplan Meier survival plot
13 BEST-TRIP Trial results Composite score: 56 in the pressure-monitoring group vs. 53 in the imaging-clinical examination group (NS) Six-month mortality was 39% in the pressure-monitoring group and 41% in the imaging-clinical examination group (NS) So is monitoring unnecessary or suboptimal???
14 Hemodynamic Monitoring vs Metabolic Neuronal Monitoring Does Hemodynamic resuscitation improve neuronal metabolic profile? Metabolic crisis (MC) persists despite adequate hemodynamic resuscitation. For every 12 h spent in MC the odds of having a poor outcome is more than doubled. Stein, Neurocritical care 2013
15 Markers of metabolic distress in the brain compartment appears to be distinct from that of the systemic circulation, with traditional hemodynamic and oxygenation goals likely underestimating the requirements of the injured brain. Systemic Resuscitation Cerebral Resuscitation.
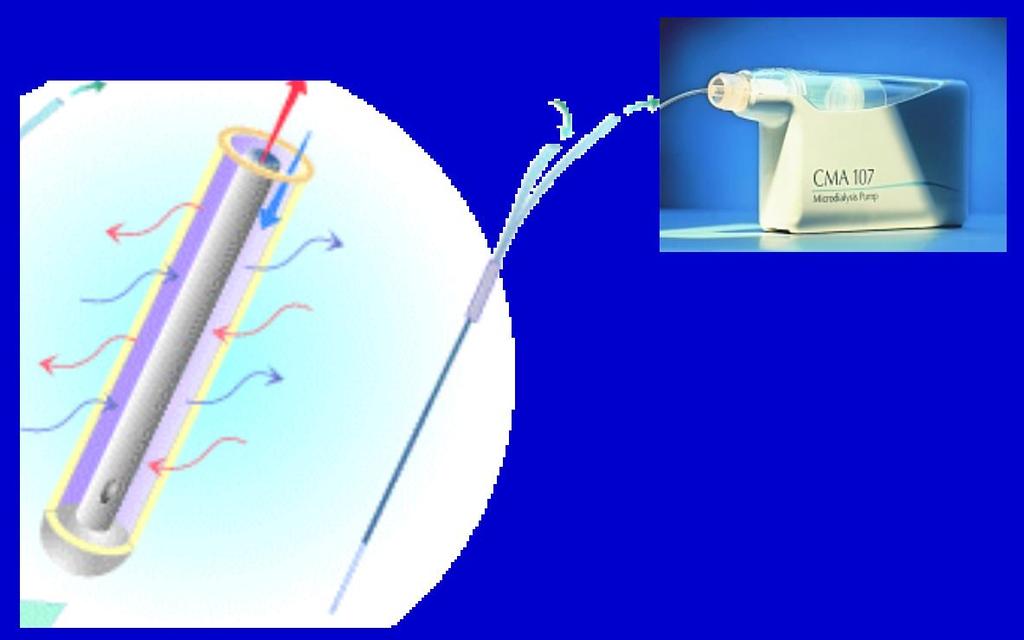
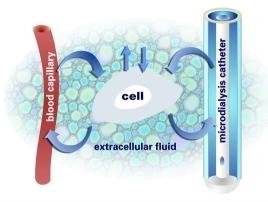



16 Cerebral Microdialysis
17 Normal Values


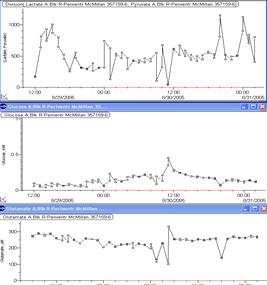
18 LPR Glucose Glutamate




19 LPR Concentration Periodic spikes in glutamate, LPR and EEG seizures Glutamate Post-Injury Hour Lac/Pyr Ratio Post-Injury Hour


20 Brain Tissue Oxygenation Monitoring




21 Rationale for Monitoring Brain Oximetry Fundamental concern about O2 delivery to the brain stems from: Brain is 2% body weight, but consumes 20% of O2 Graham et al autopsy series showing brain ischemia after trauma CMRO2 correlates with outcome The lower it is the worse the outcome Graham DI, J Neurol Neurosurg Psychiatry. 1989

22 How Does It Work? Probe covered by an O 2 permeable membrane O 2 diffuses from brain through membrane Inside probe is an electrolyte solution O 2 changes the charge of the solution Charge is carried through cables to the external Licox computer and displayed
23 Brain Tissue Oximetry Local brain tissue oxygenation + brain temp. 2.5 cm deep to pial surface, PbtO2 in 3 cm radius Location: non-dominant frontal in diffuse TBI, SAH Normal mmhg Risk of Bad clinical outcome: -P bt O 2 < 15mmHg for 30 minutes (critical brain hypoxia) -P bt O 2 < 10mmHg for 10 minutes (severe brain hypoxia) P bt O 2 <5mmHG- High Mortality P bt O 2 <2mmHg-Neuronal Death Bardt T, Acta Neurochirugica 1998 Hoffman WE, Surg Neurol 1996
 The balance between regional oxygen delivery and cellular oxygen consumption 2) Oxygen diffusion rather than total oxygen delivery or cerebral oxygen metabolism 3) Oxygen")
24 What is PbtO2 measuring? 1) The balance between regional oxygen delivery and cellular oxygen consumption 2) Oxygen diffusion rather than total oxygen delivery or cerebral oxygen metabolism 3) Oxygen that accumulates in brain tissue. 1) Oxygenation (pulmonary system) 2) Perfusion (CBF/CPP) (Cardiovascular system) 3) Metabolic state: (fever and seizure)
 (Cardiovascular system) 3) Metabolic state: (fever and seizure) Bohman LE Neurocritical")
25 Medical Management of compromised Brain Oxygen Recordings in SAH 1) Oxygenation (pulmonary system) 2) Perfusion (CBF/CPP) (Cardiovascular system) 3) Metabolic state: (fever and seizure) Bohman LE Neurocritical care 2013

26 Does the use of PtiO2 improve outcome? YES Case controlled prospective study using PtiO2 n = 28 pts with ICP + PtiO2 n = 25 historical control patients with ICP only Stiefel et al JNS p
27 Steifel et al 2005 ICP only ICP + PtiO2

28 Steifel et al 2005 outcome data P < 0.05 good good ICP PtiO2 Patients who died had more frequent PtiO2 < 15 longer durations of PtiO2 < 25
29 Non-invasive Techniques Near infrared spectroscopy Oxygen positron emission tomography Functional MRI
30 Near Infrared Spectroscopy NIRS Found to penetrate tissues 1977 Used for brain oxygenation in 1985 FDA approved 1993 Skull can be penetrated by NIR light with λ of um.


 Estimates Regional brain tissue")
31 NIRS Depth of penetration is proportional to distance between light source and detector max is about 5 cm Typical depth into brain is 1.7 cm Spatial Resolution is about 1 cm x 1.7 column 85% of signal comes from brain, 15% from other tissues (skin, bone) Estimates Regional brain tissue oxygenation Normal: 60-80%, Hypoxia-ischemia <45%, Hyperemia > 80%
32 Use of NIRS Extensive use in CEA Extensive use in cardiac bypass surgery Limited use in Cardiac Arrest Limited use in adult TBI Extensive use in neonatal brain injury
33 NIRS in CEA In CEA, rso2 desat > 12% / <45% is correlated highest risk of stroke with carotid clamping Useful post CEA, 10% increase in cerebral oximetry reading post CEA = 10 fold increase in risk of hyperperfusion syndrome. 1. Murkin JM et al 2007


34 NIRS in Status Epilepticus Pathologic Peaks Giorni et al 2009

35
36 Continuous- Spectral EEG 94 comatose patients with severe TBI and ceeg monitoring: 22% had seizures (52% nonconvulsive): Vespa et al % incidence of seizures in patients with deep ICH; 28% lobar, 26% overall (Vespa et al, 2006) (50/402)12 % of SAH patients had seizures. 100 % were nonconvulsive seizures with a mean duration of 6 hours. (De Marchis et al, 2016) For each hour that a SAH patient spend in nonconvulsive status, there is a deterimental gain equivalent to 2 years for both cognitive and functional outcomes. It no longer acceptable to make the ICU team aware of electrographic seizures many hours after the occurrence.

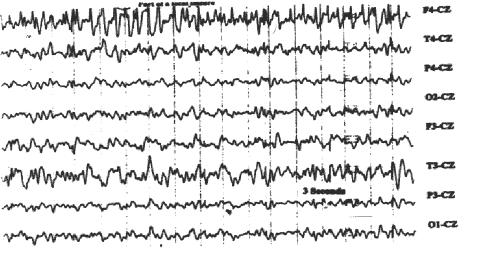
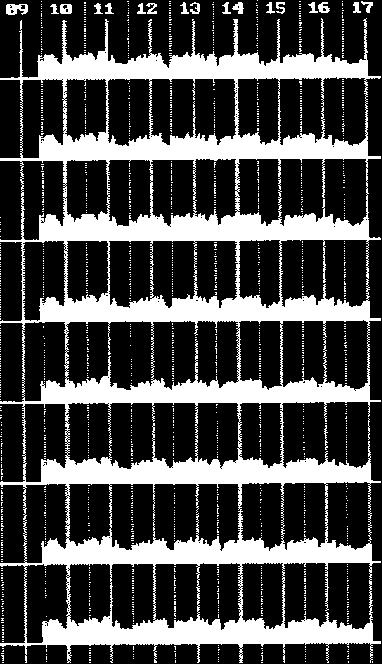
37 0:15 1:30 2:45 4:00 5:15 6:30 7:45 Quantitative EEG detects ischemia by trending changes in fast frequencies 9:00 10:15 11:30 12:45 14:00 15:15 16:30 Percent alpha 17:45 0:15 1:45 3:15 4:45 6:15 7:45 9:15 10:45 12:15 13:45 15:15 16:45 Strong Correlation between percent alpha variability and regional CBF in the acute and chronic strokes (Ingvar et al. 1976, Nuwer 1987 et al) Percent alpha trend (8-13 Hz) Variability of 8 hour trend (PAV) Normal PAV = Peak Trough Peak + Trough Ischemia Vespa et al 1997


38 F4-T4 T4-P4 P4-O2 Hour Left Percent Alpha power is less, and PAV is worse. Left MCA Stroke F3-T3 T3-P3 P3-O1

39 Early Detection of Vasospasm after SAH Vespa et. al J Clin Neurophys 103: Prospective study 19 pts with confirmed vasospasm- simultaneous decrease in PAV. 10/14 had decreased RA variability at least 2 days prior to TCD 4/14 had same-day changes of RA variability and TCD Before i During hour trends After Before During After Series1 Series2 Series3 Series4 Series5 Series6 Series7 Series8 Series9 Series10 Dur i ng Series11 Series12 Series13 Series14 Series15 Series16 Series17 Series18 Series19
40


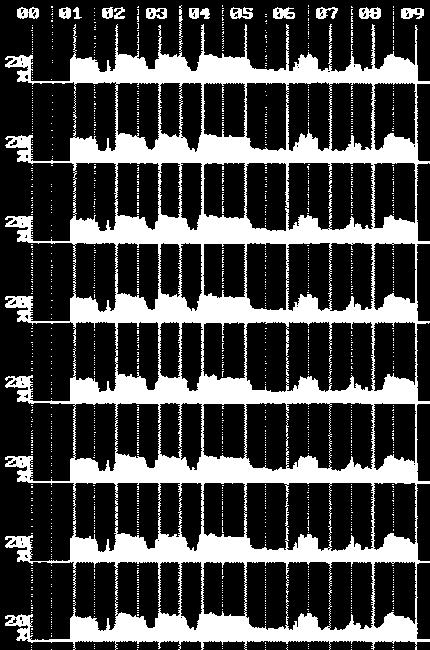



41 PAV changes during vasospasm Vasospasm Hypertensive & Hypervolemic Papaverine Infarction
 L/P ratio surpassed the defined thresholds of cerebral crisis 40 h (25 48) before onset of refractory intracranial hypertension,")
42 From day 1 3 before DC the L/P ratio increased significantly (P < 0.001) L/P ratio surpassed the defined thresholds of cerebral crisis 40 h (25 48) before onset of refractory intracranial hypertension, which occurred 4.2 h (1 10) before surgery. Nagel, Neurocrit Care 2012
Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Positron Emission Tomography Imaging in Brain Injured Patients
 Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
9/16/2018. Recognizing & Managing Seizures in Pediatric TBI. Objectives. Definitions and Epidemiology
 Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Cosa chiedo alla PtO 2
 Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
What is elevated ICP?
 What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Do Prognostic Models Matter in Neurocritical Care?
 Do Prognostic Models Matter in Neurocritical Care? Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical
Do Prognostic Models Matter in Neurocritical Care? Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS
 GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
Raw and Quantitative EEG for Identification of Ischemia
 Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosures None relevant
Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosures None relevant
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
ICP (Intracranial Pressure) Monitoring Brain Tissue Oxygen Monitoring Jugular Venous Bulb Oximetry
 Monitoring Brain Tissue Oxygen Monitoring Jugular Venous Bulb Oximetry") ICP (Intracranial Pressure) Monitoring Secondary brain injury may be a direct consequence of intracranial hypertension. Therefore monitoring of ICP and cerebral perfusion pressure (CPP) are immediate priority
ICP (Intracranial Pressure) Monitoring Secondary brain injury may be a direct consequence of intracranial hypertension. Therefore monitoring of ICP and cerebral perfusion pressure (CPP) are immediate priority
Current bedside monitors of brain blood flow and oxygen delivery
 24. Brain Chemistry Current bedside monitors of brain blood flow and oxygen delivery Global monitors Cannot detect regional abnormalities Local monitors Sample only a small region of the brain and highly
24. Brain Chemistry Current bedside monitors of brain blood flow and oxygen delivery Global monitors Cannot detect regional abnormalities Local monitors Sample only a small region of the brain and highly
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
Periodic and Rhythmic Patterns. Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina
 Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
Functional cerebral monitoring in patients with critically illness
 Functional cerebral monitoring in patients with critically illness Anne-Marie Guerguerian MD PhD Assistant Professor of Critical Care Medicine & Pediatrics Scientist in Neurosciences & Mental Health, Research
Functional cerebral monitoring in patients with critically illness Anne-Marie Guerguerian MD PhD Assistant Professor of Critical Care Medicine & Pediatrics Scientist in Neurosciences & Mental Health, Research
ICU EEG MONITORING: WHY, WHEN AND FOR WHOM
 ICU EEG MONITORING: WHY, WHEN AND FOR WHOM Aatif M. Husain, MD Duke University Veterans Affairs Medical Center Durham, NC In the last two decades much has been learned about the frequency with which seizures
ICU EEG MONITORING: WHY, WHEN AND FOR WHOM Aatif M. Husain, MD Duke University Veterans Affairs Medical Center Durham, NC In the last two decades much has been learned about the frequency with which seizures
Multimodal monitoring to individualize care in TBI
 Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Current status of temperature management in the neuro-icu
 Current status of temperature management in the neuro-icu Gregor Brössner, MD Neurologic Intensiv Care Unit Innsbruck, Austria Disclosures: Gregor Brössner has recieved an unrestricted Grant by Alsius
Current status of temperature management in the neuro-icu Gregor Brössner, MD Neurologic Intensiv Care Unit Innsbruck, Austria Disclosures: Gregor Brössner has recieved an unrestricted Grant by Alsius
12/1/2017. Disclosure. When I was invited to give a talk in Tokyo 2011 at the 4 th International. Hypothermia Symposium
 Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Continuous Peritransplant Assessment of Consciousness using Bispectral Index Monitoring for Patients with Fulminant Hepatic Failure
 Continuous Peritransplant Assessment of Consciousness using Bispectral Index Monitoring for Patients with Fulminant Hepatic Failure Purpose: Deterioration of consciousness is the most critical problem
Continuous Peritransplant Assessment of Consciousness using Bispectral Index Monitoring for Patients with Fulminant Hepatic Failure Purpose: Deterioration of consciousness is the most critical problem
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
HYPERBARIC OXYGEN BRAIN INJURY TREATMENT TRIAL: A MULTICENTER PHASE II ADAPTIVE CLINICAL TRIAL
 HYPERBARIC OXYGEN BRAIN INJURY TREATMENT TRIAL: A MULTICENTER PHASE II ADAPTIVE CLINICAL TRIAL Gaylan Rockswold, MD, PhD, Principal Investigator William Barsan, MD, Principal Investigator, CCC, SIREN Byron
HYPERBARIC OXYGEN BRAIN INJURY TREATMENT TRIAL: A MULTICENTER PHASE II ADAPTIVE CLINICAL TRIAL Gaylan Rockswold, MD, PhD, Principal Investigator William Barsan, MD, Principal Investigator, CCC, SIREN Byron
PACT module. Traumatic Brain Injury. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Severe Traumatic Brain Injury Protocol
 Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Precision Medicine in Neurocritical Care: Should we individualize care?
 Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Guidelines and Beyond: Traumatic Brain Injury
 Guidelines and Beyond: Traumatic Brain Injury Aimee Gowler, PharmD, BCCCP, BCPS Neuromedicine Critical Care Clinical Pharmacy Specialist UF Health Shands Disclosures I have no financial interests to disclose.
Guidelines and Beyond: Traumatic Brain Injury Aimee Gowler, PharmD, BCCCP, BCPS Neuromedicine Critical Care Clinical Pharmacy Specialist UF Health Shands Disclosures I have no financial interests to disclose.
Plenary Address: Medico-Legal Issues in Neuro-intensive Care
 Plenary Address: Medico-Legal Issues in Neuro-intensive Care Dr Basil Matta Divisional Director, Emergency and Perioperative Care Cambridge University Hospitals NHS Foundation Trust Medico-Legal Issues
Plenary Address: Medico-Legal Issues in Neuro-intensive Care Dr Basil Matta Divisional Director, Emergency and Perioperative Care Cambridge University Hospitals NHS Foundation Trust Medico-Legal Issues
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report
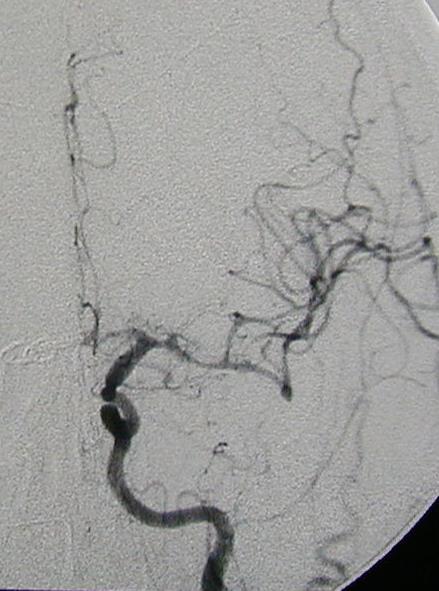
 214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Improving TBI outcome
 Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University. Director of Pediatric Cardiac Anesthesiology
 Professor of Anesthesiology, Stanford University. Director of Pediatric Cardiac Anesthesiology") Should NIRS be Standard Care for Pediatric CPB Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University Director of Pediatric Cardiac Anesthesiology Stanford Children s Hospital
Should NIRS be Standard Care for Pediatric CPB Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University Director of Pediatric Cardiac Anesthesiology Stanford Children s Hospital
NO CONFLICTS NO CONFLICTS
 Anesthesia and Critical Care Medicine Department of Surgical Specialties, Radiological Sciences and Public Health, University of Brescia; Department of Anesthesia, Critical Care and Emergency, Spedali
Anesthesia and Critical Care Medicine Department of Surgical Specialties, Radiological Sciences and Public Health, University of Brescia; Department of Anesthesia, Critical Care and Emergency, Spedali
Neurological Prognosis after Cardiac Arrest Guideline
 Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
CNS pathology Third year medical students,2019. Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Is Neuromonitoring an expensive waste of time, in Severe Traumatic Brain Injury?
 Is Neuromonitoring an expensive waste of time, in Severe Traumatic Brain Injury? Edema Engorgement Contusion Hematoma Hypoxia Diffuse Axonal Injury Ross Bullock, MD, PhD. Director, Neurotrauma,- University
Is Neuromonitoring an expensive waste of time, in Severe Traumatic Brain Injury? Edema Engorgement Contusion Hematoma Hypoxia Diffuse Axonal Injury Ross Bullock, MD, PhD. Director, Neurotrauma,- University
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Continuous EEG: A Standard in Canada?
 Continuous EEG: A Standard in Canada? Victoria McCredie MBChB Neurointensivist Sunnybrook Health Sciences Centre Critical Care Canada Forum 28 th October 2015 No conflicts of interest to disclose. Outline
Continuous EEG: A Standard in Canada? Victoria McCredie MBChB Neurointensivist Sunnybrook Health Sciences Centre Critical Care Canada Forum 28 th October 2015 No conflicts of interest to disclose. Outline
9/18/16. Management of Ischemic Stroke in the Intensive Care Unit. Outline. Introduction. Kyle B Walsh MD. Phases of Stroke Diagnosis and Treatment
 Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
CPPopt: matters to be solved before or by an RCT? Geert Meyfroidt, MD, PhD Intensive Care Medicine University Hospitals Leuven Belgium
 CPPopt: matters to be solved before or by an RCT? Geert Meyfroidt, MD, PhD Intensive Care Medicine University Hospitals Leuven Belgium Financial disclosures Research Foundation, Flanders (senior clinical
CPPopt: matters to be solved before or by an RCT? Geert Meyfroidt, MD, PhD Intensive Care Medicine University Hospitals Leuven Belgium Financial disclosures Research Foundation, Flanders (senior clinical
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
Epilepsy CASE 1 Localization Differential Diagnosis
 2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurotrauma: The Place for Cooling
 Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
Brain under pressure Managing ICP. Giuseppe
 Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
give lorazepam Page 1 UC SF First known description of status epilepticus (Sakikku cuneiform, ca. 700 B.C) NEUROCRITICAL CARE PROGRAM
 NEUROCRITICAL CARE PROGRAM") Update on Neurocritical Care J. Claude Hemphill III, MD, MAS Special Thanks to: Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University Disclosures Research Support: NIH/NINDS Stock
Update on Neurocritical Care J. Claude Hemphill III, MD, MAS Special Thanks to: Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University Disclosures Research Support: NIH/NINDS Stock
7/22/2016. Navaz Karanjia, MD. FINANCIAL DISCLOSURE: none. UNLABELED/UNAPPROVED USE DISCLOSURE: none
 Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Blood transfusions in sepsis, the elderly and patients with TBI
 Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Disclosure Statement. Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk.
 Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
The clinical evidence: Hypothermia for other indications
 Sicily, October 18 TH 2006 The clinical evidence: Hypothermia for other indications K.H. Polderman, internist/intensivist University medical center Utrecht, The Netherlands That is why we need temperature
Sicily, October 18 TH 2006 The clinical evidence: Hypothermia for other indications K.H. Polderman, internist/intensivist University medical center Utrecht, The Netherlands That is why we need temperature
Near Infrared Spectroscopy in Neonatal Intensive Care
 Near Infrared Spectroscopy in Neonatal Intensive Care Adré J. du Plessis, MBChB Fetal-Neonatal Neurology, Children s Hospital, Boston, MA Children s Hospital and Harvard Medical School Disclosure Statement
Near Infrared Spectroscopy in Neonatal Intensive Care Adré J. du Plessis, MBChB Fetal-Neonatal Neurology, Children s Hospital, Boston, MA Children s Hospital and Harvard Medical School Disclosure Statement
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Cerebral Oxygen Desaturation with Normal ICP and CPP in Severe TBI
 The Open Critical Care Medicine Journal,, 1, -3 Open Access Cerebral Oxygen Desaturation with Normal ICP and CPP in Severe TBI Sylvain Palmer *,1 and Mary Kay Bader 1 Orange County Neurological Associates,
The Open Critical Care Medicine Journal,, 1, -3 Open Access Cerebral Oxygen Desaturation with Normal ICP and CPP in Severe TBI Sylvain Palmer *,1 and Mary Kay Bader 1 Orange County Neurological Associates,
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Conflict of Interest Disclosure J. Claude Hemphill III, MD,MAS. Difficult Diagnosis and Treatment: New Onset Obtundation
 Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Recent trends in the management of head injury
 Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Continuous EEG Monitoring in Spontaneous Intracerebral Hemorrhage
 Continuous EEG Monitoring in Spontaneous Intracerebral Hemorrhage Ayman M Selim 1, Ghada R Mousa 1, Eman Awad 2, Wael Reda 3, Sherif Abdelfattah 4 Departments of Neurology, Zagazig University 1 ; Neurology,
Continuous EEG Monitoring in Spontaneous Intracerebral Hemorrhage Ayman M Selim 1, Ghada R Mousa 1, Eman Awad 2, Wael Reda 3, Sherif Abdelfattah 4 Departments of Neurology, Zagazig University 1 ; Neurology,
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
Goals and Objectives of the Educational Program
 Goals and Objectives of the Educational Program Neurosurgical Fellowship Definition: This fellowship is designed to give concise and formal training in neurosurgical anesthesia at LAC+USC Medical Center
Goals and Objectives of the Educational Program Neurosurgical Fellowship Definition: This fellowship is designed to give concise and formal training in neurosurgical anesthesia at LAC+USC Medical Center
Single Seizure of Unknown Cause
 S1: Medical Standards for Safety Critical Workers with Seizures of Unknown Cause 1. Seizure or Epilepsy of Unknown Cause are the classifications used in these medical standards for a probable seizure(s),
S1: Medical Standards for Safety Critical Workers with Seizures of Unknown Cause 1. Seizure or Epilepsy of Unknown Cause are the classifications used in these medical standards for a probable seizure(s),
Early detection of vasospasm after acute subarachnoid hemorrhage using continuous EEG ICU monitoring
 ELSEVIER Electroencephalography and clinical Neurophysiology 103 (1997) 607-615 Early detection of vasospasm after acute subarachnoid hemorrhage using continuous EEG ICU monitoring Paul M. Vespa a'*, Marc
ELSEVIER Electroencephalography and clinical Neurophysiology 103 (1997) 607-615 Early detection of vasospasm after acute subarachnoid hemorrhage using continuous EEG ICU monitoring Paul M. Vespa a'*, Marc
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal compartment syndrome, as complication of fluid resuscitation, 331 338 abdominal perfusion pressure, 332 fluid restriction practice
Index Note: Page numbers of article titles are in boldface type. A Abdominal compartment syndrome, as complication of fluid resuscitation, 331 338 abdominal perfusion pressure, 332 fluid restriction practice
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
Decompressive Hemicraniectomy in Acute Neurological Diseases
 Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8:
 Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
02/08/53. ** Thanks you to. Dr. Lawrence J. Hirsch, M.D Susan T. Herman, M.D. Jed A. Hartings, Ph.D. Thomas P. Bleck MD Denis Azzopardi
 ** Thanks you to Dr. Lawrence J. Hirsch, M.D Susan T. Herman, M.D. Jed A. Hartings, Ph.D. Thomas P. Bleck MD Denis Azzopardi 1 Why do we need ICU-EEG? Residual electrographic SE after control of visible
** Thanks you to Dr. Lawrence J. Hirsch, M.D Susan T. Herman, M.D. Jed A. Hartings, Ph.D. Thomas P. Bleck MD Denis Azzopardi 1 Why do we need ICU-EEG? Residual electrographic SE after control of visible
Critical Care Management of Acute Ischemic Stroke
 Critical Care Management of Acute Ischemic Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Neurocritical Care and Stroke Division University of Southern California USC Stroke
Critical Care Management of Acute Ischemic Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Neurocritical Care and Stroke Division University of Southern California USC Stroke