DIAGNOSTIC NEURORADIOLOGY. sequences
|
|
|
- Collin Lewis
- 5 years ago
- Views:
Transcription
1 Neuroradiology (1999) 41: 471±479 Ó Springer-Verlag 1999 DIAGNOSTIC NEURORADIOLOGY C. Oppenheim D. Dormont D. Hasboun B. Bazin S. Samson S. LehØricy M. Baulac C. Marsault Bilateral mesial temporal sclerosis: MRI with high-resolution fast spin-echo and fluid-attenuated inversion-recovery sequences Received: 19 June 1998 Accepted: 7 December 1998 C.Oppenheim ( ) ) D. Dormont D. Hasboun S.LehØricy C.Marsault Department of Neuroradiology, Bâtiment Babinski, Groupe Hospitalier PitiØ-Salp tri re, 47 Boulevard de L'Hôpital, Paris Cedex 13, France catherine.oppenheim@psl. ap-hop-paris.fr, Tel: / , Fax: D. Hasboun B.Bazin S. Samson M. Baulac Department of Neurology, Epilepsy Unit, Groupe Hospitalier PitiØ-Salp tri re, Paris VI University, Paris, France Abstract We report a retrospective analysis of MRI in 206 patients with intractable seizures and describe the findings in bilateral mesial temporal sclerosis (MTS) on fast spin-echo (FSE) and fast fluid-attenuated inversion-recovery (fflair) sequences. Criteria for MTS were atrophy, signal change and loss of the digitations of the head of the hippocampus. In patients with bilateral MRI signs of MTS, correlation with clinical electro, volumetric MRI data and neuropsychological tests, when available, was performed. Bilateral MTS was observed in seven patients. Bilateral loss of the digitations and signal change on fflair was seen in all seven. In three, bilateral atrophy was obvious. In two patients, mild bilateral atrophy was observed and in two others, the hippocampi were: asymmetrical, with obvious atrophy on only one side. Volumetric data confirmed bilateral symmetrical atrophy in five patients, and volumes were at the lowest of the normal range in the other two. The EEG showed temporal abnormalities in all patients, unilateral in five and bilateral in two. All patients had memory impairment and neuropsychological data confirmed visual and verbal memory deficits; two patients failed the Wada test on both sides. High-resolution T2-weighted FSE and fflair sequences allow diagnosis of bilateral MTS, which has important therapeutic and prognostic implications. Key words Sclerosis, hippocampal Magnetic resonance imaging Epilepsy Introduction The most common histological substrate of intractable complex partial seizures in adults is mesial temporal sclerosis (MTS) [1±4]. The probability of seizure-free outcomes following temporal lobectomy is significantly greater in patients with unilateral MTS on MRI [2, 5±9]. Unilateral MTS has been studied extensively and its MRI features are well established. According to most recent series, hippocampal atrophy and signal abnormalities on T2-weighted images can identify unilateral MTS with an accuracy approaching 90%. Pathological studies [1, 10±12], however, have shown that some histological evidence of MTS (neuronal loss and gliosis) can be observed bilaterally in up to 70±80% of patients. Despite this, bilateral MTS is seldom reported on MRI [7, 13±16]. Indeed, MRI diagnosis of bilateral MTS is difficult, because qualitative diagnosis of hippocampal atrophy relies on the comparison of the size of the hippocampal formations and until recently, most volumetric studies used ratio or volume differences between the left and right hippocampus. These techniques may thus fail to enable detection of symmetrical bilateral disease [13, 15, 17, 18]. T2-weighted high-resolution fast spin-echo (FSE) and fast fluid-attenuated inversion-recovery (fflair) sequences can improve qualitative MRI diagnosis of unilateral MTS [19±21]. From December 1996, all patients we studied with medically in-
, neuropsychological and metabolic tests when available, and hippocampal")

; T2-weighted axial spin-echo images 2800/30/90/1 through the entire brain;")
2 472 tractable partial epilepsy had these sequences as part of their investigation. In some patients, bilateral hippocampal abnormalities were observed, suggesting bilateral MTS. Our purpose here is to describe these abnormalities and to correlate the findings with clinical, electroencephalographic (EEG), neuropsychological and metabolic tests when available, and hippocampal volumetric data, to validate these MRI criteria as legitimate markers of bilateral MTS. Material and methods We studied 206 patients with a clinical diagnosis of medically intractable simple or complex partial or secondarily generalised seizures. Of the patients, 71 had a presumed temporal lobe focus. All were studied with the same protocol using a quadrature head coil on a 1.5-T unit. We performed five sequences: T1-weighted sagittal spin-echo 600/11/1 (repetition time / echo time ms / number of excitation); T2-weighted axial spin-echo images 2800/30/90/1 through the entire brain; three-dimensional spoiled gradient-recalled acquisition in the steady state (SPGR), 1.5-mm-thick sections, matrix, cm field of view, 23/5/1, 35 flip angle, providing 124 contiguous slices in the coronal plane, reformatted parallel and perpendicular to the long axis of the hippocampus; high-resolution T2-weighted FSE 3020/126/4 of the temporal lobe with 3- or 4-mm interleaved slices, matrix, cm field of view, echo-train length 8, 32 khz bandwidth, superoinferior frequency-encoding gradient; and fflair 10002/148/2200 acquisition with 5-mm interleaved slices, matrix, cm field of view, 32-kHz bandwidth, superoinferior frequency-encoding gradient. For both FSE and fflair sequences, imaging plane was perpendicular to the long axis of the hippocampus as determined on the first acquisition. All 206 MRI studies were retrospectively reviewed by two trained neuroradiologists, blinded to clinical and pathological data, and discrepancies were solved by consensus. Section-by-section visual assessment of the signal and morphology of the hippocampus was performed on sections perpendicular to the long axis of the hippocampus. Signal intensity in the hippocampi was assessed by comparing it to that of grey matter in the temporal lobe neocortex. The diagnosis of MTS was based on signal changes of the hippocampal formations on T2-weighted FSE and/or fflair, and on two morphological criteria sought on FSE or SPGR acquisitions: atrophy and loss of the digitations of the head of the hippocampus [20] (Fig. 1). In patients with MRI criteria of bilateral MTS, MRI hippocampal volume measurements were performed on a workstation, using a method described previously [22]. The volume (V) of each hippocampus and the volume relative to the a b Fig. 1 a±c hippocampi in a control. Images perpendicular to the long axis of the hippocampus at the level of its head. a 3D T1-weighted SPGR image showing normal hippocampi with no asymmetry of size. Small humps or digitations (arrowheads), are normally visible on the superior part of both hippocampal heads. b T2-weighted FSE image showing no hippocampal atrophy and sharply visible digitations (arrowheads) which protude into the temporal horns and are thus well outlined by the high-signal cerebrospinal fluid. c fflair image showing no hippocampal signal change c
3 473 Table 1 Summary of findings. % indicates that the values are below normal values Patient Age/ sex Age at onset of seizures (years) Type EEG Neuropsychological and clinical data 1 19/F 2 PSSG L temporal Memory complaints, mentally retarded, no school attendance 2 18/F 9 CPS L temporal Memory complaints, chronic psychosis 3 27/F 6 CPS R temporal Memory complaints, verbal and visual memory impairment, mentally retarded 4 26/M 3 CPS L temporal Memory complaints, verbal and visual memory impairment, normal IQ 5 46/M 17 CPS Bitemporal L>R Memory complaints 6 41/M 30 CPS R temporal Memory complaints, verbal and visual memory impairment, normal IQ 7 53/F 48 CPS Bitemporal Memory complaints PSSG simple partial seizures secondarily generalised, CPS complex partial seizures Amylobarbitone PET memory loss Bilateral dysfunction Bilateral dysfunction R temporal hypometabolism L temporal hypometabolism Atrophy on visual analysis Bilateral, symmetrical Bilateral, symmetrical Bilateral R>L Bilateral, L>R Moderate, bilateral and symmetrical Moderate, bilateral and symmetrical Signal intensitmetry Asym- changes index a on FSE and fflair Bilateral 0% Bilateral 3.7% R only on FSE, bilateral on fflair 0% Bilateral 16% L>R Doubtful on FSE, bilateral on fflair Bilateral only in head on FSE, bilateral in head and body on fflair 0% 11.4 % Hippocampal volume (ml) b Left V 2.1 % 0.22 % % V 2.6 % 0.21 % % Hippocampal volume (ml) b Right V 2.1 % 0.22 % % V 2.7 % 0.22 % % V 3.3 V % % V, V, normal normal V 2.6 % 0.23 % % V3% 0.23 % % V 3.1 % % % V3% 0.23 % % V 3.1 V % % V normal, normal V, % Bilateral, Bilateral V 2.3 % V 2.5 % symmetrical a Asymmetry index considered significant when > 14.29% b V Absolute hippocampal volume, absolute hippocampal 0.2% % 2.2% % volume divided by the global cerebral volume cerebral volume () were calculated and compared to the normal values (mean ± 2 standard deviations) obtained with this method. An asymmetry index was also calculated and compared with normal values [22]. Side-to-side hippocampal symmetry was determined by subtracting the volume of left hippocampus from that of the right, divided by the larger of the two volumes. The following values were considered as the minimum normal volume: V: 3.3 cc; : 0.261% for the right hippocampus, V: 3.4 cc; : 0.269% for the left in men, and V: 3.1 cc; : 0.263% for the right, V: 3.1 cc; : 0.265% for the left. Asymmetry indices were considered significant when greater than 14.29% (mean + 2 standard deviations). All patients with MRI criteria of bilateral MTS had a clinical examination and ictal and interictal EEG; two also had video-eeg studies. As part of presurgical investigation, two patients had positron emission tomography (PET) with 18 F-fluorodeoxyglucose and a bilateral Wada test exploring memory. Formal neuropsychological testing was carried out in three patients. Results The data are summarised in Table 1. We diagnosed unilateral MTS in 47 patients and bilateral MTS in seven. In patients 1, 2 and 7 bilateral atrophy and loss of the digitations of the head of the hippocampus were clearly seen on T1- and FSE T2-weighted images. No asymmetry in size was detected. The diagnosis was confirmed by the presence of signal changes on T2-weighted FSE and fflair images; the changes were better shown on the latter (Fig.2). In patients 5 and 6, no digitations were seen at the head of the hippocampus and both hippocampi appeared slightly small, but symmetrical. The diagnosis of bilateral MTS was confirmed by the presence of clear bilateral signal intensity abnormalities on fflair images (Fig. 3). In patients 3 and 4, the digitations in the head of the hippocampus were invisible in both hippocampal for-






4 474 a d b e c f
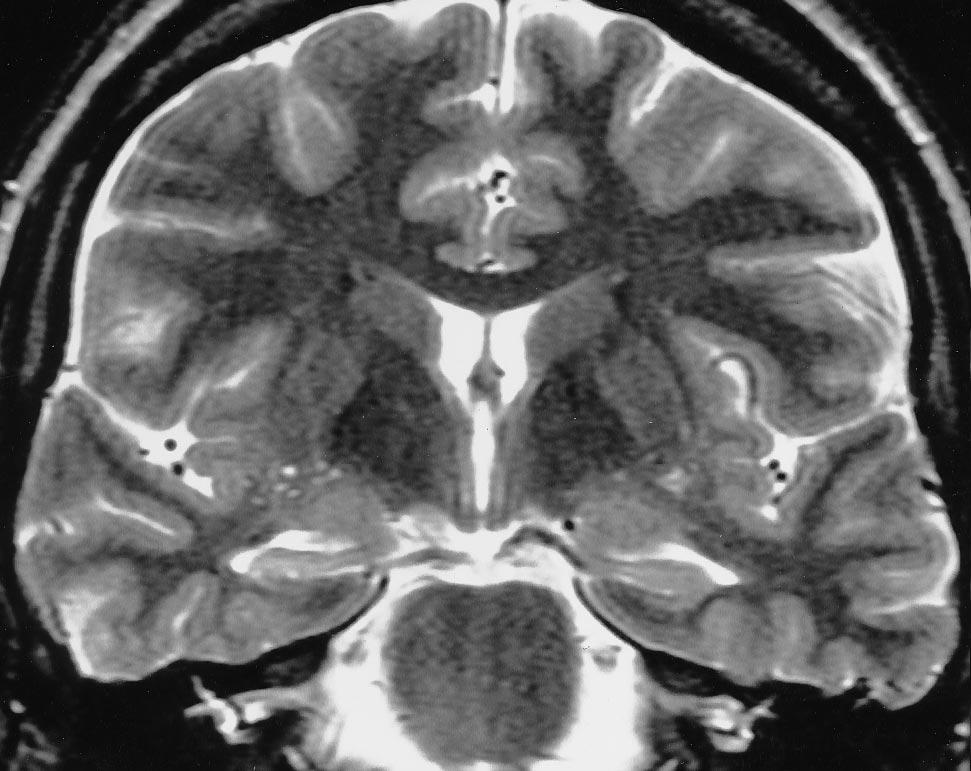
5 475 mations, which were unequal in size (Fig. 4a, 3 b). Bilateral abnormalities consistent with MTS were confirmed on the fflair images, showing signal changes in both hippocampi (Fig. 4 c). In patients 3 and 5, the fflair sequence clearly showed bilateral signal change while FSE showed signal change in only one hippocampus. The volumes of both hippocampi were less than the normal minimum value in five patients (ten hippocampi) and within the normal range in two patients (four hippocampi). In one of these four (patient 6, left hippocampus), only the value corrected by the global cerebral volume suggested atrophy; the absolute value was within the normal range. Asymmetry indices were abnormal only in patient 4. Overall, there was discordance between the quantitative and qualitative analysis of three hippocampi (right and left in patient 3, left in patient 6) in which quantitative analysis failed to detect atrophy. EEG showed temporal abnormalities in all seven patients, clearly unilateral in five (left temporal lobe in three and right in two), and bilateral in two. In patients 3 and 4, with bilateral but asymmetrical atrophy on visual analysis, seizures began from the more atrophic hippocampal formation, with the more pronounced signal abnormalities. In patient 3, volumetric measurements failed to lateralise the epileptogenic focus, as no asymmetry was found. In the other three patients with unilateral temporal lobe seizures, abnormalities were symmetrical on MRI images, without lateralising value. PET performed in patients 3 and 4, showed unilateral hypometabolism, thought to have good lateralising value. The two patients with bitemporal epileptogenic foci also had symmetrical abnormalities on MRI. Mental retardation was observed in two cases, chronic psychosis in one. All patients had memory impairment and formal neuropsychological tests, performed in patients 3, 4 and 6, confirmed visual and verbal memory impairment. In patients 3 and 4, who had Wada test, memory impairment was observed when amylobarbitone was injected into in either the right or left internal carotid artery. W Fig. 2 a±f Patient 7: a 53-year-old woman with complex partial seizures and memory disturbance. The EEG showed bilateral temporal epileptogenic foci. Volumetric MRI showed marked bilateral atrophy. a 3D T1-weighted SPGR image through the head of the hippocampus showing bilateral, symmetrical atrophy. b T2- weighted FSE image showing bilateral atrophy, slightly increased signal and bilateral loss of the digitations of the head of the hippocampus. c fflair image showing obvious bilaterally increased signal intensity. d 3D T1-weighted SPGR image through the body of the hippocampus showing bilateral atrophy, more marked on the right. e T2-weighted FSE image showing bilateral atrophy and slightly increased signal. f fflair showing bilaterally increased signal Discussion The most widely recognized MRI criteria for MTS are hippocampal atrophy and increased signal intensity on T2-weighted images [5, 18, 21, 23±28]. The reported sensitivity of MRI to unilateral MTS reaches 93% [29±31]. Patterns suggestive of unilateral MTS are observed in about two thirds of MRI studies of patients with temporal lobe seizures. Discrepancies exist between the MR and pathological data in the literature on bilateral MTS. While MRI studies very rarely describe images of bilateral MTS, post mortem investigations have shown that histological MTS is present bilaterally to some extent in 72% [11] to 90 % [12] of patients. Other groups have shown pathological evidence of asymmetrical bilateral hippocampal damage in 80% of subjects, symmetrical damage in 10% and strictly unilateral MTS in only 10% [1]. Bilateral involvement of the hippocampi by MTS has also been suggested by MR spectroscopy [6, 32, 33] and T2 relaxometry [34±36]. It is thus probable that some patients have undiagnosed bilateral hippocampal disease. This is not very surprising. Recognition of hippocampal atrophy relies on the comparison of the two sides and is thus difficult if both are atrophic; qualitative estimation of side-to-side asymmetry of signal intensity can be established with a high degree of accuracy but bilateral signal intensity change is more difficult to identify. It is also impossible to make the diagnosis of bilateral MTS with most volumetric techniques [8, 34, 37±40] which use asymmetry indices rather than absolute values. Recently, two other signs have been described for MRI diagnosis of MTS: high hippocampal signal on fflair [19] and loss of visibility of the digitations of the head of the hippocampus [20]. fflair has been shown to be more sensitive than spin-echo sequences to signal changes in MTS [19]. Although these signs have been described in unilateral MTS, they are useful for diagnosis of bilateral MTS since they do not rely on side-to-side comparison. Volumetric techniques which do not depend on side-to-side comparison have also been described, based on absolute volumetric and comparison of the volume of each hippocampus to a data base of healthy volunteers [39±41]. Using hippocampal signal intensity increase on fflair and loss of visibility of the digitations of the head of the hippocampus, we diagnosed bilateral MTS in 7 of 71 patients with temporal lobe epilepsy. They had loss of the digitations, signal changes on fflair and atrophy in both hippocampal formations. Pathological studies in operated patients with unilateral MTS have shown that these MRI signs correlate with gliosis and neuronal loss [5, 8, 17, 19, 20, 40]. It is therefore likely, when signal intensity abnormalities on fflair and loss of the digitations are observed bilaterally, that MTS is present, to some extent, bilaterally. Moreover, five of





6 476 3 a 4 a b b c c
7 477 W Fig. 3 a±c Patient 5: a 46-year-old man with intractable complex partial seizures and memory deficits with bilateral temporal epileptogenic foci on EEG. Volumetric MRI showed bilateral, symmetrical atrophy. a 3D T1-weighted SPGR image showing slight atrophy with no asymmetry. b T2-weighted FSE image showing bilateral atrophy and loss of the digitations of the head of the hippocampus. c fflair image showing obviously increased signal bilaterally Fig. 4 a±c Patient 3: a 27-year-old woman, with intractable complex partial seizures, memory disturbance and a right temporal epileptogenic focus on EEG. Volumetric MRI showed both hippocampi to have volumes at the lower limit of normal. The diagnosis of bilateral mesial temporal sclerosis was supported by neuropsychological data and bilateral failure of the Wada test. a 3D T1-weighted SPGR image showing asymmetry of the hippocampi, with obvious atrophy on only the right. b T2-weighted FSE image showing bilateral loss of digitations with increased signal on only the right. c fflair image showing obvious bilaterally increased signal the seven patients had volumetric confirmation of bilateral MTS. In the other two, absolute volume measurements were found within the normal range for our institution; their hippocampal volumes were at the lower limit of normal. The fact that the normal range is quite large means that mild atrophy cannot be unambiguously distinguished from normal [38, 41, 42]. When neuronal loss is mild, the loss of hippocampal volume may be less than the combination of measurement error and normal variation, and therefore not detectable [18, 27, 43]. It is thus probable that our seven patients had bilateral MTS. However, no histopathological proof of bilateral disease can be obtained, since bilateral removal of the hippocampus would result in dramatic persistent memory impairment [44]; confirmatory data can come only from autopsy studies. Neuropsychological examination supported bilateral hippocampal damage in all three patients. That bilateral hippocampal lesions can lead to severe memory impairment is well known; severe, persistent amnesia has been described in one patient after bitemporal lobectomy [44, 45]. Memory deficit has also been described in bilateral medial temporal lobe damage due to viral encephalitis [46], ischaemia [47] and complex partial status epilepticus with bilateral mesial temporal involvement [48]. Global memory impairment has also been reported after unilateral resection, suggesting contralateral hippocampal dysfunction [49, 50]. In two patients, contralateral hippocampal damage was confirmed at autopsy [51, 52]. All our seven patients had memory impairment. Memory battery tests, when performed, showed a global deficit strongly suggesting some degree of bilateral involvement of their hippocampal structures. The selective memory deficit found in cases of unilateral MTS, was not present. Moreover, in two patients, the amylobarbitone tests, used to predict contralateral mesial temporal dysfunction, showed a bilateral memory deficit. The percentage of bilateral MTS we reported (10 %) is higher than that in the MRI literature but is comparable with the rate of severe symmetric bilateral involvement in the pathological literature. It is likely that our patients did have severe bilateral damage. Since pathological changes due to MTS are often present bilaterally but have a marked unilateral predominance, there could be patients, considered as having unilateral MTS, with bilateral and asymmetrical abnormalities not detectable with our current MRI protocol. In clinical practice, bilateral MTS can be undiagnosed on electrical and clinical data since patients can have a well-organised unilateral temporal epileptogenic focus. Of our seven patients, five had unilateral temporal lobe EEG abnormalities and only two had bilateral temporal lobe epileptogenic zones. Bilateral hippocampal damages could not be suspected on PET, since hypometabolism was unilateral. Concerning the relationship between bilateral MTS and operative outcome, some groups report poor seizure outcome in patients with temporal lobe seizures and symmetrical hippocampi [10, 25], while others observed a seizure-free outcome [7]. However, all agree that there are important concerns for the risk of postoperative amnesia in patients with bilateral MTS. References 1. Babb TL, Brown WJ (1987) Pathological findings in epilepsy. In: Engel J Jr (ed) Surgical treatment of the epilepsies. Raven Press, New York, pp 511± Duncan JS, Sagar HJ (1987) Seizure characteristics, pathology, and outcome after temporal lobectomy. Neurology 37: 405± Engel J Jr, Driver MV, Falconer MA (1975) Electrophysiological correlates of pathology and surgical results in temporal lobe epilepsy. Brain 98: 129± Falconer MA (1974) Mesial temporal (Ammon's horn) sclerosis as a common cause of epilepsy. Aetiology, treatment, and prevention. Lancet ii: 767± Bronen R, Cheung G, Charles JT, et al (1991) Imaging findings in hippocampal sclerosis: correlation with pathology. AJNR 12: 933± Ende GR, Laxer KD, Knowlton RC, et al (1997) Temporal lobe epilepsy: bilateral hippocampal metabolite changes revealed at proton MR spectroscopic imaging. Radiology 202: 809± Jack CR, Trenerry MR, Cascino GD, Sharbrough FW, So EL, O'Brien PC (1995) Bilaterally symmetric hippocampi and surgical outcome. Neurology 45: 1353±1358
8 Lencz T, McCarthy G, Bronen RA, et al (1992) Quantitative magnetic resonance imaging in temporal lobe epilepsy: relationship to neuropathology and neuropsychological function. Ann Neurol 31: 629± National Institutes of Health Consensus Conference (1990) Surgery for epilepsy. JAMA 264: 729± Babb TL (1991) Bilateral pathological damage in temporal lobe epilepsy. Can J Neurol Sci 18: 645± Margerison JH, Corsellis JA (1966) Epilepsy and the temporal lobes: a clinical electroencephalographic and neuropathological study of the brain in epilepsy, with particular reference to the temporal lobes. Brain 89: 499± Mouritzen-Dam A (1982) Hippocampal neuronal loss in epilepsy after experimental seizures. Acta Neurol Scand 66: 601± King D, Spencer SS, McCarthy G, Luby M, Spencer DD (1995) Bilateral hippocampal atrophy in medial temporal lobe epilepsy. Epilepsia 36: 905± Kuzniecky R, Burgard S, Faught E, Morawetz R, Bartolucci A (1993) Predictive value of magnetic resonance imaging in temporal lobe epilepsy surgery. Arch Neurol 50: 65± Spencer SS, McCarty G, Spencer DD (1993) Diagnosis of medial temporal seizure onset: relative specificity and sensitivity of quantitative MRI. Neurology 43: 2117± Weishmann UC, Free SL, Everitt AD, et al (1996) Magnetic resonance imaging in epilepsy with fast FLAIR sequence. J Neurol Neurosurg Psychiatry 61: 357± Cascino GD, Jack CR, Parisi JE, et al (1991) Magnetic resonance imagingbased volume studies in temporal lobe epilepsy: pathological correlations. Ann Neurol 30: 31± Jack CR, Sharbrough FW, Twomey CK, et al (1990) Temporal lobe seizures lateralization with MR volume measurements of the hippocampal formation. Radiology 175: 423± Jack CR, Rydberg CH, Krecke KN, et al (1996) Mesial temporal sclerosis: diagnosis with fluid-attenuated inversionrecovery versus spin-echo MR imaging. Radiology 199: 367± Oppenheim C, Dormont D, Biondi A, et al (1998) Loss of digitations of the hippocampal head on high resolution fast-spin echo MR imaging: a sign of mesial temporal sclerosis. AJNR 19: 457± Tien RD, Felsberg GJ, Campi de Castro C, et al (1993) Complex partial seizures and mesial temporal sclerosis: evaluation with fast spin-echo MR imaging. Radiology 189: 835± Hasboun D, Chantôme M, Zouaoui A, et al (1996) MR determination of hippocampal volume: comparison of three methods. AJNR 17: 1091± Adam C, Baulac M, Saint-Hilaire JM, Landau J, Granat O, Laplane D (1994) Value of MRI-based measurements of hippocampal formations in partial epilepsy patients. Arch Neurol 51: 130± Berkovic SF, Andermann F, Olivier A, et al (1991) Hippocampal sclerosis in temporal lobe epilepsy demonstrated by magnetic resonance imaging. Ann Neurol 29: 175± Jack CR Jr, Sharbrough FW, Cascino GD, Hirschorn KA, O'Brien PC, Marsh WR (1992) Magnetic resonance imagebased hippocampal volumetry: correlation with outcome after temporal lobectomy. Ann Neurol 31: 138± Jackson GD, Berkovic SF, Tress BM, Kalnins RM, Fabinyi GC, Bladin PF (1990) Hippocampal sclerosis can be reliably detected by magnetic resonance imaging. Neurology 40: 1869± Jackson GD, Berkovic SF, Duncan JS, Connelly A (1993) Optimizing the diagnosis of hippocampal sclerosis using MR imaging. AJNR 14: 753± Kuzniecky R, de la Sayette V, Ethier R, et al (1987) Magnetic resonance imaging in temporal lobe epilepsy: pathological correlations. Ann Neurol 22: 341± Berkovic SF, McIntosh AM, Kalnins RM, et al (1995) Preoperative MRI predicts outcome of temporal lobectomy: an actuarial analysis. Neurology 45: 1358± Jack CR (1995) Magnetic resonance imaging. Neuroimaging Clin North Am 5: 597± LehØricy S, Semah F, Hasboun D, et al (1997) Temporal lobe epilepsy with varying severity: MRI study of 222 patients. Neuroradiology 39: 788± Connelly A, Jackson GD, Duncan JS, Kind MD, Gadian DG (1994) Magnetic resonance spectroscopy in temporal lobe epilepsy. Neurology 44: 1411± Ng TC, Comair YG, Xue M, et al (1994) Temporal lobe epilepsy: presurgical localization with proton chemical shift imaging. Radiology 193: 465± Grünewald RA, Jackson GD, Conelly A, Duncan JS (1994) MR detection of hippocampal disease in epilepsy: factors influencing T2 relaxation time. AJNR 15: 1149± Jackson GD, Connelly A, Duncan JS, Grünewald RA, Gadian DG (1993) Detection of hippocampal pathology in intractable partial epilepsy: increased sensitivity with quantitative magnetic resonance T2 relaxometry. Neurology 43: 1793± von Paesschen W, Sisodiya S, Connelly A, et al (1995) Quantitative hippocampal MRI and intractable temporal lobe epilepsy. Neurology 45: 2233± Achten E, Boon P, De Porter J, Calliauw L, Van De Kerckhove T, De Reuck J, Kunnen M (1995) An MR protocol for presurgical evaluation of patients with complex seizures of temporal origin. AJNR 16: 1201± Cook MJ, Fish DR, Shorvon SD, Straughan K, Stevens JM (1992) Hippocampal volumetric and morphometric studies in frontal and temporal lobe epilepsy. Brain 115: 1001± Jack CR (1994) MRI-based hippocampal volume measurements in epilepsy. Epilepsia 35: S21±S Lee N, Tien RD, Lewis DV, et al (1995) Fast spin-echo magnetic resonance imaging-measured hippocampal volume: correlation with neuronal density in anterior temporal lobectomy patients. Epilepsia 36: 899± Jack C, Twomey CK, Zinsmeister AR, Sharbrough FW, Petersen RC, Cascino GD (1989) Anterior temporal lobes and hippocampal formations: normative volumetric measurements from MR images in young adults. Radiology 172: 549± Jackson GD, Kuzniecky RI, Cascino GD (1994) Hippocampal sclerosis without detectable hippocampal atrophy. Neurology 44: 42± Ashtari M, Barr WB, Schaul N, Bogerts B (1991) Three-dimensional fast low angle shot imaging and computerized volume measurement of the hippocampus in patients with chronic epilepsy of the temporal lobe. AJNR 12: 941± Scoville WB, Milner B (1957) Loss of recent memory after bilateral hippocampal lesions. J Neurol Neurosurg Psychiatry 20: 11± Corking S (1984) Lasting consequence of bilateral medial temporal lobectomy: clinical course and experimental findings in HM. Semin Neurol 4: 249± Rose FC, Symonds CP (1960) Persistent memory defect following encephalitis. Brain 83: Volpe BT, Petito CK (1985) Dementia with bilateral medial temporal lobe ischemia. Neurology 35: 1793±1797
9 Lee BI, Lee BC, Hwang YM, et al (1992) Prolonged ictal amnesia with transient focal abnormalities on magnetic resonance imaging. Epilepsia 33: 1042± Loring DW, Hermann BP, Meador KJ, et al (1994) Amnesia after unilateral temporal lobectomy: a case report. Epilepsia 35: 757± Penfield W, Milner B (1958) Memory deficit produced by bilateral lesion in the hippocampal zone. Arch Neurol Psychiatry 79: 475± Penfield W, Mathieson G (1974) Memory: autopsy findings and comments on the role of the hippocampus in experiencial recall. Arch Neurol 31: 145± Warrington EK, Duchen LW (1992) A re-appraisal of a case of persistent global amnesia following right temporal lobectomy: a clinico-pathological study. Neuropsychologia 30: 437±450
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
Lateralizing Ability of Single-voxel Proton MR Spectroscopy in Hippocampal Sclerosis: Comparison with MR Imaging and Positron Emission Tomography
 AJNR Am J Neuroradiol 22:625 631, April 2001 Lateralizing Ability of Single-voxel Proton MR Spectroscopy in Hippocampal Sclerosis: Comparison with MR Imaging and Positron Emission Tomography Sun-Won Park,
AJNR Am J Neuroradiol 22:625 631, April 2001 Lateralizing Ability of Single-voxel Proton MR Spectroscopy in Hippocampal Sclerosis: Comparison with MR Imaging and Positron Emission Tomography Sun-Won Park,
The Requirement for Ictal EEG Recordings Prior to Temporal Lobe Epilepsy Surgery
 Page 1 of 7 Archives of Neurology Issue: Volume 58(4), April 2001, pp 678-680 Copyright: Copyright 2001 by the American Medical Association. All Rights Reserved. Applicable FARS/DFARS Restrictions Apply
Page 1 of 7 Archives of Neurology Issue: Volume 58(4), April 2001, pp 678-680 Copyright: Copyright 2001 by the American Medical Association. All Rights Reserved. Applicable FARS/DFARS Restrictions Apply
Methods for Normalization of Hippocampal Volumes Measured with MR
 Methods for Normalization of Hippocampal Volumes Measured with MR S. L. Free, P. S. Bergin, D. R. Fish, M. J. Cook, S. D. Shorvon, and J. M. Stevens PURPOSE: To investigate the use of six cerebral measures
Methods for Normalization of Hippocampal Volumes Measured with MR S. L. Free, P. S. Bergin, D. R. Fish, M. J. Cook, S. D. Shorvon, and J. M. Stevens PURPOSE: To investigate the use of six cerebral measures
Surgical outcome in patients with epilepsy and dual pathology
 Brain (1999), 122, 799 805 Surgical outcome in patients with epilepsy and dual pathology L. M. Li, 1 F. Cendes, 1 F. Andermann, 1 C. Watson, 2 D. R. Fish, 3 M. J. Cook, 4 F. Dubeau, 1 J. S. Duncan, 3 S.
Brain (1999), 122, 799 805 Surgical outcome in patients with epilepsy and dual pathology L. M. Li, 1 F. Cendes, 1 F. Andermann, 1 C. Watson, 2 D. R. Fish, 3 M. J. Cook, 4 F. Dubeau, 1 J. S. Duncan, 3 S.
An MR Protocol for Presurgical Evaluation of Patients with Complex Partial Seizures of Temporal Lobe Origin
 An MR Protocol for Presurgical Evaluation of Patients with Complex Partial Seizures of Temporal Lobe Origin Eric Achten, Paul Boon, John De Poorter, Luc Calliauw, Tom Van De Kerckhove, Jacques De Reuck,
An MR Protocol for Presurgical Evaluation of Patients with Complex Partial Seizures of Temporal Lobe Origin Eric Achten, Paul Boon, John De Poorter, Luc Calliauw, Tom Van De Kerckhove, Jacques De Reuck,
Usefulness of Single Voxel Proton MR Spectroscopy in the Evaluation of Hippocampal Sclerosis
 Usefulness of Single Voxel Proton MR Spectroscopy in the Evaluation of Hippocampal Sclerosis 1, 2, 3 Kee-Hyun Chang, MD Hong Dae Kim, MD 1 Sun-Won Park, MD 1 In Chan Song, PhD 2 In Kyu Yu, MD 1 1, 2, 3
Usefulness of Single Voxel Proton MR Spectroscopy in the Evaluation of Hippocampal Sclerosis 1, 2, 3 Kee-Hyun Chang, MD Hong Dae Kim, MD 1 Sun-Won Park, MD 1 In Chan Song, PhD 2 In Kyu Yu, MD 1 1, 2, 3
The Asymmetric Mamillary Body: Association with Medial Temporal Lobe Disease Demonstrated with MR
 The Mamillary Body: Association with Medial Temporal Lobe Disease Demonstrated with MR Alexander C. Mamourian, Lawrence Rodichok, and Javad Towfighi PURPOSE: To determine whether mamillary body atrophy
The Mamillary Body: Association with Medial Temporal Lobe Disease Demonstrated with MR Alexander C. Mamourian, Lawrence Rodichok, and Javad Towfighi PURPOSE: To determine whether mamillary body atrophy
Fig. 1. Localized single voxel proton MR spectroscopy was performed along the long axis of right hippocampus after extension of patient s head to
 125 A B C Fig. 1. Localized single voxel proton MR spectroscopy was performed along the long axis of right hippocampus after extension of patient s head to obtain entire dimension of the hippocampal body.
125 A B C Fig. 1. Localized single voxel proton MR spectroscopy was performed along the long axis of right hippocampus after extension of patient s head to obtain entire dimension of the hippocampal body.
José A Mendes-Ribeiro, Raquel Soares, Fernanda Simões-Ribeiro, M Luiza Guimarães
 58 Neurophysiology Unit J A Mendes-Ribeiro M L Guimarães Department of Neurology and Neurosurgery, Hospital S João, Porto, Portugal F Simões-Ribeiro Magnetic Resonance Unit, IPO, Porto, Portugal R Soares
58 Neurophysiology Unit J A Mendes-Ribeiro M L Guimarães Department of Neurology and Neurosurgery, Hospital S João, Porto, Portugal F Simões-Ribeiro Magnetic Resonance Unit, IPO, Porto, Portugal R Soares
Successful Treatment of Mesial Temporal Lobe Epilepsy with Bilateral Hippocampal Atrophy and False Temporal Scalp Ictal Onset: A case report
 Hiroshima J. Med. Sci. Vol. 61, No. 2, 37~41, June, 2012 HIJM 61 7 37 Successful Treatment of Mesial Temporal Lobe Epilepsy with Bilateral Hippocampal Atrophy and False Temporal Scalp Ictal Onset: A case
Hiroshima J. Med. Sci. Vol. 61, No. 2, 37~41, June, 2012 HIJM 61 7 37 Successful Treatment of Mesial Temporal Lobe Epilepsy with Bilateral Hippocampal Atrophy and False Temporal Scalp Ictal Onset: A case
MR Detection of Hippocampal Disease in Epilepsy: Factors Influencing T2 Relaxation Time
 MR Detection of Hippocampal Disease in Epilepsy: Factors Influencing T2 Relaxation Time R. A. Grunewald, G. D. Jackson, A. Connelly, and J. S. Duncan PURPOSE: To assess the reproducibility and stability
MR Detection of Hippocampal Disease in Epilepsy: Factors Influencing T2 Relaxation Time R. A. Grunewald, G. D. Jackson, A. Connelly, and J. S. Duncan PURPOSE: To assess the reproducibility and stability
Cerebral MRI as an important diagnostic tool in temporal lobe epilepsy
 Cerebral MRI as an important diagnostic tool in temporal lobe epilepsy Poster No.: C-2190 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Puiu, D. Negru; Iasi/RO Keywords: Neuroradiology brain,
Cerebral MRI as an important diagnostic tool in temporal lobe epilepsy Poster No.: C-2190 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Puiu, D. Negru; Iasi/RO Keywords: Neuroradiology brain,
Increased Anterior Temporal Lobe T2 Times in Cases of Hippocampal Sclerosis: A Multi-Echo T2 Relaxometry Study At 3 T
 AJNR Am J Neuroradiol 25:389 394, March 2004 Increased Anterior Temporal Lobe T2 Times in Cases of Hippocampal Sclerosis: A Multi-Echo T2 Relaxometry Study At 3 T Regula S. Briellmann, Ari Syngeniotis,
AJNR Am J Neuroradiol 25:389 394, March 2004 Increased Anterior Temporal Lobe T2 Times in Cases of Hippocampal Sclerosis: A Multi-Echo T2 Relaxometry Study At 3 T Regula S. Briellmann, Ari Syngeniotis,
Value of Single-Voxel Proton MR Spectroscopy in Temporal Lobe Epilepsy
 Value of Single-Voxel Proton MR Spectroscopy in Temporal Lobe Epilepsy Eric Achten, Paul Boon, Tom Van De Kerckhove, Jacques Caemaert, Jacques De Reuck, and Marc Kunnen PURPOSE: To study the value of different
Value of Single-Voxel Proton MR Spectroscopy in Temporal Lobe Epilepsy Eric Achten, Paul Boon, Tom Van De Kerckhove, Jacques Caemaert, Jacques De Reuck, and Marc Kunnen PURPOSE: To study the value of different
Early detection of abnormalities in partial epilepsy
 104 Institute of Child Health and Hospital for Sick Children, London, Neurosciences Unit J H Cross G D Jackson B G R Neville F J Kirkham Radiology and Physics Unit A Connelly D G Gadian Department of Clinical
104 Institute of Child Health and Hospital for Sick Children, London, Neurosciences Unit J H Cross G D Jackson B G R Neville F J Kirkham Radiology and Physics Unit A Connelly D G Gadian Department of Clinical
Role of magnetic resonance imaging for preoperative evaluation of patients with refractory epilepsy
 ACF Hui JMK Lam YL Chan KM Au-Yeung KS Wong R Kay WS Poon Key words: Epilepsy; Magnetic resonance imaging; Surgery "# Hong Kong Med J 2003;9:20-4 The Chinese University of Hong Kong, Prince of Wales Hospital,
ACF Hui JMK Lam YL Chan KM Au-Yeung KS Wong R Kay WS Poon Key words: Epilepsy; Magnetic resonance imaging; Surgery "# Hong Kong Med J 2003;9:20-4 The Chinese University of Hong Kong, Prince of Wales Hospital,
A study of the relationship between metabolism using 1 H-MRS and function using several neuropsychological
 Seizure 2001; 10: 188 193 doi:10.1053/seiz.2000.0498, available online at http://www.idealibrary.com on A study of the relationship between metabolism using 1 H-MRS and function using several neuropsychological
Seizure 2001; 10: 188 193 doi:10.1053/seiz.2000.0498, available online at http://www.idealibrary.com on A study of the relationship between metabolism using 1 H-MRS and function using several neuropsychological
Clinical Study Qualitative and Quantitative Hippocampal MRI Assessments in Intractable Epilepsy
 BioMed Research International Volume 2013, Article ID 480524, 9 pages http://dx.doi.org/10.1155/2013/480524 Clinical Study Qualitative and Quantitative Hippocampal MRI Assessments in Intractable Epilepsy
BioMed Research International Volume 2013, Article ID 480524, 9 pages http://dx.doi.org/10.1155/2013/480524 Clinical Study Qualitative and Quantitative Hippocampal MRI Assessments in Intractable Epilepsy
Magnetic Resonance Imaging of Mesial Temporal Sclerosis (MTS): What radiologists ought to know?
: What radiologists ought to know?") Magnetic Resonance Imaging of Mesial Temporal Sclerosis (MTS): What radiologists ought to know? Poster No.: C-0856 Congress: ECR 2012 Type: Educational Exhibit Authors: P. Singh, G. Mittal, R. Kaur, K.
Magnetic Resonance Imaging of Mesial Temporal Sclerosis (MTS): What radiologists ought to know? Poster No.: C-0856 Congress: ECR 2012 Type: Educational Exhibit Authors: P. Singh, G. Mittal, R. Kaur, K.
Measurements of Hippocampal Volume Using Magnetic Resonance Imaging in Sudanese Population
 International Journal Dental and Medical Sciences Research (IJDMSR) ISSN: 9-7X Volume, Issue 8 (Aug- 8), PP 6- Measurements of Hippocampal Volume Using Magnetic Resonance Imaging in Sudanese Population
International Journal Dental and Medical Sciences Research (IJDMSR) ISSN: 9-7X Volume, Issue 8 (Aug- 8), PP 6- Measurements of Hippocampal Volume Using Magnetic Resonance Imaging in Sudanese Population
Brain Structure and Epilepsy: The Impact of Modern Imaging
 Commentary Brain Structure and Epilepsy: The Impact of Modern Imaging Frederick Andermann, Professor of Neurology and Paediatrics, Department of Neurology and Neurosurgery, McGill University, Montreal,
Commentary Brain Structure and Epilepsy: The Impact of Modern Imaging Frederick Andermann, Professor of Neurology and Paediatrics, Department of Neurology and Neurosurgery, McGill University, Montreal,
Frontal Contributions to Memory Encoding Before and After Unilateral Medial Temporal Lobectomy
 Frontal Contributions to Memory Encoding Before and After Unilateral Medial Temporal Lobectomy Jeff Ojemann, MD Department of Neurological Surgery University of Washington Children s Hospital & Regional
Frontal Contributions to Memory Encoding Before and After Unilateral Medial Temporal Lobectomy Jeff Ojemann, MD Department of Neurological Surgery University of Washington Children s Hospital & Regional
MR and Positron Emission Tomography in the Diagnosis of Surgically Correctable Temporal Lobe Epilepsy
 MR and Positron Emission Tomography in the Diagnosis of Surgically Correctable Temporal Lobe Epilepsy R. Heinz, N. Ferris, E. K. Lee, R. Radtke, B. Crain, J. M. Hoffman, M. Hanson, S. Paine, and A. Friedman
MR and Positron Emission Tomography in the Diagnosis of Surgically Correctable Temporal Lobe Epilepsy R. Heinz, N. Ferris, E. K. Lee, R. Radtke, B. Crain, J. M. Hoffman, M. Hanson, S. Paine, and A. Friedman
Multimodal Imaging in Extratemporal Epilepsy Surgery
 Open Access Case Report DOI: 10.7759/cureus.2338 Multimodal Imaging in Extratemporal Epilepsy Surgery Christian Vollmar 1, Aurelia Peraud 2, Soheyl Noachtar 1 1. Epilepsy Center, Dept. of Neurology, University
Open Access Case Report DOI: 10.7759/cureus.2338 Multimodal Imaging in Extratemporal Epilepsy Surgery Christian Vollmar 1, Aurelia Peraud 2, Soheyl Noachtar 1 1. Epilepsy Center, Dept. of Neurology, University
Neuropsychological Evaluation in Epilepsy Surgery
 Epilrpsia, 38(Suppl. 4):SlS-S23, 1997 Lippincott-Raven Publishers, Philadelphia 0 International League Against Epilepsy Neuropsychological Evaluation in Epilepsy Surgery David W. Loring Department of Neurology,
Epilrpsia, 38(Suppl. 4):SlS-S23, 1997 Lippincott-Raven Publishers, Philadelphia 0 International League Against Epilepsy Neuropsychological Evaluation in Epilepsy Surgery David W. Loring Department of Neurology,
ORIGINAL CONTRIBUTION. Ictal Fear in Temporal Lobe Epilepsy
 ORIGINAL CONTRIBUTION Ictal Fear in Temporal Lobe Epilepsy Surgical Outcome and Focal Hippocampal Changes Revealed by Proton Magnetic Resonance Spectroscopy Imaging Michael Feichtinger, MD; Elisabeth Pauli,
ORIGINAL CONTRIBUTION Ictal Fear in Temporal Lobe Epilepsy Surgical Outcome and Focal Hippocampal Changes Revealed by Proton Magnetic Resonance Spectroscopy Imaging Michael Feichtinger, MD; Elisabeth Pauli,
Correlation of Apparent Diffusion Coefficient with Neuropsychological Testing in Temporal Lobe Epilepsy
 AJNR Am J Neuroradiol 26:1832 1839, August 2005 Correlation of Apparent Diffusion Coefficient with Neuropsychological Testing in Temporal Lobe Epilepsy Yvonne W. Lui, Annette O. Nusbaum, William B. Barr,
AJNR Am J Neuroradiol 26:1832 1839, August 2005 Correlation of Apparent Diffusion Coefficient with Neuropsychological Testing in Temporal Lobe Epilepsy Yvonne W. Lui, Annette O. Nusbaum, William B. Barr,
A Hippocampal Lesion Detected by High-Field 3 Tesla Magnetic Resonance Imaging in a Patient with Temporal Lobe Epilepsy
 Tohoku J. Exp. Med., 2005, A Hippocampal 205, 287-291 Lesion Detected by High Field 3 T MRI 287 A Hippocampal Lesion Detected by High-Field 3 Tesla Magnetic Resonance Imaging in a Patient with Temporal
Tohoku J. Exp. Med., 2005, A Hippocampal 205, 287-291 Lesion Detected by High Field 3 T MRI 287 A Hippocampal Lesion Detected by High-Field 3 Tesla Magnetic Resonance Imaging in a Patient with Temporal
Association between Size of the Lateral Ventricle and Asymmetry of the Fornix in Patients with Temporal Lobe Epilepsy
 AJNR Am J Neuroradiol 19:9 13, January 1998 Association between Size of the Lateral Ventricle and Asymmetry of the Fornix in Patients with Temporal Lobe Epilepsy Alexander C. Mamourian, Charles H. Cho,
AJNR Am J Neuroradiol 19:9 13, January 1998 Association between Size of the Lateral Ventricle and Asymmetry of the Fornix in Patients with Temporal Lobe Epilepsy Alexander C. Mamourian, Charles H. Cho,
Fernando Cendes, MD, PhD,* Zografos Caramanos, MA, Frederick Andermann, MD, FranGois Dubeau, MD, and Douglas L. Arnold, MD
 P Proton Magnetic Resonance Spectroscopic Imaging and Magnetic Resonance Imaging Volumetry in the Lateralization of Temporal Lobe Epilepsy: A Series of 100 Patiekts Fernando Cendes, MD, PhD,* Zografos
P Proton Magnetic Resonance Spectroscopic Imaging and Magnetic Resonance Imaging Volumetry in the Lateralization of Temporal Lobe Epilepsy: A Series of 100 Patiekts Fernando Cendes, MD, PhD,* Zografos
Surgery in temporal lobe epilepsy patients without cranial MRI lateralization
 Acta neurol. belg., 2006, 106, 9-14 Surgery in temporal lobe epilepsy patients without cranial MRI lateralization Y. B. GOMCELI 1, A. ERDEM 2, E. BILIR 3, G. KUTLU 1, S. KURT 4, E. ERDEN 5,A. KARATAS 2,
Acta neurol. belg., 2006, 106, 9-14 Surgery in temporal lobe epilepsy patients without cranial MRI lateralization Y. B. GOMCELI 1, A. ERDEM 2, E. BILIR 3, G. KUTLU 1, S. KURT 4, E. ERDEN 5,A. KARATAS 2,
PRESURGICAL EVALUATION. ISLAND OF COS Hippocrates: On the Sacred Disease. Disclosure Research-Educational Grants. Patients with seizure disorders
 PRESURGICAL EVALUATION Patients with seizure disorders Gregory D. Cascino, MD Mayo Clinic Disclosure Research-Educational Grants Mayo Foundation Neuro Pace, Inc. American Epilepsy Society American Academy
PRESURGICAL EVALUATION Patients with seizure disorders Gregory D. Cascino, MD Mayo Clinic Disclosure Research-Educational Grants Mayo Foundation Neuro Pace, Inc. American Epilepsy Society American Academy
Standard magnetic resonance imaging is inadequate for patients with refractory focal epilepsy
 PAPER Standard magnetic resonance imaging is inadequate for patients with refractory focal epilepsy J von Oertzen, H Urbach, S Jungbluth, M Kurthen, M Reuber, G Fernández, C E Elger... See Editorial Commentary
PAPER Standard magnetic resonance imaging is inadequate for patients with refractory focal epilepsy J von Oertzen, H Urbach, S Jungbluth, M Kurthen, M Reuber, G Fernández, C E Elger... See Editorial Commentary
Single-Voxel Proton MR Spectroscopy and Positron Emission Tomography for Lateralization of Refractory Temporal Lobe Epilepsy
 AJNR Am J Neuroradiol 19:1 8, January 1998 Single-Voxel Proton MR Spectroscopy and Positron Emission Tomography for Lateralization of Refractory Temporal Lobe Epilepsy Eric Achten, Patrick Santens, Paul
AJNR Am J Neuroradiol 19:1 8, January 1998 Single-Voxel Proton MR Spectroscopy and Positron Emission Tomography for Lateralization of Refractory Temporal Lobe Epilepsy Eric Achten, Patrick Santens, Paul
Temporal lobe epilepsy (TLE) is the most common type of
 is the most common type of") Differential Features of Metabolic Abnormalities Between Medial and Lateral Temporal Lobe Epilepsy: Quantitative Analysis of F-FDG PET Using SPM Yu Kyeong Kim, MD 1 ; Dong Soo Lee, MD, PhD 1 ; Sang Kun
Differential Features of Metabolic Abnormalities Between Medial and Lateral Temporal Lobe Epilepsy: Quantitative Analysis of F-FDG PET Using SPM Yu Kyeong Kim, MD 1 ; Dong Soo Lee, MD, PhD 1 ; Sang Kun
Cerebral structural lesions are found in approximately. Surgery of Intractable Temporal Lobe Epilepsy Presented with Structural Lesions
 Original Article J Chin Med Assoc 2003;66:565-571 Surgery of Intractable Temporal Lobe Epilepsy Presented with Structural Lesions Yang-Hsin Shih 1 Jiang-Fong Lirng 2 Der-Jen Yen 3 Donald M. Ho 4 Chun-Hing
Original Article J Chin Med Assoc 2003;66:565-571 Surgery of Intractable Temporal Lobe Epilepsy Presented with Structural Lesions Yang-Hsin Shih 1 Jiang-Fong Lirng 2 Der-Jen Yen 3 Donald M. Ho 4 Chun-Hing
Pharmacoresistant temporal lobe epilepsy - a diagnostic performance of standardized MRI protocol in detection of epileptogenic lesion
 Pharmacoresistant temporal lobe epilepsy - a diagnostic performance of standardized MRI protocol in detection of epileptogenic lesion Poster No.: C-2226 Congress: ECR 2013 Type: Scientific Exhibit Authors:
Pharmacoresistant temporal lobe epilepsy - a diagnostic performance of standardized MRI protocol in detection of epileptogenic lesion Poster No.: C-2226 Congress: ECR 2013 Type: Scientific Exhibit Authors:
The Clinical and Electrophysiological Characteristics of Temporal Lobe Epilepsy with Normal MRI
 Journal of Clinical Neurology / Volume 2 / March, 2006 Original Articles The Clinical and Electrophysiological Characteristics of Temporal Lobe Epilepsy with Normal MRI S.E. Kim, M.D., Ph.D., F. Andermann,
Journal of Clinical Neurology / Volume 2 / March, 2006 Original Articles The Clinical and Electrophysiological Characteristics of Temporal Lobe Epilepsy with Normal MRI S.E. Kim, M.D., Ph.D., F. Andermann,
The Low Sensitivity of Fluid-Attenuated Inversion-Recovery MR in the Detection of Multiple Sclerosis of the Spinal Cord
 The Low Sensitivity of Fluid-Attenuated Inversion-Recovery MR in the Detection of Multiple Sclerosis of the Spinal Cord Mark D. Keiper, Robert I. Grossman, John C. Brunson, and Mitchell D. Schnall PURPOSE:
The Low Sensitivity of Fluid-Attenuated Inversion-Recovery MR in the Detection of Multiple Sclerosis of the Spinal Cord Mark D. Keiper, Robert I. Grossman, John C. Brunson, and Mitchell D. Schnall PURPOSE:
Hamartomas and epilepsy: clinical and imaging characteristics
 Seizure 2003; 12: 307 311 doi:10.1016/s1059 1311(02)00272-8 Hamartomas and epilepsy: clinical and imaging characteristics B. DIEHL, R. PRAYSON, I. NAJM & P. RUGGIERI Departments of Neurology, Pathology
Seizure 2003; 12: 307 311 doi:10.1016/s1059 1311(02)00272-8 Hamartomas and epilepsy: clinical and imaging characteristics B. DIEHL, R. PRAYSON, I. NAJM & P. RUGGIERI Departments of Neurology, Pathology
Proton MR Spectroscopy in Patients with Acute Temporal Lobe Seizures
 AJN Am J Neuroradiol 22:152 157, January 2001 Proton M Spectroscopy in Patients with Acute Temporal obe Seizures Mauricio Castillo, J. Keith Smith, and ester Kwock BACKGOUND AND PUPOSE: Decreases in N-acetyl
AJN Am J Neuroradiol 22:152 157, January 2001 Proton M Spectroscopy in Patients with Acute Temporal obe Seizures Mauricio Castillo, J. Keith Smith, and ester Kwock BACKGOUND AND PUPOSE: Decreases in N-acetyl
Comparative Analysis of MR Imaging, Positron Emission Tomography, and Ictal Single-photon Emission CT in Patients with Neocortical Epilepsy
 AJNR Am J Neuroradiol 22:937 946, May 2001 Comparative Analysis of MR Imaging, Positron Emission Tomography, and Ictal Single-photon Emission CT in Patients with Neocortical Epilepsy Sung-Il Hwang, Jae
AJNR Am J Neuroradiol 22:937 946, May 2001 Comparative Analysis of MR Imaging, Positron Emission Tomography, and Ictal Single-photon Emission CT in Patients with Neocortical Epilepsy Sung-Il Hwang, Jae
Theroleofclinicalin vivo 1H-MR spectroscopy in the evaluation of epilepsies
 Spectroscopy 16 (2002) 297 306 297 IOS Press Theroleofclinicalin vivo 1H-MR spectroscopy in the evaluation of epilepsies T. Hammen a,,h.stefan a and B. Tomandl b a Clinics of Neurology Center Epilepsy,
Spectroscopy 16 (2002) 297 306 297 IOS Press Theroleofclinicalin vivo 1H-MR spectroscopy in the evaluation of epilepsies T. Hammen a,,h.stefan a and B. Tomandl b a Clinics of Neurology Center Epilepsy,
NIH Public Access Author Manuscript Epilepsia. Author manuscript; available in PMC 2010 March 18.
 NIH Public Access Author Manuscript Published in final edited form as: Epilepsia. 2009 September ; 50(9): 2053 2060. doi:10.1111/j.1528-1167.2009.02079.x. Epilepsy surgery outcomes in temporal lobe epilepsy
NIH Public Access Author Manuscript Published in final edited form as: Epilepsia. 2009 September ; 50(9): 2053 2060. doi:10.1111/j.1528-1167.2009.02079.x. Epilepsy surgery outcomes in temporal lobe epilepsy
Electro-clinical manifestations of the epilepsy associated to the different anatomical variants of hypothalamic hamartomas
 Electro-clinical manifestations of the epilepsy associated to the different anatomical variants of hypothalamic hamartomas Alberto JR Leal Hospital Fernando Fonseca, Dep. Neurology Lisbon. Abstract Objective
Electro-clinical manifestations of the epilepsy associated to the different anatomical variants of hypothalamic hamartomas Alberto JR Leal Hospital Fernando Fonseca, Dep. Neurology Lisbon. Abstract Objective
Prediction of Seizure-onset Laterality by Using Wada Memory Asymmetries in Pediatric Epilepsy Surgery Candidates
 Epilepsia, 43(9):1049 1055, 2002 Blackwell Publishing, Inc. International League Against Epilepsy Prediction of Seizure-onset Laterality by Using Wada Memory Asymmetries in Pediatric Epilepsy Surgery Candidates
Epilepsia, 43(9):1049 1055, 2002 Blackwell Publishing, Inc. International League Against Epilepsy Prediction of Seizure-onset Laterality by Using Wada Memory Asymmetries in Pediatric Epilepsy Surgery Candidates
High Resolution Ictal SPECT: Enhanced Epileptic Source Targeting?
 High Resolution Ictal SPECT: Enhanced Epileptic Source Targeting? Marvin A Rossi MD, PhD RUSH Epilepsy Center Research Lab http://www.synapticom.net Chicago, IL USA Medically-Refractory Epilepsy 500,000-800,000
High Resolution Ictal SPECT: Enhanced Epileptic Source Targeting? Marvin A Rossi MD, PhD RUSH Epilepsy Center Research Lab http://www.synapticom.net Chicago, IL USA Medically-Refractory Epilepsy 500,000-800,000
Blurring the Lines Between Lesional and Nonlesional MRI
 Current Literature In Clinical Science Blurring the Lines Between Lesional and Nonlesional MRI Blurring in Patients With Temporal Lobe Epilepsy: Clinical, High-field Imaging and Ultrastructural Study.
Current Literature In Clinical Science Blurring the Lines Between Lesional and Nonlesional MRI Blurring in Patients With Temporal Lobe Epilepsy: Clinical, High-field Imaging and Ultrastructural Study.
CHAPTER 5. The intracarotid amobarbital or Wada test: unilateral or bilateral?
 CHAPTER 5 Chapter 5 CHAPTER 5 The intracarotid amobarbital or Wada test: unilateral or bilateral? SG Uijl FSS Leijten JBAM Arends J Parra AC van Huffelen PC van Rijen KGM Moons Submitted 2007. 74 Abstract
CHAPTER 5 Chapter 5 CHAPTER 5 The intracarotid amobarbital or Wada test: unilateral or bilateral? SG Uijl FSS Leijten JBAM Arends J Parra AC van Huffelen PC van Rijen KGM Moons Submitted 2007. 74 Abstract
Focal hippocampal dysfunction initiates electrophysiologic seizures and impairs interictal cognition in patients with mesial temporal lobe epilepsy (T
 Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Thomas R. Henry,
Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Thomas R. Henry,
Morphometric MRI Analysis of the Parahippocampal Region in Temporal Lobe Epilepsy
 Morphometric MRI Analysis of the Parahippocampal Region in Temporal Lobe Epilepsy NEDA BERNASCONI, a ANDREA BERNASCONI, ZOGRAFOS CARAMANOS, FREDERICK ANDERMANN, FRANÇOIS DUBEAU, AND DOUGLAS L. ARNOLD Department
Morphometric MRI Analysis of the Parahippocampal Region in Temporal Lobe Epilepsy NEDA BERNASCONI, a ANDREA BERNASCONI, ZOGRAFOS CARAMANOS, FREDERICK ANDERMANN, FRANÇOIS DUBEAU, AND DOUGLAS L. ARNOLD Department
Seizure 20 (2011) Contents lists available at ScienceDirect. Seizure. journal homepage:
 Contents lists available at ScienceDirect. Seizure. journal homepage:") Seizure 20 (2011) 475 479 Contents lists available at ScienceDirect Seizure journal homepage: www.elsevier.com/locate/yseiz Medically intractable temporal lobe epilepsy in patients with normal MRI: Surgical
Seizure 20 (2011) 475 479 Contents lists available at ScienceDirect Seizure journal homepage: www.elsevier.com/locate/yseiz Medically intractable temporal lobe epilepsy in patients with normal MRI: Surgical
Multisection Proton MR Spectroscopy for Mesial Temporal Lobe Epilepsy
 AJNR Am J Neuroradiol 23:1359 1368, September 2002 Multisection Proton MR Spectroscopy for Mesial Temporal Lobe Epilepsy Arístides A. Capizzano, Peter Vermathen, Kenneth D. Laxer, Gerald B. Matson, Andrew
AJNR Am J Neuroradiol 23:1359 1368, September 2002 Multisection Proton MR Spectroscopy for Mesial Temporal Lobe Epilepsy Arístides A. Capizzano, Peter Vermathen, Kenneth D. Laxer, Gerald B. Matson, Andrew
Brain Mapping of Episodic Memory in Patients with Medial Temporal Lobe Epilepsy Using Activation Positron Emission Tomography
 Brain Mapping of Episodic Memory in Patients with Medial Temporal Lobe Epilepsy Using Activation Positron Emission Tomography Hyunwoo Nam, M.D., Sang-Kun Lee, M.D., Dong Soo Lee, M.D.*, Jae Sung Lee, M.S.*,
Brain Mapping of Episodic Memory in Patients with Medial Temporal Lobe Epilepsy Using Activation Positron Emission Tomography Hyunwoo Nam, M.D., Sang-Kun Lee, M.D., Dong Soo Lee, M.D.*, Jae Sung Lee, M.S.*,
MTLE is most frequently associated with hippocampal
 Published June 10, 2010 as 10.3174/ajnr.A2154 ORIGINAL RESEARCH K.L. Howe D. Dimitri C. Heyn T.-R. Kiehl D. Mikulis T. Valiante Histologically Confirmed Hippocampal Structural Features Revealed by 3T MR
Published June 10, 2010 as 10.3174/ajnr.A2154 ORIGINAL RESEARCH K.L. Howe D. Dimitri C. Heyn T.-R. Kiehl D. Mikulis T. Valiante Histologically Confirmed Hippocampal Structural Features Revealed by 3T MR
Temporal lobe dysembryoplastic neuroepithelial tumour: significance of discordant interictal spikes
 Original article Epileptic Disord 2004; 6: 10-14 Temporal lobe dysembryoplastic neuroepithelial tumour: significance of discordant interictal spikes Angelo Labate 1, Regula S. Briellmann 1,6, Anthony S.
Original article Epileptic Disord 2004; 6: 10-14 Temporal lobe dysembryoplastic neuroepithelial tumour: significance of discordant interictal spikes Angelo Labate 1, Regula S. Briellmann 1,6, Anthony S.
PET and SPECT in Epilepsy
 PET and SPECT in Epilepsy 12.6.2013 William H Theodore MD Chief, Clinical Epilepsy Section NINDS NIH Bethesda MD American Epilepsy Society Annual Meeting Disclosures Entity DIR NINDS NIH Elsevier Individual
PET and SPECT in Epilepsy 12.6.2013 William H Theodore MD Chief, Clinical Epilepsy Section NINDS NIH Bethesda MD American Epilepsy Society Annual Meeting Disclosures Entity DIR NINDS NIH Elsevier Individual
doi: /brain/awq006 Brain 2010: 133; Imaging memory in temporal lobe epilepsy: predicting the effects of temporal lobe resection
 doi:10.1093/brain/awq006 Brain 2010: 133; 1186 1199 1186 BRAIN A JOURNAL OF NEUROLOGY Imaging memory in temporal lobe epilepsy: predicting the effects of temporal lobe resection Silvia B. Bonelli, 1,2
doi:10.1093/brain/awq006 Brain 2010: 133; 1186 1199 1186 BRAIN A JOURNAL OF NEUROLOGY Imaging memory in temporal lobe epilepsy: predicting the effects of temporal lobe resection Silvia B. Bonelli, 1,2
EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG MONITORING. Meriem Bensalem-Owen, MD University of Kentucky
 EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG MONITORING Meriem Bensalem-Owen, MD University of Kentucky DISCLOSURES Received grants for sponsored research as investigator from: UCB Eisai
EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG MONITORING Meriem Bensalem-Owen, MD University of Kentucky DISCLOSURES Received grants for sponsored research as investigator from: UCB Eisai
Epilepsy surgery. John S Duncan. Who are candidates for epilepsy surgery? The context of epilepsy surgery ORIGINAL PAPERS
 ORIGINAL PAPERS Epilepsy surgery John S Duncan ABSTRACT If the first two or three antiepileptic drugs used do not control epilepsy, there is little chance that subsequent medications will be effective.
ORIGINAL PAPERS Epilepsy surgery John S Duncan ABSTRACT If the first two or three antiepileptic drugs used do not control epilepsy, there is little chance that subsequent medications will be effective.
For reprint orders, please contact Expert Rev. Neurotherapeutics 3(6), (2003)
, (2003)") Review For reprint orders, please contact reprints@future-drugs.com CONTENTS Epidemiology Etiology & pathogenesis Clinical features Diagnostic evaluation Treatment & outcome Medically refractory medial
Review For reprint orders, please contact reprints@future-drugs.com CONTENTS Epidemiology Etiology & pathogenesis Clinical features Diagnostic evaluation Treatment & outcome Medically refractory medial
ORIGINAL CONTRIBUTION
 ORIGINAL CONTRIBUTION Electroencephalographic, Volumetric, and Neuropsychological Indicators of Seizure Focus Lateralization in Temporal Lobe Epilepsy David J. Moser, PhD; Russell M. Bauer, PhD; Robin
ORIGINAL CONTRIBUTION Electroencephalographic, Volumetric, and Neuropsychological Indicators of Seizure Focus Lateralization in Temporal Lobe Epilepsy David J. Moser, PhD; Russell M. Bauer, PhD; Robin
9/30/2016. Advances in Epilepsy Surgery. Epidemiology. Epidemiology
 Advances in Epilepsy Surgery George Jallo, M.D. Director, Institute for Brain Protection Sciences Johns Hopkins All Children s Hospital St Petersburg, Florida Epidemiology WHO lists it as the second most
Advances in Epilepsy Surgery George Jallo, M.D. Director, Institute for Brain Protection Sciences Johns Hopkins All Children s Hospital St Petersburg, Florida Epidemiology WHO lists it as the second most
Age at onset in patients with medically refractory. temporal lobe epilepsy and mesial temporal sclerosis: impact on clinical manifestations and
 Thomas Jefferson University Jefferson Digital Commons Department of Neurology Faculty Papers Department of Neurology 8-1-2015 Age at onset in patients with medically refractory temporal lobe epilepsy and
Thomas Jefferson University Jefferson Digital Commons Department of Neurology Faculty Papers Department of Neurology 8-1-2015 Age at onset in patients with medically refractory temporal lobe epilepsy and
ORIGINAL CONTRIBUTION. Accurate Prediction of Postoperative Outcome in Mesial Temporal Lobe Epilepsy
 ORIGINAL CONTRIBUTION Accurate Prediction of Postoperative Outcome in Mesial Temporal Lobe Epilepsy A Study Using Positron Emission Tomography With 18 Fluorodeoxyglucose Sophi Dupont, MD; Frank Semah,
ORIGINAL CONTRIBUTION Accurate Prediction of Postoperative Outcome in Mesial Temporal Lobe Epilepsy A Study Using Positron Emission Tomography With 18 Fluorodeoxyglucose Sophi Dupont, MD; Frank Semah,
Spike frequency is dependent on epilepsy duration and seizure frequency in temporal lobe epilepsy
 Original article Epileptic Disord 2005; 7 (4): 355-9 Spike frequency is dependent on epilepsy duration and seizure frequency in temporal lobe epilepsy Jozsef Janszky 1,2,3, M. Hoppe 1, Z. Clemens 3, I.
Original article Epileptic Disord 2005; 7 (4): 355-9 Spike frequency is dependent on epilepsy duration and seizure frequency in temporal lobe epilepsy Jozsef Janszky 1,2,3, M. Hoppe 1, Z. Clemens 3, I.
Clinical utility of 11C-flumazenil positron emission tomography in intractable temporal lobe epilepsy
 Original Article Clinical utility of C-flumazenil positron emission tomography in intractable temporal lobe epilepsy M. V. Padma, Robert Simkins, Phillip White, Martin Satter*, Brad T. Christian*, Kelly
Original Article Clinical utility of C-flumazenil positron emission tomography in intractable temporal lobe epilepsy M. V. Padma, Robert Simkins, Phillip White, Martin Satter*, Brad T. Christian*, Kelly
Long-term and late seizure outcome after surgery for temporal lobe epilepsy
 Original article Epileptic Disord 2010; 12 (1): 54-8 Long-term and late seizure outcome after surgery for temporal lobe epilepsy José Pimentel 1, Carla Bentes 1,2, Alexandre Campos 3, A. Gonçalves Ferreira
Original article Epileptic Disord 2010; 12 (1): 54-8 Long-term and late seizure outcome after surgery for temporal lobe epilepsy José Pimentel 1, Carla Bentes 1,2, Alexandre Campos 3, A. Gonçalves Ferreira
Epilepsy Surgery: Who should be considered? How will patients do? Bassel Abou-Khalil, M.D.
 Epilepsy Surgery: Who should be considered? How will patients do? Bassel Abou-Khalil, M.D. Disclosures none Self-assessment questions Q1- Which qualify for drug resistance in focal epilepsy? A. Failure
Epilepsy Surgery: Who should be considered? How will patients do? Bassel Abou-Khalil, M.D. Disclosures none Self-assessment questions Q1- Which qualify for drug resistance in focal epilepsy? A. Failure
Hippocampal MRI Signal Hyperintensity After Febrile Status Epilepticus Is Predictive of Subsequent Mesial Temporal Sclerosis
 Neuroradiology Original Research Provenzale et al. Hippocampal MRI Signal After Febrile Status Epilepticus Neuroradiology Original Research James M. Provenzale 1 Daniel P. Barboriak Kevan VanLandingham
Neuroradiology Original Research Provenzale et al. Hippocampal MRI Signal After Febrile Status Epilepticus Neuroradiology Original Research James M. Provenzale 1 Daniel P. Barboriak Kevan VanLandingham
Memory function decline over 18 months after selective amygdalohippocampectomy
 Original article Epileptic Disord 2004; 6: 115-20 Memory function decline over 18 months after selective amygdalohippocampectomy Tatsuya Ogino 1, Yoko Ohtsuka 1, Yumiko Ido 2, Yoshiaki Mayanagi 3, Eiju
Original article Epileptic Disord 2004; 6: 115-20 Memory function decline over 18 months after selective amygdalohippocampectomy Tatsuya Ogino 1, Yoko Ohtsuka 1, Yumiko Ido 2, Yoshiaki Mayanagi 3, Eiju
Author's response to reviews
 Author's response to reviews Title: MRI-negative PET-positive Temporal Lobe Epilepsy (TLE) and Mesial TLE differ with Quantitative MRI and PET: a case control study Authors: Ross P Carne (carnero@svhm.org.au)
Author's response to reviews Title: MRI-negative PET-positive Temporal Lobe Epilepsy (TLE) and Mesial TLE differ with Quantitative MRI and PET: a case control study Authors: Ross P Carne (carnero@svhm.org.au)
Temporal Lobe Epilepsy: The Various MR Appearances of Histologically Proven Mesial Temporal Sclerosis
 Temporal Lobe Epilepsy: The Various MR Appearances of Histologically Proven Mesial Temporal Sclerosis Linda C. Meiners, Ad van Gils, Gerard H. Jansen, Gerard de Kort, Theo D. Witkamp, Uno M. P. Ramos,
Temporal Lobe Epilepsy: The Various MR Appearances of Histologically Proven Mesial Temporal Sclerosis Linda C. Meiners, Ad van Gils, Gerard H. Jansen, Gerard de Kort, Theo D. Witkamp, Uno M. P. Ramos,
Neuroimaging in Investigation of Patients With Epilepsy Fernando Cendes, MD, PhD
 Review Article Neuroimaging in Investigation of Patients With Epilepsy Fernando Cendes, MD, PhD ABSTRACT Purpose of Review: This review discusses the MRI and functional imaging findings in patients with
Review Article Neuroimaging in Investigation of Patients With Epilepsy Fernando Cendes, MD, PhD ABSTRACT Purpose of Review: This review discusses the MRI and functional imaging findings in patients with
HHS Public Access Author manuscript J Neuroimaging. Author manuscript; available in PMC 2016 May 01.
 Hippocampal surface deformation accuracy in T-1 weighted volumetric MRI sequences in subjects with epilepsy R. Edward Hogan, M.D., Emily D. Moseley, B.S., and Luigi Maccotta, M.D., Ph.D. Department of
Hippocampal surface deformation accuracy in T-1 weighted volumetric MRI sequences in subjects with epilepsy R. Edward Hogan, M.D., Emily D. Moseley, B.S., and Luigi Maccotta, M.D., Ph.D. Department of
Postoperative routine EEG correlates with long-term seizure outcome after epilepsy surgery
 Seizure (2005) 14, 446 451 www.elsevier.com/locate/yseiz Postoperative routine EEG correlates with long-term seizure outcome after epilepsy surgery Michelle Hildebrandt a, Reinhard Schulz b, Matthias Hoppe
Seizure (2005) 14, 446 451 www.elsevier.com/locate/yseiz Postoperative routine EEG correlates with long-term seizure outcome after epilepsy surgery Michelle Hildebrandt a, Reinhard Schulz b, Matthias Hoppe
Value of MRI in the Evaluation of Patients with Seizures: An Illustrative Case
 ISPUB.COM The Internet Journal of Neurology Volume 7 Number 1 Value of MRI in the Evaluation of Patients with Seizures: An Illustrative Case Y Patel, H Pinkert, M Kaufman Citation Y Patel, H Pinkert, M
ISPUB.COM The Internet Journal of Neurology Volume 7 Number 1 Value of MRI in the Evaluation of Patients with Seizures: An Illustrative Case Y Patel, H Pinkert, M Kaufman Citation Y Patel, H Pinkert, M
Nonverbal memory functioning following right anterior temporal lobectomy: a meta-analytic review
 Seizure (2004) 13, 446 452 REVIEW Nonverbal memory functioning following right anterior temporal lobectomy: a meta-analytic review Stephanie A.McDermid Vaz* Department of Psychology, York University, 4700
Seizure (2004) 13, 446 452 REVIEW Nonverbal memory functioning following right anterior temporal lobectomy: a meta-analytic review Stephanie A.McDermid Vaz* Department of Psychology, York University, 4700
Diffusion Tensor Imaging 12/06/2013
 12/06/2013 Beate Diehl, MD PhD FRCP University College London National Hospital for Neurology and Neurosurgery Queen Square London, UK American Epilepsy Society Annual Meeting Disclosure None Learning
12/06/2013 Beate Diehl, MD PhD FRCP University College London National Hospital for Neurology and Neurosurgery Queen Square London, UK American Epilepsy Society Annual Meeting Disclosure None Learning
Accepted Manuscript. Editorial. Responsive neurostimulation for epilepsy: more than stimulation. Jayant N. Acharya
 Accepted Manuscript Editorial Responsive neurostimulation for epilepsy: more than stimulation Jayant N. Acharya PII: S2467-981X(18)30022-2 DOI: https://doi.org/10.1016/j.cnp.2018.06.002 Reference: CNP
Accepted Manuscript Editorial Responsive neurostimulation for epilepsy: more than stimulation Jayant N. Acharya PII: S2467-981X(18)30022-2 DOI: https://doi.org/10.1016/j.cnp.2018.06.002 Reference: CNP
Neuropsychological Changes After Surgical Treatment for Temporal Lobe Epilepsy
 Epilepsia, 42(Suppl. 6):4 8, 2001 Blackwell Science, Inc. International League Against Epilepsy Symposium I Neuropsychological Changes After Surgical Treatment for Temporal Lobe Epilepsy *Manabu Wachi,
Epilepsia, 42(Suppl. 6):4 8, 2001 Blackwell Science, Inc. International League Against Epilepsy Symposium I Neuropsychological Changes After Surgical Treatment for Temporal Lobe Epilepsy *Manabu Wachi,
Subject: Magnetoencephalography/Magnetic Source Imaging
 01-95805-16 Original Effective Date: 09/01/01 Reviewed: 07/26/18 Revised: 08/15/18 Subject: Magnetoencephalography/Magnetic Source Imaging THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION,
01-95805-16 Original Effective Date: 09/01/01 Reviewed: 07/26/18 Revised: 08/15/18 Subject: Magnetoencephalography/Magnetic Source Imaging THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION,
Some epilepsy syndromes are known to be associated with more adverse cognitive consequences than others.
 1 Neuropsychology and Epilepsy David W. Loring, Ph.D. Departments of Neurology and Clinical & Health Psychology University of Florida Gainesville, Florida 32610-0236 0236 2 Factors Affecting Cognitive
1 Neuropsychology and Epilepsy David W. Loring, Ph.D. Departments of Neurology and Clinical & Health Psychology University of Florida Gainesville, Florida 32610-0236 0236 2 Factors Affecting Cognitive
Temporal lobe epilepsy represents the most common type of. Mesial Temporal Sclerosis: Accuracy of NeuroQuant versus Neuroradiologist
 Published April 23, 2015 as 10.3174/ajnr.A4313 PRACTICE PERSPECTIVES Mesial Temporal Sclerosis: Accuracy of NeuroQuant versus Neuroradiologist M. Azab, M. Carone, S.H. Ying, and D.M. Yousem ABSTRACT BACKGROUND
Published April 23, 2015 as 10.3174/ajnr.A4313 PRACTICE PERSPECTIVES Mesial Temporal Sclerosis: Accuracy of NeuroQuant versus Neuroradiologist M. Azab, M. Carone, S.H. Ying, and D.M. Yousem ABSTRACT BACKGROUND
Intracranial Studies Of Human Epilepsy In A Surgical Setting
 Intracranial Studies Of Human Epilepsy In A Surgical Setting Department of Neurology David Geffen School of Medicine at UCLA Presentation Goals Epilepsy and seizures Basics of the electroencephalogram
Intracranial Studies Of Human Epilepsy In A Surgical Setting Department of Neurology David Geffen School of Medicine at UCLA Presentation Goals Epilepsy and seizures Basics of the electroencephalogram
Imaging in Epilepsy. Nucharin Supakul, MD Ramathibodi Hospital, Mahidol University August 22, 2015
 Imaging in Epilepsy Nucharin Supakul, MD Ramathibodi Hospital, Mahidol University August 22, 2015 Nothing to disclose Outline Role of Imaging and pitfalls Imaging protocol Case scenarios Clinical & Electrophysiologic
Imaging in Epilepsy Nucharin Supakul, MD Ramathibodi Hospital, Mahidol University August 22, 2015 Nothing to disclose Outline Role of Imaging and pitfalls Imaging protocol Case scenarios Clinical & Electrophysiologic
Influence of the type of initial precipitating injury and at what age it occurs on course and outcome in patients with temporal lobe seizures
 J Neurosurg 82:220 227, 1995 Influence of the type of initial precipitating injury and at what age it occurs on course and outcome in patients with temporal lobe seizures GARY W. MATHERN, M.D., JAMES K.
J Neurosurg 82:220 227, 1995 Influence of the type of initial precipitating injury and at what age it occurs on course and outcome in patients with temporal lobe seizures GARY W. MATHERN, M.D., JAMES K.
Normalised MRI Volumetry of the Hippocampus among Normal Malay Children and Adolescents
 Original Article Normalised MRI Volumetry of the Hippocampus among Normal Malay Children and Adolescents Win Mar @ Salmah Jalaluddin 1, Norhasiza Mat Jusoh 1, Izzat Abdulla Ali Basahai 1, Mohd Shafie Abdullah
Original Article Normalised MRI Volumetry of the Hippocampus among Normal Malay Children and Adolescents Win Mar @ Salmah Jalaluddin 1, Norhasiza Mat Jusoh 1, Izzat Abdulla Ali Basahai 1, Mohd Shafie Abdullah
and MR Imaging Findings in Rasmussen Encephalitis
 AJNR Am J Neuroradiol 22:1291 1299, August 2001 18 F-Fluorodeoxyglucose Positron Emission Tomography and MR Imaging Findings in Rasmussen Encephalitis David J. Fiorella, James M. Provenzale, R. Edward
AJNR Am J Neuroradiol 22:1291 1299, August 2001 18 F-Fluorodeoxyglucose Positron Emission Tomography and MR Imaging Findings in Rasmussen Encephalitis David J. Fiorella, James M. Provenzale, R. Edward
Group, University Department of Clinical Neurology, Queen Square, London WC1N 3BG, UK
 braini0204 Brain (1997), 120, 339 377 INVITED REVIEW Imaging and epilepsy John S. Duncan Epilepsy Research Group, University Department of Clinical Neurology, National Hospital for Neurology and Neurosurgery,
braini0204 Brain (1997), 120, 339 377 INVITED REVIEW Imaging and epilepsy John S. Duncan Epilepsy Research Group, University Department of Clinical Neurology, National Hospital for Neurology and Neurosurgery,
Presurgical Evaluation before Epilepsy Surgery
 Presurgical Evaluation before Epilepsy Surgery Epilepsy Course for Neurology Resident 2015 Kanjana Unnwongse- Wehner, MD Prasat Neurological Epilepsy Center Facts About Epilepsy & Surgery Localization-related
Presurgical Evaluation before Epilepsy Surgery Epilepsy Course for Neurology Resident 2015 Kanjana Unnwongse- Wehner, MD Prasat Neurological Epilepsy Center Facts About Epilepsy & Surgery Localization-related
Neuroimaging for Diagnosis of Psychiatric Disorders
 Psychiatric Disorder Neuroimaging for Diagnosis of Psychiatric Disorders JMAJ 45(12): 538 544, 2002 Yoshio HIRAYASU Associate Professor, Department of Neuropsychiatry Kyorin University School of Medicine
Psychiatric Disorder Neuroimaging for Diagnosis of Psychiatric Disorders JMAJ 45(12): 538 544, 2002 Yoshio HIRAYASU Associate Professor, Department of Neuropsychiatry Kyorin University School of Medicine
The relevance of somatosensory auras in refractory temporal lobe epilepsies
 BRIEF COMMUNICATION The relevance of somatosensory auras in refractory temporal lobe epilepsies Ghazala Perven, Ruta Yardi, Juan Bulacio, Imad Najm, William Bingaman, Jorge Gonzalez-Martinez, and Lara
BRIEF COMMUNICATION The relevance of somatosensory auras in refractory temporal lobe epilepsies Ghazala Perven, Ruta Yardi, Juan Bulacio, Imad Najm, William Bingaman, Jorge Gonzalez-Martinez, and Lara
Henry Molaison. Biography. From Wikipedia, the free encyclopedia
 Henry Molaison From Wikipedia, the free encyclopedia Henry Gustav Molaison (February 26, 1926 December 2, 2008), known widely as H.M., was an American memory disorder patient who had a bilateral medial
Henry Molaison From Wikipedia, the free encyclopedia Henry Gustav Molaison (February 26, 1926 December 2, 2008), known widely as H.M., was an American memory disorder patient who had a bilateral medial
Is DTI Increasing the Connectivity Between the Magnet Suite and the Clinic?
 Current Literature In Clinical Science Is DTI Increasing the Connectivity Between the Magnet Suite and the Clinic? Spatial Patterns of Water Diffusion Along White Matter Tracts in Temporal Lobe Epilepsy.
Current Literature In Clinical Science Is DTI Increasing the Connectivity Between the Magnet Suite and the Clinic? Spatial Patterns of Water Diffusion Along White Matter Tracts in Temporal Lobe Epilepsy.
RADIOLOGY NEURORADIOLOGY. Iranian Journal of
 NEURORADIOLOGY Iranian Journal of RADIOLOGY RADIOLOGYwww.iranjradiol.com Value of Proton-MR-Spectroscopy in the Diagnosis of Temporal Lobe Epilepsy; Correlation of Metabolite Alterations With Electroencephalography
NEURORADIOLOGY Iranian Journal of RADIOLOGY RADIOLOGYwww.iranjradiol.com Value of Proton-MR-Spectroscopy in the Diagnosis of Temporal Lobe Epilepsy; Correlation of Metabolite Alterations With Electroencephalography
An analysis of MRI findings in patients referred with fits
 An analysis of MRI findings in patients referred with fits Pallewatte AS 1, Alahakoon S 1, Senanayake G 1, Bulathsinghela BC 1 1 National Hospital of Sri Lanka, Colombo, Sri Lanka Abstract Introduction:
An analysis of MRI findings in patients referred with fits Pallewatte AS 1, Alahakoon S 1, Senanayake G 1, Bulathsinghela BC 1 1 National Hospital of Sri Lanka, Colombo, Sri Lanka Abstract Introduction:
ORIGINAL CONTRIBUTION. Composite SISCOM Perfusion Patterns in Right and Left Temporal Seizures
 ORIGINAL CONTRIBUTION Composite SISCOM Perfusion Patterns in Right and Left Temporal Seizures R. Edward Hogan, MD; Kitti Kaiboriboon, MD; Mary E. Bertrand, MD; Venkat Rao, MD; Jayant Acharya, MD Objective:
ORIGINAL CONTRIBUTION Composite SISCOM Perfusion Patterns in Right and Left Temporal Seizures R. Edward Hogan, MD; Kitti Kaiboriboon, MD; Mary E. Bertrand, MD; Venkat Rao, MD; Jayant Acharya, MD Objective:
What is the Relationship Between Arachnoid Cysts and Seizure Foci?
 Epilepsin, 38( 10):1098-1102, 1997 Lippincott-Raven Publishers, Philadelphia 0 International League Against Epilepsy What is the Relationship Between Arachnoid Cysts and Seizure Foci? Santiago Arroyo and
Epilepsin, 38( 10):1098-1102, 1997 Lippincott-Raven Publishers, Philadelphia 0 International League Against Epilepsy What is the Relationship Between Arachnoid Cysts and Seizure Foci? Santiago Arroyo and