EVALUATION AND MEASUREMENTS. I. Devreux
|
|
|
- Daniel Anthony
- 5 years ago
- Views:
Transcription
1 EVALUATION AND MEASUREMENTS I. Devreux
2 To determine the extent and degree of muscular weakness resulting from disease, injury or disuse. The records obtained from these tests provide a base for planning therapeutic procedures and periodic re-testing. Muscle testing is an important tool for all members of the rehabilitation team.

3 At the end of this course, the student will be able to determine the muscle strength of human subject, as per the following criteria: 1. Choose the best position in which the therapist must place himself to evaluate each muscle or group of muscles. 2. Place the subject (pt.) in a suitable position that will allow him perform each task required to evaluate his muscle strength. 3. Establish the subject's passive range of motion.
4 4. Palpate the tendon or the muscle fibers being evaluated. 5. Support and stabilize the subject when necessary. 6. Obtain the maximal response from the subject and observe the contraction and the movement. 7. Identify possible substitutions and try to avoid them.
5 8. Apply manual resistance in the suitable arm when necessary. 9. Write the quotation of the evaluated muscle strength and note any limitation of range of motion. 10. Record in writing the results of each muscle or group of muscles test.

6 Muscle testing is a procedure for evaluating the function and strength of individual muscles and muscles group. It is based on effective performance of a movement in relation to the forces of gravity and manual resistance through available range of motion.
7 To provide information to a number of health professionals in differential diagnosis, ttt. planning and prognosis.! limitations in the treatment of neurological disorders, ( alteration in muscle tone or the central nervous system). The Ph.Th. must have a sound knowledge of anatomy (including joint motions, ms. origin & insertion and ms. function) & surface anatomy (to palpate ms. or tendon). The therapist must be a keen experienced in ms. testing to detect: observer and be minimal ms. contraction & mov. ms. wasting substitutions or trick movement.
8 * A consistent method of manually testing muscle strength is essential to assess accurately a patient's present status, progress and the effectiveness of the treatment program.
9 Muscular strength: The maximal amount of tension or force that a muscle or muscle group can voluntarily exert in a maximal effort, when type of muscle contraction, limb velocity and joint angle are specified.

10 Muscular Endurance: The ability of a muscle or a muscle group to perform repeated contractions against resistance or maintain an isometric contraction for a period of time.
11 The full range in which a ms. work refers to the ms. changing from a position of full stretch and contracting to a position of maximal shortening. * Outer range: Is from a position where the muscle is on full stretch to position halfway through the full range of motion. * Inner range: Is from a position halfway through the full range to a position where the muscle is fully shortened. * Middle range: Is the portion of the full range between the mid-point of the outer range and the midpoint of the inner range.
12 * Middle range: * Inner range: * Outer range:
13 The active insufficiency of a ms. that crosses two or more joints occurs when: the muscle produces simultaneous movement at all of the joints it crosses and reaches such a shortened position that it no longer has the ability to develop effective tension. When a muscle is placed in a shortened position of active insufficiency, it is described as putting the muscle on slack.
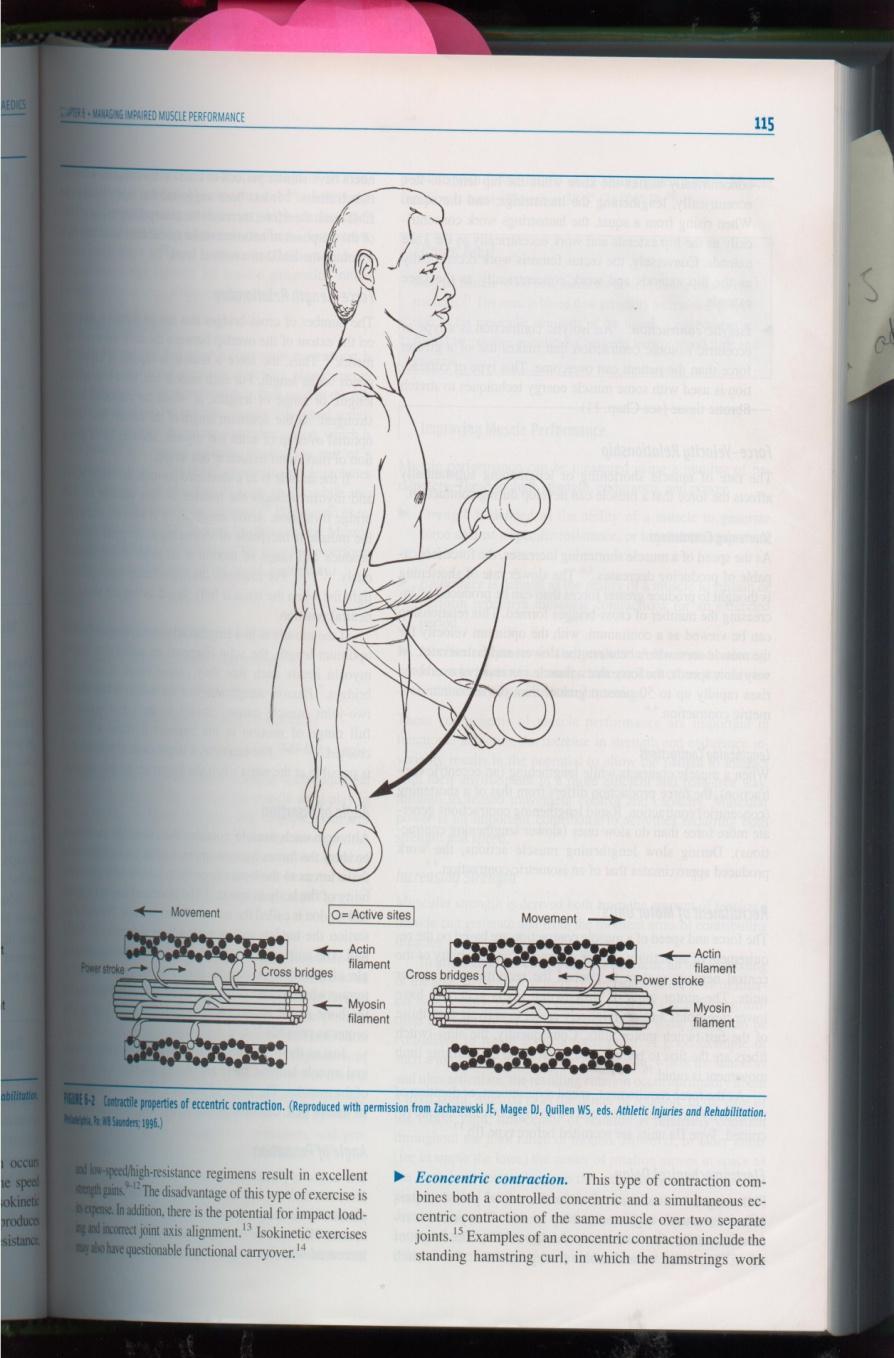
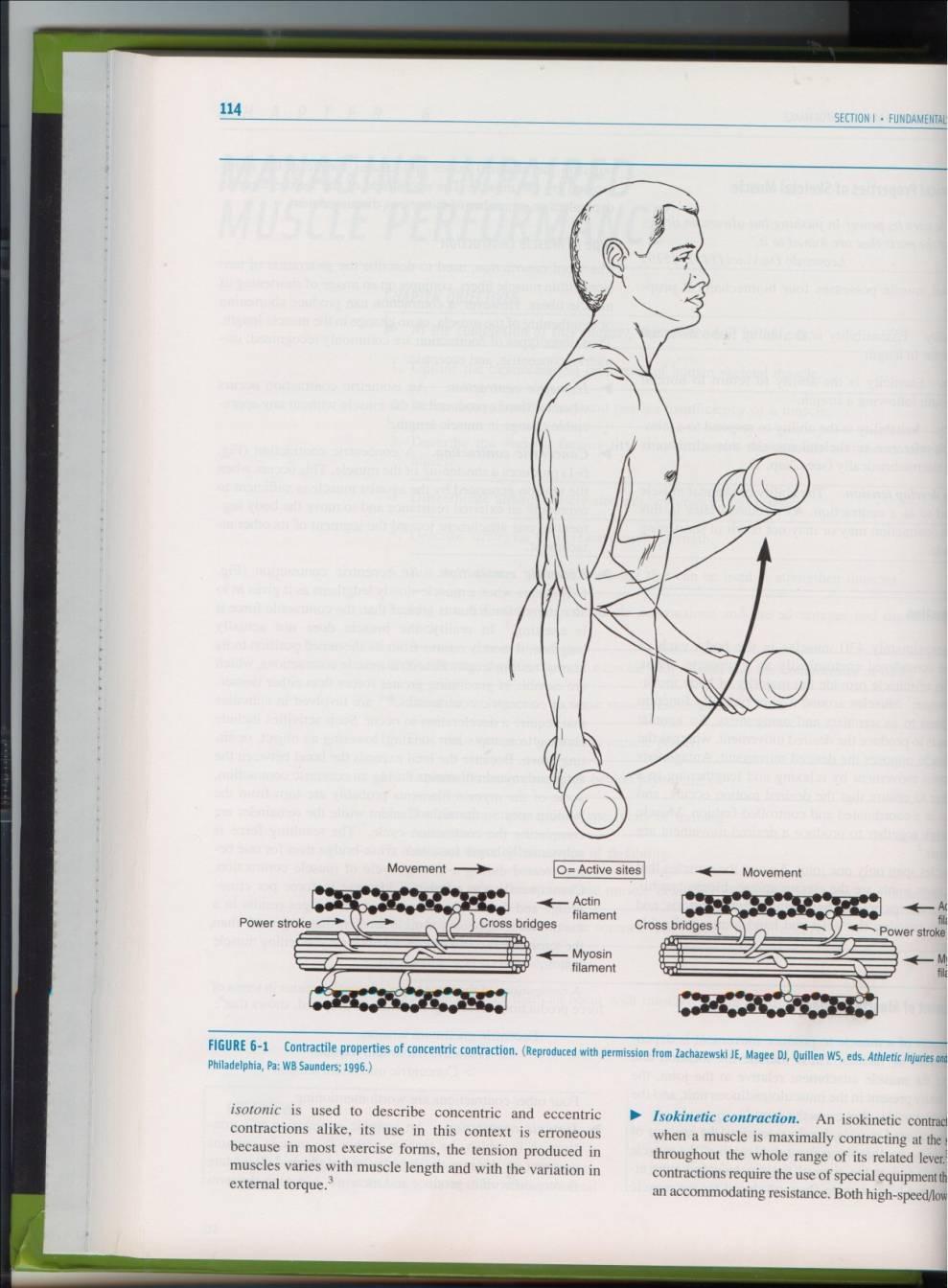
14 Isometric contraction: There is tension developed in the muscle but no movement occurs; the origin and insertion of the muscle do not change position and the muscle length does not change. Isotonic contraction: The muscle develops constant tension against a load or resistance. - Concentric contraction: Tension is developed in the muscle and the origin and insertion of the muscle move closer together; the muscle shortens. - Eccentric contraction: Tension is developed in the muscle and the origin and insertion of the muscle move farther a part; the muscle lengthens.
15
16 Muscles may be categorized as follows, according to the major role of the muscles in producing the movement. * Prime mover or agonist: A muscle or muscle group that makes the major contribution to movement at the joint. * Antagonist: A muscle or a muscle group that has an opposite action to the prime movers. The antagonist relaxes as the agonist moves the part through a range of motion.
17 * Synergist: A muscle that contracts and works along with the agonist to produce the desired movement. There are three types of synergists. - Neutralizing or counter-acting synergists: Muscles contracted to prevent unwanted movement, produced by the prime mover. For example, when the long finger flexors contract to produce finger flexion, the wrist extensors contract to prevent wrist flexion from occurring.
18 - Conjoint synergists: Two or more muscles that work together to produce the desired movement. Example: wrist extension is produced by contraction of extensor carpi radialis longus and brives and extensor carpi ulnaris. If the extensor carpi radialis longus or brevis contracts alone, the wrist extends and radially deviates, while if the extensor carpi ulnaris contracts alone, the wrist extends and ulnarly deviates. When the muscles contract as a group, the deviation actions is cancelled out and the common action of wrist results (extension).
19 - Stabilizing or Fixating Synergists: Muscles that prevent movement or control the movement at joints proximal to the moving joint to provide a fixed or stable base, from which the distal moving segment can effectively work. Example: if the elbow flexors contract to lift an object off a table anterior to the body, the muscles of the scapula and gleno-humeral joint must contract to either allow slow controlled movement or no movement to occur at the scapula and gleno-humeral joint to provide the elbow flexors with a fixed origin from which to pull. If the scapular muscles did not contract, the object could not be lifted as the elbow flexors would act to pull the shoulder girdle downward toward the table top.
20 Muscles with a common action or actions may be tested as a group or a muscle may be tested individually. For example, flexor carpi ulnaris and flexor carpi radialis may be tested together as a group in wrist flexion. Flexor carpi ulnaris may be tested more specifically in the action of wrist flexion with ulnar deviation.
21 1. Explanation and instruction: The therapist demonstrates and/ or explains briefly the mov. to be performed and/ or passively moves the pt s limb through the test movement. 2. Assessment of normal muscle strength: Initially assess and record the strength of the uninvolved limb to determine the pt s normal strength and to demonstrate the mov. before assessing the strength of the involved side, considering the factors that affect strength.

22 3. Patient position: The pt. is positioned to isolate the muscle or muscle group to be tested in either gravity elimination or against gravity position. Ensure that the patient is comfortable and well supported. The muscle or muscle group being tested is placed in full outer range, with only slight tension. 4. Stabilization: Stabilize the site of attachment of the muscle origin, so the muscle has a fixed point from which to pull.
 The patient's body weight: Used to help fix the shoulder or pelvic girdles.")
23 Prevent substitutions and trick movements by making use of the following methods: a) The patient's normal muscles: For example, the patient holds the edge of the plinth when hip flexion is tested and uses the scapular muscles when glenohumeral flexion is performed. b) The patient's body weight: Used to help fix the shoulder or pelvic girdles. c) The patient s position: For example, when assessing hip abduction muscle strength in side lying, the patient holds the non-test limb in hip and knee flexion in order to tilt the pelvis posteriorly and fix the pelvis and lumbar spine.
 Substitution and trick movements: When muscles are weak or paralyzed, other muscles may take over or gravity may be used to perform")
24 d) External forces: May be applied directly by the therapist or by devices such as belt and sandbags. e) Substitution and trick movements: When muscles are weak or paralyzed, other muscles may take over or gravity may be used to perform movements, normally carried out by the weak muscles.
25 Screen test: Used to streamline the ms. strength assessment, avoid unnecessary testing and avoid fatiguing / discouraging the pt. The ther. may screen the pt. through the information from: The previous assessment of the patient's AROM. Reading the pt s chart or previous ms. test result. Observing the pt. while performing functional activities. I.e. shaking the patients hand may indicate the strength of grasp (finger flexors). Beginning all ms. testing at a particular grade,(usually a grade of 3) The pt. is instructed to actively move the body part through full range of motion against gravity. Based upon the results of the initial test, the muscle test is either stopped or proceeds.
26 Manual grading of ms. strength is based on 3 factors: Evidence of contraction: No palpable or observable ms. contraction (grade 0) or a palpable or observable ms. contraction and no joint motion (grade 1). Gravity as a resistance: The ability to move the part through the full available range of motion with gravity eliminated (grade 2) or against gravity (grade 3) the most objective part of test. Amount of manual resistance: The ability to move the part through the full available range of motion against gravity and against moderate manual resistance (grade 4) or maximal manual resistance (grade 5). Adding (+) or (-) to the whole grades to denote variation in the range of motion. Movement through less than half of the available range of motion is denoted by a (+) (outer range). Movement through greater than half of the available range of motion by (-) (inner range).
27 Numerals Letters Description Against gravity test The patient is able to move through: 5 N (normal) The full available ROM against gravity and against maximal resistance, with hold at the end of the ROM (Hold for about 3 seconds). 4 G (good) The full available ROM against gravity and against moderate leading resistance. 4- G- Greater than one half of the available ROM against gravity and against moderate resistance. 3+ F+ Less than one half of the available ROM against gravity and against moderate resistance. 3 F The full available ROM against gravity. 3- F- Greater than one half of the available ROM against gravity. 2+ P+ Less than one half of the available ROM against gravity. Gravity eliminated test: The patient is able to actively move through: 2 P The full available ROM gravity eliminated. 2- P- Greater than one half the available ROM gravity eliminated. 1+ T+ Less than one half of the available ROM gravity eliminated. 1 T (Trace) None of the available ROM with gravity eliminated and there is palpable or observable flicker contraction. 0 0 (zero) None of the available ROM with gravity eliminated and there is no palpable or observable muscle contraction.
28 1. Age: A decrease in strength occurs with increasing () age due to deterioration in ms. mass. Ms. fibers decrease in size and number; There is an in connective tissue and fat and the respiratory capacity of the ms. decreases. Strength apparently for the first 20 years of life, remains at this level for 5 or 10 years and then gradually decreases throughout the rest of life. The changes in muscular strength by aging are different for different groups of muscles. The progressive decrease in strength is clear in the forearm flexors and muscles that raise the body.
29 2. Sex: Males are generally stronger than females. Relation between strength and sex: The strength of males rapidly from 2 to 19 years of age at a rate similar to weight and more slowly and regularly up to 30 years. After that, it declines at an increased rate to the age of 60 years. The strength of females was found to at a more uniform rate from 9 to 19 years and more slowly to 30 years, after which it falls off in a manner similar to males. It has been found that women are more 28 to 30% weaker than men at 40 to 45 years of age.
30 3. Type of muscle contraction: More tension can be developed during an eccentric contraction than during an isometric contraction. The concentric contraction has the smallest tension capability. 4. Muscle size: The larger the cross-sectional area of a ms., the greater the strength of the ms.. When testing a muscle that is small, the therapist would expect less tension to be developed than if testing a large, thick muscle.
31 5. Speed of muscle contraction: When a ms. contracts concentricity, the force of contraction decreases as the speed of contraction increases. The pt. is instructed to perform each ms. test movement at a moderate pace. 6. Previous training effect: Strength performance depends up on the ability of the nervous system to activate the ms. mass. Strength may increase as one becomes familiar with and learns the test situation. The therapist must instruct the patient well, giving him an opportunity to move through or be passively moved through the test movement at least once before strength is assessed.
32 7. Joint position: It depends on the angle of ms. pull and the length-tension relationship. The tension developed within a ms. depends up on the initial length of the muscle. Regardless of the type of ms. contraction, a ms. contracts with more-force when it is stretched than when it is shortened. The greatest amount of tension is developed when the ms. is stretched to the greatest length possible within the body; if the ms. is in full outer range.
33 8. Fatigue: As the pt. fatigues, ms. strength decreases. The therapist determines the strength of ms. using as few repetitions as possible to avoid fatigue. The pt's level of motivation, level of pain, body type, occupation and dominance are other factors that may affect strength.

34 Manual assessment of muscle strength is contraindicated where: Inflammation is present in the region. Pain is present as it will inhibit muscle contraction and will not give an accurate indication of muscle strength. Testing muscle strength in the presence of pain may cause further injury.
35 Extra care must be taken where resisted movements might aggravate the condition as in: a) Pts. w/ history problems. at risk of having cardiovascular b) Pts who had abdominal surgery or pts. with herniation of the abdominal wall to avoid unsafe level stress on the abdominal wall. c) In situations where fatigue may be detrimental to or exacerbate the pt s. condition. Pts with extreme debility, for ex. mal nutrition, malignancy and severe chronic obstructive pulmonary disease. They have not the energy to carry out strenuous testing.
36
Manual Muscle Testing. Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department
 Manual Muscle Testing Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Manual Muscle Testing Evaluation of the function and strength of individual muscles and muscles
Manual Muscle Testing Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Manual Muscle Testing Evaluation of the function and strength of individual muscles and muscles
*Agonists are the main muscles responsible for the action. *Antagonists oppose the agonists and can help neutralize actions. Since many muscles have
 1 *Agonists are the main muscles responsible for the action. *Antagonists oppose the agonists and can help neutralize actions. Since many muscles have more than 1 action sometimes a muscle has to neutralize
1 *Agonists are the main muscles responsible for the action. *Antagonists oppose the agonists and can help neutralize actions. Since many muscles have more than 1 action sometimes a muscle has to neutralize
Musculoskeletal System. Terms. Origin (Proximal Attachment) Insertion (Distal Attachment)
 Insertion (Distal Attachment)") Musculoskeletal System Terms Origin (Proximal Attachment) Insertion (Distal Attachment) Agonist- prime mover Antagonist- provides a braking force Synergist- assists indirectly in the movement Musculoskeletal
Musculoskeletal System Terms Origin (Proximal Attachment) Insertion (Distal Attachment) Agonist- prime mover Antagonist- provides a braking force Synergist- assists indirectly in the movement Musculoskeletal
When a muscle contracts, it knows no direction; it simply shortens. Lippert
 When a muscle contracts, it knows no direction; it simply shortens. Lippert Muscle is the sole producer of active force in the body which makes it responsible for all active motions. Muscles also control
When a muscle contracts, it knows no direction; it simply shortens. Lippert Muscle is the sole producer of active force in the body which makes it responsible for all active motions. Muscles also control
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK. Musculoskeletal Anatomy & Kinesiology MUSCLES, MOVEMENTS & BIOMECHANICS
 BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology MUSCLES, MOVEMENTS & BIOMECHANICS MSAK101-I Session 7 Learning Objectives: 1. List the three types
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology MUSCLES, MOVEMENTS & BIOMECHANICS MSAK101-I Session 7 Learning Objectives: 1. List the three types
When a muscle contracts, it knows no direction it simply shortens. Lippert
 When a muscle contracts, it knows no direction it simply shortens. Lippert Muscles are attached to bones and to describe the relative points of attachment, we use the terms origin and insertion. Lippert,
When a muscle contracts, it knows no direction it simply shortens. Lippert Muscles are attached to bones and to describe the relative points of attachment, we use the terms origin and insertion. Lippert,
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.
 Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.") MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
Goniometry. Wrist Flexion: Pt seated with forearm resting on table (use olecranon process & midline of ulna as reference for stationary arm)
") Goniometry Wrist Flexion: Pt seated with forearm resting on table (use olecranon process & midline of ulna as reference for stationary arm) Wrist Extension: Pt seated with forearm resting on table (Goniometer
Goniometry Wrist Flexion: Pt seated with forearm resting on table (use olecranon process & midline of ulna as reference for stationary arm) Wrist Extension: Pt seated with forearm resting on table (Goniometer
Figure 11-1: The lever-fulcrum principle is illustrated by flexion of the forearm.
 Chapter 11: The Muscular System Read pages 325 to 399 NAME Topic Outline And Objectives: A. How skeletal muscles produce movement, and naming muscles 1. Describe the relationship between bones and skeletal
Chapter 11: The Muscular System Read pages 325 to 399 NAME Topic Outline And Objectives: A. How skeletal muscles produce movement, and naming muscles 1. Describe the relationship between bones and skeletal
Benefits of Weight bearing increased awareness of the involved side decreased fear improved symmetry regulation of muscle tone
 From the information we have gathered during our Evaluation, the Clinical Reasoning we used to identify key problem areas and the Goals Established with functional outcomes we now have enough information
From the information we have gathered during our Evaluation, the Clinical Reasoning we used to identify key problem areas and the Goals Established with functional outcomes we now have enough information
Skeletal Muscles and Functions
 Skeletal Muscles and Functions Huei-Ming Chai, PT, Ph.D. School of Physical Therapy National Taiwan University Classification of Muscles striated muscles skeletal muscles: voluntary contraction cardiac
Skeletal Muscles and Functions Huei-Ming Chai, PT, Ph.D. School of Physical Therapy National Taiwan University Classification of Muscles striated muscles skeletal muscles: voluntary contraction cardiac
The Biomechanics of Human Skeletal Muscle
 AML2506 Biomechanics and Flow Simulation Day 03B The Biomechanics of Human Skeletal Muscle Session Speaker Dr. M. D. Deshpande 1 Session Objectives At the end of this session the delegate would have understood
AML2506 Biomechanics and Flow Simulation Day 03B The Biomechanics of Human Skeletal Muscle Session Speaker Dr. M. D. Deshpande 1 Session Objectives At the end of this session the delegate would have understood
CSEP-Certified Certified Personal Trainer (CSEP-CPT) CPT) Musculoskeletal Fitness Theory
 CPT) Musculoskeletal Fitness Theory") CSEP-Certified Certified Personal Trainer (CSEP-CPT) CPT) Musculoskeletal Fitness Theory 1 Basic Anatomy Key Concepts: 3.23-3.25 3.25 2 Force & Levers 1 st class» seesaw» muscles that extend neck R F AF
CSEP-Certified Certified Personal Trainer (CSEP-CPT) CPT) Musculoskeletal Fitness Theory 1 Basic Anatomy Key Concepts: 3.23-3.25 3.25 2 Force & Levers 1 st class» seesaw» muscles that extend neck R F AF
Certified Personal Trainer Re-Certification Manual
 Certified Personal Trainer Re-Certification Manual Section II 1 Anatomy & Physiology Terms Anatomy and physiology are closely related fields of study: anatomy is the study of form, and physiology is the
Certified Personal Trainer Re-Certification Manual Section II 1 Anatomy & Physiology Terms Anatomy and physiology are closely related fields of study: anatomy is the study of form, and physiology is the
Muscular Considerations for Movement. Kinesiology RHS 341 Lecture 4 Dr. Einas Al-Eisa
 Muscular Considerations for Movement Kinesiology RHS 341 Lecture 4 Dr. Einas Al-Eisa Role of muscles Prime mover Synergist Agonist Antagonist Stabilizers Neutralizers Role of muscles Agonist: Muscles producing
Muscular Considerations for Movement Kinesiology RHS 341 Lecture 4 Dr. Einas Al-Eisa Role of muscles Prime mover Synergist Agonist Antagonist Stabilizers Neutralizers Role of muscles Agonist: Muscles producing
Therapy Manual DO NOT PRINT
 Therapy Manual Contents 1. Shoulder 2. Shoulder and elbow a. Protraction: 1 DoF 1 b. Flexion: 1 DoF 1-6 c. Extension: 1 DoF 1-2 d. Abduction: 1 DoF 1-4 e. External rotation: 1 DoF 1-14 a. Combined shoulder
Therapy Manual Contents 1. Shoulder 2. Shoulder and elbow a. Protraction: 1 DoF 1 b. Flexion: 1 DoF 1-6 c. Extension: 1 DoF 1-2 d. Abduction: 1 DoF 1-4 e. External rotation: 1 DoF 1-14 a. Combined shoulder
Basics of Soft- Tissue Examination
 Basics of Soft- Tissue Examination Basics of Soft Tissue Exam For practitioners who primarily use their hands to treat the human structure: Examination must include functional tests to determine the type
Basics of Soft- Tissue Examination Basics of Soft Tissue Exam For practitioners who primarily use their hands to treat the human structure: Examination must include functional tests to determine the type
The Role of Muscles in Movement
 The Role of Muscles in Movement Muscles can t push, they can only pull as they contract, so most often body movements are the result of the activity of pairs or teams of muscles acting together or against
The Role of Muscles in Movement Muscles can t push, they can only pull as they contract, so most often body movements are the result of the activity of pairs or teams of muscles acting together or against
Key Points for Success:
 SELF WRIST & HAND 1 2 All of the stretches described in this chapter are detailed to stretch the right side. Key Points for Success: Sit comfortably in a position where you can straighten or fully extend
SELF WRIST & HAND 1 2 All of the stretches described in this chapter are detailed to stretch the right side. Key Points for Success: Sit comfortably in a position where you can straighten or fully extend
Chapter 3: Applied Kinesiology. ACE Personal Trainer Manual Third Edition
 Chapter 3: Applied Kinesiology ACE Personal Trainer Manual Third Edition Introduction Kinesiology is the study of the body s infinite number of movements, positions, and postures and is grounded in the
Chapter 3: Applied Kinesiology ACE Personal Trainer Manual Third Edition Introduction Kinesiology is the study of the body s infinite number of movements, positions, and postures and is grounded in the
1-Apley scratch test.
 1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
Muscular Analysis of Upper Extremity Exercises McGraw-Hill Higher Education. All rights reserved. 8-1
 Muscular Analysis of Upper Extremity Exercises 2007 McGraw-Hill Higher Education. All rights reserved. 8-1 Muscular Analysis of Upper Extremity Exercises Upper extremity - often one of body's weakest areas
Muscular Analysis of Upper Extremity Exercises 2007 McGraw-Hill Higher Education. All rights reserved. 8-1 Muscular Analysis of Upper Extremity Exercises Upper extremity - often one of body's weakest areas
Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body weight, height, and sex in 178 healthy subjects
 Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body weight, height, and sex in 178 healthy subjects Test protocol Muscle test procedures. Prior to each test participants
Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body weight, height, and sex in 178 healthy subjects Test protocol Muscle test procedures. Prior to each test participants
OpenSim Tutorial #2 Simulation and Analysis of a Tendon Transfer Surgery
 OpenSim Tutorial #2 Simulation and Analysis of a Tendon Transfer Surgery Laboratory Developers: Scott Delp, Wendy Murray, Samuel Hamner Neuromuscular Biomechanics Laboratory Stanford University I. OBJECTIVES
OpenSim Tutorial #2 Simulation and Analysis of a Tendon Transfer Surgery Laboratory Developers: Scott Delp, Wendy Murray, Samuel Hamner Neuromuscular Biomechanics Laboratory Stanford University I. OBJECTIVES
Biomechanics of Skeletal Muscle and the Musculoskeletal System
 Biomechanics of Skeletal Muscle and the Musculoskeletal System Hamill & Knutzen (Ch 3) Nordin & Frankel (Ch 5), or Hall (Ch. 6) Muscle Properties Ø Irritability Ø Muscle has the capability of receiving
Biomechanics of Skeletal Muscle and the Musculoskeletal System Hamill & Knutzen (Ch 3) Nordin & Frankel (Ch 5), or Hall (Ch. 6) Muscle Properties Ø Irritability Ø Muscle has the capability of receiving
INTRODUCTION. Objectives
 Objectives Functional Anatomy for Fitness Professionals focuses on functional anatomy, with an emphasis on weight training. Through the emphasis on biomechanics, neurology, and muscle physiology, participants
Objectives Functional Anatomy for Fitness Professionals focuses on functional anatomy, with an emphasis on weight training. Through the emphasis on biomechanics, neurology, and muscle physiology, participants
WTC I Term 2 Notes/Assessments
 WTC I Term 2 Notes/Assessments Muscle Identification The human body consists of many muscles and muscle groups. We will focus on a select few that are most prevalent when training. The muscular system
WTC I Term 2 Notes/Assessments Muscle Identification The human body consists of many muscles and muscle groups. We will focus on a select few that are most prevalent when training. The muscular system
Chapter 6 part 2. Skeletal Muscles of the Body
 Chapter 6 part 2 Skeletal Muscles of the Body Basic Principles 600 + muscles in the human body (you are required to learn 45, lucky kids)! Skeletal Muscles pull on bones Origin of a muscle = point of attachment
Chapter 6 part 2 Skeletal Muscles of the Body Basic Principles 600 + muscles in the human body (you are required to learn 45, lucky kids)! Skeletal Muscles pull on bones Origin of a muscle = point of attachment
GENERAL EXERCISES THUMB, WRIST, HAND BMW MANUFACTURING CO. PZ-AM-G-US I July 2017
 GENERAL EXERCISES THUMB, WRIST, HAND BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only
GENERAL EXERCISES THUMB, WRIST, HAND BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only
Chapter 13. Development of Muscular, Strength, Endurance, and Flexibility
 Chapter 13 Development of Muscular, Strength, Endurance, and Flexibility Types of Contractions Dynamic, Isotonic, or concentric Muscle shortens with varying tension while lifting constant load Isometric,
Chapter 13 Development of Muscular, Strength, Endurance, and Flexibility Types of Contractions Dynamic, Isotonic, or concentric Muscle shortens with varying tension while lifting constant load Isometric,
Elbow Muscle Power Deficits
 1 Elbow Muscle Power Deficits ICD-9-CM code: 726.32 Lateral epicondylitis ICF codes: Activities and Participation code: d4300 Lifting, d4452 Reaching, d4401 Grasping Body Structure code: s73012 Muscles
1 Elbow Muscle Power Deficits ICD-9-CM code: 726.32 Lateral epicondylitis ICF codes: Activities and Participation code: d4300 Lifting, d4452 Reaching, d4401 Grasping Body Structure code: s73012 Muscles
Clinical examination of the wrist, thumb and hand
 Clinical examination of the wrist, thumb and hand 20 CHAPTER CONTENTS Referred pain 319 History 319 Inspection 320 Functional examination 320 The distal radioulnar joint.............. 320 The wrist.......................
Clinical examination of the wrist, thumb and hand 20 CHAPTER CONTENTS Referred pain 319 History 319 Inspection 320 Functional examination 320 The distal radioulnar joint.............. 320 The wrist.......................
26a A&P: Muscular System -! Fiber Types, Actions, and Contractions
 26a A&P: Muscular System -! Fiber Types, Actions, and Contractions 26a A&P: Muscular System -! Fiber Types, Actions, and Contractions! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders
26a A&P: Muscular System -! Fiber Types, Actions, and Contractions 26a A&P: Muscular System -! Fiber Types, Actions, and Contractions! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders
WEEKEND 2 Elbow. Elbow Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Elbow Elbow Range of Motion Assessment - Patient Positioning: Sitting or supine towards the edge of the bed - Indications:
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Elbow Elbow Range of Motion Assessment - Patient Positioning: Sitting or supine towards the edge of the bed - Indications:
GENERAL EXERCISES ELBOW BMW MANUFACTURING CO. PZ-AM-G-US I July 2017
 GENERAL EXERCISES ELBOW BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only are not to be
GENERAL EXERCISES ELBOW BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only are not to be
ACE s Essentials of Exercise Science for Fitness Professionals TRUNK
 ACE s Essentials of Exercise Science for Fitness Professionals TRUNK Posture and Balance Posture refers to the biomechanical alignment of the individual body parts and the orientation of the body to the
ACE s Essentials of Exercise Science for Fitness Professionals TRUNK Posture and Balance Posture refers to the biomechanical alignment of the individual body parts and the orientation of the body to the
Protocol S8 Physical Therapy Protocol for Arthroscopic Reverse Bankart Repair or Open Posterior Capsulorrhaphy
 Phase I: Protection Phase (0-5 weeks) Allow time for labral repair to heal. Gradually increase shoulder passive range of motion (ROM) Use pain medications as needed. Wear shoulder immobilizer for 5 weeks.
Phase I: Protection Phase (0-5 weeks) Allow time for labral repair to heal. Gradually increase shoulder passive range of motion (ROM) Use pain medications as needed. Wear shoulder immobilizer for 5 weeks.
Biceps Tenodesis Protocol
 Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Pilates for Brachialis Tendonitis (Tennis Elbow)
") Pilates for Brachialis Tendonitis (Tennis Elbow) Sally Dunford September 2017 Wimbledon, UK Abstract Tennis Elbow is a term used to describe a painful condition in which the tendons of the elbow are overloaded
Pilates for Brachialis Tendonitis (Tennis Elbow) Sally Dunford September 2017 Wimbledon, UK Abstract Tennis Elbow is a term used to describe a painful condition in which the tendons of the elbow are overloaded
Muscle Lecture Test Questions Set 1
 Muscle Lecture Test Questions Set 1 Fall 2015 1. Muscle cells exhibit the greatest ability to shrink -- this quality of all protoplasm is: a. voluntary b. involuntary c. fusiform d. contractility e. conductivity
Muscle Lecture Test Questions Set 1 Fall 2015 1. Muscle cells exhibit the greatest ability to shrink -- this quality of all protoplasm is: a. voluntary b. involuntary c. fusiform d. contractility e. conductivity
Chapter 20: Muscular Fitness and Assessment
 Chapter 20: Muscular Fitness and Assessment American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York: Lippincott, Williams
Chapter 20: Muscular Fitness and Assessment American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York: Lippincott, Williams
Multi-joint Mechanics Dr. Ted Milner (KIN 416)
") Multi-joint Mechanics Dr. Ted Milner (KIN 416) Muscle Function and Activation It is not a straightforward matter to predict the activation pattern of a set of muscles when these muscles act on multiple
Multi-joint Mechanics Dr. Ted Milner (KIN 416) Muscle Function and Activation It is not a straightforward matter to predict the activation pattern of a set of muscles when these muscles act on multiple
RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Tel# Department of Physical Therapy King Saud University
 1 RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Tel# 4693601 Department of Physical Therapy King Saud University 2 The scapulae lie against the thorax approximately
1 RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Tel# 4693601 Department of Physical Therapy King Saud University 2 The scapulae lie against the thorax approximately
Home Therapy Program Lateral Epicondylitis (Tennis Elbow)
") Benjamin W. Sears, MD Home Therapy Program Lateral Epicondylitis (Tennis Elbow) PHASE 1 Goals: decrease inflammation and pain and promote tissue healing, the RICE principle: Rest - avoid further overuse,
Benjamin W. Sears, MD Home Therapy Program Lateral Epicondylitis (Tennis Elbow) PHASE 1 Goals: decrease inflammation and pain and promote tissue healing, the RICE principle: Rest - avoid further overuse,
Lab Workbook. ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone
 ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
When a muscle contracts, it knows no direction; it simply shortens. Lippert
 When a muscle contracts, it knows no direction; it simply shortens. Lippert Muscle is the sole producer of active force in the body which makes it responsible for all active motions. Muscles also control
When a muscle contracts, it knows no direction; it simply shortens. Lippert Muscle is the sole producer of active force in the body which makes it responsible for all active motions. Muscles also control
Neck Rehabilitation programme for Rugby players.
 Neck Rehabilitation programme for Rugby players. The programme consists of two parts, first the Therapeutic Exercise Programme to improve biomechanical function and secondly the Rehabilitation programme
Neck Rehabilitation programme for Rugby players. The programme consists of two parts, first the Therapeutic Exercise Programme to improve biomechanical function and secondly the Rehabilitation programme
Rotator Cuff Repair Therapy Protocol
 Bart Eastwood D.O. 825 Davis st Blacksburg, VA 24060 540-951-6000 All information contained in this protocol is to be used as general guidelines only. Specific variations may be appropriate for each patient
Bart Eastwood D.O. 825 Davis st Blacksburg, VA 24060 540-951-6000 All information contained in this protocol is to be used as general guidelines only. Specific variations may be appropriate for each patient
GENERAL EXERCISES SHOULDER BMW MANUFACTURING CO. PZ-AM-G-US I July 2017
 GENERAL EXERCISES SHOULDER BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only are not to
GENERAL EXERCISES SHOULDER BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only are not to
HOW MUSCLES WORK Readings: H (Ch. 3,13), T (Ch 2,3)*
, T (Ch 2,3)*") HOW MUSLES WORK Readings: H (h. 3,13), T (h 2,3)* How Muscle Force is Generated:! Muscles convert chemical energy into! Muscles are internal motors of human body responsible for all movements of skeletal
HOW MUSLES WORK Readings: H (h. 3,13), T (h 2,3)* How Muscle Force is Generated:! Muscles convert chemical energy into! Muscles are internal motors of human body responsible for all movements of skeletal
KNEE AND LEG EXERCISE PROGRAM
 KNEE AND LEG EXERCISE PROGRAM These exercises are specifically designed to rehabilitate the muscles of the hip and knee by increasing the strength and flexibility of the involved leg. This exercise program
KNEE AND LEG EXERCISE PROGRAM These exercises are specifically designed to rehabilitate the muscles of the hip and knee by increasing the strength and flexibility of the involved leg. This exercise program
Chapter 7 The Muscular System - Part 2. Mosby items and derived items 2012 by Mosby, Inc., an affiliate of Elsevier Inc. 1
 Chapter 7 The Muscular System - Part 2 Mosby items and derived items 2012 by Mosby, Inc., an affiliate of Elsevier Inc. 1 FUNCTIONS OF SKELETAL MUSCLE A. Functions 1. Movement 2. Posture or muscle tone
Chapter 7 The Muscular System - Part 2 Mosby items and derived items 2012 by Mosby, Inc., an affiliate of Elsevier Inc. 1 FUNCTIONS OF SKELETAL MUSCLE A. Functions 1. Movement 2. Posture or muscle tone
Bell Work. How does the muscular system relate to the following organ systems, Respiratory Circulatory Digestive
 Muscular System Bell Work How does the muscular system relate to the following organ systems, Respiratory Circulatory Digestive Exercise Science Standards 8) Review the gross and cellular anatomy and physiology
Muscular System Bell Work How does the muscular system relate to the following organ systems, Respiratory Circulatory Digestive Exercise Science Standards 8) Review the gross and cellular anatomy and physiology
The SUPPORT Trial: SUbacromial impingement syndrome and Pain: a randomised controlled trial Of exercise and injection
 The SUPPORT Trial: SUbacromial impingement syndrome and Pain: a randomised controlled trial Of exercise and injection SUPPORT Physiotherapy Intervention Training Manual Authors: Sue Jackson (SJ) Julie
The SUPPORT Trial: SUbacromial impingement syndrome and Pain: a randomised controlled trial Of exercise and injection SUPPORT Physiotherapy Intervention Training Manual Authors: Sue Jackson (SJ) Julie
Hemiplegic Shoulder. Incidence & Rationale. Shoulder Pain Assessment & Treatment
 Hemiplegic Shoulder Jeane Davis Fyfe OT, Senior Therapist Incidence & Rationale Up to 72% of stroke survivors will experience shoulder pain Shoulder pain may inhibit patient participation in rehabilitation
Hemiplegic Shoulder Jeane Davis Fyfe OT, Senior Therapist Incidence & Rationale Up to 72% of stroke survivors will experience shoulder pain Shoulder pain may inhibit patient participation in rehabilitation
بسم هللا الرحمن الرحيم
 1 بسم هللا الرحمن الرحيم Introduction to Physical Therapy Procedures RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Tel# 4693601 Department of Physical Therapy King
1 بسم هللا الرحمن الرحيم Introduction to Physical Therapy Procedures RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Tel# 4693601 Department of Physical Therapy King
GFM Platform Exercise Manual
 GFM Platform Exercise Manual STEPHEN NEWHART, CSCS*D What is Whole Body Vibration? Body vibration is delivered through a variety of machines, including the most recent inclusion of whole body vibration
GFM Platform Exercise Manual STEPHEN NEWHART, CSCS*D What is Whole Body Vibration? Body vibration is delivered through a variety of machines, including the most recent inclusion of whole body vibration
Biceps Tenodesis Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Biceps Tenodesis Protocol The intent of this protocol is to provide the clinician with a
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Biceps Tenodesis Protocol The intent of this protocol is to provide the clinician with a
Provide movement Maintain posture/stability Generate heat
 How we move.. What do muscles do for us? Provide movement Maintain posture/stability Generate heat (skeletal muscle accounts for 40% body mass) So looking at skeletal muscles.. What do skeletal muscles
How we move.. What do muscles do for us? Provide movement Maintain posture/stability Generate heat (skeletal muscle accounts for 40% body mass) So looking at skeletal muscles.. What do skeletal muscles
Limited Goals Program (Examples Include: Cuff Tear Arthropathy, Massive Irrepairable Rotator Cuff Tear, Selected Revision Surgeries)
") Limited Goals Program (Examples Include: Cuff Tear Arthropathy, Massive Irrepairable Rotator Cuff Tear, Selected Revision Surgeries) All information contained in this protocol is to be used as general
Limited Goals Program (Examples Include: Cuff Tear Arthropathy, Massive Irrepairable Rotator Cuff Tear, Selected Revision Surgeries) All information contained in this protocol is to be used as general
Do the same as above, but turn your head TOWARDS the side that you re holding on to the chair.
 Stretch 4-6 times per day and hold each stretch for a minimum of 30 seconds. Perform the stretch gently without bouncing. Discuss any problems with your Chiropractor. Sit upright with your head and shoulder
Stretch 4-6 times per day and hold each stretch for a minimum of 30 seconds. Perform the stretch gently without bouncing. Discuss any problems with your Chiropractor. Sit upright with your head and shoulder
Christopher K. Jones, MD Colorado Springs Orthopaedic Group
 Christopher K. Jones, MD Colorado Springs Orthopaedic Group 719-632-7669 Total Shoulder Replacement You have undergone a shoulder replacement procedure. The performance of the procedure is complete, but
Christopher K. Jones, MD Colorado Springs Orthopaedic Group 719-632-7669 Total Shoulder Replacement You have undergone a shoulder replacement procedure. The performance of the procedure is complete, but
Anterior Stabilization of the Shoulder: Distal Tibial Allograft
 Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
1 Pause and Practice: Facilitating Trunk and Shoulder Control with the Therapy Ball
 1 Pause and Practice: Facilitating Trunk and Shoulder Control with the Therapy Ball This is an example of Facilitating Combinations of Movements and Active Assist. Starting Position Have your patient sit
1 Pause and Practice: Facilitating Trunk and Shoulder Control with the Therapy Ball This is an example of Facilitating Combinations of Movements and Active Assist. Starting Position Have your patient sit
Muscular Strength and Endurance:
 PE 1- Assignment #5 6 1 Name: Per: Date: Teacher: STRESS BREAK Participating in physical activities that improve your self-esteem is a great way to deal with stress. The better you feel about yourself,
PE 1- Assignment #5 6 1 Name: Per: Date: Teacher: STRESS BREAK Participating in physical activities that improve your self-esteem is a great way to deal with stress. The better you feel about yourself,
CHAPTER 1: 1.1 Muscular skeletal system. Question - text book page 16. Question - text book page 20 QUESTIONS AND ANSWERS. Answers
 QUESTIONS AND ANSWERS CHAPTER 1: 1.1 Muscular skeletal system Question - text book page 16 Using the information on pages 12 to 14 above, complete the table below. joint joint type articulating bones associated
QUESTIONS AND ANSWERS CHAPTER 1: 1.1 Muscular skeletal system Question - text book page 16 Using the information on pages 12 to 14 above, complete the table below. joint joint type articulating bones associated
CHAPTER 15: KINESIOLOGY OF FITNESS AND EXERCISE
 CHAPTER 15: KINESIOLOGY OF FITNESS AND EXERCISE KINESIOLOGY Scientific Basis of Human Motion, 12th edition Hamilton, Weimar & Luttgens Presentation Created by TK Koesterer, Ph.D., ATC Humboldt State University
CHAPTER 15: KINESIOLOGY OF FITNESS AND EXERCISE KINESIOLOGY Scientific Basis of Human Motion, 12th edition Hamilton, Weimar & Luttgens Presentation Created by TK Koesterer, Ph.D., ATC Humboldt State University
Bradley C. Carofino, M.D. Shoulder Specialist 230 Clearfield Avenue, Suite 124 Virginia Beach, Virginia Phone
 Rehabilitation following Arthroscopic Rotator Cuff Repair: Medium Tears Phase I: Immediate Postsurgical Phase (Days 10-14) Precautions: No lifting of objects; No excessive arm motions; No excessive external
Rehabilitation following Arthroscopic Rotator Cuff Repair: Medium Tears Phase I: Immediate Postsurgical Phase (Days 10-14) Precautions: No lifting of objects; No excessive arm motions; No excessive external
Performance Enhancement. Strength Training
 Performance Enhancement Strength Training Muscle Fiber type & Performance Slow twitch More efficient using oxygen to generate fuel for continuous extended muscle contractions Contract slowly, but continue
Performance Enhancement Strength Training Muscle Fiber type & Performance Slow twitch More efficient using oxygen to generate fuel for continuous extended muscle contractions Contract slowly, but continue
Basics of kinetics. Kinesiology RHS 341 Lecture 7 Dr. Einas Al-Eisa
 Basics of kinetics Kinesiology RHS 341 Lecture 7 Dr. Einas Al-Eisa Mass The amount of matter in an object Weight A force, which depends on the mass and acceleration Free-body analysis A technique of looking
Basics of kinetics Kinesiology RHS 341 Lecture 7 Dr. Einas Al-Eisa Mass The amount of matter in an object Weight A force, which depends on the mass and acceleration Free-body analysis A technique of looking
The Muscular System. Chapter 10 Part C. PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College
 Chapter 10 Part C The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.9: Muscles Crossing the Shoulder
Chapter 10 Part C The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.9: Muscles Crossing the Shoulder
Exploring the Rotator Cuff
 Exploring the Rotator Cuff Improving one s performance in sports and daily activity is a factor of neuromuscular efficiency and metabolic enhancements. To attain proficiency, reaction force must be effectively
Exploring the Rotator Cuff Improving one s performance in sports and daily activity is a factor of neuromuscular efficiency and metabolic enhancements. To attain proficiency, reaction force must be effectively
Lever system. Rigid bar. Fulcrum. Force (effort) Resistance (load)
 Resistance (load)") Lever system lever is any elongated, rigid (bar) object that move or rotates around a fixed point called the fulcrum when force is applied to overcome resistance. Force (effort) Resistance (load) R Rigid
Lever system lever is any elongated, rigid (bar) object that move or rotates around a fixed point called the fulcrum when force is applied to overcome resistance. Force (effort) Resistance (load) R Rigid
Handling Skills Used in the Management of Adult Hemiplegia: A Lab Manual
 Handling Skills Used in the Management of Adult Hemiplegia: A Lab Manual 2nd Edition Isabelle M. Bohman, M.S., P.T., NDT Coordinator Instructor TM Published by Clinician s View Albuquerque, NM 505-880-0058
Handling Skills Used in the Management of Adult Hemiplegia: A Lab Manual 2nd Edition Isabelle M. Bohman, M.S., P.T., NDT Coordinator Instructor TM Published by Clinician s View Albuquerque, NM 505-880-0058
Chapter 9: Exercise Instructions
 RESOURCES RESEARCHERS / MEDICAL HOW TO HELP SPONSORS GEHRIG CONNECTION MEDIA TELETHON MDA.ORG search our site Go MDA/ALS Newsmagazine Current Issue Home> Publications >Everyday Life With ALS: A Practical
RESOURCES RESEARCHERS / MEDICAL HOW TO HELP SPONSORS GEHRIG CONNECTION MEDIA TELETHON MDA.ORG search our site Go MDA/ALS Newsmagazine Current Issue Home> Publications >Everyday Life With ALS: A Practical
10/15/2014. Wrist. Clarification of Terms. Clarification of Terms cont
 Wrist Clarification of Terms Palmar is synonymous with anterior aspect of the wrist and hand Ventral is also synonymous with anterior aspect of the wrist and hand Dorsal refers to the posterior aspect
Wrist Clarification of Terms Palmar is synonymous with anterior aspect of the wrist and hand Ventral is also synonymous with anterior aspect of the wrist and hand Dorsal refers to the posterior aspect
Active-Assisted Stretches
 1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
Biceps Tenotomy Protocol
 Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
D: Doorway Stretch E: Towel Stretch for Pectoralis Minor Blackburn Exercises: 6 Positions A: Prone Horizontal Abduction (Neutral)
") D: Doorway Stretch Bring your shoulder into a horizontal position out to your side (abduction) and flex your elbow 90û Place your elbow against the edge of a doorway Lead forward and downwards with your
D: Doorway Stretch Bring your shoulder into a horizontal position out to your side (abduction) and flex your elbow 90û Place your elbow against the edge of a doorway Lead forward and downwards with your
Practical 2 Worksheet
 Practical 2 Worksheet Upper Extremity BONES 1. Which end of the clavicle is on the lateral side (acromial or sternal)? 2. Describe the difference in the appearance of the acromial and sternal ends of the
Practical 2 Worksheet Upper Extremity BONES 1. Which end of the clavicle is on the lateral side (acromial or sternal)? 2. Describe the difference in the appearance of the acromial and sternal ends of the
CLINICAL ASSESSMENT OF STABILITY DYSFUNCTION
 CLINICAL ASSESSMENT OF STABILITY DYSFUNCTION Dysfunction can be evaluated, quantified and compared against a normal measure, ideal standard or some validated benchmark. The measurement of dysfunction,
CLINICAL ASSESSMENT OF STABILITY DYSFUNCTION Dysfunction can be evaluated, quantified and compared against a normal measure, ideal standard or some validated benchmark. The measurement of dysfunction,
Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill Check- offs
 Evidence- Based Examination of the Shoulder Practice Session & Skills Check- offs Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill
Evidence- Based Examination of the Shoulder Practice Session & Skills Check- offs Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill
What is Kinesiology? Basic Biomechanics. Mechanics
 What is Kinesiology? The study of movement, but this definition is too broad Brings together anatomy, physiology, physics, geometry and relates them to human movement Lippert pg 3 Basic Biomechanics the
What is Kinesiology? The study of movement, but this definition is too broad Brings together anatomy, physiology, physics, geometry and relates them to human movement Lippert pg 3 Basic Biomechanics the
Biceps Tenotomy Protocol
 Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that has undergone
Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that has undergone
Rehab protocol. Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits. Goals:
 Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Chapter 11 The Muscular System. Copyright 2009, John Wiley & Sons, Inc.
 Chapter 11 The Muscular System Muscle Attachment Sites Skeletal muscles cause movements by exerting force on tendons, which pulls on bones or other structures. the attachment of a tendon to the stationary
Chapter 11 The Muscular System Muscle Attachment Sites Skeletal muscles cause movements by exerting force on tendons, which pulls on bones or other structures. the attachment of a tendon to the stationary
Section III: Concept 11: Muscular Fitness
 Section III: Concept 11: Muscular Fitness ١ Health Benefits of Muscular Fitness Include muscular strength and ٢ endurance Promote many health benefits Avoiding back problems Reducing risks of injury Reducing
Section III: Concept 11: Muscular Fitness ١ Health Benefits of Muscular Fitness Include muscular strength and ٢ endurance Promote many health benefits Avoiding back problems Reducing risks of injury Reducing
Type II SLAP lesions are created when the biceps anchor has pulled away from the glenoid attachment.
 Arthroscopic Superior Labral (SLAP) Repair Protocol-Type II, IV, and Complex Tears The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of
Arthroscopic Superior Labral (SLAP) Repair Protocol-Type II, IV, and Complex Tears The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of
Muscle Energy Technique
 PRACTICE SESSION: Muscle Energy Technique BE AN ARTIST and work out the best way for you to use the Muscle Energy Technique (MET). This technique works best when muscles are shortened. If you try MET on
PRACTICE SESSION: Muscle Energy Technique BE AN ARTIST and work out the best way for you to use the Muscle Energy Technique (MET). This technique works best when muscles are shortened. If you try MET on
BASIC ORTHOPEDIC ASSESSMENT Muscle and Joint Testing
 BASIC ORTHOPEDIC ASSESSMENT Muscle and Joint Testing The following tests are for the purpose of determining relative shortening, restriction or bind of muscle tissues. In this context the term bind in
BASIC ORTHOPEDIC ASSESSMENT Muscle and Joint Testing The following tests are for the purpose of determining relative shortening, restriction or bind of muscle tissues. In this context the term bind in
Anterior Labrum Repair Protocol
 Anterior Labrum Repair Protocol Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain scapular
Anterior Labrum Repair Protocol Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain scapular
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
Rehabilitation Guidelines for Large Rotator Cuff Repair
 Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Hands on Sports Therapy KNOWLEDGE REVIEW QUESTIONS 2004 Thomson Learning. Q1:From the following list of acronyms, write down the full title of each
 CHAPTER 09 Knowledge Review Q1:From the following list of acronyms, write down the full title of each treatment technique: NMT; PRT; SCS; FT; MET; PNF; PIR; RI; CRAC; INIT; ICT; ICCT. A1: NMT: Neuromuscular
CHAPTER 09 Knowledge Review Q1:From the following list of acronyms, write down the full title of each treatment technique: NMT; PRT; SCS; FT; MET; PNF; PIR; RI; CRAC; INIT; ICT; ICCT. A1: NMT: Neuromuscular
PROM is not stretching!
 Dx: o Right o Left Shoulder Replacement/Hemiarthroplasty Rehab Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: The intent
Dx: o Right o Left Shoulder Replacement/Hemiarthroplasty Rehab Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: The intent
Total Shoulder Rehab Protocol Dr. Payne
 Total Shoulder Rehab Protocol Dr. Payne Phase I Immediate Post Surgical Phase (0-4 weeks): Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase passive range of motion (PROM)
Total Shoulder Rehab Protocol Dr. Payne Phase I Immediate Post Surgical Phase (0-4 weeks): Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase passive range of motion (PROM)
Chapter 14 Training Muscles to Become Stronger
 Chapter 14 Training Muscles to Become Stronger Slide Show developed by: Richard C. Krejci, Ph.D. Professor of Public Health Columbia College 11.22.11 Objectives 1. Describe the following four methods to
Chapter 14 Training Muscles to Become Stronger Slide Show developed by: Richard C. Krejci, Ph.D. Professor of Public Health Columbia College 11.22.11 Objectives 1. Describe the following four methods to
"Locating & Feeling" the Muscles of your "Core"
 "Locating & Feeling" the Muscles of your "Core" To realize the full benefit of these exercises, it is important to sense the abdominal muscles that stabilize your "core". Starting position: Lie on your
"Locating & Feeling" the Muscles of your "Core" To realize the full benefit of these exercises, it is important to sense the abdominal muscles that stabilize your "core". Starting position: Lie on your
Core deconditioning Smoking Outpatient Phase 1 ROM Other
 whereby the ball does not stay properly centered in the shoulder socket during shoulder movement. This condition may be associated with impingement of the rotator cuff on the acromion bone and coracoacromial
whereby the ball does not stay properly centered in the shoulder socket during shoulder movement. This condition may be associated with impingement of the rotator cuff on the acromion bone and coracoacromial